Back to Journals » Risk Management and Healthcare Policy » Volume 18
Development and Validation of a Risk Prediction Model for Interdialytic Hyperkalemia in Patients Undergoing Maintenance Hemodialysis
Authors Wang P, Xiao JN, Liu YY, Xiao L, Chen JL, Wang Y, Yang LH, Feng XL
Received 1 August 2025
Accepted for publication 7 November 2025
Published 20 November 2025 Volume 2025:18 Pages 3713—3724
DOI https://doi.org/10.2147/RMHP.S552431
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Mecit Can Emre Simsekler
Pan Wang,1,* Jun-Nan Xiao,1,* Yan-Yu Liu,2 Long Xiao,1 Jie-Li Chen,1 Yu Wang,1 Li-Hua Yang,3 Xiu-Li Feng4
1Blood Purification Centre, The Second Affiliated Hospital, Guangzhou Medical University, Guangzhou, 510000, People’s Republic of China; 2Department of Emergency, Panyu Branch, The Second Affiliated Hospital, Guangzhou Medical University, Guangzhou, 510000, People’s Republic of China; 3Department of Neurology, Panyu Branch, The Second Affiliated Hospital, Guangzhou Medical University, Guangzhou, 511447, People’s Republic of China; 4Management Committee, Panyu Branch, The Second Affiliated Hospital, Guangzhou Medical University, Guangzhou, 511447, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Xiu-Li Feng, Management Committee, Panyu Branch, the second Affiliated Hospital, Guangzhou Medical University, No. 63 South Asian Games Road, Asian Games Town, Panyu District, Guangzhou, 511447, People’s Republic of China, Tel +86 18127805232, Email [email protected] Li-Hua Yang, Department of neurology, Panyu Branch, The Second Affiliated Hospital, Guangzhou Medical University, No. 63 South Asian Games Road, Asian Games Town, Panyu District, Guangzhou, 511447, People’s Republic of China, Tel +86 15902010792, Email [email protected]
Background: Interdialytic hyperkalemia is linked to a heightened risk of adverse clinical outcomes among patients undergoing maintenance hemodialysis (MHD). This study aimed to develop and validate a nomogram to assess the risk of interdialytic hyperkalemia in this patient population.
Methods: A total of 312 patients undergoing MHD were retrospectively enrolled from two hemodialysis centers between January 2024 and December 2024. The group was randomly divided into a training set and a validation set in a 7:3 ratio. Least absolute shrinkage and selection operator regression was applied to identify independent predictors of hyperkalemia, which were subsequently incorporated into a multivariate logistic regression model. Model performance was assessed using receiver operating characteristic curve analysis, area under the curve (AUC), calibration plots, and decision curve analysis (DCA) to assess both discrimination and clinical utility.
Results: The overall incidence of interdialytic hyperkalemia was 28.2%. The final nomogram included seven predictors: dietary potassium intake, dietary phosphorus intake, serum albumin concentration, pre-dialysis blood glucose level, interdialytic weight gain rate, time interval since the last dialysis session, and a history of hyperkalemia within the preceding three months. The model demonstrated strong discriminatory ability with an AUC of 0.905 (95% Confidence Interval (CI): 0.883– 0.931) in the training set and 0.782 (95% CI: 0.756– 0.819) in the validation set. Calibration plots indicated good agreement between predicted and observed outcomes. DCA confirmed the clinical applicability of the model by demonstrating a net benefit across a range of threshold probabilities.
Conclusion: A nomogram-based risk prediction model for interdialytic hyperkalemia in patients undergoing MHD was developed and externally validated. The model demonstrated robust predictive performance and may assist clinicians in early identification of patients who are at high-risk, thereby supporting timely interventions.
Keywords: hemodialysis, hyperkalemia, interdialytic period, model development, model validation, prediction model
Background
Hemodialysis, as a principal modality of renal replacement therapy for patients with end-stage renal disease, substantially prolongs survival. According to national registry data, the number of patients receiving hemodialysis in China surpassed 900,000 by the end of 2023, reflecting an approximately 290% increase compared to 2011. The Dialysis Outcomes and Practice Patterns Study reported that the prevalence of hyperkalemia defined as a serum potassium concentration exceeding 5.0 mmol/L varied by region, affecting 30% of patients in North America, 47% in Europe, and 37% in the Asia-Pacific region (Australia/New Zealand/Japan).1 Recent studies have indicated that 75% of patients undergoing maintenance hemodialysis (MHD) experienced peak pre-dialysis serum potassium levels above 5.0 mmol/L within a four-month period.2 In patients receiving Maintenance Hemodialysis (MHD), hyperkalemia can result from reduced renal potassium excretion, dietary intake, insufficient dialysis adequacy, and use of medications like Renin-Angiotensin-Aldosterone System (RAAS) inhibitors. Clinical manifestations of hyperkalemia primarily include muscle weakness, palpitations, nausea, and vomiting. Hyperkalemia is recognized as a key risk factor for malignant arrhythmias and sudden cardiac death, and is associated with significantly increased adverse outcomes in the MHD population.3
The interdialytic period, defined as the interval between two hemodialysis sessions, constitutes a high-risk phase for the development of hyperkalemia, as most patients remain outside of direct clinical supervision during this time. Due to the limited availability of timely medical intervention, hyperkalemia occurring during this period may result in life-threatening consequences. Existing domestic and international studies have primarily focused on identifying factors associated with hyperkalemia in MHD populations; The set of established risk factors comprises the interdialytic interval, diabetes, heart failure, and certain laboratory indices. However, there remains a lack of validated, targeted tools for individualized risk assessment.4,5 Therefore, early prediction of interdialytic hyperkalemia in patients receiving MHD is critically important.
Participants and Methods
Study Participants
A total of 312 patients diagnosed with MHD meeting the inclusion criteria from 2 hemodialysis centers between January 2024 and December 2024 were included. Patients with serum potassium levels ≥ 5.0 mmol/L were classified into the hyperkalemia group, and those with serum potassium levels < 5.0 mmol/L were classified into the hypokalemia group. Inclusion criteria: (1) receiving hemodialysis treatment for at least 3 months; (2) age ≥ 18 years; (3) at least one serum potassium test performed within 3 months with complete data; (4) signed informed consent form. Exclusion criteria: (1) incomplete data with missing key analytical indicators; (2) occurrence of major trauma, rhabdomyolysis, severe infection, malignant tumor, severe malnutrition or cachexia, severe organ dysfunction, or pregnancy within the past month; (3) consciousness disorder or cognitive dysfunction; (4) inability to cooperate. Sample size calculation: This study included 37 variables. According to the sample size calculation formula, the sample size should be 5–10 times the number of independent variables, yielding a required sample size of at least 185–365 cases. Considering 10% invalid samples, the final required sample size was 203–402 cases. All patients provided informed consent and voluntarily participated in this study. This study adhered to ethical principles, with ethics approval number No.2024-hs-17-02.
Research Methods
Data Collection
Comprehensive potential influencing factors for hyperkalemia were identified through a review of relevant literature and consultation with clinical experts. From these factors, a standardized data collection form was developed to record the occurrence of hyperkalemia in patients undergoing MHD. Relevant data were retrieved and exported from the unified information system utilized by the blood purification centers at both hospital campuses.
Data collection included the following components:
(1) General data: sex, age, primary diagnosis, history of hypertension, history of diabetes mellitus, and prior history of hyperkalemia. Hemodialysis-related variables included dialysis frequency, ultrafiltration volume, time interval since the previous dialysis session, interdialytic weight gain rate, use of angiotensin-converting enzyme inhibitors or angiotensin II receptor blockers, and urea clearance index.
(2) Laboratory test results: pre-dialysis white blood cell count, hemoglobin concentration, high-sensitivity C-reactive protein, hematocrit, platelet count, serum phosphorus, serum calcium, carbon dioxide combining power, blood glucose, serum potassium, urea, creatinine, serum albumin, total iron-binding capacity, ferritin, transferrin saturation, serum iron, high-density lipoprotein cholesterol, low-density lipoprotein cholesterol, and triglycerides.
Dietary Intake Survey (3-Day Dietary Diary Method)
A standardized dietary record form was used to assist patients in documenting all dietary intake over three consecutive days. The recorded data included food items, quantities consumed, types of seasonings used, and methods of preparation. Daily intake of energy, macronutrients (protein, fat, and carbohydrates), and electrolytes (potassium, sodium, and phosphorus) was calculated independently by two members of the study team using professional nutrition analysis software (Kaitong Recipe Calculator).
Statistical Methods
Data processing was conducted using SPSS version 23.0 and R software version 4.2.1. The Shapiro–Wilk test was applied to assess the normality of continuous variables. Variables following a normal distribution were expressed as mean ± standard deviation, and between-group comparisons were performed using the independent samples t-test. Non-normally distributed variables were presented as median and interquartile range, and the Mann–Whitney U-test was applied for between-group analysis. Categorical variables were reported as frequency and percentage, and comparisons between groups were conducted using the chi-squared test (χ2) or Fisher’s exact test, as appropriate.
Least absolute shrinkage and selection operator (LASSO) regression was used to identify potential predictors significantly associated with hyperkalemia. Variables selected through LASSO regression were subsequently entered into a multivariate logistic regression model to construct a risk prediction model. A nomogram was generated using the rms package in R for visual representation.
Model performance was assessed in terms of discrimination, calibration, and internal validation. Discrimination was assessed by plotting receiver operating characteristic (ROC) curves and calculating the area under the curve (AUC), with AUC > 0.8 indicating strong discriminative power. Calibration was evaluated using calibration curves to compare predicted probabilities with observed outcomes, with closer alignment to the reference line indicating better goodness of fit. Internal validation was conducted using bootstrap resampling (1000 iterations). The optimal cut-off value was determined by maximizing the Youden index, and the corresponding sensitivity and specificity were calculated.
Results
Data Comparison Between Hyperkalemia Group and Non-Hyperkalemia Group in Patients Undergoing MHD
Among the 312 patients undergoing MHD, hyperkalemia occurred in 88 cases (28.2%), while 224 cases (71.8%) did not exhibit hyperkalemia. A comparison of baseline characteristics between the hyperkalemia and non-hyperkalemia groups is presented in Table 1.
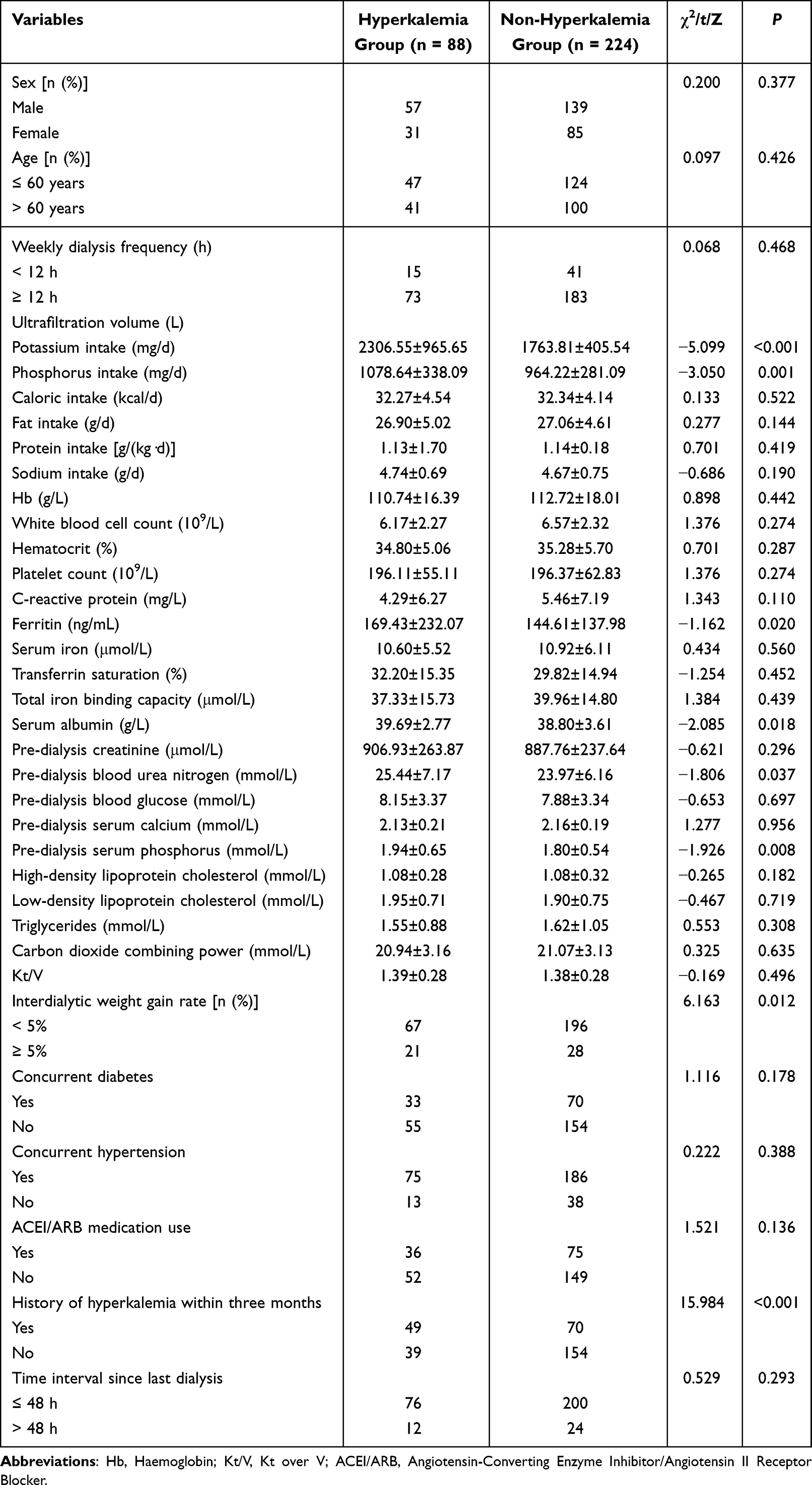 |
Table 1 Comparison of Baseline Characteristics Between the Hyperkalemia and Non-Hyperkalemia Groups |
Selection of Hyperkalemia-Related Variables Using LASSO Regression
Using hyperkalemia occurrence status as the response variable, LASSO regularized regression was applied to 37 candidate predictors (Figure 1). The optimal penalty parameter was identified through ten-fold cross-validation (λ = 0.039), based on the lambda.1se criterion. A total of seven variables with non-zero coefficients were retained: potassium intake, phosphorus intake, serum albumin, pre-dialysis blood glucose, interdialytic weight gain rate, history of hyperkalemia within the past three months, and time interval since the last dialysis session.
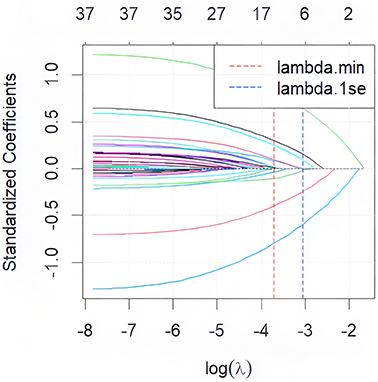 |
Figure 1 LASSO regression coefficient path. Abbreviation: LASSO, Least absolute shrinkage and selection operator. |
Multivariate Logistic Regression Analysis
Hyperkalemia occurrence was used as the dependent variable, and the seven independent variables identified through LASSO regression were assigned values accordingly (Table 2). A multivariate logistic regression model was then constructed. The analysis indicated that all seven variables were significantly associated with hyperkalemia (p < 0.05 for all): potassium intake, phosphorus intake, serum albumin level, pre-dialysis blood glucose, interdialytic weight gain rate, history of hyperkalemia within the past three months, and time interval since the last dialysis session. Detailed results are presented in Table 3.
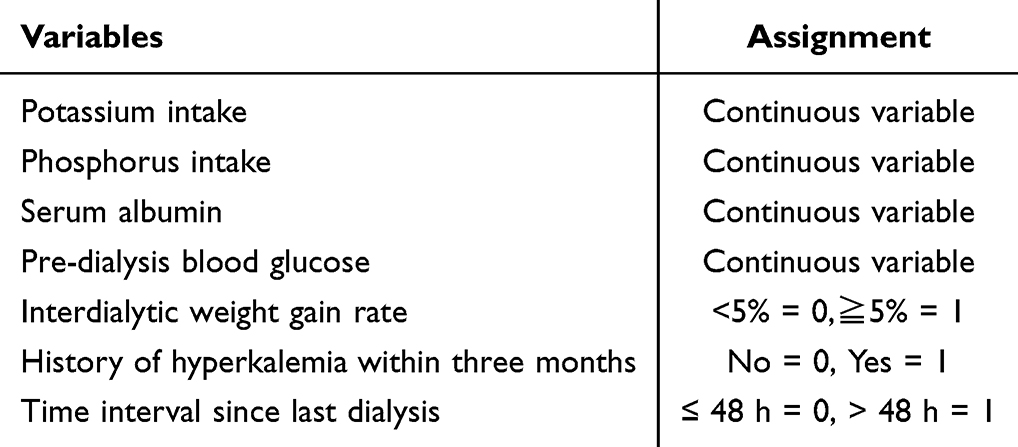 |
Table 2 Variable Assignment |
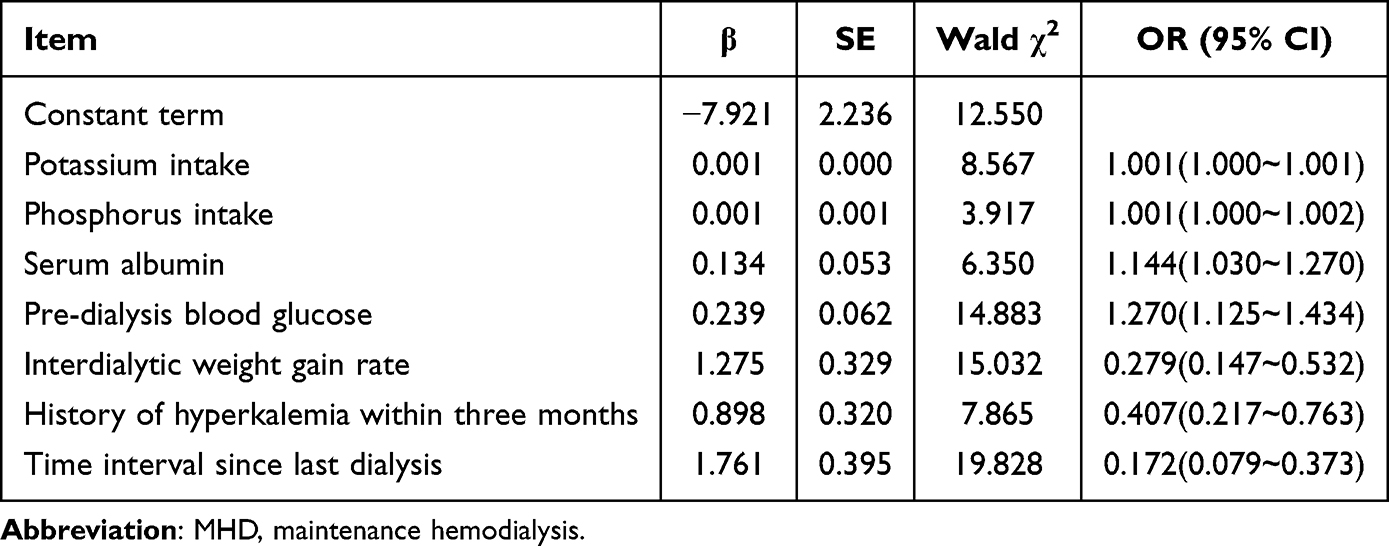 |
Table 3 Multivariate Analysis of Factors Affecting Hyperkalemia Occurrence in Patients Undergoing MHD |
Development and Evaluation of a Hyperkalemia Risk Prediction Model
Independent risk factors for hyperkalemia in patients undergoing MHD were identified through multivariate logistic regression analysis, and a corresponding risk prediction model, along with its mathematical formula, was developed. A nomogram based on this model was constructed using RStudio (version 4.2.1) and is presented in Figure 2.
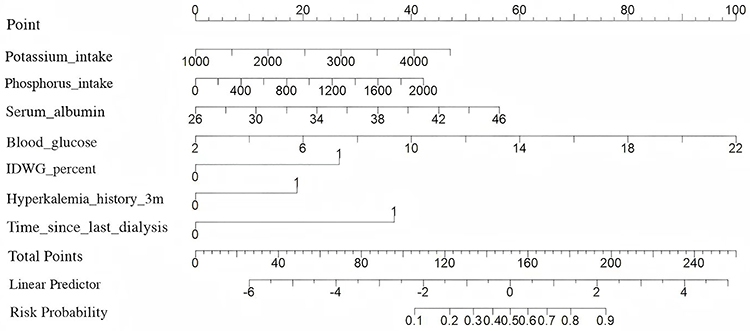 |
Figure 2 Hyperkalemia risk prediction model for patients undergoing MHD. Abbreviations: MHD, maintenance hemodialysis; IDWG, Interdialytic Weight Gain. |
The model demonstrated good discriminatory performance, with an area under the ROC curve of 0.856 (95% Confidence Interval (CI): 0.807–0.905). At the optimal cut-off value determined by maximizing the Youden index (1.598), the sensitivity and specificity of the model were 83.0% and 93.33%, respectively.
Model calibration was assessed using the Hosmer–Lemeshow goodness-of-fit test (χ2 = 11.67, P = 0.167), indicating no significant lack of fit. The calibration curve is presented in Figure 3.
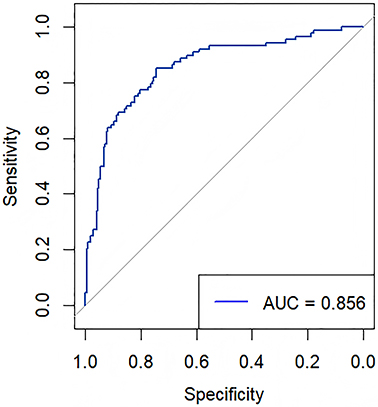 |
Figure 3 ROC curve of hyperkalemia risk model for patients undergoing MHD. Abbreviations: MHD, maintenance hemodialysis; AUC, area under the curve. |
Clinical Application Value Assessment of Risk Prediction Model
Internal validation was conducted using the bootstrap resampling technique, with 1000 repeated samples drawn from the original dataset. Calibration assessment results (Figure 4) indicated good agreement between predicted and observed outcomes, demonstrating satisfactory calibration of the model. Decision curve analysis, as presented in Figure 5, demonstrated that within the clinically relevant threshold range for hyperkalemia risk prediction in patients undergoing maintenance hemodialysis, the model provided a positive net benefit, supporting its potential utility in clinical decision-making.
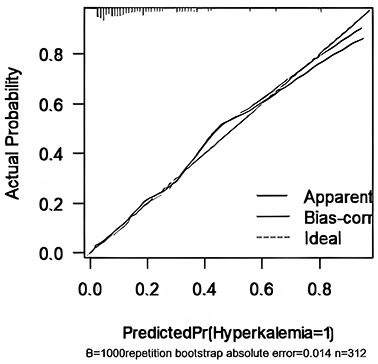 |
Figure 4 Calibration curve of nomogram. |
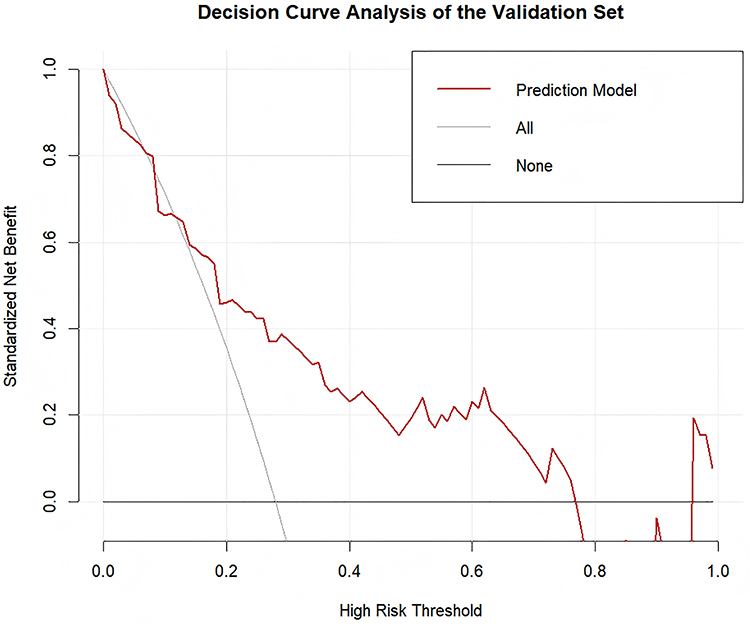 |
Figure 5 Clinical decision curve of nomogram. |
Risk Prediction Model Performance Validation
ROC curve analysis demonstrated that the model exhibited excellent discriminatory ability in the training set, with an AUC of 0.905 (95% Confidence Interval [CI]: 0.883–0.931) (Figure 6). The mean absolute error (MAE) derived from the calibration curve was 0.14, indicating strong agreement between predicted probabilities and observed outcomes. In the validation set, the model yielded an AUC of 0.782 (95% CI: 0.756–0.819), with a sensitivity of 87.2% and specificity of 89.5%. The corresponding calibration MAE was 0.042 (Figure 6). These comprehensive metrics indicate that the model possesses robust predictive performance.
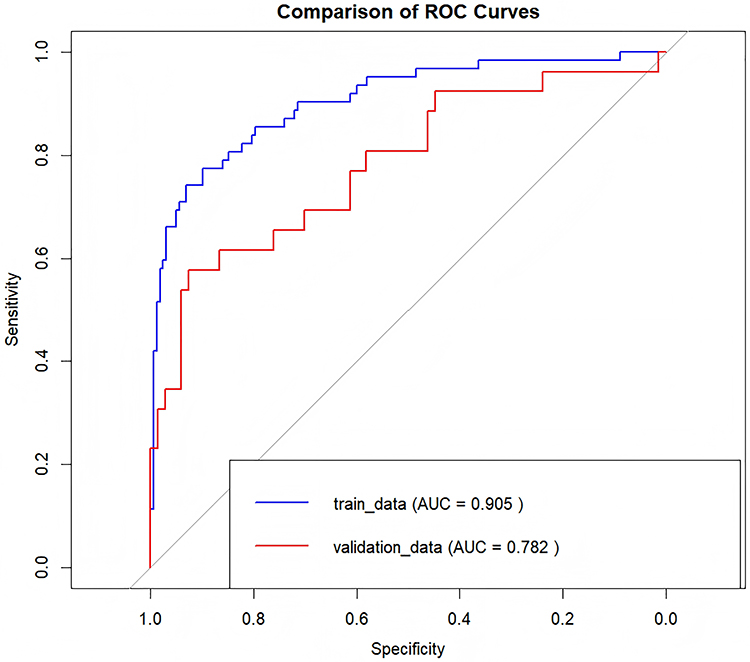 |
Figure 6 Comparison of ROC curves between training and validation sets. Abbreviations: AUC, area under the curve; ROC, receiver operating characteristic. |
Discussion
Current Status of Hyperkalemia Occurrence in Patients Undergoing MHD
The current status of hyperkalemia among patients undergoing MHD was examined. A total of 312 patients from the hemodialysis centers of two tertiary grade A hospitals in Guangdong Province were included as study participants. The findings indicated that the incidence of hyperkalemia reached 28.2%, with approximately 10% of patients having experienced the condition. Existing literature identifies hyperkalemia as a frequent indication for additional hemodialysis sessions, second only to heart failure. Given that hyperkalemia may contribute to the progression of renal dysfunction and increased mortality risk, further investigation into its contributing factors is essential to facilitate early identification and timely intervention.
Analysis of Influencing Factors for Hyperkalemia Occurrence in Patients Undergoing MHD
Potassium Intake, Phosphorus Intake, Serum Albumin, Interdialytic Weight Gain Rate
The research team discovered potassium intake, phosphorus intake, serum albumin level, and interdialytic weight gain rate as significant risk factors for the occurrence of hyperkalemia in patients undergoing MHD. In healthy individuals, potassium is absorbed via the gastrointestinal tract and distributed between the intracellular and extracellular compartments, with approximately 90% excreted by the kidneys to maintain serum potassium concentrations within the normal physiological range of 3.5–5.0 mmol/L. Serum phosphorus levels are similarly regulated by gastrointestinal absorption and renal excretion. A decline in glomerular filtration rate and impaired phosphorus excretion result in elevated serum phosphorus levels.6
In patients receiving hemodialysis, dietary intake is closely associated with pre-dialysis serum potassium and phosphorus levels. Excessive intake of potassium and phosphorus may contribute to the development of hyperkalemia and hyperphosphatemia. Prior studies have reported a positive correlation between serum albumin levels and the risk of hyperkalemia in patients undergoing MHD.7 This association may be attributed to two primary mechanisms: first, patients with higher serum albumin levels typically exhibit better nutritional status and may have increased dietary potassium intake; second, the metabolic byproducts of high protein consumption may exacerbate metabolic acidosis, thereby promoting the transcellular shift of potassium from the intracellular to the extracellular space, ultimately leading to elevated pre-dialysis serum potassium levels.8
In addition, protein-rich foods serve as a major source of dietary phosphorus, and phosphorus intake is closely linked to protein consumption. Among patients with chronic kidney disease, high protein intake markedly increases phosphorus load, thereby contributing to hyperphosphatemia.9 In patients undergoing MHD, the presence of renal parenchymal damage, decreased glomerular filtration rate, and severe renal impairment often result in concurrent elevations in serum potassium and phosphorus concentrations. A higher interdialytic weight gain rate has been associated with suboptimal dietary adherence, and such dietary behaviors serve as an important context for assessing the risk of excessive potassium intake.10,11
Given these risk factors, close monitoring is warranted, and individualized dietary guidance from qualified nutrition professionals should be implemented. Comprehensive and regular assessments of dietary composition, with a focus on increasing protein and caloric intake while appropriately limiting dietary potassium and phosphorus, are essential. These interventions play a key role in optimizing nutritional status, correcting electrolyte imbalances, and mitigating disturbances in bone and mineral metabolism in patients undergoing dialysis.
Pre-Dialysis Blood Glucose
The findings of this study indicated that pre-dialysis blood glucose level is an independent risk factor for the occurrence of hyperkalemia in patients undergoing MHD. Elevated blood glucose levels contribute to increased serum potassium concentrations primarily through osmotic mechanisms and insulin resistance. In hyperosmolar states, water shifts from the intracellular to the extracellular compartment, accompanied by the translocation of potassium ions into the extracellular space.12
Among individuals without diabetes, marked hyperglycemia may induce transient “glucose toxicity”, which impairs both insulin secretion and insulin sensitivity. In this study, 33% of patients were identified as having coexisting diabetes mellitus. In this patient population, absolute or relative insulin deficiency, as well as insulin resistance, is frequently observed.13
Therefore, in patients undergoing MHD, particularly those with concurrent diabetes strict monitoring and regulation of blood glucose levels are essential. Preventing episodes of severe hyperglycemia is a critical strategy in mitigating the risk of interdialytic hyperkalemia and reducing the likelihood of associated life-threatening complications.
History of Hyperkalemia Within Three Months and Time Interval Since Last Dialysis
The study findings indicated that both a history of hyperkalemia within the preceding three months and the time interval since the last dialysis session were significant risk factors for hyperkalemia in patients undergoing MHD. A prospective cohort study conducted in France reported that 26.4% of patients undergoing MHD had serum potassium > 5.1 mmol/L at baseline, and among these, 73.2% experienced recurrent hyperkalemia within three months.14 These findings highlight the high incidence and recurrence rate of hyperkalemia in this population.
The time interval since the last dialysis session serves as a reflection of dialysis frequency. Adequate dialysis contributes to the effective removal of endogenous toxins and excess fluid, correction of electrolyte disturbances, and alleviation of clinical symptoms. A study involving 132 patients demonstrated that pre-dialysis serum potassium levels were significantly higher following 3-day interdialytic intervals compared to 2-day intervals (5.8 mmol/L vs 5.2 mmol/L, p < 0.001), with a 2.3-fold increase in hyperkalemia incidence observed during longer intervals.15 An additional observational study reported a 22% higher risk of sudden death in patients experiencing 3-day interdialytic intervals compared to those with 2-day intervals, primarily attributed to arrhythmias induced by hyperkalemia.16
In light of these findings, regular electrolyte monitoring should be emphasized in MHD patients, particularly in those with a recent history of hyperkalemia, who should be prioritized for enhanced surveillance. Individualized dietary guidance should be provided to support patients in recognizing symptoms associated with hyperkalemia. The availability of oral potassium-lowering agents for home use should be encouraged. Furthermore, strategies such as increasing dialysis frequency, improving the management of extended interdialytic intervals, and optimizing individualized dialysis prescriptions are essential for reducing the risk of serious complications associated with hyperkalemia.
Predictive Value of Hyperkalemia Risk Prediction Model in Patients Undergoing MHD
LASSO regression analysis was used to identify relevant risk factors. When compared with traditional logistic regression, LASSO regression offers the advantage of effectively minimizing multicollinearity among independent variables and is particularly suited for clinical studies characterized by a large number of predictors, limited sample sizes, or high inter-variable correlations.
The hyperkalemia risk prediction model developed for patients undergoing MHD demonstrated strong discriminative performance, with an AUC of 0.856 (95% Confidence Interval: 0.807–0.905), sensitivity of 83.0%, and specificity of 93.33%.
Model calibration was assessed using the Hosmer–Lemeshow goodness-of-fit test (χ2 = 11.67, p = 0.167), which yielded non-significant results, indicating satisfactory model fit. Further internal validation using 1000 bootstrap resampling iterations confirmed that the model retained high sensitivity and specificity, demonstrating strong agreement between predicted and observed probabilities and supporting the model’s robust predictive accuracy.
Univariate analysis in this study revealed that serum ferritin levels were significantly higher in the hyperkalemia group compared to the non-hyperkalemia group (P=0.020). However, ferritin did not emerge as an independent risk factor for interdialytic hyperkalemia in the multivariate logistic regression analysis. This apparent discrepancy warrants further exploration. As an acute-phase reactant, elevated ferritin levels are associated with body iron stores and inflammatory status. Although no significant difference was observed in C-reactive protein (CRP) levels between the two groups (P=0.110), suggesting that baseline systemic inflammation might not be the primary reason for the ferritin difference, the potential influence of unmeasured subclinical or local inflammation as a confounding factor cannot be entirely ruled out. An alternative explanation is that the difference in ferritin may more directly reflect heterogeneity in iron metabolism or nutritional status among the patient cohort. These factors could indirectly influence serum potassium levels through more complex pathways, such as mechanisms related to muscle mass, dietary intake, or comorbidities. When variables like serum albumin and pre-dialysis phosphorus were included in the multivariate model, the direct effect of ferritin itself may have been attenuated.
A limitation of this study is the primary use of CRP for inflammation assessment, without including more specific and sensitive inflammatory markers such as interleukin-6 (IL-6). Therefore, future studies incorporating a broader spectrum of inflammatory markers would be valuable to elucidate more clearly the precise relationships between inflammatory status, iron metabolism, and the risk of hyperkalemia.
Conclusion
The results of this study demonstrated that potassium intake, phosphorus intake, serum albumin level, pre-dialysis blood glucose, interdialytic weight gain rate, history of hyperkalemia within the past three months, and time interval since the last dialysis session as significant risk factors for the occurrence of hyperkalemia in patients undergoing MHD. The nomogram model constructed based on these variables may help healthcare professionals in identifying patients at high risk for hyperkalemia within the MHD population.
This study was adequately powered based on an initial sample size calculation. Further validation in larger and more diverse populations will be valuable to confirm and broaden the applicability of the prediction model.
Abbreviations
MHD, maintenance hemodialysis; ROC, Receiver Operating Characteristic; AUC, Area Under the Curve; DCA, Decision Curve Analysis; DOPPS, Dialysis Outcomes and Practice Patterns Study; IDWG, Interdialytic Weight Gain; ACEI, Angiotensin-Converting Enzyme Inhibitor; ARB, Angiotensin II Receptor Blocker; Hb, Haemoglobin.
Data Sharing Statement
All data generated or analysed during this study are included in this article. Further enquiries can be directed to the corresponding author.
Ethics Approval
The study was conducted in accordance with the Declaration of Helsinki (as was revised in 2013). The study was approved by Ethics Committee of the Second Affiliated Hospital, Guangzhou Medical University (No.2024-hs-17-02). Written informed consent was obtained from all participants.
Funding
Guangzhou Health Science and Technology General Guidance Project (20241A010060).
Disclosure
The authors declare that they have no competing interests.
References
1. a X, Ashfaq A, Karaboyas A, et a1. Prevalence of hyperkalemia in D00PS: a real world, international cohort of hemodialysis patients. Nephrol Dial Transplant. 2017;32(suppl3):iii563. doi:10.1093/ndt/gfx170.MP371
2. Karaboyas A, Robinson BM, James G, et al. Hyperkalemia excursions are associated with an increased risk of mortality and hospitalizations in hemodialysis patients. Kidney J. 2020;14(7):1760–1769. doi:10.1093/ckj/sfaa208
3. Bansal S, Pergola PE. Current management of hyperkalemia in patients on dialysis. Kidney Int Rep. 2020;5(6):779–789. doi:10.1016/j.ekir.2020.02.1028
4. Weng JM, Huang BH, Zhang WC, et al. The association between residual renal function and symptom burden in maintenance hemodialysis patients. Chin J Blood Purif. 2019;18(8):524–534.
5. Lacson E, Wang W, Ma L, Passlick-Deetjen J. Serum magnesium and mortality in hemodialysis patients in the united states: a cohort study. Am J Kidney Dis. 2015;66(6):1056–1066. doi:10.1053/j.ajkd.2015.06.014
6. Zhao XJ, Niu QY, Gan LY, et al. Analysis of the prevalence and related influencing factors of hyperkalemia in Chinese hemodialysis patients based on DOPPS study. Zhongguo Xue Ye Jing Hua. 2021;20(3):145–156. doi:10.3969/j.issn.1671-4091.2021.03.002
7. Kovesdy CP, Regidor DL, Mehrotra R, et al. Serum and dialysate potassium concentrations and survival in hemodialysis patients. Clin J Am Soc Nephrol. 2007;2(5):999–1007. doi:10.2215/CJN.04451206
8. Boaz M, Smetana S. Regression equation predicts dietary phosphorus intake from estimate of dietary protein intake. J Am Diet Assoc. 1996;96(12):1268–1270. doi:10.1016/S0002-8223(96)00331-8
9. Wang XX, Hu RH, Wang Y, Gao LY. Analysis of related factors for recurrent hyperkalemia and severe hyperkalemia in maintenance hemodialysis patients. Zhejiang Pract Med. 2023;28(6):466–470,487.
10. Torlén K, Kalantar-Zadeh K, Molnar MZ, et al. Dialysis modality and interdialytic weight gain. Am J Nephrol. 2012;36(5):439–446.
11. Gennari F. J.Hypokalemia: Disorders of potassium homeostasis. New England J Med. 2011;365(23):2227–2236.
12. Kovesdy CP. Management of hyperkalaemia in chronic kidney disease. Nat Rev Nephrol. 2014;10(11):653–662. doi:10.1038/nrneph.2014.168
13. DeFronzo RA, Alvestrand A, Smith D, Hendler R, Hendler E, Wahren J. Insulin resistance in uremia. J Clin Invest. 1981;67(2):563–568. doi:10.1172/JCI110067
14. Rossignol P, Lamiral Z, Frimat L, et al. Hyperkalaemia prevalence, recurrence and management in chronic haemodialysis: a prospective multicentre French regional registry 2-year survey. Nephrol Dial Transplant. 2017;32(12):2112–2118. doi:10.1093/ndt/gfx053
15. Bem D, Sugrue D, Wilding B, et al. The effect of hyperkalemia and long inter-dialytic interval on morbidity and mortality in patients receiving hemodialysis: a systematic review. Ren Fail. 2021;43(1):241–254. doi:10.1080/0886022X.2020.1871012
16. Foley RN, Gilbertson DT, Murray T, Collins AJ. Long interdialytic interval and mortality among patients receiving hemodialysis. N Engl J Med. 2011;365(12):1099–1107. doi:10.1056/NEJMoa1103313
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Research Progress on the Efficacy and Safety of Spironolactone in Reversing Left Ventricular Hypertrophy in Hemodialysis Patients
Sun Z, Chen Z, Liu R, Lu G, Li Z, Sun Y
Drug Design, Development and Therapy 2023, 17:181-190
Published Date: 23 January 2023
Complete Atrioventricular Block Due to Severe Hyperkalemia in a Hemodialysis Patient: Successful Management with Temporary Transvenous Pacing
Abdi AE, Arın CB, Abdi IA, Ahmed SA, Dahir OF, Aden AS, Hassan MO
International Medical Case Reports Journal 2026, 19:596948
Published Date: 2 May 2026