Back to Journals » International Journal of General Medicine » Volume 15
Development and Validation of a Self-Administered Screening Test for Betel Quid Use Disorders in Betel Quid Chewers in Hunan, China
Authors Yang L ![]() , Dang W, Yu X
, Dang W, Yu X ![]() , He Y, Shi C, Yi J, Gao L, Li S, Zhou T
, He Y, Shi C, Yi J, Gao L, Li S, Zhou T ![]() , Ma Y
, Ma Y
Received 22 August 2022
Accepted for publication 31 October 2022
Published 14 November 2022 Volume 2022:15 Pages 8183—8190
DOI https://doi.org/10.2147/IJGM.S386539
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Dr Scott Fraser
Lei Yang,1,2 Weimin Dang,2,3 Xin Yu,1,2 Yi He,4,5 Chuan Shi,1,2 Jialong Yi,1,2 Lu Gao,6 Siheng Li,7 Tianhang Zhou,1,2 Yantao Ma1,2
1Department of Clinical Research, Peking University Sixth Hospital (Institute of Mental Health), Beijing, People’s Republic of China; 2NHC Key Laboratory of Mental Health (Peking University), National Clinical Research Center for Mental Disorders (Peking University Sixth Hospital), Beijing, People’s Republic of China; 3The Division of Medical Affairs, Peking University Sixth Hospital (Institute of Mental Health), Beijing, People’s Republic of China; 4Key Laboratory of Carcinogenesis and Translational Research (Ministry of Education), Beijing, People’s Republic of China; 5Department of Psycho-Oncology, Peking University Cancer Hospital & Institute, Beijing, People’s Republic of China; 6Department of Stomatology, Beijing Children’s Hospital, Capital Medical University, Beijing, People’s Republic of China; 7Department of Neurology, Peking University First Hospital, Beijing, People’s Republic of China
Correspondence: Xin Yu, Peking University Sixth Hospital, No. 51 Hua Yuan Bei Road, Haidian District, Beijing, 100191, People’s Republic of China, Tel +86 13718747842, Fax +86-10-62026310, Email [email protected]
Introduction: Processed betel quid product chewing is a public health problem in areca non-plant areas in China. However, there is no valid instrument to screen for betel quid use disorder (BQUD) in mainland China. We developed a self-administered screening test for betel quid use disorders (SST-BQUD) and tested its reliability and validity in a sample of betel quid chewers (BQCers) in Hunan, China.
Methods: Items of SST-BQUD were selected from the test results of an item pool, which includes 52 questions related to the psycho-social and behavioral presentations of BQUD. All participants, in a self-administered manner, completed the item pool. A subsample completed the re-test one week later. Two psychiatrists interviewed all participants to ascertain the presence of BQUD. The receiver Operating Characteristic curve was used to determine the best cut-off value to discriminate BQUD.
Results: One hundred and twelve BQCers were recruited. Based on the statistical analysis of receiver operating characteristic (ROC) curves, 14 yes/no questions were selected for SST-BQUD. As indicated by Cronbach’s α coefficient, the internal consistency was 0.876. The area under the curve of SST-BQUD was 0.881, representing a satisfactory diagnostic value. The one-week re-test reliability test was 0.771 (P< 0.001), suggesting good stability over time. The optimal cut-off score for BQUD screening was six, with a sensitivity of 0.921 and a specificity of 0.716, implying the satisfactory accuracy of SST-BQUD to screen for BQUD.
Conclusion: The standard version of SST-BQUD consists of 14 items. The total score of SST-BQUD was the sum of affirmative answers, with higher scores denoting a more severe BQUD symptom. If one answered six or more times “yes” to these 14 questions, they can be classified with BQUD. The SST-BQUD is a valid screening method for BQUD among BQCers in betel quid processed area.
Keywords: betel quid use disorders, screener, development, validity, diagnostic test
Introduction
Betel quid is the fourth most popular addictive substance in the world, following tobacco, alcohol, and caffeine.1 In 2020, the output of areca nut in the major producing areas in China was almost eight times that of 20 years ago.2 The effects of Betel quid chewing (BQC) are described as pleasurable and generally stimulating, inducing a sense of well-being, euphoria, heightened alertness, a warm sensation throughout the body, and an increased capacity to work.3 So, it causes drivers, labor workers, and adolescents to chew betel quid. In recent years, the current prevalence rates of BQC in Hunan China were 73.9% in drivers, 52.7% in labor workers, 49.7% in senior middle school students, 47.2% in secondary vocational school students, 40.8% in junior middle school students, 31.8% in pupils.4–6 The proportion of men chewing betel quid is significantly higher than that of women.7
The areca nut is classified as a Group 1 human carcinogen.8 Evidence has shown that BQC is associated with an increased risk of many adverse health outcomes, including oral submucous fibrosis, oral cancers, chronic kidney disease, coronary artery disease, and premature deaths.9–11 The risk of oral and pharyngeal cancer increased with increasing daily amount and duration (years) of chewing betel quid.12 As of 2016, BQC caused close to 25,000 cases of oral cancer in Hunan, China, resulting in about ¥5 billion in accumulated financial loss.13 Therefore, BQC has been a significant public health challenge in China, particularly in China’s southern regions, with the custom of BQC.14
Empirical data suggest that despite increasing awareness of the health risk of BQC and having suffered from oral diseases, the betel quid chewers (BQCers) still chew betel quid.15,16 Relieving fatigue, betel addiction, and social needs (exchanging packaged betel areca products in social situations is etiquette in some parts of southern China) are commonly reported reasons for using betel quid in China.15 In terms of prevention and intervention programs for betel quid cessation, it is essential to identify whether a chewer has a betel quid use disorder (BQUD) that is defined by the inability to control the use of betel quid despite harmful consequences. Unfortunately, due to inadequate mental health services resources, psychiatric assessment by mental health workers is not feasible for large-scale population-based intervention programs. In response to that, a brief, reliable and valid self-report measure for screening for and assessing the severity of BQUD helps address this issue.
Until now, Chinese researchers have developed some self-rating scales to screen for BQUD: the Self-report Screening Test for Areca-quid Abuser (SSTAA), Betel Quid Dependence Instrument (BQDI), and Betel Quid Dependence Scale (BQDS).17–19 However, these scales are designed for BQCers in fresh areca nuts use areas. Due to their short shelf life, fresh areca nuts are only available in the tropical regions of their origin. Inland China consumers prefer chewing processed betel quid products, consisting of dried areca nuts, spices, sugar, and rosewater or other additives that are manufactured industrially and marketed commercially.20 In traditional Chinese medicine, dried areca nut is recommended for improving digestion and maintaining good health. Areca nuts are often exchanged as gifts, perceived as a token of love or friendship in China. The exchange of processed betel quid on social occasions has become a local social etiquette.20 Due to the different areca-cultural and ingredients of popular betel quid, these available scales may not be applicable for screening BQUD in areca non-plant areas. A particular version of the betel quid screening test is necessary for clinical practice.
Based on previous works and the urgent need for contemporary screening tests, we developed the Self-administered Screening Test for BQUD (SST-BQUD). Further, we tested its reliability and validity among a sample of BQCers in Hunan, China.
Methods
Participants
From November to December 2010, we recruited a convenience sample of BQCers from Hengyang, China. Hengyang is an extensive inland municipality in Hunan province. In 2018–19, the overall prevalence of BQC in Hengyang residents was as high as 27.4%.5 Based on the findings from our pilot study, the prevalence of BQUD in BQCers was 30%, the response rate was 80%, and the sensitivity and specificity of the SST-BQUD were 80% and 80%, respectively. A total sample size of 104, including 35 BQCers with BQUD, was obtained by using the formula for estimating the sample size for a diagnostic test, which achieved 91% power to detect a change in sensitivity from 0.5 to 0.8 using a two-sided binomial test and 100% power to detect a change in specificity from 0.5 to 0.8 using a two-sided binomial test. The target significance level is 0.05.
Adults 18 or older who reported “often chewing betel quid” and voluntarily participated in this study were recruited from local communities. Written informed consent was collected from all participants. There was no pre-existing relationship between participants and investigators. The study was approved by the Institutional Review Board of Peking University Sixth Hospital (No.2010-50). All procedures were tightly followed the guidelines of the Declaration of Helsinki.
Instruments and Procedures
After informing the authors with verbal permission, researchers introduced the initial screening test used to develop the Self-report Screening Test for Areca quid Abusers (SSTAA)17 as our item pool. There were a total of 52 yes/no questions in the initial screening test, which were developed based on the diagnostic criteria for substance use disorders in SCAN (Schedules for Clinical Assessment in Neuropsychiatry),21 ICD-10 (Clinical descriptions and diagnostic guidelines: The ICD-10 Classification of Mental and Behavioral disorder),22 and DSM-IV (Diagnostic and Statistical Manual of Mental disorders).23 These questions included: (1) the onset age and frequency (4 questions); (2) subjective craving and feeling (7 questions); (3) social problems due to betel quid chewing (7 questions); (4) physical problems due to betel quid chewing (11 questions); (5) oral symptoms (4 questions); (6) psychological and abstinence-related problems (12 questions);(7) the motivation and capacity to abstain (7 questions).17 This simplified Chinese item pool was further pilot-tested, and necessary modifications were made to ensure cultural appropriateness and clarity. The item pool was completed by all participants in a self-administered manner. In addition, trained investigators were arranged to read questions for people having difficulties completing the questionnaire.
To ascertain the presence of BQUD, all participants were interviewed with Structured Clinical Interview for DSM-IV-TR Axis I Disorders (SCID-I) by two experienced psychiatrists trained before the formal study and blinded to the test results of the item pool. We define individuals with BQUD as users of betel quid who met the diagnostic criteria for substance use disorders of DSM-IV by SCID-I. To examine the re-test reliability, a subsample of the BQCers were invited to complete the item pool again one week after the first administration.
Statistical Analysis
The statistical analysis strategy aims to identify a set of screening questions that can best discriminate participants with and without BQUD. The Chi-square test was used to compare the proportions of affirmative answers to item pool questions between participants with and without DSM-IV BQUD. Items with statistically significant differences consisted of the preliminary version of the SST-BQUD. In the reliability analysis, we deleted items with corrected item-total correlation coefficients <0.30, and the final version of SST-BQUD was generated.
Cronbach’s α coefficient was calculated to assess the internal consistency of SST-BQUD. Pearson correlation coefficient of the total scores between the first and second administrations was used to evaluate the re-test reliability. The Receiver Operating Characteristic (ROC) curve was used to determine the best cut-off value to discriminate BQUD. Corresponding area under the curve (AUC), sensitivity, specificity, and Youden’s index were also calculated. SPSS software version 22.0 was used to analyze the data. All tests were two-tailed, and the significance level was P<0.05.
Results
Sample Characteristics
In total, 112 BQCers completed the item pool, and 32 BQCers completed the re-test of SST-BQUD one week later. The mean age of the 112 BQCers was 33.7 years (range: 19–57, standard deviation [SD]: 8.4), and 107 (95.5%) were male. The average length of chewing was 91.2 months (range: 6–336, SD: 67.3), and the frequency of chewing was 5.9 per week (range: 1–7, SD: 1.9). Of the 112 BQCers, 38 BQCers met the DSM-IV criteria for BQUD. Demographic data regarding BQCers are shown in Table 1. The consumption of betel quid between the groups with or without BQUD is compared in Table 2.
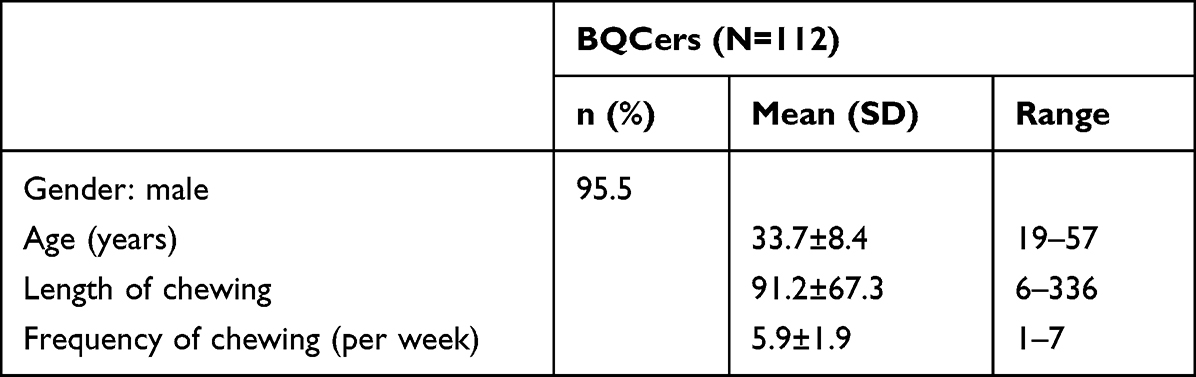 |
Table 1 Demographic Data and Characteristics of BQCers |
 |
Table 2 Consumption of Betel Quid Between the Groups with or Without BQUD |
The Development of SST-BQUD
Chi-square test results showed that BQCers with and without BQUD differed significantly in 15 items (χ2=4.149–23.076, P≤0.023). After removing an item with a corrected item-total correlation coefficient of 0.299, 14 items were retained and consisted of the standard version of SST-BQUD (Table 3). Six items are about subjective craving and feeling, five are about social problems due to betel quid chewing, one item on physical problems due to betel acid chewing, one item on oral problems due to betel quid chewing, and one item on psychological and abstinence-related problems. The total score of SST-BQUD was the sum of affirmative answers, with higher scores denoting more severe BQUD symptoms.
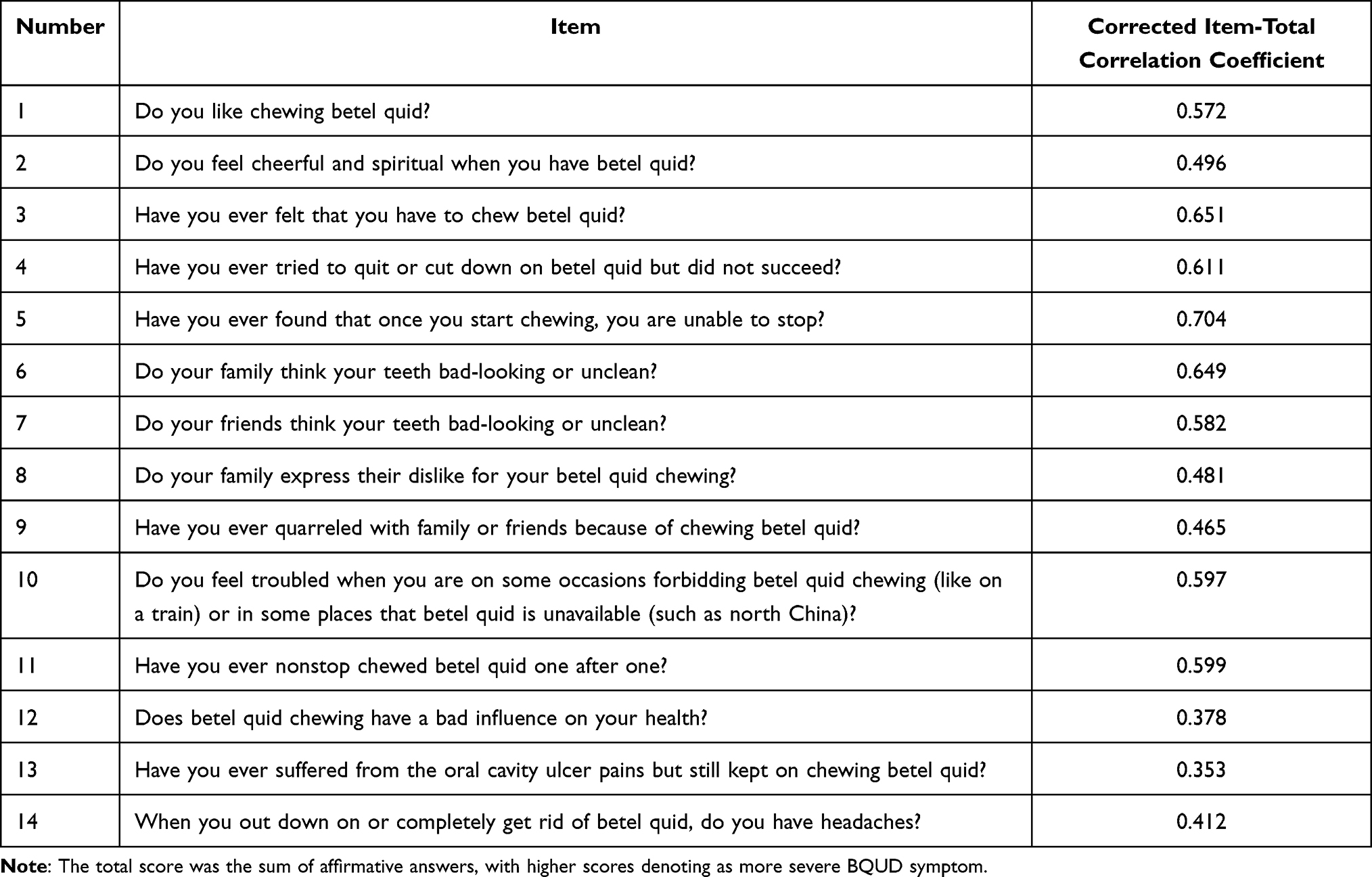 |
Table 3 The Self-Administered Screening Test for Betel Quid Use Disorders: Items and Corrected Item-Total Correlation Coefficients |
Reliability of SST-BQUD
Corrected item-total correlation coefficients of the 14 items of SST-BQUD ranged between 0.353 and 0.704, with a mean of 0.539 (Table 3). The Cronbach’s α coefficient was 0.876. The one-week re-test reliability test was 0.771 (P<0.001).
Validity of SST-BQUD
The AUC of SST-BQUD was 0.881. As shown in Table 4, the highest Youden’s index was achieved when the cut-point was set at 6, with a sensitivity of 0.921 and a specificity of 0.716. Hence, for the screening test SST-BQUD, if one answered six or more times “yes” to these 14 questions, they can be classified with BQUD.
 |
Table 4 The Identification of Cut-Point for the Self-Administered Screening Test for Betel Quid Use Disorders |
Discussion
The practice of chewing processed dried areca nut products in areca non-plant areas in China is unique in the world.20 Along with recent progress in food manufacturing industrialization, processed betel products have spread to nearly all areas of China. Betel nut-associated oral cancer cases also have been increasing rapidly in the past years in China.13 In 2019, the Ministry of Public Health of China presented the Healthy Oral Action Program (2019–2025), which focuses on the long-term oral health consequences of betel quid chewing and proposed targeted education and oral health examinations to promote early diagnosis and treatment of periodontal disease in areas where chewing betel quid is common.24
Our study is the first work to provide a reliable and valid screener for BQUD that is more adaptive to areca non-plant areas. Items in SST-BQUD seem to be consistent with the clinical presentations of BQUD, suggesting good face validity. For example, item 2 reflects the feeling of euphoria that a BQCer has, item 3 measures the patient’s craving for betel quid, item 10 measures the severity of psychological withdrawal symptoms, item 11 measures the presence of compulsive betel-taking behavior, and items 6–9 investigates social malfunction due to problematic betel quid use (Table 3). Because these items measure different aspects of BQUD and are specific to BQUD, it is reasonable to find a high internal consistency of SST-BQUD (α = 0.876). The AUC value of 0.881 in our study represents the satisfactory diagnostic value of a screening test. Accordingly, the SST-BQUD has an excellent practical value for screening for BQUD. This may be explained by the comprehensive and specific items of SST-BQUD. The cut-off score of six SST-BQUD results in high sensitivity (0.921), while the corresponding specificity seems slightly low (0.716). Given the deleterious outcomes of BQUD, it is acceptable to have a slightly over-inclusive criterion for BQUD screening. In sum, the high sensitivity and specificity imply the strong ability of SST-BQUD to apply to its target population. The one-week re-test reliability test of 0.771 also entails a fair level of reliability, which could be helpful for further studies in the future.
Researchers introduced the initial screening test used to develop SSTAA,17 which included 52 questions based on the SCAN, ICD-10, and DSM-IV. Despite the same item pool used, the standard version of SST-BQUD in our study is different from SSTAA. We speculated that this might be primarily due to the different areca-cultural and ingredients of popular betel quid. Secondly, methodological differences in screening the patients and their level of betel quid use disorder may also explain this difference in item selection. For example, the authors of SSTAA used the unstructured clinical interview to diagnose betel quid abuse, but our research team used a stricter instrument, SCID-I. Both SST-BQUD and SSTAA are developed for community BQCers as an instrument of self-administered screening. They both include several “subjective craving and feeling” questions, of which SST-BQUD has six questions, and SSTAA has five. From the information above, it can be assumed that the pool of entries designed in accordance with ICD-10 and DSM- IV in the Chinese-speaking region has similar good suitability for the subjective craving and feeling of betel nut chewing.
There are two differences between SST-BQUD and SSTAA.17 The first one is that some questions entered SST-BQUD but not SSTAA: four “social problems due to betel quid chewing”, one “subjective craving and feeling”, one “physical problems due to betel acid chewing”, one “oral problems due to betel quid chewing” and one “psychological and abstinence related problems”. Second, some questions which were in SSTAA did not enter SST-BQUD: “psychological and abstinence related problems” (2 questions), “oral problems due to betel quid drinking” (3 questions), “the motivation and capacity to abstinence” (1 question).
From the above two differences, it can be considered that item “social problems due to betel quid chewing” have a more significant impact on BQCers in areca non-plant areas, while item “oral problems due to betel quid chewing” have a greater impact on BQCers in areca plant areas. Betel quid chewing has social and cultural characteristics, such as being a method of interpersonal communication. Consumers chew fresh areca nuts in areca plant areas, which is less convenient in interpersonal communication than processed betel nuts. Inland provinces, on the other hand, have a habit of eating processed betel nuts which are easier to carry and exchange in social situations. Handing betel nut to each other when meeting even becomes an essential interpersonal communication behavior. Accordingly, among the millions of people who chew processed betel nut in areca non-plant areas, it would be better to use the screening questionnaire with items like “social problems due to betel quid chewing” for it better identifies the abusive behavior of chewers and better reflects the use of screening scale.
The current study has some limitations. Our survey was conducted in 2010. Times have changed, which may affect the application of this screener. However, there is no noticeable change in the use pattern of betel quid in areca non-plant areas, and the research methodology is not outdated. The SST-BQUD is still a valid screening instrument for BQUD, but it may need to be revised in future practice. The sample size was relatively small (n=112). The sample of BQCers was not randomly selected from communities, so the majority of participants were male, and the sample representativeness of our sample may be limited.
Despite the limitations stated above, our findings suggest that SST-BQUD is a reliable and valid scale for screening BQUD among BQCers in betel quid processed areas. Based on our experiences, in summary, the test can be completed by self-administered in five minutes, so it is also user-friendly. The SST-BQUD has excellent potential for public health research and intervention programs aiming at reducing betel quid use in the Chinese population.
Conclusion
The standard version of SST-BQUD consists of 14 items. The total score of SST-BQUD was the sum of affirmative answers, with higher scores denoting a more severe BQUD symptom. If one answered six or more times “yes” to these 14 questions, they can be classified with BQUD. The SST-BQUD is a valid screening method for BQUD among BQCers in betel quid processed areas.
Acknowledgments
We would like to thank Yuan-Hwa Chou MD, PhD for helping us acquire the permission of the item pool to develop SSTAA. We are also grateful to Baoliang Zhong PhD and Kai-Yuan Luo for proof reading. This work is supported by WHO:To Develop Resource Materials on Mental health to Support a Pilot Study of Early Recognition and Intervention of Depression in the Workplace. It is also supported by the Department of health of Hainan Province, PRC:Research on mental health development planning in Hainan Province and the Ministry of Land and Resources, PRC (No. 200220190002).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Chen PH, Mahmood Q, Mariottini GL, Chiang TA, Lee KW. Adverse Health Effects of Betel Quid and the Risk of Oral and Pharyngeal Cancers. Biomed Res Int. 2017;2017:3904098. doi:10.1155/2017/3904098
2. Hainan Provincial Bureau of Statistics Survey Office of National Bureau of Statistics in Hainan. Hainan statistical yearbook 2007–2021; 2022. Available from: http://stats.hainan.gov.cn/tjj/tjsu/ndsj/.
3. Cox S, Ullah M, Zoellner H. Chapter 78 - oral and systemic health effects of compulsive areca nut use. In: Preedy VR, editor. Neuropathology of Drug Addictions and Substance Misuse. San Diego: Academic Press; 2016:785–793.
4. Fan XH, Nie XW, Chen FJ. Effect of parental and peers’ factors on adolescent areca quid chewing behavior. Chin J Clin Psychol. 2019;27(1):119–123.
5. Xu XM, Wang C, Zhang Y, Zhu ZH, Dong SQ, Huang B. Investigation on the status and influencing factors of chewing betel nuts among residents aged 15 years and above in Hengyang city. J Occupat Health Damage. 2020;2020(35):20–24.
6. Zeng Z, Zhang TC, Li K, Kang J. Current situation and influencing factors of betel nut chewing behavior among students in secondary vocational schools in Xiangxi Autonomous Prefecture. Henan J Prevent Med. 2019;30(8):572–575.
7. Central South University. Epidemiological Investigation of Betel Nut Chewing in Changsha, Hunan. Changsha, China: Central South University; 2010.
8. IARC Working Group on the Evaluation of Carcinogenic Risks to Humans. Betel-quid and areca-nut chewing and some areca-nut derived nitrosamines. IARC Monogr Eval Carcinog Risks Hum. 2004;85:1–334.
9. Garg A, Chaturvedi P, Gupta PC. A review of the systemic adverse effects of areca nut or betel nut. Indian J Med Paediatr Oncol. 2014;35(1):3–9. doi:10.4103/0971-5851.133702
10. Wang M, Yu SY, Lv ZT, Yao Y. Betel nut chewing and the risk of chronic kidney disease: evidence from a meta-analysis. Int Urol Nephrol. 2018;50(6):1097–1104. doi:10.1007/s11255-018-1819-8
11. Yamada T, Hara K, Kadowaki T, Bayer A. Chewing betel quid and the risk of metabolic disease, cardiovascular disease, and all-cause mortality: a meta-analysis. PLoS One. 2013;8(8):e70679. doi:10.1371/journal.pone.0070679
12. Guha N, Warnakulasuriya S, Vlaanderen J, Straif K. Betel quid chewing and the risk of oral and oropharyngeal cancers: a meta-analysis with implications for cancer control. Int J Cancer. 2014;135(6):1433–1443. doi:10.1002/ijc.28643
13. Hu YJ, Chen J, Zhong WS, et al. Trend analysis of betel nut-associated oral cancer and health burden in China. Chin J Dent Res. 2017;20(2):69–78. doi:10.3290/j.cjdr.a38271
14. Zhang X, Reichart PA. A review of betel quid chewing, oral cancer and precancer in Mainland China. Oral Oncol. 2007;43(5):424–430. doi:10.1016/j.oraloncology.2006.08.010
15. Shao XJ, Wang JZ, Lin XZ, Han XD, Xi Q, Liang LM. Epidemiological investigation and analysis of betel nut chewing and related oral diseases in Sanya. China Trop Med. 2018;18(10):994–998, 1028.
16. Zhong BL, Chen SL, Tu X, Conwell Y. Loneliness and cognitive function in older adults: findings from the Chinese longitudinal healthy longevity survey. J Gerontol B Psychol Sci Soc Sci. 2017;72(1):120–128. doi:10.1093/geronb/gbw037
17. Chen MJ, Yang YH, Shieh TY. Evaluation of a self-rating screening test for areca quid abusers in Taiwan. Public Health. 2002;116(4):195–200. doi:10.1016/S0033-3506(02)90066-1
18. Lee CY, Chang CS, Shieh TY, Chang YY. Development and validation of a self-rating scale for betel quid chewers based on a male-prisoner population in Taiwan: the Betel Quid Dependence Scale. Drug Alcohol Depend. 2012;121(1–2):18–22. doi:10.1016/j.drugalcdep.2011.07.027
19. Tsai MH, Li TC, Li CI, et al. Development and preliminary validation of a mandarin Chinese language questionnaire measuring betel quid dependency among adults in Taiwan. Psychiatry Res. 2019;271:153–160. doi:10.1016/j.psychres.2018.11.027
20. Yu C. Two Thousand Years of Chewing: The Prevalent History of Areca Nut in China. China CITIC Press; 2022.
21. Wing JK, Babor T, Brugha T, et al. SCAN. schedules for clinical assessment in neuropsychiatry. Arch Gen Psychiatry. 1990;47(6):589–593. doi:10.1001/archpsyc.1990.01810180089012
22. World Health Organization. Clinical Descriptions and Diagnostic Guidelines: The ICD-10 Classification of Mental and Behavioral Disorder, 10th Revision.
23. American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders.
24. Ministry of public health of china healthy oral action program (2019–2025); 2019. Available from: http://www.gov.cn/xinwen/2019-02/16/content_5366239.htm.
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.