Back to Journals » International Journal of General Medicine » Volume 18
Development and Validation of Deep Learning Model for Predicting Long-Term Prognosis in Patients with Symptomatic Intracranial Arterial Stenosis
Authors Ding Q, Zhang S ![]() , Pan L
, Pan L
Received 3 June 2025
Accepted for publication 18 September 2025
Published 24 October 2025 Volume 2025:18 Pages 6455—6465
DOI https://doi.org/10.2147/IJGM.S538889
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Redoy Ranjan
Qianjin Ding,1 Shaojie Zhang,2 Li Pan2
1Department of Neurosurgery, Xinxiang Center Hospital, Xinxiang, Henan, 453000, People’s Republic of China; 2Department of Neurosurgery, Yangtze River Shipping General Hospital, Wuhan, Hubei, 430014, People’s Republic of China
Correspondence: Li Pan, Department of Neurosurgery, Yangtze River Shipping General Hospital, No. 5 Huijiroad, Jiangan District, Wuhan, Hubei, 430014, People’s Republic of China, Email [email protected] Shaojie Zhang, Department of Neurosurgery, Yangtze River Shipping General Hospital, No. 5 Huijiroad, Jiangan District, Wuhan, Hubei, 430014, People’s Republic of China, Email [email protected]
Background and Aim: Symptomatic intracranial arterial stenosis (ICAS) is a leading cause of ischemic stroke, and its progression is associated with an increased risk of stroke recurrence and poor outcomes. Accurate prediction of the risk of progression in ICAS patients is crucial for timely intervention and management. This study aims to develop and validate logistic regression and deep learning models to predict the risk of progression in symptomatic ICAS patients and compare their predictive performance.
Methods: A retrospective study was conducted on 266 symptomatic ICAS patients who were followed for at least 3 years. The dataset was randomly split into a training set (70%) and a validation set (30%). Data preprocessing involved normalization, feature selection, and class balancing techniques to enhance model performance. Logistic regression, and deep learning models were developed to predict the risk of ICAS progression. The models were evaluated using accuracy, sensitivity, specificity, precision, F1-score, and the area under the receiver operating characteristic curve (AUC).
Results: The logistic regression model achieved an AUC of 0.771 (training) and 0.767 (validation; 95% CI: 0.702– 0.832). The deep learning model demonstrated superior performance with an AUC of 0.898 (training) and 0.863 (validation; 95% CI: 0.801– 0.925), showing a statistically significant improvement (p = 0.016, DeLong’s test). Feature importance analysis identified hypertension, diabetes, stenosis degree, and prior stroke history as the most influential predictors of ICAS progression. These results highlight the value of early risk stratification to guide timely clinical intervention.
Conclusion: Compared to logistic regression, the deep learning model exhibited significantly improved predictive accuracy for the risk of progression in symptomatic ICAS patients. The high performance and reliability of the deep learning model highlight its potential clinical utility in predicting ICAS progression, ultimately aiding in risk stratification and personalized treatment strategies.
Keywords: symptomatic intracranial arterial stenosis, risk of progression, logistic regression, deep learning
Introduction
Symptomatic intracranial arterial stenosis (ICAS) is a major cause of ischemic stroke, accounting for approximately 8–10% of all cases worldwide, and is associated with high rates of recurrence (15–20% annually) and long-term disability despite standard medical therapy.1–3 It occurs when narrowing of the brain’s blood vessels reduces cerebral blood flow, leading to neurological impairments. Despite advances in treatment options, including antiplatelet therapy and surgical interventions, predicting ICAS progression remains a significant challenge. Early identification of patients at high risk of progression is crucial for optimizing treatment plans and improving clinical outcomes.
Previous attempts to predict ICAS progression have primarily relied on clinical markers and imaging techniques. Common risk factors such as hypertension, diabetes, and the degree of stenosis have been linked to worse outcomes. Kim et al4 analyzed blood samples from 409 patients and found that platelet-derived growth factors were associated with the progression of symptomatic intracranial atherosclerotic stenosis. Imaging techniques like magnetic resonance angiography (MRA) and computed tomography angiography (CTA) have been used to assess the severity of stenosis. Yu et al5 conducted a study using questionnaires, blood tests, and high-resolution vessel wall magnetic resonance (MR) imaging, and identified carotid artery plaques as an important predictor of ICAS progression. However, traditional methods such as logistic regression often fail to capture the complex interactions between multiple risk factors and variables, limiting their predictive power.
In recent years, machine learning (ML) approaches, especially deep learning (DL), have demonstrated superior capabilities in predicting medical outcomes by analyzing large datasets and identifying complex, nonlinear patterns that may not be apparent through traditional statistical methods.6–9 These models have been successfully applied in various medical fields, including stroke prediction, cardiovascular risk assessment, and neuroimaging-based disease classification, often outperforming conventional regression-based approaches. Their ability to integrate multidimensional data, such as clinical characteristics, laboratory markers, and imaging features, enables more precise risk stratification and outcome prediction.10–12 However, despite their success in other domains, the application of ML and DL models in predicting the progression of symptomatic ICAS remains limited. Further research is needed to explore their potential in improving early detection, risk assessment, and personalized treatment strategies for ICAS patients.
We hypothesize that a deep learning–based prediction model will outperform traditional logistic regression in accurately identifying patients at high risk of ICAS progression. This study aims to address this gap by developing and validating predictive models using logistic regression, and deep learning techniques. By analyzing data from 266 symptomatic ICAS patients, we aim to create a tool that can predict the risk of ICAS progression with high accuracy. The results of this study may provide valuable insights for clinicians to identify high-risk patients early and tailor treatment plans accordingly, ultimately improving patient management and reducing stroke-related morbidity.
Materials and Methods
Study Design and Data Collection
A retrospective study was conducted on 266 patients diagnosed with symptomatic ICAS between 2019 and 2021 at Xinxiang Center Hospital and Yangtze River Shipping General Hospital. Of the 266 patients, 162 were enrolled from Xinxiang Central Hospital and 104 from Yangtze River Shipping General Hospital. The study aimed to develop and validate logistic regression and deep learning models for predicting the risk of ICAS progression. Clinical and imaging data were collected from electronic medical records including demographic information medical history hypertension diabetes smoking status imaging characteristics degree of stenosis hemodynamic parameters and treatment methods medical therapy or interventional procedures. All data were de-identified to maintain patient confidentiality. Inclusion criteria included patients diagnosed with symptomatic ICAS confirmed by magnetic resonance angiography MRA or computed tomography angiography CTA at least one follow-up imaging study to assess ICAS progression and availability of complete baseline clinical and imaging data. Exclusion criteria included a history of non-atherosclerotic cerebrovascular disease such as vasculitis or moyamoya disease patients with severe systemic conditions affecting prognosis such as malignancies or renal failure and those with missing critical follow-up data. This study was approved by the Institutional Review Board and conducted in accordance with the Declaration of Helsinki.
Outcome Definition and ICAS Progression Assessment
ICAS progression was defined based on follow-up imaging findings and clinical deterioration. Patients were classified into two groups stable ICAS and progressive ICAS. Stable ICAS was defined as no significant change in arterial stenosis severity over the follow-up period. Progressive ICAS was defined as a ≥20% increase in the degree of stenosis on follow-up imaging, while stable ICAS was defined as <20% change. The percentage of stenosis was calculated using the Warfarin-Aspirin Symptomatic Intracranial Disease WASID trial methodology by measuring the residual lumen diameter at the most stenotic segment and comparing it with the estimated normal artery diameter.
Clinical events were also recorded during the follow-up period including ischemic stroke transient ischemic attacks TIA and any neurological deterioration related to cerebrovascular insufficiency. Patients with progressive stenosis on imaging who also exhibited new ischemic symptoms were classified as high-risk progressors. Follow-up imaging was performed at intervals of 6 months to 1 year depending on clinical severity and treatment strategy.
Data Preprocessing
To optimize model performance and reduce bias extensive data preprocessing was conducted. Continuous variables such as blood pressure and lipid levels were standardized to ensure uniform feature scaling. Missing values accounting for less than five percent of the dataset were imputed using the mean for continuous variables and mode for categorical variables. Feature selection was performed based on univariate logistic regression analysis and expert clinical evaluation to enhance model interpretability.
The dataset was randomly split into two subsets with a training set consisting of seventy percent of the data for model development and a validation set of thirty percent for performance evaluation.
Model Development
Three predictive models were developed logistic regression and a deep learning neural network to evaluate the risk of ICAS progression.
The logistic regression LR model was constructed using selected independent variables with clinical relevance including age sex hypertension diabetes baseline stenosis degree and prior stroke history. It served as the baseline model for comparison against more complex machine learning algorithms.
The deep learning DL model was implemented as a fully connected artificial neural network ANN. The input layer consisted of preprocessed clinical and imaging variables. A total of 18 features were used as model input. The deep learning model consisted of three hidden layers with 96, 60, and 36 neurons, respectively. Each layer used ReLU activation and dropout regularization. To reduce overfitting dropout regularization was applied with dropout rates ranging from 0.2 to 0.5 in different layers. The output layer used a sigmoid activation function to produce probability scores for ICAS progression. Hyperparameter tuning for the deep learning model was performed using Bayesian optimization to determine optimal learning rate batch size and dropout rates. The model was trained using an adaptive moment estimation Adam optimizer with binary cross-entropy as the loss function.
Feature importance analysis was performed using SHapley Additive exPlanations SHAP values to interpret the contribution of each variable in both traditional and machine learning models. Model training was conducted using Python’s TensorFlow and Scikit-learn libraries and computational resources were provided through a high-performance computing cluster.
Model Evaluation
Predictive performance was assessed using multiple metrics including accuracy which measures the proportion of correctly classified cases sensitivity which evaluates the ability to correctly identify patients with ICAS progression specificity which determines the ability to correctly classify patients without progression and precision and F1-score which balance false positives and false negatives. The area under the receiver operating characteristic curve AUC-ROC was used to measure overall model discrimination.
Data Analysis
Continuous variables were expressed as median with interquartile range IQR and compared using the independent t-test or Mann–Whitney U-test. Categorical variables were presented as frequencies and percentages and compared using the chi-square test or Fisher’s exact test.
To identify risk factors associated with ICAS progression univariate logistic regression analysis was performed. Variables with a P-value less than 0.05 in the univariate analysis were included in a multivariate logistic regression model using a backward stepwise selection method. The variance inflation factor VIF was calculated to detect multicollinearity and variables with VIF greater than five were excluded from the final model. To compare model performance receiver operating characteristic ROC curves were generated and AUC-ROC values were used as the primary performance metric. Delong’s test was conducted to determine whether differences in AUC-ROC values among models were statistically significant.
All statistical analyses were performed using SPSS version 25.0 IBM Corp Armonk NY USA. Machine learning models were implemented using Python version 3.8 Python Software Foundation Wilmington DE USA and R software version 4.1.2 R Foundation for Statistical Computing Vienna Austria was used for additional model evaluation and visualization.
Results
Baseline Characteristics of the Training, Validation Cohorts
A total of 328 patients diagnosed with intracranial arterial stenosis were initially screened during the study period. Sixty-two patients were excluded due to the following reasons: history of non-atherosclerotic cerebrovascular disease (n=27), severe systemic conditions affecting prognosis (n=20), missing follow-up imaging data (n=8), or missing critical clinical data (n=7). As a result, 266 patients were included in the final analysis. The median follow-up duration was 30 months (IQR: 24–36 months). A total of 12 patients were excluded due to incomplete follow-up imaging, and 9 were lost to follow-up, leaving 266 for analysis. Patients were randomly assigned to training and validation cohorts in a 0.7:0.3 ratio, with 186 patients in the training cohort and 80 in the validation cohort. The inclusion and exclusion process is illustrated in Figure 1. The distribution of key clinical characteristics was balanced between the two cohorts (p > 0.05 for all variables). Table 1 presents the baseline demographic, clinical, and imaging characteristics of patients in each cohort. There were no significant differences in age, sex, degree of stenosis, or treatment approach between the groups, indicating an appropriate randomization process.
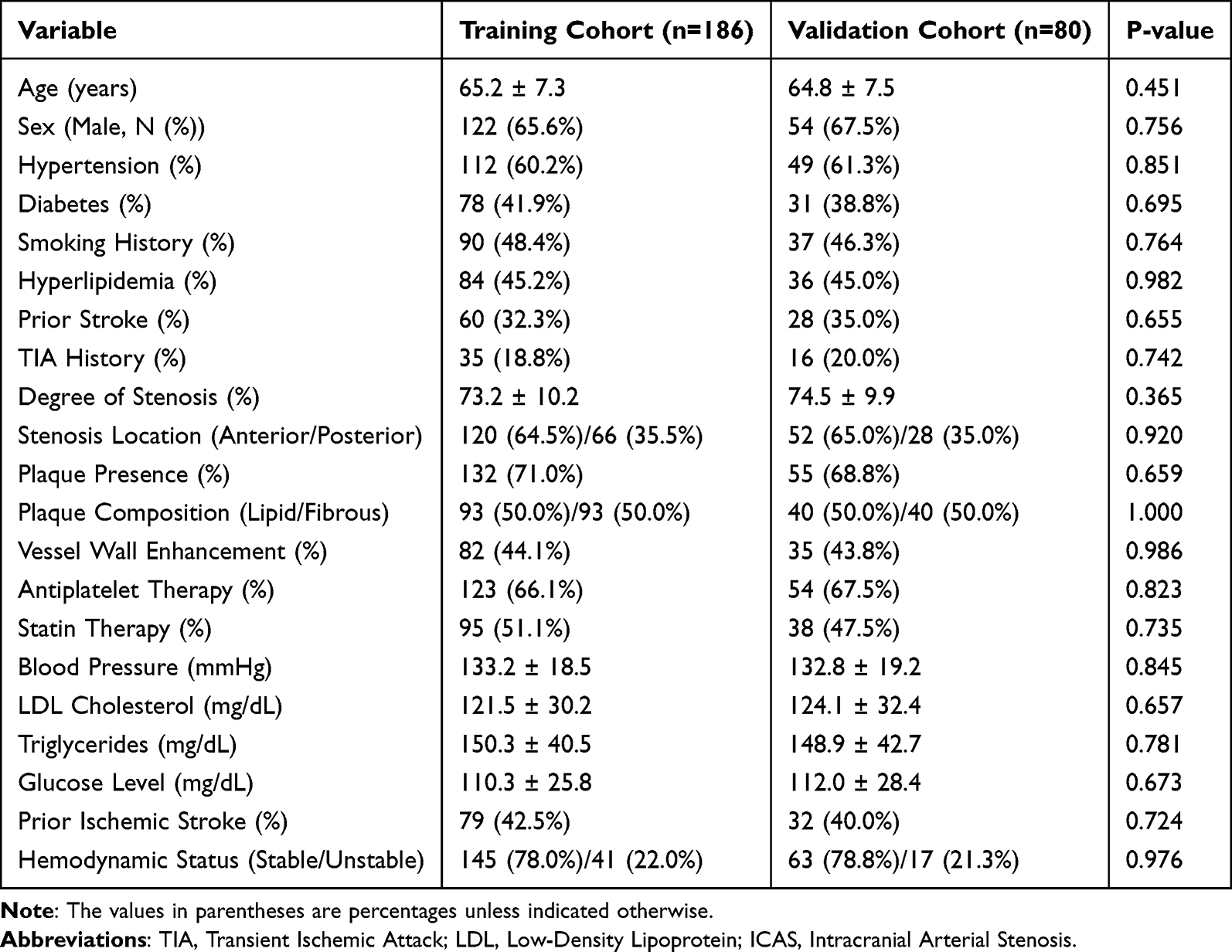 |
Table 1 Baseline Characteristics of the Training, Validation, and Test Cohorts of HCC Patients (N = 266) |
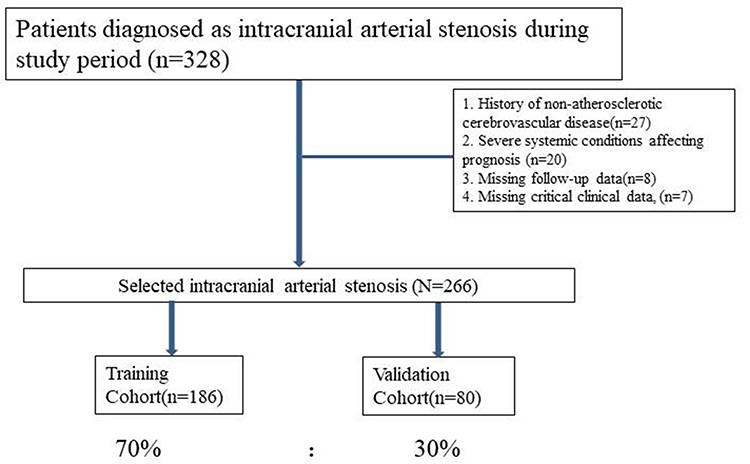 |
Figure 1 Flow chart for inclusion and exclusion of patients with Symptomatic Intracranial Arterial Stenosis. |
Univariate and Multivariate Logistic Regression Analysis of ICAS Progression in the Training Cohort
Univariate logistic regression analysis was conducted in the training cohort to assess potential risk factors associated with ICAS progression. Variables with p < 0.05 in the univariate analysis were included in the multivariate logistic regression model. The results of the univariate analysis revealed that age, sex, hypertension, diabetes, prior stroke, degree of stenosis, plaque presence, and vessel wall enhancement were significantly associated with ICAS progression. Specifically, degree of stenosis (OR = 2.31, 95% CI: 2.05–2.80, p = 0.012) were identified as important univariate predictors. Additionally, prior stroke (OR = 1.75, 95% CI: 1.42–2.11, p = 0.021) and vessel wall enhancement (OR = 1.89, 95% CI: 1.61–2.33, p = 0.038) emerged as significant indicators of ICAS progression. The multivariate logistic regression analysis identified degree of stenosis (OR = 2.12, 95% CI: 1.93–2.50, p = 0.025), plaque presence (OR = 1.95, 95% CI: 1.65–2.40, p = 0.007), and vessel wall enhancement (OR = 1.72, 95% CI: 1.50–2.18, p = 0.044) as significant independent predictors of ICAS progression. The multivariate model indicated that patients with higher degrees of stenosis and plaque presence were more likely to experience progression of ICAS. Other variables, such as smoking history, glucose levels, and blood pressure, were also significant in univariate analysis but did not remain significant in the multivariate analysis. The full results of univariate and multivariate logistic regression analyses are presented in Table 2.
 |
Table 2 Multivariate and Univariate Logistic Regression Analysis of ICAS Progression in the Training Cohort |
Comparison of Logistic Regression, Support Vector Machine, and Deep Learning Models
The logistic regression model was constructed using significant predictors identified from multivariate analysis. The model demonstrated an AUC of 0.771 in the training cohort and 0.767 in the validation cohort (Figure 2).
 |
Figure 2 Performance of the Logistics Regression Model for ROC curve. |
A total of 18 features were used as input, including demographic, clinical, laboratory, and imaging variables. The deep learning model was developed using a fully connected neural network architecture designed to analyze complex relationships between clinical and imaging variables. The model consisted of an input layer integrating preprocessed clinical and imaging features followed by three hidden layers. The first hidden layer contained 96 neurons with a ReLU activation function and a dropout layer with a dropout rate of 0.2. The second hidden layer had 60 neurons followed by ReLU activation and another dropout layer with a dropout rate of 0.2. The third hidden layer comprised 36 neurons with ReLU activation and dropout regularization. The output layer applied a sigmoid activation function to predict the probability of ICAS progression. The model was optimized using the Adam optimizer with an initial learning rate of 0.001. A binary cross-entropy loss function was used, and early stopping was implemented to prevent overfitting. The architecture of the deep learning model is illustrated in Figure 3A.
 |
Figure 3 Performance of the Deep Learning Model. (A) represents the model architecture diagram, and (B) represents the ROC curve of the model on the training and validation sets. |
After hyperparameter tuning, the deep learning model achieved an AUC of 0.898 in the training cohort and 0.863 in the validation cohort (Figure 3B). The deep learning model outperformed logistic regression in both datasets, indicating superior predictive accuracy.
Performance of Multiple Models
The performance comparison between the logistic regression, and deep learning models is summarized in Table 3. The deep learning model consistently outperformed both logistic regression across all datasets, demonstrating superior sensitivity, specificity, and F1-score. In the training cohort, the deep learning model achieved an AUC of 0.898 and an F1-score of 0.865, whereas the logistic regression model had an AUC of 0.771 and an F1-score of 0.733. In the validation cohort, the deep learning model maintained strong predictive performance with an AUC of 0.863 and an F1-score of 0.849, while the logistic regression model exhibited lower accuracy, achieving an AUC of 0.767 and an F1-score of 0.724. DeLong’s test showed that the AUC of the deep learning model was significantly higher than that of the logistic regression model (p = 0.016). These results indicate that the deep learning model provides superior predictive capability and may serve as a more effective clinical tool for assessing the risk of ICAS progression. To enhance clinical relevance, we additionally calculated the positive predictive value (PPV) for both models. In the validation cohort, the deep learning model achieved a PPV of 82.8%, while the logistic regression model achieved a PPV of 72.6%, further supporting the superior predictive accuracy and potential clinical utility of the deep learning approach. As shown in Supplementary Figure 1, the calibration plot demonstrates that the deep learning model consistently exhibited better agreement between predicted probabilities and observed outcomes across all probability ranges, indicating superior overall calibration compared to the logistic regression model.
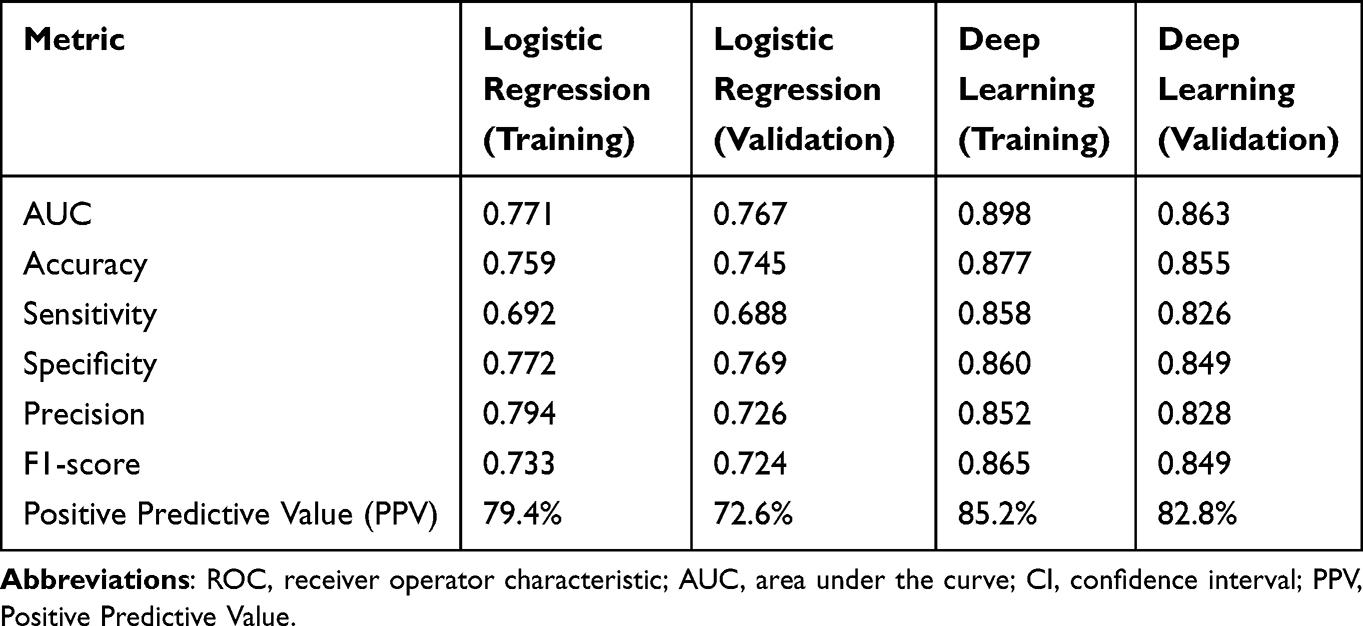 |
Table 3 Evaluation Indicators for Each Model |
Discussion
The findings of this study demonstrate that deep learning models outperform traditional logistic regression in predicting the progression of symptomatic intracranial arterial stenosis (ICAS). The superior performance of deep learning is likely attributed to its ability to identify complex nonlinear relationships among clinical and imaging variables that traditional statistical methods may not fully capture. Logistic regression, while widely used for risk factor analysis, has limitations in handling high-dimensional datasets with intricate interactions. Our results align with emerging evidence supporting the integration of artificial intelligence in vascular disease prediction to enhance risk stratification and clinical decision-making.
Previous studies investigating ICAS progression have primarily focused on conventional statistical models or specific biomarkers, yielding mixed results. For example, Li et al13 suggested that the dynamic and unstable inflammatory processes within intracranial arteries are associated with miRNAs (miR-155, miR-27a/b, miR-342-5p, miR-21, miR-124, and miR-223), which may be involved in the progression of intracranial atherosclerotic plaques. Xie et al14 conducted a large-scale study and found that triglyceride-glucose index is a useful indicator for ICA and severe stenosis. Su et al15 analyzed serum inflammatory markers and found that elevated C-reactive protein and interleukin-6 levels were associated with an increased risk of ICAS progression. Additionally, Zhang et al16 performed a cohort study using high-resolution vessel wall imaging and demonstrated that patients with positive remodeling and lipid-rich necrotic core plaques were more likely to experience disease progression. However, these studies did not incorporate machine learning techniques to assess overall predictive accuracy. Our study not only confirmed the significance of hypertension, diabetes, degree of stenosis, and prior ischemic stroke as key risk factors but also demonstrated that deep learning models significantly outperform logistic regression in predictive accuracy. In our study, the AUC for the logistic regression model was 0.771, indicating moderate predictive ability, whereas the deep learning model significantly outperformed it with an AUC of 0.863. Our findings also align with population-based studies such as the Tromsø 7 Study,17 which emphasized the role of vascular risk factor burden in long-term cerebrovascular disease progression. Such studies reinforce the clinical relevance of using predictive models for early risk stratification in high-risk populations.
Currently, no widely established deep learning models have been designed specifically for ICAS progression prediction, but recent advancements in machine learning have shown great promise in predicting stroke risk and vascular disease outcomes. Unlike logistic regression, deep neural networks can extract meaningful patterns from complex patient data, allowing for a more precise classification of high-risk individuals. Several studies have demonstrated the advantages of machine learning in stroke prediction. For instance, Sun et al18 developed a deep learning model to predict recurrent strokes in patients with large artery atherosclerosis and found that deep learning significantly improved prediction accuracy compared to traditional models. Similarly, a study by Zhao et al19 applied machine learning techniques to intracranial atherosclerosis prognosis and reported that nonlinear models such as deep learning and gradient boosting outperformed conventional statistical approaches. Our study represents one of the first to apply deep learning specifically to ICAS progression prediction and validate its performance using a well-structured dataset. The deep learning model’s ability to integrate clinical and imaging features without requiring explicit feature selection provides a key advantage over traditional methods. The model architecture was designed to optimize predictive accuracy while minimizing overfitting, utilizing three hidden layers with 96, 60, and 36 neurons respectively, ReLU activation functions, and dropout regularization. The tuning of hyperparameters, such as learning rate, batch size, and dropout rate, further enhanced the model’s stability and generalizability. The resulting AUC values of 0.898 in the training cohort and 0.863 in the validation cohort confirm the model’s robust predictive ability. An AUC of 0.898 indicates a high discriminative ability to distinguish patients at risk of ICAS progression. This level of performance may support earlier identification of high-risk individuals who could benefit from intensified medical therapy or closer imaging follow-up, thus potentially improving long-term outcomes. Unlike prior studies focusing on isolated biomarkers or imaging features, our deep learning model integrates a multidimensional dataset—including clinical, imaging, and laboratory variables—allowing for more robust prediction of ICAS progression. This holistic approach enhances predictive performance beyond traditional regression or single-modality biomarker models.
Feature importance analysis provided further insights into the key predictors of ICAS progression. SHapley Additive exPlanations (SHAP) values identified hypertension, diabetes, stenosis severity, and prior ischemic stroke as the most influential variables contributing to model predictions. These findings align with prior research, reinforcing the importance of these clinical and imaging markers. For example, a study by Tang et al highlighted that patients with severe stenosis and a history of hypertension had a significantly higher risk of recurrent ischemic events, while another study by Wang et al emphasized the role of carotid plaques and hemodynamic changes in predicting ICAS progression. Our results support these findings, suggesting that integrating multiple clinical parameters into an artificial intelligence-based model provides a more comprehensive risk assessment framework for ICAS patients.
Accurate prediction of ICAS progression has important clinical implications. Patients identified as high-risk could benefit from more aggressive treatment strategies, including closer monitoring, earlier initiation of intensive medical therapy such as dual antiplatelet agents and high-dose statins, and consideration for endovascular intervention when appropriate. Additionally, lifestyle modifications, including blood pressure control and glucose regulation, may play a key role in slowing disease progression.20–22 The implementation of an artificial intelligence-based ICAS progression prediction tool in clinical practice could help neurologists and vascular specialists refine patient management, personalize treatment decisions, and potentially reduce stroke recurrence rates.
This study has several limitations that should be acknowledged. First, the retrospective design may introduce selection bias, despite the careful curation of data and well-defined inclusion criteria. Additionally, all patients were enrolled from two centers within a similar geographic region, which may limit the generalizability of the findings. Notably, the absence of an external validation cohort represents a key limitation. To enhance robustness and clinical applicability, future studies should employ larger, multicenter prospective cohorts to externally validate the model across diverse populations and healthcare settings. Second, while we used univariate logistic regression combined with clinical judgment for initial feature selection, this approach may not capture complex multivariate interactions. In future work, more robust feature selection methods, such as LASSO regression or recursive feature elimination (RFE), could be employed to improve model stability and reduce overfitting. Third, the interpretability of deep learning models remains a challenge. Although SHAP (SHapley Additive exPlanations) analysis was utilized to identify influential predictors, the model still functions as a “black box” in many aspects, which may hinder its integration into clinical workflows. To address this, future research should consider incorporating additional explainable AI (XAI) techniques, such as LIME (Local Interpretable Model-Agnostic Explanations) or attention-based visualization methods, to enhance transparency, align with clinical reasoning, and foster greater trust among healthcare professionals.
Conclusion
In conclusion, this study demonstrates the potential of a deep learning–based model to predict long-term progression in patients with symptomatic intracranial arterial stenosis with high accuracy. The model outperformed traditional logistic regression and identified key clinical factors associated with disease progression. These findings may assist in early risk stratification and individualized clinical decision-making. To further establish the clinical utility of this model, future studies should focus on prospective validation using large, multicenter cohorts across diverse populations. Additionally, efforts should be made to integrate the model into clinical workflows, ideally through decision support systems that provide transparent and interpretable outputs to clinicians.
Data Sharing Statement
The datasets used and analyzed during the current study are available from the corresponding author (Li Pan) on reasonable request.
Ethics Approval and Consent to Participate
This retrospective study was approved by the Ethics Committee of Xinxiang Center Hospital and Yangtze River Shipping General Hospital (No.YL2019055), and was conducted in accordance with the ethical principles of the Declaration of Helsinki. The requirement for written informed consent was waived by the institutional ethics committee due to the retrospective nature of the study and the use of de-identified data.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
There is no funding to report.
Disclosure
The authors declare that they have no competing interests in this work.
References
1. Carvalho M, Oliveira A, Azevedo E, Bastos-Leite AJ. Intracranial arterial stenosis. J Stroke Cerebrovascular Dis. 2014;23(4):599–609. doi:10.1016/j.jstrokecerebrovasdis.2013.06.006
2. Sun Y, Li X, Ding Y, et al. Balloon angioplasty vs. stenting for symptomatic intracranial arterial stenosis. Front Neurol. 2022;13:878179. doi:10.3389/fneur.2022.878179
3. Wang T, Yang K, Luo J, et al. Outcomes after stenting for symptomatic intracranial arterial stenosis: a systematic review and meta-analysis. J Neurol. 2020;267(3):581–590. doi:10.1007/s00415-018-09176-x
4. Kim KJ, Jeong SW, Ryu WS, et al. Platelet-derived growth factor is associated with progression of symptomatic intracranial atherosclerotic stenosis. J Clin Neurol. 2021;17(1):70–76. doi:10.3988/jcn.2021.17.1.70
5. Yu M, Yang D, Zhang R, et al. Carotid atherosclerotic plaque predicts progression of intracranial artery atherosclerosis: a MR imaging-based community cohort study. Eur J Radiol. 2024;172:111300. doi:10.1016/j.ejrad.2024.111300
6. Choi RY, Coyner AS, Kalpathy-Cramer J, Chiang MF, Campbell JP. Introduction to machine learning, neural networks, and deep learning. Trans Vision Sci Technol. 2020;9(2):14.
7. Deo RC. Machine learning in medicine. Circulation. 2015;132(20):1920–1930. doi:10.1161/CIRCULATIONAHA.115.001593
8. Greener JG, Kandathil SM, Moffat L, Jones DT. A guide to machine learning for biologists. Nat Rev Mol Cell Biol. 2022;23(1):40–55. doi:10.1038/s41580-021-00407-0
9. Xia F, Chen Q, Liu Z, et al. Machine learning models for predicting postoperative peritoneal metastasis after hepatocellular carcinoma rupture: a multicenter cohort study in China. Oncologist. 2025;30(1). doi:10.1093/oncolo/oyae341
10. Campagnini S, Arienti C, Patrini M, Liuzzi P, Mannini A, Carrozza MC. Machine learning methods for functional recovery prediction and prognosis in post-stroke rehabilitation: a systematic review. J Neuroeng Rehabil. 2022;19(1):54. doi:10.1186/s12984-022-01032-4
11. Gautam N, Mueller J, Alqaisi O, et al. Machine learning in cardiovascular risk prediction and precision preventive approaches. Curr Atherosclerosis Rep. 2023;25(12):1069–1081. doi:10.1007/s11883-023-01174-3
12. Heo J, Yoon JG, Park H, Kim YD, Nam HS, Heo JH. Machine learning-based model for prediction of outcomes in acute stroke. Stroke. 2019;50(5):1263–1265. doi:10.1161/STROKEAHA.118.024293
13. Li J, Li K, Chen X. Inflammation-regulatory microRNAs: valuable targets for intracranial atherosclerosis. J Neurosci Res. 2019;97(10):1242–1252. doi:10.1002/jnr.24487
14. Xie Y, Cen K, Dan B, et al. Association between triglyceride-glucose index and intracranial/extracranial atherosclerotic stenosis: findings from a retrospective study. Cardiovasc Diabetol. 2024;23(1):95. doi:10.1186/s12933-024-02187-1
15. Su BJ, Dong Y, Tan CC, et al. Elevated Hs-CRP levels are associated with higher risk of intracranial arterial stenosis. Neurotox Res. 2020;37(2):425–432. doi:10.1007/s12640-019-00108-9
16. Han Y, Qiao H, Chen S, et al. Intracranial artery stenosis magnetic resonance imaging aetiology and progression study: rationale and design. Brain and Behavior. 2018;8(12):e01154. doi:10.1002/brb3.1154
17. Staxrud F, Mulic A, Kopperud SE. Dentists’ treatment decisions concerning restorations in adult patients in north norway: a cross-sectional tromsø 7 study. Caries Res. 2025;59(2):151–162. doi:10.1159/000541777
18. Sun TH, Wang CC, Wu YL, Hsu KC, Lee TH. Machine learning approaches for biomarker discovery to predict large-artery atherosclerosis. Sci Rep. 2023;13(1):15139. doi:10.1038/s41598-023-42338-0
19. Zhao Y, Song P, Feng P, et al. Plaque enhancement predicts recurrence in acute ischemic stroke patients with large artery intracranial atherosclerosis. J Stroke Cerebrovascular Dis. 2023;32(12):107406. doi:10.1016/j.jstrokecerebrovasdis.2023.107406
20. Cen K, Huang Y, Xie Y, Liu Y. The Guardian of intracranial vessels: why the pericyte? Biomed Pharmacother. 2024;176:116870. doi:10.1016/j.biopha.2024.116870
21. Gutierrez J, Turan TN, Hoh BL, Chimowitz MI. Intracranial atherosclerotic stenosis: risk factors, diagnosis, and treatment. Lancet Neurol. 2022;21(4):355–368. doi:10.1016/S1474-4422(21)00376-8
22. Wang Y, Meng R, Liu G, et al. Intracranial atherosclerotic disease. Neurobiol Dis. 2019;124:118–132. doi:10.1016/j.nbd.2018.11.008
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.