Back to Journals » Infection and Drug Resistance » Volume 19
Development of a Prediction Model for Severe Pediatric Mycoplasma pneumoniae Pneumonia: A Single-Center Retrospective Study
Authors Zeng Z, Li G ![]() , Xu Y, Dong N, Zhu D, Yin R, Zhong H, Yuan L, Shen L, Ding G, Dong X
, Xu Y, Dong N, Zhu D, Yin R, Zhong H, Yuan L, Shen L, Ding G, Dong X
Received 20 January 2026
Accepted for publication 18 May 2026
Published 27 May 2026 Volume 2026:19 593932
DOI https://doi.org/10.2147/IDR.S593932
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Hazrat Bilal
Zeyu Zeng,1,2,* Guang Li,3,* Yanbing Xu,3 Na Dong,1 Danying Zhu,1,2 Rong Yin,1 Haiqin Zhong,1 Lang Yuan,1 Libing Shen,4 Guohui Ding,4 Xiaoyan Dong1,2
1Department of Pulmonology, Shanghai Children’s Hospital, School of Medicine, Shanghai Jiao Tong University, Shanghai, People’s Republic of China; 2Institute of Pediatric Infection, Immunity, and Critical Care Medicine, Shanghai Jiao Tong University School of Medicine, Shanghai, People’s Republic of China; 3Daozhi Precision Medicine Technology (Shanghai) Co., Ltd, Shanghai, People’s Republic of China; 4Institute for Digital Health, International Human Phenome Institutes (Shanghai), Shanghai, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Xiaoyan Dong, Department of Pulmonology, Shanghai Children’s Hospital, School of Medicine, Shanghai Jiao Tong University, 355 Luding Road, Shanghai, 200062, People’s Republic of China, Email [email protected]
Background: Mycoplasma pneumoniae pneumonia (MPP) is a common pediatric respiratory infection, with 10– 40% of cases progressing to severe MPP (SMPP). Macrolide-resistant Mycoplasma pneumoniae (MRMP) harboring the A2063/2064G mutation is closely associated with disease severity and treatment failure, posing a major clinical challenge. This study aimed to establish an early prediction model for SMPP and explore personalized treatment strategies for children with A2063/2064G-mutated infections.
Methods: A total of 2381 children diagnosed with MPP at Shanghai Children’s Hospital between November 2019 and December 2023 were retrospectively analyzed. Clinical characteristics, laboratory indices, and A2063/2064G mutation status were compared between SMPP and general MPP groups. A predictive model for SMPP was developed using multivariate logistic regression, and its performance was evaluated by receiver operating characteristic (ROC) curve analysis. Medication patterns and length of hospital stay in patients with A2063/2064G mutations were further assessed to formulate personalized treatment strategies.
Results: Of 2381 patients, 71.3% developed SMPP; 46.9% of all cases carried the A2063/2064G mutation, and the mutation rate was significantly higher in the SMPP group (54.7% vs. 27.5%, P < 0.001). The seven-indicator model (fever duration, lactate dehydrogenase (LDH), albumin (ALB), creatine kinase-MB (CK-MB), neutrophil percentage (Neu%), white blood cell (WBC) count and D-dimer) exhibited excellent performance (area under the curve (AUC) = 0.899, 95% confidence interval (CI) = [0.861, 0.937], sensitivity = 0.827, specificity = 0.861). In mutation-positive patients, those requiring tetracyclines (TCs)/fluoroquinolones (FQs) had higher SMPP rates than macrolide antibiotics (MACs)-responsive cases (89.6% vs. 78.0%, P < 0.001). Early TCs/FQs shortened hospital stay (7.30 ± 1.96 vs. 8.38 ± 2.20 days, P < 0.001). The model performed consistently across groups, and age-stratified analysis showed the highest TCs/FQs usage in patients with both mutation and model-predicted SMPP.
Conclusion: The prediction model effectively identifies SMPP and guides interventions when combined with mutation status. Early TCs/FQs may benefit children with A2063/2064G-mutated MP when predicted as SMPP.
Keywords: Mycoplasma pneumoniae pneumonia, clinical prediction model, A2063/2064G mutation, macrolide resistance, personalized treatment
Background
Mycoplasma pneumoniae pneumonia (MPP) is a significant respiratory infection among pediatric populations, accounting for 10–40% of community-acquired pneumonia (CAP) cases.1,2 Severe MPP (SMPP) is characterized by rapid clinical deterioration and high complication rates, posing a major challenge to pediatric clinical management.3,4 Current clinical evaluation of SMPP mainly depends on conventional clinical manifestations and laboratory indicators, which often only reflect advanced disease status and are insufficient for early risk warning.5,6 With the widespread application of macrolide antibiotics (MACs), the prevalence of macrolide-resistant Mycoplasma pneumoniae (MRMP) has increased globally,7,8 with resistance rates exceeding 90% in some Asian regions.9,10 The A2063/2064G gene mutation has been confirmed as the primary molecular mechanism of macrolide resistance and an independent risk factor for SMPP progression,11,12 while tetracyclines (TCs) and fluoroquinolones (FQs) are recommended as alternative therapeutic options for eligible children with resistant infection.13,14
Nevertheless, current prediction models and relevant literature still present several unresolved shortcomings.15,16 Existing models adopt heterogeneous variable selection frameworks and lack a unified standardized indicator system, leading to unstable predictive performance across different clinical settings.15 In addition, most models rely on sophisticated and non-routine biomarkers that are not universally accessible in general clinical practice, which limits their popularization and practical application value.16 Notably, few prediction models incorporate the A2063/2064G mutation into the risk stratification system, and the quantitative association between this mutation genotype, disease severity and treatment response remains insufficiently clarified.11,12 Moreover, standardized personalized treatment strategies that integrate resistance mutation profiles and individual clinical characteristics are still lacking.14
To address these unresolved problems in existing studies and prediction models, this study aims: (1) to construct a clinically applicable early prediction model for SMPP based on readily available routine clinical parameters; (2) to explore the clinical significance of the A2063/2064G mutation in disease progression and therapeutic outcomes; (3) to formulate individualized treatment strategies according to drug resistance profiles and clinical manifestations. The findings will provide evidence-based reference for early identification, risk stratification and precise management of pediatric SMPP.
Methods
Study Subjects
This study was conducted at Shanghai Children’s Hospital and included medical history data from hospitalized patients with MPP from November 2019 to December 2023. Data collected included basic demographic information and clinical characteristics of the children, such as age, gender, admission time, symptoms and signs, pulmonary imaging findings, length of hospital stay, and medication use. Laboratory examination results included routine blood tests, C-reactive protein (CRP), serum amyloid A (SAA), procalcitonin (PCT), erythrocyte sedimentation rate (ESR), serum ferritin (SF), interleukin (IL)-17, IL-1β, tumor necrosis factor (TNF)-α, lactate dehydrogenase (LDH), creatine kinase (CK), creatine kinase-MB (CK-MB), alanine aminotransferase (ALT), aspartate aminotransferase (AST), albumin (ALB), and D-dimer.
The inclusion criteria for pneumonia were as follows: 1) Presence of fever, cough, and wheezing; 2) Lung examination revealing crackles; 3) Imaging studies showing lung inflammation. MPP was diagnosed among children with pneumonia based on one or both of the following criteria: 1) A single serum Mycoplasma pneumoniae (MP) antibody titer of ≥ 1:160 (by particle agglutination, PA method) or a fourfold or greater increase in serum MP antibody titer during the course of the disease; 2) Positivity for MP-DNA or RNA.
Exclusion criteria included: 1) Patients with immunodeficiency or underlying diseases; 2) Incomplete clinical or laboratory data.
The inclusion criteria for SMPP were based on the severity of the disease, meeting the criteria for severe CAP, which included any of the following: 1) Persistent high fever for ≥ 5 days or fever for ≥ 7 days without a decline in peak temperature; 2) Hypoxemia; 3) Extrapulmonary complications; 4) Refusal to eat and signs of dehydration; 5) Imaging showing ≥ 2/3 lung involvement, multilobar infiltrates, pleural effusion, pneumothorax, atelectasis, lung necrosis, or lung abscess; 6) Poor general condition or altered mental status.
This study was approved by the Medical Ethics Review Committee of Shanghai Children’s Hospital (Ethical Approval Number: 2023R051-F01), and informed consent was obtained from the guardians of the patients.
MP Serological Detection
Venous blood samples (2–3 mL) were collected from all children. The samples were centrifuged at 270×g for 5 minutes to separate the serum. The MP antibody titer was then detected using the FUJIREBIO MP antibody detection kit (passive agglutination method) from Japan. Results were assessed visually. A MP antibody titer of ≥ 1:160 was considered serologically positive for MP infection.
MP DNA and Drug Resistance Site Detection
Real-time quantitative polymerase chain reaction (RT-PCR) was employed to detect MP DNA in throat swab or bronchoalveolar lavage fluid samples from the children. The reagents used were from the MP nucleic acid and drug resistance mutation site detection kit (Jiangsu Mole Bio-Tech Co., Ltd)., and the detection instrument was the ABI 7500 real-time quantitative PCR system (ABI, USA). Nucleic acid extraction and amplification were performed strictly according to the manufacturer’s instructions. The DNA detection was quantitative, with a reference value of < 500 copies/mL. A result of ≥ 500 copies/mL was considered positive for nucleic acid testing. If the result was below the lower limit of detection, it was reported as < 500 copies/mL. The presence of A2063G or A2064G mutations was used as the criterion for drug resistance.
Statistical Analysis
Statistical analyses were performed using SPSS version 27.0 (IBM Corporation, Armonk, NY, USA) and R version 4.1.3 (R Foundation for Statistical Computing, Vienna, Austria). A two-sided P-value of < 0.05 was considered to indicate statistical significance. Normally distributed continuous variables were presented as mean ± standard deviation (SD) and compared using Student’s t-test. Categorical variables were described as percentages or frequencies and analyzed using the chi-square test. Multivariate analysis was conducted using a stepwise logistic regression model. Receiver operating characteristic (ROC) curve analysis was employed to predict SMPP and to assess the sensitivity and specificity of the model. Post-hoc statistical power analysis was performed to verify that the current sample size provided adequate statistical power for detecting meaningful differences and stable regression model construction, ensuring the reliability and validity of the statistical results.
Results
Patient Baseline Characteristics Distribution
During the study period, 3635 patients (38.22%, 3,635/9,511) were diagnosed with MPP. After applying the exclusion criteria, 2381 MPP patients were ultimately included. Of these, 1697 were classified as SMPP patients, and 684 as general Mycoplasma pneumoniae pneumonia (GMPP) patients, based on disease severity. Additionally, 1117 patients had MP strains with the A2063/2064G mutation, while 1264 patients had strains with normal A2063/2064G loci, as determined by the presence of drug resistance mutations. A flowchart of the study design is provided in Figure 1. Demographic, clinical, and laboratory data for all patients are summarized in Table 1.
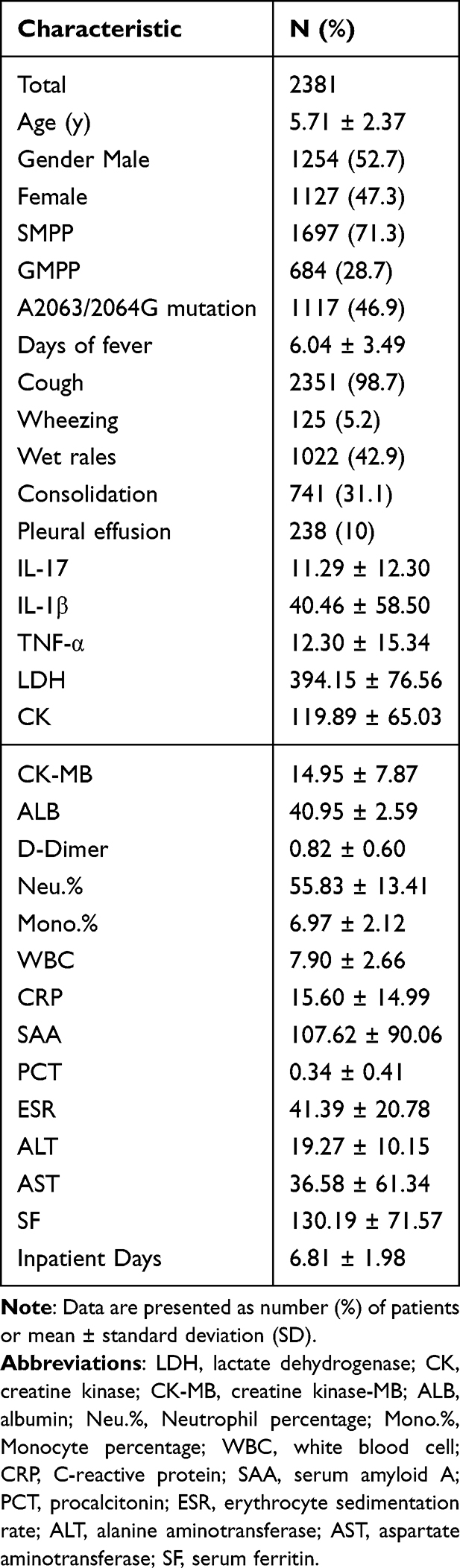 |
Table 1 General Characteristics of the Patients |
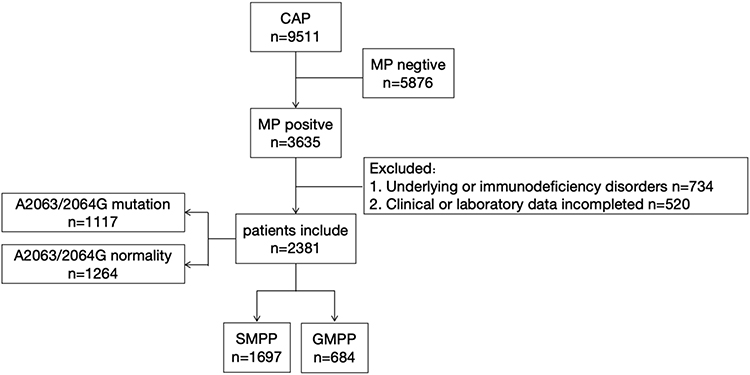 |
Figure 1 Flow diagram illustrating the design of the present study. |
Comparison of Characteristics Between SMPP and GMPP
Among the 2381 MPP patients, 1697 were classified into the SMPP group and 684 into the GMPP group. A detailed comparison of their characteristics is summarized in Table 2. No significant difference was observed in gender distribution between the two groups. However, a significant difference was noted in age (P < 0.001). The prevalence of the A2063/2064G mutation was significantly higher in the SMPP group (54.7%, 929/1697) than in the GMPP group (27.5%, 188/684) (P < 0.001).
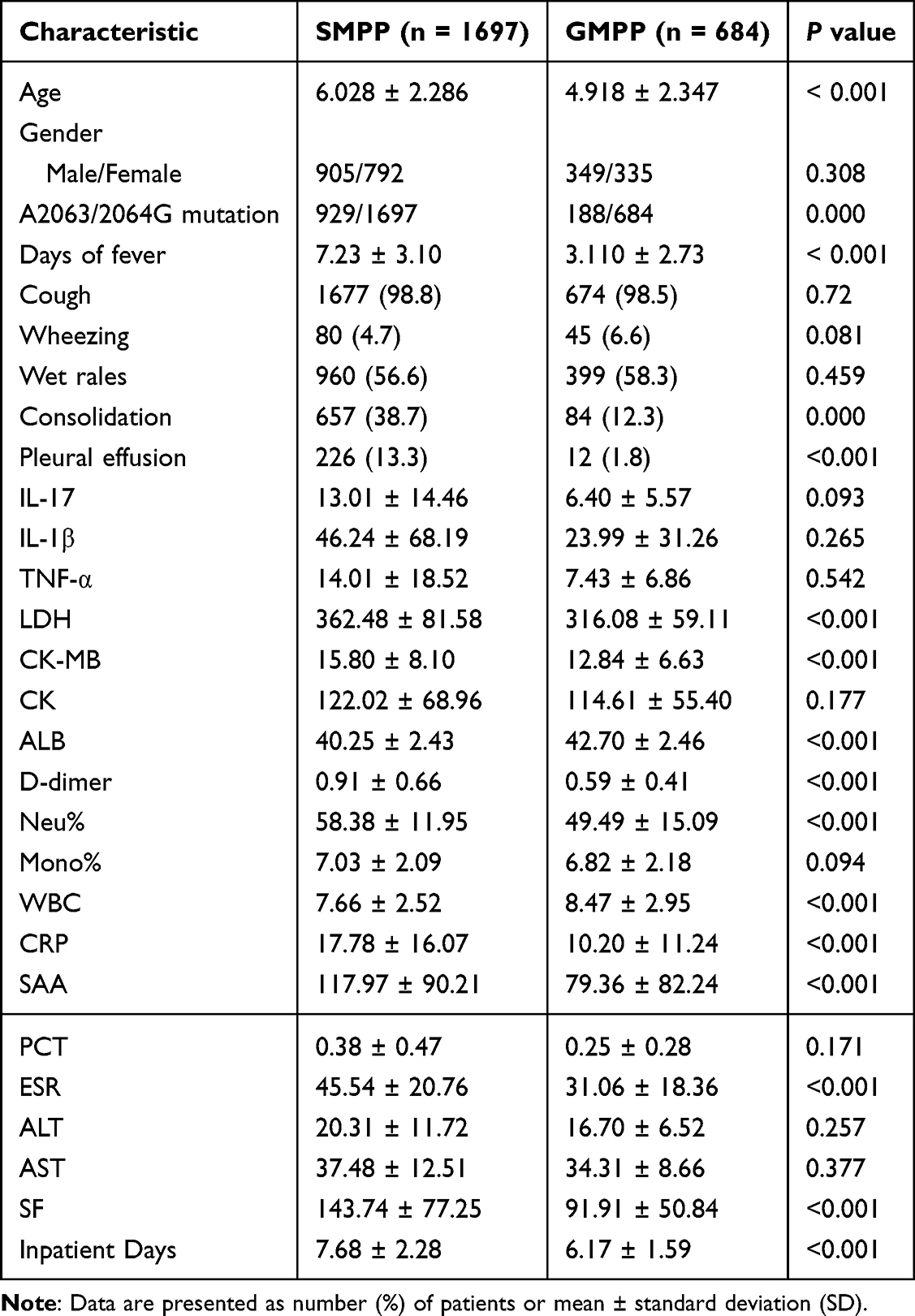 |
Table 2 Characteristics of SMPP and GMPP |
In terms of clinical manifestations, the SMPP group exhibited a significantly longer duration of fever (P < 0.001), higher incidences of lung consolidation (38.7% vs. 12.3%, P < 0.001) and pleural effusion (13.3% vs. 1.8%, P < 0.001). In contrast, no significant differences were observed in the incidence of cough, wheezing, or lung rales between the two groups.
Laboratory test results revealed that levels of LDH, CK-MB, ALB, D-dimer, Neu%, WBC count, CRP, SAA, ESR, and SF were significantly higher in the SMPP group than in the GMPP group (all P < 0.001). However, no significant differences were observed in IL-17, IL-1β, TNF-α, CK, Mono%, ALT, AST, or PCT levels between the two groups.
Regarding prognosis, the SMPP group had a significantly longer hospital stay (7.679 ± 2.282 days) compared to the GMPP group (6.171 ± 1.592 days, P < 0.001).
Selection of Predictive Factors and Construction of the SMPP Prediction Model
Predictive factors for the model were selected based on clinical significance, variables previously reported to be associated with SMPP, and those exhibiting statistical significance in Table 2. Multivariate logistic regression analysis was employed to determine the association of these variables with SMPP. Considering clinical prevalence and feasibility, seven indicators were ultimately identified as predictive factors for SMPP: Days of fever (X1) (OR = 6.554, 95% CI = [5.113, 8.401], P < 0.001), LDH (X2) (OR = 1.513, 95% CI = [1.166, 1.963], P = 0.002), ALB (X3) (OR = 0.345, 95% CI = [0.221, 0.537], P < 0.001), CK-MB (X4) (OR = 2.037, 95% CI = [1.323, 3.137], P = 0.001), Neu% (X5) (OR = 1.516, 95% CI = [1.270, 1.811], P < 0.001), WBC (X6) (OR = 0.680, 95% CI = [0.529, 0.874], P = 0.003), and D-dimer (X7) (OR = 1.242, 95% CI = [0.956, 1.613], P = 0.105) (Table 3).
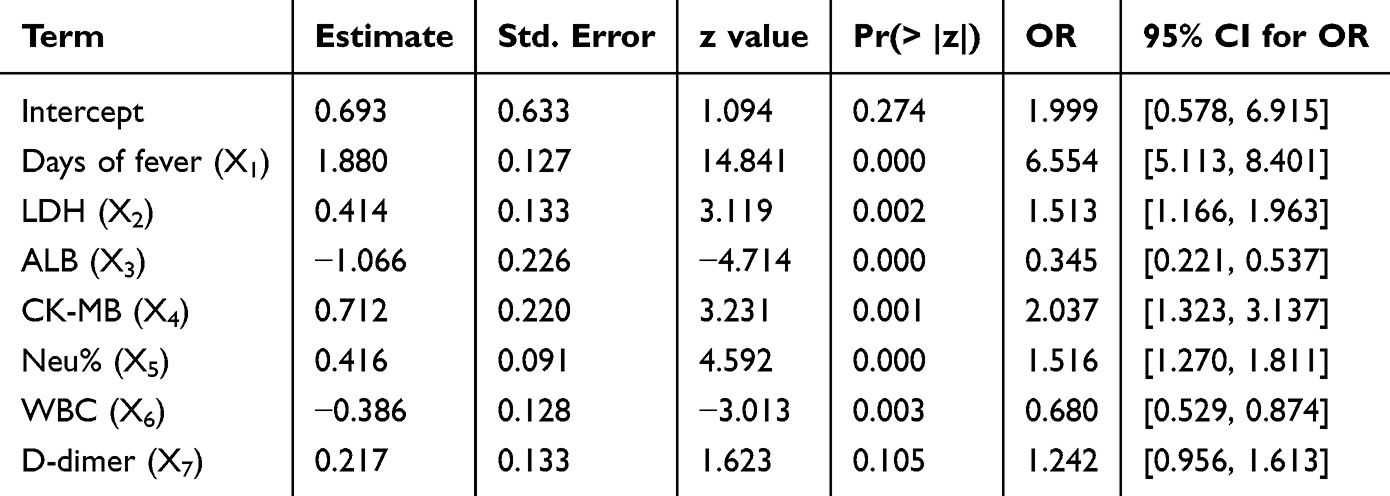 |
Table 3 Multivariate Logistic Regression Analysis Predictors of SMPP |
Based on these factors, a logistic regression-based prediction model for SMPP was developed: ln(p/(1-p)) = 0.693 + 1.880×1 + 0.414×2 − 1.066×3 + 0.712×4 + 0.416×5 − 0.386×6 + 0.217×7. The predictive performance of the individual risk factors and the model was evaluated using ROC curve analysis, which demonstrated high diagnostic accuracy with an area under the curve (AUC) of 0.899 (95% CI = [0.861, 0.937]) (Table 4 and Figure 2). The cutoff threshold for the model was set at 0.628, which yielded a sensitivity of 0.827, specificity of 0.861, accuracy of 0.838, and precision of 0.932 in the validation set.
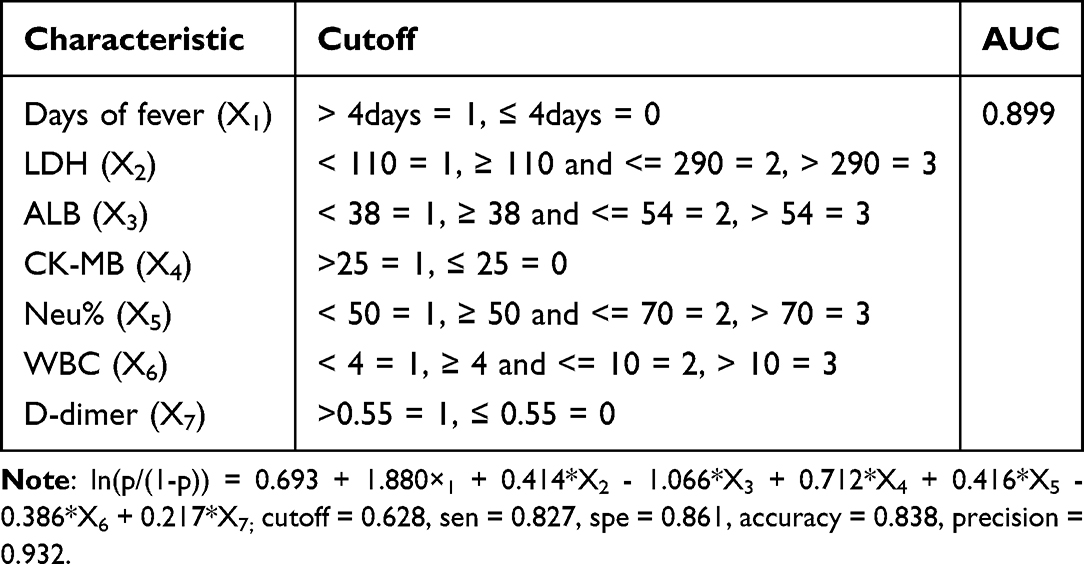 |
Table 4 Development of an Early Warning Model for SMPP |
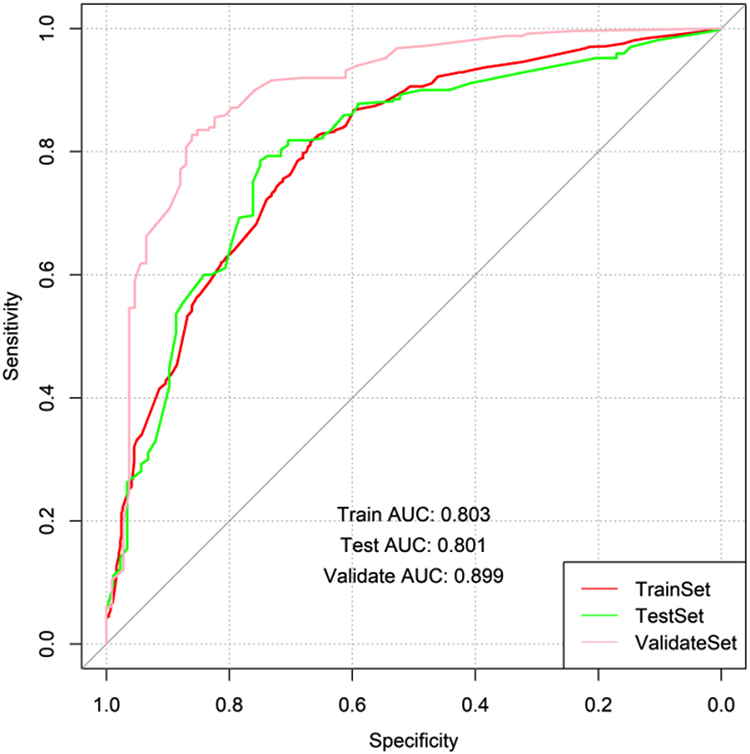 |
Figure 2 Receiver Operating Characteristic Curve Analysis of the SMPP Prediction Model. |
Characteristics of MPP Patients with MP A2063/2064G Mutation
Among the 2381 MPP patients, 1117 had the A2063/2064G mutation in the infecting MP, while the remaining 1264 did not have this mutation. A comparison of the general characteristics between these two groups is summarized in Table 5. No significant difference in gender distribution was observed between the groups, but a significant difference in age was noted (P < 0.001). The proportion of patients with SMPP was significantly higher in the A2063/2064G mutation group (83.2%, 929/1117) than in the non-mutation group (60.8%, 768/1,264, P < 0.001).
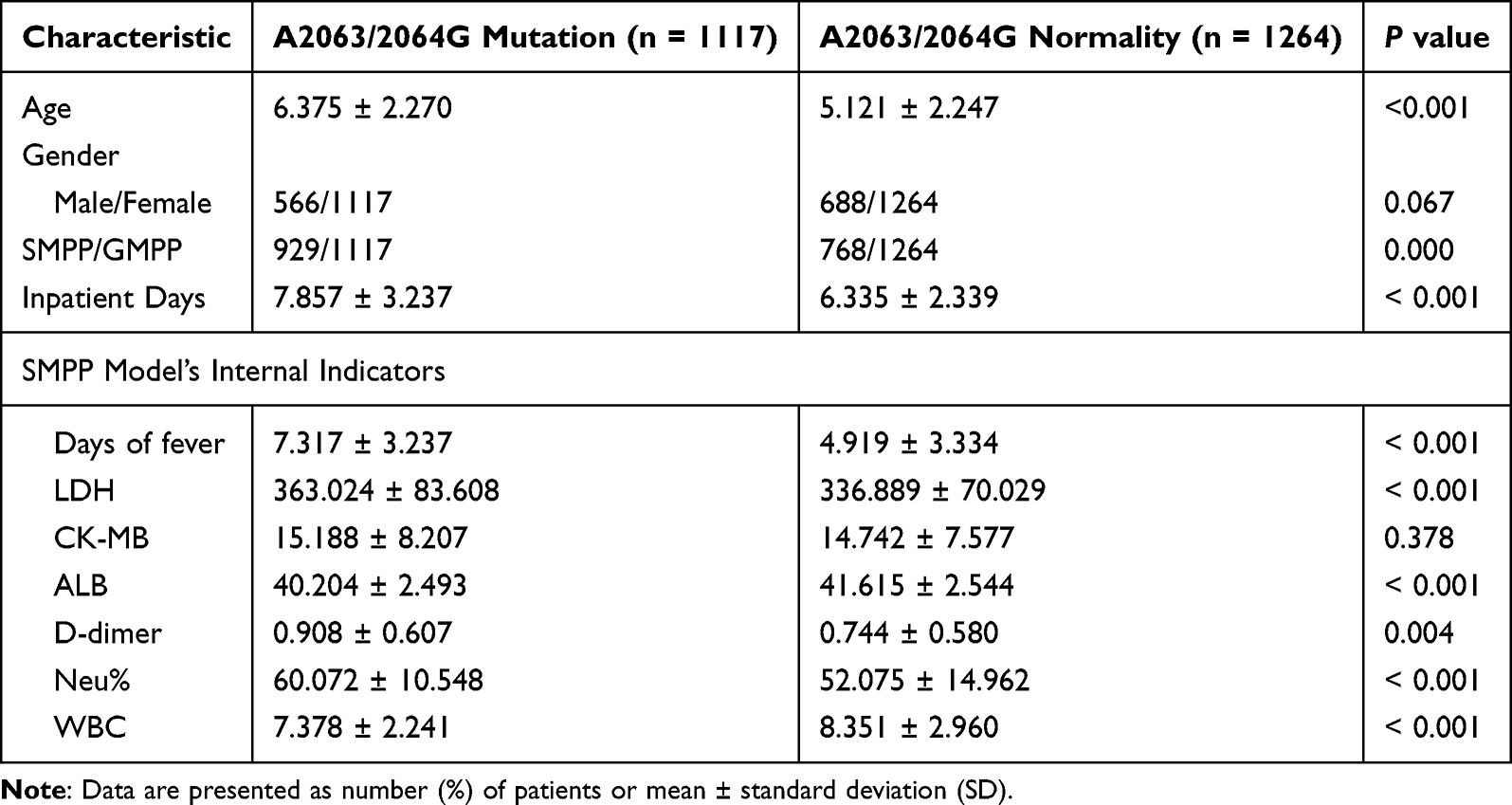 |
Table 5 Comparison of Characteristics Between A2063/2064G Mutation and Non-Mutation Groups |
Regarding the seven indicators within the SMPP prediction model, the A2063/2064G mutation group exhibited a significantly longer duration of fever (P < 0.001) and significantly higher levels of LDH (P < 0.001), ALB (P < 0.001), D-dimer (P = 0.004), Neu% (P < 0.001), and WBC (P < 0.001) compared to the non-mutation group. However, no significant difference in CK-MB levels was observed between the two groups. Additionally, the length of hospital stay was significantly longer for the A2063/2064G mutation group (7.857 ± 3.237 days) compared to the non-mutation group (6.335 ± 2.339 days, P < 0.001).
Clinical Medication Usage and Hospitalization Duration Among Patients Infected with the A2063/2064G Mutation of MP
Among the 1117 patients infected with the A2063/2064G mutation of MP, 619 responded well to MACs and did not receive TCs or FQs (indicating no clinical consideration of resistance, 619/1117), of whom 483 (78%, 483/619) were diagnosed with SMPP. In contrast, 498 patients who had an inadequate or no response to MACs were treated with TCs or FQs (suggesting clinical consideration of resistance, 498/1117), and 446 of these (90%, 446/498) were diagnosed with SMPP. The proportion of SMPP was significantly higher in the latter group than in the former group (χ2 = 26.206, P < 0.001) (Table 6).
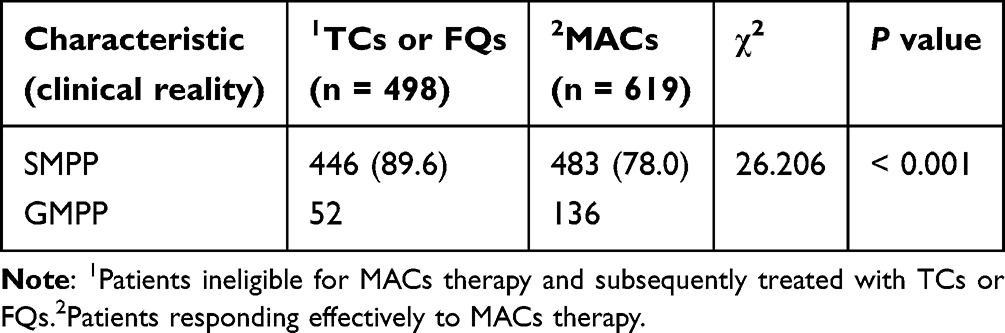 |
Table 6 SMPP Rates in A2063/2064G Mutation Patients Across Medication Treatments |
Regarding hospitalization duration, patients who responded well to MACs and did not receive TCs or FQs (group M) had an average hospital stay of 6.50 ± 1.34 days. In contrast, patients who were switched to TCs or FQs after failing MACs treatment (group MTF) had a significantly longer average hospital stay (8.38 ± 2.20 days) compared to those who received TCs or FQs as first-line treatment upon admission (group TF, 7.30 ± 1.96 days, P < 0.001) (Figure 3).
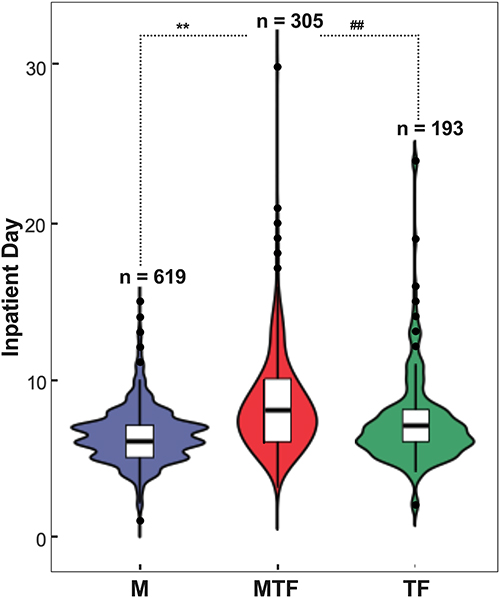 |
Figure 3 Comparison of Hospitalization Duration Among Patients with A2063/2064G Mutated MP Across Different Treatments. M group (n = 619): Patients who responded well to MACs without receiving TCs or FQs treatment. MTF group (n = 305): Patients who were switched to TCs or FQs following failure of MACs treatment. TF group (n = 193): Patients who received TCs or FQs as first-line treatment upon admission. Data are presented as mean ± SD, **P<0.001 versus M group; ##P<0.001 versus TF group. |
Individualized Treatment Clues for Patients with the A2063/2064G Mutation via the SMPP Prediction Model
We validated the actual medication usage in 1117 patients with the A2063/2064G mutation in MP using the established SMPP prediction model. Among the 619 patients who responded well to MACs without receiving TCs or FQs, 468 (76%, 468/619) were predicted to have SMPP by the model. In contrast, among the 498 patients who had an inadequate or no response to MACs and received TCs or FQs, 430 (86%, 430/498) were predicted to have SMPP, with a significantly higher proportion than the former group (χ2 = 20.194, P < 0.001) (Table 7). Moreover, the predicted results were essentially consistent with the actual SMPP proportions in both scenarios.
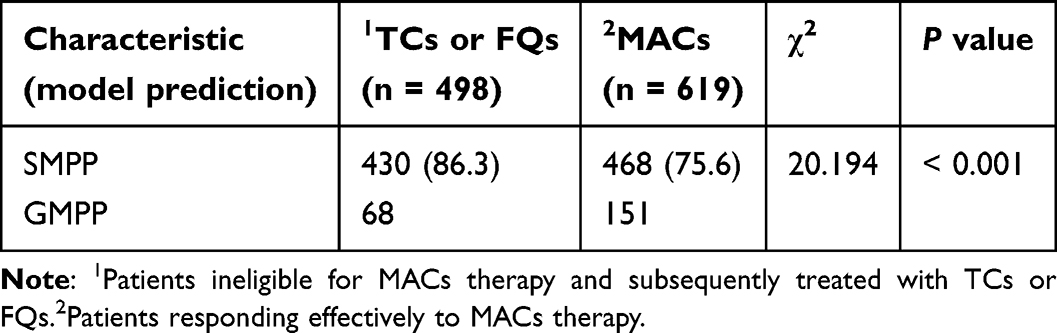 |
Table 7 Model Prediction Results in A2063/2064G Mutation Patients Across Medication Treatments |
Additionally, age was identified as a significant factor influencing the use of TCs or FQs. Therefore, we further stratified the study subjects into four groups (MPP, SMPP, MP A2063/2064G mutation, MP A2063/2064G mutation + model-predicted SMPP) and examined the proportion of TCs or FQs use among patients of different ages in each group. As shown in Figure 4, the proportion of TCs or FQs use increased with age in all groups. The proportion was highest in the “MP A2063/2064G mutation + model-predicted SMPP” group across all age groups. When age exceeded 10 years, the proportion of TCs or FQs use in the “MP A2063/2064G mutation + model-predicted SMPP” group was similar to that in the “MP A2063/2064G mutation” group.
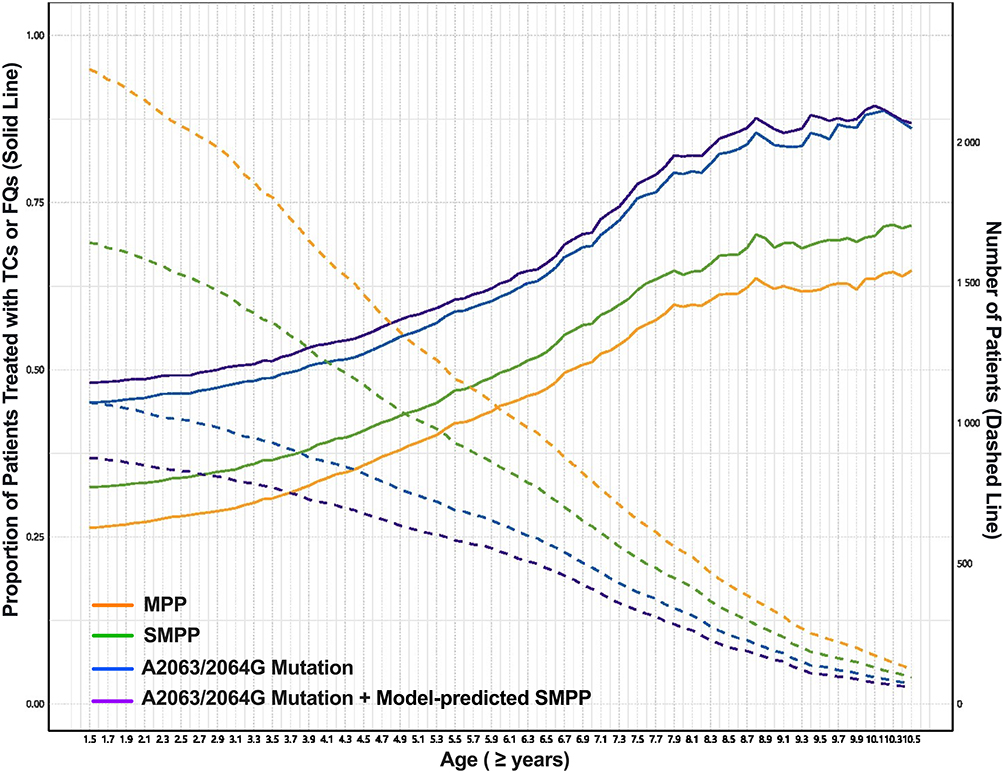 |
Figure 4 Proportion of Patients Treated with TCs or FQs Across Different Age Groups. Patients were categorized into four groups: MPP, SMPP, A2063/2064G mutation, and A2063/2064G mutation + model-predicted SMPP. The solid line represents the proportion of patients in each age group receiving TCs or FQs treatment, while the dashed line indicates the number of patients in each age group. |
Overall, the present study observed the association between MP A2063/2064G mutation and SMPP progression, and established a predictive model based on routine clinical indicators. Additionally, we explored the correlation between drug resistance mutation, clinical treatment response and hospitalization duration, and provided age-stratified medication clues for mutation-positive pediatric patients. These observations, which integrate drug resistance analysis with SMPP prediction and focus on clinically accessible indicators, differ from the focus of most prior studies that primarily examined either SMPP prediction or MP drug resistance independently, and we hope these findings might complement existing research in this field.
Discussion
MP is a significant pathogen causing CAP in both school-aged and preschool-aged children. Despite the availability of diagnostic and therapeutic interventions, some pediatric patients still progress to severe or critical stages, highlighting the importance of early identification of SMPP as a critical clinical challenge—this directly addresses our core research question of improving SMPP early detection to optimize clinical management. Additionally, the increasing incidence of MRMP infections in the post-COVID-19 era has further complicated the selection of appropriate antibiotics for pediatric patients, which aligns with our second core objective: integrating MP drug resistance data with clinical decision-making to guide antibiotic use. At our institution, the proportion of hospitalized MPP cases among CAP patients was 38.22%, consistent with global epidemiological data,1 providing a representative cohort for our study. Among these hospitalized cases, the proportion of SMPP reached 71.3% under stringent hospitalization criteria, underscoring the clinical urgency of our research. Our study indicated that SMPP was more prevalent among school-aged children compared to preschool-aged children, likely due to more robust immune responses in the older age group17—this finding advances current understanding by clarifying age-related differences in SMPP susceptibility, which was not fully elaborated in prior studies. Compared to GMPP, SMPP cases exhibited higher rates of lung consolidation and pleural effusion on imaging, prolonged durations of fever and hospitalization, and elevated levels of LDH, CK-MB, D-dimer, neutrophil percentage (Neu%), CRP, SAA, ESR, and SF, alongside decreased levels of WBC and ALB. These results directly address our core research question by identifying key clinical and laboratory markers that distinguish SMPP from GMPP, laying the foundation for our predictive model. In response to these observations, we assessed the significant differences between SMPP and GMPP by examining several factors: (1) the influence of parameter combinations on the performance of predictive models, (2) the feasibility and applicability of the model across various clinical settings, and (3) concerns from families regarding radiation exposure from imaging studies. Consequently, we developed a predictive model for SMPP based on seven optimal parameters (duration of fever, LDH, CK-MB, D-dimer, Neu%, WBC, and ALB) and employed it to guide antibiotic selection for pediatric patients across different age groups infected with A2063/2064G mutation strains of MP, thereby bridging the gap between SMPP prediction and clinical antibiotic decision-making.
An extended duration of fever generally indicates ongoing inflammatory responses and reduced effectiveness of antibiotic treatment. Studies have shown that fever duration is significantly longer in patients with MPP than in those with non-MPP,18 with most children presenting with febrile symptoms.19 Additionally, prolonged fever duration is associated with an increased risk of complications and serves as a critical risk factor in evaluating MPP severity.20 Building on previous research findings, our study further identified that fever duration carries a very high weight in constructing the SMPP early prediction model, which indicates that fever duration is a key factor in the SMPP prediction model.
The pathogenesis of SMPP is characterized by the interplay between MP virulence factors and the host’s immune response. LDH, a critical enzyme in cellular metabolism, is released into the bloodstream due to tissue damage, and its concentration serves as an indicator of both the inflammatory response and the degree of tissue injury.21 Elevated LDH levels have been strongly correlated with the manifestation of plastic bronchitis and pleural effusion in MPP.22,23 Consequently, LDH is a valuable biomarker for evaluating MPP severity and informing clinical decisions regarding glucocorticoid therapy.23–25 Building on previous evidence, our study verified LDH as a critical predictor for SMPP, supporting our aim of identifying readily available markers for early SMPP screening. Elevated LDH in the SMPP group further validated its predictive value, and inclusion of LDH in our multi‑indicator model achieved better diagnostic performance than single biomarkers in earlier studies.
D-dimer, a specific degradation product of fibrinolysis, increases markedly when the coagulation cascade is activated, leading to fibrin formation and concurrent activation of the fibrinolytic system. Elevated D-dimer levels are commonly observed in MPP. As MPP progresses, immune cells release inflammatory mediators that exacerbate vascular endothelial damage and activate the coagulation system, resulting in a significant rise in D-dimer levels.26 Research indicates that D-dimer concentrations are substantially higher in children with SMPP compared to those with GMPP.27 Furthermore, patients with elevated D-dimer levels tend to exhibit more SMPP symptoms, a higher incidence of extrapulmonary complications, and a more pronounced inflammatory response.28 This suggests that a hypercoagulable state may intensify the inflammatory response in MPP. Our study incorporated D-dimer into a multi-parameter predictive model to improve the specificity of SMPP detection, aiming to facilitate early identification of severe cases. A close correlation between D-dimer level and SMPP development was validated, supporting D-dimer as a reliable severity marker that may contribute to a more comprehensive predictive model when combined with other indicators.
Studies have shown that MP triggers the production and activation of neutrophils, which is a critical mechanism in its pathogenesis.29 An animal study revealed a correlation between elevated neutrophil levels and SMPP, suggesting that neutrophil inhibition can ameliorate the progression of MPP.30 Clinical investigations have also shown that the Neu% is significantly higher in SMPP patients compared to those with GMPP.27 Conversely, MP has been found to suppress lymphocyte expression and diminish their activity through mechanisms such as immune adhesion and the detrimental effects of metabolic byproducts, ultimately precipitating rapid lymphocyte apoptosis.31 Consequently, MP infections in peripheral blood are characterized by increased neutrophil counts and decreased lymphocyte levels.32 Furthermore, leukopenia is a characteristic feature of severe pneumonia. As MPP progresses, the intensified immune response leads to increased consumption of leukocytes. In some cases, this may be accompanied by bone marrow suppression, resulting in decreased leukocyte levels. Going beyond these known findings, our study advances the field by demonstrating that the combined assessment of peripheral blood leukocyte count (WBC count) and Neu% holds significant predictive value for SMPP—this novel combination improves predictive accuracy compared to single parameters used in prior research and directly contributes to our core objective of developing a robust SMPP prediction model.
In this study, albumin and CK-MB levels were incorporated as predictive variables within the model. Albumin serves as an indicator of the body’s nutritional status and is inhibited in synthesis by a robust inflammatory response. Notably, albumin levels were significantly lower in SMPP patients compared to those with GMPP,33,34 and reduced albumin levels were correlated with moderate to large pleural effusions in MPP.35 Conversely, CK-MB, a cardiac-specific enzymatic marker, is seldom expressed in non-cardiac tissues. Cardiac involvement is the most prevalent extrapulmonary complication of MPP, and elevated CK-MB levels in MPP patients are associated with elevated D-dimer levels, which may indicate concurrent myocarditis.27 The myocardial damage and increased CK-MB levels resulting from MP infection are attributed to the synergistic effects of inflammatory mediators and autoimmune responses. Prior research has identified CK-MB as a significant predictor of SMPP,15 corroborating our findings. Our study innovatively combined albumin and CK‑MB within one predictive framework. Building on earlier work that largely evaluated these biomarkers separately, this combined panel helps strengthen clinical practicability and offers a new reference for the early recognition of SMPP.
Consequently, this study used seven indicators—fever duration, LDH, D-dimer, Neu%, WBC count, albumin, and CK-MB—as internal parameters to develop the SMPP early warning model. The model achieved an AUC of 0.899, demonstrating high sensitivity and specificity. By relying on routine clinical parameters, the model is highly accessible and cost-effective, making it well-suited for implementation in primary healthcare settings.
In recent years, the increasing prevalence of MRMP infections has been accompanied by a steady rise in the proportion of SMPP cases.36 Our study revealed that the proportion of severe cases was significantly higher among patients infected with MP strains harboring resistance site mutations compared to those infected with non-mutated MP strains. Moreover, patients infected with resistance site-mutated MP exhibited characteristics typical of SMPP, such as prolonged hospitalization and significant alterations in the model’s internal parameter indicators. These findings establish a direct linkage between MP A2063/2064G mutations and SMPP progression, indicating that resistant-site mutated MP markedly facilitates SMPP onset and deterioration, and supporting our core aim of incorporating resistance profiles into clinical decision-making.
The primary mechanism of macrolide resistance in MP is mutations in the V domain of 23S rRNA, with A2063G being the most common mutation, followed by A2064G. These mutations are associated with high-level resistance to 14-membered macrolides.37,38 Clinically, resistance is determined by detecting resistance site mutations, but the current status of resistance testing is also influenced by factors such as the self-limiting nature of the disease. Therefore, in vitro resistance does not necessarily equate to clinical drug ineffectiveness.20 Our study showed that among 1117 patients infected with MP harboring A2063/2064G mutations, 619 (55.4%) responded effectively to macrolides, of whom 483 (78.1%) were classified as SMPP. In contrast, 498 (44.6%) were unresponsive to macrolides and were treated with TCs or FQs, among whom 446 (89.6%) were classified as SMPP. The severe case rate was significantly higher in the latter group, suggesting that macrolide ineffectiveness in patients infected with resistance site-mutated MP may indicate the development of SMPP. Furthermore, when comparing hospitalization durations under different treatment regimens for patients infected with A2063/2064G-mutated MP, our study found that patients who received TCs or FQs immediately upon admission had significantly shorter hospitalization durations than those initially treated with macrolides, which were ineffective, and later switched to TCs or FQs. This result provides practical guidance for early antibiotic selection, bridging the gap between in vitro resistance data and clinical decision-making, and supporting individualized treatment for MP mutant-positive patients.
However, the use of TCs or FQs is subject to age-related restrictions. TCs may cause permanent dental enamel hypoplasia in children under 8 years of age,39 while FQs may lead to skeletal growth inhibition and other side effects in children under 18 years of age.40 Therefore, their use should be guided by clinical considerations and under the supervision of a physician. This consideration is integral to our central research objective, gently highlighting the need for individualized antibiotic administration.
Based on the strong association between A2063/2064G-mutated MP and SMPP, as well as the unique considerations in drug therapy for children infected with A2063/2064G-mutated MP, we integrated resistance site data with the SMPP prediction model to provide stronger evidence for the use of TCs or FQs in these cases. First, we internally validated the model using 619 samples where MACs were effective and 498 samples where MACs were ineffective. The predicted proportions of severe cases were 76% (468/619) and 86% (430/498), respectively, which were consistent with the actual proportions of severe cases. Second, we plotted curves showing the proportion of patients receiving TCs or FQs under four different conditions across various age groups: MPP, SMPP, A2063/2064G-mutated MP infection, and A2063/2064G-mutated MP infection + model-predicted SMPP. The results indicated that patients in the “A2063/2064G-mutated MP infection + model-predicted SMPP” group had the highest proportion of TC or FQ use across all age groups. This finding suggests that when a child is infected with A2063/2064G-mutated MP and the model predicts SMPP, there is a greater tendency to use TCs or FQs for treatment. Clinically, it can be recommended that such children receive TCs or FQs as early as possible to prevent disease progression. On the other hand, when the age exceeds 10 years, the curves for the “A2063/2064G-mutated MP infection” group and the “A2063/2064G-mutated MP infection + model-predicted SMPP” group nearly overlap. This suggests that for children over 10 years old infected with A2063/2064G-mutated MP, early use of TCs or FQs can be directly recommended. These results offer age-stratified, evidence-based antibiotic recommendations for children with MP mutations, filling an unmet clinical demand and shedding new insight into the rational optimization of therapeutic regimens.
In recent decades, global antimicrobial resistance (AMR) has presented a continuously escalating public health crisis, posing an enormous threat to human health and being recognized as one of the most severe global challenges comparable to climate change. The widespread overuse and misuse of antibiotics have accelerated the emergence and spread of multidrug-resistant (MDR) bacterial pathogens, severely limiting conventional therapeutic options and increasing the risk of treatment failure, severe complications and mortality. Therefore, it is urgent to develop innovative alternative strategies to curb the progression of AMR and replenish the antibacterial therapeutic arsenal. Promising emerging approaches include but are not limited to the following three directions. First, bacteriophage-based therapeutics serve as a precise alternative strategy to combat MDR bacterial strains, exhibiting high host specificity and low propensity to induce cross-resistance.41 Second, targeting bacterial ultra-structures and key functional components such as bacterial metallophores can effectively weaken bacterial virulence and provide novel targets for new antibiotic development.42 Third, the Trojan Horse technique enables targeted delivery of antibiotics into bacterial interior compartments, effectively bypassing intrinsic and acquired drug resistance mechanisms of pathogens.43 These novel strategies are expected to complement traditional antibiotics and open new avenues for managing drug-resistant MP and other MDR respiratory pathogens in the future.
Limitation
This study has several limitations. First, it was conducted as a single-center retrospective observational analysis, which may introduce selection bias and limit the generalizability of the established prediction model to other regional populations and medical institutions. Second, although we constructed and internally verified the early warning model, external multicenter prospective validation is still required to further confirm its stability and clinical applicability. Third, this study mainly focused on short-term clinical outcomes and laboratory indicators; long-term follow-up data of children with MP infection were not included, which cannot reflect the long-term prognosis and sequelae of the disease. Therefore, further large-sample, multicenter, prospective studies are warranted to optimize and externally validate the model in the future.
Conclusion
This study confirms that combining A2063/2064G mutation profiling with multidimensional clinical prediction modeling offers important clinical implications for improving risk stratification and optimizing treatment algorithms in pediatric MPP. Incorporating resistance genotype into clinical evaluation overcomes the limitation of conventional empirical management and facilitates early identification of high-risk individuals. Notably, the established model relies on routine clinical and laboratory indicators, which makes it simple, cost-effective, and highly suitable for popularization and application in primary grassroots medical institutions. The proposed age-stratified antibiotic strategy, tailored to the presence or absence of macrolide-resistant mutations, represents a valuable refinement toward personalized and precise clinical care, which can serve as a practical reference for routine clinical practice and future related research.
Abbreviations
ALB, albumin; ALT, alanine aminotransferase; AST, aspartate aminotransferase; AUC, Area under the curve; CAP, community-acquired pneumonia; CK, creatine kinase; CK-MB, creatine kinase-MB; CRP, C-reactive protein; ESR, erythrocyte sedimentation rate; FQs, fluoroquinolones; GMPP, general Mycoplasma pneumoniae pneumonia; IL, interleukin; LDH, lactate dehydrogenase; MACs, macrolide antibiotics; MP, Mycoplasma pneumoniae; MPP, Mycoplasma pneumoniae pneumonia; MRMP, macrolide-resistant Mycoplasma pneumoniae; Neu%, Neutrophil percentage; PCT, procalcitonin; ROC, Receiver operating characteristic; RT-PCR:Real-time quantitative polymerase chain reaction; SAA, serum amyloid A; SD, standard deviation; SF, serum ferritin; SMPP, Severe Mycoplasma pneumoniae pneumonia; TCs, tetracyclines; TNF, tumor necrosis factor; WBC, white blood cell.
Data Sharing Statement
The data supporting this article cannot be made publicly available due to privacy concerns of the individuals who participated in the study. However, the dataset will be shared upon reasonable request to the corresponding author.
Ethics Approval and Consent to Participate
This study was approved by the Medical Ethics Review Committee of Shanghai Children’s Hospital (Ethical Approval Number: 2023R051-F01) and was conducted in accordance with the Declaration of Helsinki. Informed consent was obtained from the guardians of the patients.
Acknowledgments
We extend our sincere appreciation to the collaborative efforts of all investigators and staff members involved in this research. Their dedication and hard work were instrumental in the success of this study. Special thanks go to the participants for their invaluable contributions and willingness to take part in this research endeavor. This paper has been uploaded to the following servers as a preprint:
https://www.researchsquare.com/article/rs-6546335/v1 and,
https://sciety.org/articles/activity/10.21203/rs.3.rs-6546335/v1 and,
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was sponsored by the Shanghai Municipal Health Commission Project (No. 202340070), and Shanghai Children’s Hospital National Natural Science Foundation Cultivation Project (2023YGZQ03).
Disclosure
The authors declare no competing interests in this work.
References
1. Oumei H, Xuefeng W, Jianping L, et al. Etiology of community-acquired pneumonia in 1500 hospitalized children. J Med Virol. 2018;90(3):421–16. doi:10.1002/jmv.24963
2. Gao LW, Yin J, Hu YH, et al. The epidemiology of paediatric Mycoplasma pneumoniae pneumonia in North China: 2006 to 2016. Epidemiol Infect. 2019;147:e192. doi:10.1017/S0950268819000839
3. Zheng B, Zhao J, Cao L. The clinical characteristics and risk factors for necrotizing pneumonia caused by Mycoplasma pneumoniae in children. BMC Infect Dis. 2020;20(1):391. doi:10.1186/s12879-020-05110-7
4. Wang Z, Peng Y, Yang S, et al. Risk factors for complications of Mycoplasma pneumoniae pneumonia in hospitalized children in China: a systematic review and meta-analysis. BMC Pediatr. 2024;24(1):810. doi:10.1186/s12887-024-05279-9
5. Zhao X, Lv J, Wu M, Wu Q. Clinical characteristics and risk factors for Mycoplasma pneumoniae pneumonia in children. Front Pediatr. 2024;12:1438631. doi:10.3389/fped.2024.1438631
6. Gao L, Sun Y. Laboratory diagnosis and treatment of Mycoplasma pneumoniae infection in children: a review. Ann Med. 2024;56(1):2386636. doi:10.1080/07853890.2024.2386636
7. Wang G, Wu P, Tang R, Zhang W. Global prevalence of resistance to macrolides in Mycoplasma pneumoniae: a systematic review and meta-analysis. J Antimicrob Chemother. 2022;77(9):2353–2363. doi:10.1093/jac/dkac170
8. Kim K, Jung S, Kim M, Park S, Yang HJ, Lee E. Global trends in the proportion of macrolide-resistant Mycoplasma pneumoniae infections: a systematic review and meta-analysis. JAMA Netw Open. 2022;5(7):e2220949. doi:10.1001/jamanetworkopen.2022.20949
9. Liu Y, Ye X, Zhang H, et al. Characterization of macrolide resistance in Mycoplasma pneumoniae isolated from children in Shanghai, China. Diagn Microbiol Infect Dis. 2010;67(4):355–358. doi:10.1016/j.diagmicrobio.2010.03.004
10. Alavi Darazam I, Rabiei MM, Javandoust Gharehbagh F, et al. Recent macrolide resistance pattern of Mycoplasma pneumonia in the world: a systematic review and meta-analysis. Iran J Public Health. 2025;54(3):530–541. doi:10.18502/ijph.v54i3.18246
11. Yang HJ, Song DJ, Shim JY. Mechanism of resistance acquisition and treatment of macrolide-resistant Mycoplasma pneumoniae pneumonia in children. Korean J Pediatr. 2017;60(6):167–174. doi:10.3345/kjp.2017.60.6.167
12. Yen MH, Yan DC, Wang CJ, et al. The clinical significance of and the factors associated with macrolide resistance and poor macrolide response in pediatric Mycoplasma pneumoniae infection: a retrospective study. J Microbiol Immunol Infect. 2023;56(3):634–640. doi:10.1016/j.jmii.2023.01.010
13. Ahn JG, Cho HK, Li D, et al. Efficacy of tetracyclines and fluoroquinolones for the treatment of macrolide-refractory Mycoplasma pneumoniae pneumonia in children: a systematic review and meta-analysis. BMC Infect Dis. 2021;21(1):1003. doi:10.1186/s12879-021-06508-7
14. Wang YS, Zhou YL, Bai GN, et al. Expert consensus on the diagnosis and treatment of macrolide-resistant Mycoplasma pneumoniae pneumonia in children. World J Pediatr. 2024;20(9):901–914. doi:10.1007/s12519-024-00831-0
15. He B, Li X, Dong R, et al. Development of machine learning-based differential diagnosis model and risk prediction model of organ damage for severe Mycoplasma pneumoniae pneumonia in children. Sci Rep. 2025;15(1):9431. doi:10.1038/s41598-025-92089-3
16. Xie S, Wu M, Shang Y, et al. Development and validation of an early diagnosis model for severe mycoplasma pneumonia in children based on interpretable machine learning. Respir Res. 2025;26(1):182. doi:10.1186/s12931-025-03262-1
17. Yang B, Zhang W, Gu W, et al. Differences of clinical features and prognosis between Mycoplasma pneumoniae necrotizing pneumonia and non-Mycoplasma pneumoniae necrotizing pneumonia in children. BMC Infect Dis. 2021;21(1):797. doi:10.1186/s12879-021-06469-x
18. Fan F, Lv J, Yang Q, Jiang F. Clinical characteristics and serum inflammatory markers of community-acquired mycoplasma pneumonia in children. Clin Respir J. 2023;17(7):607–617. doi:10.1111/crj.13620
19. Søndergaard MJ, Friis MB, Hansen DS, Jørgensen IM. Clinical manifestations in infants and children with Mycoplasma pneumoniae infection. PLoS One. 2018;13(4):e0195288. doi:10.1371/journal.pone.0195288
20. Subspecialty Group of Respiratory. the society of pediatrics, chinese medical association; china national clinical research center of respiratory diseases; editorial board, chinese journal of pediatrics. evidence-based guideline for the diagnosis and treatment of Mycoplasma pneumoniae pneumonia in children (2023). Zhonghua Er Ke Za Zhi. 2024;62(12):1137–1144. doi:10.3760/cma.j.cn112140-20240722-00503
21. Su D, Li J, Ren J, et al. The relationship between serum lactate dehydrogenase level and mortality in critically ill patients. Biomarker Med. 2021;15(8):551–559. doi:10.2217/bmm-2020-0671
22. Yang L, Zhang Y, Shen C, et al. Clinical features and risk factors of plastic bronchitis caused by Mycoplasma pneumoniae pneumonia in children. BMC Pulm Med. 2023;23(1):468. doi:10.1186/s12890-023-02766-0
23. Lee E, Choi I. Clinical usefulness of serum lactate dehydrogenase levels in Mycoplasma pneumoniae pneumonia in children. Indian J Pediatr. 2022;89(10):1003–1009. doi:10.1007/s12098-022-04205-0
24. Izumikawa K. Clinical features of severe or fatal Mycoplasma pneumoniae pneumonia. Front Microbiol. 2016;7:800. doi:10.3389/fmicb.2016.00800
25. Miyashita N, Kawai Y, Inamura N, et al. Setting a standard for the initiation of steroid therapy in refractory or severe Mycoplasma pneumoniae pneumonia in adolescents and adults. J Infect Chemother. 2015;21(3):153–160. doi:10.1016/j.jiac.2014.10.008
26. Mishra KP, Ganju L, Singh SB. Hypoxia modulates innate immune factors: a review. Int Immunopharmacol. 2015;28(1):425–428. doi:10.1016/j.intimp.2015.07.008
27. Qiu J, Ge J, Cao L. D-dimer: the risk factor of children’s severe Mycoplasma pneumoniae pneumonia. Front Pediatr. 2022;10:828437. doi:10.3389/fped.2022.828437
28. Zheng Y, Hua L, Zhao Q, et al. The level of d-dimer is positively correlated with the severity of Mycoplasma pneumoniae pneumonia in children. Front Cell Infect Microbiol. 2021;11:687391. doi:10.3389/fcimb.2021.687391
29. Cacciotto C, Cubeddu T, Addis MF, et al. Mycoplasma lipoproteins are major determinants of neutrophil extracellular trap formation. Cell Microbiol. 2016;18(12):1751–1762. doi:10.1111/cmi.12613
30. Wang C, Wen J, Yan Z, et al. Suppressing neutrophil itaconate production attenuates Mycoplasma pneumoniae pneumonia. PLoS Pathog. 2024;20(11):e1012614. doi:10.1371/journal.ppat.1012614
31. Li D, Gu H, Chen L, et al. Neutrophil-to-lymphocyte ratio as a predictor of poor outcomes of Mycoplasma pneumoniae pneumonia. Front Immunol. 2023;14:1302702. doi:10.3389/fimmu.2023.1302702
32. Zou Y. Clinical significance of abnormal inflammatory markers in Mycoplasma pneumoniae pneumonia. Chin J Appl Clin Pediatr. 2021;36(16):1209–1214.
33. Shen W, Sun X. Construction of a nomogram for early diagnosis of refractory Mycoplasma pneumoniae pneumonia in children. Transl Pediatr. 2024;13(7):1119–1129. doi:10.21037/tp-24-16
34. Chang Q, Chen HL, Wu NS, Gao YM, Yu R, Zhu WM. Prediction model for severe Mycoplasma pneumoniae pneumonia in pediatric patients by admission laboratory indicators. J Trop Pediatr. 2022;68(4):fmac059. doi:10.1093/tropej/fmac059
35. Luo XQ, Luo J, Wang CJ, Luo ZX, Tian DY, Xie XH. Clinical features of severe Mycoplasma pneumoniae pneumonia with pulmonary complications in childhood: a retrospective study. Pediatr Pulmonol. 2023;58(10):2815–2822. doi:10.1002/ppul.26593
36. Oishi T, Yoshioka D, Nakano T, Ouchi K. Recent trend of antimicrobial susceptibility among Mycoplasma pneumoniae isolated from japanese children. Microorganisms. 2022;10(12):2428. doi:10.3390/microorganisms10122428
37. Cao B, Zhao CJ, Yin YD, et al. High prevalence of macrolide resistance in Mycoplasma pneumoniae isolates from adult and adolescent patients with respiratory tract infection in China. Clin Infect Dis. 2010;51(2):189–194. doi:10.1086/653535
38. Acute Respiratory Diseases Study Group. Morozumi M, Iwata S, Hasegawa K, et al. Increased macrolide resistance of Mycoplasma pneumoniae in pediatric patients with community-acquired pneumonia. Antimicrob Agents Chemother. 2008;52(1):348–350. doi:10.1128/AAC.00779-07.
39. Ming D. Progress in the pharmacological treatment of paediatric Mycoplasma pneumoniae. Clin Med. 2021;41(1):120–122.
40. Waites KB, Xiao L, Liu Y, Balish MF, Atkinson TP. Mycoplasma pneumoniae from the respiratory tract and beyond. Clin Microbiol Rev. 2017;30(3):747–809. doi:10.1128/CMR.00114-16
41. Subramanian A. Emerging roles of bacteriophage-based therapeutics in combating antibiotic resistance. Front Microbiol. 2024;15:1384164. doi:10.3389/fmicb.2024.1384164
42. Ezzeddine Z, Ghssein G. Towards new antibiotics classes targeting bacterial metallophores. Microb Pathog. 2023;182:106221. doi:10.1016/j.micpath.2023.106221
43. Tillotson GS. Trojan horse antibiotics-a novel way to circumvent gram-negative bacterial resistance? Infect Dis. 2016;9:45–52. doi:10.4137/IDRT.S31567
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.