Back to Journals » Drug Design, Development and Therapy » Volume 19
Development and Validation of a Predictive Model for HBsAg Seroclearance After Peg-IFN-Based Therapy: A Multicentre Study
Authors Liu HH ![]() , Jiang XM, Cui C
, Jiang XM, Cui C ![]() , Zhao J, Xu J, Wang SK, Hu LH, Yin YP, Wang X, Yu LJ, Xu C, Zhao ZH, Xing YQ
, Zhao J, Xu J, Wang SK, Hu LH, Yin YP, Wang X, Yu LJ, Xu C, Zhao ZH, Xing YQ ![]() , Liu Y, Wang K, Gao S
, Liu Y, Wang K, Gao S
Received 9 June 2025
Accepted for publication 28 October 2025
Published 7 November 2025 Volume 2025:19 Pages 9973—9982
DOI https://doi.org/10.2147/DDDT.S545700
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Muzammal Hussain
Hui-Hui Liu,1 Xue-Mei Jiang,2 Chao Cui,3 Jing Zhao,4 Juan Xu,5 Si-Kui Wang,6 Lei-Hua Hu,7 Yan-Ping Yin,8 Xiao Wang,9 Li-Jun Yu,10 Cheng Xu,11 Zheng-Hua Zhao,12 Yan-Qing Xing,13 Yue Liu,3 Kai Wang,1 Shuai Gao1
1Department of Hepatology, Qilu Hospital of Shandong University, Jinan, Shandong, People’s Republic of China; 2Department of Hepatology, Shandong Public Health Clinical Center, Jinan, Shandong, People’s Republic of China; 3Department of Infectious Disease, Qilu Hospital of Shandong University Dezhou Hospital, Dezhou, Shandong, People’s Republic of China; 4Department of Infectious Disease, Weifang People’s Hospital, Shandong Second Medical University, Weifang, Shandong, People’s Republic of China; 5Department of Infectious Disease, Shengli Oilfield Central Hospital, Dongying, Shandong, People’s Republic of China; 6Department of Infectious Disease, Liaocheng People’s Hospital, Liaocheng, Shandong, People’s Republic of China; 7Department of Internal Medicine, Jinmen Lake Street Community Health Service Center, Tianjin, People’s Republic of China; 8Department of Gastroenterology, Yantai City Yantai Mountain Hospital, Yantai, Shandong, People’s Republic of China; 9Liver Disease Center, Digestive Diseases Hospital of Shandong First Medical University, Jining, Shandong, People’s Republic of China; 10Department of Epidemiology, The First Affiliated Hospital of Shandong First Medical University & Shandong Provincial Qianfoshan Hospital, Jinan, Shandong, People’s Republic of China; 11Department of Infectious Disease, Linyi People’s Hospital, Linyi, Shandong, People’s Republic of China; 12Department of Infectious Disease, Taian City Central Hospital, Taian, Shandong, People’s Republic of China; 13Department of Infectious Disease, Zibo Central Hospital, Zibo, Shandong, People’s Republic of China
Correspondence: Shuai Gao, Department of Hepatology, Qilu Hospital of Shandong University, No. 107, Wenhuaxi Road, Jinan, Shandong, 250012, People’s Republic of China, Tel +86-531-82169596, Fax +86-531-86927544, Email [email protected]
Purpose: Early prediction of HBsAg seroclearance prior to the application of Peg-IFN-based therapy has important clinical implications. This study aims to construct a predictive model with baseline parameters for HBsAg seroclearance after Peg-IFN-based therapy in virally suppressed patients with HBeAg-negative chronic hepatitis B (CHB).
Patients and Methods: From January 1, 2018 to May 1, 2023, we retrospectively enrolled 377 nucleos(t)ide analogue-suppressed patients with HBeAg-negative CHB who received a 48-week Peg-IFN-based therapy from 10 centers in China. A multivariate cox regression model was developed for predicting HBsAg seroclearance in a development cohort with 229 patients recruited from 5 centers, then validated in an independent validation cohort with 148 patients recruited from another 5 centers. This study is registered with ClinicalTrials.gov, number NCT06196632.
Results: In the development and validation cohort, 17.9% (41/229) and 20.27% (30/148) of patients achieved HBsAg seroclearance, respectively. The best performing model was constructed by age (HR 0.962, 95% CI 0.928– 0.997), baseline HBsAg (HR 0.998, 95% CI 0.997– 0.999) and alanine aminotransferase (HR 1.008, 95% CI 1.003– 1.012). It showed good predictive performance in predicting HBsAg seroclearance in both the development [area under the receiver operating characteristic curve (AUC) 0.842] and validation cohort (AUC 0.852). Using cut-off points of − 2.7 and − 1.3, it can identify HBeAg-negative CHB patients with high, intermediate and low incidence rate of HBsAg seroclearance.
Conclusion: A model was constructed with baseline parameters for predicting HBsAg seroclearance after Peg-IFN-based therapy in virally suppressed patients with HBeAg-negative CHB. It showed good predictive value and can provide guidance for the clinical application of Peg-IFN-based therapy.
Keywords: chronic hepatitis B, pegylated interferon alfa, HBsAg seroclearance, multicentre study, predictive model
Introduction
Hepatitis B virus (HBV) infection is a major public health problem worldwide.1 In 2019, it was estimated that 296 million people were chronically infected with HBV across the world.2,3 Patients with chronic hepatitis B (CHB) are at high risk of developing liver cirrhosis (LC), hepatocellular carcinoma (HCC) and liver failure.4 The optimal treatment endpoint for patients with CHB is achieving functional cure, which is characterized by HBsAg seroclearance and HBV DNA less than the lower limit of quantitation.5,6 It allows a safe discontinuation of antiviral treatment and associates with significantly lower risk of LC and HCC.7 However, the rate of HBsAg seroclearance in treatment-naive adults with chronic HBV infection is only about 1% per year.8,9
Current therapies of CHB mainly include nucleos(t)ide analogues (NUC) and pegylated interferon alfa (Peg-IFN-α).10,11 NUC can profoundly suppress HBV replication. However, it requires long-term therapy and is associated with low incidence rate of HBsAg seroclearance. Peg-IFN-α, which has both immune modulatory and antiviral effects, is associated with better response rate than NUC. Nevertheless, Peg-IFN-α has several side-effects, such as influenza-like symptoms, neutropenia, thrombocytopenia, depression, as well as exacerbation of liver biochemistry and thyroid function, etc.4 In addition, the contraindications for Peg-IFN-α include decompensated cirrhosis, pregnancy, autoimmune illnesses, etc.12 Given its side-effects and contraindications, Peg-IFN-based therapy should be performed individualized.13
In patients who already achieved virological response with long-term NUC treatment, adding on Peg-IFN-α can result in significantly higher HBsAg seroclearance rate.12 In several randomized controlled trials, the incidence rate of HBsAg seroclearance can be increased to more than 30% in selected patients.14,15 Early identification of CHB patients who are likely to achieve HBsAg seroclearance is essential for guiding the application of Peg-IFN-based therapy.
In previous studies, several predictive models have been proposed for predicting HBsAg seroclearance in patients with CHB. However, most of these models include parameters such as HBV RNA, HBcrAg or intrahepatic cccDNA, which limited the clinical usage.15–17 There is an urgent need for simple models to guide precision therapy decision, ensuring Peg-IFN-based therapy is prioritized for patients most likely to benefit while sparing others from ineffective treatment and associated side effects.
In this study, we aim to develop and validate a predictive model with simple baseline parameters for HBsAg seroclearance in virally suppressed patients with HBeAg-negative CHB who received a 48-week Peg-IFN-based therapy. It can be applied in most hospitals and provide guidance for the clinical application of Peg-IFN-based therapy.
Materials and Methods
Patients and Control
This retrospective cohort study was conducted from January 1, 2018, to May 1, 2023. The participants were enrolled from 10 centers in China. Patients with CHB, HBeAg-negative and aged 18–65 years, who had received NUC treatment for more than a year and HBV DNA less than lower limit of quantification (<100 copies/mL) were eligible for inclusion. Then, the participants were treated with 48 weeks of Peg-IFN-ɑ (180μg/week) combined with NUC.
Exclusion criteria included: (1) co-infected with hepatitis A, C, D, E virus or human immunodeficiency virus; (2) other liver diseases such as alcoholic hepatitis, autoimmune liver diseases; (3) liver cirrhosis; (4) liver malignancy or other malignancy; (5) pregnancy or lactation; (6) receiving interferon within the previous 6 months; (6) allergy or other contraindication to Peg-IFN-α; (7) decline to participate; (8) loss to follow-up.
Informed consent was obtained from each participant. The potential benefits to participants include a high chance of functional cure and better prognosis. All co-authors had reviewed and approved the final manuscript. The study protocol was approved by the local Research and Ethics Committee in Qilu Hospital of Shandong University and other participating centers, in accordance with the guidelines of the 1975 Declaration of Helsinki (approval number: KYLL-202312-004-1).
Data Collection
Demographic data were collected by experienced clinicians. BMI (body mass index) was calculated according to the formula: BMI = weight/height2 (kg/m2). The type of NUC was also evaluated as a variable in this study, which includes entecavir (ETV), tenofovir disoproxil fumarate (TDF) or tenofovir alafenamide hemifumarate (TAF).
Blood samples were drawn from each participant by trained physicians at baseline prior to the application of Peg-IFN-based therapy. All participants were fasting for at least 12 hours prior to the collection of blood samples. The serum biochemical parameters (COBAS, Roche Diagnostics) included ALT, aspartate aminotransferase (AST), gamma-glutamyl transferase (GGT), alkaline phosphatase (ALP), total bilirubin (TBIL), direct bilirubin (DBIL), albumin (ALB), blood urea nitrogen (BUN), creatinine (Cr). Haematological markers (Sysmex XE-2100, Sysmex Corporation) included white blood cell (WBC), hemoglobin (HGB) and platelet (PLT), lymphocyte (LYM) and neutrophils (NEU). HBV serological markers (Abbott, Chicago, IL, USA) included HBsAg, HBeAg and HBcAb-IgG. HBV DNA was measured by the Cobas Taqman assay (Roche Diagnostics).
Statistical Analysis
Quantitative variables were expressed as median (centile 25; centile 75). Categorical variables were expressed as number (percentage). SPSS 16.0 statistical software was used to analyze the data. Quantitative variables were compared using Student’s t test and Mann–Whitney U-test. Categorical variables were compared using Chi-square test. In the development cohort, we used univariate cox proportional hazards regression analysis to determine the association between the variables and HBsAg seroclearance. Then, the variables with a P value of <0.05 entered a forward conditional step-wise cox proportional hazards regression. The receiver operating characteristic (ROC) curve was used to determine the predictive value of the model for HBsAg seroclearance. Sensitivity, specificity, positive-predictive value (PPV) and negative-predictive value (NPV) were calculated to determine the diagnostic accuracy. Kaplan–Meier survival analysis was used to estimate cumulative HBsAg seroclearance rate. All statistical analyses were two sided. P < 0.05 was considered to be statistically significant.
Results
General Characteristics
From January 1, 2018 to May 1, 2023, a total of 485 virally suppressed patients with HBeAg-negative CHB were screened at 10 centers in China. In the development cohort, we screened 293 patients from 5 centers (Qilu Hospital of Shandong University, Shandong Public Health Clinical Center, Digestive Diseases Hospital of Shandong First Medical University, The First Affiliated Hospital of Shandong First Medical University & Shandong Provincial Qianfoshan Hospital, Weifang People’s Hospital). Eighteen patients were excluded for decline to participate and 46 patients for loss of follow-up. In the validation cohort, we screened 192 patients from another 5 centers (Linyi People’s Hospital, Liaocheng People’s Hospital, Shengli Oilfield Central Hospital, Taian City Central Hospital, Zibo Central Hospital). Twenty patients were excluded for decline to participate and 24 patients for loss of follow-up. Finally, 229 patients entered the development cohort, and 148 patients entered the external validation cohort (Supplementary Figure 1).
Baseline characteristics of the patients in the development and validation cohorts were presented in Table 1. In the development cohort, 82.1% (188/229) of patients were male. The median age was 40 years. The median baseline HBsAg and ALT were 372.02 IU/mL and 29 U/L, respectively. In the validation cohort, 80.41% (119/148) of patients were male. The median age was 40 years. The median baseline HBsAg and ALT were 779.32 IU/mL and 33.85 U/L, respectively. About 74.24% (170/229) patients in the development cohort and 75% (111/148) patients in the validation cohort had HBsAg level less than 1500IU/mL. After 48-week treatment, 17.9% (41/229) and 20.27% (30/148) of patients achieved HBsAg seroclearance respectively in the development and validation cohort, respectively. No significant differences were observed between the demographic, biochemical and clinical parameters in the development and validation cohorts.
 |
Table 1 Baseline Characteristics of Participants Included in the Development and Validation Cohorts |
Baseline characteristics of participants received HBsAg seroclearance and those not in the development cohort was presented in Table 2. No significant difference was observed in gender, BMI, NUC, HBcAb-IgG, GGT, AKP, TBIL, DBIL, ALB, BUN, Cr, WBC, HGB, PLT, NEU, LYM at baseline between participants received HBsAg seroclearance after treatment and those not. However, participants received HBsAg seroclearance were significantly younger (P < 0.01). Meanwhile, they had significantly lower baseline HBsAg (P < 0.01) and higher ALT (P < 0.01), AST level (P < 0.01).
 |
Table 2 Baseline Characteristics of Participants Received HBsAg Seroclearance and Those Not in the Development Cohort |
Predictors of HBsAg Seroclearance After Peg-IFN-Based Therapy
In the development cohort, univariate analysis identified four variables including age (P = 0.009), HBsAg (P = 0.001), ALT (P < 0.001), AST (P = 0.001). Then these variables were introduced into a multivariate analysis. Age (HR 0.962, 95% CI 0.928–0.997, P = 0.035), HBsAg (HR 0.998, 95% CI 0.997–0.999, P = 0.003) and ALT (HR 1.008, 95% CI 1.003–1.012, P = 0.001) were identified to be independent predictors for HBsAg seroclearance after Peg-IFN-based therapy in virally-suppressed patients with HBeAg-negative CHB (Table 3).
 |
Table 3 Identification of Independent Predictors for HBsAg Seroclearance |
Construction of the Prognostic Model
A prognostic model for predicting HBsAg seroclearance after Peg-IFN-based therapy in patients with HBeAg-negative CHB was constructed by combining the three independent predictors with the regression coefficients reported in Table 3. It was calculated according to the formula: FC-48w score = 0.008 × baseline ALT - 0.039 × age - 0.002 × baseline HBsAg.
The Validation of FC-48w Score
The FC-48w score in patients with HBeAg-negative CHB received HBsAg seroclearance were significantly higher than those not in the development cohort (Z = −6.863, P < 0.001) (Figure 1A), validation cohort (Z = −5.948, P < 0.001) (Figure 1B) as well as the entire cohort (Z = −8.937, P < 0.001) (Figure 1C). The AUC of the FC-48w score in predicting HBsAg seroclearance was 0.842 (standard error [SE] 0.032, 95% confidence interval [CI] 0.788–0.887) in the development cohort (Figure 2A), 0.852 (SE 0.035, 95% CI 0.785–0.905) (Figure 2B) in the validation cohort and 0.840 (SE 0.024, 95% CI 0.799–0.876) (Figure 2C) in the entire cohort.
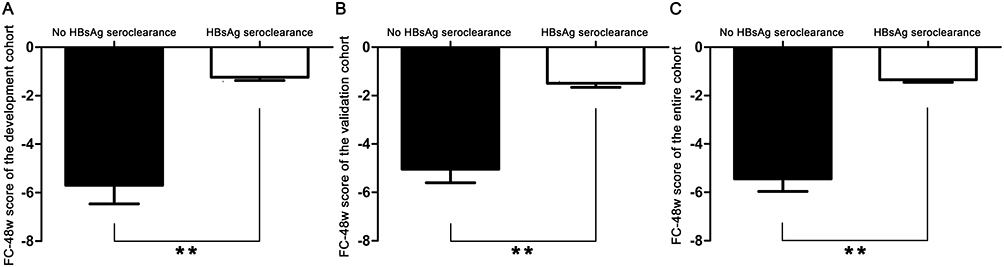 |
Figure 1 The comparison of FC-48w scores between patients received HBsAg seroclearance and those not in the development cohort (A), validation cohort (B) and entire cohort (C). ** P < 0.01. |
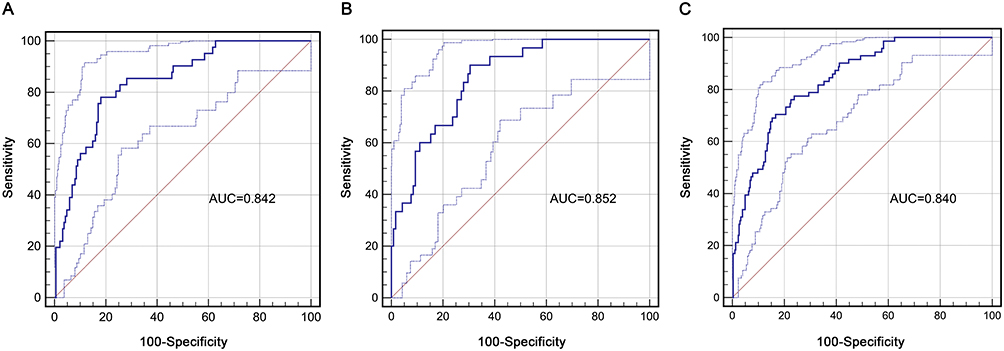 |
Figure 2 The ROC curves of the FC-48w score in predicting HBsAg seroclearance after Peg-IFN-based therapy in the development cohort (A), validation cohort (B) and entire cohort (C). |
In the development cohort, two cut-off points were chosen for FC-48w score to predict HBsAg seroclearance after Peg-IFN-based therapy in patients with HBeAg-negative CHB. A high cut-off point was chosen based on the ROC analysis of FC-48w score to provide a specificity of at least 85%. A low cut-off point was chosen to provide a sensitivity of at least 90%.18 Finally, −1.3 was identified as a high cut-off point and −2.7 as a low cut-off point (Supplementary Table 1). In the development cohort, 96 patients (41.92%) had an FC-48w score ≤ −2.7, 84 (36.68%) had a FC-48w score between −2.7 and −1.3, and 49 patients (21.40%) had a FC-48w score > −1.3. The cut-off point of −2.7 provided a sensitivity of 90.24%. The cut-off point of −1.3 provided a specificity of 86.70%. In the validation cohort, 73 patients (49.32%) had an FC-48w score ≤ −2.7, 55 (37.16%) had a FC-48w score between −2.7 and −1.3, and 20 patients (13.51%) had a FC-48w score > −1.3. The cut-off point of −2.7 provided a sensitivity of 93.33%. The cut-off point of −1.3 provided a specificity of 92.37%.
Using the cut-off points of −2.7 and −1.3, FC-48w score successfully identified HBeAg-negative CHB patients with high-, intermediate- and low-incidence rate of HBsAg seroclearance after Peg-IFN-based therapy (Supplementary Table 2). In the development cohort, only 4 of the 96 patients (4.17%) in the low-probability group achieved HBsAg seroclearance. Thirteen of the 84 patients (15.48%) in the intermediate-probability group achieved HBsAg seroclearance. Twenty-four of the 49 patients (48.98%) in the high-probability group achieved HBsAg seroclearance. In the validation cohort, only 2 of the 73 patients (2.74%) in the low-probability group achieved HBsAg seroclearance. Seventeen of the 55 patients (30.91%) in the intermediate-probability group achieved HBsAg seroclearance. Eleven of the 20 patients (55.00%) in the high-probability group achieved HBsAg seroclearance. In the entire cohort, only 6 of the 169 patients (3.55%) in the low-probability group achieved HBsAg seroclearance. Thirty of the 139 patients (21.58%) in the intermediate-probability group achieved HBsAg seroclearance. Thirty-five of the 69 patients (50.72%) in the high-probability group achieved HBsAg seroclearance.
Then, we use Kaplan–Meier survival analysis compare the cumulative HBsAg seroclearance rate of patients in the low-, intermediate- and high-probability group. As shown in Figure 3A–C, the cut-off points of −2.7 and −1.3 successfully identified HBeAg-negative CHB patients with low, intermediate and high incidence rate of HBsAg seroclearance after Peg-IFN-based therapy in the development cohort, validation cohort and entire cohort (P < 0.001, respectively).
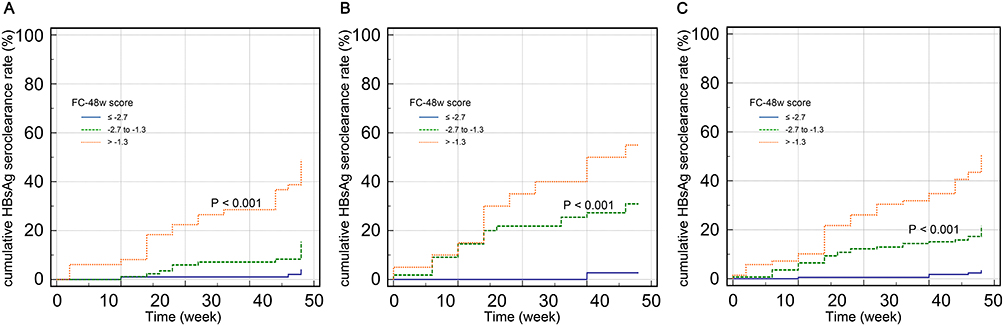 |
Figure 3 Kaplan-Meier graphs showing cumulative HBsAg seroclearance rate in patients within the low-, intermediate- and high-probability group in the development cohort (A), validation cohort (B) and entire cohort (C). |
Clinical Application of FC-48w Score
Algorithm for FC-48w score to guide the clinical application of Peg-IFN-based therapy was presented in Supplementary Figure 2. Patients with HBeAg-negative CHB can be classified into low-, intermediate- and high-probability group by FC-48w score. Peg-IFN-based therapy is highly recommended for patients in high-probability group, which have HBsAg seroclearance rate of about 50%. Peg-IFN-based therapy is not recommended for patients in low-probability group, which have HBsAg seroclearance rate of less than 5%. In the intermediate-probability group, the patients have HBsAg seroclearance rate of about 20%. Therefore, Peg-IFN-based therapy might also be suggested in them but should be individualized.
Discussion
In this study, a model was constructed and externally validated for predicting HBsAg seroclearance after Peg-IFN-based therapy in virally suppressed patients with HBeAg-negative CHB. The FC-48w score showed good predictive performance in both the development and validation cohort. It was constructed by baseline parameters and can be widely used in clinical practice for guiding the application of Peg-IFN-based therapy. With the cut-off points of −2.7 and −1.3, FC-48w score successfully identified HBeAg-negative CHB patients with low, intermediate and high incidence rate of HBsAg seroclearance after Peg-IFN-based therapy.
Functional cure, which is characterized by sustained HBsAg loss, is recommended as the optimal treatment endpoint for patients with CHB.19,20 Although NUCs remain the most common therapeutic strategy for patients with CHB, the HBsAg seroclearance rate of NUC is extremely low.21 Peg-IFN-based therapy showed significantly better response rate and the HBsAg seroclearance rate can be increased to more than 30% in selected patients.22 However, predicting who will achieve HBsAg seroclearance remains challenging and is essential for the application of Peg-IFN-based therapy. Therefore, the FC-48w score’s primary clinical value lies in its ability to guide precision therapy decision, ensuring Peg-IFN-based therapy is prioritized for patients most likely to benefit while sparing others from ineffective treatment and associated side effects. This enhances cost-effectiveness and reduces unnecessary healthcare burdens. Additionally, by improving patient selection, the model increases the therapeutic success rate, thus offering better long-term outcomes. Clinically, this model provides real-world applicability-requiring only routine laboratory markers-making it feasible for widespread adoption in diverse healthcare settings. It empowers clinicians to make evidence-based, individualized decisions, ultimately advancing the goal of functional cure in appropriately selected CHB patients.
In this study, age, baseline HBsAg and baseline ALT were identified to be independent predictors of HBsAg seroclearance. Younger patients might have better immune response against HBV. Therefore, they might also have had better treatment response to Peg-IFN-α-based therapy.23 The low level of HBsAg in serum reflected a smaller amount of cccDNA in the liver. Therefore, baseline HBsAg was found to be an indicator for HBsAg seroclearance in patients with CHB underwent NUC or Peg-IFN-α treatment.24 ALT, which reflected the liver inflammation, might also be associated with the immune clearance of HBV and the treatment efficacy of antiviral therapy. In a study performed by Leung RH et al, ALT to HBsAg ratio was found to be effective in predicting HBsAg seroclearance after entecavir cessation in patients with CHB.25 In another study, the ALT to qHBsAg ratio was also found to be a promising predictor of HBsAg seroclearance in patients with treatment-naïve CHB received Peg-IFN-α-based therapy.26 However, few studies have been proposed to identify predictors for HBsAg seroclearance after Peg-IFN-based therapy in virally suppressed patients with HBeAg-negative CHB.
The longitudinal changes in HBV markers such as the HBsAg decline at week 12 might also have good predictive value for HBsAg seroclearance.27 However, identifying patients who are likely to achieve HBsAg seroclearance prior to the application of Peg-IFN-based therapy is more valuable in clinical work. Therefore, we only evaluated the variables at baseline. Meanwhile, several other variables such as HBV RNA, HBcrAg or intrahepatic cccDNA might enhance the predictive value of the model.16,28,29 However, these variables were not routinely tested in a large proportion of hospitals, which limited the clinical usage of them.
There were also several limitations in this study. Because Peg-IFN-based therapy was usually applied for CHB patients with relatively low HBsAg level in current clinical work. Most of the CHB patients enrolled in this study had HBsAg level less than 1500IU/mL. Meanwhile, this study was performed in a Chinese population. Therefore, the FC-48w score still needed to be validated prior to its application outside China.
Conclusion
In conclusion, we have developed a predictive model utilizing baseline parameters to forecast HBsAg seroclearance following Peg-IFN-based therapy in patients with HBeAg-negative CHB who are virologically suppressed. This model demonstrates robust predictive accuracy, with AUC values of 0.842 and 0.852 in the development and validation cohorts, respectively. By identifying patients with high, intermediate, and low incidence rates of HBsAg seroclearance using specific cut-off points, our model offers valuable guidance for the clinical application of Peg-IFN-based therapy. This study is significant as it contributes to a better understanding of the factors influencing HBsAg seroclearance and aids in the individualization of treatment strategies for patients with HBeAg-negative CHB.
Highlights
In this study, we created a simple tool to predict which chronic hepatitis B patients would benefit most from pegylated interferon alfa-based therapy. By analyzing 377 patients, we found three key predictors of successful treatment: younger age, lower starting HBsAg levels, and higher liver enzyme levels. Our model accurately identifies patients with high, medium, or low chances of clearing hepatitis B virus, helping doctors choose the best candidates for Peg-IFN-based therapy and avoid unnecessary treatment for others. This tool makes treatment decisions smarter and gives patients better chances of overcoming chronic hepatitis B.
Consent for Publication
The authors confirm that this study is registered with ClinicalTrials.gov, number NCT06196632. The abstract of this article has been submitted to the 34th Annual Meeting of Asia-Pacific Association for the Study of the Liver (APASL 2025 BEIJING). The full article has not been published previously and is not under consideration for publication elsewhere. All authors have approved the manuscript for publication and agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Funding
This work was supported by the National Key Research and Development Program of China (2021YFC2301801), Natural Science Foundation of Shandong Province (ZR2022MH006), Crosswise Project of Shandong University (6010123188, 6010125191).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Hur MH, Yip TC, Kim SU, et al. A machine learning model to predict liver-related outcomes after the functional cure of chronic hepatitis B. J Hepatol. 2025;82(2):235–244. doi:10.1016/j.jhep.2024.08.016
2. Sarin SK, Kumar M, Lau GK, et al. Asian-Pacific clinical practice guidelines on the management of hepatitis B: a 2015 update. Hepatol Internat. 2016;10(1):1–98. doi:10.1007/s12072-015-9675-4
3. Jeng WJ, Papatheodoridis GV, Lok ASF. Hepatitis B. Lancet. 2023;401(10381):1039–1052. doi:10.1016/s0140-6736(22)01468-4
4. Terrault NA, Lok ASF, McMahon BJ, et al. Update on prevention, diagnosis, and treatment of chronic hepatitis B: AASLD 2018 hepatitis B guidance. Hepatology. 2018;67(4):1560–1599. doi:10.1002/hep.29800
5. Ghany MG, Buti M, Lampertico P, Lee HM. Guidance on treatment endpoints and study design for clinical trials aiming to achieve cure in chronic hepatitis B and D: report from the 2022 AASLD-EASL HBV-HDV treatment endpoints conference. J Hepatol. 2023;79(5):1254–1269. doi:10.1016/j.jhep.2023.06.002
6. Cornberg M, Lok AS, Terrault NA, Zoulim F. Guidance for design and endpoints of clinical trials in chronic hepatitis B - Report from the 2019 EASL-AASLD HBV Treatment Endpoints Conference(‡). J Hepatol. 2020;72(3):539–557. doi:10.1016/j.jhep.2019.11.003
7. Zhang JW, Lai RM, Wang LF, et al. Varied immune responses of HBV-specific B cells in patients undergoing pegylated interferon-alpha treatment for chronic hepatitis B. J Hepatol. 2024;81(6):960–970. doi:10.1016/j.jhep.2024.06.033
8. Zhou K, Contag C, Whitaker E, Terrault N. Spontaneous loss of surface antigen among adults living with chronic hepatitis B virus infection: a systematic review and pooled meta-analyses. Lancet Gastroenterol Hepatol. 2019;4(3):227–238. doi:10.1016/s2468-1253(18)30308-x
9. Yeo YH, Ho HJ, Yang HI, et al. Factors associated with rates of HBsAg seroclearance in adults with chronic HBV infection: a systematic review and meta-analysis. Gastroenterology. 2019;156(3):635–646e9. doi:10.1053/j.gastro.2018.10.027
10. Agarwal K, Brunetto M, Seto WK, et al. 96 weeks treatment of tenofovir alafenamide vs. tenofovir disoproxil fumarate for hepatitis B virus infection. J Hepatol. 2018;68(4):672–681. doi:10.1016/j.jhep.2017.11.039
11. Lee SK, Kwon JH, Lee SW, et al. Sustained off therapy response after peglyated interferon favours functional cure and no disease progression in chronic hepatitis B. Liver Int. 2021;41(2):288–294. doi:10.1111/liv.14701
12. Hu Q, Qi X, Yu Y, et al. The efficacy and safety of adding on or switching to peginterferon α-2b in HBeAg-positive chronic hepatitis B patients with long-term entecavir treatment: a multicentre randomised controlled trial. Aliment Pharmacol Ther. 2022;56(9):1394–1407. doi:10.1111/apt.17222
13. Ning Q, Wu D, Wang GQ, et al. Roadmap to functional cure of chronic hepatitis B: an expert consensus. J Viral Hepatitis. 2019;26(10):1146–1155. doi:10.1111/jvh.13126
14. Wu D, Wang P, Han M, et al. Sequential combination therapy with interferon, interleukin-2 and therapeutic vaccine in entecavir-suppressed chronic hepatitis B patients: the Endeavor study. Hepatol Internat. 2019;13(5):573–586. doi:10.1007/s12072-019-09956-1
15. Huang D, Wu D, Wang P, et al. End-of-treatment HBcrAg and HBsAb levels identify durable functional cure after Peg-IFN-based therapy in patients with CHB. J Hepatol. 2022;77(1):42–54. doi:10.1016/j.jhep.2022.01.021
16. Gao N, Guan G, Xu G, et al. Integrated HBV DNA and cccDNA maintain transcriptional activity in intrahepatic HBsAg-positive patients with functional cure following PEG-IFN-based therapy. Aliment Pharmacol Ther. 2023;58(10):1086–1098. doi:10.1111/apt.17670
17. Lim SG, Baumert TF, Boni C, et al. The scientific basis of combination therapy for chronic hepatitis B functional cure. Nat Rev Gastroenterol Hepatol. 2023;20(4):238–253. doi:10.1038/s41575-022-00724-5
18. Gao S, Han LY, Fan YC, Wang K. Early prediction model for prognosis of patients with hepatitis-B-virus-related acute-on-chronic liver failure received glucocorticoid therapy. Eur J Med Res. 2022;27(1):248. doi:10.1186/s40001-022-00891-w
19. Yardeni D, Chang KM, Ghany MG. Current best practice in hepatitis B management and understanding long-term prospects for cure. Gastroenterology. 2023;164(1):42–60e6. doi:10.1053/j.gastro.2022.10.008
20. Lok ASF. Toward a functional cure for hepatitis B. Gut Liver. 2024;18(4):593–601. doi:10.5009/gnl240023
21. Nguyen MH, Wong G, Gane E, Kao JH, Dusheiko G. Hepatitis B virus: advances in prevention, diagnosis, and therapy. Clin Microbiol Rev. 2020;33(2). doi:10.1128/cmr.00046-19
22. Liu J, Wang T, Zhang W, Cheng Y, He Q, Wang FS. Effect of combination treatment based on interferon and nucleos(t)ide analogues on functional cure of chronic hepatitis B: a systematic review and meta-analysis. Hepatol Internat. 2020;14(6):958–972. doi:10.1007/s12072-020-10099-x
23. Tang Q, Ye J, Zhang Y, et al. Establishment of a multi-parameter prediction model for the functional cure of HBeAg-negative chronic hepatitis B patients treated with pegylated interferonα and decision process based on response-guided therapy strategy. BMC Infect Dis. 2023;23(1):456. doi:10.1186/s12879-023-08443-1
24. Lim SG, Phyo WW, Ling JZJ, et al. Comparative biomarkers for HBsAg loss with antiviral therapy shows dominant influence of quantitative HBsAg (qHBsAg). Aliment Pharmacol Ther. 2021;53(1):172–182. doi:10.1111/apt.16149
25. Leung RH, Hui RW, Mak LY, et al. ALT to qHBsAg ratio predicts long-term HBsAg seroclearance after entecavir cessation in Chinese patients with chronic hepatitis B. J Hepatol. 2024;81(2):218–226. doi:10.1016/j.jhep.2024.03.022
26. Wang J, Zhang Q, Zhang S, Wu C, Huang R. ALT to qHBsAg ratio predicts HBsAg seroclearance in HBeAg-negative patients receiving Peg-IFN-α-based therapy. J Hepatol. 2025;82(5):e226–e227. doi:10.1016/j.jhep.2024.10.008
27. Li GJ, Yu YQ, Chen SL, et al. Sequential combination therapy with pegylated interferon leads to loss of hepatitis B surface antigen and hepatitis B e antigen (HBeAg) seroconversion in HBeAg-positive chronic hepatitis B patients receiving long-term entecavir treatment. Antimicrob Agents Chemother. 2015;59(7):4121–4128. doi:10.1128/aac.00249-15
28. Chuaypen N, Posuwan N, Chittmittraprap S, et al. Predictive role of serum HBsAg and HBcrAg kinetics in patients with HBeAg-negative chronic hepatitis B receiving pegylated interferon-based therapy. Clin Microbiol Infection. 2018;24(3):306e7–306e13. doi:10.1016/j.cmi.2017.07.016
29. Zeng G, Koffas A, Mak LY, Gill US, Kennedy PTF. Utility of novel viral and immune markers in predicting HBV treatment endpoints: a systematic review of treatment discontinuation studies. JHEP Reports. 2023;5(6):100720. doi:10.1016/j.jhepr.2023.100720
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.