Back to Journals » Risk Management and Healthcare Policy » Volume 19
Development and Validation of a Robust Prediction Model for Postoperative Pneumonia in Elderly Patients with Hip Fracture: Integrating Frailty, Nutrition, and Comprehensive Risk Assessment
Authors Ma L, Tu J, Fu Y, Guan L, Tian Z
Received 3 June 2025
Accepted for publication 21 December 2025
Published 7 June 2026 Volume 2026:19 532215
DOI https://doi.org/10.2147/RMHP.S532215
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Gulsum Kaya
Liping Ma, Jiahong Tu, Yan Fu, Lan Guan, Zhaoxing Tian
Department of Emergency Medicine, Beijing Jishuitan Hospital, Capital Medical University, Beijing, People’s Republic of China
Correspondence: Zhaoxing Tian, Department of Emergency Medicine, Beijing Jishuitan Hospital, Capital Medical University, No. 31 Xinjiekou East Street, Xicheng District, Beijing, 100035, People’s Republic of China, Email [email protected]
Objective: To develop and rigorously validate a multivariable prediction model for postoperative pneumonia (POP) in elderly patients with hip fracture by integrating the five-item modified frailty index (5‑mFI), the Geriatric Nutritional Risk Index (GNRI), and various clinical variables, with comprehensive assessment of model performance.
Methods: We conducted a retrospective cohort study of 2183 patients aged ≥ 65 years undergoing hip fracture surgery. Predictors included comorbidities, laboratory values (including partial pressure of oxygen [PO2], B-type natriuretic peptide [BNP], and GNRI), and the 5-mFI. We employed multivariable logistic regression to develop original and extended models, the latter adjusting for functional status and perioperative factors. Model performance was evaluated via area under the curve (AUC), bootstrap-corrected AUC, calibration, and decision curve analysis. Time-to-event and competing risk analyses were performed, and machine learning models (Random Forest, XGBoost) were compared.
Results: The extended logistic regression model identified chronic obstructive pulmonary disease (odds ratio [OR]=2.60), postoperative intensive care unit admission (OR=2.72), lower PO2 (OR=0.987), lower GNRI (OR=0.871), higher 5-mFI (OR=1.94), and higher BNP (OR=1.000) as independent predictors. The model demonstrated robust discrimination (AUC=0.781; bootstrap-corrected AUC=0.773), good calibration, and clinical utility. Results were consistent in competing risk analysis and robust to multiple imputation of missing data. Machine learning models confirmed GNRI and 5-mFI as top predictors, with comparable yet miscalibrated performance (XGBoost corrected AUC=0.791).
Conclusion: We developed and internally validated a robust prediction model for POP that integrates frailty, nutrition, and key clinical variables. The model demonstrates strong, validated performance and clinical utility, providing a practical tool for preoperative risk stratification to guide targeted preventive measures in elderly patients with hip fracture.
Keywords: hip fracture, postoperative pneumonia, frailty, nutritional status, risk prediction model, machine learning
Introduction
The incidence of hip fractures is rising globally among older adults, projected to reach 5 million cases by 2050. Surgical intervention remains the cornerstone of management to improve outcomes in this age group. Nonetheless, older adults face elevated rates of postoperative complications due to diminished physiological reserves, frailty, and nutritional deficits. These complications may include postoperative disability, cardiovascular and cerebrovascular issues, depression, and even mortality.1 Consequently, it is imperative for healthcare professionals to promptly and accurately assess the risk of postoperative complications following hip fractures in older patients.
Postoperative pneumonia (POP) frequently affects this population, with reported incidence ranging from 5.1% to 14.9%.2–4 Treatment typically includes antibiotics and supportive care, yet these approaches may be insufficient due to the intricate physiological aspects and concurrent health issues related to ageing.5 This can impede recovery post-surgery, prolong hospital stays, increase medical costs, and potentially lead to fatalities,6,7 causing physical distress to patients and financial strain on healthcare systems. Therefore, it is crucial to identify the risk factors linked to POP and establish proactive strategies to improve patient prognosis. Numerous research studies have explored various patient characteristics and risk factors linked to the development of POP. Factors including age, gender, body mass index (BMI), living conditions, and a variety of biological markers have been recognised as key elements influencing the risk of post-surgery pneumonia.8 Notably, studies have emphasised the substantial impact of concurrent conditions such as chronic obstructive pulmonary disease (COPD) and hypertension, prevalent in older patients, which markedly increase the likelihood of postoperative complications.9 Furthermore, the significance of nutritional status, assessed through, for example, the Geriatric Nutritional Risk Index (GNRI) and biomarkers such as serum albumin levels, has emerged as a crucial area of interest, shedding light on the intricate relationship between nutritional inadequacy and infection risk.10 These research findings stress the importance of comprehending the interaction between patient characteristics and comorbid conditions in the realm of POP, thus highlighting the potential for improved clinical decision-making and risk assessment.
The five-item modified frailty index (5-mFI) and GNRI are two promising, easily obtainable tools that respectively assess the comorbidity burden and nutritional risk in elderly patients.11,12 While individually associated with postoperative outcomes, the potential synergistic value of combining these geriatric-specific metrics with established clinical risk factors to predict POP in hip fracture patients remains to be established. Therefore, the primary aim of this study was to develop and validate a multivariable prediction model for POP in elderly patients undergoing hip fracture surgery by integrating the 5-mFI, GNRI, and other relevant clinical variables. We hypothesized that a composite model would provide superior predictive performance compared to individual factors alone, ultimately aiming to aid in preoperative risk stratification and identify high-risk patients who might benefit from intensified prophylactic measures.
Materials and Methods
Methods
We conducted a retrospective analysis of patient records from January 2019 to December 2020 at Beijing Jishuitan Hospital, Capital Medical University, including all individuals aged ≥65 years who underwent hip fracture surgery.
Patients were eligible if they presented within 3 weeks of fracture; cases of fractures older than 3 weeks, pathological or periprosthetic femoral fractures, multiple or open fractures, preoperative pneumonia, haematological or autoimmune disorders (eg leukaemia, rheumatoid arthritis, systemic lupus erythematosus), nonoperative management, or cases with incomplete data were excluded. A total of 2183 patients met these criteria and were included in subsequent analyses. The study received approval from the Ethics Committee of Beijing Jishuitan Hospital, Capital Medical University, and was conducted in accordance with the ethical standards of the Declaration of Helsinki. The requirement for individual informed consent was waived by the ethics committee due to the retrospective nature of the study. Only patient clinical data will be collected, without interfering with the patient’s treatment plan, and there will be no physiological risks to the patient. The researchers will make every effort to protect the information provided by the patients from disclosing personal privacy. All patient data were anonymised and de-identified prior to analysis to ensure confidentiality and privacy.
Data Collection
The collected demographical variables comprised age, sex, BMI, living status, preoperative ambulatory status (categorised as independent community ambulator or limited community/household ambulator), and a socioeconomic proxy (insurance type, categorised as basic medical insurance or other/self-pay). We also recorded the time from fracture to surgery and the length of hospitalisation.
We recorded comorbidities, including hypertension, diabetes, COPD, congestive heart failure, stroke, chronic liver disease, chronic kidney disease, and malignancy. Behavioural factors, such as current smoking status and alcohol use, were also extracted from medical records.
Perioperative details encompassed fracture type, American Society of Anesthesiologists (ASA) classification, surgical approach, anaesthesia modality, anaesthesia duration, operative time, intraoperative blood loss, postoperative ICU monitoring, and transfusion requirements. The duration of prophylactic antibiotic use (categorised as ≤24 or >24 hours) was recorded as a key perioperative management variable.
Laboratory parameters measured preoperatively included white and red blood cell counts, neutrophil and lymphocyte count, haemoglobin, platelets, total protein, albumin, total bilirubin, blood glucose, creatinine, BNP, and arterial blood gas values (pH, PO2, PCO2, lactate, SpO2), along with calculation of the 5‑mFI and GNRI.
All data collectors received standardised training, and entries were independently duplicated and cross‑checked, with discrepancies resolved by consensus.
Calculation of the Risk Score
The 5-mFI was chosen due to its validated ability to assess frailty and comorbidity burden in elderly surgical populations, and the GNRI was selected for its established role in evaluating nutritional risk, a critical factor in postoperative recovery. These indices were prioritised based on their clinical relevance, ease of calculation, and prior evidence linking them to postoperative complications.
The 5-mFI includes five variables: congestive heart failure, COPD, hypertension requiring medication, diabetes, and non-independent functional status. Each variable contributes 1 point, resulting in an index score ranging from 0 to 5.
The GNRI is calculated using the following formula:
GNRI = [1.489×albumin (g/L)]+[41.7×(weight/WLo)].13
Here, WLo represents the ideal weight calculated using the Lorentz formula, and if the actual weight exceeds this value, we set WLo = 1, following the approach outlined by Buzby et al (Note: Buzby originally used usual weight instead of WLo).14
Postoperative pneumonia is defined as the appearance of new infiltrates on postoperative chest X-rays or chest computed tomography scans, accompanied by respiratory symptoms and signs, or confirmed by a pulmonologist’s consultation and diagnosis. The diagnosis of POP follows the criteria set out in the American Thoracic Society (ATS) guidelines for healthcare-associated pneumonia,15 which include the following: 1) new and/or progressive respiratory symptoms such as cough and purulent sputum; 2) postoperative fever (body temperature >38.0°C) or hypothermia (body temperature <36.0°C); 3) physical examination findings indicating lung consolidation and auscultatory crackles; 4) white blood cell count exceeding 10×109/L or falling below 4×109/L; and 5) identification of patchy inflammatory shadows or interstitial changes on chest X-rays.
A diagnosis of POP is made if the patient meets any of criteria 1 to 4, along with criterion 5, provided that other pulmonary conditions, such as lung cancer, tuberculosis, or pulmonary embolism, have been excluded. The assessment of POP as the primary outcome is conducted from the first 24 hours after surgery until discharge. Diagnoses are performed by a specialised team of pulmonologists and radiologists at Beijing Jishuitan Hospital, following standardised ATS guidelines to ensure accuracy and consistency in diagnosis.
Statistical Methods
All statistical analyses were performed using IBM SPSS Statistics (version 22.0) and R software (version 4.5.0; R Foundation for Statistical Computing). A two-sided P-value <0.05 was considered statistically significant. Continuous variables were tested for normality using the Shapiro–Wilk test. Normally distributed data were presented as mean ± standard deviation and compared using the Student’s t-test, whereas non-normally distributed data were summarised as medians with interquartile ranges (IQR) and compared using the Mann–Whitney U-test. Categorical variables were expressed as counts (percentages) and compared using the chi-square test or Fisher’s exact test, as appropriate.
The pattern and proportion of missing data were assessed for all variables. To handle missing data, we employed multiple imputation by chained equations (MICE) to create 20 complete datasets under the missing-at-random assumption. The imputation model included all variables from the final extended model and the outcome variable. Results from the pooled analyses of the imputed datasets are presented alongside the complete-case analysis as a sensitivity analysis.
Multiple predictive models were developed using different statistical approaches. Multivariable logistic regression was used to identify independent predictors of POP, with two primary models constructed: an original model with pre-specified predictors and an extended model that additionally adjusted for potential confounders. Multicollinearity was assessed using variance inflation factors (VIF), with values >5 indicating significant collinearity. To account for variable follow-up time, time-to-event analyses were performed using Kaplan–Meier curves, with Log rank tests for group comparisons, multivariable Cox proportional hazards regression, and Fine–Gray competing risk regression to account for in-hospital death as a competing event. Additionally, to complement the regression-based approaches, we trained two ensemble machine learning models: Random Forest (RF) and XGBoost. Both models were trained using the same predictor set as the extended logistic regression model. Hyperparameters for both models (eg number of trees, maximum depth, learning rate for XGBoost) were optimised via randomised search with five-fold cross-validation. The feature importance derived from these models was analysed and reported.
Model performance was evaluated on a randomly split test set (30% of data). Discrimination was assessed using the area under the ROC curve (AUC), with sensitivity, specificity, and their 95% confidence intervals (CIs) reported at the optimal cutoff, determined by maximising the Youden index. Internal validation and overfitting assessment were performed using bootstrap resampling with 1000 repetitions, with optimism-corrected AUC values reported. Calibration was evaluated using calibration plots and the Hosmer–Lemeshow goodness-of-fit test. Clinical utility across a range of decision thresholds was assessed using decision curve analysis.
Results
Patient Demographics and Clinical Characteristics
A total of 2183 patients met the inclusion criteria, with a mean age of 80 years; women comprised 71.3% of the cohort, and 75.6% were living independently prior to their fracture. Femoral neck fractures were the most common type, accounting for 55.1% of the cases, which is in line with the typical distribution of fracture types in the elderly population. Among the sample, 281 patients (12.9%) experienced POP. This incidence rate highlights the significant vulnerability of this population to postoperative complications, emphasising the need for improved risk assessment and preventive strategies.
Univariate analysis of baseline characteristics between patients with and without POP demonstrated significant differences concerning multiple variables (Table 1). Patients who developed POP were significantly older (median 83 vs 80 years, P<0.001), had lower BMI (median 21.51 vs 22.87, P<0.001), and were more likely to be men (37% vs 27.4%, P=0.001). Regarding functional status, patients with POP had higher rates of partial dependence in living conditions (32.7% vs 23.2%, P=0.001).
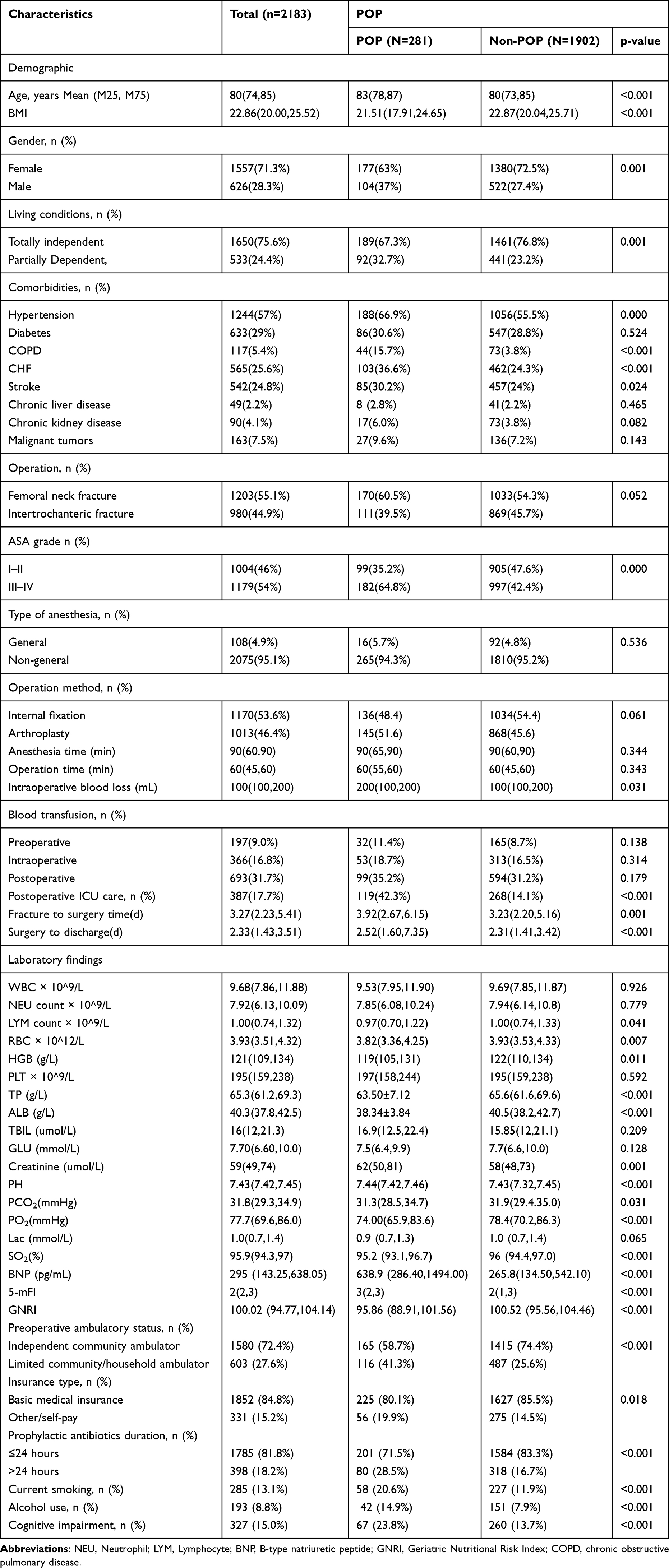 |
Table 1 Baseline Characteristics of the 2183 Patients with Hip Fractures |
Comorbidities were more prevalent in the POP group, including hypertension (66.9% vs 55.5%, P<0.001), COPD (15.7% vs 3.8%, P<0.001), congestive heart failure (36.6% vs 24.3%, P<0.001), and stroke (30.2% vs 24%, P=0.024). Surgical factors also differed significantly, with patients with POP having higher ASA grades (64.8% vs 52.4% for ASA III–IV, P<0.001), greater intraoperative blood loss (median 200 vs 100 mL, P=0.031), and more frequent postoperative ICU care (42.3% vs 14.1%, P<0.001). Time from fracture to surgery was longer in patients with POP (median 3.92 vs 3.23 days, P=0.001), as was postoperative length of stay (median 2.52 vs 2.31 days, P<0.001).
Laboratory parameters showed consistent patterns of compromise in patients with POP, with significantly lower lymphocyte counts, red blood cell counts, haemoglobin, total protein, albumin, and GNRI scores, alongside elevated creatinine and BNP levels (all P<0.05). Arterial blood gas analysis revealed lower PO2 (median 74.00 vs 78.4 mmHg, P<0.001) and SO2 (median 95.2% vs 96%, P<0.001) in patients with POP. The 5-mFI scores were significantly higher in the POP group (median 3 vs 2, P<0.001).
Multivariable Logistic Regression Models for Postoperative Pneumonia
Multivariable logistic regression was employed to identify independent predictors of POP. We constructed and compared two models (Table 2). The original model (Model 1) included the pre-specified predictors of interest: COPD, postoperative ICU care, PO2, GNRI, 5-mFI, and BNP. Prior to analysis, the VIFs for all variables in both models were below 2.0, indicating no concerning multicollinearity.
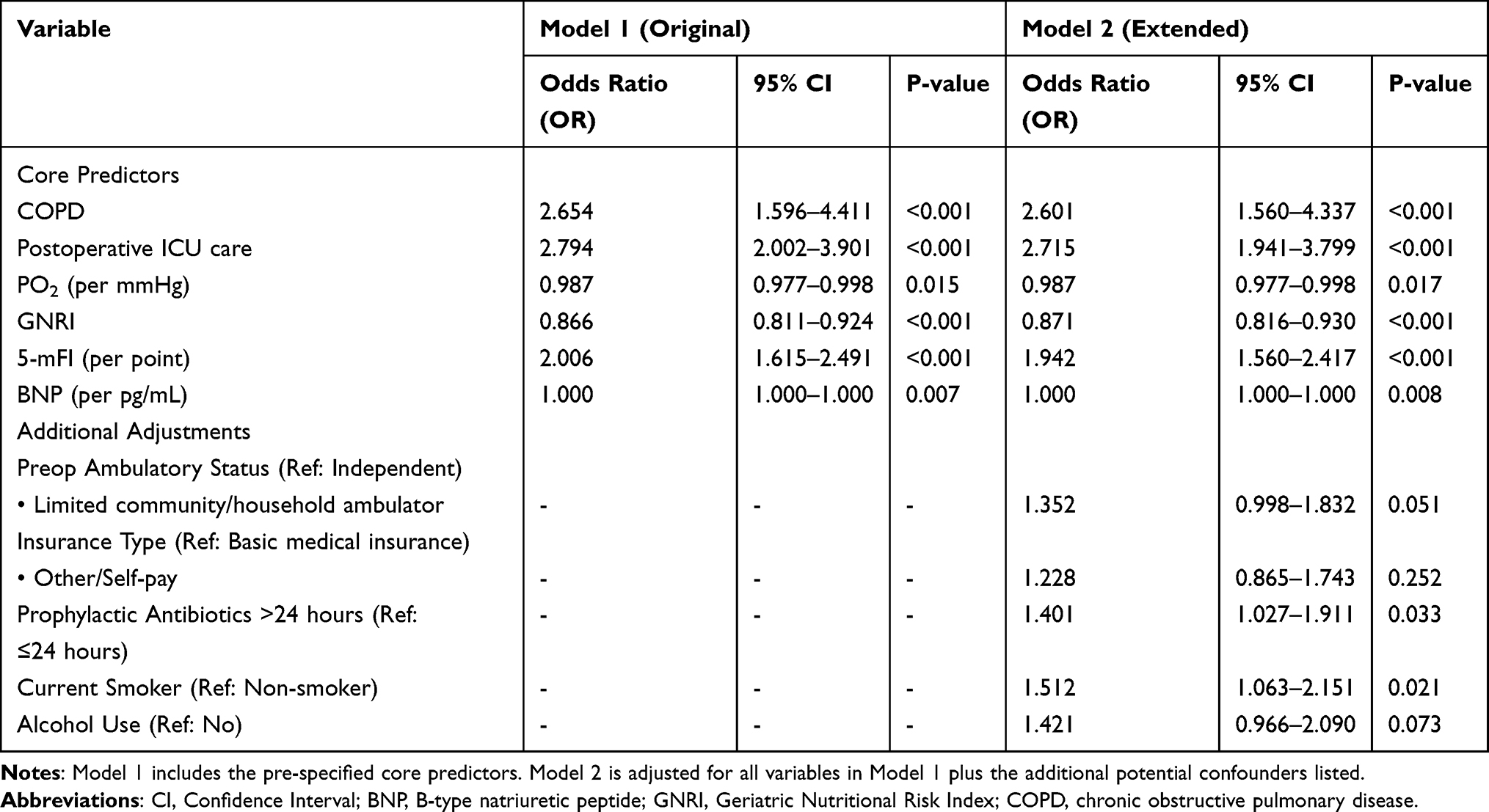 |
Table 2 Comparison of Multivariable Logistic Regression Models for Predicting Postoperative Pneumonia |
In Model 1, all six variables were independently associated with POP. The strongest predictors were postoperative ICU care (odds ratio [OR]=2.794, 95% CI: 2.002–3.901, P<0.001) and COPD (OR=2.654, 95% CI: 1.596–4.411, P<0.001). Each point increase in the 5-mFI was associated with a doubling of the odds of POP (OR=2.006, 95% CI: 1.615–2.491, P<0.001), whereas a higher GNRI was protective (OR=0.866, 95% CI: 0.811–0.924, P<0.001). Lower preoperative PO2 (OR=0.987, 95% CI: 0.977–0.998, P=0.015) and higher BNP levels (OR=1.000, 95% CI: 1.000–1.000, P=0.007) were also significant independent predictors.
To assess the robustness of these findings against potential confounding, we built an extended model (Model 2), which incorporated additional variables related to functional status, socioeconomic proxy, and perioperative management (specifically: preoperative ambulatory status, insurance type, prophylactic antibiotic duration, smoking history, and alcohol use). The results of Model 2 are presented in Table 2. Critically, the effect sizes and significance levels of the six core predictors remained largely unchanged after adjusting for these additional potential confounders. This consistency demonstrates the robustness of the original findings.
Sensitivity Analysis for Missing Data
To address the potential impact of missing data on the robustness of our findings, we performed a sensitivity analysis using multiple imputation. The variable with the highest proportion of missingness was BNP (12.5%), whereas all other variables had missing rates below 5%. We created 20 complete datasets using MICE, under the assumption that data were missing at random. The imputation model included all variables from the extended multivariable model (Model 2), as well as the outcome variable (POP).
The pooled results from the analyses of the 20 imputed datasets are presented in Table 3. Here, all six core predictors (COPD, postoperative ICU care, PO2, GNRI, 5-mFI, and BNP) retained their statistical significance, with ORs and CIs almost identical to those obtained from the complete-case analysis (Table 2, Model 2). The effect estimates for the additionally adjusted confounders also remained consistent. This high degree of concordance between the complete-case and multiple imputed analyses strongly suggests that our primary findings are robust to the missing data mechanism present in this cohort.
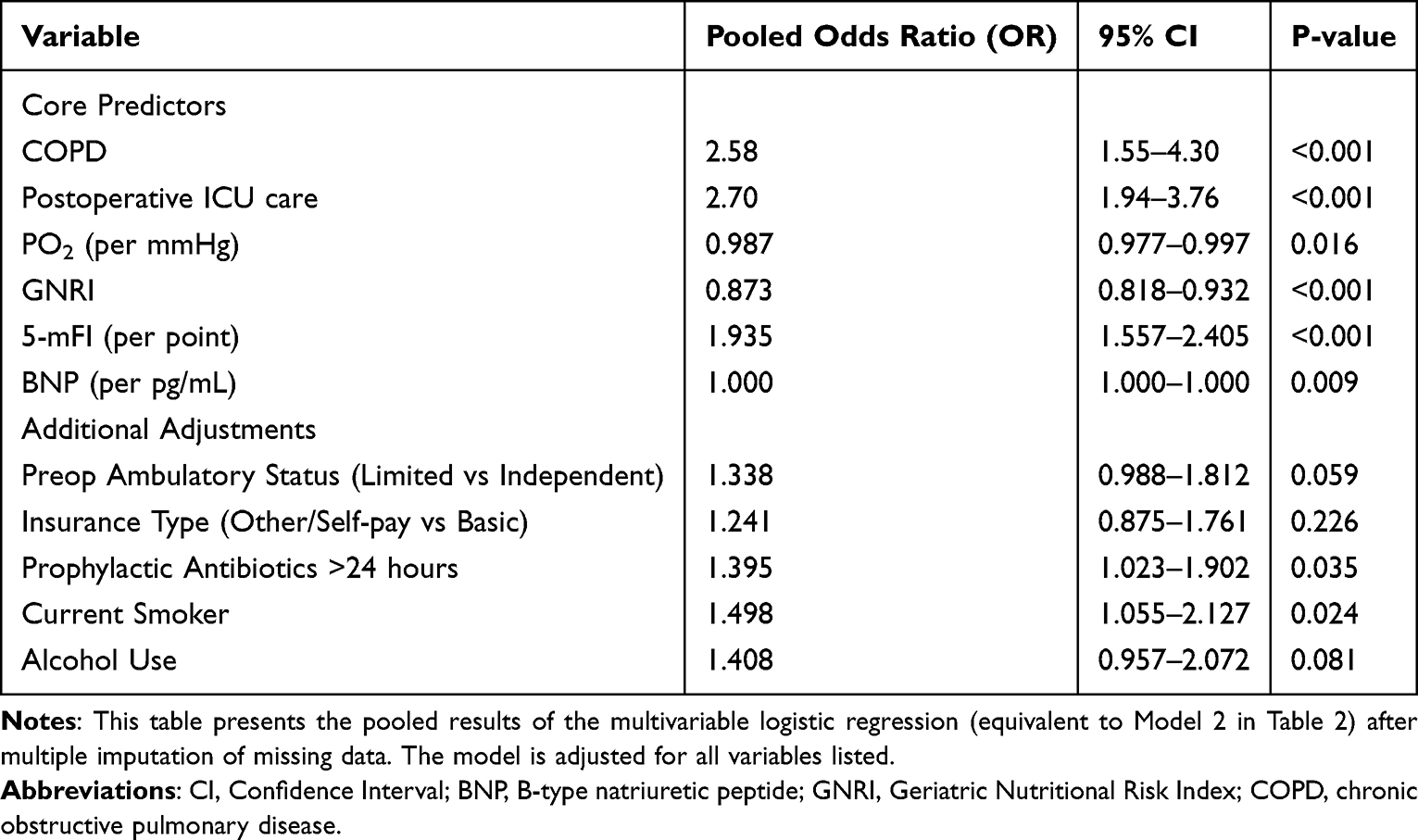 |
Table 3 Sensitivity Analysis: Pooled Results from Multiple Imputation (n=20 Imputed Datasets) |
Time-to-Event Analysis and Competing Risk Analysis
The median time from surgery to POP diagnosis was 3.5 days (IQR: 2.1–6.0 days). Kaplan–Meier curves demonstrated a significantly higher cumulative incidence of POP in patients with a 5-mFI≥2 than those with a 5-mFI<2 (Log-rank P<0.001) (Figure 1). The multivariable Cox and Fine–Gray models were adjusted for the same comprehensive set of variables as in the extended logistic regression model (Model 2).
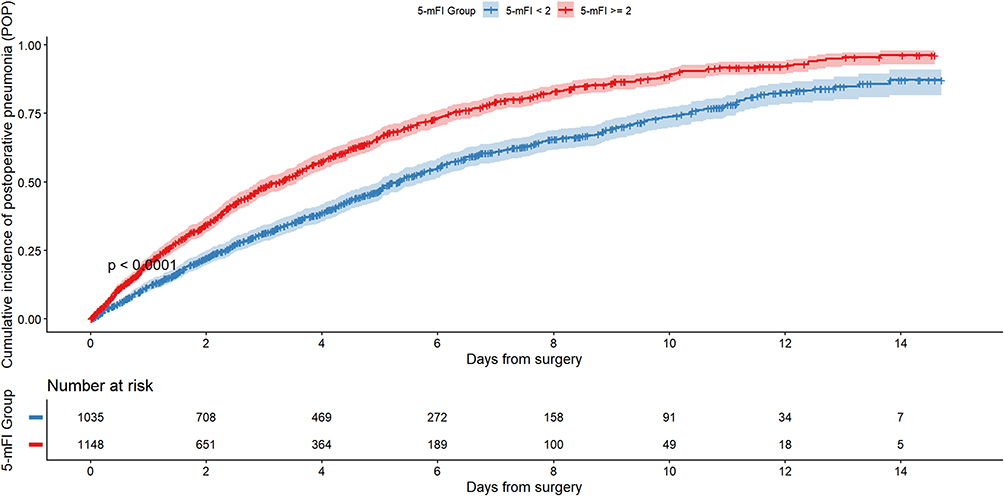 |
Figure 1 Kaplan-Meier curves of cumulative incidence of postoperative pneumonia (POP) within 15 days stratified by 5-mFI score group (< 2 vs ≥ 2). The y-axis represents cumulative incidence (1 − survival probability), and the x-axis shows days from surgery. Shaded areas 95% confidence intervals. Numbers at risk at each time point are displayed below the x-axis. The Log rank test was used to compare incidence between groups; the corresponding p-value is indicated on the plot. |
In the multivariable Cox proportional hazards model, COPD, postoperative ICU care, lower GNRI, higher 5-mFI, and higher BNP remained significantly associated with an increased hazard of POP over time. The Fine–Gray competing risk model, accounting for in-hospital death as a competing event, yielded qualitatively similar results, with all key predictors retaining statistical significance. However, as expected, the magnitude of association for most factors was slightly attenuated in the competing risk model compared with the Cox model, reflecting the adjustment for the competing risk of death (Table 4).
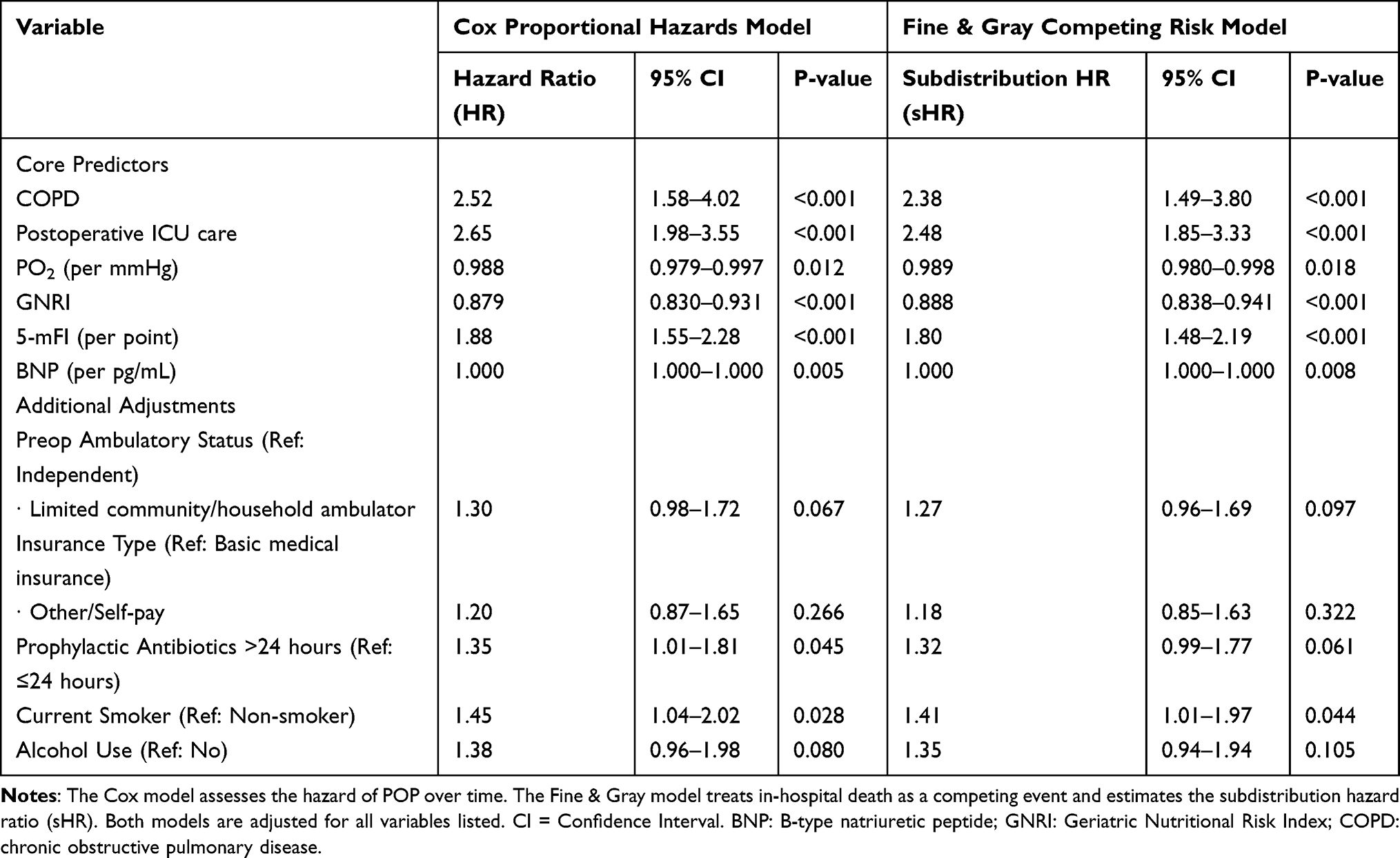 |
Table 4 Multivariable Time-to-Event Analysis for Predictors of Postoperative Pneumonia |
Comparison with Machine Learning Models and Comprehensive Performance Assessment
We evaluated the performance of the multivariable logistic regression models alongside two machine learning algorithms, RF and XGBoost. All models were trained and evaluated using the full set of predictors from the extended model (Model 2) to ensure a fair comparison. The predictive performance was assessed comprehensively in the test set regarding discrimination, calibration, and clinical utility.
The discriminative ability of each model is summarised in Table 5 and visualised in Figure 2. The original logistic regression model (LR-Original) achieved an AUC of 0.777 (95% CI: 0.749–0.805). The extended logistic regression model (LR-Extended), which included additional clinical variables, showed a comparable AUC of 0.781 (95% CI: 0.753–0.809). At the optimal cutoff, the LR-Extended model demonstrated a sensitivity of 78.3% (95% CI: 73.1–82.9%) and specificity of 63.5% (95% CI: 61.2–65.7%). The RF and XGBoost models demonstrated marginally higher apparent AUCs of 0.795 (95% CI: 0.768–0.822) and 0.802 (95% CI: 0.775–0.828), respectively. However, following bootstrap internal validation (1000 repetitions) to correct for optimism, the AUCs for all models were slightly attenuated. The optimism-corrected AUC for the LR-Extended model was 0.773 (95% CI: 0.745–0.802), whereas the RF and XGBoost models achieved corrected AUCs of 0.785 (95% CI: 0.757–0.812) and 0.791 (95% CI: 0.764–0.819), respectively, indicating comparable and robust discrimination.
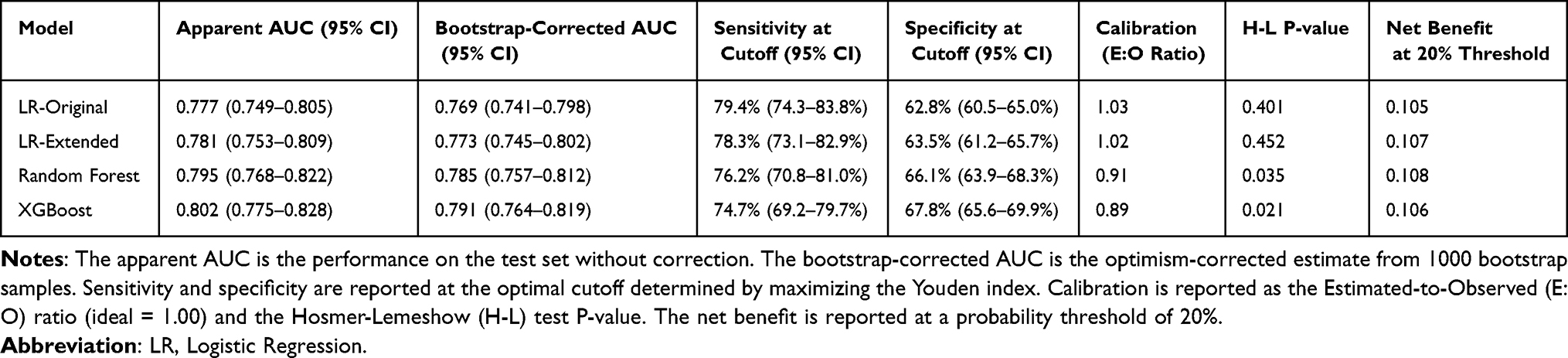 |
Table 5 Comprehensive Performance Comparison of Prediction Models for Postoperative Pneumonia |
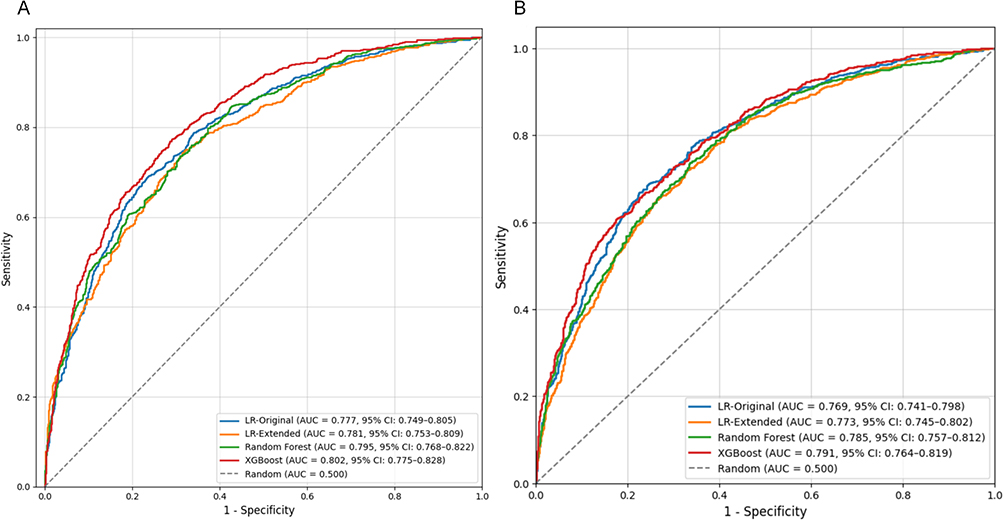 |
Figure 2 Receiver Operating Characteristic (ROC) curves comparing the discriminative ability of the four prediction models for postoperative pneumonia. Subfigure (A) displays the apparent performance of the models. Subfigure (B) shows the optimism-corrected performance derived from 1000 bootstrap repetitions. For each curve, the area under the curve (AUC) and its 95% confidence interval (CI) are reported. |
Feature importance analysis from both machine learning models (Figure 3) consistently identified GNRI, 5-mFI, and BNP as the top three predictors of POP, aligning with the findings from the logistic regression analysis. This convergence across different modelling approaches reinforces the fundamental importance of nutritional status, frailty burden, and cardiac strain in POP risk stratification. The specific hyperparameters used for tuning the machine learning models are provided in Table 6.
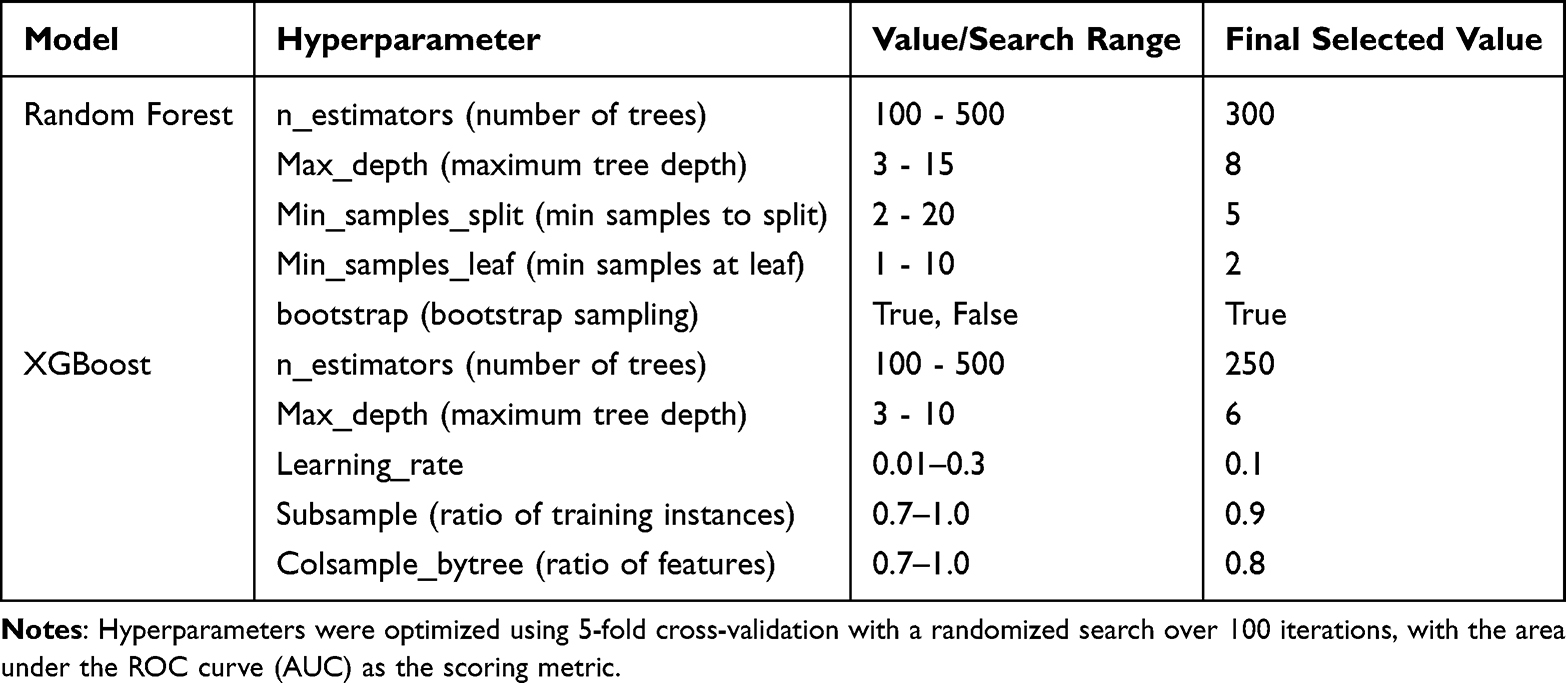 |
Table 6 Hyperparameter Settings for Machine Learning Models |
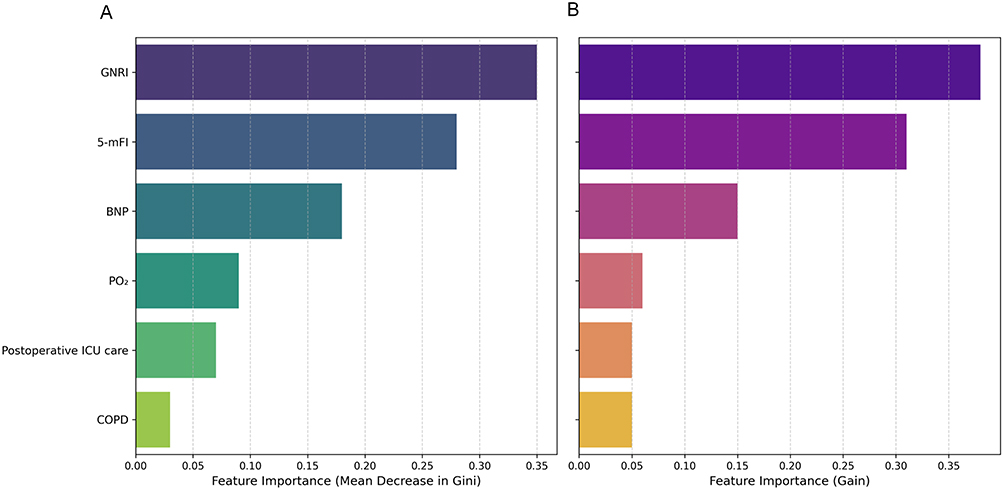 |
Figure 3 Variable importance plots for the machine learning models in predicting postoperative pneumonia. (A) Feature importance ranking from the Random Forest model, determined by the mean decrease in Gini impurity. (B) Feature importance ranking from the XGBoost model, based on the total gain, which measures the relative contribution of each feature to the model. Features are ranked in descending order of importance. |
Calibration performance varied across the models (Figure 4A). The LR-Extended model demonstrated excellent calibration, with a calibration intercept near 0 and a slope near 1 (Estimated/Observed ratio: E:O = 1.02; Hosmer–Lemeshow test: P=0.452). By contrast, both machine learning models showed signs of miscalibration. The RF model tended to overestimate risk in the intermediate probability range, whereas the XGBoost model was overconfident, compressing predicted probabilities towards the extremes.
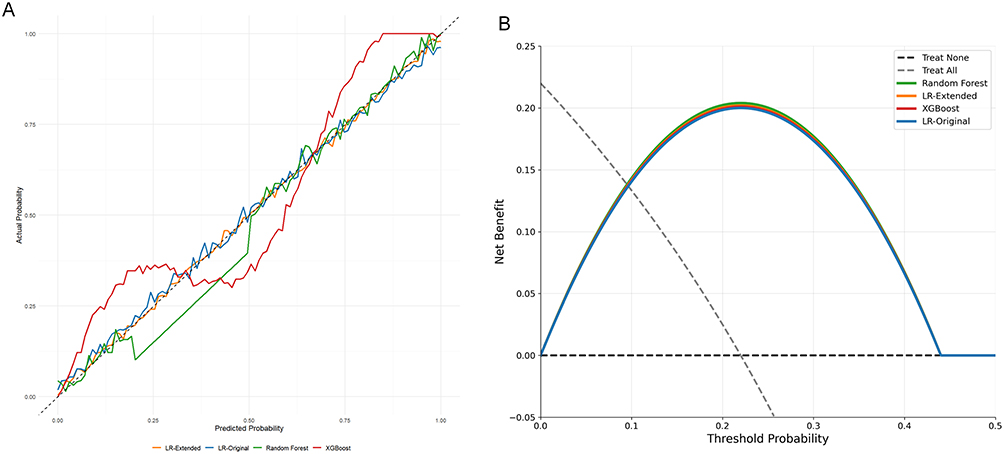 |
Figure 4 Assessment of model calibration and clinical utility. (A) Calibration curves comparing the predicted probabilities against the observed frequencies of postoperative pneumonia for the four models. The dashed diagonal line represents perfect calibration. (B) Decision curve analysis evaluating the net benefit of the four prediction models across a range of threshold probabilities. The horizontal black dashed line indicates the net benefit of the “treat-none” strategy, while the gray sloped dashed line represents the “treat-all” strategy. |
Decision curve analysis (Figure 4B) was used to evaluate the clinical utility of the models across a range of decision thresholds. All three prediction models provided a greater net benefit than the “treat-all” or “treat-none” strategies for probability thresholds between approximately 10% and 35%. Within this clinically relevant range, the net benefit of the three models was highly similar, with no single model demonstrating a clear and substantial superiority over the others.
Discussion
Our findings have direct and actionable implications for clinical practice. The 5-mFI and GNRI are both easily obtainable in routine care at minimal cost, and their integration substantially enhances POP prediction, advancing individualised preoperative assessment. To translate these findings into tangible clinical benefits, we propose a structured implementation pathway. Upon admission for hip fracture, patients would be systematically assessed using the 5-mFI and GNRI. The results should be integrated into a simple risk score (eg, low, intermediate, high), which could then trigger predefined, protocol-driven care bundles. For instance, patients stratified as high-risk (eg, 5-mFI≥2 and GNRI≤92) could be automatically referred for preoperative nutritional consultation and supervised respiratory physiotherapy, including incentive spirometry and cough exercises. For those with a low GNRI, preoperative nutritional optimisation (eg, protein supplementation) can be initiated promptly to bolster immune function. For patients with a high 5-mFI, enhanced perioperative monitoring and aggressive respiratory rehabilitation can help preserve pulmonary function. This model facilitates a shift from a reactive to a proactive, preventive paradigm, potentially improving outcomes and optimising resource allocation by targeting interventions to those who need them most.
The study revealed the importance of age and gender as fundamental clinical characteristics, with an average patient age of 80 years and a predominance of female patients (71.3%). Notably, the incidence of POP was identified as 12.9%, underscoring the vulnerability of this population to postoperative complications. This aligns with previous studies that documented similar trends, emphasising that older age is a consistent risk factor for adverse surgical outcomes, including POP, due to physiological changes and the presence of comorbidities in this demographic.3,5 The role of gender also merits further discussion, as some studies suggest that women may experience higher rates of certain postoperative complications, potentially due to hormonal differences or variations in health-seeking behaviours.16
Notably, we identified independent risk factors associated with POP, including COPD, postoperative ICU admission, PO2, GNRI, 5-mFI, and BNP. These findings align with prior reports but extend the understanding of how these factors distinctly correlate with POP in the hip fracture population.17,18 The association of COPD with POP is particularly well-documented, as this condition compromises pulmonary function and increases susceptibility to respiratory infections post-surgery.9,19 For hypoxaemia (lower preoperative PO2), reduced arterial oxygen tension impairs alveolar macrophage function-a critical component of pulmonary innate immunity-by inhibiting phagocytosis of pathogens and reducing reactive oxygen species production.20 In elderly hip fracture patients, pre-existing pulmonary compromise (eg, mild COPD) or perioperative pain-induced shallow breathing may exacerbate hypoxaemia, creating a pro-inflammatory microenvironment that promotes bacterial colonisation and pneumonia development.21 For BNP, a marker of cardiac strain, elevated levels reflect increased left ventricular filling pressure, which induces subclinical pulmonary oedema. This oedema disrupts the alveolar-capillary barrier, impairs gas exchange, and provides a nutrient-rich environment for bacterial growth.22 Additionally, BNP elevation is often accompanied by systemic inflammation in elderly patients, which further suppresses immune function and enhances susceptibility to postoperative infections.23 These mechanisms explain why these predictors are functionally related to the pathogenesis of POP, enhancing the biological rationality of our model.
Our findings have direct implications for clinical practice. The 5-mFI and GNRI are both easily obtainable in routine care at minimal cost, and their integration substantially enhances POP prediction, advancing individualised preoperative assessment. The 5-mFI is a reliable prognostic indicator for postoperative complications,24,25 with a score >2 linked to a two-fold increase in 30-day mortality.26,27 However, it does not capture acute issues such as nutritional deficits or trauma-induced inflammation. This gap is filled by the GNRI, a simple tool for grading nutritional risk28 that correlates with serum albumin and serves as an established prognostic marker.29,30 Specifically, in patients with hip fracture, a low GNRI predicts higher risks of postoperative mortality and complications.29,30 These insights translate into actionable strategies. Integrating the 5-mFI and GNRI into preoperative assessments can identify high-risk patients (eg 5-mFI≥2 and GNRI≤92) for targeted interventions. For those with low GNRI, preoperative nutritional optimisation (eg protein supplementation) can bolster immune function.31 For patients with a high 5-mFI, enhanced respiratory rehabilitation (eg incentive spirometry, early mobilisation) can help preserve pulmonary function. Furthermore, our results reinforce the need for timely surgery, a principle underscored by the increased morbidity associated with surgical delays during the COVID-19 pandemic.32 Implementing this risk-stratified approach can inform clinical guidelines and improve care for this vulnerable population.
The ultimate value of a prediction model lies in its ability to inform clinical care. To translate our findings into practice, we propose a structured implementation pathway. First, upon admission for hip fracture, patients would be systematically assessed using the 5-mFI and GNRI, with results integrated into a simple risk score (eg low, intermediate, high). This risk stratification could then trigger predefined, protocol-driven care bundles. For example, high-risk patients (eg 5-mFI≥2 and GNRI≤92) could be automatically referred for preoperative nutritional consultation and supervised respiratory physiotherapy, including incentive spirometry and cough exercises. This model facilitates a shift from a reactive to a proactive, preventive paradigm.
This study has several limitations that should be considered when interpreting the results. First, although our model demonstrated robust predictive performance (AUC=0.777) within the studied cohort, its generalisability to other populations requires careful consideration. Second, the retrospective, single-centre design, although enabling a large sample size, inherently carries risks of unmeasured confounding and selection bias. It may also capture unique local practices and patient demographics, potentially limiting the generalisability of our model to other healthcare settings. Third, although we employed multiple imputation to handle missing data, the absence of systematically recorded data on specific medications (eg immunosuppressants, acid-suppressive drugs), detailed surgical techniques, and pre-admission functional scores limits our ability to control for their potential confounding effects. Fourth, our model’s performance, although robust, was evaluated through internal validation alone. External validation in independent, prospective, and multicentric cohorts is crucial to verify its transportability and for calibration for different populations. Finally, the model is primarily designed for preoperative use and does not incorporate dynamic postoperative variables, which could further refine risk stratification during the hospital stay.
Future research should prioritise external validation across diverse geographic and healthcare settings. Furthermore, incorporating more granular data on pharmacotherapy, surgical nuances, and functional status, potentially through prospective study designs, could enhance model precision. Exploring the integration of our model with machine learning approaches on larger datasets may also uncover non-linear interactions and improve predictive accuracy.
Conclusions
This study developed and rigorously validated a multivariable prediction model for POP in elderly patients with hip fracture. The model robustly identifies COPD, postoperative ICU care, hypoxaemia (lower PaO2), nutritional status (GNRI), frailty (5-mFI), and cardiac strain (BNP) as key independent predictors. Its strong, internally validated performance (AUC=0.781) and the convergence of findings across logistic regression, time-to-event, and machine learning analyses affirm that integrating frailty and nutrition with core clinical markers provides a superior foundation for risk assessment.
Crucially, this model offers a direct pathway for enhancing clinical management. It can be pragmatically integrated into perioperative workflows by systematically calculating the 5-mFI and GNRI upon patient admission. This allows for the preoperative stratification of patients into risk tiers (eg high-risk: 5-mFI≥2 and GNRI≤92), enabling targeted allocation of preventive resources. High-risk individuals could then immediately receive protocol-driven care bundles, such as preoperative nutritional optimisation and supervised respiratory physiotherapy, which have the potential to improve outcomes and optimise resource use. By moving beyond demographic proxies and existing models that lack these integrated geriatric assessments, our tool provides a more holistic and actionable framework for preoperative planning, ultimately aiming to reduce the burden of POP in this vulnerable population.
Data Sharing Statement
The datasets generated and/or analyzed during the current study are not publicly available due to patient confidentiality and privacy regulations but are available from the corresponding author on reasonable request.
Ethics Approval
The study received approval from the Ethics Committee of Beijing Jishuitan Hospital, Capital Medical University, and was conducted in accordance with the Declaration of Helsinki.
The Ethics Committee waived the requirement for individual informed consent.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Disclosure
The authors had no any personal, financial, commercial, or academic conflicts of interest.
References
1. Veronese N, Maggi S. Epidemiology and social costs of hip fracture. Injury. 2018;49(8):1458–15. doi:10.1016/j.injury.2018.04.015
2. Bohl DD, Sershon RA, Saltzman BM, et al. Incidence, risk factors, and clinical implications of pneumonia after surgery for geriatric hip fracture. J Arthroplasty. 2018;33(5):1552–1556.e1. doi:10.1016/j.arth.2017.11.068
3. Lv H, Yin P, Long A, et al. Clinical characteristics and risk factors of postoperative pneumonia after hip fracture surgery: a prospective cohort study. Osteoporos Int. 2016;27(10):3001–3009. doi:10.1007/s00198-016-3624-5
4. Tian Y, Zhu Y, Zhang K, et al. Relationship between preoperative hypoalbuminemia and postoperative pneumonia following geriatric hip fracture surgery: a propensity-score matched and conditional logistic regression analysis. Clin Interv Aging. 2022;17:495–503. doi:10.2147/CIA.S352736
5. Shin KH, Kim JJ, Son SW, et al. Early postoperative hypoalbuminaemia as a risk factor for postoperative pneumonia following hip fracture surgery. Clin Interv Aging. 2020;15:1907–1915. doi:10.2147/CIA.S272610
6. Ahn J, Chang JS, Kim JW. Postoperative pneumonia and aspiration pneumonia following elderly hip fractures. J Nutr Health Aging. 2022;26(7):732–738. doi:10.1007/s12603-022-1821-9
7. Tian Y, Zhu Y, Zhang K, et al. Incidence and risk factors for postoperative pneumonia following surgically treated hip fracture in geriatric patients: a retrospective cohort study. J Orthop Surg Res. 2022;17(1):179. doi:10.1186/s13018-022-03071-y
8. Geerds MAJ, Folbert EC, Visschedijk SFM, et al. Implementation of a pneumonia prevention protocol to decrease the incidence of postoperative pneumonia in patients after hip fracture surgery. Injury. 2022;53(8):2818–2822. doi:10.1016/j.injury.2022.06.017
9. Chen X, Shen Y, Hou L, et al. Sarcopenia index based on serum creatinine and cystatin C predicts the risk of postoperative complications following hip fracture surgery in older adults. BMC Geriatr. 2021;21(1):541. doi:10.1186/s12877-021-02522-1
10. Barceló M, Torres OH, Mascaró J, et al. Hip fracture and mortality: study of specific causes of death and risk factors. Arch Osteoporos. 2021;16(1):15. doi:10.1007/s11657-020-00873-7
11. Pierce KE, Naessig S, Kummer N, et al. The five-item modified frailty index is predictive of 30-day postoperative complications in patients undergoing spine surgery. Spine. 2021;46(14):939–943. doi:10.1097/BRS.0000000000003936
12. Xie D, Huang T, Yang C, et al. Predictive performance of the geriatric nutritional risk index for sarcopenia: a meta-analysis. Arch Gerontol Geriatr. 2025;138:105985. doi:10.1016/j.archger.2025.105985
13. Pablo AM, Izaga MA, Alday LA. Assessment of nutritional status on hospital admission: nutritional scores. Eur J Clin Nutr. 2003;57(7):824–831. doi:10.1038/sj.ejcn.1601616
14. Buzby GP, Williford WO, Peterson OL, et al. A randomized clinical trial of total parenteral nutrition in malnourished surgical patients: the rationale and impact of previous clinical trials and pilot study on protocol design. Am J Clin Nutr. 1988;47(2 Suppl):357–365. doi:10.1093/ajcn/47.2.357
15. Kalil AC, Metersky ML, Klompas M, et al. Management of adults with hospital-acquired and ventilator-associated pneumonia: 2016 clinical practice guidelines by the infectious diseases society of America and the American Thoracic Society. Clin Infect Dis. 2016;63(5):e61–e111. doi:10.1093/cid/ciw353
16. Tang MT, Li S, Liu X, et al. Early detection of pneumonia with the help of dementia in geriatric hip fracture patients. Orthop Surg. 2022;14(1):129–138. doi:10.1111/os.13199
17. Yu Y, Zheng P. Determination of risk factors of postoperative pneumonia in elderly patients with Hip fracture: what can we do? PLoS One. 2022;17(8):e0273350. doi:10.1371/journal.pone.0273350
18. Sasabuchi Y, Matsui H, Lefor AK, et al. Timing of surgery for hip fractures in the elderly: a retrospective cohort study. Injury. 2018;49(10):1848–1854. doi:10.1016/j.injury.2018.07.026
19. Surti U, Yatsenko S, Hu J, et al. Maternal GRB10 microdeletion is a novel cause of cystic placenta: spectrum of genomic changes in the etiology of enlarged cystic placenta. Placenta. 2017;57:33–41. doi:10.1016/j.placenta.2017.05.018
20. Sturrock A, Woller D, Freeman A, et al. Consequences of hypoxia for the pulmonary alveolar epithelial cell innate immune response. J Immunol. 2018;201(11):3411–3420. doi:10.4049/jimmunol.1701387
21. Lee S, Hong H, Cho H, et al. Association between preoperative oxygen reserve index and postoperative pulmonary complications: a prospective observational study. Kor J Anesthesiol. 2025;78(3):224–235. doi:10.4097/kja.24420
22. Liu Q, Sun G, Huang L. Association of the NLR, BNP, PCT, CRP, and D-D with the severity of community-acquired pneumonia in older adults. Clin Lab. 2023;69(12). doi:10.7754/Clin.Lab.2023.220330
23. Poredos P, Komadina R. Inflammation and perioperative cardiovascular events. Cells. 2025;14(17):1362. doi:10.3390/cells14171362
24. Bellamy JL, Runner RP, Vu CCL, et al. Modified frailty index is an effective risk assessment tool in primary total hip arthroplasty. J Arthroplasty. 2017;32(10):2963–2968. doi:10.1016/j.arth.2017.04.056
25. Shin JI, Keswani A, Lovy AJ, et al. Simplified frailty index as a predictor of adverse outcomes in total hip and knee arthroplasty. J Arthroplasty. 2016;31(11):2389–2394. doi:10.1016/j.arth.2016.04.020
26. Keller DS, Reif de Paula T, Kiran RP, et al. Evaluating the association of the new national surgical quality improvement program modified 5-factor frailty index with outcomes in elective colorectal surgery. Colorectal Dis. 2020;22(10):1396–1405. doi:10.1111/codi.15066
27. Li CQ, Zhang C, Yu F, et al. The composite risk index based on frailty predicts postoperative complications in older patients recovering from elective digestive tract surgery: a retrospective cohort study. BMC Anesthesiol. 2022;22(1):7. doi:10.1186/s12871-021-01549-6
28. Bouillanne O, Morineau G, Dupont C, et al. Geriatric nutritional risk index: a new index for evaluating at-risk elderly medical patients. Am J Clin Nutr. 2005;82(4):777–783. doi:10.1093/ajcn/82.4.777
29. Su WT, Wu SC, Huang CY, et al. Geriatric nutritional risk index as a screening tool to identify patients with malnutrition at a high risk of in-hospital mortality among elderly patients with femoral fractures-a retrospective study in a Level I trauma center. Int J Environ Res Public Health. 2020;17(23):8920. doi:10.3390/ijerph17238920
30. Liu X, Xie D. Geriatric nutritional risk index predicts postoperative prognosis in older patients with Hip fracture: a meta-analysis. Medicine. 2024;103(17):e37996. doi:10.1097/MD.0000000000037996
31. Tsutsui T, Fujiwara T, Matsumoto Y, et al. Geriatric nutritional risk index as the prognostic factor in older patients with fragility Hip fractures. Osteoporos Int. 2023;34(7):1207–1221. doi:10.1007/s00198-023-06753-3
32. Ding L, Wei J, Wang B. The impact of COVID-19 on the prevalence, mortality, and associated risk factors for mortality in patients with hip fractures: a meta-analysis. J Am Med Dir Assoc. 2023;24(6):846–854. doi:10.1016/j.jamda.2023.03.011
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.