Back to Journals » Journal of Multidisciplinary Healthcare » Volume 16
Development of a Multidisciplinary Clinic for Patients with Ehlers Danlos Syndromes: Considerations and Strategies
Authors Black WR ![]() , Jones JT
, Jones JT ![]() , Rush ET, Malloy Walton L, Harding A
, Rush ET, Malloy Walton L, Harding A
Received 5 November 2022
Accepted for publication 8 January 2023
Published 21 January 2023 Volume 2023:16 Pages 191—195
DOI https://doi.org/10.2147/JMDH.S396221
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Scott Fraser
William R Black,1,2 Jordan T Jones,1,3,4 Eric T Rush,1,3,4 Lindsey Malloy Walton,1,3,4 Ashley Harding5
1Department of Pediatrics, University of Kansas School of Medicine, Kansas City, KS, USA; 2Center for Children’s Healthy Lifestyles and Nutrition, Children’s Mercy Kansas City, Kansas City, MO, USA; 3Department of Pediatrics, Children’s Mercy Kansas City, Kansas City, MO, USA; 4University of Missouri-Kansas City School of Medicine, Kansas City, MO, USA; 5Children’s Mercy Kansas City, Kansas City, KS, USA
Correspondence: William R Black, Department of Pediatrics, University of Kansas School of Medicine, 3901 Rainbow Blvd, Kansas City, KS, 66103, USA, Tel +1 913 588 6323, Email [email protected]
Abstract: Ehlers-Danlos Syndromes (EDS) is a group of connective tissue disorders often encountered within rheumatology clinics and is associated with several overlapping symptoms, which may require attention from other medical subspecialities. Barriers exist to implementing multidisciplinary care for EDS, including a lack of knowledge, comfort, and time managing EDS. In the absence of multidisciplinary care, patients are often forced to self-coordinate care. This can lead to gaps in care and a lack of clarity of medical ownership over the patient’s care. Integrated multidisciplinary clinics are sorely needed, but the development and implementation of such clinics is limited by resources and personnel. As such, the development of a multidisciplinary clinic can be daunting and may serve to discourage providers with competencies in EDS from attempting to develop this service. In this editorial, we share our experiences in developing a multidisciplinary clinic for EDS at a moderately-sized children’s hospital, relying on several core disciplines with established EDS clinical loads (ie, rheumatology, cardiology, genetics, and psychology). We discuss considerations for the expansion of this service, pitfalls, and barriers throughout the development of the clinic, and our rationale underlying our process-related decisions. Development of a greater number of multidisciplinary EDS clinics, even in the potential absence of larger institutional support, is both possible and imperative for improving EDS care globally.
Keywords: Ehlers-Danlos, hypermobility, multidisciplinary, pediatrics
Introduction
Ehlers-Danlos Syndromes (EDS) represent a family of heritable connective tissue disorders with features that include joint hypermobility, tissue fragility, and skin hyperextensibility.1 Conservative estimates suggest that EDS occurs in approximately 1 in 2500 to 5000 babies worldwide annually.2 There are currently 13 recognized distinct clinical subtypes of EDS.1 Symptomatic joint hypermobility, which includes the most common subtype of EDS (ie, hypermobile EDS [hEDS]), has an estimated prevalence of 20 per 1000.3 hEDS also involves multiple body systems including neurologic, cardiovascular, gastrointestinal, musculoskeletal, and mental health and cognitive symptoms.3 Other areas of difficulty, including attention and working memory,4 and proprioception,5 may have wide-reaching impacts on other areas of functioning. These variable presenting symptoms necessitates the involvement of numerous subspecialists. With each symptom more specialty referrals are added, which leads to a need for coordinated multidisciplinary care from EDS knowledgeable providers.6
Barriers exist that may prevent implementation of an EDS multidisciplinary care model, including lack of knowledge, comfort, and time in managing patients with EDS.7 Additionally, providers report greater comfort co-managing EDS in conjunction with a team of EDS specialists rather than developing their own management plans,7 which further supports a multidisciplinary care model with each specialty focused on the patients’ symptoms that fall into their expertise. Another barrier occurs when coordinated multidisciplinary care is lacking and patients are forced to coordinate their own multidisciplinary care as this self-coordinated care can lead to unclear ownership of the patient, lack of a medical home, and overutilization of healthcare. There is a critical opportunity to provide coordinated care for those with EDS that is convenient and of higher quality than patients self-coordinated care among multiple health-care systems and sub-specialty providers.
There has been greater recognition of the need for integrated multi-disciplinary care for adults with EDS, specifically those with hEDS,8,9 but comprehensive EDS-focused care has been limited by resources and personnel to commit to such programs from the onset. Here, we discuss our experiences in developing a multidisciplinary clinic for the treatment of EDS, how it has grown and been modified, and provide rationale for our model of care.
Clinic Development
The clinic began organically as several specialties identified a cohort of shared pediatric patients with a diagnosis of EDS that had overlapping clinical needs that were utilizing similar resources in the healthcare system. Patients were being seen by the same specialties, but there was variability in diagnosis, education, and flow through the healthcare system. A core of highly utilized specialties that included cardiology, genetics, physical therapy, psychology, and rheumatology came together to provide EDS-focused care. Initially, all hypermobile patients were referred to a multidisciplinary EDS clinic. This initial model included a four-hour clinic visit that included an initial evaluation by genetics to determine EDS diagnosis. If confirmed, then the other multidisciplinary providers would individually evaluate and provide recommendations, but if a diagnosis was not provided, then patients were not seen by the multidisciplinary providers (see Figure 1). The multidisciplinary team discussed each patient in an ongoing case conference during the visit. This typically included an initial description of the patients and presenting concerns by AH after the patient was roomed. A brief synopsis and handoff was provided among providers as they rotated through the patients. Several issues emerged with this model:
- Families complained about the length of the visit and amount of information received (diagnosis and management recommendations from several specialties).
- With longer appointments, fewer patients could be scheduled and seen during a clinic day, worsening clinic visit wait times.
- Those that did not receive an EDS diagnosis did not see any other providers and their slots went unused, which underutilized specialty providers, and also worsened clinic visit wait times.
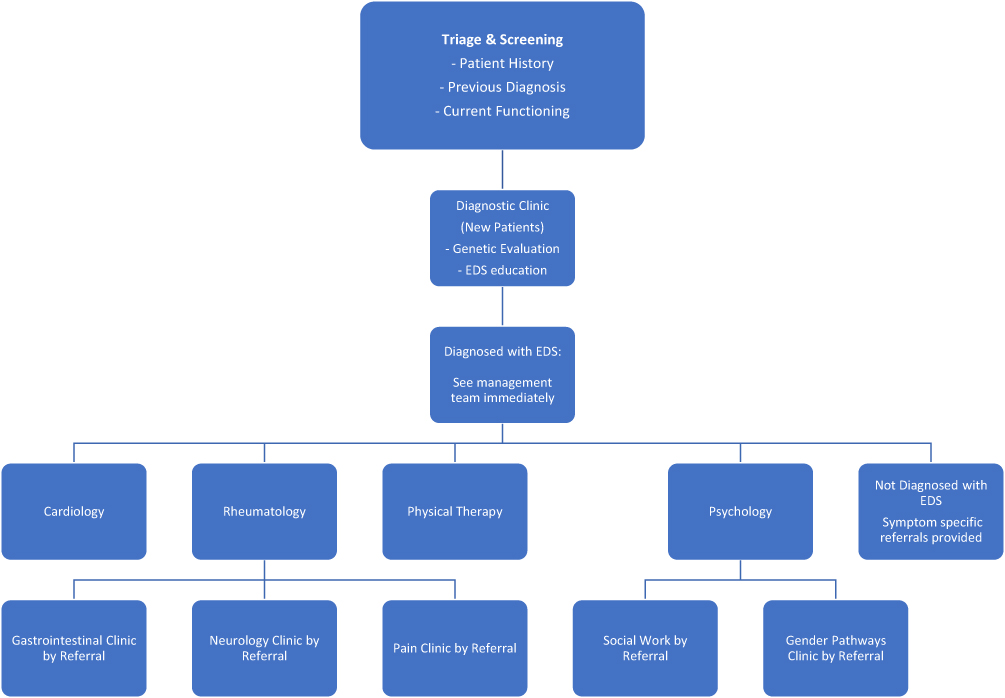 |
Figure 1 Multidisciplinary EDS clinic flow: original version. |
To address these issues, a parallel clinic model was initiated with separate diagnostic and multidisciplinary management (MDC) paths that would run simultaneously (Figure 2). This allowed those without a diagnosis to be seen and diagnosed, while those previously diagnosed could be managed by the MDC. Referrals were triaged appropriately, and the parallel model yielded three immediate benefits:
- It provided a more direct route for specific referral needs.
- Reduced wasted clinic time via fewer un-filled appointment slots.
- It increased the number of patients diagnosed and managed and decreased clinic visit wait times.
 |
Figure 2 Multidisciplinary EDS clinic flow: current version. |
The parallel clinics ran simultaneously one full day per month, with new patients seeing the genetics team and established patients seeing the multidisciplinary team. “Established” patients include those that had previously seen the genetics team or were referred to a clinic with a reliable diagnosis of EDS. Previous to adjusting to this parallel format, over 4 months, the multidisciplinary providers saw 58% (11/19) of patients that had been scheduled and seen by our genetics providers. Furthermore, four additional patient slots were unfilled due to last minute cancellations or no-shows, meaning that only 48% (11/23) of possible multidisciplinary slots were seen. After implementation of this model, in the next 6-month period, out of 35 possible appointment slots, 34 patients were seen by multidisciplinary providers (97% of appointment slots). Additionally, the initial wait time for the EDS clinic decreased from 24 months to 16 months for each path of the clinic. A second full clinic day was then added per month and the wait times decreased to 12 months. The diagnostic visits average 1 hour and the MDC visits average close to 3 hours.
Future Goals
We receive many requests for additional subspecialty care as part of the MDC and have not been able to include all needed providers due to coordination issues and logistics around organizing multi-hour team visits. At present, we utilize our core clinic disciplines to identify and refer to other clinics as needed (see Figure 2). This has been challenging as it requires specialty knowledge, availability, interest, coordination, and leads to longer visits. There may be an opportunity to use our triage process to assign patients to different “days” (eg, 1 day with psychology available, 1 day with GI available). Additionally, we have started education initiatives to connect to local and regional providers and better involve community clinicians in providing EDS care. Additionally, providers managing medical conditions in which pain is a presenting symptom, such as rheumatologists and primary care providers, are well positioned to help guide and manage EDS patients with multiple comorbidities. While MDC care may not be feasible for some institutions initially, referral lines and expertise can be developed. Our clinic’s focus has been on diagnosis and initial treatment planning, and we are evaluating models for routine follow-up care.
Here, we highlight the approach and early considerations in developing a multidisciplinary clinic for EDS. The development of the clinic was able to focus largely on reducing barriers to care and more efficiently addressing patient needs. We arrived at our model (parallel diagnostic and MDC clinics) as an attempt to improve convenience for families, increase clinical efficiency, decrease wait-list times, and provide patients with access to multiple providers. Since the initial development of this clinic, we have attempted to modify our processes to better meet the needs of our local EDS population and remain vigilant to continued opportunities for growth and novel approaches to deliver care.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Disclosure
Dr Eric T Rush reports grants and/or personal fees from Alexion AstraZeneca Rare Disease, Ultragenyx Pharmaceuticals, BioMarin Pharmaceuticals, Inozyme Pharma, Ascendis Pharma, Kyowa Kirin Pharmaceuticals, and Angitia Bio, outside the submitted work. The authors declared no other potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
References
1. Malfait F, Castori M, Francomano CA, Giunta C, Kosho T, Byers PH. The Ehlers-Danlos syndromes. Nat Rev Dis Primers. 2020;6(1):64. doi:10.1038/s41572-020-0194-9
2. Joseph AW, Joseph SS, Francomano CA, Kontis TC. Characteristics, diagnosis, and management of Ehlers-Danlos syndromes: a review. JAMA Facial Plast Surg. 2018;20(1):70–75. doi:10.1001/jamafacial.2017.0793
3. Tinkle B, Castori M, Berglund B, et al. Hypermobile Ehlers-Danlos syndrome (a.k.a. Ehlers-Danlos syndrome Type III and Ehlers-Danlos syndrome hypermobility type): clinical description and natural history. Am J Med Genet C Semin Med Genet. 2017;175(1):48–69. doi:10.1002/ajmg.c.31538
4. Baeza-Velasco C, Bulbena A, Polanco-Carrasco R, Jaussaud R. Cognitive, emotional, and behavioral considerations for chronic pain management in the Ehlers-Danlos syndrome hypermobility-type: a narrative review. Disabil Rehabil. 2019;41(9):1110–1118. doi:10.1080/09638288.2017.1419294
5. Scheper MC, Engelbert RH, Rameckers EA, Verbunt J, Remvig L, Juul-Kristensen B. Children with generalised joint hypermobility and musculoskeletal complaints: state of the art on diagnostics, clinical characteristics, and treatment. Biomed Res Int. 2013;2013:121054. doi:10.1155/2013/121054
6. Jones JT, Black WR, Cogan W, Callen E. Resource utilization and multidisciplinary care needs for patients with Ehlers-Danlos syndrome. Mol Genet Genomic Med. 2022;10(11):e2057. doi:10.1002/mgg3.2057
7. Jones JT, Black WR. Provider knowledge and experience in care, management, and education of pediatric Ehlers-Danlos syndrome. Glob Pediatr Health. 2022;9:2333794X221112841. doi:10.1177/2333794X221112841
8. Knight DRT, Confiado SM, Bruno KA, et al. Establishing an Ehlers-Danlos syndrome clinic: lessons learned. SN Compr Clin Med. 2022;4(1):138. doi:10.1007/s42399-022-01218-w
9. Mittal N, Mina DS, McGillis L, et al. The GoodHope Ehlers Danlos Syndrome Clinic: development and implementation of the first interdisciplinary program for multi-system issues in connective tissue disorders at the Toronto General Hospital. Orphanet J Rare Dis. 2021;16(1):357. doi:10.1186/s13023-021-01962-7
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.