Back to Journals » Journal of Inflammation Research » Volume 19
Development of a Prognostic Nomogram Model and Establishment of a Risk Stratification System Based on the Naples Prognostic Score for Patients with Oropharyngeal Squamous Cell Carcinoma Who Have Undergone Radical Surgery
Authors Meng X, Wang J, Shen W, Yang S, Zhao K, Wang J, Hu Q, Chen X, Cheng H ![]() , Xu X
, Xu X ![]()
Received 30 January 2026
Accepted for publication 16 May 2026
Published 24 May 2026 Volume 2026:19 590986
DOI https://doi.org/10.2147/JIR.S590986
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Subhasis Chattopadhyay
Xiangli Meng,1 Jin Wang,1 Wei Shen,1 Shanshan Yang,1 Kelei Zhao,1 Jingjing Wang,2 Qiangwang Hu,1 Xiaonan Chen,1 Hao Cheng,2,3 Xuelian Xu2
1Department of Oncology, The First Affiliated Hospital of Xinxiang Medical University, Xinxiang, Henan, 453100, People’s Republic of China; 2Department of Radiotherapy Oncology, The First Affiliated Hospital of Xinxiang Medical University, Xinxiang, Henan, 453100, People’s Republic of China; 3Department of Radiotherapy Oncology, Affiliated Cancer Hospital of Zhengzhou University, Zhengzhou, Henan, 450000, People’s Republic of China
Correspondence: Hao Cheng, Email [email protected] Xuelian Xu, Email [email protected]
Background: The Naples prognostic score (NPS), a comprehensive indicator of inflammation and nutritional status, has demonstrated favorable prognostic predictive value in a multitude of malignant tumors. Nevertheless, its clinical significance in oropharyngeal squamous cell carcinoma (OPSCC) remains ambiguous.
Methods: This is a multicenter retrospective investigation encompassing 372 patients with OPSCC who underwent radical surgery from August 2010 to September 2020. The univariate and multivariate Cox regression analyses were conducted to screen the independent prognostic factors influencing disease - free survival (DFS) and overall survival (OS). Based on these analyses, two prognostic nomogram incorporating the NPS was constructed. The predictive performance of the models was evaluated using the concordance index (C - index), receiver operating characteristic curve (ROC), calibration curve, decision curve analysis (DCA), integrated discrimination improvement index (IDI), and net reclassification index (NRI). A risk stratification system was further established according to the total risk score of the nomograms, and the survival benefit of adjuvant radiotherapy in different risk subgroups was analyzed.
Results: Multivariate analysis indicated that AJCC stage, p16 expression status, perineural invasion, NPS, and age - adjusted Charlson comorbidity index (ACCI) were independent prognostic factors for DFS and OS. The constructed DFS and OS nomograms demonstrated stable prediction performance in both the training and validation sets, with C - indexes of 0.661 and 0.665, respectively, and the area under the ROC curve was greater than 0.65. The calibration curve revealed that the prediction results of the model were in good agreement with the actual observation results. DCA demonstrated that the model had a higher net clinical benefit than the AJCC staging system. The IDI and NRI analyses further corroborated the significant advantages of the new model in discrimination power and risk reclassification. The analysis based on the risk stratification system indicated that adjuvant radiotherapy was significantly associated with survival benefit only in the high - risk group, while no significant benefit was observed in the intermediate - risk and low - risk groups.
Conclusion: NPS is an important independent prognostic indicator for DFS and OS in postoperative OPSCC patients. The incorporation of NPS into the nomogram can enhance the accuracy of survival prediction and offer a reference for personalized medicine.
Keywords: Naples prognostic score, oropharyngeal squamous cell carcinoma, nomogram, risk stratification system, adjuvant radiotherapy
Background
Oropharyngeal carcinoma is defined as the primary malignant tumors that originating in the tonsil, base of the tongue, soft palate, and posterior pharyngeal wall.1 A 2018 report released by the International Agency for Research on Cancer indicated that the quantity of new cases of oropharyngeal cancer constituted 0.5% of all tumors.2 In most countries, the incidence rate of oropharyngeal carcinoma is on the rise.1,3 Oropharyngeal squamous cell carcinoma (OPSCC) is the most common pathological subtype of oropharyngeal cancer, and the causal relationship between high-risk human papillomavirus (HPV) and OPSCC has been widely recognized, representing one of the most important and thoroughly validated findings in the field of head and neck oncology.4,5 Marked biological and clinical heterogeneity exists between HPV-positive and HPV-negative OPSCC, indicating that they represent distinct disease entities beyond conventional staging systems.6,7 Therefore, additional prognostic factors beyond TNM staging are required for more accurate risk stratification.7 Host-related factors, particularly systemic inflammation and nutritional status, have emerged as important determinants of tumor progression and survival in head and neck cancer.8,9 Integrating tumor-specific features such as HPV status with host-related conditions may improve prognostic stratification and provide a more comprehensive understanding of disease behavior.7 Radical surgery stands as one of the primary treatment modalities.10
Currently, the American Joint Committee on Cancer (AJCC) staging system, 8th edition, stands as the most crucial tool for predicting the survival for OPSCC.11 This system integrates multiple clinical factors, including tumor size, local spread, extranodal extension (ENE), regional nodal and distant metastases, and high - risk HPV association.12 However, this staging system fails to consider numerous potential clinical predictors that may impact prognosis, such as gender,13 age,14 smoking,6,14 nutritional status,15 immune - inflammatory markers,16,17 and comorbidities.18 The objective of these studies was to concentrate on other clinical predictors that were not encompassed by the AJCC staging system.
In recent years, increasing evidence has highlighted the critical role of the tumor immune microenvironment (TIME) in the progression of head and neck cancers.19 The dynamic interactions between tumor cells and immune components—including neutrophils, lymphocytes, tumor-associated macrophages, and regulatory T cells—contribute to immune evasion and tumor progression.20 These immune cells shape an immunosuppressive microenvironment through cytokine secretion, immune checkpoint activation, and metabolic reprogramming.19 Importantly, systemic inflammatory and nutritional markers are closely linked to the tumor immune microenvironment.4,20,21 Elevated neutrophil levels are associated with tumor-promoting inflammation, whereas decreased lymphocyte counts may reflect impaired anti-tumor immunity.21 In addition, hypoalbuminemia and altered lipid metabolism are indicative of cancer-related malnutrition and chronic inflammation, both of which are closely associated with immune dysfunction.22 Recent studies have demonstrated that these peripheral blood biomarkers may serve as surrogate indicators of the immune status in patients with head and neck cancers.4,21 Therefore, composite indices integrating inflammatory and nutritional parameters, such as the Naples Prognostic Score (NPS), may reflect the complex interplay between systemic inflammation, nutritional status, and tumor immunity, providing a strong biological rationale for their prognostic value.20,22
Among these prognostic factors, the NPS is an innovative marker combining inflammation and nutritional status. NPS is calculated based on neutrophil count, lymphocyte count, monocyte count, total cholesterol (TC), and serum albumin concentration. Originally developed to assess long-term postoperative survival in colorectal cancer patients,23 NPS has gained increasing attention for its significant prognostic value. Numerous studies have highlighted its role as a critical predictor of survival in various malignancies,24–27 including head and neck cancers.28,29 However, no research has investigated whether the NPS influences the prognosis of OPSCC. In light of this, the current study aimed to assess the prognostic value of NPS in patients with postoperative OPSCC and incorporate it into a prognostic nomogram model to offer valuable perspectives for personalized treatment approaches.30
Methods
Study Population
This study conducts a multicenter retrospective analysis. It encompasses the clinical data of patients with postoperative OPSCC who were admitted to the First Affiliated Hospital of Xinxiang Medical University, the Affiliated Cancer Hospital of Zhengzhou University, and the First People’s Hospital of Shangqiu between August 2010 and September 2020. The inclusion criteria are as follows: patients should have a tumor of oropharyngeal origin confirmed by imaging, a histologically - verified squamous cell carcinoma, an age of at least 18 years, and Eastern Cooperative Oncology Group performance status (ECOG PS) < 3. The exclusion criteria consist of: distant metastasis (N = 124), multiple primary tumors (N = 22), incomplete clinical data (N = 44, applicable only when the proportion of a single missing variable was less than 5%), lack of regular follow - up (N = 46), age less than 18 years (N = 2), absence of radical surgery (N = 122), receipt of neoadjuvant radiotherapy (N = 20), receipt of only adjuvant chemotherapy (N = 9), and receipt of immunotherapy (N = 7). Ultimately, 372 postoperative OPSCC patients who met the inclusion criteria were incorporated into the analysis. Regarding the treatment plan, a variety of advanced radiotherapy techniques were employed in this study, including intensity - modulated radiotherapy (IMRT), conformal radiotherapy (CRT), and volume - modulated arc therapy (VMAT). The total radiation dose was set within the range of 59.4–70.0 Gy, with a daily dose ranging from 1.8–2.2 Gy, and the treatment cycle was 5 days per week. For cases with ENE and/or a close surgical margin, concurrent chemoradiotherapy was utilized. Fluorouracil, platinum, and taxanes were adopted in the chemotherapy regimen. Accurate clinical staging was carried out in accordance with the 8th edition of the American Joint Committee on Cancer (AJCC) staging system in combination with pathological staging criteria. Figure 1 depicts the flow of the study, and Table 1 elaborates on the baseline characteristics for the cases enrolled in the study.
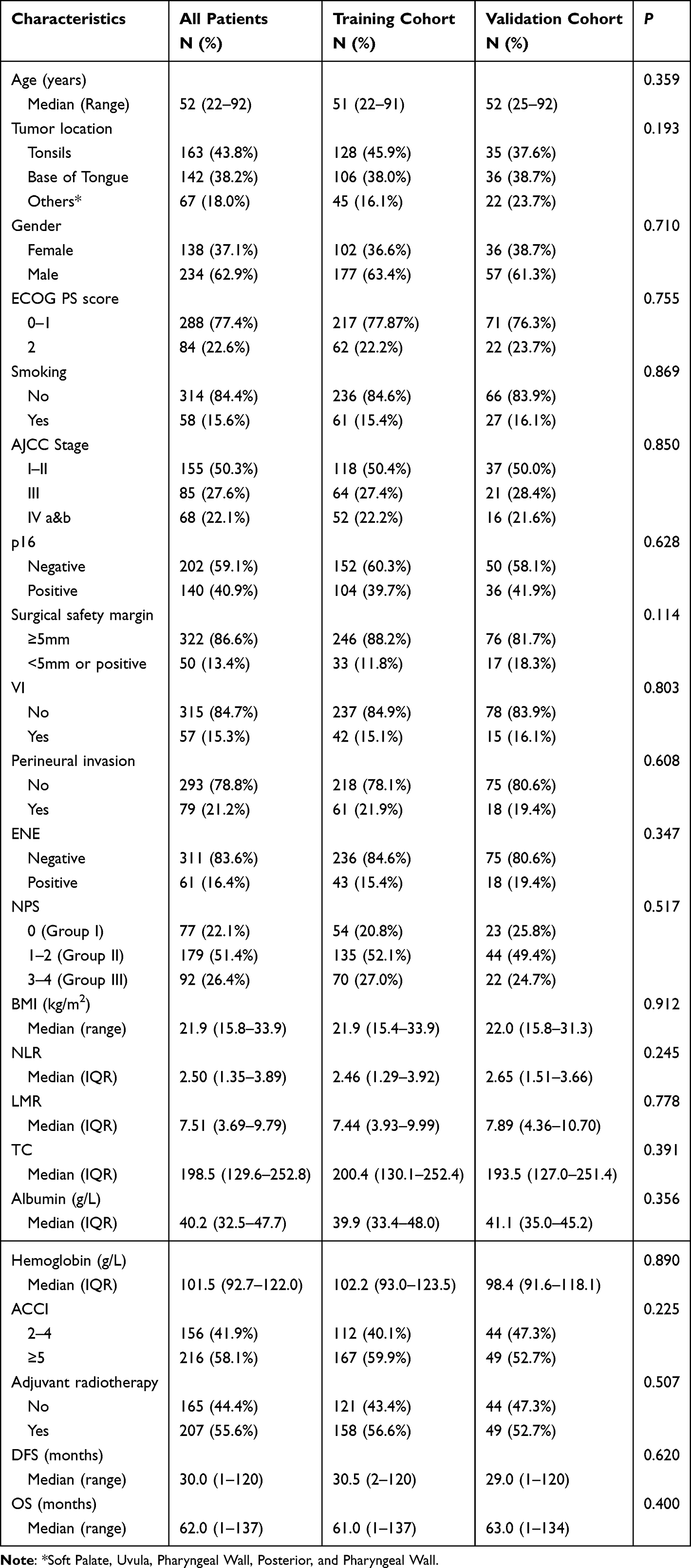 |
Table 1 The Baseline Characteristics of OPSCC Patients Following Surgical Treatment and the Disparities Between the Two Cohorts |
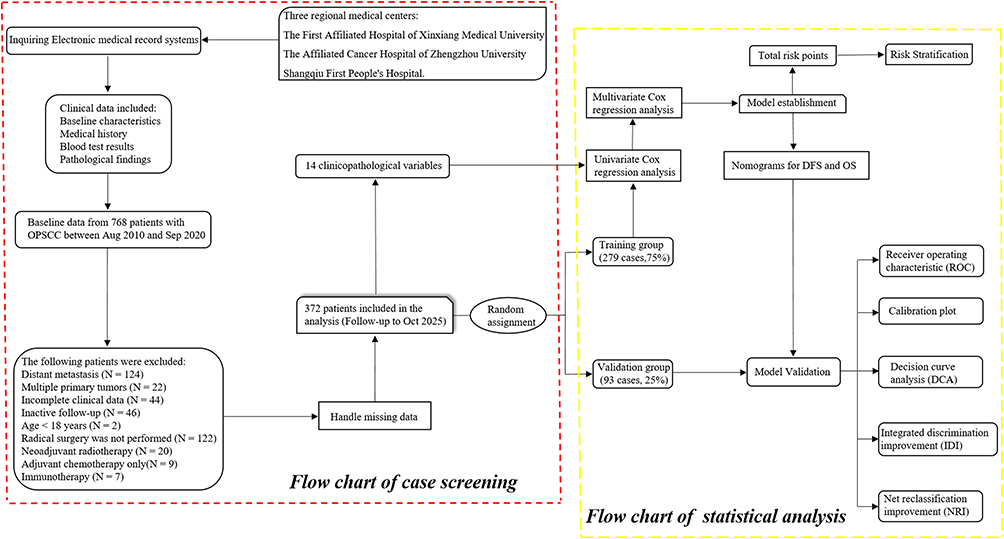 |
Figure 1 The flowchart illustrating the enrollment and exclusion procedure. The sample selection process is shown within the red dashed lines, while the statistical methods are depicted within the yellow dashed lines. Abbreviations: DCA, decision curve analysis; IDI, integrated discrimination improvement; NRI, net reclassification index; OPSCC, oropharyngeal squamous cell carcinoma; ROC, receiver operating characteristic. |
Variables
The data utilized in this study encompassed 14 independent variables, which were retrieved from the electronic medical record system and patient follow - up records. The specific variables comprised: Age at diagnosis, tumor location, gender, ECOG PS score, AJCC stage, p16 expression, surgical safe margin, extranodal invasion (ENE), vascular invasion (VI), perineural invasion, Naples prognostic score (NPS), body mass index (BMI), age - adjusted Charlson comorbidity index (ACCI), utilization of adjuvant radiotherapy, disease - free survival (DFS), and overall survival (OS). The primary endpoints of the study were DFS and OS.
Calculation
Table S1 presents formulas for the computation of multiple preoperative inflammatory and nutritional indicators, including the NPS, lympho-to-neutrophil ratio (LMR), neutrophil-to-lymphocyte ratio (NLR), and BMI. Table S2 specifies the scoring methods for the ACCI. Moreover, the calculation process of the NPS score is presented once more in Figure S1 to enable a more lucid understanding of its calculation steps.
Analysis
Data analysis was carried out using X-tile (version 3.6.1), SPSS (version 26.0), and R (version 4.22) software. Initially, a normality analysis was conducted on the continuous variables within the baseline characteristics data (Table S3). Employing SPSS software, all patients were randomly partitioned into training and validation sets at an approximate ratio of 3:1. Subsequently, the disparities in baseline characteristics between the two groups were compared. Regarding categorical variables, the chi - square test was utilized, whereas for continuous variables, either the independent samples t - test (for data with a normal distribution) or the Mann–Whitney U-test (for data without a normal distribution) was implemented. To assess the presence of multicollinearity among the included independent variables, the Tolerance and variance inflation factor (VIF) values were computed through linear regression analysis, as detailed in Table S4. Variable screening and model building were both conducted on the training set. The objective was to construct a reliable prediction model through the systematic selection of variables associated with the outcome. Data from the training set were utilized to identify the most predictive features and to ascertain their significance in prediction via statistical analysis. The validation set is primarily employed to assess the external validation performance of the model and guarantee its generalization ability across different datasets.
In this study, diverse methods were employed to address missing data (Table S5), with appropriate imputation of variables conducted in accordance with the missing rate. Regarding variables with a missing rate of less than 5%, complete - case analysis was adopted to remove rows with fewer missing values due to the limited quantity of missing data. For variables exhibiting missing rates ranging from 5% to 20%, the predictive mean matching method was utilized for imputation. After the imputed data set was processed, an appropriate regression method was selected based on the variable type. Logistic Regression was applied to dichotomous variables, while Multinomial Regression was used for multinomial variables. These regression methods were employed to generate 10 imputed data sets, each of which was then independently analyzed using the Cox proportional - hazards model. By applying Rubin’s rules, the estimates from each data set were combined to obtain the pooled hazard ratio (HR) and its 95% confidence interval (CI), thereby ensuring the stability and accuracy of the analysis. On this foundation, univariate Cox regression analysis was carried out to screen potential prognostic factors among the 14 explanatory variables. Through univariate analysis, variables associated with DFS and OS were identified. Subsequently, multivariate Cox regression analysis was performed using stepwise backward elimination to further identify independent prognostic factors influencing DFS and OS.
After the identification of independent prognostic factors, two nomograms were constructed: one for the prediction of DFS and the other for the prediction of OS. These nomograms were established based on the independent prognostic factors and were intended to offer clinicians a straightforward and effective instrument for individualized risk assessment in clinical practice. Finally, to validate the predictive performance of the nomograms, a comprehensive evaluation was carried out using R software. Receiver operating characteristic (ROC) curves were constructed, integrated discrimination improvement (IDI) and net reclassification improvement (NRI) were calculated, and calibration curves were generated. Additionally, decision curve analysis (DCA) was performed to further evaluate the effectiveness and reliability of the nomograms in practical application.
Each patient is assigned a corresponding risk score within the respective nomogram. X - tile software was employed to determine the optimal cutoff point for classifying all patients into three distinct subgroups based on the risk score: high - risk, medium - risk, and low - risk groups. Consequently, an effective prognostic stratification system was established. Subsequently, the log - rank test and Kaplan - Meier curve were utilized to analyze the differences in DFS and OS among patients in different risk subgroups. Moreover, the effect of adjuvant radiotherapy on DFS and OS in these risk subgroups was evaluated using a log - rank test to elucidate the role and effectiveness of adjuvant radiotherapy in different prognostic risk subgroups.
The study was reported in strict accordance with the REporting of studies Conducted using Observational Routinely-collected health Data (RECORD) guidelines.31 A comprehensively completed RECORD checklist and a study flow chart (if applicable) have been presented as supplementary material (Table S6).
Results
Descriptive Statistics
In this study, a total of 372 patients were included, and the clinicopathological characteristics are presented in Table 1. The median age was 52 years, with an age range from 22 to 92 years. The tumor location was as follows: 163 patients (43.8%) had tumors in the tonsil, 142 patients (38.2%) had tumors in the tongue base, and 67 patients (18.0%) had tumors in other locations. The expression of p16 was negative in 202 patients (59.1%) and positive in 140 patients (40.9%). The gender distribution was as follows: there were 138 female patients (37.1%) and 234 male (62.9%) patients. Regarding adjuvant radiotherapy, 165 patients (44.4%) did not receive radiotherapy, while 207 patients (55.6%) received it. The distribution of the Napus prognostic score (NPS) was as follows: 77 patients (22.1%) belonged to NPS = 0, 179 patients (51.4%) belonged to NPS = 1–2, and 92 patients (26.4%) belonged to NPS = 3–4. Additionally, Table 1 presents a comparison of the baseline characteristics between the training group and the validation group. The results indicate that there are no significant differences among all the baseline characteristics.
Univariate and Multivariate Analysis Results
Prior to commencing the analysis, a multicollinearity test was conducted on all the variables incorporated in both the univariate and multivariate analyses. The results are presented in Table S4. All VIF values were less than 5, indicating that there was no substantial multicollinearity among the variables.
In terms of predicting DFS (Table 2), univariate analysis indicated that age, AJCC stage, p16 status, surgical margin, vascular invasion, perineural invasion, extranodal invasion, Naples prognostic score, and age - adjusted comorbidity index were significantly correlated with DFS. Multivariate analysis further determined five independent prognostic factors: advanced AJCC stage (stage III: HR = 1.55, 95% CI 1.04–2.31, P = 0.033; stage IVa&b: HR = 2.18, 95% CI 1.47–3.24, P < 0.001), p16 positivity (HR = 0.70, 95% CI 0.50–0.98, P = 0.039), perineural invasion (HR = 1.82, 95% CI 1.23–2.68, P = 0.003), higher Naples prognostic score (NPS 3–4, Group III: HR = 1.96, 95% CI 1.20–3.20, P = 0.007), and higher age - adjusted comorbidity index (ACCI ≥ 5: HR = 1.71, 95% CI 1.20–2.44, P = 0.003). Similarly, prognostic variables influencing OS were analyzed (Table 3). Univariate analysis indicated that an ECOG PS score of 2 or higher, a later AJCC stage, p16 negativity, an inadequate surgical margin, VI, PNI, ENE, a higher NPS, and a higher ACCI were significantly correlated with OS. Multivariate analysis further identified five independent prognostic factors: an advanced AJCC stage (stage III: HR = 1.59, 95% CI 1.05–2.41, P = 0.029; stage IVa&b: HR = 2.22, 95% CI 1.46–3.38, P < 0.001), p16 positivity (HR = 0.67, 95% CI 0.47–0.96, P = 0.029), perineural invasion (HR = 1.88, 95% CI 1.23–2.89, P = 0.004), a higher NPS (NPS 3–4, Group III: HR = 2.38, 95% CI 1.40–4.06, P = 0.001), and a higher ACCI (≥5: HR = 1.51, 95% CI 1.04–2.20, P = 0.030).
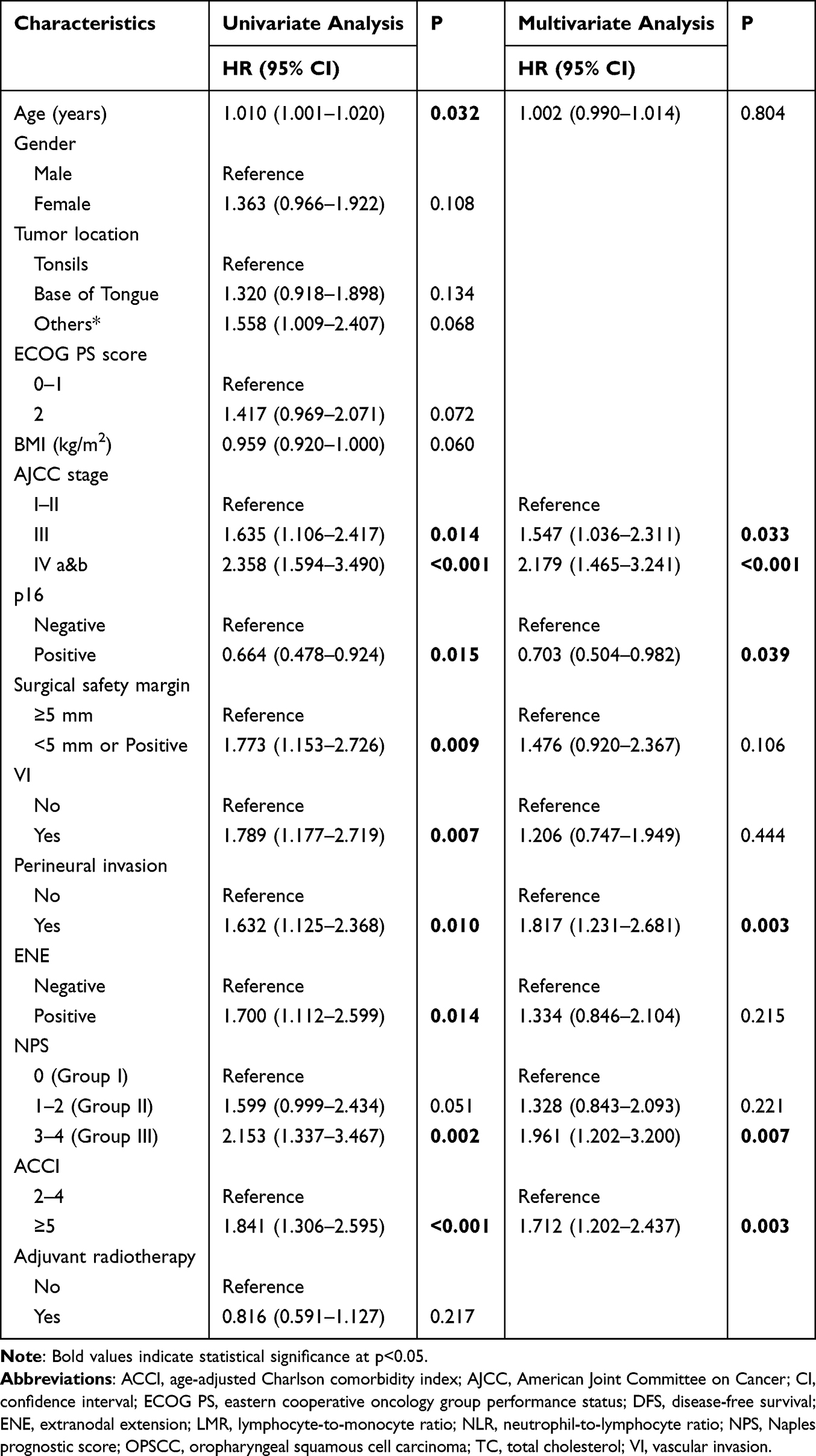 |
Table 2 Univariate and Multivariate Cox Regression Analyses of Variables in OPSCC Patients Undergoing Curative-Intent Surgery for DFS |
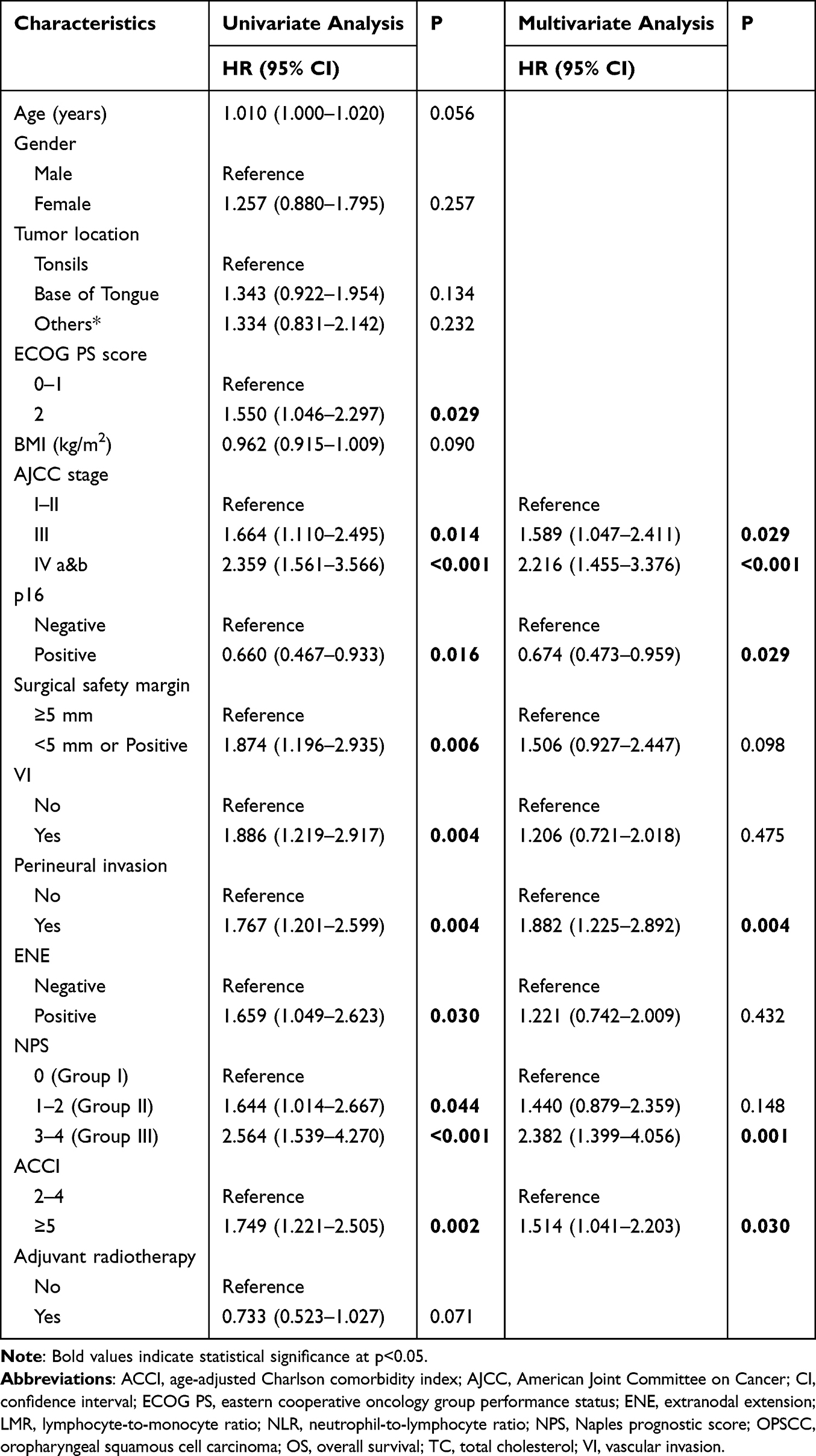 |
Table 3 Univariate and Multivariate Cox Regression Analyses of Variables in OPSCC Patients Undergoing Curative-Intent Surgery for OS |
Nomogram Establishment
Based on the independent prognostic factors identified through multivariate Cox regression analysis, we respectively constructed a nomogram model for predicting DFS and overall OS. Figure 2 presents the nomograms and an example of utilizing the nomograms to predict the prognosis of a specific patient. The concordance index (C-index) values of the new model for DFS and OS were 0.661 and 0.665, respectively, indicating that the new model might possess borderline acceptable discrimination. Comprehensive ROC curve analysis indicated that when the novel model was employed to predict the 3-year and 5-year OS and DFS, the area under the curve (AUC) values of the training set and the validation set exceeded 0.65 (Figure 3). In conjunction with the aforementioned C-index results, the stable and reliable predictive performance of the novel model was verified. The calibration plot is in close proximity to the diagonal (Figure 4), which demonstrates that the predicted probability of the model exhibits a high degree of agreement with the observed actual probability. The DCA results demonstrated that, compared with the current AJCC staging criteria, the application of the nomogram model developed in this study for risk stratification and clinical decision-making may provide greater clinical net benefit to patients across a broad range of threshold probabilities (Figure 5). In addition, Table 4 indicated that all NRI and IDI were >0, all P<0.001, suggesting that the new model was significantly better than the traditional AJCC staging system in risk classification accuracy and overall discrimination ability.
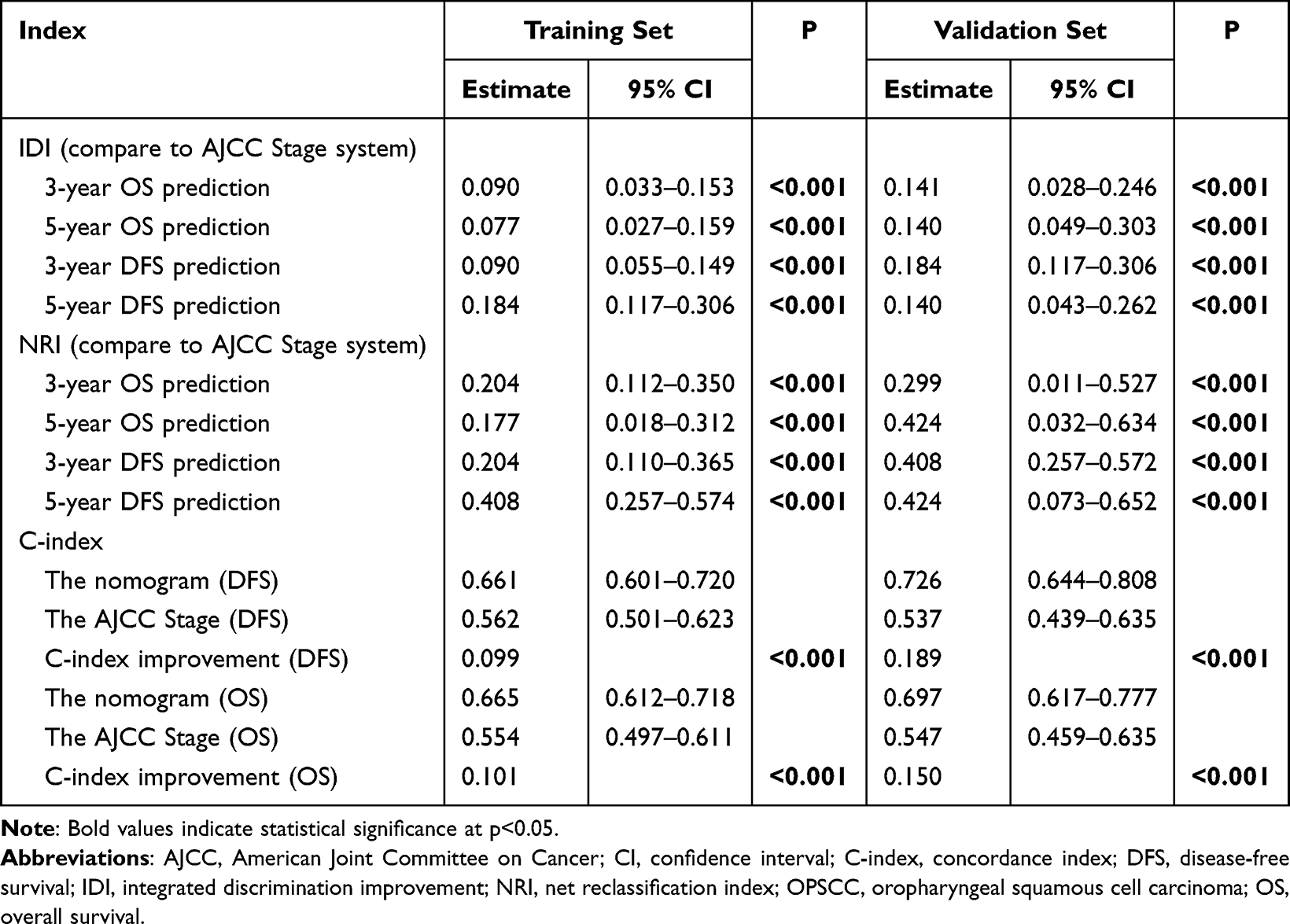 |
Table 4 The IDI, NRI, and C-Index of the Nomogram, as Well as the Improvement in Their Predictive Value for OS and DFS Compared with the AJCC Stage Among OPSCC Patients Undergoing Curative-Intent Surgery |
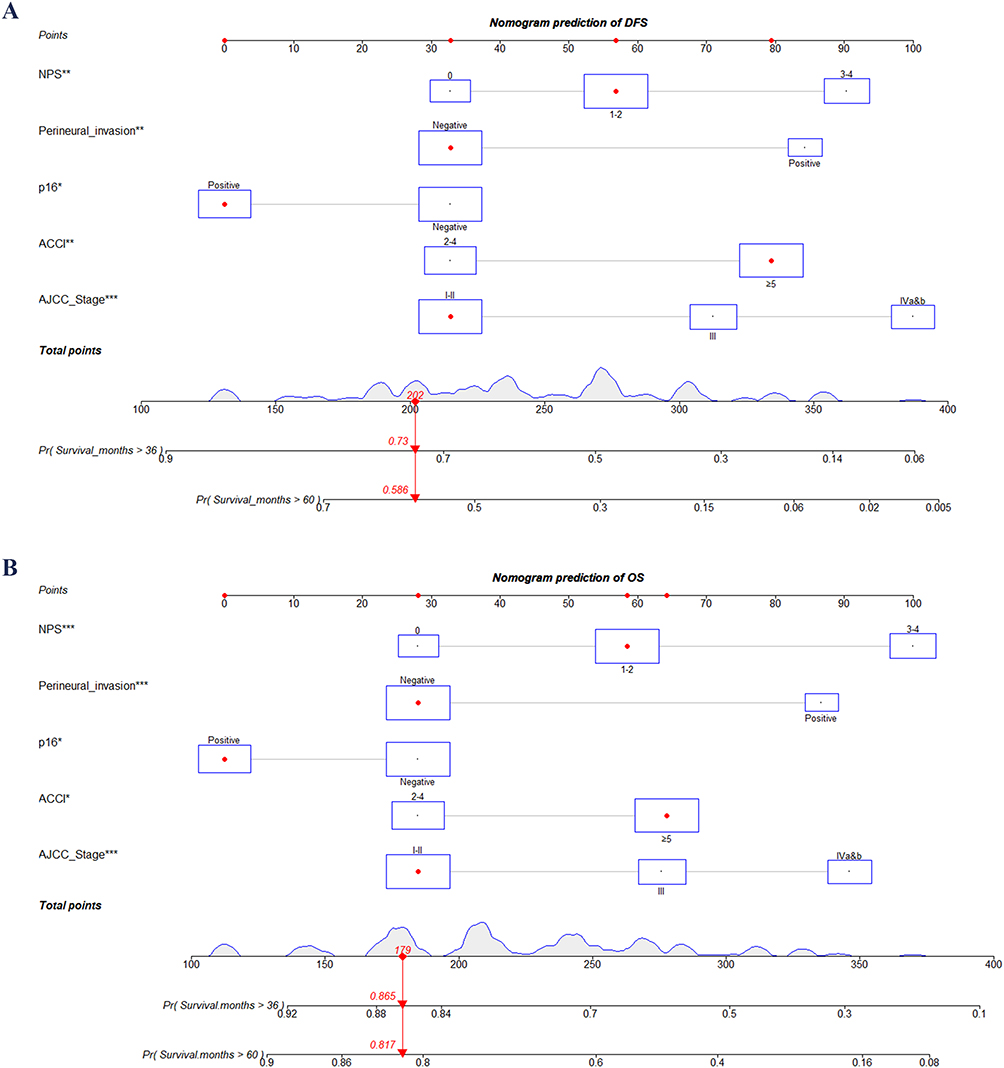 |
Figure 2 Nomogram-based prediction of DFS (A) and OS (B) in OSCC patients undergoing curative-intent surgery. Abbreviations: ACCI, age-adjusted Charlson comorbidity index; AJCC, American Joint Committee on Cancer; DFS, disease-free survival; NPS, Naples prognostic score; OPSCC, oropharyngeal squamous cell carcinoma; OS, overall survival. |
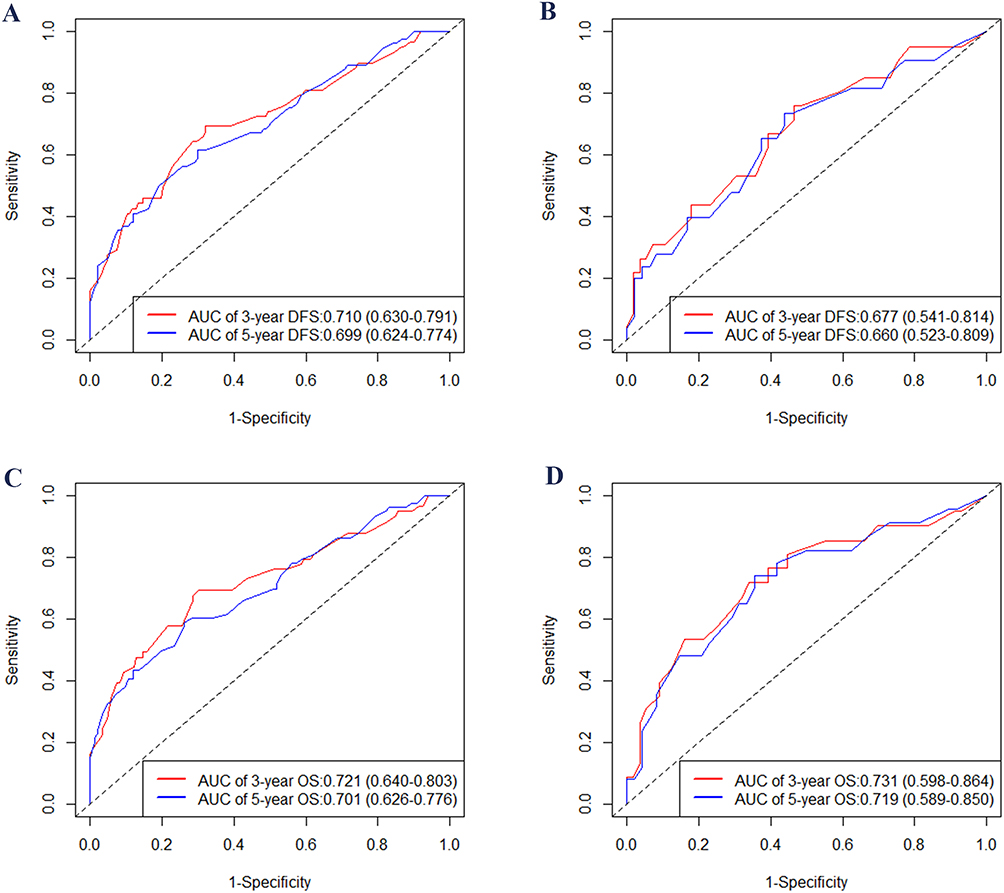 |
Figure 3 Time-dependent ROC curves of the nomograms. The AUC values for predicting 3- and 5-year DFS in the training (A) and validation (B) cohorts, as well as the AUC values for 3- and 5-year OS in the training (C) and validation (D) cohorts, are shown. Abbreviations: AUC, area under curve; OS, overall survival; DFS, disease-free survival; ROC, receiver operating characteristic. |
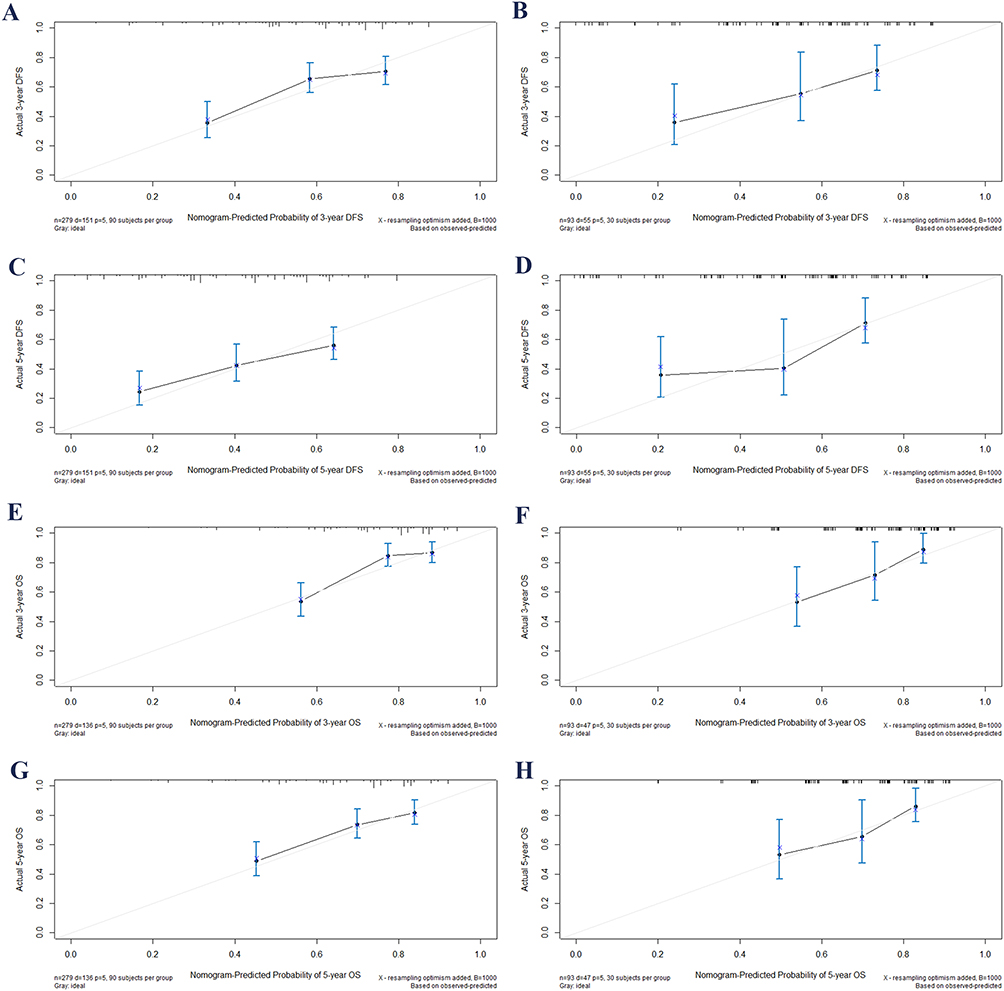 |
Figure 4 Calibration plots for 3- and 5-year DFS and OS in OPSCC patients undergoing curative-intent surgery. Calibration plots of 3-, and 5-year DFS in the training cohort (A and C), as well as in the validation cohort (B and D). Calibration plots of 3- and 5-year OS in the training cohort (E and G), as well as in the validation cohort (F and H). Abbreviations: OS, overall survival; DFS, disease-free survival; OPSCC, oropharyngeal squamous cell carcinoma. |
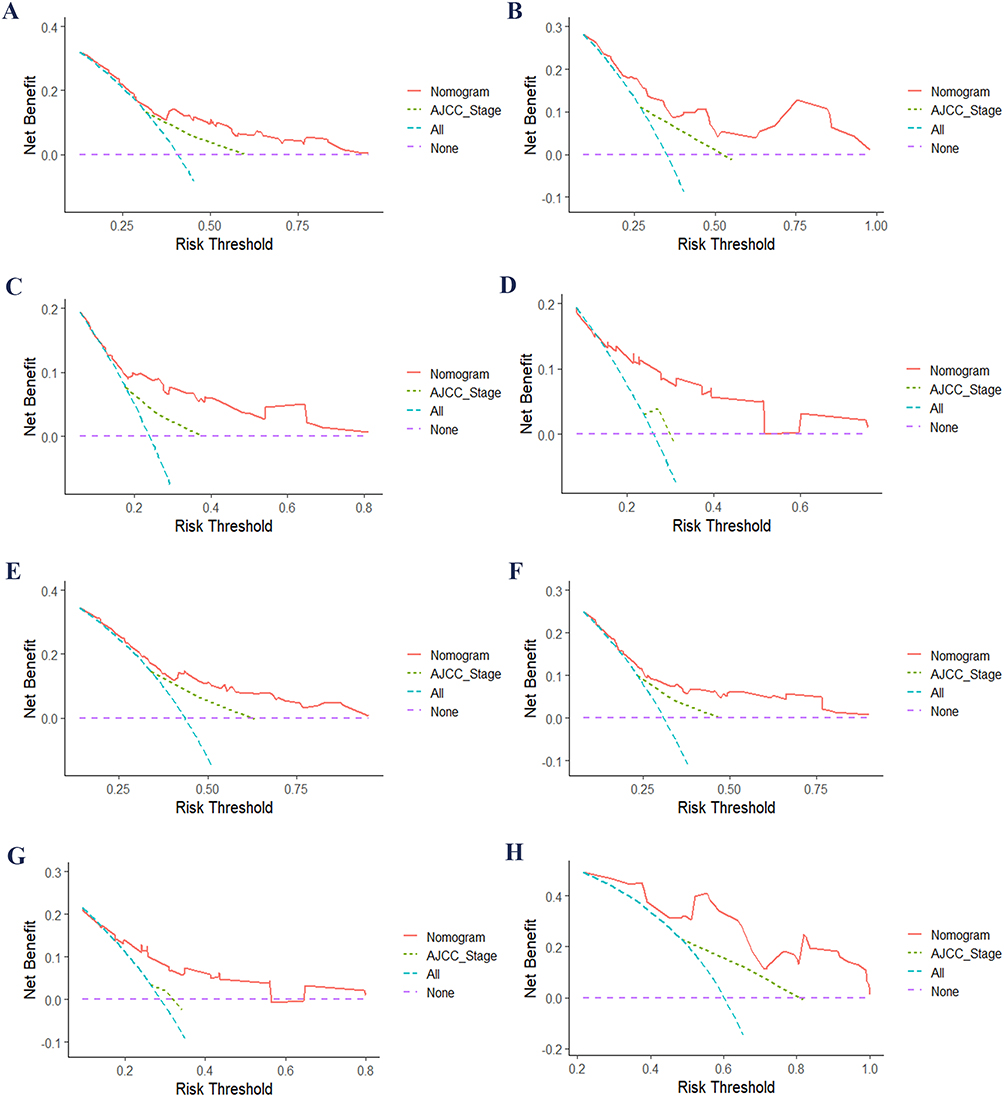 |
Figure 5 DCA of nomograms and AJCC stage for DFS and OS: DCA curves for 3- and 5-year DFS in the training (A and E) and validation (B and F) cohorts; DCA curves for 3- and 5-year OS in the training (C and G) and validation (D and H) cohorts. Abbreviations: AJCC, American Joint Committee on Cancer; DCA, decision curve analysis; DFS, disease-free survival; OS, overall survival. |
Sensitivity Analysis for Missing Data
To evaluate the robustness of multiple imputation for the missing AJCC staging data (18.1%), a complete case analysis (n = 305) was carried out. The outcomes were in line with those from the imputed data set, featuring similar independent prognostic factors and comparable C - index values (DFS: 0.658 vs 0.661; OS: 0.662 vs 0.665; Table S8), which verified the robustness of the study findings.
Establishment of Risk Stratification System
Based on the total risk score, patients were classified into three groups: the high - risk group with a total risk score of ≥120.5, the medium - risk group with a total risk score ranging from 77.0 to 118.0, and the low - risk group with a total risk score of ≤78.9. In the prediction of OS, a total risk score of 133.5 or higher was defined as the high - risk group, a score ranging from 80.4 to 132.0 as the medium - risk group, and a score of 79.9 or lower as the low - risk group. Through the analysis of the Kaplan - Meier survival curve (log - rank test), the results demonstrated significant differences in DFS and OS among the three groups (as shown in Figure 6), suggesting that the survival outcomes of the training set and the validation set were notably different. A further analysis of the impact of adjuvant radiotherapy on survival outcomes revealed that adjuvant radiotherapy was associated with an improved prognosis for patients in the high - risk group, while patients in the medium - and low - risk groups did not gain any benefit from adjuvant radiotherapy in terms of DFS or OS (as shown in Figure 7 and Table S7).
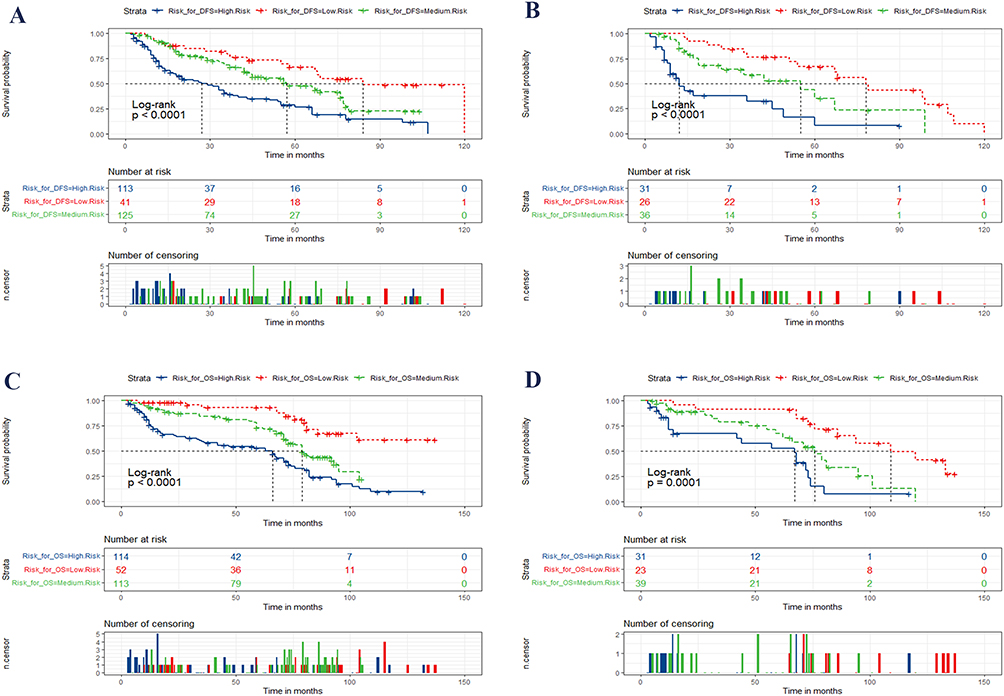 |
Figure 6 Kaplan-Meier curves based on the new risk stratification system for OPSCC patients undergoing curative-intent surgery. The new risk stratification system was used to predict DFS and OS in the training cohort (A and C) and the validation cohort (B and D). Abbreviations: AJCC, American Joint Committee on Cancer; DFS, disease-free survival; OPSCC, oropharyngeal squamous cell carcinoma; OS, overall survival. |
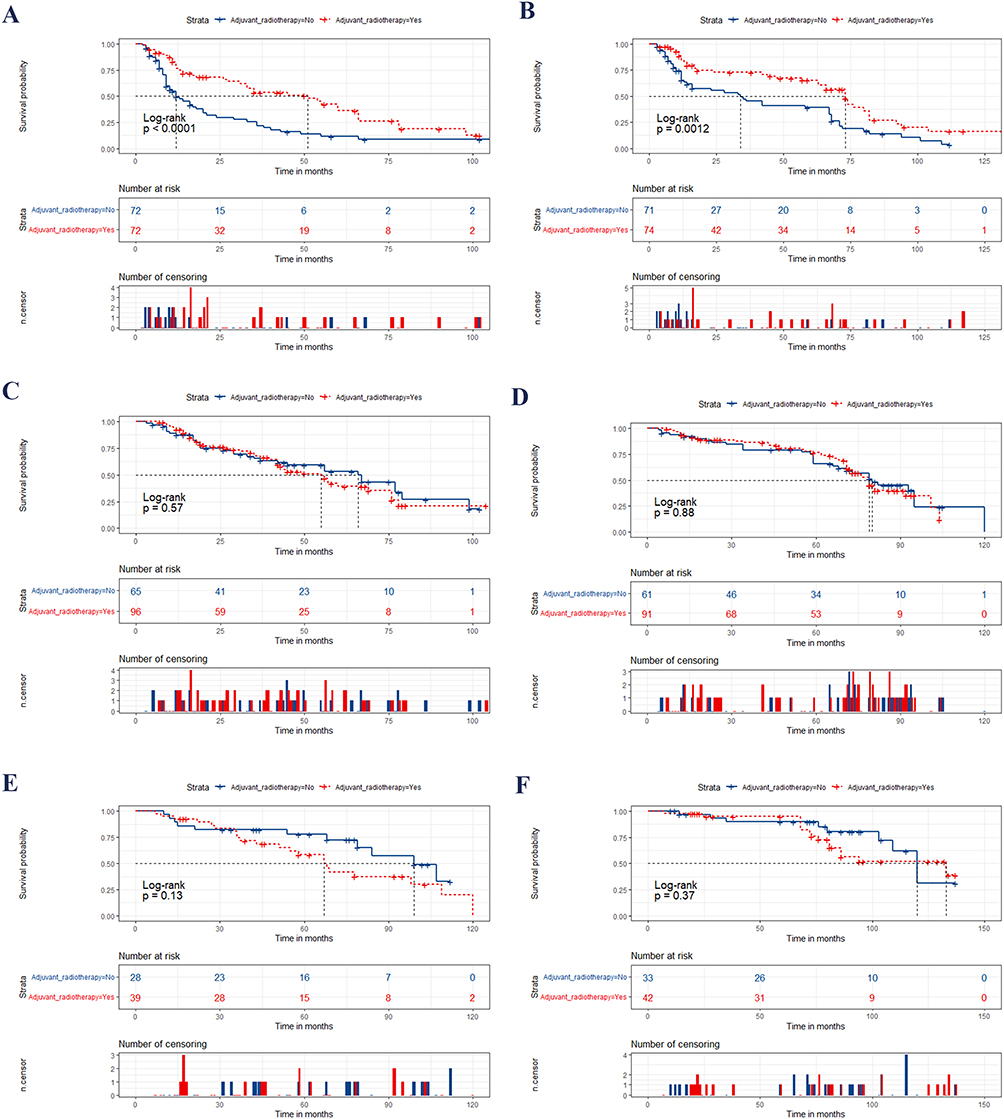 |
Figure 7 Kaplan-Meier curves based on the new risk stratification system to predict the impact of adjuvant radiotherapy on DFS and OS across different subgroups. Kaplan-Meier curves (A, C, and E) demonstrate the impact of adjuvant radiotherapy on DFS in the high-, medium-, and low-risk groups, respectively. Kaplan-Meier curves (B, D, and F) illustrate the effect of adjuvant radiotherapy on OS in the high-, medium-, and low-risk groups, respectively. Abbreviations: DFS, disease-free survival; OS, overall survival. |
Discussion
Accurate and reliable individualized prognostic assessment remains a central challenge in clinical decision-making. In recent years, advances in statistical methodology and the accumulation of clinical data have enabled the widespread application of various predictive models for prognosis across multiple cancer types. Among these, nomograms translate multivariable prediction models into intuitive graphical formats, facilitating quantitative, individualized estimation of clinical outcome risk.30,32 Previous research has indicated that the nomogram surpasses the traditional AJCC staging system in terms of prognostic prediction performance for a variety of malignancies.32 Consequently, it is regarded as an important supplement to the AJCC staging system and may even have potential alternative value in specific clinical scenarios. In the context of OPSCC, previous studies have developed standardized nomograms and risk stratification models across various research directions.33–36 This not only facilitates the unification of prognosis assessment and risk stratification for patients but also offers a scientific foundation for individualized treatment decisions in clinical practice and patient inclusion and stratification in clinical trials. In this context, our study further developed and validated a nomogram model specifically designed for predicting DFS and OS in patients with OPSCC who underwent radical surgery. The findings demonstrated that the newly developed nomogram exhibited good discriminatory ability in predicting DFS and OS, with C - indexes of 0.661 and 0.665 respectively, which were 0.99 and 1.01 higher than those of the AJCC staging system. This nomogram outperforms traditional staging in individualized prognosis for postoperative OPSCC patients, enabling more precise risk stratification and clinical decision-making.
Inflammation and nutritional imbalance are intricately associated with the prognosis of various malignant tumors. An increasing number of studies have indicated that certain routine blood examination indicators are crucial for the survival prognosis of patients.21,22,37–40 Emerging evidence suggests that these systemic conditions are not merely epiphenomena but actively participate in shaping the tumor immune microenvironment.41–43 From a biological perspective, the prognostic value of NPS may be closely associated with the TIME.42,44 Head and neck cancers are characterized by a highly immunosuppressive microenvironment, where various immune cells, including tumor-associated macrophages, neutrophils, and regulatory T cells, interact with tumor cells to promote tumor progression and immune evasion.44,45 Neutrophils can enhance tumor growth by releasing pro-inflammatory cytokines and angiogenic factors, whereas lymphocytes, particularly cytotoxic T cells, play a key role in anti-tumor immunity.41,45 A decreased lymphocyte count may therefore indicate impaired immune surveillance.41 Moreover, nutritional status is tightly linked to immune function.17,46 Serum albumin not only reflects nutritional status but also serves as an indicator of systemic inflammation and immune competence.46 Hypoalbuminemia has been associated with increased inflammatory burden and weakened immune response.46 In addition, cholesterol metabolism plays an important role in maintaining immune cell membrane integrity and signaling pathways, and its dysregulation may further impair immune responses.43 Recent studies have emphasized the close relationship between inflammatory-nutritional indices and tumor immunity in head and neck cancers.17,42 For instance, Litsou (2025) highlighted the central role of immune cells in shaping an immunosuppressive tumor microenvironment,44 while Uri et al (2024) demonstrated that nutritional indices are strongly associated with survival outcomes.17 These findings support the hypothesis that systemic inflammatory markers may serve as indirect indicators of tumor immune status.41,45
In recent years, the NPS, a comprehensive marker reflecting the inflammatory and nutritional status of patients, has garnered extensive attention. The NPS integrates multiple biological indicators commonly employed in clinical practice, such as albumin level, neutrophils, lymphocytes, monocytes, and total cholesterol, enabling a more comprehensive assessment of patients’ health status.23 This nomogram improves individualized prognosis for postoperative OPSCC patients beyond traditional staging, supporting more precise risk stratification and clinical decisions. Numerous studies have substantiated the significant clinical value of the NPS in the prognosis evaluation of diverse cancers. In a study of 126 patients, Yanfei Zhang et al confirmed the prognostic role of NPS in SCLC patients receiving neoadjuvant chemotherapy and surgery, with higher NPS suggesting a possible poor OS.47 In the research on esophageal cancer, Chen, W et al identified NPS as an independent prognostic factor for the prognosis of esophageal squamous cell carcinoma.48 In the context of hepatocellular carcinoma research, the findings of a study encompassing 476 patients with hepatocellular carcinoma indicated that patients with higher NPS exhibited lower OS and recurrence - free survival (RFS).49 In addition, the exploration of the prognostic value of NPS in gallbladder cancer has also yielded favorable research outcomes.50 Multivariate analysis indicated that NPS was an independent risk factor influencing OS. The prognostic model of gallbladder cancer based on NPS also demonstrated satisfactory performance. In the context of the prognosis study of head - and - neck cancer, the NPS exhibited a significant correlation with the prognosis of oral51 and hypopharyngeal carcinoma.29 Some researchers have also conducted investigations into the prognostic value of the Modified Naples Prognostic Score among patients with Oral Squamous Cell Carcinoma.52 Although many studies link NPS to tumor prognosis, no such research exists for OPSCC. Consequently, this study is the first to bridge this research gap by investigating the relationship between NPS and OPSCC prognosis. Moreover, this study not only represents the first attempt to incorporate NPS into the prognostic model of OPSCC but also the first to establish a risk stratification system based on NPS, which is both significant and innovative.
High-risk HPV infection is commonly assessed indirectly by detecting the overexpression of the p16 protein and has been extensively validated as a strong predictor of favorable prognosis in OPSCC.5 Compared with HPV-negative tumors, HPV-positive OPSCC exhibits distinct biological characteristics and demonstrates increased sensitivity to radiotherapy,53–55 resulting in superior treatment responses and improved survival outcomes. One of the most significant updates in the 8th edition of the AJCC staging system is the establishment of a distinct staging system for high - risk HPV - associated oropharyngeal cancer. The 8th Edition of the AJCC staging system introduces a separate staging system for high-risk HPV–associated OPSCC—a major update reflecting its strong prognostic value.11,12 The results of the current study also indicate that patients associated with HPV have a more favorable prognosis, which is in line with the findings of other studies investigating the prognosis of OPSCC.6,14,56
In the present study, perineural invasion, another pathological feature incorporated into the prediction model, was identified as an independent adverse prognostic factor. Its presence was strongly associated with poor survival outcome. This finding is consistent with previous research. For instance, Albergotti et al reported that perineural invasion was significantly correlated with event - free and overall survival among 201 patients with HPV - positive oropharyngeal cancer.57 Similarly, Miles et al concluded in an analysis of HPV - positive patients who underwent surgery that perineural invasion was associated with worse survival.58 Moreover, a 2024 meta - analysis indicates that perineural invasion is also strongly associated with poor prognosis in surgically treated HPV - negative patients.59 These findings suggest that perineural invasion reflects the aggressive nature of the tumor and holds important predictive value for postoperative patient survival. It is emphasized that its presence should be fully considered in postoperative risk assessment and individualized treatment decisions.
When discussing the prognosis of OPSCC, comorbidities should be duly considered. The impact of comorbidities on the prognosis of oropharyngeal cancer is evident, as has been confirmed by numerous studies.18,60,61 The ACCI is computed by integrating multiple prevalent comorbidities, assigning a weighted score to each comorbidity, and ultimately calculating an aggregate score. This score facilitates the assessment of the patient’s overall health, particularly in the field of oncology, where it can assist physicians in predicting patient survival, treatment risk, complication rate, and other relevant factors. The predictive capacity of the ACCI for survival in malignant tumors has been substantiated in multiple studies.51,62–66 This study represents the initial endeavor to investigate the utilization of the ACCI for survival prediction in OPSCC. A higher ACCI was significantly associated with poorer survival, consistent with findings in other cancers. These results may offer new insights for clinical practice.
It is important to note that while ENE and surgical margin status were significantly correlated with prognosis in univariate analysis, they did not emerge as independent prognostic factors in multivariate analysis. The possible reasons are as follows: patients with positive ENE or positive margins underwent more postoperative adjuvant radiotherapy, and radiotherapy itself can enhance prognosis, thus attenuating the independent predictive impact of these two factors on prognosis. Additionally, the sample size and the number of events in this study may have been insufficient to detect their independent effects after multiple corrections. It is important to emphasize that the ENE and the status of the resection margin continue to be of significant importance in clinical practice, especially in guiding decisions related to postoperative adjuvant therapy.67 As this study centered on the prognostic value of NPS, the aforementioned two factors were not investigated in depth.
Although this study offers valuable insights into the prognostic assessment of patients with OPSCC and incorporates the NPS into a prognostic model for the first time, certain limitations exist. Firstly, the study adopted a retrospective, multicenter design. Despite the large sample size, variations in treatment protocols among centers may be present, which could impact the generalizability of the findings. Retrospective studies are prone to selection bias and information bias, and it is difficult to establish causal relationships. Secondly, our study solely included patients who underwent radical surgery, and the effects of other treatment modalities (eg, definitive concurrent chemoradiotherapy or sequential chemoradiotherapy) were not taken into account. Hence, the applicability of our conclusions in different treatment settings requires further verification. Thirdly, although multiple approaches were employed to handle missing data, bias introduced by missing data may still persist. Fourthly, our study used p16 immunohistochemistry as a surrogate marker for HPV status without confirmatory HPV DNA/RNA testing by polymerase chain reaction (PCR). Although p16 overexpression is a widely accepted surrogate in clinical practice, misclassification may occur in a small proportion of cases. Future studies should incorporate molecular HPV confirmation to improve diagnostic accuracy. Sixth, the absence of genomic or molecular profiling data in this study precludes exploration of the potential biological interactions between the Naples Prognostic Score and tumor molecular subtypes. Future studies incorporating multi-omics data are warranted to further elucidate these mechanisms. Additionally, while this study established a prognostic risk stratification system based on NPS, the clinical practicality and operability of this system demand verification in large - scale prospective studies. Finally, the statistical models and scoring systems utilized in this study did not comprehensively consider some potential confounding factors, such as regional disparities, genetic background, living habits, psychological state, economic status, and differences in the tumor microenvironment, which may affect the accuracy and generalization ability of the models. It should be emphasized that the model we constructed is not applicable to clinical decision-making and is positioned merely for exploratory analysis. The current C-index is low and that the model is not ready for independent clinical application, but should be considered only as an exploratory tool. The results of this study should be further validated and optimized in future research to ensure their application in a broader range of clinical settings.
Conclusion
This study ascertained that the NPS was one of the independent prognostic factors for DFS and OS in patients with OPSCC following surgery. In conjunction with the AJCC stage, p16 expression, perineural invasion, and the ACCI, two nomogram models was established to predict DFS and OS, in which NPS played a pivotal role. The predictive ability of this model was superior to that of the traditional AJCC staging. Based on the risk stratification, the patients were classified into high-, medium-, and low-risk groups. Adjuvant radiotherapy can significantly enhance the prognosis of patients in the high-risk group, whereas patients in the low- and medium-risk groups do not derive significant benefits.
Abbreviations
ACCI, age-adjusted Charlson comorbidity index; AJCC, American Joint Committee on Cancer; AUC, area under curve; BMI, body mass index; CI, confidence interval; C-index, concordance index; DCA, decision curve analysis; DFS, disease-free survival; ECOG PS, eastern cooperative oncology group performance status; ENE, extranodal extension; HR, hazard ratio; IDI, integrated discrimination improvement; IQR, interquartile range; LMR, lymphocyte-to-monocyte ratio; NLR, neutrophil-to-lymphocyte ratio; NPS, Naples prognostic score; NRI, net reclassification index; OPSCC, oropharyngeal squamous cell carcinoma; OS, overall survival; PCR, polymerase chain reaction; RECORD, REporting of studies Conducted using Observational Routinely-collected health Data; ROC, receiver operating characteristic; TIME, tumor immune microenvironment; TC, total cholesterol; VI, vascular invasion; VIF, variance inflation factor.
Data Sharing Statement
The corresponding author can provide the data upon a reasonable request.
Ethics Statement
This study adhered to the Declaration of Helsinki and received approval from the Ethics Committees of the First Affiliated Hospital of Xinxiang Medical University (Ethics number: EC 2025742). The requirement for informed consent was formally waived by the Ethics Committees due to the retrospective nature of this study.
Acknowledgments
Thanks to all researchers involved in this study for their valuable contributions.
Author Contributions
XM: Investigation, Data curation, Formal analysis, Visualization, Writing – original draft; JW: Investigation, Data curation, Writing – review & editing; WS: Investigation, Data curation, Writing – review & editing; SY: Investigation, Data curation, Writing – review & editing; KZ: Investigation, Data curation, Writing – review & editing; JW: Investigation, Data curation, Writing – review & editing; QH: Investigation, Data curation, Writing – review & editing; XC: Investigation, Data curation, Writing – review & editing; HC: Methodology, Formal analysis, Funding acquisition, Writing – original draft, Writing – review & editing; XX: Conceptualization, Methodology, Funding acquisition, Visualization, Writing – review & editing. All authors gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
The research was supported from the funding of Natural Science Fundation of Henan Province (232300420281), and the Joint Project of Henan Province and Ministry (LHGJ20200516).
Disclosure
All the authors declare no conflicts of interest, financial or otherwise, related to this research.
References
1. Chi AC, Day TA, Neville BW. Oral cavity and oropharyngeal squamous cell carcinoma--an update. CA Cancer J Clin. 2015;65(5):401–20. doi:10.3322/caac.21293
2. Bray F, Ferlay J, Soerjomataram I, Siegel RL, Torre LA, Jemal A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2018;68(6):394–424. doi:10.3322/caac.21492
3. Zumsteg ZS, Luu M, Rosenberg PS, et al. Global epidemiologic patterns of oropharyngeal cancer incidence trends. J Natl Cancer Inst. 2023;115(12):1544–1554. doi:10.1093/jnci/djad169
4. Ferris RL, Westra W. Oropharyngeal carcinoma with a special focus on HPV-related squamous cell carcinoma. Annu Rev Pathol. 2023;18(1):515–535. doi:10.1146/annurev-pathmechdis-031521-041424
5. Lechner M, Liu J, Masterson L, Fenton TR. HPV-associated oropharyngeal cancer: epidemiology, molecular biology and clinical management. Nat Rev Clin Oncol. 2022;19(5):306–327. doi:10.1038/s41571-022-00603-7
6. Ang KK, Harris J, Wheeler R, et al. Human papillomavirus and survival of patients with oropharyngeal cancer. N Engl J Med. 2010;363(1):24–35. doi:10.1056/NEJMoa0912217
7. Leemans CR, Snijders PJF, Brakenhoff RH. The molecular landscape of head and neck cancer. Nat Rev Cancer. 2018;18(5):269–282. doi:10.1038/nrc.2018.11
8. Arends J, Bachmann P, Baracos V, et al. ESPEN guidelines on nutrition in cancer patients. Clin Nutr. 2017;36(1):11–48. doi:10.1016/j.clnu.2016.07.015
9. Gonzalez H, Hagerling C, Werb Z. Roles of the immune system in cancer: from tumor initiation to metastatic progression. Genes Dev. 2018;32(19–20):1267–1284. doi:10.1101/gad.314617.118
10. Pfister DG, Spencer S, Adelstein D, et al. Head and neck cancers, Version 2.2020, NCCN clinical practice guidelines in oncology. J Natl Compr Canc Netw. 2020;18(7):873–898. doi:10.6004/jnccn.2020.0031
11. Huang SH, O’Sullivan B. Overview of the 8th Edition TNM classification for head and neck cancer. Curr Treat Options Oncol. 2017;18(7):40. doi:10.1007/s11864-017-0484-y
12. Lydiatt WM, Patel SG, O’Sullivan B, et al. Head and neck cancers-major changes in the American joint committee on cancer eighth edition cancer staging manual. CA Cancer J Clin. 2017;67(2):122–137. doi:10.3322/caac.21389
13. Kalavacherla S, Poulhazan S, Funk E, Sacco AG, Guo T. Sex-specific survival and treatment delay in oropharyngeal squamous cell carcinoma. Otolaryngol Head Neck Surg. 2024;171(3):764–776. doi:10.1002/ohn.795
14. Li J, Zhuo F, Wang X, Guo Y, Jiang L. Clinical data, survival, and prognosis of 426 cases of oropharyngeal cancer: a retrospective analysis. Clin Oral Investig. 2023;27(11):6597–6606. doi:10.1007/s00784-023-05265-y
15. Wu CY, Lin YH, Lo WC, et al. Nutritional status at diagnosis is prognostic for pharyngeal cancer patients: a retrospective study. Eur Arch Otorhinolaryngol. 2022;279(7):3671–3678. doi:10.1007/s00405-021-07222-5
16. Gan X, Gou Q, Zhu J, Zhang T. Dynamic change of the systemic immune inflammation index is a risk factor for patients with oropharyngeal cancer: a case control study and an additional HPV-status subgroup analysis. Eur J Med Res. 2023;28(1):191. doi:10.1186/s40001-023-01157-9
17. Uri I, Horvath A, Tamas L, Polony G, Danos K. Prognostic nutritional index (PNI) correlates with survival in head and neck cancer patients more precisely than other nutritional markers - real world data. Eur Arch Otorhinolaryngol. 2024;281(12):6599–6611. doi:10.1007/s00405-024-08865-w
18. Olsen MH, Frederiksen K, Lassen P, et al. Association of smoking, comorbidity, clinical stage, and treatment intent with socioeconomic differences in survival after oropharyngeal squamous cell carcinoma in Denmark. JAMA Network Open. 2022;5(12):e2245510. doi:10.1001/jamanetworkopen.2022.45510
19. Litsou E, Goussia A, Sioka C, Katiniotis G, Zarkavelis G. Clinical and treatment approach of multiple head and neck cancers. MAEDICA. 2025;20(3):583–590. doi:10.26574/maedica.2025.20.3.583
20. Hong Q, Ding S, Xing C, Mu Z. Advances in tumor immune microenvironment of head and neck squamous cell carcinoma: a review of literature. Medicine. 2024;103(9):e37387. doi:10.1097/MD.0000000000037387
21. Zhou J, Wei S, Guo X, et al. Correlation between preoperative peripheral blood NLR, PLR, LMR and prognosis of patients with head and neck squamous cell carcinoma. BMC Cancer. 2023;23(1):1247. doi:10.1186/s12885-023-11752-y
22. Zhang CL, Gao MQ, Jiang XC, et al. Research progress and value of albumin-related inflammatory markers in the prognosis of non-small cell lung cancer: a review of clinical evidence. Ann Med. 2023;55(1):1294–1307. doi:10.1080/07853890.2023.2192047
23. Galizia G, Lieto E, Auricchio A, et al. Naples prognostic score, based on nutritional and inflammatory status, is an independent predictor of long-term outcome in patients undergoing surgery for colorectal cancer. Dis Colon Rectum. 2017;60(12):1273–1284. doi:10.1097/DCR.0000000000000961
24. Chen S, Liu S, Xu S, et al. Naples prognostic score is an independent prognostic factor in patients with small cell lung cancer and nomogram predictive model established. J Inflamm Res. 2022;15:3719–3731. doi:10.2147/JIR.S371545
25. Elia S, Patirelis A, Hardavella G, Santone A, Carlea F, Pompeo E. The Naples prognostic score is a useful tool to assess surgical treatment in non-small cell lung cancer. Diagnostics. 2023;13(24):3641.
26. Demir M, Demircan NC. The Naples prognostic score in esophagus cancer: prognostic and beyond. Bull Cancer. 2023;110(10):1027–1040. doi:10.1016/j.bulcan.2023.06.007
27. Xiu Y, Jiang C, Huang Q, et al. Naples score: a novel prognostic biomarker for breast cancer patients undergoing neoadjuvant chemotherapy. J Cancer Res Clin Oncol. 2023;149(17):16097–16110. doi:10.1007/s00432-023-05366-x
28. Xu XL, Cheng H. Development of a prognostic nomogram incorporating the Naples prognostic score for postoperative oral squamous cell carcinoma patients. J Inflamm Res. 2025;18:325–345. doi:10.2147/JIR.S500518
29. Xu XL, Cheng H. A novel survival prediction nomogram based on the Naples prognostic score and clinicopathological factors for postoperative hypopharyngeal squamous cell carcinoma patients. J Inflamm Res. 2025;18:7243–7262. doi:10.2147/JIR.S521901
30. Balachandran VP, Gonen M, Smith JJ, DeMatteo RP. Nomograms in oncology: more than meets the eye. Lancet Oncol. 2015;16(4):e173–180. doi:10.1016/S1470-2045(14)71116-7
31. Benchimol EI, Smeeth L, Guttmann A, et al. The REporting of studies conducted using observational routinely-collected health data (RECORD) statement. PLoS Med. 2015;12(10):e1001885. doi:10.1371/journal.pmed.1001885
32. Iasonos A, Schrag D, Raj GV, Panageas KS. How to build and interpret a nomogram for cancer prognosis. J Clin Oncol. 2008;26(8):1364–1370. doi:10.1200/JCO.2007.12.9791
33. Bossi P, Gili R, Calza S, et al. Validation of a prognostic nomogram for locally advanced oropharyngeal carcinoma treated with intensity-modulated radiotherapy with/without systemic therapy. ESMO Open. 2025;10(11):105859. doi:10.1016/j.esmoop.2025.105859
34. Cheng NM, Yao J, Cai J, et al. Deep learning for fully automated prediction of overall survival in patients with oropharyngeal cancer using FDG-PET imaging. Clin Cancer Res. 2021;27(14):3948–3959. doi:10.1158/1078-0432.CCR-20-4935
35. Costantino A, Paleri V, Holsinger FC, Alamoudi U, Haughey BH, Magnuson JS. Transoral surgery versus radiotherapy as primary treatment for HPV -related oropharyngeal cancer in the elderly. Head Neck. 2025;47(7):1867–1877. doi:10.1002/hed.28097
36. De Felice F, Humbert-Vidan L, Lei M, King A, Guerrero Urbano T. Dynamic nomogram for long-term survival in patients with locally advanced oropharyngeal cancer after (chemo)radiotherapy. Eur Arch Otorhinolaryngol. 2023;280(4):1955–1961. doi:10.1007/s00405-022-07757-1
37. Zhou Y, Liu X, Wu B, et al. AGR, LMR and SIRI are the optimal combinations for risk stratification in advanced patients with non-small cell lung cancer following immune checkpoint blockers. Int Immunopharmacol. 2025;149:114215. doi:10.1016/j.intimp.2025.114215
38. Tan S, Zheng Q, Zhang W, Zhou M, Xia C, Feng W. Prognostic value of inflammatory markers NLR, PLR, and LMR in gastric cancer patients treated with immune checkpoint inhibitors: a meta-analysis and systematic review. Front Immunol. 2024;15:1408700. doi:10.3389/fimmu.2024.1408700
39. Kubota K, Shimizu A, Notake T, et al. Preoperative peripheral blood lymphocyte-to-monocyte ratio predicts long-term outcome for patients with pancreatic ductal adenocarcinoma. Ann Surg Oncol. 2022;29(2):1437–1448. doi:10.1245/s10434-021-10848-8
40. Zeng H, Zhang D, Yang Z, et al. Cholesterol and C-reactive protein prognostic score predicted prognosis of immune checkpoint inhibitors based interventional therapies for intermediate-to-advanced hepatocellular carcinoma patients. Int Immunopharmacol. 2023;115:109651. doi:10.1016/j.intimp.2022.109651
41. Fridman WH, Pages F, Sautes-Fridman C, Galon J. The immune contexture in human tumours: impact on clinical outcome. Nat Rev Cancer. 2012;12(4):298–306. doi:10.1038/nrc3245
42. Chen SMY, Krinsky AL, Woolaver RA, Wang X, Chen Z, Wang JH. Tumor immune microenvironment in head and neck cancers. Mol Carcinog. 2020;59(7):766–774. doi:10.1002/mc.23162
43. Tall AR, Yvan-Charvet L. Cholesterol, inflammation and innate immunity. Nat Rev Immunol. 2015;15(2):104–116. doi:10.1038/nri3793
44. Litsou E. Immune cells and their role in immunosuppressive tumor microenvironment of head and neck cancer. IntechOpen. 2025.
45. Mantovani A, Marchesi F, Malesci A, Laghi L, Allavena P. Tumour-associated macrophages as treatment targets in oncology. Nat Rev Clin Oncol. 2017;14(7):399–416. doi:10.1038/nrclinonc.2016.217
46. Don BR, Kaysen G. Serum albumin: relationship to inflammation and nutrition. Semin Dial. 2004;17(6):432–437. doi:10.1111/j.0894-0959.2004.17603.x
47. Zhang Y, Tang C, Yang M, et al. The predictive value of Naples prognostic score for patients with locally advanced non-small cell lung cancer undergoing surgery after neoadjuvant chemotherapy. Front Immunol. 2025;16:1578896. doi:10.3389/fimmu.2025.1578896
48. Chen W, Xu G, Yan X, et al. Naples prognostic score as a novel prognostic prediction tool for resectable locally advanced esophageal squamous cell carcinoma after neoadjuvant therapy. J Inflamm Res. 2025;18:4843–4856. doi:10.2147/JIR.S502058
49. Xie YM, Lu W, Cheng J, et al. Naples prognostic score is an independent prognostic factor in patients undergoing hepatectomy for hepatocellular carcinoma. J Hepatocell Carcinoma. 2023;10:1423–1433. doi:10.2147/JHC.S414789
50. Yang J, Lv L, Zhao F, Mei X, Zhou H, Yu F. The value of the preoperative Naples prognostic score in predicting prognosis in gallbladder cancer surgery patients. World J Surg Oncol. 2023;21(1):303. doi:10.1186/s12957-023-03198-0
51. Xu XL, Wu CC, Cheng H. Prognostic significance of preoperative Naples prognostic score for disease-free and overall survival in oral cavity squamous cell carcinoma post-surgery. BMC Cancer. 2025;25(1):757. doi:10.1186/s12885-025-14146-4
52. Ran J, Liu Y, Yi X, Zhang F. Modified Naples prognostic score for postoperative prognostic stratification in patients with oral squamous cell carcinoma. J Inflamm Res. 2025;18:11593–11610. doi:10.2147/JIR.S537870
53. Vu HL, Sikora AG, Fu S, Kao J. HPV-induced oropharyngeal cancer, immune response and response to therapy. Cancer Lett. 2010;288(2):149–155. doi:10.1016/j.canlet.2009.06.026
54. Mirghani H, Amen F, Tao Y, Deutsch E, Levy A. Increased radiosensitivity of HPV-positive head and neck cancers: molecular basis and therapeutic perspectives. Cancer Treat Rev. 2015;41(10):844–852. doi:10.1016/j.ctrv.2015.10.001
55. Chen AM. HPV-mediated radiosensitivity in oropharyngeal squamous cell carcinoma: molecular mechanisms and cellular pathways. Curr Oncol Rep. 2025;27(5):634–641. doi:10.1007/s11912-025-01666-2
56. Boscolo-Rizzo P, Tagliabue M, Polesel J, et al. HPV status and survival outcomes in patients 70 years and older after surgery for oropharyngeal carcinoma. JAMA Otolaryngol Head Neck Surg. 2025;151(8):795–805. doi:10.1001/jamaoto.2025.1722
57. Albergotti WG, Schwarzbach HL, Abberbock S, et al. Defining the prevalence and prognostic value of perineural invasion and angiolymphatic invasion in human papillomavirus-positive oropharyngeal carcinoma. JAMA Otolaryngol Head Neck Surg. 2017;143(12):1236–1243. doi:10.1001/jamaoto.2017.2019
58. Miles BA, Posner MR, Gupta V, et al. De-escalated adjuvant therapy after transoral robotic surgery for human papillomavirus-related oropharyngeal carcinoma: the sinai robotic surgery (SIRS) trial. Oncologist. 2021;26(6):504–513. doi:10.1002/onco.13742
59. Chua BQY, Chong VWS, Kadir HBA, et al. Histopathological prognostic factors of surgically treated HPV-associated oropharyngeal squamous cell carcinoma: a systematic review and meta-analysis. Ann Surg Oncol. 2025;32(2):1280–1300. doi:10.1245/s10434-024-16362-x
60. Skillington SA, Kallogjeri D, Lewis JS, Piccirillo JF. Prognostic importance of comorbidity and the association between comorbidity and p16 in oropharyngeal squamous cell carcinoma. JAMA Otolaryngol Head Neck Surg. 2016;142(6):568–575. doi:10.1001/jamaoto.2016.0347
61. Gronhoj C, Kronberg Jakobsen K, Kjaer E, Friborg J, von Buchwald C. Comorbidity in HPV+ and HPV- oropharyngeal cancer patients: a population-based, case-control study. Oral Oncol. 2019;96:1–6. doi:10.1016/j.oraloncology.2019.06.035
62. Vibert JJM, Siegenthaler F, Saner FAM, Mohr S, Mueller MD, Imboden S. Usefulness of geriatric parameters in preoperative evaluation of patients undergoing minimally invasive surgery for endometrial cancer: a retrospective cohort study. Ann Surg Oncol. 2025;32(8):5603–5615. doi:10.1245/s10434-025-17376-9
63. Shao J, Gao Z, Shen Q, et al. Prognostic value and association of the age-adjusted Charlson comorbidity index with sarcopenia within patients with gastric cancer after radical resection. J Gastrointest Surg. 2024;28(7):1089–1094. doi:10.1016/j.gassur.2024.04.027
64. Barz M, Bette S, Janssen I, et al. Age-adjusted Charlson comorbidity index in recurrent glioblastoma: a new prognostic factor? BMC Neurol. 2022;22(1):32. doi:10.1186/s12883-021-02532-x
65. Koseki Y, Hikage M, Fujiya K, et al. Utility of a modified age-adjusted Charlson comorbidity index in predicting cause-specific survival among patients with gastric cancer. Eur J Surg Oncol. 2021;47(8):2010–2015. doi:10.1016/j.ejso.2021.01.026
66. Kahl A, du Bois A, Harter P, et al. Prognostic value of the age-adjusted charlson comorbidity index (ACCI) on short- and long-term outcome in patients with advanced primary epithelial ovarian cancer. Ann Surg Oncol. 2017;24(12):3692–3699. doi:10.1245/s10434-017-6079-9
67. Bernier J, Cooper JS, Pajak TF, et al. Defining risk levels in locally advanced head and neck cancers: a comparative analysis of concurrent postoperative radiation plus chemotherapy trials of the EORTC (#22931) and RTOG (# 9501). Head Neck. 2005;27(10):843–850. doi:10.1002/hed.20279
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
A CRP-Albumin-Lymphocyte (CALLY) Index–Based Nomogram for Predicting Survival After Radical Surgery for Hypopharyngeal Squamous Cell Carcinoma
Meng X, Wang J, Shen W, Yang S, Zhao K, Liu X, Cheng K, Tian L, Cheng H, Xu X
Journal of Inflammation Research 2026, 19:599865
Published Date: 21 April 2026