Back to Journals » Patient Preference and Adherence » Volume 20
Development of a Complex Biofeedback-Based Intervention to Improve Methotrexate Adherence in Rheumatoid Arthritis: A COM-B Model Informed Qualitative Study
Authors Shafi H ![]() , Armitage CJ, Verstappen SMM, Barton A, Lee RR, Bluett J
, Armitage CJ, Verstappen SMM, Barton A, Lee RR, Bluett J ![]()
Received 7 July 2025
Accepted for publication 14 January 2026
Published 26 February 2026 Volume 2026:20 548188
DOI https://doi.org/10.2147/PPA.S548188
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Ramón Morillo-Verdugo
Hannah Shafi,1 Christopher J Armitage,2 Suzanne M M Verstappen,3,4 Anne Barton,1,4 Rebecca R Lee,2,3 James Bluett1,4
1Versus Arthritis Centre for Genetics and Genomics, Centre for Musculoskeletal Research, the University of Manchester, Manchester, UK; 2Manchester Centre for Health Psychology, Division of Psychology and Mental Health, NIHR Greater Manchester Patient Safety Research Collaboration, Manchester University NHS Foundation Trust, Manchester Academic Health Science Centre, The University of Manchester, Manchester, UK; 3The Centre for Epidemiology, the Centre for Musculoskeletal Research, the Division of Musculoskeletal and Dermatological Sciences, the Faculty of Biology, Medicine and Health, The University of Manchester, Manchester Academic Health Science Centre, Manchester, UK; 4NIHR Manchester Biomedical Research Centre, Manchester University NHS Foundation Trust, Manchester Academic Health Science Centre, Manchester, UK
Correspondence: Hannah Shafi, Versus Arthritis Centre for Genetics and Genomics, Centre for Musculoskeletal Research, the University of Manchester, Manchester, UK, Tel +441613061249, Email [email protected]
Introduction: Methotrexate (MTX) is one of the first-line treatments for Rheumatoid arthritis (RA) but sub-optimal adherence to MTX is common. Adherence can be challenging to detect in the clinic but can be assessed objectively using a MTX biochemical adherence test measuring levels of MTX in the blood. However, it remains unknown how to use the results of MTX biochemical adherence tests to improve adherence. COMMIT (development of a COMplex Methotrexate adherence IntervenTion utilising biofeedback) is a qualitative study designed to explore adherence to MTX in RA patients and aid the development of a behaviour change intervention that can be delivered alongside MTX biochemical adherence testing.
Methods: Potential participants were identified from the Rheumatoid Arthritis Medications Study (RAMS), a large national study of patients with RA commencing MTX. An interview topic guide was developed using the Capability, Opportunity and Motivation to Behaviour (COM-B) model and the Theoretical Domains Framework (TDF). Consenting participants took part in a 1:1 semi-structured telephone interview. Transcripts were inductively analysed and mapped to themes.
Results: Seventeen participants treated with MTX for a mean 3 years (range 3– 20) took part in the semi-structured interviews. Five overarching themes were identified and mapped to behaviour change techniques. Themes included 1. Knowledge of MTX and its impact, 2. Motivators versus barriers for continuation of MTX, 3. The healthcare approach in shaping patient adherence, 4. Creating habits and routines 5. MTX biochemical adherence blood tests and external monitoring of behaviour.
Conclusion: This study has identified many of the key facilitators and barriers that influence adherence to methotrexate in RA patients. Through identifying the capabilities, opportunities, and motivations that shape engagement with MTX biochemical adherence testing, we can select targeted behaviour change techniques to address these factors. This theory-driven approach offers a novel pathway to improving uptake of MTX adherence testing.
Keywords: biochemical adherence, qualitative research, methotrexate, self-management
Introduction
Rheumatoid arthritis (RA) is a chronic disease for which there is no known cure that affects ~1% of the adult population.1 The hallmark of RA is symmetrical joint inflammation which, when left untreated, can lead to joint destruction, disability, multimorbidity and reduced life expectancy by up to 10 years.2 RA treatment is predominantly aimed at controlling joint inflammation and early effective therapy reduces disability, joint damage and mortality.3,4 Conventional Synthetic Disease Modifying Anti-Rheumatic drugs (csDMARDs) aim to lower disease activity and manage symptoms associated with RA such as pain associated with the inflammation which may prevent individuals from completing usual activities. For example, oral methotrexate (MTX) is a first-line therapy for RA and is often used in other conditions such as psoriasis. MTX has a number of potential serious side effects such as life-threatening pneumonitis, leukopenia and gastro-intestinal toxicity.5,6 Patients with RA are expected to adhere consistently over a long period of time to MTX, as well as a range of other medications to manage other aspects of their conditions (e.g. pain relief, fatigue and emotional well-being). Adherence to MTX is not universal and is likely to be influenced by biological (e.g. no response to MTX), clinical (e.g. age), psychological (e.g. beliefs about the medication and its impact) and/or social factors (e.g. not wanting to miss out on opportunities with friends/family due to medication side-effects). Better adherence with MTX is strongly correlated with patients believing that the treatment is necessary and effective, as well as with absence of low mood or medication concerns.7,8
Existing strategies to improve MTX adherence in RA have largely centred on education, communication, and patient engagement. Evidence shows that educational and clinician-led interventions, such as the use of visual aids, can improve patients’ understanding and adherence.9,10 More recent work has emphasised the role of mindset and patient–clinician collaboration in supporting adherence.11 Theory-based approaches also demonstrate how behaviour change techniques can be systematically mapped onto intervention components. For example, a study on pain medication adherence in chronic pain patents identified target behaviours to address adherence such as routine patient education, habit formation, and open discussion of treatment concerns.12 These elements align with the Behaviour Change Wheel, where educational materials and clinician-led support correspond to the Education and Training functions aimed at strengthening patients psychological capability.13 Previous research has shown that MTX adherence is suboptimal ranging from 59 to 107%, with the latter figure representing overdosage which is also a form of non-adherence. It was further found that non-adherence was associated with poor treatment response.7 The prescriber is often unable to determine if a patient is adherent and there is no gold-standard method to assess or monitor adherence. Current National Institute for Health and Care Excellence (NICE) guidelines in the UK on medicines adherence suggest assessing non-adherence by asking the patient if they have missed any doses of medicines recently.12 Self-reporting can, however, lead to over- or under estimation of adherence. In contrast, biochemical measurement of adherence is objective compared to a self-report but can be considered as intrusive to patients (e.g. patients may feel that the healthcare professional has questioned the credibility of the patients’ responses). Concurrently, providing the patient a biochemical result with the aim of eliciting a positive behaviour change (“biofeedback”), is a behaviour change technique in its own right.13 Adherence to MTX can be measured biochemically using selected reaction monitoring-mass spectrometry (HPLC-SRM-MS,14 but it is not yet known how best to deliver the results of the blood test to improve MTX adherence.
In summary, biofeedback is an objective method of optimising adherence, but some patients may perceive it as intrusive. To date, no research has examined patients’ perspectives on the potential of MTX adherence biofeedback to influence their adherence behaviours. Thus, the aim of the study was to explore adult RA patients’ capabilities, opportunities and motivations for adhering or not to MTX. The Capabilities, Opportunities and Motivations model of Behaviour change (COM-B) model15 is a comprehensive model that can be used to explore behavioural determinants to medication adherence.16 This model suggests that the behaviour of taking prescribed medicine is a result of interactions between capability (psychological or physical), opportunity (social or physical) and motivation (automatic or reflective). The COM-B model can provide explanations of behavioural determinants in qualitative studies and support the development of targeted behaviour change interventions.15 Using the COM-B model to explore adherence to MTX in RA patients could aid the development of a behaviour change intervention that incorporates MTX biofeedback.
Methods
This section describes the study design, participant recruitment, study procedures, and data analysis of qualitative interviews.
Study Design
One-to-one semi-structured telephone interviews were conducted with patients who had a diagnosis of RA and experience of oral MTX therapy. This study has been reported in line with The Standards for Reporting Qualitative Research (SRQR). Please see Supplementary Table 1 for the completed SRQR checklist.
Participants
Twenty participants were recruited from the Rheumatoid Arthritis Medications Study (RAMS) approved by the Central Manchester NHS Research Ethics Committee (reference 08/H1008/25). This study complies with the Declaration of Helsinki. RAMS is a large national (UK) multi-centre (n = 38 centres) study of patients with a physician diagnosis of RA who are commencing MTX for the first time.17 Individuals who have taken part in RAMS and have indicated that they would be happy to be involved in future research projects were contacted by the study coordinators of COMMIT with the COMMIT invitation letter, patient information sheet (PIS), consent form and registration slip. RAMS participants were allocated a random number using the random number command in STATA version 12.0 (STATA).18 The allocated number was ordered, and participants were contacted in blocks of 30. As part of the protocol development, the invitation letters, protocol including topic guide, PIS and consent form were reviewed by a Research User Group, a group of people living with or caring for someone with a long-term musculoskeletal illness such as RA. The PIS informed potential participants that the aim of the study was to aid the development of an effective biofeedback tool for MTX adherence and that the research was being conducted by JB. Participants were asked to return their preferred contact details and time of contact (name, address, email address and telephone number) on a separate slip of paper. Participants were free to conduct the interview at a place of their convenience (eg at their home, at their workplace) and could take as long as they required to decide whether to take part. The PIS further described that all participant responses are confidential, and the interviews are anonymised. The participants were aware that any data collected would be kept securely on a system which only the researchers or auditors may access. The anonymised data was made available through OpenAccess publication, and this was highlighted to participants before being consented. A flowchart of study methodology is presented in Figure 1. For a Study, inclusion and exclusion criteria were as follows:
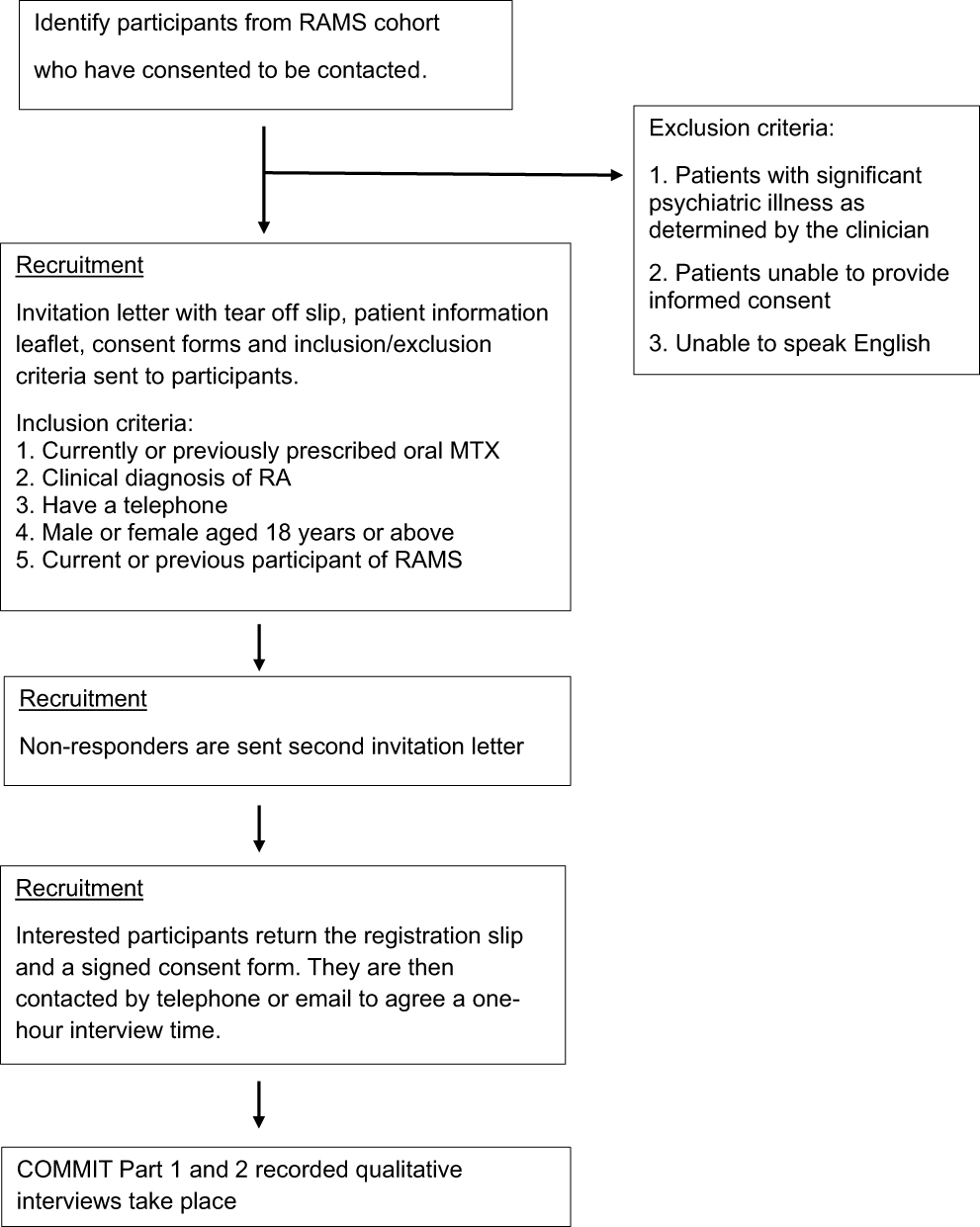 |
Figure 1 Flowchart of COMMIT study methodology. |
Inclusion Criteria
- Currently or previously prescribed oral MTX
- Clinical diagnosis of RA
- Have a telephone
- Male or female aged 18 years or above
- Current or previous participant of RAMS
Exclusion Criteria
- Patients with significant psychiatric illness as determined by the clinician
- Patients unable to provide informed consent
- Unable to speak English
Data collection was terminated when data saturation was achieved.19 Ethical approval for the current study was received from the University of Manchester Research Ethics Committee (Ref: 2021–10,990-17,851). This study complies with the Declaration of Helsinki.
Study Procedures
The lead researcher (JB), a male Consultant Academic Rheumatologist with training in behaviour change and intervention development, conducted the telephone interviews. No one else was present for the telephone interviews besides the participants and researchers. The researcher had no contact with the patients prior to this study. Informed consent forms were signed by the participant prior to the semi-structured interview being scheduled. Consent forms included agreement that anonymised responses and direct quotes would be included for publication.
The interview topic guide (Supplementary Table 2) drafted by JB was informed by the COM-B model (10). This model can be linked with intervention strategies for behaviour change.20 The TDF draws together the cognitive, emotional, environmental and social influence of behaviour and can be used to map into the domains of the COM-B model in order to give a more detailed insight into adherence behaviours.16,20 The interview topic guide covered the patients’ understanding of MTX, general perceptions towards adherence and feedback around biochemical adherence.
Telephone interviews were recorded with consent, transcribed by a university approved transcription service and anonymised for analysis. Participants did not review the transcriptions or provide feedback on the findings.
Data Analysis
A framework analysis approach was used to explore and compare similarities and differences in the beliefs and experiences of participants.21 Three authors (JB, RRL and HS) individually analysed the transcripts using NVivo version 1222 and results were compared. Data collection was stopped when no new themes were identified, and saturation was reached.19 Data analysis included the following processes which were conducted in a non-sequential order with reflection and updating of each process following discussion. Notes were updated throughout the process as adapted from Ritchie et al21 Figure 2 details the data analysis process. Three guiding questions were used throughout the analysis to support theme development: (1) What capabilities influence patients’ adherence to methotrexate (MTX)? (2) What opportunities facilitate or hinder adherence and (3) How do patients motivations shape their adherence to MTX?
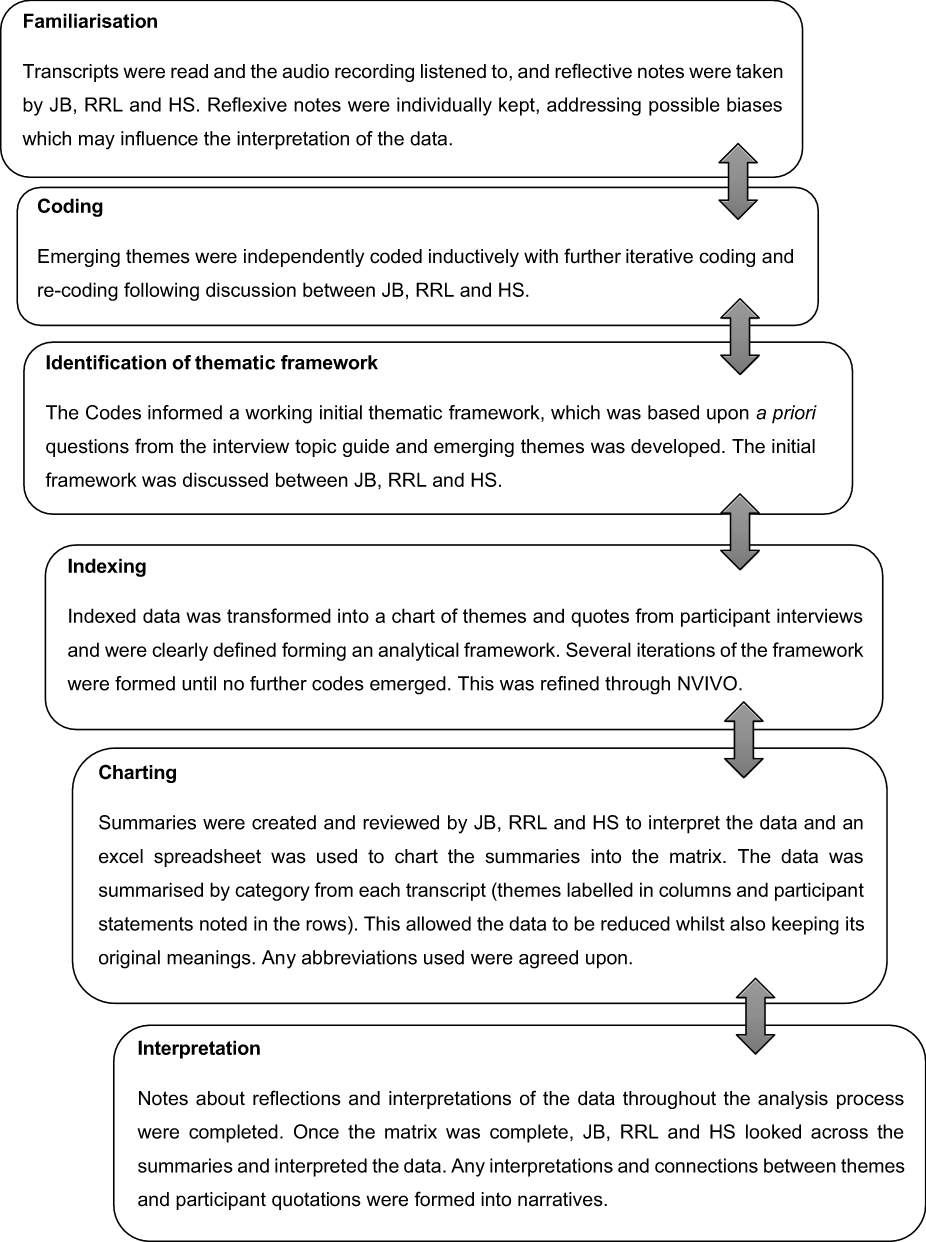 |
Figure 2 Data analysis process for COMMIT study. |
Results
Participant Clinico-Demographics
The final study sample was 17 participants, as further recruitment was stopped due to data saturation. Interviews lasted 22 to 45 minutes. Baseline clinico-demographics are presented in Table 1.
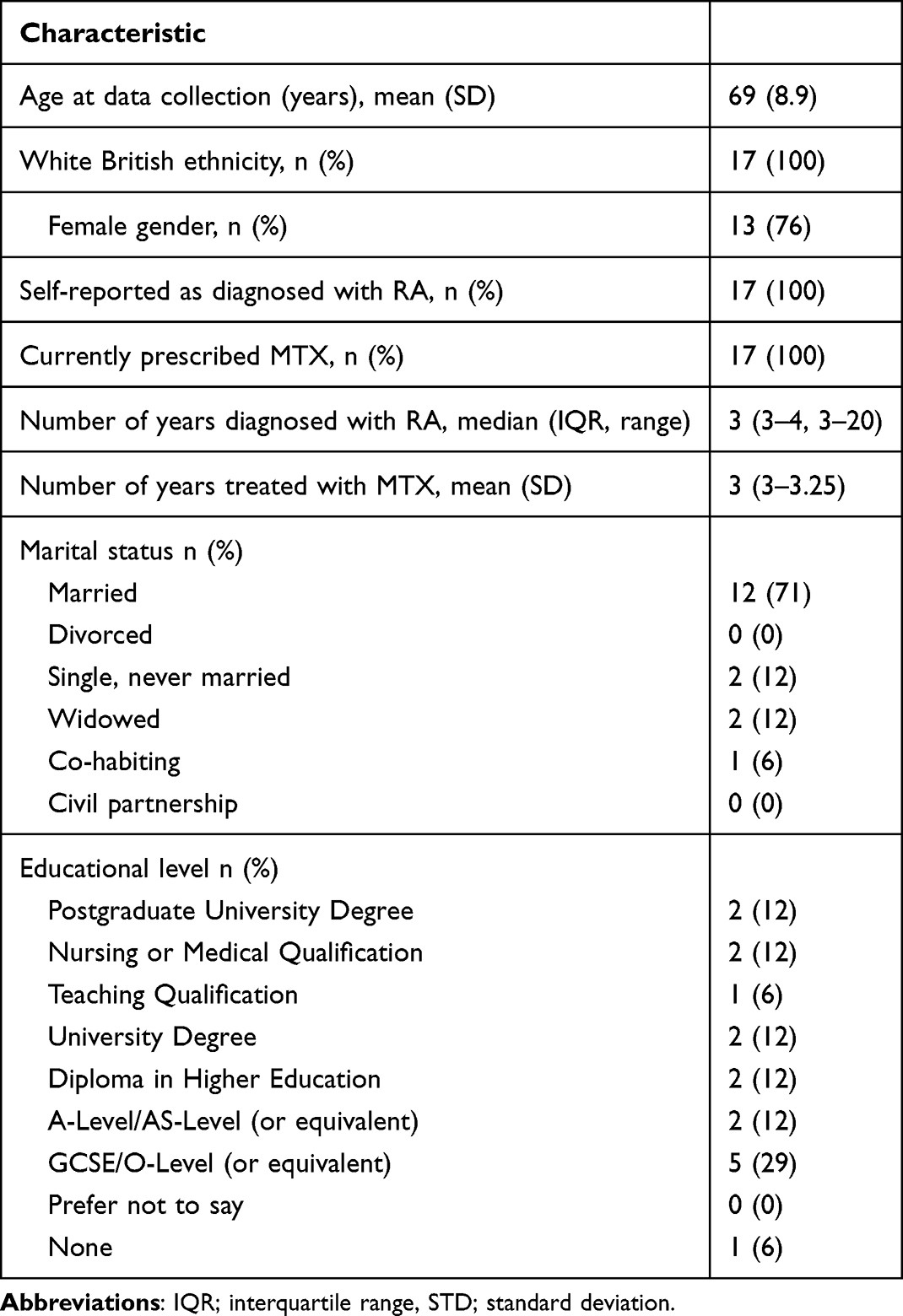 |
Table 1 Baseline Clinico-Demographic Variables |
Five overarching themes were identified as modifiers of MTX adherence behaviour that could be targeted as part of a biofeedback intervention:
- Knowledge of MTX and its impact
- Motivators versus barriers for continuation of MTX
- The healthcare approach in shaping patient adherence
- Creating habits and routines
- MTX biochemical adherence blood tests and external monitoring of behaviour
Theme 1: Knowledge of MTX and Its Impact
Themes 1 and 2 describe participants understanding of MTX and how their experiences shape their motivation and ability to continue treatment. Table 2 presents direct quotes linked to these themes.
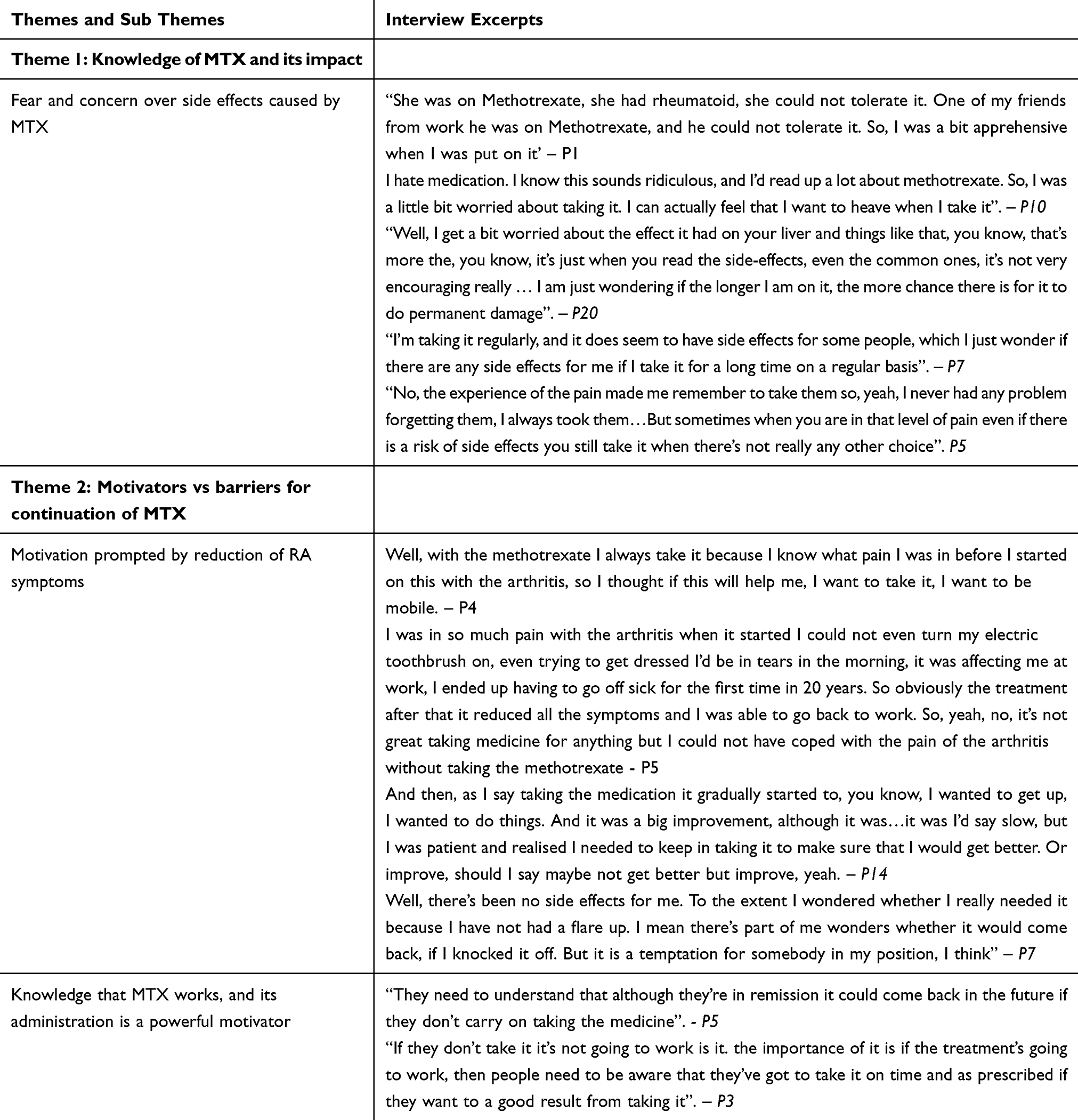 |
Table 2 Themes 1 and 2, Subthemes and Associated Interview Excerpts |
Fear and Concern Over Side-Effects Caused by MTX
One participant reported having a physical reaction to MTX, and after learning more about it, they became even more hesitant to continue. Concerns about using MTX were reported to be influenced by other people’s experiences with the medication. Fears were heightened when participants heard about the side effects, others have faced and the challenges in managing such side effects, thus leading to intentional non-adherence. Other participants expressed concerns about the long-term side effects of prolonged MTX use. While they continue to take the medication regularly, there is an underlying fear that MTX may cause toxicity over time. Participants awareness of both common and rare side effects can intensify this fear. Additionally, participants noted that the number of tablets they must take can be inconvenient, reducing their motivation to adhere to the dose.
Similar to previous motivations for adhering to MTX, it was found that the necessity of taking the medication is a strong motivator. Most participants conveyed a fear of returning to their initial pain levels, which drives them to continue taking MTX. This fear alone acts as a powerful incentive to stay consistent in taking the MTX.
Theme 2: Motivators vs Barriers for Continuation of MTX
Motivation Prompted by Reduction of RA Symptoms
The participants reflected on the need to follow the suggested dosage, noting that their inflammation and pain returned if they stopped MTX. This acted as a key motivator to take the medication as directed, in order to achieve its full benefits. Although the process of continually taking MTX was gradual, they noted that consistent use of MTX leads to long-term symptom improvement and enhanced quality of life. This portrays participants’ perceptions of the importance of patience and persistence with the treatment. However, some participants stated that they may stop taking MTX because they have not experienced any flare-ups. The absence of symptoms, paradoxically, leads them to believe that they would not experience recurrence of RA without MTX. This leads to participants questioning the effectiveness of MTX or that RA has perhaps been cured and does not require any further treatment.
Knowledge That MTX Works and Its Administration is a Powerful Motivator
Overall, the participants showed a general understanding of how MTX works and the importance of adhering to the prescribed dose regardless of short- or long-term concerns. Participants expressed that they adhere to MTX due to the significant pain relief it provides, resulting in an improved quality of life. This improvement acted as a strong motivator to continue taking the medication, as reduced symptoms have allowed them to engage in activities they were previously unable to do. Participants suggested that providing more detailed information about MTX (how it works and the potential consequences of not taking it as prescribed) could improve adherence. They believed that this information should be delivered in a formal manner, such as an official letter from their GP, to emphasise the seriousness of missing doses. This approach could also aid healthcare professionals (HCPs) in identifying the root causes of the patient’s non-adherence. Offering education about MTX would give participants a deeper understanding of their condition which in turn could motivate them to take their dose consistently.
Theme 3: The Healthcare Approach in Shaping Patient Adherence
Themes 3 and 4 describe how both the healthcare approach and patient led strategies contribute to maintaining MTX adherence. Together, they highlight the interplay between professional guidance and personal habit formation in sustained MTX adherence. Table 3 presents direct quotes for Themes 3 and 4.
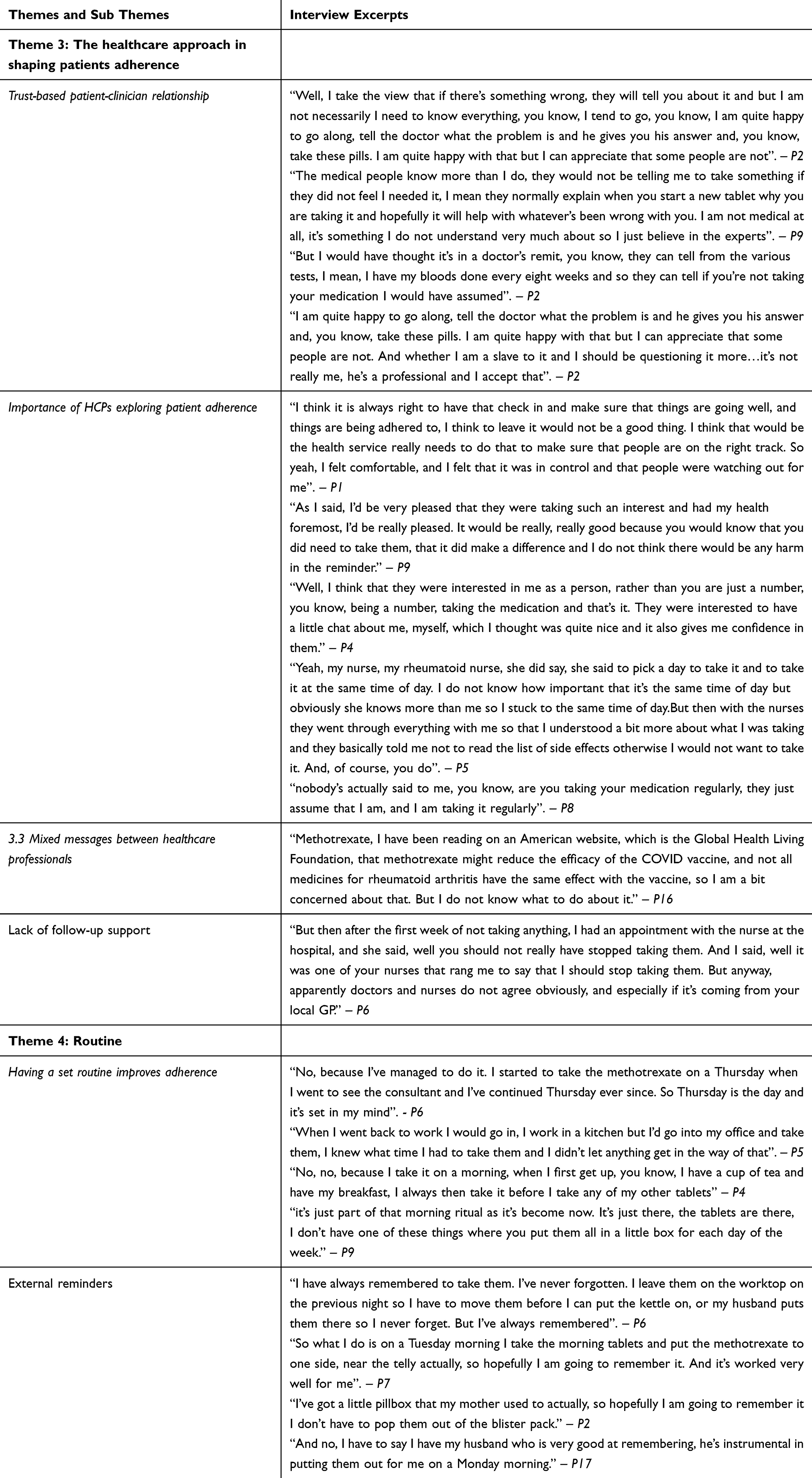 |
Table 3 Themes 3 and 4, Subthemes and Associated Interview Excerpts |
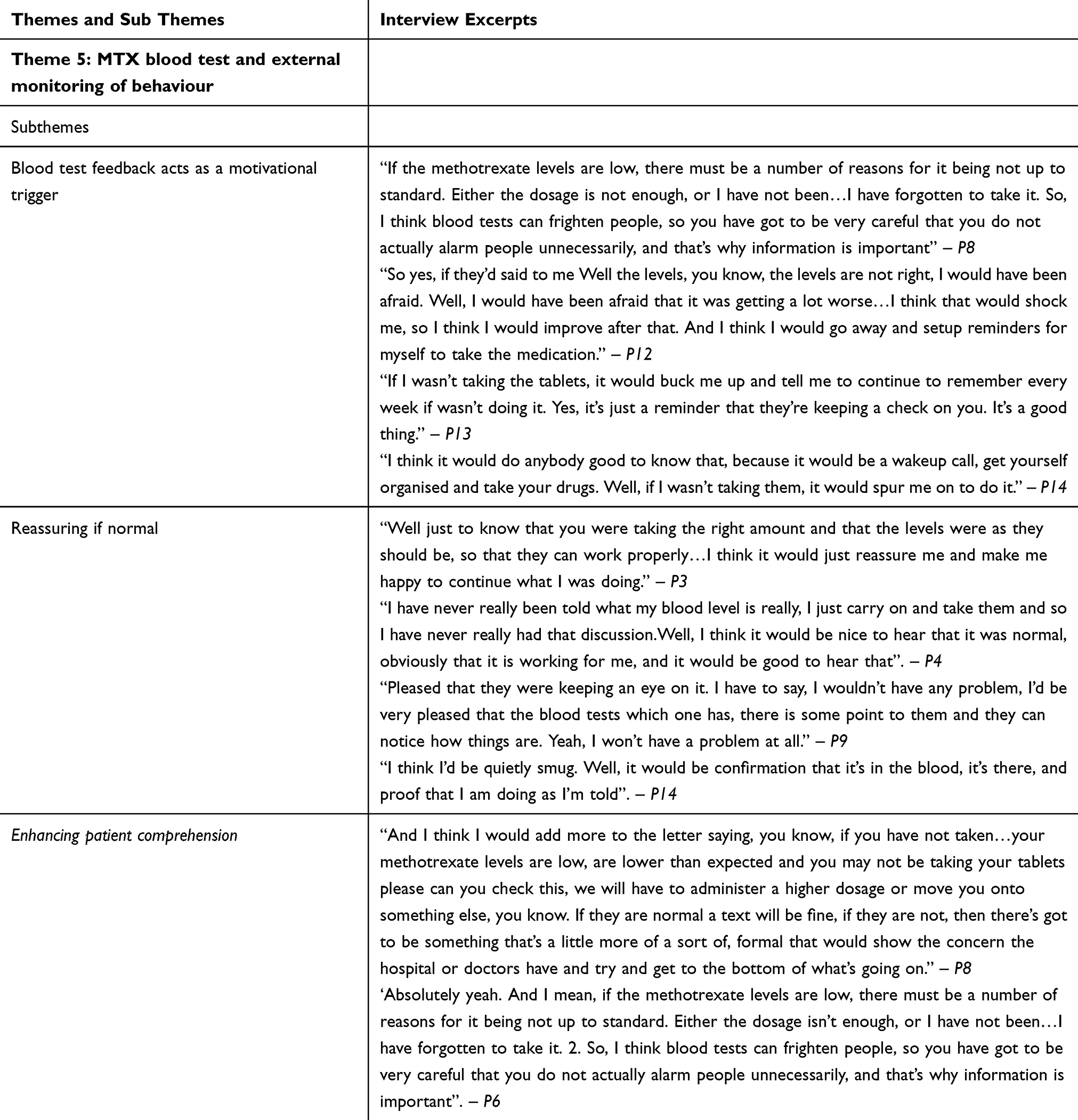 |
Table 4 Theme 5, Subthemes and Associated Interview Excerpts |
Trust-Based Patient-Clinician Relationship
Several participants spoke about their beliefs that taking MTX as prescribed would improve their symptoms. The majority stated that they had no doubts or concerns about following the instructions given by HCPs. In addition, participants trusted that HCPs were the most knowledgeable about the medication and they would not over question their advice. Participants felt that they lacked expertise to challenge the HCPs opinion and instead placed their full trust in the HCPs. Another participant expressed a similar feeling stating that they would take MTX without hesitation with full confidence it would be effective. However, following the advice given by HCPs, participants believed that it is the patient’s responsibility to ensure that they are taking their dose as prescribed.
Importance of HCPs Exploring Patient Adherence
Some participants believed that it was the role of the HCPs to ensure that medication is being adhered to. Participants felt it was the HCPs responsibility to check how patients were coping with the medication and whether they experienced any problems. The involvement of the HCPs was found to be very helpful and reassuring by participants in the current study. The participants felt that they were interested in them and cared for the progression of their health. Other participants felt that their HCPs showed a genuine interest of their situation, which encouraged them to open up about their troubles with adherence. Being able to ask questions helped alleviate fears about taking MTX. These conversations aided in boosting the participants’ confidence and motivation, making them feel more comfortable with their medication. The participants reflected that the HCPs were patient rather than forceful. They offered suggestions in a respectful manner and allowed participants to consider their advice at their own pace.
Mixed Messages Between Healthcare Professionals
Participants reported an issue with the lack of communication between HCPs. In instances, a GP may prescribe MTX, but the nurse does not agree that they should be taking it. As a result, patients may reduce or stop taking their MTX due to conflicting information. Participants also discussed how different medical websites offer different and sometime contradicting information about MTX and its effect on other medications being taken. This can raise concerns as information is not consistent and may reduce the motivation to adhere to MTX treatment.
Lack of Follow-Up Support
Some participants mentioned a lack of follow-up support from healthcare professionals after being prescribed MTX; with the HCP assuming the patient was adhering to their medication. As a result, no further follow-up was provided. The level of support from HCPs varied, with some participants receiving plenty of advice and reassurance, whilst others feeling they were left on their own after being prescribed MTX with no follow-up support or advice about side effects.
Theme 4: Creating Habits and Routine
Having a Set Routine Improves Adherence
Participants talked about the importance of routine in adherence. Those who took their MTX on a specific time and day of the week, were more likely to remember to take their medication. This can reduce the chances of missing a dose. Participants shared that they ensured they took their medication on time, regardless of their plans, making their routine so ingrained that they rarely forgot. Similarly, it was reported that incorporating MTX into routine, often in the morning with breakfast, ensures consistent adherence. This eliminated the need to organise their medication such as using labelled tablet boxes as the act of taking their dose is embedded in their routine and they were unlikely to forget.
External Reminders
Other participants valued having external reminders (such as pill boxes and phone alarms) to help take the correct dose on time. An example of another external reminder includes personal habits like placing their MTX in a visible spot as a visual cue. Family and friends also serve as a reminder. Participants explained that they share the responsibility of adhering to their MTX by relying on others to help them remember to take it.
Theme 5: MTX Biochemical Adherence Blood Tests and External Monitoring of Behaviour
Table 4 shows direct quotes for Theme 5, exploring the role of blood tests in MTX adherence.
Blood Test Feedback Acts as a Motivational Trigger
Blood tests results prove to be a major motivator for patients to adhere to MTX. Negative blood test results can instil fear and as a result, encourages patients to take their medication more regularly. These tests prompt patients to reflect on why their MTX levels may be low and whether this is linked to their inconsistent adherence of MTX. Some may use these blood tests as a way to improve their adherence to MTX. Without improvement in their test results, they realise there will be no change in their RA.
Reassuring if Normal
In contrast to instilling fear when negative, participants reported that blood tests would provide reassurance to patients when they are normal or within range. Participants discussed how the biochemical adherence tests can help determine if they are following the treatment correctly and are seen as valuable in confirming that the medication is working effectively. Participants reported that biofeedback about their MTX levels would be very beneficial even if it is normal as it can motivate them to stay on track with their current routine and make necessary adjustments if their levels drop. As well as reassurance, a MTX biochemical adherence test could provide participants with confidence. Participants appreciated that the results could confirm that the MTX is working for them. This helps them feel positive as they are following the given instructions.
Enhancing Patient Comprehension
Participants highlighted the need for providing information about the importance of blood tests in relation to MTX, as the blood tests itself can be frightening for a patient. This can prevent people from unnecessarily being alarmed if they are asked to have frequent blood tests. Patients commented that further information about the use of MTX and how it works can contribute to patients taking MTX more routinely.
Discussion
MTX is one of the first-line disease modifying anti-rheumatic drugs for RA but patients’ capabilities, opportunities and motivations for adhering to MTX have not been explored in the context of a biofeedback intervention. This research is the first to explore the patients’ perspectives of biofeedback to influence their adherence behaviours. Blood tests were found to play a potential important role in supporting adherence to MTX. Findings showed that blood test results can invoke a sense of fear and feelings of guilt (automatic motivation) as participants believe the tests could reveal to HCPs that they have not been adhering to their prescribed dose.
This fear arising from blood tests could be managed by HCPs reassuring patients that they will not be reprimanded for not adhering and instead emphasise a collaborative approach to address their concerns. On the other hand, blood tests also served as a source of reassurance and motivation. Our study found that normal or improved test results provided participants with confidence that they were taking their medication correctly, reinforcing their adherence behaviour (reflective motivation). Therefore, blood tests not only serve a clinical purpose but also act as a behavioural motivator for patients to maintain adherence if concerns around negative blood test results can be managed. This could also be an opportunity for HCPs to have a valuable social influence on the patient and encourage open discussions with them about their blood test results.
Some participants reflected on their motivations to take MTX, with a key driver being the desire to avoid returning to the disabling pain they experienced prior to receiving MTX which is in line with previous findings.23 In our study, HCPs reinforcing the risks of non-adherence with regard to pain levels had acted as a strong motivator to patients to adhere to their MTX dose. This aligns with the Necessity concerns framework24 which suggests that patients’ decisions to comply with medication rely on balancing the perceived necessity of taking the medication against concerns about its use. An example of this is seen in our findings as participants viewed MTX as essential for reducing pain but had also raised concerns regarding long-term side effects associated with prolonged use. Fear of long-term side effects have previously been linked to poor adherence to MTX.25 The knowledge of potential long-term side effects contributed to anxiety about adherence which in turn may lead to some participants reducing their dosage or stopping MTX altogether.26,27 Therefore, whilst MTX was considered necessary for pain management, concerns about its safety over time negatively impacted on adherence. Interventions should focus on balancing these opposing beliefs through structured communication and ongoing support.
Our findings underscore the critical role of communication HCPs play in promoting adherence to MTX. Study participants expressed a strong sense of trust in HCPs, especially when given administration instructions for their prescribed MTX dose (social opportunity). This trust is well supported by existing literature on the importance of HCPs in guiding medication use.28–30 However, our study highlighted that some patients felt they lacked the expertise to question or challenge the advice given by HCPs. As a result, they may adhere to their MTX dose without fully understanding potential side effects or how to manage them effectively.
Additionally, HCPs showing genuine interest and support to patients may further motivate them to adhere to their MTX regime. By demonstrating care and compassion, the HCPs can create a social opportunity to support patients in improving their adherence to MTX. This ongoing social support fosters a sense of being valued and allows the patient to be reflective on their motivations through encouragement by the HCP. This could lead to patients feeling more motivated to adhere to their prescribed MTX out of both appreciation for the support received from the HCP and the desire to maintain a positive relationship with them.
This aligns with findings from another study which examined adherence to rheumatic treatments such as adalimumab, where higher levels of perceived support from HCPs were associated with improved adherence.31 In other studies, looking at rheumatic diseases, it was found that patients who had a better therapeutic alliance with their clinician displayed better medication adherence.32–34 Therapeutic alliance refers to the collaborative relationship between the clinician and patient and can affect the patient’s attitude towards therapeutic outcomes such as medication adherence.35 This highlights the critical role clinicians have in order to achieve desired results and may lead to possible implications in staff training for HCPs on how to better collaborate with their patients when reviewing their MTX use.
Research shows that adherence relies on shared decision-making and these treatments cannot be implemented without prior discussion between HCPs and patients as HCPs would be the experts on the medical evidence whilst the patients are experts of living with RA.36,37
Healthcare professionals providing support in the form of education emerged as an important factor in promoting adherence. They highlighted the importance for a coherent understanding of what MTX is, how it works in relation to their RA and the consequences of non-adherence. The themes that emerged from this study suggest that patients who lack understanding may have increased anxiety about taking the prescribed medicine. To lessen this fear, patient education in the form of written or visual media could be provided to enhance understanding about MTX use. Our findings reflect previous research, which showed that non-adherent patients had a poor understanding of their disease,38 emphasising the need for good-quality patient education. Training programs aimed at enhancing HCPs communication skills may enable them to engage in more effective discussions about adherence, address patient concerns, and provide tailored support. Through open communication and actively supporting adherence efforts, HCPs may contribute to improved patient motivation and more consistent adherence to MTX.
These steps outline how to develop a biofeedback intervention that addresses key barriers and facilitators to adherence, while remaining cost-effective and avoiding additional burden for patients and healthcare professionals. The findings relating to healthcare professionals can translate directly into practice, and the APEASE criteria could allow us to consider whether these approaches are feasible and realistic. The APEASE criteria (Acceptability, Practicability, Effectiveness, Affordability, Side-effects and Equity) can be used to iteratively assess all stages of intervention design.39 The different aspects of the APEASE criteria can aid decisions about which behaviour change techniques, intervention functions and policy categories can be included in the initial stages of intervention development. Using these criteria alongside the COM-B model allows us to be systematic and account for context in the different intervention functions.40
We can start to investigate whether using targeted training session for HCPs is acceptable and practical for delivery especially if incorporated into existing training. This framework also encourages consideration of cost-effectiveness and potential unintended consequences. For example, additional or extended training sessions may require more of HCPs time, which could be difficult to accommodate and may affect the length or availability of clinical appointments. Similarly, incorporating structured discussions about blood test results and adherence during patient appointments may lead to longer consultation times, carrying further time and cost implications. These factors highlight the importance of evaluating not only the practicality of implementing the intervention but also its broader organisational impact. To understand the overall effectiveness, further investigation would be needed, such as gathering feedback from patients who have recently discussed their blood test results and adherence with an HCP. Interviews or surveys could help determine whether the training improves the quality of these conversations and ultimately supports better adherence. Finally, the intervention has the potential to enhance equity. We have identified a clear need for educational resources tailored to MTX adherence and patient capabilities. By ensuring these resources are co-created with diverse groups and offered in multiple accessible formats, the intervention can be delivered in a more inclusive and equitable way. There are several limitations of the study. All recruited participants were of White British ethnicity. This limits the diversity of the perspectives represented as previous research has shown that individuals from a White background self-report higher adherence compared to non-white patients with RA.41 Future research should include more heterogeneous samples to enhance the generalisability and inclusivity of this work.
Our cohort included individuals with a high level of education, and this is often found to be linked with high adherence to MTX.42 Adherence could be influenced by other factors such as ethnicity and socio-economic background and therefore a more diverse sample would be required to gain a deeper insight into reasons for non-adherence. We are unable to exclude selection bias from this study as the cohort of patients which we recruited may be more likely to adhere to their prescribed medication and may not accurately reflect the outlook of those who are non-adherent. Identifying specific individuals who are known to be non-adherent to MTX could provide us with a better context as to why patients do not comply with their prescribed dose. While this study provides insight into methotrexate adherence in RA, there is a potential for resource constraints which may influence the feasibility of implementing a biofeedback intervention based on the discussed evidence in clinical practice. This can include clinician workload and time pressures as HCPs may not have the availability to spend adequate time discussing biofeedback results and adherence with each patient.
Our study has important implications for practice. The themes were mapped onto COM-B constructs that could be incorporated as part of a biofeedback intervention (See Supplementary Table 3 for mapping process). Biochemical adherence blood tests provide a valuable opportunity for patients to assess their MTX adherence through offering a basis for reflection and discussion. Encouraging patients to engage with discussions of their blood test results may enhance their understanding of adherence and reinforce adherence-related behaviours. To support this, tailored informational resources can be developed to improve patients’ comprehension of their test results and the implications for medication adherence. These resources could strengthen adherence behaviours and can address overwhelming fears associated with MTX. Future research will focus on co-designing and piloting a COM-B–informed biofeedback intervention. Drawing on this study’s findings, we can develop an approach that incorporates blood tests to monitor MTX adherence and includes targeted training for healthcare professionals. Achieving this will require meaningful engagement with relevant stakeholders to ensure that both the intervention and training resources reflect the perspectives of patients and HCPs. Stakeholders can also provide valuable insights into preferred training formats and the economic considerations such as costs and potential benefits needed to offer decision makers a comprehensive assessment of feasibility.
Acknowledgment
The abstract of this paper was presented at the EULAR 2025: European Congress of Rheumatology as a conference abstract (publication only) with interim findings. The abstract was published in “Annals of Rheumatic Diseases” in The EULAR Journal: https://doi.org/10.1016/j.ard.2025.06.1637.
Funding
This study has been delivered through the National Institute for Health and Care Research (NIHR) Manchester Biomedical Research Centre (BRC) (NIHR203308). The views expressed are those of the author(s) and not necessarily those of the Manchester Academic Health Science Centre (MAHSC), the NIHR or the Department of Health and Social Care. This report includes independent research funded by the Manchester Academic Health Science Centre. The views expressed in this publication are those of the author(s) and not necessarily those of the NHS, or the Department of Health.
Disclosure
Armitage is supported by the NIHR Greater Manchester Patient Safety Research Collaboration. Hannah Shafi reports grants from Health Innovation Manchester, during the conduct of the study. Anne Barton reports grants from NIHR, grants from Health Innovation Manchester, during the conduct of the study. James Bluett reports grants from Health Innovation Manchester, during the conduct of the study. The authors report no other conflicts of interest in this work.
References
1. Symmons D. The prevalence of rheumatoid arthritis in the United Kingdom: new estimates for a new century. Rheumatology. 2002;41(7):793–16. doi:10.1093/rheumatology/41.7.793
2. Myasoedova E, Davis JM 3rd, Crowson CS, Gabriel SE. Epidemiology of rheumatoid arthritis: rheumatoid arthritis and mortality. Curr Rheumatol Rep. 2010;12(5):379–385. doi:10.1007/s11926-010-0117-y
3. Lard LR, Visser H, Speyer I, et al. Early versus delayed treatment in patients with recent-onset rheumatoid arthritis: comparison of two cohorts who received different treatment strategies. Am J Med. 2001;111(6):446–451. doi:10.1016/s0002-9343(01)00872-5
4. Gwinnutt JM, Symmons DPM, MacGregor AJ, et al. Twenty-year outcome and association between early treatment and mortality and disability in an inception cohort of patients with rheumatoid arthritis: results from the norfolk arthritis register. Arthritis Rheumatol. 2017;69(8):1566–1575. doi:10.1002/art.40090
5. Sherbini AA, Sharma SD, Gwinnutt JM, Hyrich KL, Verstappen SMM. Prevalence and predictors of adverse events with methotrexate mono- and combination-therapy for rheumatoid arthritis: a systematic review. Rheumatology. 2021;60(9):4001–4017. doi:10.1093/rheumatology/keab304
6. Sherbini AA, Gwinnutt JM, Hyrich KL, Adebajo RAMS, Ahmed K. Rates and predictors of methotrexate-related adverse events in patients with early rheumatoid arthritis: results from a nationwide UK study. Rheumatology. 2022;61(10):3930–3938. doi:10.1093/rheumatology/keab917
7. Hope HF, Bluett J, Barton A, Hyrich KL, Cordingley L, Verstappen SMM. Psychological factors predict adherence to methotrexate in rheumatoid arthritis; findings from a systematic review of rates, predictors and associations with patient-reported and clinical outcomes. RMD Open. 2016;2(1):e000171. doi:10.1136/rmdopen-2015-000171
8. Hope HF, Hyrich KL, Anderson J, et al. The predictors of and reasons for non-adherence in an observational cohort of patients with rheumatoid arthritis commencing methotrexate. Rheumatology. 2020;59(1):213–223. doi:10.1093/rheumatology/kez274
9. Lavielle M, Puyraimond-Zemmour D, Romand X, et al. Methods to improve medication adherence in patients with chronic inflammatory rheumatic diseases: a systematic literature review. RMD Open. 2018;4(2):e000684. doi:10.1136/rmdopen-2018-000684
10. Joplin S, van der Zwan R, Joshua F, Wong PKK. Medication adherence in patients with rheumatoid arthritis: the effect of patient education, health literacy, and musculoskeletal ultrasound. Biomed Res Int. 2015;2015:150658. doi:10.1155/2015/150658
11. Timmerman L, Stronks DL, Huygen FJPM. The design of a theory-based intervention to improve medication adherence in chronic pain patients. Curr Med Res Opin. 2017;33(7):1293–1301. doi:10.1080/03007995.2017.1314955
12. NICE. Medicines adherence: involving patients in decisions about prescribed medicines and supporting adherence (CG76). National Institute for Health and Care Excellence; 2009. Available from: https://www.nice.org.uk/Guidance/CG76.
13. Michie S, Atkins L, West R. The Behaviour Change Wheel: A Guide to Designing Interventions. Silverback Publishing; 2014.
14. Bluett J, Riba-Garcia I, Verstappen SMM, et al. Development and validation of a methotrexate adherence assay. Ann Rheum Dis. 2019;78(9):1192–1197. doi:10.1136/annrheumdis-2019-215446
15. Michie S, van Stralen MM, West R. The behaviour change wheel: a new method for characterising and designing behaviour change interventions. Implement Sci. 2011;6(1):42. doi:10.1186/1748-5908-6-42
16. Easthall C, Barnett N. Using theory to explore the determinants of medication adherence; moving away from a one-size-fits-all approach. Pharmacy. 2017;5(3):50. doi:10.3390/pharmacy5030050
17. Sergeant JC, Hyrich KL, Anderson J, et al. Prediction of primary non-response to methotrexate therapy using demographic, clinical and psychosocial variables: results from the UK rheumatoid arthritis medication study (RAMS). Arthritis Res Ther. 2018;20(1):147. doi:10.1186/s13075-018-1645-5
18. StataCorp. Stata Statistical Software: Release 12. StataCorp LP; 2011.
19. Francis JJ, Johnston M, Robertson C, et al. What is an adequate sample size? Operationalising data saturation for theory-based interview studies. Psychol Health. 2010;25(10):1229–1245. doi:10.1080/08870440903194015
20. Cane J, O’Connor D, Michie S. Validation of the theoretical domains framework for use in behaviour change and implementation research. Implement Sci. 2012;7(1):37. doi:10.1186/1748-5908-7-37
21. Ritchie J, Lewis J. Qualitative Research Practice: A Guide for Social Science Students and Researchers.
22. Dhakal K. NVivo. J Med Libr Assoc. 2022;110(2):270–272. doi:10.5195/jmla.2022.1271
23. de Thurah A, Nørgaard M, Harder I, Stengaard-Pedersen K. Compliance with methotrexate treatment in patients with rheumatoid arthritis: influence of patients’ beliefs about the medicine. A prospective cohort study. Rheumatol Int. 2010;30(11):1441–1448. doi:10.1007/s00296-009-1160-8
24. Horne R, Weinman J. Patients’ beliefs about prescribed medicines and their role in adherence to treatment in chronic physical illness. J Psychosom Res. 1999;47(6):555–567. doi:10.1016/s0022-3999(99)00057-4
25. DiBenedetti DB, Zhou X, Reynolds M, Ogale S, Best JH. Assessing methotrexate adherence in rheumatoid arthritis: a cross-sectional survey. Rheumatol Ther. 2015;2(1):73–84. doi:10.1007/s40744-015-0011-1
26. Hayden C, Neame R, Tarrant C. Patients’ adherence-related beliefs about methotrexate: a qualitative study of the role of written patient information. BMJ Open. 2015;5(5):e006918. doi:10.1136/bmjopen-2014-006918
27. Nagafuchi H, Goto Y, Kiyokawa T, Kawahata K. Reasons for discontinuation of methotrexate in the treatment of rheumatoid arthritis and challenges of methotrexate resumption: a single-center, retrospective study. Egypt Rheumatol Rehabil. 2022;49(1). doi:10.1186/s43166-022-00162-w
28. Kelly A, Tymms K, Tunnicliffe DJ, et al. Patients’ attitudes and experiences of disease-modifying antirheumatic drugs in rheumatoid arthritis and spondyloarthritis: a qualitative synthesis. Arthritis Care Res. 2018;70(4):525–532. doi:10.1002/acr.23329
29. Haag H, Liang T, Avina-Zubieta JA, De Vera MA. How do patients with systemic autoimmune rheumatic disease perceive the use of their medications: a systematic review and thematic synthesis of qualitative research. BMC Rheumatol. 2018;2(1):9. doi:10.1186/s41927-018-0017-8
30. Rai SK, Howren A, Wilcox ES, et al. Exploring strategies to support medication adherence in patients with inflammatory arthritis: a patient-oriented qualitative study using an interactive focus group activity. Patient Prefer Adherence. 2018;12:2015–2025. doi:10.2147/PPA.S174672
31. Morgan C, McBeth J, Cordingley L, et al. The influence of behavioural and psychological factors on medication adherence over time in rheumatoid arthritis patients: a study in the biologics era. Rheumatology. 2015;54(10):1780–1791. doi:10.1093/rheumatology/kev105
32. Yfantopoulos J, Protopapa M, Mantalias K, et al. Patients’ and doctors’ beliefs about treatment and long-term adherence in rheumatic diseases. Mediterr J Rheumatol. 2020;31(Suppl 1):152–162. doi:10.31138/mjr.31.1.152
33. Bennett JK, Fuertes JN, Keitel M, Phillips R. The role of patient attachment and working alliance on patient adherence, satisfaction, and health-related quality of life in lupus treatment. Patient Educ Couns. 2011;85(1):53–59. doi:10.1016/j.pec.2010.08.005
34. Lohse A, Lemelle I, Pillet P, et al. Therapeutic alliance is associated to treatment adherence in children with juvenile idiopathic arthritis. Joint Bone Spine. 2021;88(4):105151. doi:10.1016/j.jbspin.2021.105151
35. Hausner RS. The therapeutic and working alliances. J Ame Psychoanaly Assoc. 2000;48(1):155–187. doi:10.1177/00030651000480011001
36. Spatz ES, Krumholz HM, Moulton BW. Prime time for shared decision making. JAMA. 2017;317(13):1309–1310. doi:10.1001/jama.2017.0616
37. Ritschl V, Stamm TA, Aletaha D, et al. Prevention, screening, assessing and managing of non-adherent behaviour in people with rheumatic and musculoskeletal diseases: systematic reviews informing the 2020 EULAR points to consider. RMD Open. 2020;6(3):e001432. doi:10.1136/rmdopen-2020-001432
38. Raghunath S, Hijjawi R, Hoon E, Shanahan EM, Goldblatt F. Qualitative assessment of medication adherence in patients with rheumatic diseases on biologic therapy. Clin Rheumatol. 2019;38(10):2699–2707. doi:10.1007/s10067-019-04609-y
39. Public Health England. Achieving behaviour change a guide for local government and partners. Public Health England; 2019. Available from: https://assets.publishing.service.gov.uk/government/uploads/system/uploads/attachment_data/file/875385/PHEBI_Achieving_Behaviour_Change_Local_Government.pdf.
40. Atkins L, Michie S. Designing interventions to change eating behaviours. Proc Nutr Soc. 2015;74(2):164–170. doi:10.1017/S0029665115000075
41. Salt E, Frazier SK. Predictors of medication adherence in patients with rheumatoid arthritis. Drug Dev Res. 2011;72(8):756–763. doi:10.1002/ddr.20484
42. Yajima N, Kawaguchi T, Takahashi R, et al. Adherence to methotrexate and associated factors considering social desirability in patients with rheumatoid arthritis: a multicenter cross-sectional study. BMC Rheumatol. 2022;6(1):75. doi:10.1186/s41927-022-00305-8
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.