Back to Journals » Risk Management and Healthcare Policy » Volume 19
Development of a Risk Prediction Model for Post-Stroke Functional Recovery Based on Clinical and Nursing Factors
Received 20 March 2026
Accepted for publication 11 May 2026
Published 27 May 2026 Volume 2026:19 609869
DOI https://doi.org/10.2147/RMHP.S609869
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Keon-Hyung Lee
Ruilin Sun,* Zhaojun Liu*
Stroke Center, Affiliated Second Clinical Hospital, Harbin Medical University, Harbin, Heilongjiang, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Ruilin Sun, Stroke Center, Affiliated Second Clinical Hospital, Harbin Medical University, No. 246, Xuefu Road, Nangang District, Harbin, Heilongjiang, 150001, People’s Republic of China, Email [email protected]
Objective: This study aimed to develop and validate a risk prediction model for unfavorable functional recovery at 6 months after stroke, incorporating clinical and modifiable nursing-related predictors to support early risk stratification and individualized nursing interventions.
Methods: A retrospective cohort study included 1340 stroke patients from a tertiary hospital. Demographic, clinical, imaging, nursing, and psychosocial data were collected. The dataset was split into training and testing sets at a 7:3 ratio using outcome-stratified sampling. Univariate analysis and multivariable logistic regression were used as a predictor screening procedure. A nomogram-based risk prediction model was developed and evaluated for discrimination, calibration, and clinical utility. Patients were further stratified into low-, intermediate-, and high-risk groups based on predicted probability tertiles from the training set.
Results: Older age, prior stroke history, comorbidity burden, longer onset-to-admission time, greater neurological deficit severity, lower Glasgow Coma Scale score, and brainstem lesions were independent predictors of unfavorable recovery. Early out-of-bed mobilization within 48 hours, higher self-management behavior score, absence of depressive symptoms, and better social support were linked to reduced risk. The model showed good discrimination and calibration in both sets. Risk stratification showed a stepwise increase in unfavorable recovery rates across the three risk groups. Decision curve analysis indicated net clinical benefit within a reasonable threshold probability range.
Conclusion: The developed model combines clinical and modifiable nursing-related predictors and demonstrates good predictive performance. It may serve as a practical tool for early risk stratification and targeted nursing interventions in stroke patients.
Keywords: stroke, functional recovery, nursing-related predictors, early risk identification, rehabilitation management
Introduction
Stroke places a substantial burden on patients and health care systems worldwide. Despite advances in acute management, functional outcomes after discharge remain highly heterogeneous, and a notable proportion of patients continue to experience activity limitations that impair daily functioning and social participation.1–3 Therefore, identifying individuals at high risk of poor recovery early after stroke and applying targeted interventions remains a key issue in stroke rehabilitation and nursing management. Functional recovery after stroke is affected by many factors.4 Clinical characteristics such as age, stroke severity, lesion location, and comorbidity burden have been confirmed to relate closely to prognosis, yet most of these features are not modifiable or are difficult to change in a short period.5–7 In recent years, increasing attention has been given to the roles of nursing behaviors, patient self-management capacity, and psychosocial factors during rehabilitation. Elements such as early mobilization, rehabilitation adherence, emotional status, and social support may influence long-term outcomes by affecting rehabilitation engagement and neural recovery processes.8 Nevertheless, existing studies often focus on one or only a few nursing factors, and analyses that integrate clinical, nursing, and psychosocial variables in one framework remain limited. Against this background, risk prediction models have become important tools for outcome assessment after stroke. Prediction models based on multivariable regression can stratify risk early and support clinical decision-making.9 However, many previous models mainly emphasize medical indicators, underuse the potential value of nursing and behavioral factors, and some tools show limited practicality, which restricts their application in nursing practice. For these reasons, building a model that combines clinical features with modifiable nursing factors is meaningful for guiding targeted nursing interventions after stroke.
Accordingly, this retrospective cohort study collected demographic, clinical, imaging, nursing, and psychosocial measures in patients with stroke. A risk prediction model for unfavorable functional recovery after stroke was developed and validated by combining clinical and modifiable nursing-related predictors. Patients were further assigned to risk groups based on predicted probabilities. The model was presented as a nomogram, and its discrimination, calibration, and decision curve performance were assessed. This study aimed to provide evidence for early risk stratification and individualized nursing interventions in patients with stroke. The results may support decision-making in nursing assessment and rehabilitation management.
Participants and Methods
Participants
A retrospective cohort study was conducted at a single tertiary hospital. Consecutive patients with stroke admitted between January 2024 and December 2024 were included. Clinical data were retrieved from the electronic medical record system. Inclusion criteria were: (1) age ≥ 18 years; (2) diagnosis of stroke based on established diagnostic criteria and confirmed by imaging examinations;2 (3) receipt of standardized acute-phase treatment during hospitalization (including but not limited to intravenous thrombolysis, endovascular therapy, or standard medical therapy); (4) ability to complete at least 6 months of follow-up after discharge with complete follow-up data; (5) complete medical records, including admission National Institutes of Health Stroke Scale (NIHSS) score, imaging findings, and treatment and nursing records. Exclusion criteria were: (1) severe neurodegenerative disease, end-stage disease, or other conditions that substantially affect functional recovery; (2) missing or incomplete data that prevented valid analysis; (3) no follow-up after discharge or inability to provide 6-month follow-up data.
Sample size was determined based on stability principles for prediction modeling. Using the rule of at least 15–20 outcome events per variable, together with 18 candidate predictors and an unfavorable recovery rate of about 30% at 6 months,10 and further allowing a 10% increase for potential loss to follow-up or missing outcome data, the target sample size was set at no less than 18×20 / 0.3 / 0.9 = 1334. Ultimately, 1,340 patients with complete 6-month follow-up and outcome data were included. The study was reviewed and approved by the Ethics Committee of Affiliated Second Clinical Hospital, Harbin Medical University (approval number: KY2025-194). As this study employed a retrospective design and did not involve any additional interventions, all clinical data were anonymized prior to analysis. The ethics committee approved a waiver of written informed consent. All methods were carried out in accordance with Declaration of Helsinki.
Measures
Candidate predictors were chosen based on published findings from prior studies on post-stroke functional outcomes and on clinical practice experience.3,11 The variables covered demographic characteristics, disease severity, nursing-related measures, and psychosocial factors. This approach ensured that the screening process took both statistical validity and clinical practicality into account.
Validated scales and assessment tools were used to support reliability and validity. Functional outcome was mainly assessed using the modified Rankin Scale (mRS), ranging from 0 to 6. Scores of 0–2 were defined as favorable recovery, and scores ≥3 were defined as unfavorable recovery. The mRS score at 6 months after discharge served as the primary outcome measure. Patients were divided into a favorable recovery group and an unfavorable recovery group based on this score. The grouping was used for model construction.12
For disease severity, the NIHSS was used to assess neurological deficit at admission. The NIHSS yields scores between 0 and 42, with increasing scores reflecting greater neurological impairment.12 The Glasgow Coma Scale (GCS) was used to assess consciousness, ranging from 3 to 15, where lower values denote more severe impairment of consciousness.13
Regarding modifiable nursing factors, self-management behavior was measured by the Stroke Self-Management Behaviors Performance Scale (SSBPS). The scale provides a total score from 0 to 100, with higher scores representing stronger self-management capacity.14 This scale reflects self-management in disease management, rehabilitation behaviors, and health promotion.
Depression severity was measured with the Patient Health Questionnaire-9 (PHQ-9). This instrument generates scores ranging from 0 to 27, with higher values indicating greater severity of depressive symptoms. Based on prior research and commonly used clinical cutoffs,15 PHQ-9 ≥10 was defined as clinically significant depressive symptoms.
Social support was assessed using the Social Support Rating Scale (SSRS), a tool routinely applied in stroke nursing assessments at the study hospital. It is generally completed within 48–72 h after admission when the patient is relatively stable, under nurse guidance via face-to-face interview, and recorded in the electronic medical record system. The total score ranges from 12 to 66, with higher scores reflecting greater levels of social support. At present, there is no unified clinical cutoff value for the SSRS in stroke populations, and the purpose of this study was risk prediction rather than clinical classification of social support levels. Therefore, a sample distribution–based stratification strategy was adopted, in which patients were categorized according to the median total SSRS score of the study sample. This approach helped avoid bias introduced by arbitrary cutoff selection and ensured statistical stability and reproducibility during model development. SSRS ≥40 was defined as “high social support” and <40 as “non-high social support”.16
Rehabilitation training adherence was measured using the Adherence Rating for Rehabilitation Scale (ARRS). This score was derived from daily records of rehabilitation implementation by therapists and responsible nurses during hospitalization, and it is stored in structured form in the electronic medical record system. The ARRS yields a total score between 0 and 100, with higher scores denoting better adherence to rehabilitation training. According to the scale’s recommended standard,17 ARRS ≥80 was defined as “high adherence”, and <80 as “non-high adherence”.
Data Collection
Relevant clinical data, encompassing patient demographics, disease severity measures, treatment information, and hospitalization processes, were obtained from the hospital’s electronic medical record system through retrospective review of clinical charts. Functional recovery data were obtained from follow-up records after discharge. Accuracy and completeness of the data were confirmed through independent checks conducted by trained staff.
Quality control procedures were implemented as follows. First, all data collectors received standardized training covering chart extraction, data entry requirements, and completeness checks. Second, data entry was performed independently by two researchers with double verification. When discrepancies occurred, a third researcher reviewed the source records to confirm the final values. In addition, periodic internal checks were conducted during data collection to maintain consistency and completeness.
Missing data were handled using the following strategy. The primary outcome variable (mRS score at 6 months after discharge) was not imputed. Cases with missing outcome data were removed at the inclusion stage. For missing values in predictor variables, the missing at random (MAR) assumption was considered appropriate. All data came from a standardized electronic medical record system. No clear systematic link was found between the reason for missingness and patient outcomes. Under this assumption, multiple imputation by chained equations (MICE) was applied. Five imputed datasets were generated and pooled according to Rubin’s rules before regression analyses were conducted. Predictor variables with more than 30% missing data were excluded prior to imputation and omitted from all subsequent analyses. The number of excluded cases was consistent with the loss rate prespecified in the sample size estimation in Participants. After data collection, a final audit was conducted to confirm completeness, accuracy, and internal consistency.
Statistical Analysis
All statistical analyses were conducted using SPSS software. All analyses were two-sided, and a P value < 0.05 was considered statistically significant. Continuous variables were summarized as mean ± standard deviation or median (interquartile range), depending on data distribution. Group comparisons for continuous variables were performed using the independent-samples t test or the Mann–Whitney U-test, as appropriate. Categorical variables were presented as counts (percentages) and compared using the χ2-test. Unfavorable functional recovery at 6 months after discharge (mRS ≥3) was defined as the outcome variable. Univariate analyses were first performed. Variables with P < 0.10 in univariate analysis were entered into a multivariable logistic regression model. This step served as a predictor screening procedure to identify independent predictors for inclusion in the final model. Continuous variables were included in the model as original values, and categorical variables were coded as yes = 1 and no = 0. Regression results were expressed as odds ratios (OR) with 95% confidence intervals (CI).
All participants were divided into a training set and a testing set at a 7:3 ratio using outcome-stratified random sampling. The training set was used for model development and the testing set was used for validation. Discrimination was assessed using the receiver operating characteristic (ROC) curve and the area under the curve (AUC). Calibration was evaluated using the Hosmer-Lemeshow test, calibration curve, and Brier score. Clinical utility was examined using decision curve analysis (DCA). To further evaluate internal stability, 10-fold cross-validation was performed on the full dataset. The data were split into 10 equal parts, with nine parts used for training and one part used for validation in each iteration. This process was repeated 10 times and mean performance metrics were calculated to assess predictive stability across different data partitions. The 33rd and 66th percentiles of predicted probabilities from the training set were calculated as tertile-based cut-off points. These thresholds were used to classify patients into low-, intermediate-, and high-risk groups. The same cut-off values were then applied to the testing set to evaluate the model’s risk stratification performance in an independent sample.
Results
Baseline Characteristics Comparison
Among the 1,340 patients included, 469 (35.0%) had unfavorable functional recovery at 6 months after discharge, while 871 (65.0%) showed favorable recovery. After outcome-stratified random splitting at a 7:3 ratio, the training set and test set included 938 and 402 patients, respectively. No statistically significant differences were observed between the two sets in functional outcome, age, sex, prior stroke history, comorbidity count, stroke type, onset-to-admission time, admission NIHSS, GCS score, lesion location distribution, or multiple nursing-related variables (all P > 0.05), indicating good comparability in demographic features, disease severity, and nursing-related factors. (Table 1).
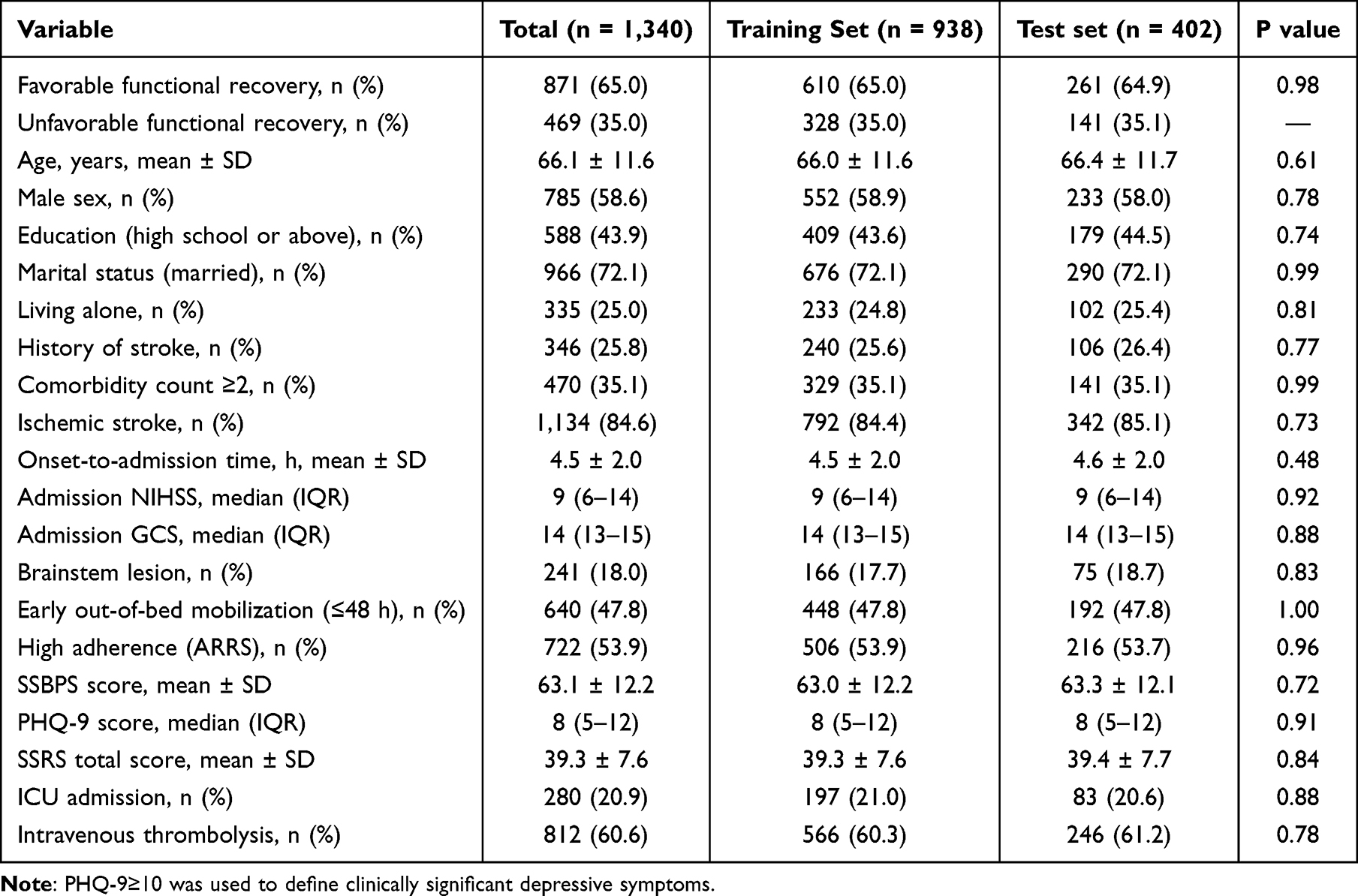 |
Table 1 Baseline Characteristics Comparison |
Univariate Analysis of Patients With Different Functional Outcomes
Univariate analysis showed that age, educational level, living arrangement, prior stroke history, comorbidity count, onset-to-admission time, admission NIHSS score, admission GCS score, brainstem lesions, as well as SSBPS score, early out-of-bed mobilization within 48 h, high ARRS, PHQ-9 ≥10, and high SSRS score were significantly associated with unfavorable functional recovery at 6 months (P < 0.05) (Table 2).
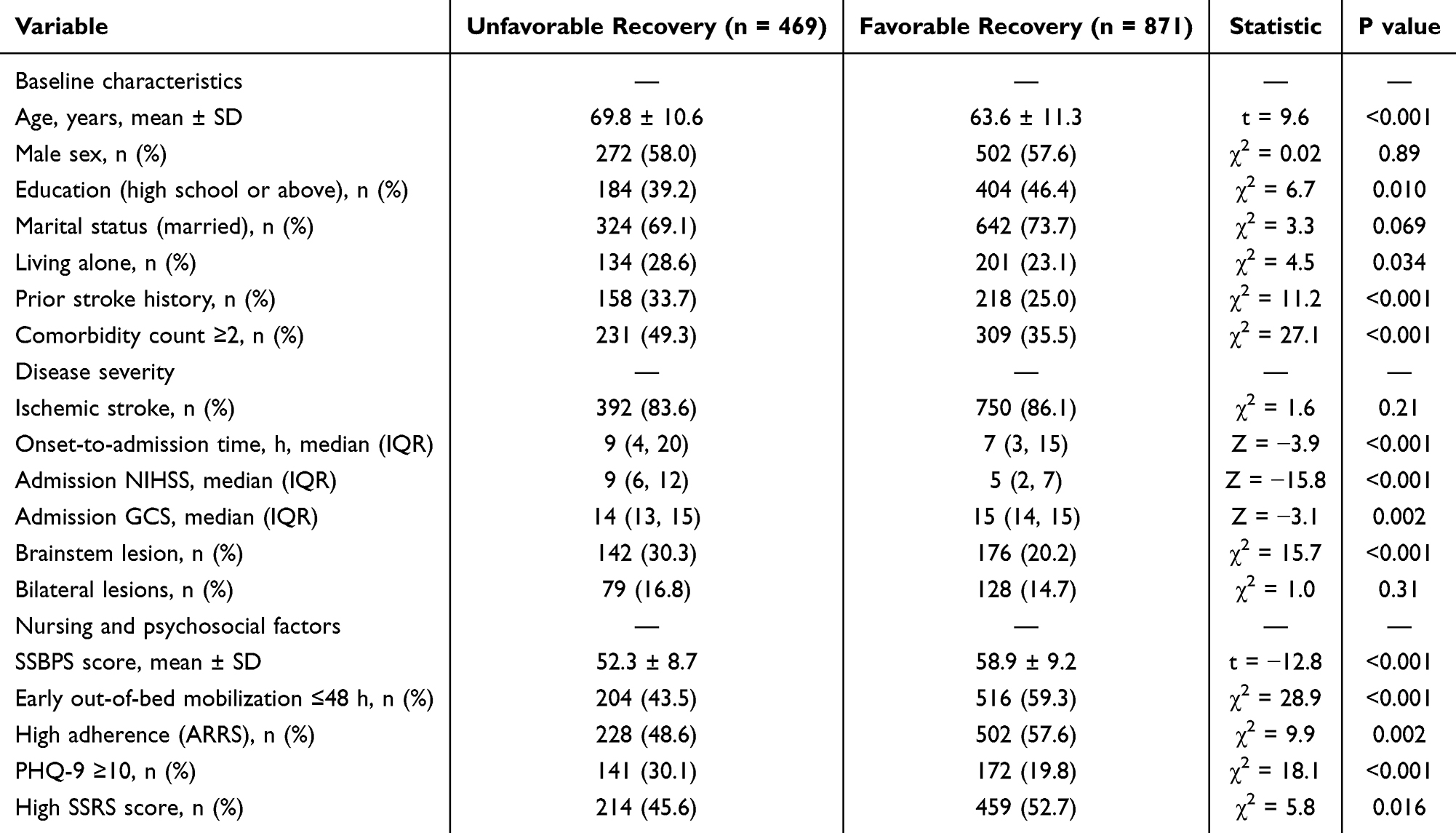 |
Table 2 Univariate Analysis of Unfavorable Functional Recovery at 6 Months After Discharge in Patients with Stroke (n = 1,340) |
Multivariable Logistic Regression for Predictor Selection
Multivariable analysis revealed that older age, prior stroke history, comorbidity count ≥ 2, longer onset-to-admission time, higher admission NIHSS score, brainstem lesions, and PHQ-9 ≥ 10 were independent predictors of increased risk of unfavorable functional recovery (P < 0.05). Higher admission GCS score, higher SSBPS score, early out-of-bed mobilization within 48 hours, and higher SSRS score were independent predictors of reduced risk of unfavorable functional recovery (P < 0.05). These variables were subsequently incorporated into the risk prediction model. (Table 3).
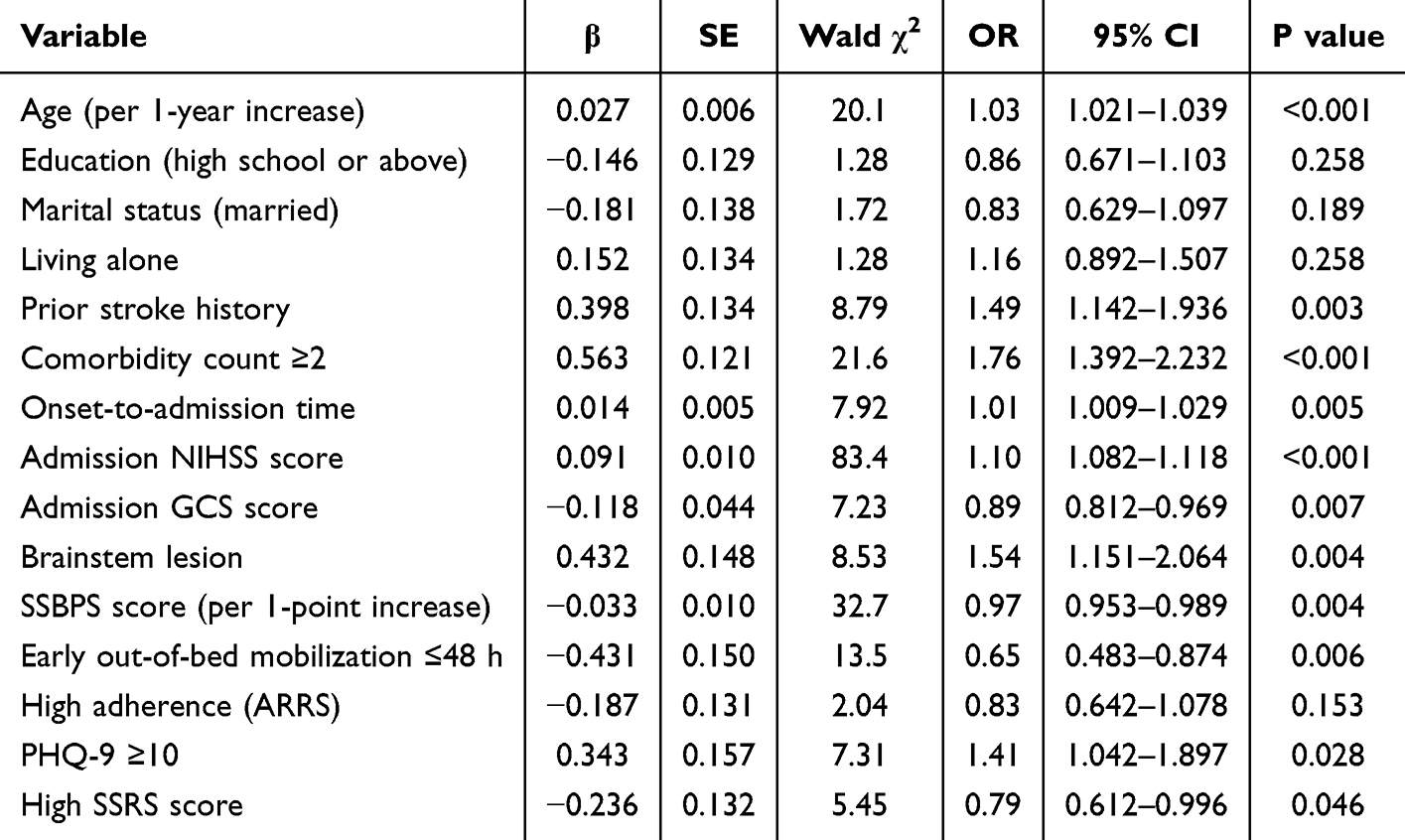 |
Table 3 Multivariate Logistic Regression Results for Predictor Selection in Model Development (n = 938) |
Development and Evaluation of the Risk Prediction Model for Unfavorable Functional Recovery After Stroke
Independent predictors identified through multivariable logistic regression were used to develop a risk prediction model for unfavorable functional recovery at 6 months after stroke in the training set (n = 938). The model was then validated in the testing set (n = 402). A logistic regression model was constructed with these predictors as independent variables. The regression equation was as follows:
logit(P)=ln[P/(1−P)]=−3.214+0.027×(Age)+0.398×(Prior stroke)+0.563×(Comorbidity count≥2)+0.014×(Onset-to-admission time)+0.091×(Admission NIHSS)−0.118×(Admission GCS)+0.432×(Brainstem lesion)−0.033×(SSBPS score)−0.431×(Early mobilization≤48 h)+0.343×(PHQ-9≥10) −0.236×(High social support). In this equation, P represents the predicted probability of unfavorable functional recovery at 6 months after discharge. Categorical variables were coded as yes = 1 and no = 0. Positive coefficients indicate increased risk, whereas negative coefficients indicate reduced risk.
The logistic regression model was further visualized as a nomogram. Each predictor corresponded to a specific number of points, and the total score was obtained by summing points across variables. The total score was then mapped to the predicted probability of unfavorable recovery at 6 months. Higher total points indicate a higher predicted risk (Figure 1).
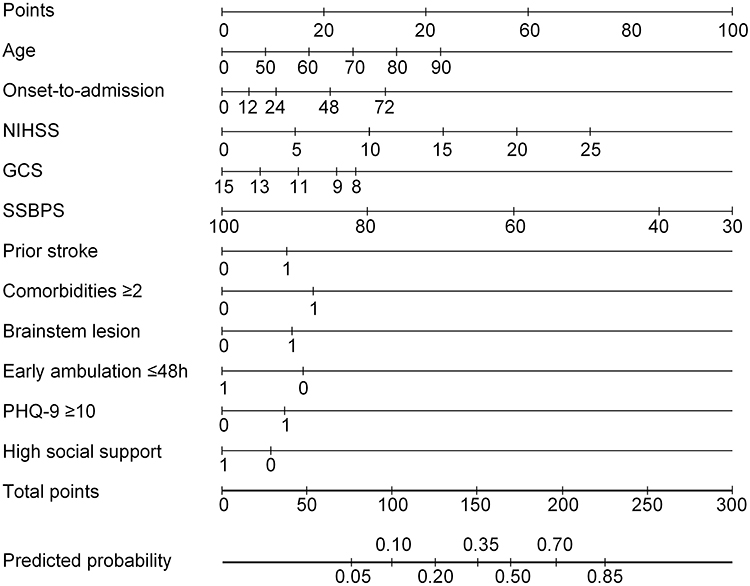 |
Figure 1 Nomogram for predicting 6-month unfavorable functional recovery in stroke. |
Discriminative performance of the model was strong. The AUC was 0.883 during training and remained high at 0.854 in the test set. Sensitivity and specificity at the Youden-based cutoff were 83.2% and 76.4% in the training set and 81.9% and 75.6% in the test set. 10-fold cross-validation showed a mean AUC of 0.871, which was consistent with the results from both the training and testing sets. This finding suggested that the model maintained good predictive stability across different data partitions. (Figure 2, Table 4).
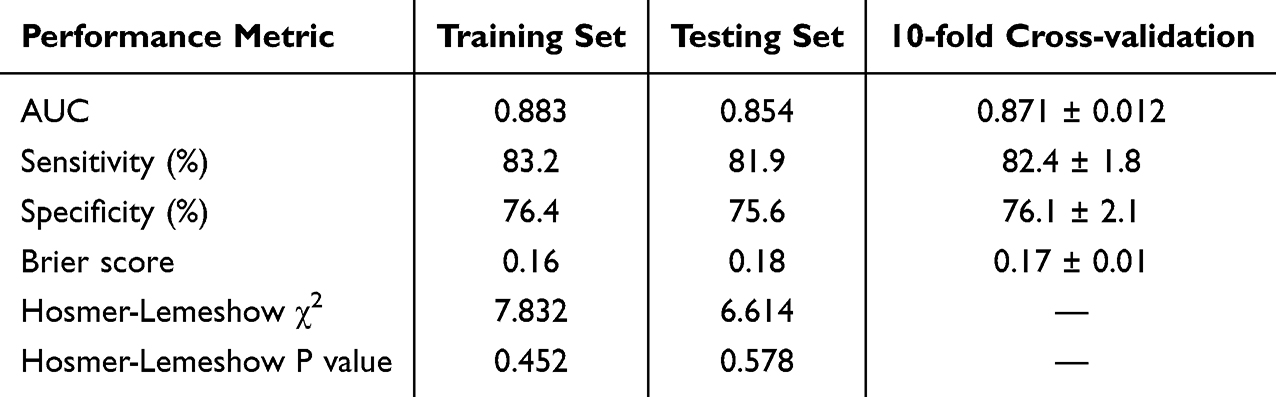 |
Table 4 Performance Metrics of the Risk Prediction Model Across Validation |
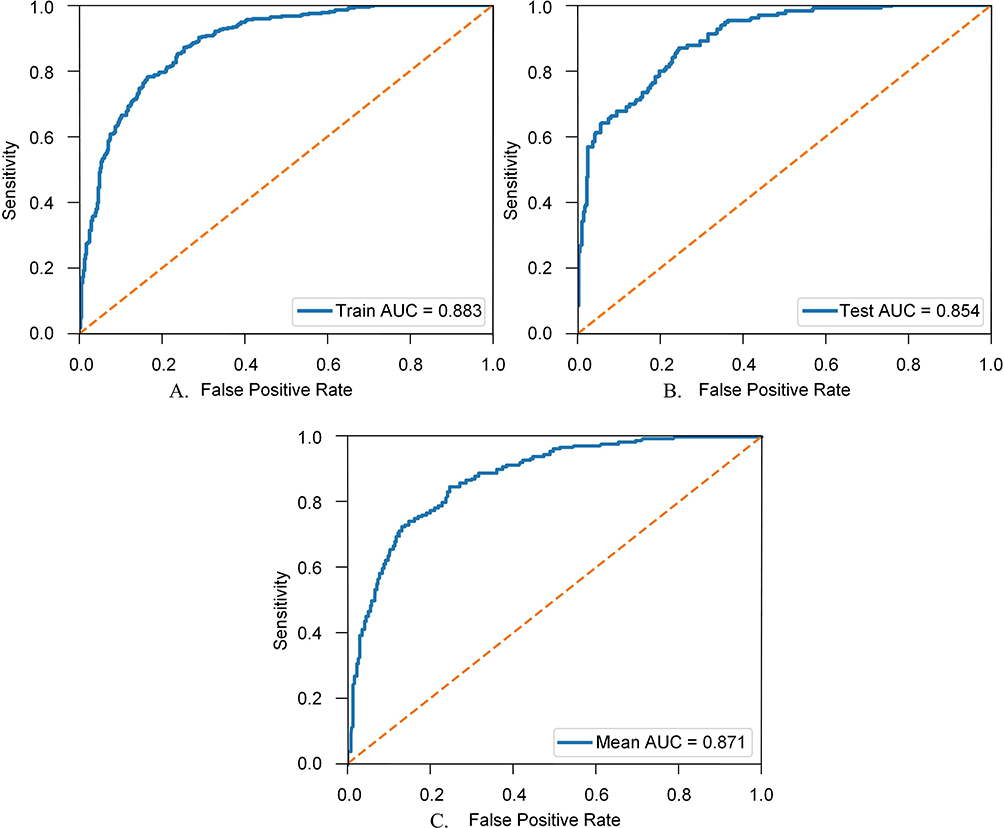 |
Figure 2 ROC curves of the prediction model. (A) ROC curve in the training set. (B) ROC curve in the testing set. (C) ROC curve from 10-fold cross-validation. Abbreviations: AUC, area under the curve; ROC, receiver operating characteristic. |
Bias-corrected calibration curves in both datasets showed close alignment with the ideal line, reflecting good consistency between estimated risks and actual outcomes. The Hosmer-Lemeshow test showed χ2 = 7.832 and P = 0.452 in the training set, and χ2 = 6.614 and P = 0.578 in the testing set, indicating adequate model fit. At the same time, the Brier scores were 0.16 in the training set and 0.18 in the testing set. The mean Brier score from 10-fold cross-validation was 0.17. These results suggested that the overall prediction error was remained within an acceptable range. (Figure 3, Table 4).
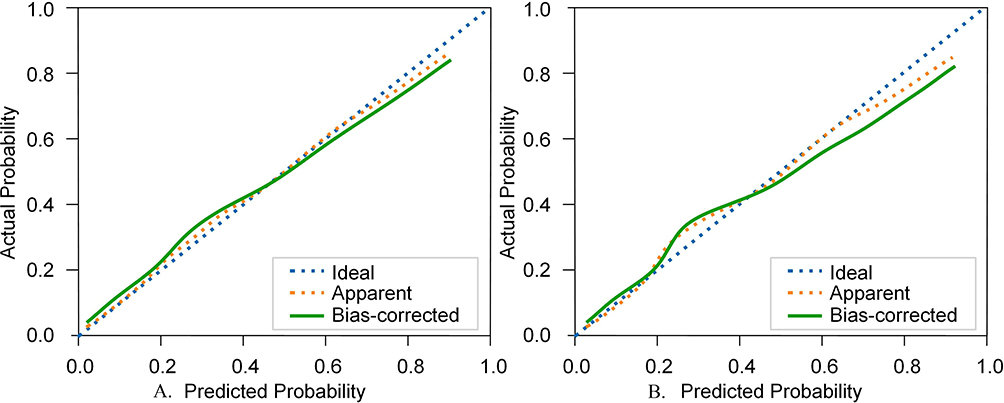 |
Figure 3 Calibration curves of the prediction model. (A) Calibration curve in the training set. (B) Calibration curve in the testing set. The dotted blue line represents the ideal calibration, the Orange dotted line represents the apparent calibration, and the green solid line represents the bias-corrected calibration. |
DCA demonstrated that the model achieved greater net benefit than the treat-all and treat-none strategies across a broad range of threshold probabilities. The curves for the training set and the test set showed similar trends, and the cross-validated curves were close to the apparent curves, suggesting good model stability and and consistent decision performance within the study sample (Figure 4).
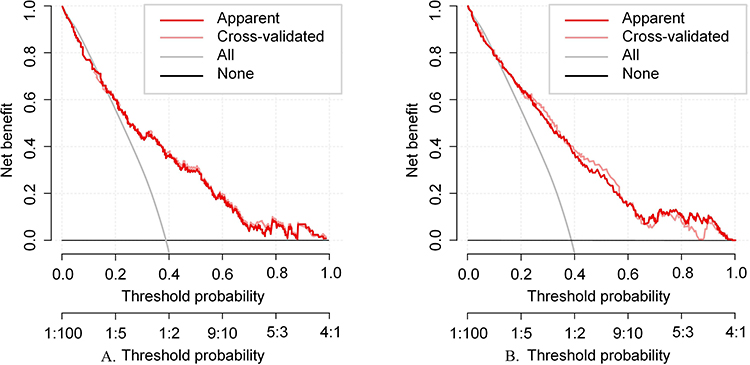 |
Figure 4 Decision curve analysis of the prediction model in the training set and the test set. (A) Decision curve analysis in the training set. (B) Decision curve analysis in the testing set. The pink solid lines represent the apparent and cross-validated net benefit curves of the model. The gray line represents the “treat all” strategy, and the black line represents the “treat none” strategy. |
Based on the tertiles of predicted probabilities from the training set, risk stratification cut-off points were set at 0.24 and 0.48. Patients were classified into three groups: low-risk (≤0.24), intermediate-risk (0.25–0.47), and high-risk (≥0.48). The rate of unfavorable functional recovery increased stepwise across risk groups in both the training and testing sets, ranging from 7.7% in the low-risk group to 54.3% in the high-risk group (training set) and from 8.8% to 59.8% (testing set), indicating good risk stratification performance. (Table 5).
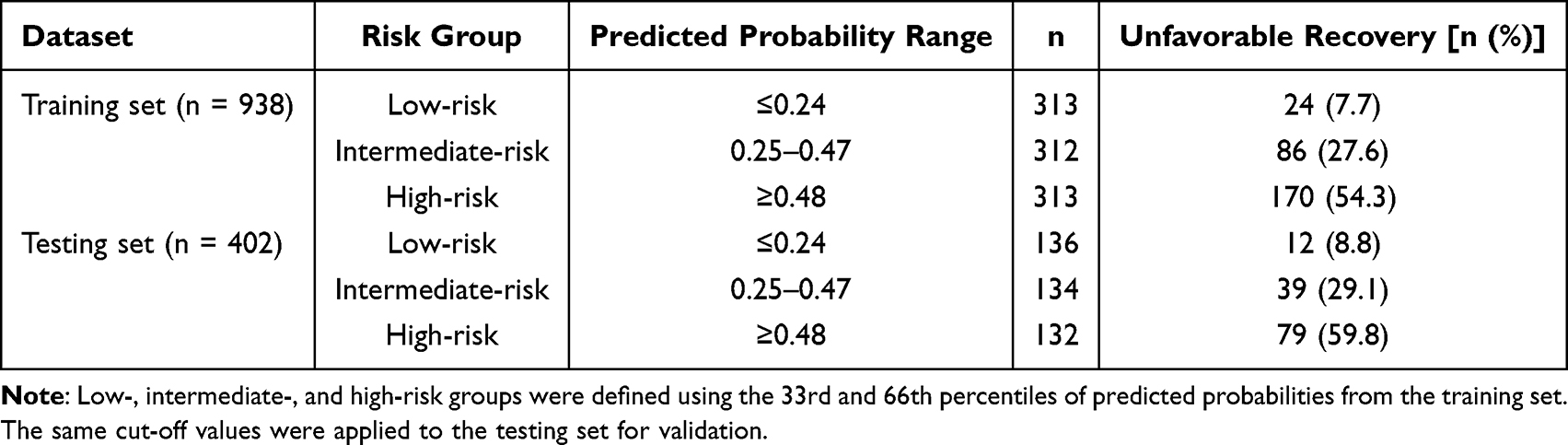 |
Table 5 Risk Stratification Results of the Prediction Model in the Training and Testing Sets |
Discussion
Poor functional recovery after stroke is a complex outcome resulting from the combined effects of neural injury, physiological compensation, nursing processes, and psychosocial factors.4 This study examined factors associated with functional outcomes at 6 months after discharge in patients with stroke and developed a risk prediction model based on these factors. The suggest that long-term functional outcomes are not only closely related to the severity of acute neurological impairment but are also significantly associated with nursing behaviors, self-management capacity, and psychosocial support. These results highlight the importance of early identification and management of modifiable nursing-related factors in addition to routine disease assessment to improve stroke prognosis.
Regarding clinical predictors, older age, prior stroke history, comorbidity count ≥2, longer onset-to-admission time, higher admission NIHSS score, lower GCS score, and brainstem lesions were all identified as independent predictors of unfavorable functional recovery. Previous studies have consistently shown that greater neurological deficits in the acute phase, as reflected by higher NIHSS scores, are linked to poorer mid- and long-term mRS outcomes, supporting the central role of NIHSS in prognostic stratification.18
The association between admission consciousness level, measured by the GCS, and functional outcomes has also been repeatedly demonstrated in early rehabilitation admission studies, supporting its value as a comprehensive indicator of impaired brain function and limited systemic compensation. In this study, brainstem lesions were independently associated with poor functional recovery, which is consistent with evidence indicating that lesion location and topological characteristics influence stroke outcomes. Previous cohort studies on brainstem infarction have shown that lesion location and extent are closely related to disability severity, supporting the sustained impact of brainstem damage on swallowing, postural control, and gait function.19
Longer onset-to-admission time was also associated with unfavorable recovery, in line with studies showing that prehospital delay affects neurological improvement and clinical outcomes.20 Clinical guidelines and evidence-based care pathways repeatedly emphasize that “time is brain” and identify shortening the time from symptom onset to treatment as a key strategy for improving functional outcomes.21
A lower SSBPS score was identified as an independent predictor of unfavorable functional recovery, suggesting that self-management capacity is an important behavioral indicator of long-term recovery trajectory. Previous studies have shown that the Stroke Self-Management Behaviors Performance Scale demonstrates good reliability and validity, supporting its use in clinical risk evaluation. Evidence from self-management support interventions suggests that improvements in self-management are accompanied by favorable changes in selected rehabilitation-related outcomes, which supports the inclusion of self-management assessment and targeted enhancement within routine stroke nursing care pathways.22 Based on this finding, nursing staff can provide structured self-management education during hospitalization, covering disease knowledge, rehabilitation guidance, and training in self-monitoring skills after discharge.
Early out-of-bed mobilization within 48 hours was identified as an independent predictor of reduced risk, suggesting that early activity, when feasible, is associated with better long-term outcomes. In contrast, the AVERT randomized controlled trial reported that very early, high-dose mobilization within 24 hours reduced the likelihood of favorable outcomes at 3 months, indicating that the timing and intensity of early mobilization require careful control. Based on this evidence, the AHA/ASA guidelines clearly state that very early high-dose mobilization within 24 hours should not be implemented, as it reduces the probability of good outcomes.5 Accordingly, the present finding regarding mobilization within 48 hours complements the AVERT results and supports a stratified, gradual, and tolerable early mobilization approach rather than a uniform high-intensity strategy. After the patient’s condition stabilizes, nursing staff should develop a gradual and individualized mobilization plan based on patient tolerance, assist with the first out-of-bed activity within 48 hours, and adjust activity intensity throughout the care process.
Psychological and social factors also played an important role in this study. PHQ-9 ≥10 was identified as an independent predictor of higher risk, indicating a consistent association between depressive symptoms and long-term disability after stroke. Evidence from systematic reviews and meta-analyses has shown that post-stroke depression is significantly related to poorer functional outcomes and underscores the importance of early identification and management of depressive symptoms during stroke care.23 In addition, longitudinal studies have confirmed associations between post-stroke depression and adverse outcomes, including functional decline and recurrence, highlighting the clinical value of routine psychological screening.23 Depression screening should be incorporated into routine stroke nursing assessment, and patients with PHQ-9 ≥10 should receive timely psychological support or referral to professional mental health services to reduce the impact of depressive symptoms on functional recovery.
Higher social support level was identified as an independent predictor of reduced risk, suggesting that social resources and care support have a protective role in long-term recovery. Studies on social support in stroke populations have shown that social connection and participation are associated with better physical and psychological outcomes, supporting the role of social support in recovery through enhanced rehabilitation engagement and emotional regulation.24 However, some studies have reported inconsistent associations between social support and certain functional or quality-of-life outcomes, indicating that the effects of social support may vary according to measurement dimensions, outcome types, and population characteristics.25 Including social support as a predictor in the present model facilitates early identification of patients with limited social resources and supports targeted allocation of nursing care, which is consistent with evidence on the role of social support in stroke outcomes. For patients with limited social support, nursing staff should assess family support resources during hospitalization, collaborate with social workers to develop post-discharge support plans, and encourage family involvement in the rehabilitation process. Based on the combined influence of the above clinical and nursing-related predictors, risk stratification was further performed. The rate of unfavorable functional recovery increased in a stepwise manner across risk groups, suggesting that the model not only has good predictive ability but also helps nursing staff identify high-risk patients early and implement targeted interventions.
Regarding variable selection, ARRS showed a significant association with unfavorable functional recovery in univariate screening but was not retained as an independent predictor in the multivariable logistic regression model. This finding suggests that the effect of ARRS on functional outcomes may be influenced by other related factors within a multivariable framework. ARRS may be conceptually and practically correlated with nursing-related variables such as early mobilization and SSBPS, and its effect may therefore be partially overlapped or substituted in the multivariable model, leading to attenuation of its independent association. In addition, ARRS is a composite score derived from routine inpatient nursing records, and its measurement process may be affected by differences in documentation standards among rehabilitation therapists and nursing staff, which could reduce the stability of its effect in multivariable analysis. Moreover, ARRS mainly reflects rehabilitation implementation during hospitalization, whereas long-term functional outcomes may be more strongly influenced by early neurological injury as well as sustained self-management behaviors and social support. After adjustment for these factors, the independent predictive value of ARRS may have been weakened. These findings indicate that the role of rehabilitation adherence indicators may be more complex in real-world studies, and future research may further clarify their mechanisms using more refined adherence measurements and pathway analysis approaches.
This study used multivariable logistic regression to develop the prediction model, which has a well-established methodological basis in clinical prediction research and produces interpretable and clinically applicable results. However, post-stroke functional recovery is influenced by complex interactions among multiple factors. Some relationships, such as the dose-dependent effect of early mobilization and the collinearity between rehabilitation adherence and other nursing factors, may exceed the capacity of a linear regression framework. Future studies with larger samples could explore machine learning and non-linear modelling approaches to better capture these relationships and improve model performance.
In clinical practice, the nomogram can be completed within 48–72 hours of admission. Clinicians calculate a total score based on routinely collected clinical, nursing, and psychosocial data and map it to the predicted probability of unfavorable recovery at 6 months. For patients identified as high-risk, early mobilization guidance, psychological support, discharge planning, and enhanced follow-up can be prioritized to support individualized nursing decisions. All predictors in the final model are obtainable through routine early assessment without additional testing. Future work could identify core variables and develop a simplified bedside tool to improve practical efficiency. Although the model has not been validated on an independent external dataset, all included variables are routine clinical measures, which provides a basis for potential use across different settings. External generalizability still requires confirmation through multi-center prospective studies. Multiple imputation was used to handle missing data, but this approach relies on the missing at random assumption. If the actual missing data mechanism deviates from this assumption, some bias in model estimates and predictive performance may remain.
Conclusion
A risk prediction model for unfavorable post-stroke functional recovery was developed and validated. The model combined clinical and modifiable nursing-related predictors and showed good discrimination, calibration, and clinical net benefit in both the training and testing sets. Risk stratification based on predicted probabilities further confirmed the model’s ability to differentiate patient risk levels, providing nursing staff with a practical basis for risk-guided care decisions. The model can serve as a tool to support early risk stratification before discharge, help nursing staff identify high-risk patients, and guide targeted interventions, providing evidence for evidence-based nursing and rehabilitation management in stroke care.
This study has several limitations.
(1) A single-center retrospective design was used and some variables were extracted from routine medical records, which may introduce selection bias and information bias. Although internal validation was performed using a 7:3 split combined with 10-fold cross-validation, external validation on an independent dataset was not conducted. The model’s generalizability across different regions, populations, and healthcare settings requires confirmation through multi-center prospective research.
(2) Quantitative imaging indicators and longer-term follow-up outcomes were not included, which limits the model’s ability to capture the dynamic nature of stroke recovery.
(3) A univariate pre-screening combined with multivariable logistic regression was used for predictor selection. Although the model showed good predictive performance, more systematic methods such as LASSO were not applied to further optimize the predictor subset.
(4) The model was built on main-effect predictors. Potential interactions among age, stroke severity, early mobilization, and psychosocial factors were not systematically assessed, and including these relationships may improve model performance.
(5) Continuous predictors were entered as raw values without systematic assessment of potential non-linear relationships using methods such as fractional polynomials. This approach is common in stroke prognostic prediction research,26 but more flexible modelling strategies could be explored in future studies to further improve predictive performance.
(6) Clinical and modifiable nursing factors were integrated into a single prediction model. A two-stage framework using fixed clinical factors for initial risk stratification followed by modifiable nursing factors to guide intervention was not developed. Future studies with larger samples could explore this stepwise approach to further enhance clinical utility.
(7) This study completed model development and internal validation but did not assess model impact. Whether the model improves nursing decisions and patient functional outcomes in real clinical use has not been confirmed, and prospective implementation studies are needed to address this gap.
Data Sharing Statement
The experimental data used to support the findings of this study are available from the corresponding author upon request.
Funding
The work was not supported by any funding.
Disclosure
Ruilin Sun and Zhaojun Liu are the co-first authors for this study. The authors declared that they have no conflicts of interest regarding this work.
References
1. GBD 2019 Stroke Collaborators. Global, regional, and national burden of stroke and its risk factors, 1990–2019: a systematic analysis for the Global Burden of Disease Study 2019. Lancet Neurol. 2021;20(10):795. doi:10.1016/S1474-4422(21)00252-0
2. Feske SK. Ischemic stroke. Am J Med. 2021;134(12):1457–13. doi:10.1016/j.amjmed.2021.07.027
3. Campagnini S, Sodero A, Baccini M, et al. Prediction of the functional outcome of intensive inpatient rehabilitation after stroke using machine learning methods. Sci Rep. 2025;15(1):16083. doi:10.1038/s41598-025-00781-1
4. Belagaje SR. Stroke rehabilitation. Continuum. 2017;23(1):238–253. doi:10.1212/CON.0000000000000423
5. Warner JJ, Harrington RA, Sacco RL, et al. Guidelines for the early management of patients with acute ischemic stroke: 2019 update to the 2018 guidelines for the early management of acute ischemic stroke. Stroke. 2019;50(12):3331–3332. doi:10.1161/STROKEAHA.119.027708
6. Fukuda S, Yamamoto N, Tomita Y, et al. Development and validation of clinical prediction model for functional Independence measure following stroke rehabilitation. J Stroke Cerebrovasc Dis. 2025;34(2):108185. doi:10.1016/j.jstrokecerebrovasdis.2024.108185
7. Harvey DY, Parchure S, Hamilton RH. Factors predicting long-term recovery from post-stroke aphasia. Aphasiology. 2022;36(11):1351–1372. doi:10.1080/02687038.2021.1966374
8. Yen HC, Pan GS, Jeng JS, et al. Impact of early mobilization on patients with acute ischemic stroke treated with thrombolysis or thrombectomy: a randomized controlled trial. Neurorehabil Neural Repair. 2024;38(5):339–349. doi:10.1177/15459683241236443
9. Feller D, Wingbermuhle R, Berg B, et al. Improvements are needed in the adherence to the TRIPOD statement for clinical prediction models for patients with spinal pain or osteoarthritis: a metaresearch study. J Pain. 2024;25(11):104624. doi:10.1016/j.jpain.2024.104624
10. De Silva DA, Narasimhalu K, Huang IW, et al. Long-term post-stroke functional outcomes: a comparison of diabetics and nondiabetics. Cerebrovasc Dis Extra. 2022;12(1):7–13. doi:10.1159/000521442
11. Yan C, Zheng Y, Zhang X, et al. Development and validation of a nomogram model for predicting unfavorable functional outcomes in ischemic stroke patients after acute phase. Front Aging Neurosci. 2023;15:1161016. doi:10.3389/fnagi.2023.1161016
12. Sato H, Mitsui N, Fujikawa S, et al. Critical evaluation of the modified Rankin Scale for assessment of the efficacy of mechanical thrombectomy: a retrospective comparison between the modified Rankin Scale and functional Independence measure. Intervent Neuroradiol. 2025;31(6):771–777. doi:10.1177/15910199231185635
13. Padwale V, Chivate C, Kirnake V, et al. Comparative prognostic value of the National Institutes of Health Stroke Scale (NIHSS) and the Glasgow Coma Scale (GCS) in supratentorial and infratentorial stroke patients in Western India. Cureus. 2024;16(7).
14. Lo SHS, Chau JPC, Choi KC. Development and psychometric evaluation of a questionnaire for assessing self-management behaviors in stroke survivors. J Stroke Cerebrovasc Dis. 2022;31(4):106389. doi:10.1016/j.jstrokecerebrovasdis.2022.106389
15. Panov S. Nurse-led post Stroke Depression Screening (PSD) for patients with acute stroke using Patient Health Questionnaire-9 (PHQ9); 2023.
16. Li Y, Tang A, Ge L, et al. The relationship between social and psychological factors with cognitive impairment after stroke: a prospective study. Front Psychiatry. 2024;15:1403027. doi:10.3389/fpsyt.2024.1403027
17. Long Q, Wu L, Li Y, et al. Impact of frailty on rehabilitation exercise adherence in patients with ischemic stroke. Front Med. 2025;12:1679267. doi:10.3389/fmed.2025.1679267
18. Ortega-Martorell S, Olier I, Ohlsson M, et al. Advancing personalised care in atrial fibrillation and stroke: the potential impact of AI from prevention to rehabilitation. Trends Cardiovasc Med. 2025;35(4):205–211. doi:10.1016/j.tcm.2024.12.003
19. Chen P, Pan Y, Wang J, et al. The value of computed tomography perfusion deficit volumes in acute isolated brainstem infarction. Front Neurol. 2023;14:1233784. doi:10.3389/fneur.2023.1233784
20. Lee EJ, Kim SJ, Bae J, et al. Impact of onset-to-door time on outcomes and factors associated with late hospital arrival in patients with acute ischemic stroke. PLoS One. 2021;16(3):e0247829. doi:10.1371/journal.pone.0247829
21. Ho JP, Powers WJ. Contemporary management of acute ischemic stroke. Ann Rev Med. 2025;76:417–429. doi:10.1146/annurev-med-050823-094312
22. Oh HX, De Silva DA, Toh ZA, et al. The effectiveness of self-management interventions with action-taking components in improving health-related outcomes for adult stroke survivors: a systematic review and meta-analysis. Disability Rehabil. 2022;44(25):7751–7766. doi:10.1080/09638288.2021.2001057
23. Butsing N, Zauszniewski JA, Ruksakulpiwat S, et al. Association between post-stroke depression and functional outcomes: a systematic review. PLoS One. 2024;19(8):e0309158. doi:10.1371/journal.pone.0309158
24. Espernberger K, Fini NA, Peiris CL. Identity, social engagement and community participation impact physical activity levels of stroke survivors: a mixed-methods study. Clin Rehabil. 2023;37(6):836–850. doi:10.1177/02692155221141977
25. Bi H, Wang M. Role of social support in poststroke depression: a meta-analysis. Frontiers in Psychiatry. 2022;13:924277. doi:10.3389/fpsyt.2022.924277
26. Bao J, et al. Development and validation of a novel nomogram model predicting the unfavorable outcome based on NAR and collaterals status for patients with AIS. J Stroke Cerebrovasc Dis. 2024;33(9):107855. doi:10.1016/j.jstrokecerebrovasdis.2024.107855
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.