Back to Journals » Advances in Medical Education and Practice » Volume 17
Development of a Simulation-Based Educational Intervention to Improve Nursing Competencies for Stroke Care in Southwestern Uganda
Authors Najjuma JN, Bajunirwe F ![]() , Ssedyabane F
, Ssedyabane F ![]() , Kaddumukasa M
, Kaddumukasa M ![]() , Mbalinda SN
, Mbalinda SN ![]() , Moore S, Tebulwa JB, Nankunda S, Atukunda EC
, Moore S, Tebulwa JB, Nankunda S, Atukunda EC ![]()
Received 11 April 2026
Accepted for publication 10 July 2026
Published 17 July 2026 Volume 2026:17 616139
DOI https://doi.org/10.2147/AMEP.S616139
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Sateesh Arja
Josephine N Najjuma,1 Francis Bajunirwe,1 Frank Ssedyabane,1 Mark Kaddumukasa,2 Scovia N Mbalinda,2 Shirley Moore,3 Joanita B Tebulwa,1 Shifra Nankunda,1 Esther C Atukunda1
1Faculty of Health Sciences, Mbarara University of Science and Technology, Mbarara, Uganda; 2College of Health Sciences, Makerere University, Kampala, Uganda; 3Frances Payne Bolton School of Nursing, Case Western Reserve University, Cleveland, OH, USA
Correspondence: Josephine N Najjuma, Faculty of Health Sciences, Mbarara University of Science and Technology, P. O Box 1410, Mbarara, Uganda, Email [email protected]
Introduction: Stroke is one of the leading causes of disability worldwide, and its prevalence is increasing in low- and middle-income countries (LMIC) like Uganda, presenting nursing care challenges. Simulation-based learning has been used successfully to train nurses in general care in LMIC but has not been applied to training for stroke care. In this study, we aimed to develop a simulation-based stroke care education intervention for nurses involved in care for patients with stroke at a large hospital in southwestern Uganda.
Methods: Between February 2024 and March 2025, we used the iterative design to develop an educational intervention for stroke care. We engaged stroke care content experts through in-depth qualitative interviews (n=14), generated content, and developed the first version of the intervention. Transcripts were derived, reviewed and coded to generate themes and categories using inductive content analytic approach. We then tested, analyzed and refined the intervention through three repetitive exposures of the intervention to final year Bachelor of Nursing students (n=20), with improvements after every exposure. That were grouped in teams of 5 students.
Results: Qualitative data from content experts revealed three thematic areas of patient care including admission of a stroke patient, care for a stroke patient during their hospital stay and discharge of a stroke patient as key content for consideration during intervention development. This content was integrated into the "Uganda Simulation-Based Nursing Stroke Care intervention”. Post-exposure qualitative interviews with final year Bachelor of Nursing students revealed great satisfaction with the intervention, improved preparedness and ease to assess stroke patients. There were also high teamwork scores and improved clinical skills. To maintain efficiency with stroke care competencies, they preferred at least three exposures to the intervention per year.
Conclusion: With diverse stakeholders, we used an iterative approach to develop a context specific, simulation-based stroke educational intervention. Future work will examine the feasibility, acceptability, and effectiveness of this intervention among nurses working with stroke patients and its effect on the patient outcomes.
Keywords: stroke care, simulation educational interventions, nursing, Uganda
Background
Stroke is the second commonest cause of mortality and disability in the world.1 The incidence and burden of stroke is increasing faster in low and middle income countries (LMIC) compared to resource rich countries.2,3 The annual incidence rate of stroke in Africa is 316 per 100,000 individuals.4 It is estimated that 70% of deaths from stroke and 87% of stroke-related disability occur in the LMIC setting.4
Given the rising burden of stroke, nurses working in stroke units require stroke specialist training and development of competencies in dealing with neurological emergencies plus working in multidisciplinary teams to manage stroke.5 Nurses are indispensable in the care for patients with stroke,6,7 and it is known that education and training not only enhance patients’ self-care abilities, nursing care outcomes and satisfaction but also have a positive impact on the knowledge, skills and practice of nurses.8 Educational theory suggests that experiential learning with colleagues in real-life settings may provide transferable results to the workplace with improved performance.
Simulation training has been shown to deliver experiential and situational training without compromising patient safety and has shown to improve both technical and non-technical skills.5 It is also known that simulation training provides transferable experiential learning and may improve clinical and non-clinical skills.5 Simulation is a teaching method that is described as “an engaging modality of medical education that leverages adult learning theory”.9 The approach has been used to train clinical skills, teamwork and communication and improve knowledge, and it is the preferred method for neurological assessment training.10 Simulation is increasingly being harnessed to enhance team and organization learning in different settings including pre-hospital and in-hospital settings.11
Whereas simulation-based learning has been applied in multiple clinical disciplines including trauma, surgery and midwifery,12,13 there is limited application in stroke care training. Nurses are an underutilized resource for care of stroke patients, and this is mostly due to their lack of knowledge and skills and other competencies for stroke care. Nurses involved in stroke care need to receive stroke specific training to align the core competencies.14 As critical members of interdisciplinary teams caring for stroke patients, nurses should be competent in addressing the holistic needs of stroke patients. However, there is a dearth of education interventions for stroke management targeting the nursing cadre. Whereas the barriers and facilitators of implementing the simulation-based education in stroke nursing have been studied by our team,15 there is no stroke specific simulation training. Therefore, the aim of this study was to develop a stroke simulation education intervention for nurses involved in stroke care in a hospital setting in a low resource setting, in southwestern Uganda.
Materials and Methods
Study Design
This study used the iterative development approach (Figure 1), utilizing mixed methods. We conducted the activities in three steps: 1) Key informant interviews among stakeholders to identify key priorities for nursing stroke patient care. These stakeholders included neurologists, emergency specialists, medical officers, nurses, physiotherapists, simulation experts and physicians, 2) Developed content for the simulation intervention and this was reviewed by content experts and simulation experts, 3) Pilot testing the intervention and obtaining feedback from for content refinement, through participant feedback, simulation facilitator feedback and exit interviews with final year Bachelor of Nursing students that were exposed to the different versions of the intervention. We tested the intervention among final year nursing students who were in their last semester since they had exposure to stroke nursing care at the hospital for which the intervention was designed for, and because of their prior exposure the simulation they would give constructive feedback for the intervention.
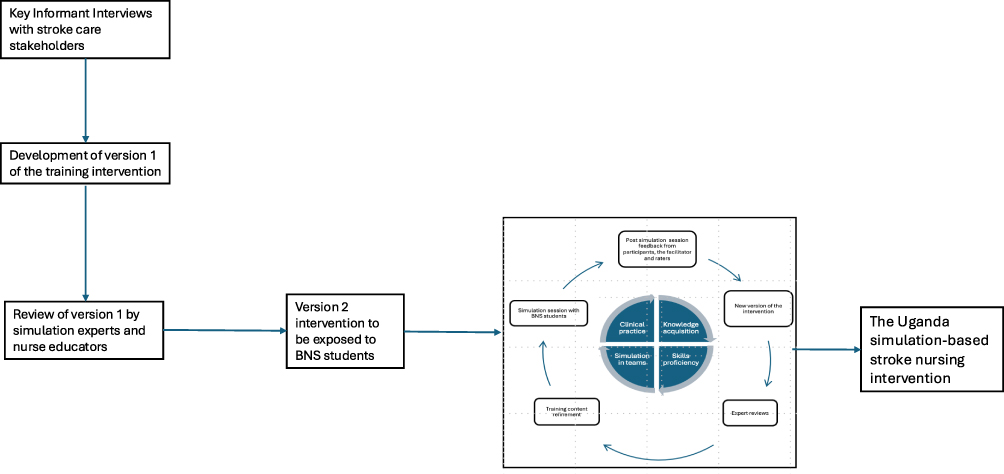 |
Figure 1 Iterative development of the simulation-based stroke nursing intervention. |
Study Setting
The study was conducted at the Simulation center of Mbarara University of Science and Technology (MUST), located in southwestern Uganda. The simulation center was established in 2016 and has two scenario execution laboratories and one debriefing room. The space is available for teaching and learning for pre-service and in-service health care professionals. The simulation center is usually scheduled for Bachelor of nursing and Bachelor of medicine and surgery students to attend simulations. The simulation center has staff that run the scenarios, and these include both technical/trained simulation facilitators and non-technical staff. The non-technical staff include the information technology officer as well as the patient actors.
Sampling and Recruitment of Participants
We purposively selected stakeholders including nurses, physicians, educators and other health care providers involved in stroke care. For students, we used systematic sampling method. We also recruited final year Bachelor of Nursing Students with vital and diverse experience and knowledge about simulation-based learning and stroke care. They were recruited through their class leader, to participate in the scenario testing. Contact with participants was initiated by a trained research assistant, who arranged for interviews after obtaining their written informed consent.
Data Collection
Stakeholder Interviews
For the formative interviews, we interviewed individuals involved in stroke care and stroke education at Mbarara Regional Referral Hospital (MRRH) and Mbarara University of Science and Technology (MUST). The aim of the interviews was to understand the current priorities of stroke nursing care and what the stroke nursing care training content should entail. We purposively selected individuals that had more than one year of experience working with stroke, who were nurses or/and had experience worked with nurses in their units/wards. We excluded individuals that were working with stroke patients but did not work with nurses. We used an interview guide that was developed by the researcher using the available literature on stroke nursing care and simulation education. The interview guide was tested with stroke care specialist and a nurse educator that were not part of the study population. Data on stroke nursing care priorities and competencies was collected. We used probes to elicit details corresponding to each of the highlighted topics. The interviews were carried out by a trained and experienced qualitative researcher with a nursing background. The interviewer was not part of the study team. Field notes were collected and included in each of the individual debrief notes by research assistants. We continuously reviewed emerging content together to refine the interview questions and add new potential probes. Demographic information: age, gender, profession, years of experience, highest level of education – were collected to describe our study sample. We included 14 participants until saturation was achieved.16 The interviews were recorded verbatim and transcripts analyzed manually using thematic analysis.17
Content Development
The simulation training content was done to educate, support, prepare and motivate nurses to engage in care for stroke patients and eventually improve the outcomes of stroke patients. We engaged five (5) different stakeholders (not previously interviewed) including stroke health care providers, educators, nurse leaders and simulation experts of both nursing and medical background to develop relevant content for the simulation training around the Health Care Providers (HCP) identified categories/themes identified from previous interviews. The objectives of the scenarios were guided by bloom’s taxonomy that categorizes the objectives into cognitive (knowledge), affective (attitude) and psychomotor (skills) domains.
The scenarios were developed using the MUST Simulation center scenario development guidelines and scenario template and were pre-designed to cover the three thematic areas identified by the key informants, and these were as follows: i) Nursing care for stroke patient admission to the hospital, ii) Nursing care for an inpatient stroke patient and iii) Nursing care given to stroke patients at discharge. During scenario execution, we used a manikin with a trained and experienced actor that played the role of either the patient or caretaker/family member.
Prototype Design
We worked with a simulation educationist with vast experience in developing simulation educational content as well as an implementation science specialist also experienced in developing user-centered interventions. We developed the first draft of simulation-based stroke educational intervention aimed to improve stroke care competencies among nurses. The first version of the scenarios was reviewed before they were tested on the nursing students’ teams by the 4 simulation experts. These 4 simulation experts included 2 medical doctors with 3 and 5 years of simulation experience respectively. The 2 nurses that had 3 and 6 years of simulation experience, respectively. The simulations were guided by Kolb’s experiential learning theory, which provides a framework for engaging learners, reflecting on observations, abstract conceptualization and active experimentation.18
Intervention Refinement
We recruited 20 final year Bachelor of nursing students, divided them in sets of 5 and exposed them to the intervention. Three sets of five students were exposed to all scenarios and one group only completed one scenario. There data was not included in the final analysis. All participants had undergone clinical rotations in the units where stroke patients are admitted at the Mbarara Regional Referral Hospital, the teaching hospital for Mbarara University of Science and Technology. Each group of 5 students was exposed to all three scenario-set (iteration 1). After each iteration, the facilitator and feedback collected from the students and the facilitator, the simulation experts and stroke care experts, reviewed the feedback and incorporated it in the subsequent version. The aim was to obtain feedback and improve the flow, clarity and objectives of the scenarios for the intervention and enable us to improve it progressively. We held three iterations with qualitative interviews after every group. These interviews were conducted using interview guides developed using constructs from the PEARLS framework19 and post simulation questions that had been used previously by Metha 2018.20 During the refinement process, the three components of simulation exposure (pre-brief, scenario execution and debrief) took place within one hour per scenario. The students maintained their groups throughout the study and were exposed to all three scenarios on different days. They were exposed to the scenarios in the same order, 1. Admission of the stroke patient, 2. Care for a stroke patient and 3. Discharging a stroke patient.
We used an iterative approach in the development in the development the Uganda-simulation stroke nursing training/intervention. This constituted the pilot testing of the simulation-based experience before full implementation, a final step in the best practices for Healthcare simulation standards of Best Practice: Simulation design.21
Data Collection Tools
We used clinical skills checklist and clinical teamwork score, which had already been validated for use in Uganda. At the end of every simulation session, all participants were debriefed and gave feedback using the Promoting Excellence And Reflective Learning in Simulation (PEARLS) framework.19 Clinical skills checklist and Clinical Teamwork scale22 has been used previously in our local setting.23
Data Management and Analysis
We described the demographics of all the qualitative and iterative process participants using descriptive statistics. Quantitative data from post-simulation feedback forms and checklists were analyzed and summaries presented as frequencies and proportions in tables.
The aim of the qualitative data analysis was to inductively construct categories that identify the preferred content tailored for the simulation-based stroke educational intervention aimed to improve stroke care competencies among nurses. We constructed categories through repeated review of transcripts by two members of the research team (FS, ECA) to identify relevant content, which served as the basis for developing a code book. The rest of the transcripts were coded by research assistants using the developed code book, aided by the qualitative data management software, NVivo 12. We iteratively reviewed, sorted and analyzed data using inductive content analysis approach.24 Descriptive labels and elaborating verbatim text to define and specify each category’s meaning, plus illustrative quotes from the key informant interview data were included. For the refinement phase, data on clinical skills and teamwork checklists were summarized using frequencies and proportions and means with standard deviations, respectively.
Ethics Consideration
All methods were carried out in accordance with the relevant ethics guidelines for conducting research in Uganda. Before the data collection, the research protocol was submitted for ethical review at the MUST Research Ethics Committee (MUST-2023-1157). The study also received clearance from the Uganda National Council of Science and Technology (HS3535ES). All participants provided written informed consent before taking part in the research activities. Participants also provided consent for audio-recording of the interviews. Participants informed consent included publication of anonymized responses/direct quotes. Each participant was given a unique identifier. Only participant identification numbers were included in the transcripts. All study data was collected in password protected laptop that is only accessed by the study team.
Results
We conducted a total of 14 key informant interviews among key stroke care stakeholders. All of them had worked in stroke care for at least 1 year, 57% of the participants were male. About 50% were nurses, 28% were medical doctors and 21% were physiotherapists. Close to 70% (10/14) had attained at least a bachelor’s degree in health-related disciplines, and others had a diploma and a certificate education.
Qualitative Results from KIIs
Participants were optimistic about the simulation-based stroke intervention and emphasized that the intervention may improve stroke care outcomes, especially if the intervention is context specific and aims at using the available resources in LMICs. The stakeholders observed that if nurses are exposed to simulation that cover the three themes or major care points including i) Nursing care for stroke patient admission to the hospital, ii) care for an inpatient stroke patient and iii) discharging a stroke patient, this may improve care. The themes and codes are summarized in Table 1. It was generally agreed that since stroke care requires a multidisciplinary team, teamwork and communication with patients, care takers and other professionals should be emphasized.
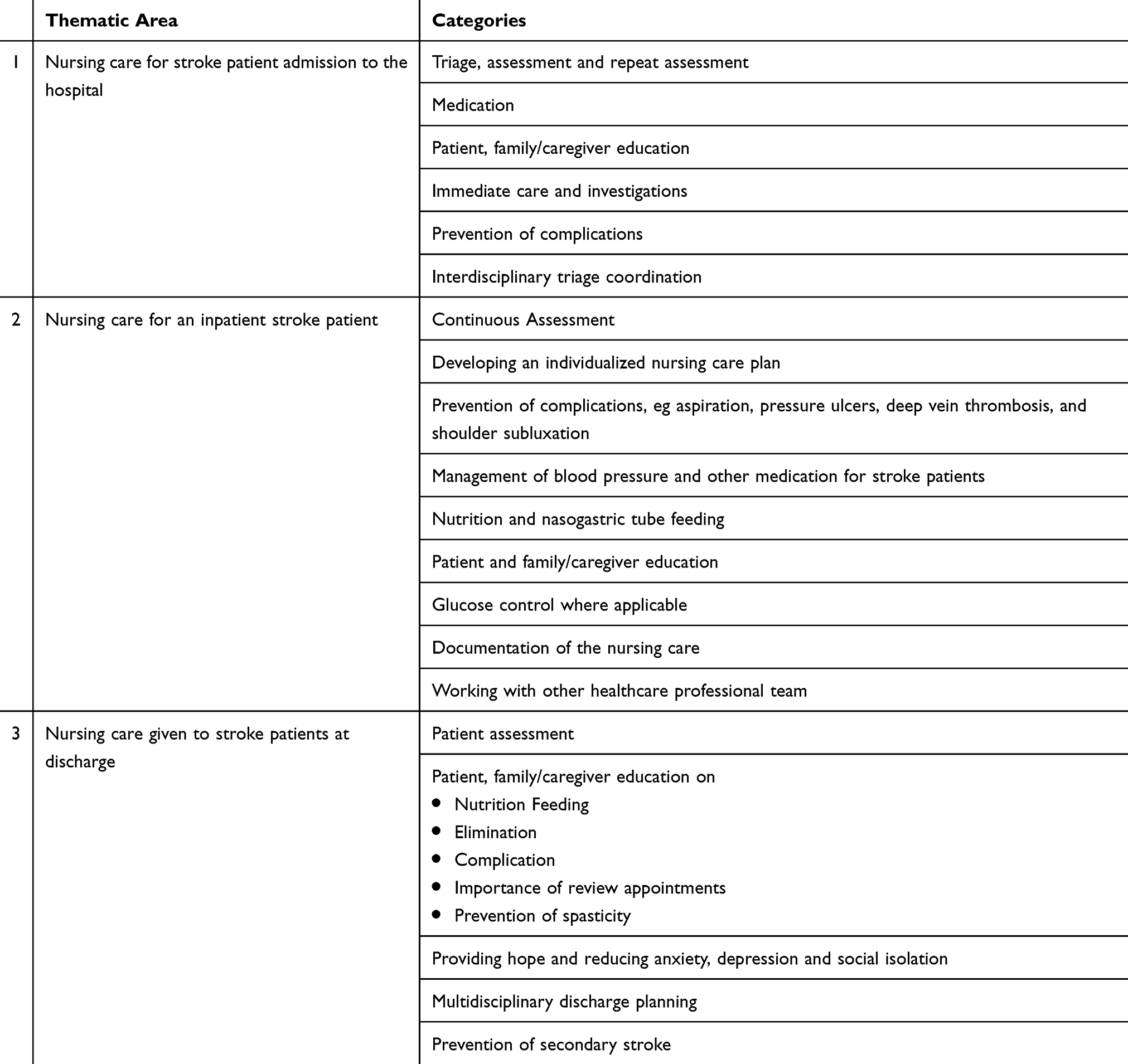 |
Table 1 Summary of Qualitative Results |
Nursing Care for Stroke Patient Admission to the Hospital
Stakeholders believed that the admission of patients that came to the hospital with signs of stroke was very important. Nurses play an important role in patient admission, thus understanding their roles and responsibilities for patients that report to hospital and are admitted with signs of stroke was identified as important.
According to Participant 2;
…. The nurses work with the rest of the teams. the resident doctors outline something called first hugs in bed. It’s a mnemonic that manages critically ill patients and this entails having catheters, a feeding plan, NG tubes in situ, turning the patient, thrombolysis. And when you look at this first hugs in bed, it caters for this patient who, for instance, might not from time to time be able to turn himself and has a risk of secondary insults in the body that can worsen the outcome. So, the nurses should come in to assess patient, interpret and implement what we have written down by resident doctors. (Male, Medical Doctor)
The other roles of nurses at admission included giving treatments to the suspected cause of the stroke, patient and family education, and neurological assessment. These assessments will continuously be done to assess for any improvements or deterioration.
At admission giving the patients treatment for whatever is the cause of the stroke. So if it is oral meds, giving the treatment and teach the family what to do, the patient’s family do most of the giving. Nurses should also do neurologic assessment. To assess the level of paralysis and see improvements. Nurses should also assess NG tubes, talking to the attendants to turn them and prevent ulcers, pressure ulcers. That’s basically it. And elimination. (Participant 4, Female Physiotherapist)
Nursing Care for an Inpatient Stroke Patient
It was emphasized that during admission nurses spend more time with the stroke patients compared to other health care professionals, and their roles and responsibilities contribute a lot to the patient outcomes. Participants recognized that for stroke patients, nurses work around the clock to prevent any complications.
Participant 2 said
The care is really to prevent symptoms, prevent aspiration, prevent infection, and prevent contractures. Give treatment, antibiotics. If they have been on antiplatelet aspirin, they continue. If they have been on these other drugs for lipid reduction, they can continue. Basically, that is what they do. (Participant 2, Male medical Doctor)
It was also emphasized that nurses are involved in providing nursing care that include the activities of daily living including bed bath, feeding plus providing medication for patients.
These days, we find nurses turning patients in bed uh is it called bed baths, because today I saw some trying to bathe the patients. They administer drugs which have been prescribed. They also teach caretakers how to feed. (Participant 9, Male, Medical doctor)
Participants emphasized that depending on the assessment some stroke patients might be stable on ward, and continuous nursing care should be emphasized for such patients not to deteriorate. Participant 7 emphasized the need for continuous nursing care even when the patient has improved.
If this is not done, you may find urine bags on the bed. In some cases when the patient starts to gain some consciousness, start to talk, they may be neglected because there they are not receiving much of the medication, no longer on an IV line. The physician is still monitoring and writes to monitor the vitals 2hourly, but the vitals will not be monitored by the nurses. The nurses are asked why they are not monitoring the patient, and their reason is that one is already fine. The patient is already getting UTIs. (Participant 7, Male nurse)
Nursing Care Given to Stroke Patients at Discharge
It was emphasized by participants that it is very important that nursing care at discharge is given the required attention. This is because most of the patients are discharged to go home and live with their family members who might not be aware of the care that the patient requires. Participants emphasized the importance of patient and family/caregiver education on the care for activities of daily living, giving hope to the patient, medication, preventing of complications and a recurrent stroke and how identify this and attending review clinics with the physicians and rehabilitation specialists.
About patient education at discharge, participant 5 said;
Discharge, the nurses will give instructions to the caregivers on mainly medications, because the nurses are responsible for how the patient gets the medicines, how they are responding to it and all that. And they work hand in hand with the doctors. So, upon discharge, the doctor usually gives all the instructions to the nurse. The nurse has the responsibility of explaining all the details to the patient, explain how medications will be taken, explain how they will go and the care that they need to continue with from home. (participant 5, Male Nurse)
For prevention of complication like contractures, secondary stroke and pressure ulcers, it was emphasized that nurses should provide health education.
Stroke patients should not be discharged like any other patients. They need physiotherapy which comes in and should continuously review the patient. These patients and the relatives are trained to do the continuous physiotherapy to cub the contractures. And told the importance of the drugs these patients may continue. And when to refill the medicines. And to prevent complication like another stroke and pressure ulcers among others. Then health education, you find the nurses do not give the health education to the patients about the cause of the stroke. They should provide health education on the management and the care of those conditions. Telling them the signs and symptoms in case they are approaching or going into the crises. (Participant 6, Male, physiotherapist)
The interviews indicated that it is important to link patients to other facilities where they can receive physiotherapy, prevention of a secondary stroke education should be reemphasized by nurses at discharge. One of the participants said;
Nurse should discuss the option of linking stroke patients to a nearby facility near their home so that they can do rehabilitation, and where applicable provide the number when you reach you can be able to call them… nurses should participate in both planning discharge and its implementation. (Participant 14, Male, Nurse)
Working with other health care team members to assess the patient and provide discharge education to family/caregiver and the patient.
On discharge, when the team is satisfied that this patient is out of danger, then, they discharge. Now, what is our role as nurses on discharge? Still health education on; body hygiene, two hourly returning, physiotherapy – for avoiding the contractures from developing. What makes the body parts function? We gain the strength and then they feed him on what, what kind of feeds, how much to give. (Participant 8, Male, Medical doctor)
Other component of health education for the family members was the emphasis on return to normal activities and psychosocial care.
You know, we teach these caregivers to be with the stroke, to have time with them. Not abandon them, just dump them in the bed and go away, all day. We are like, be, talk to them, occupy them, show them there is hope, okay? (Participant 13, female, Nurse)
Another participant emphasized that the nurse should make sure that the family members have understood all the education given. These aspects of the education included activities of daily living, nutrition and the does and don’ts of stroke care. One of the doctors said:
The nurse has taught the caretaker that has really understood that this patient, this is how we are going to care about him or her, this is how we are going to feed him or her. So, you they make sure I see they make sure that the if a caretaker is well cooperative learn them show that they have understood, they let them go and continue with the care at home. (Participant 10, Male, Medical Doctor)
The Intervention
The intervention covers content on different competencies including knowledge, clinical skills, confidence, communication and teamwork. The intervention is broad enough to cover all competencies but also brief enough to be covered in one hour. This intervention “Uganda Simulation-Based Nursing Stroke Care intervention” was prepared as three hard-copy scenario scripts, representing the three thematic areas, just like other simulation scenario scripts, ready for refinement. The “Uganda Simulation-Based Nursing Stroke Care intervention” is summarized in Table 2.
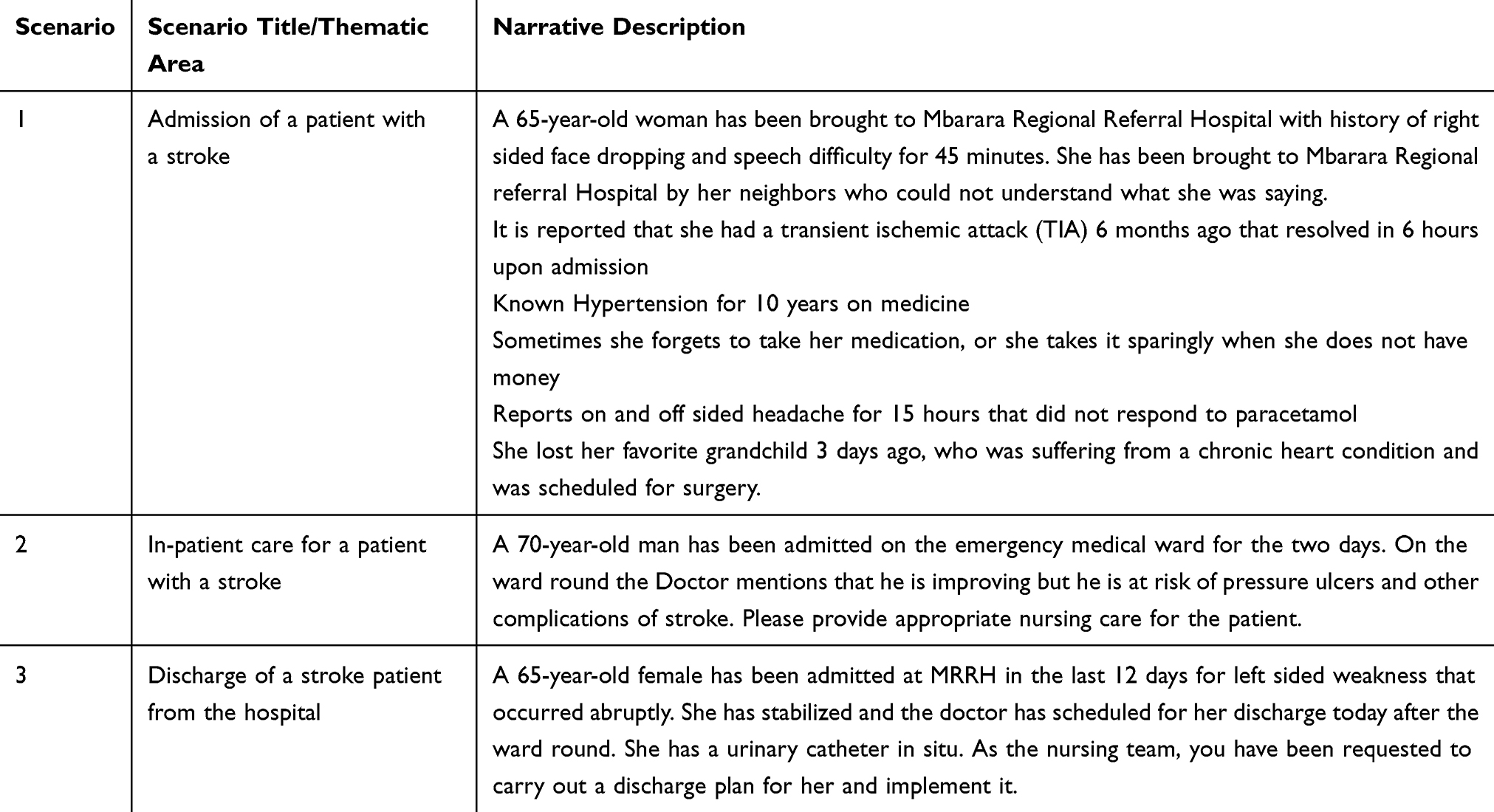 |
Table 2 Simulation Clinical Scenarios for Uganda Simulation-Stroke Nursing Training |
Scenario Exposure Results from the Nursing Students
Demographics
A total of 20 nursing students were enrolled in the study, whose mean age was 23 years, and all had prior exposure to at least 5 simulations. They all had completed medical-surgical nursing courses and had rotated on the wards where stroke patients are admitted at MRRH.
Teamwork and Communication Skills
During the refinement of developed intervention, the mean scores of the CTS improved with every iteration. This was observed across all simulation scenarios, with the least mean score being 8.3, as seen in Table 3.
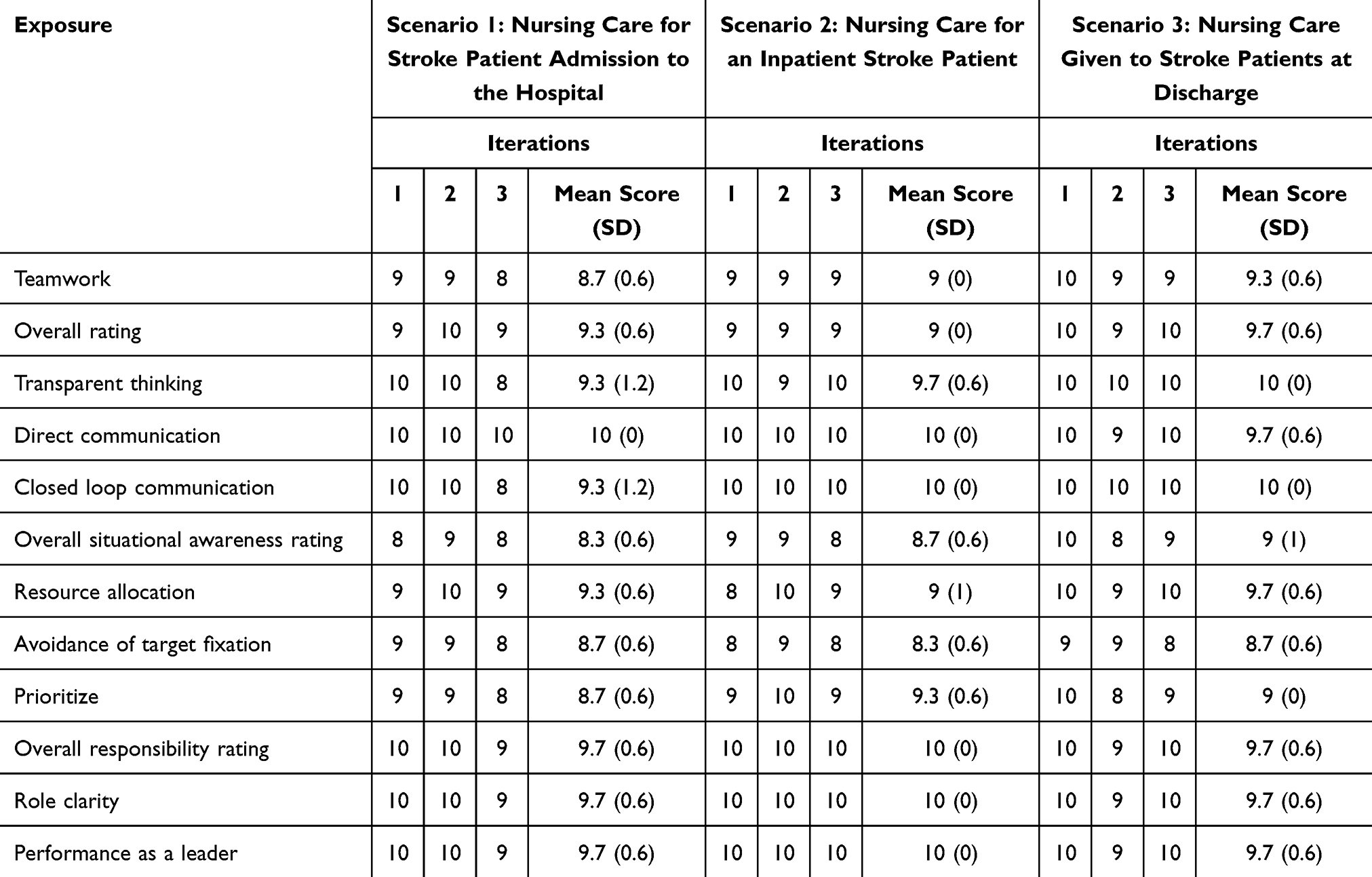 |
Table 3 Pilot Testing of Nursing Students’ Teamwork and Communication Skills |
Clinical Skills
During the intervention refinement, nursing students portrayed improved scores in clinical skills by the time they finished the third iteration. Specifically, nursing students scored 95%, up from 70% in the thematic area of nursing care for stroke patient admission to the hospital. Details of the scores in clinical skills are shown in Table 4.
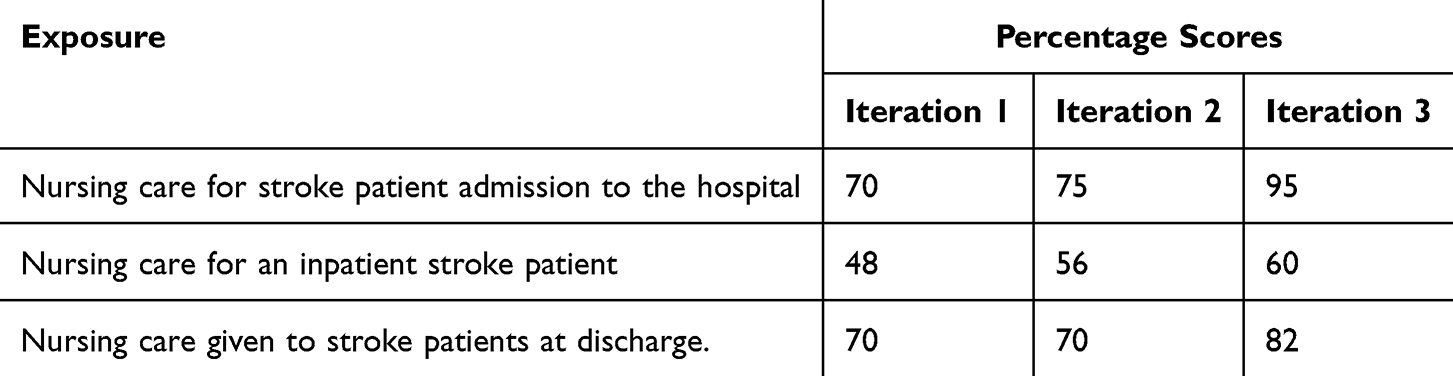 |
Table 4 Pilot Testing of Nursing Students’ Clinical Skills |
Discussion
This study describes the process of developing and testing the training intervention for nurses using the iterative process. We used qualitative methods to identify training competencies and priorities for stroke nursing care. The three thematic areas and simulation scenarios developed for the “Uganda Simulation-Based Nursing Stroke Care intervention”. Through the iterative process, we collected feedback, tested and refined the intervention as we assessed it. The three themes were admission of a stroke patient, care for a stroke patient during their hospital stay and discharge of a stroke patient as key content for consideration during intervention development.
We developed this first ever Uganda Simulation-based nursing care intervention owing to the fact that other training interventions have been developed in developed countries.8 We used the simulation-based methodologies which are known to be preferred by nurses and hence improving overall health care provider competencies.25
The Uganda Simulation-based nursing care intervention was developed with context specific stroke care content. Interventions developed using context specific approaches have been shown to be relevant and effectiveness in respective populations.26 Moreover, the Knowledge-to-Action framework emphasizes that evidence-based interventions should be adapted to the local context to improve uptake, relevance and effectiveness.27 This shows the highly likely effectiveness, acceptability and feasibility of this Uganda Simulation-based nursing care intervention to improve nursing stroke care in Uganda and related populations.
The Uganda Simulation-based nursing care intervention caters for the three major in hospital categories of nursing care. These include admission, inpatient care and discharge of a stroke patient. If a nurse is trained in all these aspects, they become equipped with the competencies to care for patients in whichever ward they are posted, which fit into the working dynamics of nurses in LMIC where they are rotated randomly.
The content of all the scenarios, caters for the five sequential steps of the nursing process for a stroke patient: Assessment, Diagnosis, Planning, Implementation and Evaluation. This has been shown to improve outcome since individualized planned care is provided. It also covers content related to teamwork and communication. This helps in interprofessional care which is essential in delivering care for stroke patients.28 This shows the likely possibility for this intervention enhancing interprofessional collaboration and eventually improving stroke patient outcomes.
The major strength of this study is that the content development was not limited to nurses alone, but rather other stakeholders including neurologists, emergency medicine physicians, medical officers, physiotherapists and simulation experts. This multidisciplinary approach significantly enhances the clinical accuracy and validity of the intervention. We used the PEARLS framework which is widely considered the gold standard in the simulation literature for post simulation debriefing.
Our design has some weaknesses. The study did not include the views of the patients in the development. We developed the intervention using nursing students as participants who may have recently had lectures on stroke care and other exposures in simulation that might have influenced their acceptance to participate in the study and their scores in clinical skills, and teamwork and communication. This has been explained in the circle of learning, that other teaching and exposures enhance learning. The study was carried out in one site, although we included views for both pre-service and in-service nurses. We are proposing a future study to test the intervention among in-service nurses. We only had three iterations, and thus we had a small sample size that we were not able to carry out inferential statistics.
Conclusions and Recommendations
We developed the Uganda Simulation-based nursing care intervention using context specific content from different stakeholders. The intervention showed improvement in clinical skills and teamwork and communication. We recommend future studies to assess the effectiveness of the intervention on in-services nurses’ clinical skills and teamwork and communication as well as stroke patient outcomes. We also recommend exploring the possibilities of integrating the intervention into the hospital staffing policies, continuous nursing education, undergraduate nursing curriculum and stroke care protocols in Uganda and similar settings.
Acknowledgments
We acknowledge the staff of Mbarara University of Science and Technology and the Simulation FOR Life program. The authors would like to acknowledge the students that participated in the study and the experts for the review. Many thanks to the research assistants Ms. Sarah Mwijukye, Ms. Brenda Arinaitwe, and Ms. Gerald Mwebembezi for the contribution to this work.
Funding
Research reported was partly supported by the National Institute of Neurological Disorders and Stroke of the National Institutes of Health under Award Number R01NS118544. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Feigin VL, Abate MD, Abate YH, et al. Global, regional, and national burden of stroke and its risk factors, 1990–2021: a systematic analysis for the global burden of disease study 2021. Lancet Neurol. 2024;23(10):973–12.
2. Feigin VL, Nichols E, Alam T; GBD-2016 Neurology C. Global, regional, and national burden of neurological disorders, 1990-2016: a systematic analysis for the global burden of disease study 2016. Lancet Neurol. 2019;18(5):459–480. doi:10.1016/S1474-4422(18)30499-X
3. Okekunle AP, Jones S, Adeniji O, et al. Stroke in Africa: a systematic review and meta-analysis of the incidence and case-fatality rates. Int J Stroke. 2023;18(6):634–644. doi:10.1177/17474930221147164
4. Akinyemi RO, Ovbiagele B, Adeniji OA, et al. Stroke in Africa: profile, progress, prospects and priorities. Nat Rev Neurol. 2021;17(10):634–656. doi:10.1038/s41582-021-00542-4
5. Roots A, Thomas L, Jaye P, Birns J. Simulation training for hyperacute stroke unit nurses. Br J Nurs. 2011;20(21):1352–1356. doi:10.12968/bjon.2011.20.21.1352
6. Cheng W, Tu J, Shen X. Registered nurses’ role experiences of caring for older stroke patients: a qualitative study. BMC Nurs. 2021;20(1):96. doi:10.1186/s12912-021-00626-y
7. Burton CR. A description of the nursing role in stroke rehabilitation. J Adv Nurs. 2000;32(1):174–181. doi:10.1046/j.1365-2648.2000.01411.x
8. Zhao Y, Xu Y, Ma D, et al. The impact of education/training on nurses caring for patients with stroke: a scoping review. BMC Nurs. 2024;23(1):90. doi:10.1186/s12912-024-01754-x
9. Albin CSW, Greene JP, LaHue SC, et al. Reviews in medical education: advances in simulation to address new challenges in neurology. Neurol Educ. 2023;2(1):e200042. doi:10.1212/NE9.0000000000200042
10. Bae KS, Roh YS. Training needs analysis of Korean nurses’ neurological assessment competency. Nurs Health Sci. 2020;22(1):99–107. doi:10.1111/nhs.12654
11. Gormley GJ, Carr D, Murphy P, Tallentire VR, Smith SE. Unlocking the learning potential of simulation-based education. Br J Hosp Med. 2023;84(12):1–8. doi:10.12968/hmed.2023.0353
12. Hashmi Y, Ayyaz N, Umar H, Jawaid A, Ahmed Z. Are trauma surgery simulation courses beneficial in low-and middle-income countries—a systematic review and meta-analysis. Trauma Care. 2021;1(3):130–142. doi:10.3390/traumacare1030012
13. Jolly L, Ooms A, Ransome H. Student midwives’ experiences of high-fidelity simulation in midwifery education in the university setting: a qualitative systematic review. Nurse Educ Today. 2025;152:106779. doi:10.1016/j.nedt.2025.106779
14. Nelson ML, MacEachern E, Prvu Bettger J, et al. Exploring the inclusion of person-centered care domains in stroke transitions of care interventions: a scientific statement from the American heart association. Stroke. 2024;55(6):e169–e181. doi:10.1161/STR.0000000000000462
15. Najjuma JN, Bajunirwe F, Mbalinda SN, et al. Barriers and facilitators of simulation-based education in stroke nursing management at a regional referral hospital in Southwestern Uganda: a qualitative study. Adv Med Educ Pract. 2025;16:1317–1329. doi:10.2147/AMEP.S535086
16. Braun V, Clarke V. To saturate or not to saturate? Questioning data saturation as a useful concept for thematic analysis and sample-size rationales. Qual Res Sport Exerc Health. 2019;13:1–16.
17. Braun V, Clarke V. Using thematic analysis in psychology. Qual Res Psychol. 2006;3(2):77–101. doi:10.1191/1478088706qp063oa
18. Kolb DA. Experiential Learning: Experience as the Source of Learning and Development. New Jersay: Pearson Education Inc; 2015.
19. Eppich W, Cheng A. Promoting excellence and reflective learning in simulation (PEARLS): development and rationale for a blended approach to health care simulation debriefing. Simul Healthc. 2015;10(2):106–115. doi:10.1097/SIH.0000000000000072
20. Mehta T, Strauss S, Beland D, Fortunato G, Staff I, Lee N. Stroke simulation improves acute stroke management: a systems-based practice experience. J Graduate Med Educ. 2018;10(1):57–62. doi:10.4300/JGME-D-17-00167.1
21. Committee IS, Watts PI, McDermott DS, et al. Healthcare simulation standards of best practiceTM simulation design. Clin Simul Nurs. 2021;58:14–21. doi:10.1016/j.ecns.2021.08.009
22. Guise J-M, Deering SH, Kanki BG, et al. Validation of a tool to measure and promote clinical teamwork. Simul Healthc. 2008;3(4):217–223. doi:10.1097/SIH.0b013e31816fdd0a
23. Data S, Dubé MM, Bajunirwe F, et al. Feasibility of an interprofessional, simulation-based curriculum to improve teamwork skills, clinical skills, and knowledge of undergraduate medical and nursing students in Uganda: a cohort study. Simul Healthc. 2020;16(6):e100–8.
24. Elo S, Kyngäs H. The qualitative content analysis process. J Adv Nurs. 2008;62(1):107–115. doi:10.1111/j.1365-2648.2007.04569.x
25. Mishra R, Trivedi D, Trivedi D. Simulation-based learning in nursing curriculum- time to prepare quality nurses: a systematic review and meta-analysis. Heliyon. 2023;9(5):e16014. doi:10.1016/j.heliyon.2023.e16014
26. Damschroder LJ, Aron DC, Keith RE, Kirsh SR, Alexander JA, Lowery JC. Fostering implementation of health services research findings into practice: a consolidated framework for advancing implementation science. Implement Sci. 2009;4(1):50. doi:10.1186/1748-5908-4-50
27. Graham ID, Logan J, Harrison MB, et al. Lost in knowledge translation: time for a map? J Contin Educ Health Prof. 2006;26(1):13–24. doi:10.1002/chp.47
28. Summers D, Leonard A, Wentworth D, et al. Comprehensive overview of nursing and interdisciplinary care of the acute ischemic stroke patient: a scientific statement from the American heart association. Stroke. 2009;40(8):2911–2944. doi:10.1161/STROKEAHA.109.192362
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.