Back to Journals » Nature and Science of Sleep » Volume 13
Development and Validation of Nomogram Prediction Model for Postoperative Sleep Disturbance in Patients Undergoing Non-Cardiac Surgery: A Prospective Cohort Study
Authors Yang S, Zhang Q, Xu Y, Chen F, Shen F, Zhang Q, Liu H ![]() , Zhang Y
, Zhang Y
Received 15 May 2021
Accepted for publication 28 July 2021
Published 24 August 2021 Volume 2021:13 Pages 1473—1483
DOI https://doi.org/10.2147/NSS.S319339
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Prof. Dr. Ahmed BaHammam
Shuting Yang,1 Qian Zhang,1 Yifan Xu,1 Futeng Chen,1 Fangming Shen,1 Qin Zhang,1 He Liu,2 Yueying Zhang3
1Xuzhou Medical University, Xuzhou City, Jiangsu Province, People’s Republic of China; 2Department of Anesthesiology, The Affiliated Huzhou Hospital, Zhejiang University School of Medicine; Huzhou Central Hospital, Huzhou City, Zhejiang Province, People’s Republic of China; 3Department of Anesthesiology, The Affiliated Hospital of Xuzhou Medical University, Xuzhou City, Jiangsu Province, People’s Republic of China
Correspondence: Yueying Zhang
Department of Anesthesiology, The Affiliated Hospital of Xuzhou Medical University, Xuzhou City, Jiangsu Province, People’s Republic of China
Tel +86 138 1531 0789
Email [email protected]
Purpose: To develop a risk prediction nomogram of postoperative sleep disturbance (PSD) in patients undergoing non-cardiac surgery.
Patients and methods: Data on 881 consecutive patients who underwent non-cardiac surgery at the Affiliated Hospital of Xuzhou Medical University between June 2020 and April 2021 were prospectively collected. Of these, we randomly divided 881 non-cardiac patients into two groups, training cohort (n = 617) and validation cohort (n = 264) at the ratio of 7:3. Characteristic variables were selected based on the data of training cohort through least absolute shrinkage and selection operator (LASSO) regression. Multivariate logistic regression was used to identify the independent risk factors associated with PSD that then were incorporated into the nomogram. The predictive performance of the nomogram was measured by concordance index (C index), receiver operating characteristic (ROC) curve, and calibration with 1000 bootstrap samples to decrease the over-fit bias.
Results: PSD was found in 443 of 617 patients (71.8%) and 190 of 264 patients (72.0%) in the training and validation cohorts, respectively. The perioperative risk factors associated with PSD were female sex, anxiety, dissatisfaction of ward environment, absence of combined regional nerve block, postoperative nausea and vomiting (PONV), the longer duration stayed in post anesthesia care unit (PACU), the higher dose of midazolam and sufentanil, the higher postoperative numeric rating score for pain (NRS) score. Incorporating these 9 factors, the nomogram achieved good concordance indexes of 0.82 (95% confidence interval [CI], 0.78– 0.85) and 0.80 (95% CI, 0.74– 0.85) in predicting PSD in the training and validation cohorts, respectively, and obtained well-fitted calibration curves. The sensitivity and specificity (95% CIs) of the nomogram were calculated, resulting in sensitivity of 74.0% (70.0– 78.2%) and 75.3% (68.4– 81.7%) and specificity of 79.3% (72.5– 85.2%) and 70.3% (58.4– 80.7%) for the training and validation cohorts, respectively. Patients who had a nomogram score of less than 262 or 262 or greater were considered to have low or high risks of PSD presence, respectively.
Conclusion: The proposed nomogram achieved an optimal prediction of PSD in patients undergoing non-cardiac surgery. The risks for an individual patient to harbor PSD can be determined by this model, which can lead to a reasonable preventive and treatment measures.
Keywords: postoperative sleep disturbance, surgery, LASSO regression analysis, nomogram
A Letter to the Editor has been published for this article.
Introduction
In recent years, with the development of comfortable medical concept, and the growth of people’s demand for health level, sleep disturbance has evoked much attention than before. PSD is a common postoperative complication and patients may report decreased sleep time, increased numbers of arousals or awakening, frequent nightmares, fragmented sleep and lowered sleep quality after operation.1 In previous studies, the prevalence of PSD was 65.7%, and even up to approximately 95% in severe cases.2,3 About 25% of the patients reported lack of sleep again on the 15th day after surgery, and 24% of them needed medication to correct sleep disturbance.4 10–61% of the patients even had sleep problems over 6 months after discharge, which seriously affected the long-term recovery.5 Moreover, PSD are associated with the development of episodic hypoxemia, hemodynamic instability, early postoperative fatigue, cognitive impairment, pain sensitivity and mood disturbances, all with a potential adverse effect on postoperative outcome.6,7
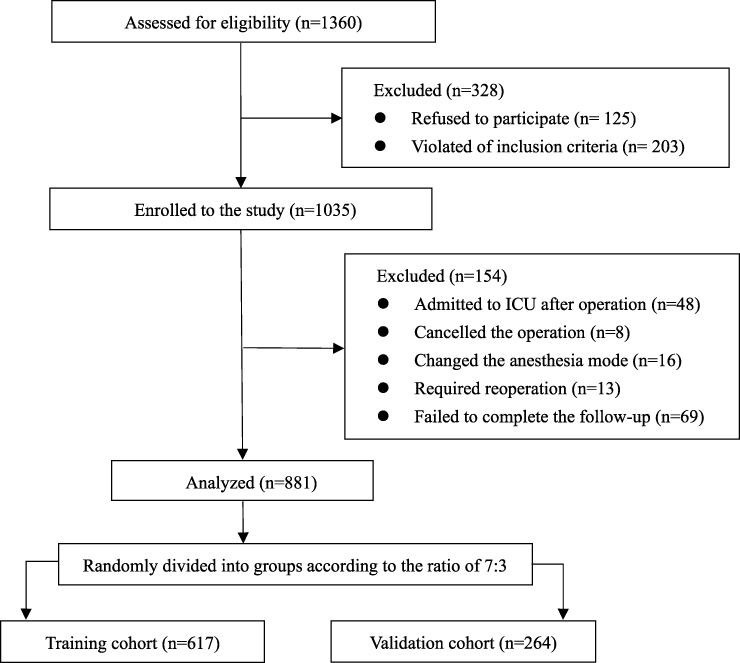 |
Figure 1 Flow chart of patients screening and recruitment. |
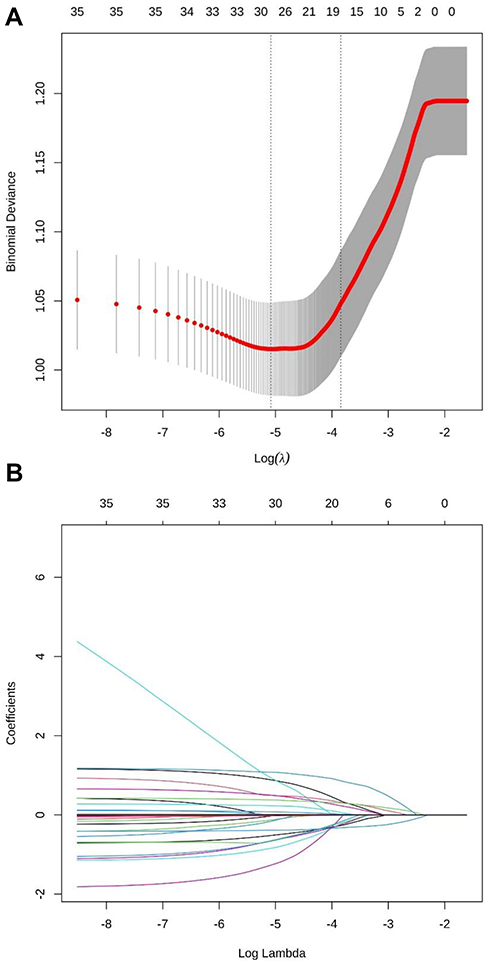 |
Figure 2 Demographic and clinical feature selection using the Least Absolute Shrinkage and Selection Operator (LASSO) regression. (A) The selection of the tuning parameter (lambda) in the LASSO model used 5-fold cross-validation with the minimum criteria. The relationship curve between partial likelihood deviation (binomial deviation) and log(lambda) was plotted. Dotted vertical lines were drawn at the optimal values by using the minimum criteria and the 1 standard error (SE) of the minimum criteria (the 1-SE criteria). (B) LASSO coefficient profiles of the 16 features. A coefficient profile plot was produced against the log(lambda) sequence. Vertical line was drawn at the value selected using 5-fold cross-validation, where optimal lambda resulted in 16 features with non-zero coefficients. |
 |
Figure 3 Nomogram for perioperative estimation of PSD risk. To use the nomogram, find the position of each variable on the corresponding axis, draw a line to the points axis for the number of points, add the points from all of the variables, and draw a line from the total points axis to determine the PSD probabilities at the lower line of the nomogram. |
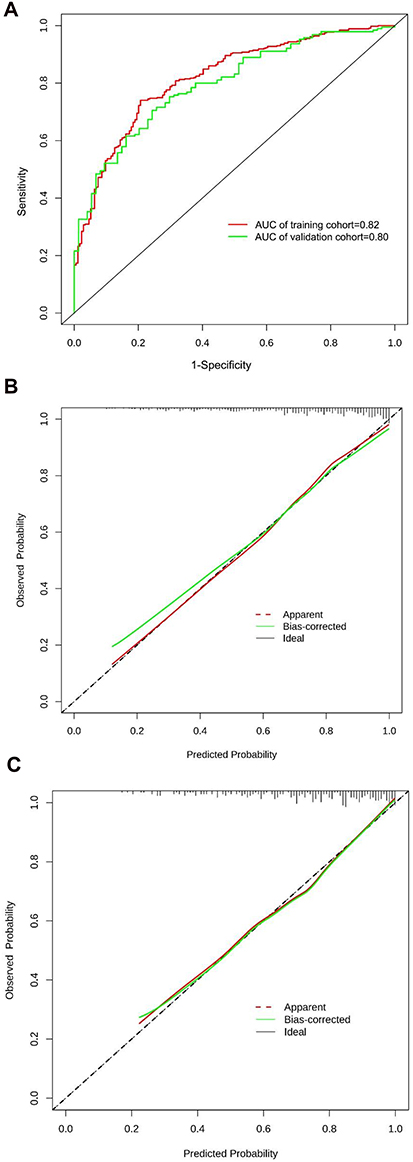 |
Figure 4 The predictive performance of PSD risk nomogram. (A) The receiver operating characteristic (ROC) curve was compared between training cohort and validation cohort. The area under the curve (AUC) of training cohort and validation cohort were 0.82 and 0.80, respectively. (B) Validity of the predictive performance of the nomogram in estimating the risk of PSD presence in the training cohort (n = 617). (C) Validity of the predictive performance of the nomogram in estimating the risk of PSD presence in the validation cohort (n = 264). |
The mechanisms leading to sleep disturbance in patients are complex, with relevance to the environmental, pharmaceutical and medical factors, such as surgical inflammatory response, severity of surgery, type of anesthesia, pain, anxiety, as well as their interactions.6,8,9 While PSD itself is well recognized, perioperative management of patients is a relatively neglected field of research. Currently, the treatment strategies for PSD include dexmedetomidine, zolpidem, melatonin, enhanced recovery after surgery (ERAS) protocol and improving of ward environment.10,11 However, these research perspectives of sleep disturbance during perioperative period were emphasizing intervention rather than focusing on risk prediction, especially the clinical modifiable risks.
Medical staff should pay attention to the prevention of sleep problems in patients.12 The aim of the present study was to investigate risk factors of PSD, and develop a prediction model for the accurate prediction of PSD in patients undergoing non-cardiac surgery.
Patients and Methods
This is a prospective cohort study, which has been approved by the Research Ethics Committee of the Affiliated Hospital of Xuzhou Medical University (Xuzhou city, Jiangsu province, China) on 28 May (XYFY2020-KL057-01) and registered in the Chinese Clinical Trial Registry (ChiCTR1900024172). Written informed consent was obtained from all study participants before the operation.
Participants
From June 2020 to April 2021, data on consecutive patients who underwent non-cardiac surgery were prospectively collected at the Affiliated Hospital of Xuzhou Medical University.
The study had the following inclusion criteria: (1) Chinese-speaking patients aged ≥18 years with the ability to provide informed consent, scheduled for elective non-cardiac surgical under general anesthesia; (2) American Society of Anesthesiologists physical status classification (ASA) grade I–III. Patients were excluded if they: (1) had preoperative sleep disorders [Pittsburgh Sleep Quality Index (PSQI) score > 7]; (2) received brain surgery; (3) received daytime surgery; (4) had cognitive dysfunction, psychiatric disease, or motor dysfunction; (5) had long time use of sedatives, antidepressants, drugs or alcohol dependence. Patients were eliminated if they: (1) admitted to intensive care unit (ICU) after surgery; (2) cancelled the operation; (3) changed the anesthesia method; (4) required reoperation; (5) failed to complete the follow-up.
Clinical Variables
Potential predictive factors were filtrated based on the literature and clinical practice. Preoperative variables included demographics [sex, age, body mass index (BMI), educational level, alcohol or smoking consumption], past medical history [obstructive sleep apnea hypopnea syndrome (OSAHS), hypertension, diabetes mellitus, anxiety, depression, sleep disorders], NRS score, ASA grade, satisfaction of ward environment, preoperative hospital stay. Intraoperative variables included anesthesia method, operation method, operation time, anesthesia time, amount of fluid infusion and blood loss, urine volume. Postoperative variables included the duration stayed in PACU, the use of patient-controlled intravenous analgesia (PCIA), post-surgical complications (fever, hypoxemia, hypotension, PONV), postoperative NRS score, postoperative hospital stay.
Clinical data were collected continuously during hospital stay and at the follow-up visit 1 week postoperatively. Communication methods between the researchers and patients included face-to-face and telephone contacts. The average score of postoperative NRS for three consecutive days was defined as the postoperative NRS score in this study.
Development and Internal Validation Population
With the aid of R software (version 3.6.2; https://www.R-project.org), a total of 881 patients were enrolled in total and were separated randomly into training cohort (n=617) and validation cohort (n=264) at a theoretical ratio of 7:3.
Evaluation of Sleep Disturbance
Sleep quality was assessed using the PSQI, a well-validated self-report questionnaire designed to assist in the diagnosis of sleep disorders.13 The PSQI has 7 components including sleep latency, sleep duration, habitual sleep efficiency, sleep disturbances, daytime dysfunction, and hypnotic drugs which range 0–3, respectively. The global PSQI score ranging from 0 to 21 is generated by summing up all the seven component scores, where 0 indicates no difficulty and 21 is severe difficulty in all areas. A global cut-off score of PSQI greater than 7 is used to distinguish poor sleepers from good sleepers. In this study, experienced investigators used PSQI questionnaire to evaluate the sleep quality of non-cardiac patients before and 1 week after the operation.
Statistical Analysis
For the normal distribution data, the data were expressed as mean ± standard deviation (SD) and compared using the independent sample t-test. For the categorical data, the data were presented as number and percentages, and compared using the Chi-square test or Fisher’s exact test.
LASSO regression and multivariate logistic regression analysis were utilized to filter possible indicators in the training cohort. Non-zero characteristic factors selected through LASSO analysis were put into the multivariate logistic regression analysis to identify the independent risk factors associated with PSD. A nomogram was formulated based on the results of multivariate logistic regression analysis by using the rms package of R software. The backward stepdown process based on the Akaike information criterion (AIC) was used to control the over-fitting of the model. The predictive performance of the nomogram was measured by C index, ROC curve and calibration with 1000 bootstrap samples to decrease the over-fit bias based on the data from training cohort and validation cohort.14
For clinical use of the model, the total points of each patient were calculated based on the proposed nomogram. ROC curve analysis was used to calculate the optimal cutoff values that were determined by maximizing the Youden index. Accuracy of the optimal cutoff value was assessed by the sensitivity, specificity, predictive values, and likelihood ratios.
Statistical analysis was performed with R software (version 3.6.2; https://www.R-project.org). The reported statistical significance levels were all two-sided, with statistical significance set at 0.05.
Results
Participant Characteristics
We initially assessed 1360 patients for eligibility to participate in our study (Figure 1). Of these, 125 patients refused to participate, 203 patients did not meet the inclusion criteria and the remaining 1035 patients enrolled to the study. Following the completion of the study, 154 patients were excluded from the study: 48 patients admitted to ICU after operation, 8 patients cancelled the operation, 16 patients changed the anesthesia mode, 13 patients required reoperation, 69 patients failed to complete the follow-up. Finally, the data of 881 patients were analyzed in the present study. The training cohort composed of 617 patients. The average age was 54.62±12.91 years, 41.3% were male and 71.8% had PSD. The validation cohort consisted of 264 patients. The average age was 54.53±14.30 years, 42.8% were male and 72.0% had PSD. The prevalence of PSD among all patients was 71.9%. All characteristics were no statistically significant differences between training cohort and validation cohort (all P > 0.05) (Table 1).
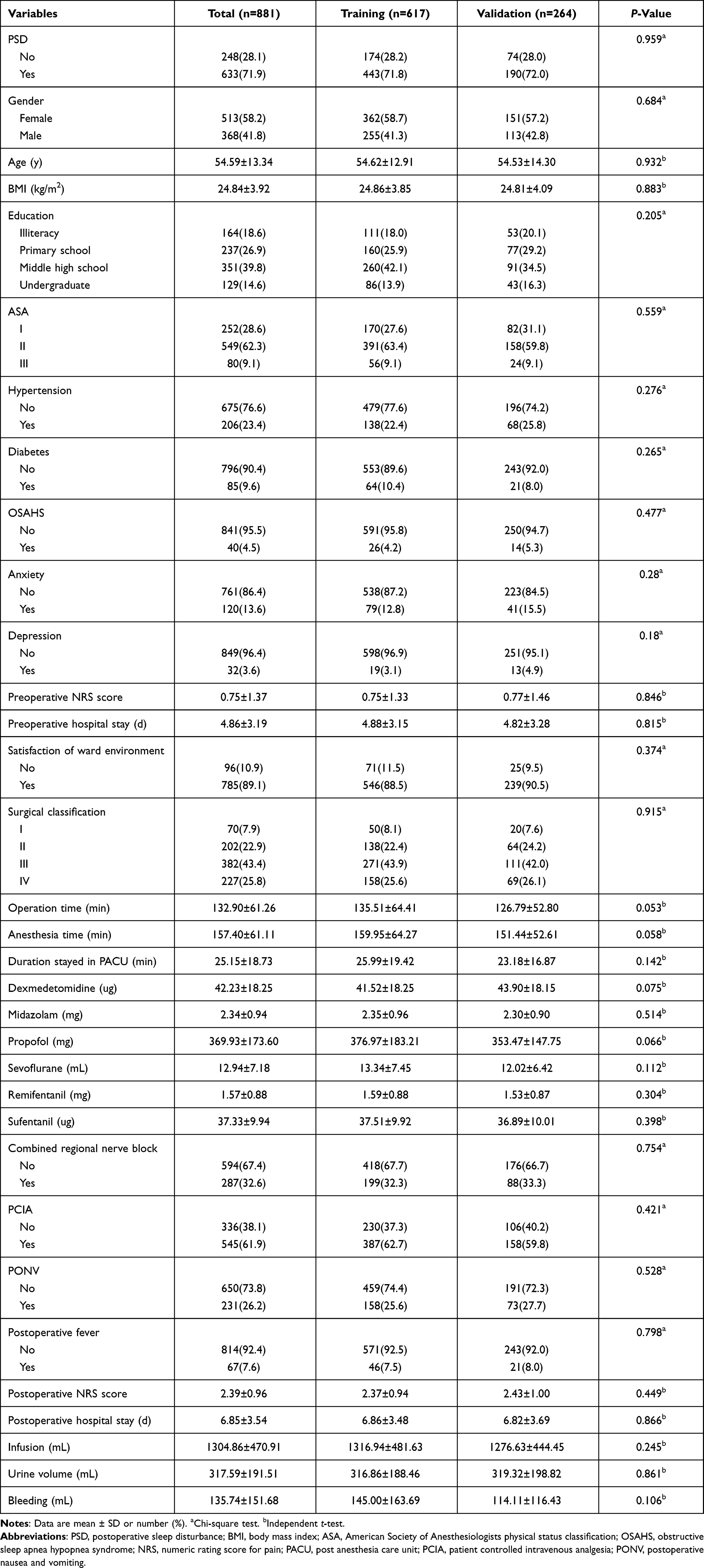 |
Table 1 Participant Characteristics |
Construction of Prediction Model in the Training Cohort
Thirty-two potential risk factors from perioperative clinical indicators were included in the LASSO regression analysis (Figure 2A and B). We selected 16 non-zero characteristic variables including gender, ASA, hypertension, anxiety, satisfaction of ward environment, surgical classification, combined regional nerve block, PCIA, PONV, duration stayed in PACU, dexmedetomidine, midazolam, sufentanil, postoperative NRS score, postoperative hospital stay, infusion (Table 2).
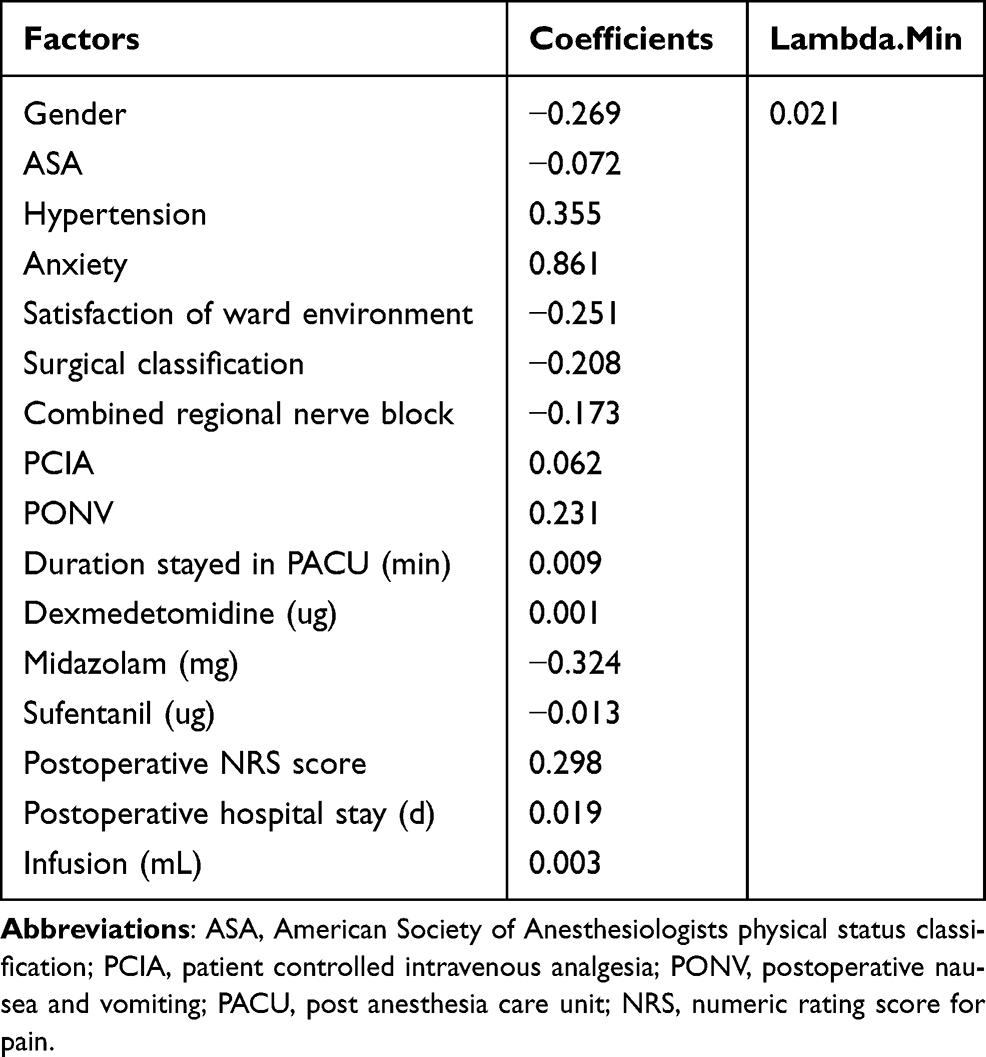 |
Table 2 Coefficients and Lambda.Min Value of the LASSO Regression |
The results of multivariate logistic analysis are presented in Table 3. On multivariate analysis, with results reported as odds ratio (95% CI), male sex [0.54(0.32–0.88)], anxiety [4.69(1.83–14.64)], satisfaction of ward environment [0.38(0.17–0.80)], combined regional nerve block [0.46(0.28–0.75)], PONV [1.92(1.11–3.41)], the longer duration stayed in PACU [1.02(1.01–1.03)], the higher dose of midazolam [0.62(0.49–0.79)] and sufentanil [0.97(0.95–0.99)], the higher postoperative NRS score [1.59(1.23–2.07)] were independently associated with PSD.
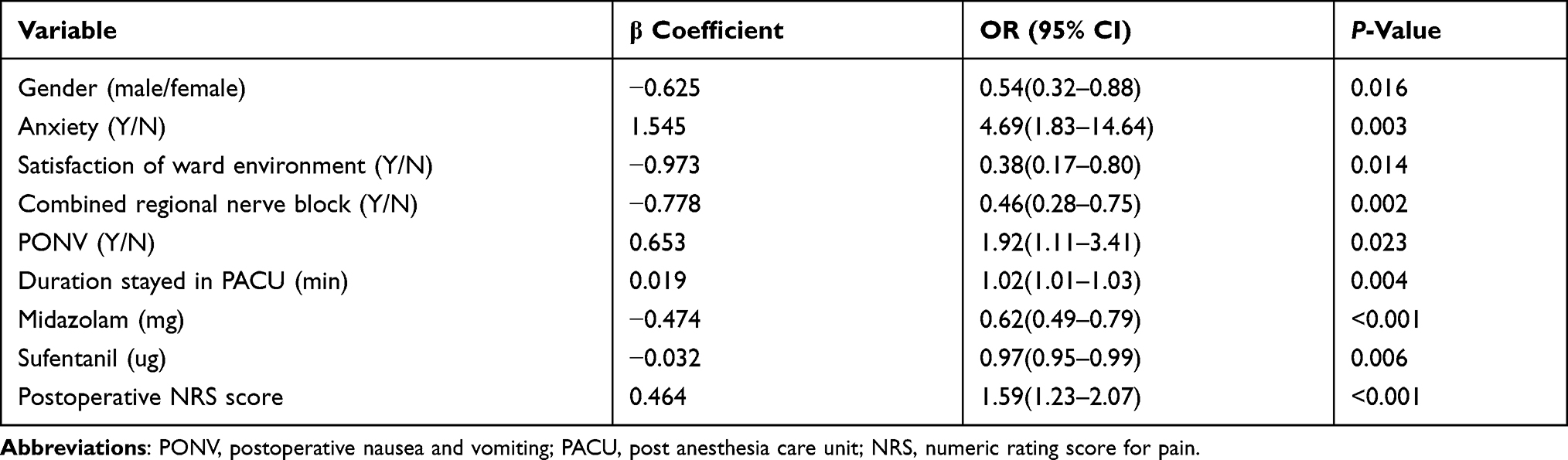 |
Table 3 Multivariate Logistic Regression Analysis of PSD Presence Based on Perioperative Data in the Training Cohort |
Development and Validation of the PSD-Predicting Nomogram
These independently associated risk factors were used to build a PSD risk prediction model (Figure 3). The resulting model was internally validated using the bootstrap validation method. The nomogram showed good accuracy in estimating the risk of PSD, with an unadjusted C index of 0.82 (95% CI, 0.78–0.85) and a bootstrap-corrected C index of 0.79 (Figure 4A). Besides, the calibration plots graphically demonstrated good agreement on the presence of PSD between the risk estimation by the nomogram and analysis results of actual clinical data (Figure 4B). In the validation cohort, the nomogram displayed an unadjusted C index of 0.80 (95% CI, 0.74–0.85) and a bootstrap-corrected C index of 0.80 for the estimation of PSD risk (Figure 4A). There was also a good calibration curve for the risk estimation (Figure 4C).
Risk of PSD Based on the Nomogram Scores
The optimal cutoff value of the total nomogram scores was determined to be 262. The sensitivity, specificity, positive predictive value, and negative predictive value when used in differentiating the presence from absence of PSD were 74.0%, 79.3%, 90.1%, and 54.5% in the training cohort, and 75.3%, 70.3%, 86.7%, and 52.5% in the validation cohort, respectively (Table 4).
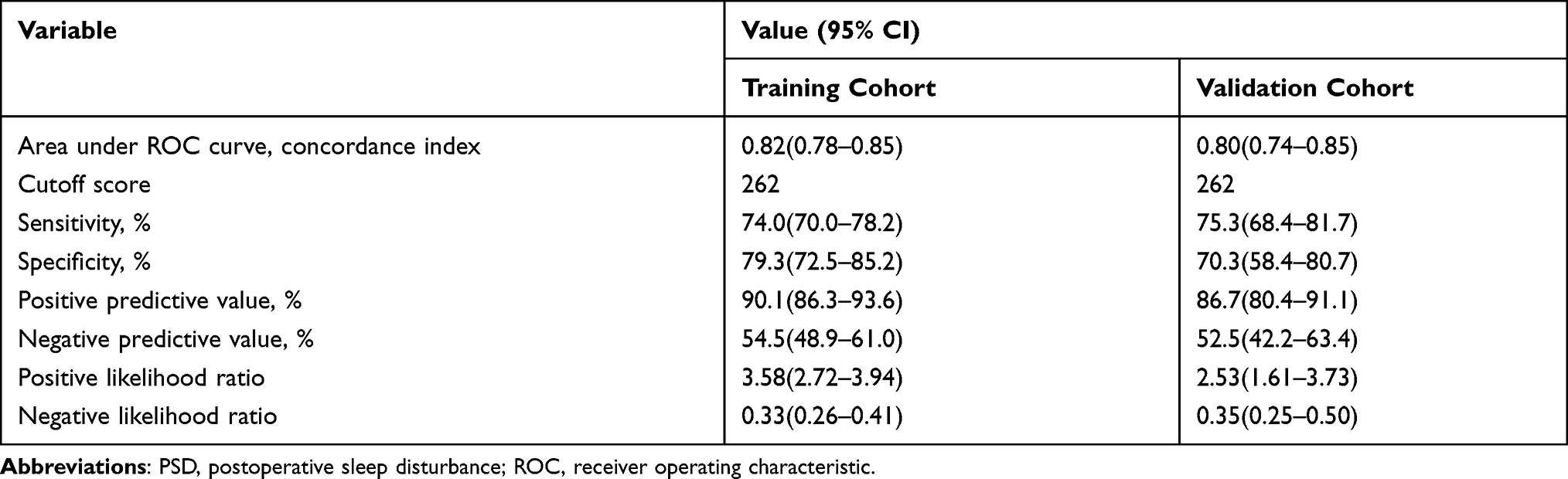 |
Table 4 Accuracy of the Prediction Score of the Nomogram for Estimating the Risk of PSD Presence |
Discussion
Of the currently available prediction tools, the nomogram is a superior visual tool with the user-friendly display, easily understand, high accuracy and good discrimination characteristics in predicting results.15–17 Here, we generated and validated a novel nomogram to accurately forecast PSD risk in non-cardiac surgery patients. As far as we know, this is the first attempt to predict PSD in non-cardiac surgery patients. The proposed nomogram, which incorporated 9 comprehensive and easily available perioperative variables: gender, anxiety, satisfaction of ward environment, combined regional nerve block, PONV, the duration stayed in PACU, midazolam, sufentanil and the postoperative NRS score, performed well as supported by the C index values of 0.82 and 0.80 in the training and validation cohorts, respectively, and the optimal calibration curves demonstrating the agreements between prediction and actual observation.
In the PSD risk estimation nomogram, pain, absence of combined regional nerve block, anxiety, PONV and dissatisfaction of ward environment have been reported to increase the possibility of sleep disturbance.18–26 Our study demonstrated that these factors were also significantly associated with PSD in non-cardiac surgery patients. In addition, we demonstrated that female sex, the longer duration stayed in PACU, and the lower dose of midazolam were associated with an increased probability of PSD in non-cardiac surgery patients.
Midazolam is a short-acting water-soluble benzodiazepine sedative. Midazolam produces sedative, hypnotic, anticonvulsant, and anxiolytic effects by altering the configuration of the GABAA receptor complex and opening the chloride channel. The effect of antegrade amnesia, combined with opioids, etomidate, propofol drugs can produce synergistic or additive effects, resulting in analgesic effect.27,28 Previous studies have found that midazolam could shorten sleep latency, reduce wakefulness frequency, improve objective sleep evaluation and reduce daytime sleepiness.29 However, some scholars have also pointed out that long-term application of benzodiazepines could lead to an increase of shallow sleep and increased risk of adverse effects such as cognitive impairment and falling, especially in the elderly.22,30 Despite dexmedetomidine showed the characteristic of a potential protective effect on sleep, this effect did not occur in our study.18 Therefore, it is necessary to find a balance between clinical treatment and sleep.
Although the incidence of PSD was higher in women than in men, the reasons for this gender difference were not clear. A possible explanation about the gender difference is the fact that women have higher rates of both acute and chronic insomnia than men from general population studies regardless the setting.31,32 Stein et al reported that in the general population, women suffer insomnia at higher rates than men and onset is often associated with physical problems of aging.33 These issues deserve further investigation, ideally with longitudinal or experimental study designs to establish the direction of the effects amongst gender, age, sleep disorders and surgery. In most instances, an extended PACU stay from anesthesia was attributed to longer anesthetic exposure and bigger surgical trauma. Residual anesthetic, analgesic medications and surgical trauma could potentially lead to worse sleep quality of patients.34
With higher degree of internal homogeneity, overall consistency and clinical validity than any other test available, the PSQI originally described by Buysse in 1989, has become the main tool for the assessment of quality of sleep.13 Generally speaking, the reporting period of PSQI is 1 month, but the PSQI was used for short-term evaluation for 1 week in this study. Broderick et al once had evaluated the accuracy of PSQI across different lengths of reporting periods (3-, 7- and 28-days). They found there was no significant difference in item scores when electronic daily ratings were compared with recall ratings regardless of the length of the reporting period.35 In addition, some previously studies investigated the short-term sleep quality using PSQI.36–38 Therefore, PSQI can be also administered confidingly for weeklong reporting periods between subject analyses.
LASSO regression is a popular method for variable selection in fitting high-dimension generalized linear model, which can obtain a more refined model by constructing a penalty function to reduce the variable numbers and effectively avoid overfitting.39,40 Therefore, we applied the LASSO regression for feature selection and build prediction model in this study.
The nomogram we proposed has several advantages. The selected variables were common and easy to obtain from clinical practice, helping the perioperative management of surgeon. The scoring system of nomogram was simple and comprehensible which achieved good predictive accuracy and favorable stability. By producing an accurate prognosis, this nomogram could help surgeons to stratify patients and make individual clinical treatment strategies under variable conditions.
However, there were still some limitations in the present study. First, this analysis was based on data from a single institution, it is necessary to validate the results from other centers. Second, the risk factors of PSD are complex and there are far more factors to be investigated and used to predict the prognosis of PSD. Third, the follow-up duration was relatively short, and a large prospective study with a long-term follow-up should be performed in the future. Thus, the accuracy of this prediction model will be improved to a certain extent.
Conclusion
In short, this study constructed a predictive model which was presented as nomogram to quantify the risk of PSD in non-cardiac surgery patients. The nomogram showed a powerful predictive ability and could help clinicians make better therapeutic strategy.
Abbreviations
AIC, Akaike information criterion; ASA, American Society of Anesthesiologists physical status classification; BMI, body mass index; CI, confidence interval; C index, concordance index; ERAS, enhanced recovery after surgery; ICU, intensive care unit; LASSO, least absolute shrinkage and selection operator; OSAHS, obstructive sleep apnea-hypopnea syndrome; PACU, post-anesthesia care unit; PCIA, patient controlled intravenous analgesia; PONV, postoperative nausea and vomiting; PSD, postoperative sleep disturbance; PSQI, Pittsburgh Sleep Quality Index; ROC, receiver operating characteristic curve; SD, standard deviation.
Data Sharing Statement
The data sets used and analyzed in this study are available from the corresponding author upon reasonable request.
Ethics Approval and Informed Consent
The study has been approved by the Research Ethics Committee of Affiliated hospital of Xuzhou Medical University (Xuzhou, Jiangsu, People’s Republic of China) on 28 May (XYFY2020-KL057-01). In conformation with the Declaration of Helsinki, every patient or patient’s legally authorized representative provided written informed consent before entering the trial.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Su X, Wang DX. Improve postoperative sleep: what can we do? Curr Opin Anaesthesiol. 2018;31(1):83–88. doi:10.1097/ACO.0000000000000538
2. Dette F, Cassel W, Urban F, et al. Occurrence of rapid eye movement sleep deprivation after surgery under regional anesthesia. Anesth Analg. 2013;116(4):939–943. doi:10.1213/ANE.0b013e3182860e58
3. Ghorbani A, Hajizadeh F, Sheykhi MR, et al. The effects of deep-breathing exercises on postoperative sleep duration and quality in patients undergoing Coronary Artery Bypass Graft (CABG): a randomized clinical trial. J Caring Sci. 2018;8(4):219–224. doi:10.15171/jcs.2019.031
4. Kain ZN, Caldwell-Andrews AA. Sleeping characteristics of adults undergoing outpatient elective surgery: a cohort study. J Clin Anesth. 2003;15(7):505–509. doi:10.1016/j.jclinane.2003.02.002
5. Altman MT, Knauert MP, Pisani MA. Sleep disturbance after hospitalization and critical illness: a systematic review. Ann Am Thorac Soc. 2017;14(9):1457–1468. doi:10.1513/AnnalsATS.201702-148SR
6. Rampes S, Ma K, Divecha YA, et al. Postoperative sleep disorders and their potential impacts on surgical outcomes. J Biomed Res. 2019;34(4):271–280. doi:10.7555/JBR.33.20190054
7. Eloy JD, Anthony C, Amin S, et al. Gabapentin does not appear to improve postoperative pain and sleep patterns in patients who concomitantly receive regional anesthesia for lower extremity orthopedic surgery: a randomized control trial. Pain Res Manag. 2017;2017:2310382. doi:10.1155/2017/2310382
8. Li Y, Zhao L, Yang C, et al. Development and validation of a clinical prediction model for sleep disorders in the ICU: a Retrospective Cohort Study. Front Neurosci. 2021;15:644845. doi:10.3389/fnins.2021.644845
9. Song B, Li Y, Teng X, et al. The effect of intraoperative use of dexmedetomidine during the daytime operation vs the nighttime operation on postoperative sleep quality and pain under general anesthesia. Nat Sci Sleep. 2019;11:207–215. doi:10.2147/NSS.S225041
10. Rosenberg J. Sleep disturbances after non-cardiac surgery. Sleep Med Rev. 2001;5(2):129–137. doi:10.1053/smrv.2000.0121
11. Hillman DR. Postoperative sleep disturbances: understanding and emerging therapies. Adv Anesth. 2017;35(1):1–24. doi:10.1016/j.aan.2017.07.001
12. Devlin JW, Skrobik Y, Gélinas C, et al. Clinical practice guidelines for the prevention and management of pain, agitation/ sedation, delirium, immobility, and sleep disruption in adult patients in the ICU. Crit Care Med. 2018;46(9):e825–e873. doi:10.1097/CCM.0000000000003299
13. Buysse DJ, Reynolds CF
14. Steyerberg EW, Vergouwe Y. Towards better clinical prediction models: seven steps for development and an ABCD for validation. Eur Heart J. 2014;35(29):1925–1931. doi:10.1093/eurheartj/ehu207
15. Du X, Guo CN, Bao XD. A powerful nomogram based on the novel D-index to predict prognosis after surgical resection of hepatocellular carcinoma. Cancer Manag Res. 2021;13:2581–2594. doi:10.2147/CMAR.S305253
16. Zou W, Xu NL. Development and internal validation of a nomogram used to predict chemotherapy-induced neutropenia in non-small cell lung cancer patients: a Retrospective Cohort Study. Cancer Manag Res. 2021;13:2797–2804. doi:10.2147/CMAR.S302722
17. Huang YQ, Liang CH, He L, et al. Development and validation of a radiomics nomogram for preoperative prediction of lymph node metastasis in colorectal cancer. J Clin Oncol. 2016;34(18):2157–2164. doi:10.1200/JCO.2015.65.9128
18. Okifuji A, Hare BD. Do sleep disorders contribute to pain sensitivity? Curr Rheumatol Rep. 2011;13(6):528–534. doi:10.1007/s11926-011-0204-8
19. Sommer M, de Rijke JM, van Kleef M, et al. Predictors of acute postoperative pain after elective surgery. Clin J Pain. 2010;26(2):87–94. doi:10.1097/AJP.0b013e3181b43d68
20. Rehberg S, Weber TP, Van Aken H, et al. Sleep disturbances after posterior scoliosis surgery with an intraoperative wake-up test using remifentanil. Anesthesiology. 2008;109(4):629–641. doi:10.1097/ALN.0b013e31818629c2
21. Fayezizadeh M, Majumder A, Neupane R, et al. Efficacy of transversus abdominis plane block with liposomal bupivacaine during open abdominal wall reconstruction. Am J Surg. 2016;212(3):399–405. doi:10.1016/j.amjsurg.2015.12.026
22. Kneeland ET, Dovidio JF, Joormann J, et al. Emotion malleability beliefs, emotion regulation, and psychopathology: integrating affective and clinical science. Clin Psychol Rev. 2016;45:81–88. doi:10.1016/j.cpr.2016.03.008
23. Gregory AM, Sadeh A. Sleep, emotional and behavioral difficulties in children and adolescents. Sleep Med Rev. 2012;16(2):129–136. doi:10.1016/j.smrv.2011.03.007
24. Dolan R, Huh J, Tiwari N, et al. A prospective analysis of sleep deprivation and disturbance in surgical patients. Ann Med Surg. 2016;6:1–5. doi:10.1016/j.amsu.2015.12.046
25. Freedman NS, Kotzer N, Schwab RJ. Patient perception of sleep quality and etiology of sleep disruption in the intensive care unit. Am J Respir Crit Care Med. 1999;159(4):1155–1162. doi:10.1164/ajrccm.159.4.9806141
26. Cmiel CA, Karr DM, Gasser DM, et al. Noise control: a nursing team’s approach to sleep promotion. Am J Nurs. 2004;104(2):40–49. doi:10.1097/00000446-200402000-00019
27. Balk M, Hentschke H, Rudolph U, et al. Differential depression of neuronal network activity by midazolam and its main metabolite 1-hydroxymidazolam in cultured neocortical slices. Sci Rep. 2017;7(1):3503–3515. doi:10.1038/s41598-017-03154-5
28. Tan W-F, Miao E-Y, Jin F, et al. Changes in first postoperative night bispectral index after daytime sedation induced by dexmedetomidine or midazolam under regional anesthesia: a randomized controlled trial. Reg Anesth Pain Med. 2016;41(3):380–386. doi:10.1097/AAP.0000000000000370
29. Wang XL, Ke YN; Midazolam Trenting Hypentension with Insomnia Study Group. [Effects of midazolam and estazolam as hypnotics in hypertensive patients with chronic insomnia: a multicentre, open labeled, randomized clinical trial]. Zhonghua Xin Xue Guan Bing Za Zhi. 2006;34(4):338–340. Chinese.
30. Öbrink E, Jildenstål P, Oddby E, et al. Post-operative nausea and vomiting: update on predicting the probability and ways to minimize its occurrence, with focus on ambulatory surgery. Int J Surg. 2015;15:100–106. doi:10.1016/j.ijsu.2015.01.024
31. Sivertsen B, Krokstad S, Øverland S, et al. The epidemiology of insomnia: associations with physical and mental health. The HUNT-2 study. J Psychosom Res. 2009;67(2):109–116. doi:10.1016/j.jpsychores.2009.05.001
32. Ford DE, Kamerow DB. Epidemiologic study of sleep disturbances and psychiatric disorders. An opportunity for prevention? JAMA. 1989;262(11):1479–1484. doi:10.1001/jama.262.11.1479
33. Stein MB, McCarthy MJ, Chen CY, et al. Genome-wide analysis of insomnia disorder. Mol Psychiatry. 2018;23(11):2238–2250. doi:10.1038/s41380-018-0033-5
34. Stenveld F, Bosman S, van Munster BC, et al. Melatonin, temazepam and placebo in hospitalised older patients with sleeping problems (MATCH): a study protocol of randomised controlled trial. BMJ Open. 2019;9(5):e025514. doi:10.1136/bmjopen-2018-025514
35. Broderick JE, Junghaenel DU, Schneider S, et al. Pittsburgh and Epworth sleep scale items: accuracy of ratings across different reporting periods. Behav Sleep Med. 2013;11(3):173–188. doi:10.1080/15402002.2012.654549
36. Lei M, Zhang P, Liu Y, et al. Propofol and sufentanil may affect the patients’ sleep quality independently of the surgical stress response: a prospective nonrandomized controlled trial in 1033 patients’ undergone diagnostic upper gastrointestinal endoscopy. BMC Anesthesiol. 2017;17(1):53. doi:10.1186/s12871-017-0341-3
37. Yilmaz H, Iskesen I. Follow-up with objective and subjective tests of the sleep characteristics of patients after cardiac surgery. Circ J. 2007;71(10):1506–1510. doi:10.1253/circj.71.1506
38. Yilmaz M, Sayin Y, Gurler H. Sleep quality of hospitalized patients in surgical units. Nurs Forum. 2012;47(3):183–192. doi:10.1111/j.1744-6198.2012.00268.x
39. Zhang X, Smith N, Spear E, et al. Neighborhood characteristics associated with COVID-19 burden-the modifying effect of age. J Expo Sci Environ Epidemiol. 2021;4:1–13. doi:10.1038/s41370-021-00329-1
40. Sha L, Xu T, Ge X, et al. Predictors of death within 6 months of stroke onset: a model with Barthel index, platelet/lymphocyte ratio and serum albumin. Nurs Open. 2020;8(3):1380–1392. doi:10.1002/nop2.754
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.