Back to Journals » International Journal of General Medicine » Volume 15
Development and Validation of a Prognostic Nomogram for Predicting Overall Survival for T1 High-Grade Patients After Radical Cystectomy: A Study Based on SEER
Authors Zhan X, Chen L, Jiang M, Fu B
Received 24 December 2021
Accepted for publication 7 March 2022
Published 5 April 2022 Volume 2022:15 Pages 3753—3765
DOI https://doi.org/10.2147/IJGM.S354740
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Xiangpeng Zhan, Luyao Chen, Ming Jiang, Bin Fu
Department of Urology, The First Affiliated Hospital of Nanchang University, Nanchang, Jiangxi Province, People’s Republic of China
Correspondence: Bin Fu; Luyao Chen, Email [email protected]; [email protected]
Objective: To construct a prognostic model that estimates the probability of overall survival for T1 high-grade bladder cancer patients after radical cystectomy.
Patients and Methods: We enrolled 801 patients diagnosed with T1 high grade and received radical cystectomy from the Surveillance, Epidemiology, and End Results (SEER) database (2004– 2015). All patients were randomly divided into the development group (n = 561) and validation group (n = 240) with the ratio of 7:3. Cox proportional hazards regression analyses were used to filter variables and the Kaplan–Meier method to evaluate survival outcomes. The results of sensitivity analysis determined the variables in the final model. The performance of the model was internally validated by calibration curves, the receiver operating characteristic (ROC) curves, and the concordance index (C-index).
Results: The mean survival months were 56.086 in the development group and 58.21 in the validation group. Six variables including age, marital status, tumour size, tumour sites, region nodes examined, and N stage were incorporated in the final nomogram. The accuracy of the nomogram for prediction of overall survival was estimated by C-index (0.732; 0.712– 0.752) and AUC (0.771 for 3-year; 0.766 for 5-year) in the development group. In the validation group, the C-index of the nomogram was 0.752 (0.723– 0.781), and AUC was 0.761 for 3-year as well as 0.793 for 5-year. These results all showed better performance than the AJCC stage. Calibration plots for 3- and 5-year overall survival presented good concordance in both the development and validation group.
Conclusion: We have established a prognostic nomogram that provides a more accurate and relevant individualized probability of overall survival for patients with T1HG bladder transitional cell carcinoma after radical cystectomy. It can contribute to improving patient counselling and treatment selection.
Keywords: T1 high-grade, SEER, nomogram, prognosis, radical cystectomy, bladder cancer
Introduction
Bladder cancer (BC) was the fourth and ninth most common malignancy in men and women, with estimated 549,000 new cases and 200,000 deaths in 2018, respectively.1,2 Approximately 70% of bladder cancers were classified as non-muscle-invasive bladder cancer (NMIBC) at diagnosis, and patients with T1 stage accounted for 20%.3
T1 bladder cancer is invasive of the lamina propria and usually high-grade. The International Consultation on Urologic Diseases (ICUD) bladder pathology guidelines suggested that all T1 stage bladder cancer should be generally regarded as high-grade regardless of the degree of invasion.4 There has been controversy over the treatment option of bladder preservation or early radical cystectomy in T1 high grade (T1HG) patients. Recently, the proportion of patients undergoing radical cystectomy with T1 lesion had increased from 5.5% between 1998 and 2000 to 9.9% between 2010 and 2012.5,6 Meanwhile, early cystectomy was suggested for T1HG tumors with additional risk factors like carcinoma in situ, lymphatic vessel invasion, variant histology, persistent T1HG on repeat transurethral bladder tumors resection, and multiple or large T1HG tumors according to AUA and EAU guidelines.6,7 Radical cystectomy was increasingly important in the treatment for patients with T1 bladder cancer.
The interest in picking out suitable T1HG patients to receive an early radical cystectomy was gradually increasing. It was essential to predict clinical and oncologic outcomes of T1HG tumours after RC on the basis of risk factors so as to pick out patients with poor estimated survival but might be benefited from bladder preservation treatment or potential clinical trials. Traditionally, the prognosis of tumors was easily assessed by the American Joint Committee of Cancer (AJCC) stage system with the TNM stage. At the same time, it did not match well with T1HG patients owing to not considering demographic factors or treatment information, especially for the surgical approach.
Nomogram is a visible and reliable prediction tool and widely used to assess the prognosis of the disease, in which different variables, such as significant demographic, clinical, pathological, or treatment features are combined and assigned values according to the magnitude of the effect on the outcome.8 Some nomograms predicting survival outcome after RC have been previously developed and externally validated.9–11 They all included some representative factors like age, gender, marital status, tumour size, lymphatic vessel invasion (LVI), and lymph node-positive to improve the accuracy and applicability of the model. Although acceptable accuracy was obtained in these models, they seemed to fail to get good applicability for particular patients diagnosed with T1HG bladder cancer and receiving RC. Moreover, variables in their models like LVI were not generally available, and some vital factors for RC like lymph nodes dissected failed to enroll. Thus, it is urgent to construct a specific model to evaluate the prognosis of TIHG considering its particularity. To our knowledge, there was still no study to construct a nomogram to predict overall survival (OS) for T1HG bladder cancer patients who had received RC.
In our study, we exploited data from the Surveillance, Epidemiology, and End Results (SEER) database of T1HG BC patients from 2004 to 2015 considering the few T1HG patients with RC. We intend to establish and internally verified a prognostic nomogram including some specific and essential relevant prognostic factors to estimate the overall survival (OS) for T1HG bladder cancer patients after RC. In addition, we hope that this model can select TIHG patients who fail to obtain survival benefits from RC to consider other potential treatments. Moreover, the nomogram’s discriminative ability and clinical practicality were also evaluated by comparing with the AJCC stage.
Patients and Methods
Patient Selection
Patient data were obtained from the Surveillance, Epidemiology, and End Results (SEER) which collected patient demographic and cancer data from the US population, and 801 patients were enrolled in our study. The inclusion criteria were as follows (n = 942): 1) diagnosed from 2004 to 2014; 2) T stage: T1 high grade; 3) Histology behavior: Transitional cell carcinoma; 4) Surgical approach: Radical cystectomy (RC) or Pelvic exenteration (PE). The exclusion criteria were as follows (n = 801): 1) M1 or MX stage; 2) NX; 3) Race unknown; 4) Grade unknown (n = 61); 5) Regional nodes examined unknown (n = 9); 6) Tumor size unknown (n = 29); 7) Survival month unknown (n = 2); 8) Die of other cancer (n = 23).
Data Collection and Variables Defined
The variables from the SEER database included: age, sex, race, marital status, histology, tumor size, grade, tumor size, extension, number of tumors, N stage, systemic therapy, chemotherapy, regional nodes examined, survival time, and vital status. According to the “RX Summ-Surg Prim Site (1998+)” column in the SEER database, the surgical approach includes radical cystectomy and pelvic exenteration (code 60–64,70–73,80). Patients with T1 high-grade bladder cancer were contained based on the “CS site-specific factor 1 (Code 20)” column. Age, as a numeric factor, was divided into four subgroups: < 60, 60–70,70–80, >80 years. The race was classified into three categories: white, black, others (including American Indian, Alaska Native, Asian, and Pacific Islander). Marital status was defined as married, separated, divorced or widowed (SDW), and Single. There are two types of histology containing transitional cell carcinoma and papillary transitional cell carcinoma. The tumor site based on ICD-O-3 topography was divided into two groups: other sites and the posterior wall of the bladder. Extension referred to as the column of “CS Extension” was clarified as non-extension and prostatic urethra (PU) or distal ureter (DU) involvement. N stage coded with the sixth edition of AJCC stages was separated into N0, N1, and N2. Regional nodes examined were a numeric factor, and for application simplicity, it was converted into three degrees which included 0 nodes, <10 nodes and ≥10. Other variables included: (1) sex (female, male); (2) grade (grade II, grade III, grade IV); (3) tumor size (<3 cm, ≥3 cm); (4) number of tumor (single, multiple); (5) systemic therapy (non, systemic therapy before surgery, systemic therapy after surgery, both before and after surgery, Intraoperative systemic therapy); chemotherapy (no/unknown, yes).
Endpoints
The primary endpoints were overall mortality (OM) referred to as the death of patients, including any cause. Survival time was defined as the duration from the initial diagnosis to death from any cause or the last follow-up. Any patients who died after the study cutoff date still were coded as alive. The unit of survival time was recorded as month.
Statistical Analysis
Patients in this study were randomly split into development and validation groups at the ratio of 7:3. The significant differences in patient’s baseline characteristics between the two groups were confirmed by the SPSS 22.0. Continuous variables were compared using the t-test or Mann–Whitney U-test, while the Chi-square test was used for categorical variables.
The univariate Cox regression analysis was performed in the development group to identify potentially significant prognostic factors whose p-value of 0.05 or less was included as candidate variables for the multivariate analysis to determine their independent association with overall survival. The results were presented as hazards ratios (HR) and 95% confidence intervals (95% CI). Survival analyses were performed using the Kaplan–Meier method and compared using the Log rank test to evaluate the differences in OS stratified by each factor.
A nomogram was constructed based on the results of multivariate analysis and for visualized prediction of 3- and 5-year survival probability in the development group. The internal validation was performed in the validation group. The accuracy of the nomogram was evaluated using the concordance index (C-index) and the receiver operating characteristic (ROC) curves with the calculated area under the curve (AUC). The sensitivity analysis by entering variables was gradually performed in the final model selection,12 and the model with the largest C-index was adopted. Calibration plots were performed with the package of RMS in RStudio and used to compare predicted and actual outcomes of 3- and 5-year survival time. Bootstraps with 1000 resample were used for these activities.
All statistical analyses were conducted using SPSS 22.0 (IBM Corp, Armonk, NY) and RStudio version 3.6.3 (https://cran.r-project.org/bin/windows/base/old/3.6.3). All results P-values were two-tailed, and a P < 0.050 was considered significant.
Results
Patient Characteristics
Eight hundred and one patients diagnosed with T1 high-grade bladder cancer and receiving radical cystectomy or pelvic exenteration were enrolled in this study. There were 561 patients in the development group and 240 patients in the validation group (Figure 1). Table 1 reveals the detailed demographic information and clinical characteristics of the development group and validation group. Demographic characteristics contained age at diagnosis, gender, race, and marital status. Tumor characteristics included histology, tumor location, grade, tumor size, extension, number of tumors, and N stage. Treatment information included the systemic therapy, chemotherapy, and regional nodes examined. The mean survival time of the development group was 56.086 months, while 58.21 in the validation group, respectively. They all contain the same median survival time (56 months). The 3- and 5-year OS rates were 77.36% and 46.88%, respectively, in the development group, while they were 80.5% and 46.89% in the validation group. A higher proportion of papillary transitional cell carcinoma (63.1%vs 54.2%; P = 0.018) was showed in the development group. Statistical differences in other characteristics between the two groups were not seen.
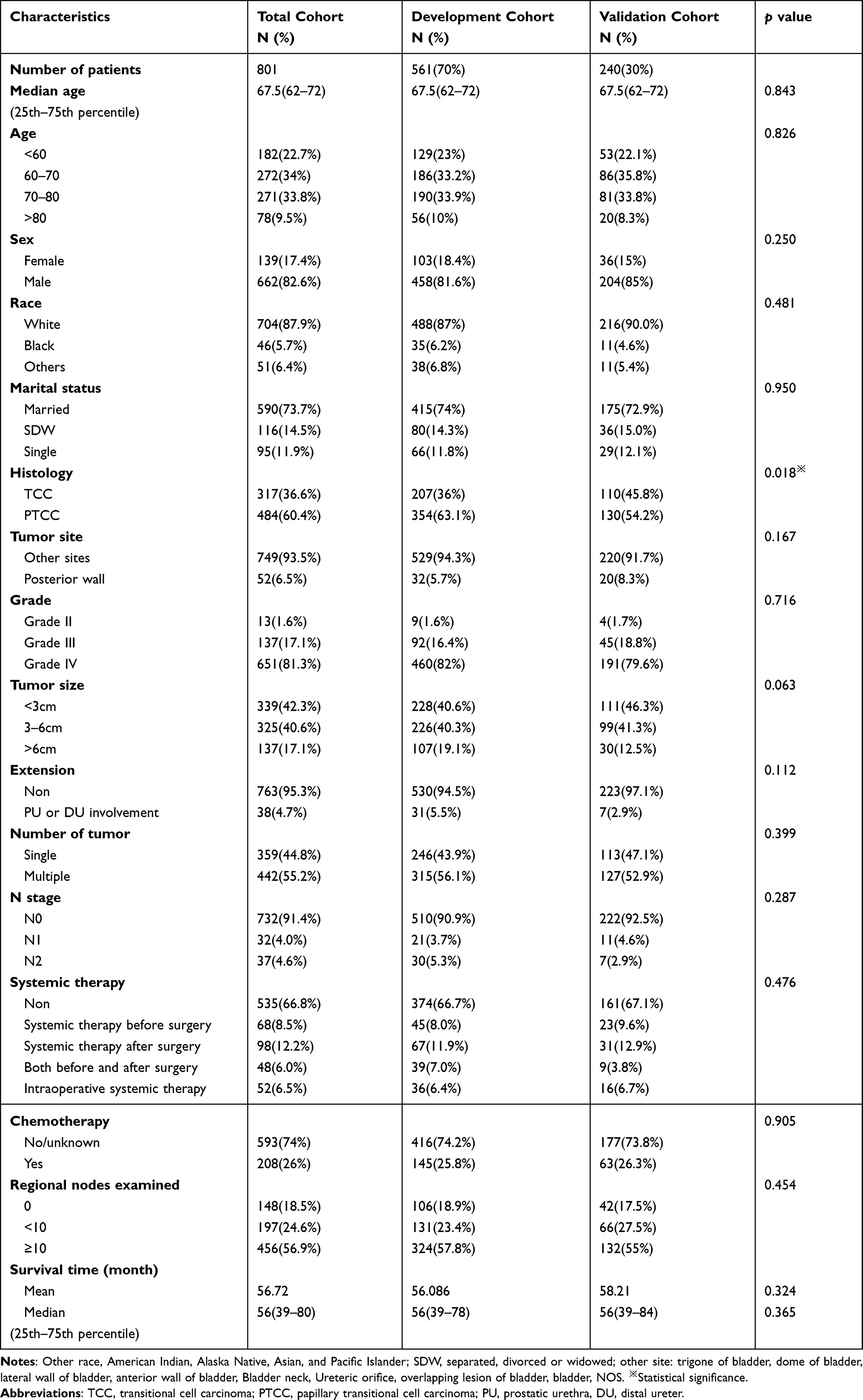 |
Table 1 Baseline Demographical and Clinicopathological Characteristics of Patients |
 |
Figure 1 Flow-chart showing the procedure used to identify patients receiving RC with T1 bladder cancer registered in the SEER database from 2004 to 2015. |
Prognostic Factors in the Development Group
The multivariate analysis incorporated six factors according to the results of the univariate Cox regression analysis and the clinical relevance of factors. It finally determined four independent risk factors as following: Age 70–80 (HR = 2.207, 95% CI: 1.339–3.639, P = 0.002), Age >80 (HR = 4.430, 95% CI: 2.529–7.760, P < 0.001); tumor size 3–6 cm (HR = 1.647, 95% CI: 1.133–2.397, P = 0.009); N1 stage (HR = 3.525, 95% CI: 1.896–6.552, P < 0.001), N2 stage (HR = 4.384, 95% CI: 2.598–7.398, P < 0.001); regional nodes examined <10 (HR = 0.612, 95% CI: 0.402–0.931, P = 0.022), regional nodes examined ≥ 10 (HR = 0.476, 95% CI: 0.329–0.689, P < 0.001). (Table 2) Although these two variables of marital status and tumor site are not statistically different in the multivariate analysis, we still used them as candidates for the model in order to obtain a more accurate model. Survival analysis by Kaplan–Meier method revealed different survival outcomes stratified by each variable (Figure 2). Patients with posterior wall tumor showed better survival outcome than other sites while failing to represent statistical differences (P = 0.13).
 |
Table 2 Univariate and Multivariate Regression Analyses for ACM |
 |
Figure 2 Kaplan–Meier plots for describing overall survival in T1HG patients after radical cystectomy stratified by factors: (A) age (<60 vs 60–70,70–80 or >80); (B) N stage (N0 vs N1 or N2); (C) node examined (0 vs<10 or ≥10); (D) tumor size (<3 cm vs 3–6 cm or >6 cm); (E) marital status: (married vs SDW or single); (F) tumor site (other sites vs posterior wall). |
Prognostic Nomogram for OS
As Table 3 shows, six models were constructed by incorporating variables progressively. The model 6 including the most C-index (0.732, 95% CI, 0.712 to 0.752) and AUC (0.771 for 3-year; 0.793 for 5-year) was defined the most ideal model. The prognostic nomogram predicting 3- and 5-year OS probability was established based on all significant factors using 561 patients from the development group (Figure 3). N stage and age contributed most to the prognosis of OS, as Figure 3 shows.
 |
Table 3 Results of Sensitivity Analysis by Enter Factor Gradually |
 |
Figure 3 Nomogram predicting 3- and 5-year bladder overall survival probability for T1HG patients after radical cystectomy. Variables include age, marital status, tumour size, tumour site, region nodes examined, N stage. Use: locate patient values at each axis. Draw a vertical line to the “Point”axis to determine how many points are attributed for each variable value. Sum the points for all variables. Locate the sum on the “Total Points” line. Draw a vertical line towards the 3Yrs.Surv. Prob. and 5Yrs. Surv. Prob, Prob. axes to determine respectively the 3-, and 5-year survival probabilities. |
Validation of the Nomogram
Internal validation was performed for the nomogram of OS. The C-index of the nomogram was 0.732 (0.712–0.752) in the development group and 0.752 (0.723–0.781) in the validation group. It was significantly higher than that of the AJCC stage, which was 0.590 and 0.559, respectively. The calibration curve in the development and validation group showed good agreement between actual observations and predicted outcomes in the probability of 3-year and 5-year survival (Figures 4 and 5). Meanwhile, ROC curves were used to investigate the discriminative ability of the model (Figures 6 and 7). The 3-year and 5-year AUC in the development group was higher than that of the AJCC stage (0.771 vs 0.614 for 3-year; 0.766 vs 0.594 for 5-year). A similar condition was also seen in the validation group (0.761 vs 0.548 for 3-year; 0.793 vs 0.576 for 5-year). All these results suggested that the nomogram’s better predictive performance was confirmed compared with the traditional AJCC staging system.
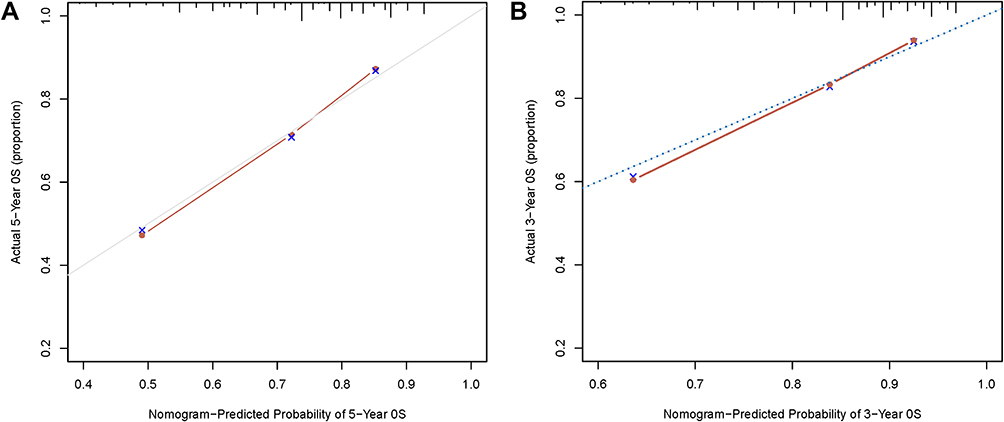 |
Figure 4 The development group. (A) Calibration plots of the nomogram for 5-year; (B) calibration plots of the nomogram for 3-year. |
 |
Figure 5 The validation group. (A) Calibration plots of the nomogram for 3-year; (B) calibration plots of the nomogram for 5-year. |
 |
Figure 6 (A) ROC curves of the nomogram predicting 3-year OS of the development group; (B) ROC curves of the nomogram predicting 5-year OS of the development group. Abbreviation: ROC, receiver operating characteristic. |
 |
Figure 7 (A) ROC curves of the nomogram predicting 3-year OS of the validation group; (B) ROC curves of the nomogram predicting 5-year OS of the validation group. Abbreviation: ROC, receiver operating characteristic. |
Discussion
Twenty percent superficial bladder tumours are diagnosed with T1 stage at presentation.13 More and more studies have proposed that all T1 bladder tumors should all be diagnosed as high-grade, although there is still a conclusion of “T1 low grade” given by some pathologists.14,15 A central review of 98 patients with T1LG bladder cancer found that almost all patients were not incorrectly classified and diagnosed with an underestimated grade.16 Compared with other styles of superficial bladder tumours, T1HG tumours were potentially fatal cancers with higher degrees of aggressiveness and progression rates (30–50%), which might be higher with long-term follow-up and lower survival rate.16–19 Due to the clinical heterogeneity, there have always been controversies on choosing the best treatment for a patient based on the aggressiveness of their cancer. For instance, a patient with T1HG treated with BCG and progressing to muscle-invasive bladder cancer or N1 was undertreated, whereas a patient who could have responded to BUG but received RC was considered overtreated.19 Early radical cystectomy had taken an increasingly important position in the treatment of T1HG patients, although BCG therapy remained the current gold-standard adjuvant therapy.18 A tool, which could predict the prognosis of T1HG patients after RC, was urgently needed to provide recommendations on treatment options.
Our study established and internally validated a highly accurate and discriminating nomogram based on several factors, including demographic, tumour characteristics, and treatment data to predict OS for TIHG bladder cancer patients after RC. The most accurate and ideal nomogram predicting OS was based on the reduced model, which deleted some non-essential and noninformative variables. The univariate and multivariate Cox regression analysis firstly filtered influential variables as candidates for the final model. We performed sensitivity analysis by entering variables gradually into the model, with the C-index, 3-year AUC and 5-year AUC as the measure of accuracy (Table 3). This method generated a highly accurate and informative model, which only included practical factors without sacrificing accuracy. The nomogram offered a friendly interface to obtain the exact probability of OS at a specific time instead of using the notion of relative risk. For example, the clinicians usually use conventional histopathology like tumour grade and stage to provide some prognostic stratification and suggestions for therapy.19 However, the nomogram method was evaluated with C-index, a global measure of model accuracy and provided individual estimates of overall survival at specific time points after cystectomy.9,20,21 Furthermore, the nomogram model was tailored to the risk referring to characteristics of personal cancer, which was more relevant to the patient. Precise prediction could act on individual patient counselling and follow-up schedule.
We also compared the clinical value of our nomogram with that of the AJCC classification using the C-index and AUC. We excluded M stage patients and only focused on T1HG patients due to the particularity of our research. The N stage was the only remaining variable in the AJCC system. The nomogram showed better discriminative ability and accuracy than the AJCC stage in the development and validation groups with higher C-indices and AUCs.12 Meanwhile, there had been several predictive and verified models for bladder cancer after RC and the International Bladder Cancer Nomogram Consortium (IBCNC) and the Bladder Cancer Research Consortium (BCRC) nomograms were the most common to perform prognostic prediction after RC.9–11,22–25 IBCNC was used for recurrence, while BCRC was used for cancer-specific, overall, and recurrence-free survival after RC. Good model performance with better discriminative ability and accuracy was confirmed in the internal and external verification.24,25 However, they all seem not to be tailored to the special groups who had T1HG tumours after RC. First, patients with T1HG tumours had a small proportion in all patients receiving RC. Thus, a model containing all patients after RC might not be a good choice for T1HG patients. In addition, uncommonly recoding factor-like lymphovascular invasion, as well as uncommonly applied factor-like adjuvant radiotherapy, could limit their applicability.
The nomogram for OS probability prediction incorporated six factors: age, marital status, tumor size, tumor site, region nodes examined, and N stage. Two factors, including marital status and tumour site, were failed to gain statistical differences in the multivariate Cox regression analysis (P > 0.05). Nevertheless, they all showed differences before all patients splitting into the development and validation groups in the multivariate analysis (P < 0.05). This outcome might result in an insufficient sample size in the development group. Table 3 reveals that model 6 possessed the best discriminative ability and accuracy owing to higher C-index and AUCs. It is always an interesting study on the tumour site of the bladder, while there was not still a unanimous and convincing conclusion.26,27 We found that patients with a tumour on the posterior wall of the bladder demonstrated better overall survival than other sites. Easily spotted by cystoscopy and getting treatment earlier might be the reason for this result. Tao obtained the result that being married was an indicator of lower all-cause mortality compared with SDW and single status.28 Lymph node metastasis was always a risk factor for bladder cancer.13 In addition, tumor size was also related to the prognosis of cancer.29,30 Regional lymph node dissection (LND) is a crucial part of RC and evidence in recent years has suggested that a more extended LND and more lymph nodes removed provide therapeutic benefits in radical cystectomy.22,31,32 All in all, the variables used to create the model were statistically reliable as well as included based on previous research results.
There are some limitations to our study. First and most significant are the limitations in all retrospective analyses. We excluded the patients who lacked some variables information and M1 stage patients, creating selection bias. In addition, SEER was a public database that collected information on patients in multiple regions and hospitals. Different degrees of surgical techniques and pathological evaluation standards were also the cause of bias. Moreover, some vital factors like LVI and CIS, which were proven to be related to T1HG bladder cancer, were lacking in the SEER database. Simultaneously, surgical techniques and methods, such as nerve-sparing radical cystectomy, degree of extent of lymph node dissection, and robot-assisted surgery, are gradually improving with time going by. More subgroup analysis was needed to evaluate the effect of these changes. Lastly, the accuracy of our nomograms is not perfect, and it is a defect of all prognostic models. Our model could provide a survival rate in a defined period based on the results of similar patients, but we could not confirm it will occur. Therefore, large prospective clinical trials are needed for external validation.
Conclusion
We constructed a discriminative and precise nomogram that predicts the individualized probability of overall survival for patients with T1HG bladder transitional cell carcinoma after radical cystectomy. The nomogram showed a significant improvement in discriminating and accurate prediction compared to the AJCC system. Meanwhile, our model was more suitable for T1HG patients than other predicting nomograms. This nomogram may help clinicians decide treatment, patient counselling, and follow-up schedule for T1HG patients. Nonetheless, external and prospective validation is needed for wide application.
Data Sharing Statement
The data in this article come from the SEER database. This data can be found here: https://seer.cancer.gov/data/.
Ethical Approval Statement
The data from SEER are publicly available and de-identified. Consent is not requested. The study was conducted in accordance with the Declaration of Helsinki. This study used previously collected deidentified data, which was deemed exempt from review by The First Affiliated Hospital of Nanchang University.
Acknowledgments
This statement is to certify that all authors have approved the manuscript being submitted, have contributed significantly to the work, attest to the validity and legitimacy of the data and its interpretation, and agree to its submission to the International Journal of General Medicine.
Funding
This study was supported by the National Natural Science Foundation of P.R. China (Grant Nos. 81560419, 81960512, and 81760457) and Jiangxi Provincial “Double Thousand Plan” Fund Project (Grant No. jxsq2019201027).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Burger M, Catto JW, Dalbagni G, et al. Epidemiology and risk factors of urothelial bladder cancer. Eur Urol. 2013;63(2):234–241. doi:10.1016/j.eururo.2012.07.033
2. Bray F, Ferlay J, Soerjomataram I, Siegel RL, Torre LA, Jemal A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2018;68(6):394–424. doi:10.3322/caac.21492
3. Kirkali Z, Chan T, Manoharan M, et al. Bladder cancer: epidemiology, staging and grading, and diagnosis. Urology. 2005;66(6 Suppl 1):4–34. doi:10.1016/j.urology.2005.07.062
4. Witjes JA. Bladder cancer in 2015: improving indication, technique and outcome of radical cystectomy. Nat Rev Urol. 2016;13(2):74–76. doi:10.1038/nrurol.2015.272
5. Matulewicz RS, Frainey BT, Oberlin DT, Meeks JJ. high-risk of adverse pathologic features in patients with clinical T1 high-grade bladder cancer undergoing radical cystectomy. J Natl Compr Canc Netw. 2016;14(11):1403–1411. doi:10.6004/jnccn.2016.0150
6. Babjuk M, Burger M, Comperat EM, et al. European Association of urology guidelines on non-muscle-invasive bladder cancer (TaT1 and Carcinoma In Situ) - 2019 update. Eur Urol. 2019;76(5):639–657. doi:10.1016/j.eururo.2019.08.016
7. Chang SS, Boorjian SA, Chou R, et al. Diagnosis and treatment of non-muscle invasive bladder cancer: AUA/SUO guideline. J Urol. 2016;196(4):1021–1029. doi:10.1016/j.juro.2016.06.049
8. Wang J, Wu Y, He W, Yang B, Gou X. Nomogram for predicting overall survival of patients with bladder cancer: a population-based study. Int J Biol Markers. 2020;35(2):29–39. doi:10.1177/1724600820907605
9. Shariat SF, Karakiewicz PI, Palapattu GS, et al. Nomograms provide improved accuracy for predicting survival after radical cystectomy. Clin Cancer Res. 2006;12(22):6663–6676. doi:10.1158/1078-0432.CCR-06-0372
10. Nomogram C, Bochner BH, Kattan MW, Vora KC; International Bladder Cancer. Postoperative nomogram predicting risk of recurrence after radical cystectomy for bladder cancer. J Clin Oncol. 2006;24(24):3967–3972.
11. Yang Z, Bai Y, Liu M, Hu X, Han P. Development and validation of a prognostic nomogram for predicting cancer-specific survival after radical cystectomy in patients with bladder cancer: a population-based study. Cancer Med. 2020;9(24):9303–9314. doi:10.1002/cam4.3535
12. Harrell FE
13. Babjuk M, Bohle A, Burger M, et al. EAU guidelines on non-muscle-invasive urothelial carcinoma of the bladder: update 2016. Eur Urol. 2017;71(3):447–461. doi:10.1016/j.eururo.2016.05.041
14. Drew PA, Furman J, Civantos F, Murphy WM. The nested variant of transitional cell carcinoma: an aggressive neoplasm with innocuous histology. Mod Pathol. 1996;9(10):989–994.
15. Truong M, Liang L, Kukreja J, O’Brien J, Jean-Gilles J, Messing E. Cautery artifact understages urothelial cancer at initial transurethral resection of large bladder tumours. Can Urol Assoc J. 2017;11(5):E203–e6. doi:10.5489/cuaj.4172
16. Solberg A, Viset T, Haugen OA, Mjønes J, Klepp O, Angelsen A. Histopathological outcome in 167 patients operated on with radical retropubic prostatectomy. Scand J Urol Nephrol. 2005;39(4):283–288. doi:10.1080/00365590510031219x
17. Herr HW. Progression of stage T1 bladder tumors after intravesical bacillus Calmette-Guerin. J Urol. 1991;145(1):40–43. doi:10.1016/S0022-5347(17)38242-3
18. Morales A, Eidinger D, Bruce AW. Intracavitary bacillus Calmette-Guerin in the treatment of superficial bladder tumors. J Urol. 2017;197(2S):S142–S5. doi:10.1016/j.juro.2016.10.101
19. Jordan B, Meeks JJ. T1 bladder cancer: current considerations for diagnosis and management. Nat Rev Urol. 2019;16(1):23–34. doi:10.1038/s41585-018-0105-y
20. Kattan MW, Eastham JA, Stapleton AM, Wheeler TM, Scardino PT. A preoperative nomogram for disease recurrence following radical prostatectomy for prostate cancer. J Natl Cancer Inst. 1998;90(10):766–771. doi:10.1093/jnci/90.10.766
21. Kattan MW, Wheeler TM, Scardino PT. Postoperative nomogram for disease recurrence after radical prostatectomy for prostate cancer. J Clin Oncol. 1999;17(5):1499–1507. doi:10.1200/JCO.1999.17.5.1499
22. Karakiewicz PI, Shariat SF, Palapattu GS, et al. Nomogram for predicting disease recurrence after radical cystectomy for transitional cell carcinoma of the bladder. J Urol. 2006;176(4 Pt 1):
23. Dotan ZA, Kavanagh K, Yossepowitch O, et al. Positive surgical margins in soft tissue following radical cystectomy for bladder cancer and cancer specific survival. J Urol. 2007;178(6):
24. Al-Daghmin A, English S, Kauffman EC, et al. External validation of preoperative and postoperative nomograms for prediction of cancer-specific survival, overall survival and recurrence after robot-assisted radical cystectomy for urothelial carcinoma of the bladder. BJU Int. 2014;114(2):253–260. doi:10.1111/bju.12484
25. Zaak D, Burger M, Otto W, et al. Predicting individual outcomes after radical cystectomy: an external validation of current nomograms. BJU Int. 2010;106(3):342–348. doi:10.1111/j.1464-410X.2009.09138.x
26. Dutta R, Abdelhalim A, Martin JW, et al. Effect of tumor location on survival in urinary bladder adenocarcinoma: a population-based analysis. Urol Oncol. 2016;34(12):
27. Wedel SA, Jones J, Tsaur I, et al. Association of intravesical tumor location with metastases to the pelvic lymph nodes in transitional cell cancer of the bladder. Am J Med Sci. 2010;339(4):341–344. doi:10.1097/MAJ.0b013e3181d2c590
28. Tao L, Pan X, Zhang L, et al. Marital status and prognostic nomogram for bladder cancer with distant metastasis: a SEER-based study. Front Oncol. 2020;10:586458. doi:10.3389/fonc.2020.586458
29. Soria F, Pisano F, Gontero P, et al. Predictors of oncological outcomes in T1G3 patients treated with BCG who undergo radical cystectomy. World J Urol. 2018;36(11):1775–1781. doi:10.1007/s00345-018-2450-0
30. Xie HY, Zhu Y, Yao XD, et al. Development of a nomogram to predict non-organ-confined bladder urothelial cancer before radical cystectomy. Int Urol Nephrol. 2012;44(6):1711–1719. doi:10.1007/s11255-012-0273-2
31. Perera M, McGrath S, Sengupta S, Crozier J, Bolton D, Lawrentschuk N. Pelvic lymph node dissection during radical cystectomy for muscle-invasive bladder cancer. Nat Rev Urol. 2018;15(11):686–692. doi:10.1038/s41585-018-0066-1
32. Lerner SP, Svatek RS. What is the standard of care for pelvic lymphadenectomy performed at the time of radical cystectomy? Eur Urol. 2019;75(4):612–614. doi:10.1016/j.eururo.2018.12.028
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.