Back to Journals » Journal of Hepatocellular Carcinoma » Volume 13
Development and Validation of a Nomogram Predictive Model for Massive Ascites After Hepatectomy in Patients with Primary Hepatocellular Carcinoma
Authors Men A, Sun D, Sun X, Jin L, Liu B, Chen F, Nan B ![]() , Wang W, Han L, Zhang W
, Wang W, Han L, Zhang W
Received 23 March 2026
Accepted for publication 18 May 2026
Published 11 June 2026 Volume 2026:13 610812
DOI https://doi.org/10.2147/JHC.S610812
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Ali Hosni
Ao Men,1,2,* Dapeng Sun,1,* Xiuqing Sun,1,* Luyuan Jin,1 Bailiang Liu,1 Fengyang Chen,1 Boyuan Nan,1 Wenxin Wang,1,2 Lei Han,1 Wei Zhang1
1Department of Hepatobiliary and Thyroid Surgery, General Hospital of Northern Theater Command, Shenyang, Liaoning, People’s Republic of China; 2Graduate School, Dalian Medical University, Dalian, Liaoning, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Wei Zhang; Lei Han, Department of Hepatobiliary and Thyroid Surgery, General Hospital of Northern Theater Command, Shenyang, Liaoning, 110016, People’s Republic of China, Email [email protected]; [email protected]
Objective: To develop and validate a nomogram for predicting massive ascites after hepatectomy in hepatocellular carcinoma (HCC) patients.
Methods: A retrospective, single‑center study of 232 HCC patients who underwent hepatectomy (February 2021 – July 2025) was conducted. Patients with preoperative bile leakage or active hemorrhage were excluded. Patients were grouped by postoperative ascites status (massive, n=66; non-massive, n=166). Predictors were screened via univariate and multivariate logistic regression. A nomogram was built and internally validated using 1000 bootstrap samples. Performance was assessed via ROC analysis, calibration, and decision curve analysis (DCA), Clinical Impact Curve (CIC.
Results: Multivariate analysis identified four independent predictors: platelet count (OR=0.985), AST (OR=1.027), portal hypertension (OR=5.288), and operative time (OR=5.011). The nomogram achieved an AUC of 0.837 (95% CI: 0.781– 0.892) with good calibration (H-L test, P=0.860). DCA showed clinical net benefit across thresholds [0.00– 0.71] and [0.86– 0.93]and the clinical impact curve showing good concordance at risk thresholds above 0.4.
Conclusion: The nomogram accurately predicts massive ascites risk using four perioperative variables and demonstrates strong clinical utility for individualized management.
Keywords: hepatectomy, hepatocellular carcinoma, postoperative complications, ascites, nomogram
Introduction
According to the 2022 Global Cancer Statistics released by the International Agency for Research on Cancer (IARC), liver cancer ranks sixth in global incidence and third in cancer-related mortality worldwide.1 In China—a region with a high burden of viral hepatitis—liver cancer is the fourth most commonly diagnosed malignancy and the second leading cause of cancer death.2 Current therapeutic strategies for hepatocellular carcinoma (HCC) are no longer limited to conventional surgical intervention, and a growing number of novel research approaches have emerged. Natural compounds represented by tocotrienols are regarded as promising alternative and adjuvant anticancer candidates, and their underlying molecular mechanisms have attracted increasing research attention.3 In patients with unresectable HCC, combination therapies such as TACE plus microwave or radiofrequency ablation have been shown to improve tumor response, as demonstrated in a randomized controlled study by Sheta et al4 Nevertheless, hepatectomy remains the primary curative treatment for HCC and can remarkably improve patients’ survival outcomes. However, HCC often arises in the context of underlying chronic liver disease, such as viral hepatitis, alcohol-related liver injury, or cirrhosis. In addition, the liver’s complex anatomical architecture, abundant vascular supply, and central metabolic role make hepatectomy a technically demanding procedure with a substantial risk of postoperative complications.5,6 Post‑hepatectomy complications occur in 20–40% of patients, among which ascites is one of the most common and clinically challenging. Another post‑hepatectomy complications include hemorrhage, infection, liver failure, bile leakage, portal vein thrombosis, pleural effusion, and more. Among common complications following hepatectomy, ascites occurs in 5–56% of cases.7 Massive postoperative ascites can lead to a range of secondary sequelae, including abdominal infection, electrolyte imbalance, and hypoalbuminemia. In severe instances, it may precipitate liver failure, substantially prolong hospitalization and elevate healthcare expenditures. Beyond its clinical impact, massive ascites also adversely affects quality of life and may increase the risk of tumor recurrence.8 The underlying pathophysiology involves multiple mechanisms, such as impaired hepatic albumin synthesis, dysregulation of fluid and sodium balance, portal hypertension, and altered hepatic lymph production.9,10 However, existing studies have predominantly examined ascites formation in the context of an unperturbed liver, thereby failing to capture the clinical complexities associated with hepatic injury. Intraoperative factors—including surgical trauma, anesthetic exposure, blood loss and transfusion, and parenchymal transection—collectively perturb hepatic hemodynamics and metabolic homeostasis, rendering the pathogenesis of postoperative ascites considerably more intricate. Consequently, conventional theories of ascites development may be insufficient to fully account for the substantial fluid accumulation observed following surgical interventions. In recent years, several preoperative indicators—including Child–Pugh classification, indocyanine green retention rate at 15 minutes (ICG-R15), magnetic resonance elastography (MRE), and Mac-2 binding protein glycosylated isomer (M2BPGi)—have shown utility in predicting postoperative complications.11–13 These tools contribute to improved risk stratification and support clinical efforts to reduce perioperative morbidity and mortality. Nevertheless, the prediction and management of massive ascites following hepatectomy warrant further in-depth investigation. Although the number of studies on post-hepatectomy ascites has been increasing globally, most remain focused on risk factor analysis, with a notable lack of systematic predictive model development.7,8,14 Specifically, a practical nomogram designed solely for massive ascites—as distinct from any ascites or post‑hepatectomy liver failure—using only routine perioperative variables is currently unavailable. As an intuitive and individualized predictive tool, the nomogram can integrate multiple predictors to provide a quantitative basis for clinical decision-making. Therefore, this study seeks to construct and validate a nomogram for predicting massive ascites after hepatectomy in patients with hepatocellular carcinoma (HCC), aiming to offer a novel approach for precise risk assessment and perioperative strategy optimization.
Materials and Methods
Research Participants
We conducted a retrospective cohort study, systematically collecting clinical data from 312 patients who underwent hepatectomy for primary hepatocellular carcinoma (HCC) at the Department of Hepatobiliary and Pancreatic Surgery, General Hospital of Northern Theater Command, from February 2021 to July 2025. The inclusion criteria were as follows: (1) diagnosis of HCC consistent with the Guidelines for the Diagnosis and Treatment of Primary Liver Cancer (2024 Edition),15 with postoperative pathological confirmation; (2) availability of complete clinical data without critical missing information; and (3) undergoing primary hepatectomy as the initial treatment. Patients were excluded based on the following criteria: (1) preoperative receipt of any conversion therapy for liver cancer, such as transarterial chemoembolization (TACE), radiofrequency ablation (RFA), targeted therapy, immunotherapy, chemotherapy, or radiotherapy, which may influence intraoperative bleeding or postoperative recovery; (2) significant incompleteness of clinical data; (3) prior history of hepatic surgery (eg, pericardial devascularization or portosystemic shunt) that could alter hepatic hemodynamics; (4) occurrence of postoperative complications such as bile leakage or hemorrhage, which could confound the assessment of ascites volume. Following rigorous application of the inclusion and exclusion criteria, 80 patients were excluded from the study. Specific reasons for exclusion included: preoperative conversion therapy (n=14), substantially incomplete clinical data (n=37), prior hepatic surgery for portal hypertension (specifically, pericardial devascularization, n=1), previous liver surgery for hepatocellular carcinoma (n=18), and postoperative complications such as bile leakage (n=10). A total of 232 patients were consequently included in the final cohort. Comprehensive preoperative, intraoperative, and postoperative clinical data were collected for all enrolled patients. Based on the presence of massive postoperative ascites—defined as either a maximum daily drainage volume exceeding 10 mL/kg of preoperative body weight or a cumulative drainage volume greater than 1500 mL within one week after surgery16—patients were categorized into a massive ascites group (n=66) and a non-massive ascites group (n=166). Owing to the invasive nature of portal venous pressure measurement, it is not routinely performed in clinical practice and was therefore excluded from preoperative assessment in this study. Preoperative diagnosis of portal hypertension was primarily based on imaging findings, with laboratory parameters serving as complementary indicators. Specifically, portal hypertension was diagnosed when imaging (computed tomography, magnetic resonance imaging, or ultrasonography) demonstrated at least two of the following: (1) splenomegaly with persistent thrombocytopenia (platelet count <100 × 109/L); (2) definite portosystemic collateral vessels, accompanied by imaging-detected ascites; and/or (3) esophagogastric varices, along with cirrhotic features such as nodular liver surface and caudate lobe hypertrophy.17
Ethics Statement
This study was conducted in accordance with the Declaration of Helsinki. The protocol for this retrospective study was reviewed and approved by the Ethics Committee of the General Hospital of the Northern Theater Command on July 2, 2025 (Approval No: Y(2025) 302). This was a retrospective, single‑center study that did not involve direct interventions or additional invasive examinations. Accordingly, the ethics committee waived the need for informed consent. All patient medical records were anonymized and de-identified prior to analysis to ensure strict confidentiality. Data were handled in compliance with relevant institutional and national privacy protection regulations.
Clinical Data Collection
Patient data were systematically collected, encompassing demographic characteristics (age, sex, body mass index), comorbidities (coronary heart disease, hypertension, diabetes), laboratory test results, and tumor-related parameters. Laboratory assessments included platelet count, hemoglobin, alpha-fetoprotein, aspartate aminotransferase, alanine aminotransferase, albumin, total bilirubin, prothrombin activity, activated partial thromboplastin time, blood urea nitrogen, creatinine, and alkaline phosphatase. Disease-specific variables consisted of hepatitis history, portal hypertension status, and Child–Pugh classificationIntraoperative variables recorded included the presence of cirrhosis, extent of hepatectomy (major resection was defined as removal of ≥3 segments, minor as <3 segments),18 duration of hepatic inflow occlusion, intraoperative blood transfusion, operative time, and surgical approach (laparoscopic, open, or conversion to laparotomy). Postoperative pathological data were also collected, with emphasis on microvascular invasion (MVI), capsular invasion, maximum tumor diameter, tumor number, histological grade, and the presence of vascular tumor thrombus.
Perioperative Management and Surgical Technique
All enrolled patients underwent comprehensive preoperative imaging to delineate tumor number, size, location, and anatomical relationships with intra- and extrahepatic vasculature and bile ducts. Patients with preoperative liver dysfunction received routine hepatoprotective therapy. All hepatectomies were performed by experienced attending surgeons (associate senior title or higher). Intraoperatively, perihepatic ligaments were mobilized, and tumor-feeding vessels were ligated. The Pringle maneuver was applied when indicated for hepatic inflow control. Liver transection was performed incrementally using an ultrasonic dissector, electrocautery, or the clamp-crush technique. Hemostasis at the resection margin was achieved by ligation, suture, or electrocoagulation, supplemented by absorbable hemostatic gauze. After thorough irrigation and confirmation of hemostasis and absence of bile leakage, drains were placed at the resection surface and Winslow’s foramen as needed. Postoperatively, abdominal drainage was closely monitored for volume, character, and color to promptly identify complications such as infection, hemorrhage, or bile leak.
Non-contrast or contrast-enhanced computed tomography (CT) of the hepatobiliary-pancreatic system was routinely performed within one week after surgery to evaluate drainage catheter placement and detect fluid collections in the surgical area. When necessary, CT- or ultrasonography-guided percutaneous catheter drainage was utilized to manage inadequate drainage. All patients were managed according to a standardized postoperative protocol, which included prophylactic antibiotics, intravenous fluid support, and hepatoprotective therapy. Symptom-directed treatments—such as analgesics, acid suppressants, and antipyretics—were administered as needed, along with intermittent pneumatic compression for deep vein thrombosis prophylaxis. After the return of bowel function (evidenced by flatus or defecation), oral intake was gradually advanced from semi-liquid to liquid and eventually to a regular diet. Laboratory tests—including complete blood count and liver and kidney function panels—were performed daily for the first three postoperative days and every three days thereafter. Treatment plans were adjusted dynamically based on hepatic function recovery and strict fluid balance records. The drainage tube may be removed when imaging examination rules out intraperitoneal fluid collection, and the drainage fluid is clear with a volume of less than 20 mL.
For patients diagnosed with massive ascites, intensive hepatoprotective therapy was initiated. When serum albumin levels dropped below 30 g/L, human albumin was promptly supplemented at a daily dose of 20 g, combined with intravenous loop diuretics (eg, furosemide 20 mg twice daily) and oral aldosterone antagonists (eg, spironolactone 20 mg three times daily) or arginine vasopressin V2 receptor antagonists (eg, tolvaptan 15 mg daily) until significant resolution of ascites was achieved.
Statistical Analysis
All data were managed in Microsoft Excel and analyzed using SPSS version 27.0.1. Study variables encompassed preoperative, intraoperative, and postoperative parameters. The Shapiro–Wilk test was used to assess normality. Normally distributed continuous variables were expressed as mean ± standard deviation (SD) and compared using the independent samples t-test; non-normally distributed variables were summarized as median with interquartile range [M (P25–P75)] and compared using the Mann–Whitney U-test. Categorical variables were presented as frequencies and compared with the chi-square test. A two-tailed P-value < 0.05 was considered statistically significant.
Univariate and multivariate binary logistic regression analyses were performed to identify risk factors for massive ascites, with results reported as odds ratios (ORs) and 95% confidence intervals (CIs). Variables significantly associated with the outcome (P < 0.05) in the multivariate model were considered independent risk factors. A nomogram was developed using the “rms” package in R (version 4.1.0) based on independent predictors identified through multivariate logistic regression. The model’s discriminative performance was evaluated by the area under the receiver operating characteristic (ROC) curve. Calibration was assessed using the Hosmer–Lemeshow test and a calibration plot. In addition, decision curve analysis (DCA) and clinical impact curve (CIC) were performed to quantify the net clinical benefit and clinical utility of the nomogram across different threshold probabilities.
Results
This study included 232 patients, comprising 191 (82.3%) males and 41 (17.7%) females. The mean age was 62 years, with a range of 24 to 84 years. Postoperative massive ascites occurred in 66 patients (28.4%), demarcating the massive ascites group, while the remaining 166 patients (71.6%) constituted the non-massive ascites group. The detailed baseline characteristics of all enrolled patients are summarized in Table 1.
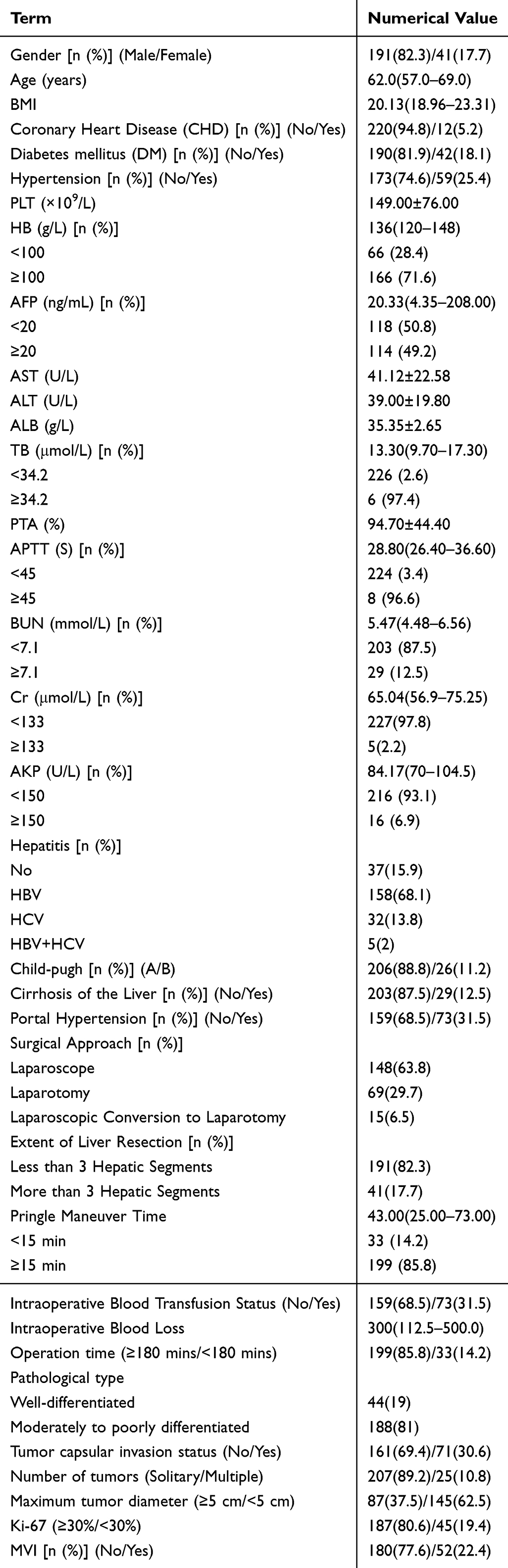 |
Table 1 Baseline Characteristics of Hepatocellular Carcinoma Patients |
Univariate Analysis of Massive Ascites in Patients with HCC
Univariate logistic regression was performed to identify factors associated with massive ascites following hepatectomy in 232 hepatocellular carcinoma patients. The analysis identified eleven variables with statistically significant differences between the massive and non-massive ascites groups: platelet count (PLT), AFP, albumin (ALB), aspartate aminotransferase (AST), alanine aminotransferase (ALT), portal hypertension, Cirrhosis of the Liver, Pringle Maneuver Time, Intraoperative Blood Transfusion Status, Intraoperative Blood Loss and operative time. These results indicate their potential association with the occurrence of postoperative massive ascites. Detailed results are provided in Table 2.
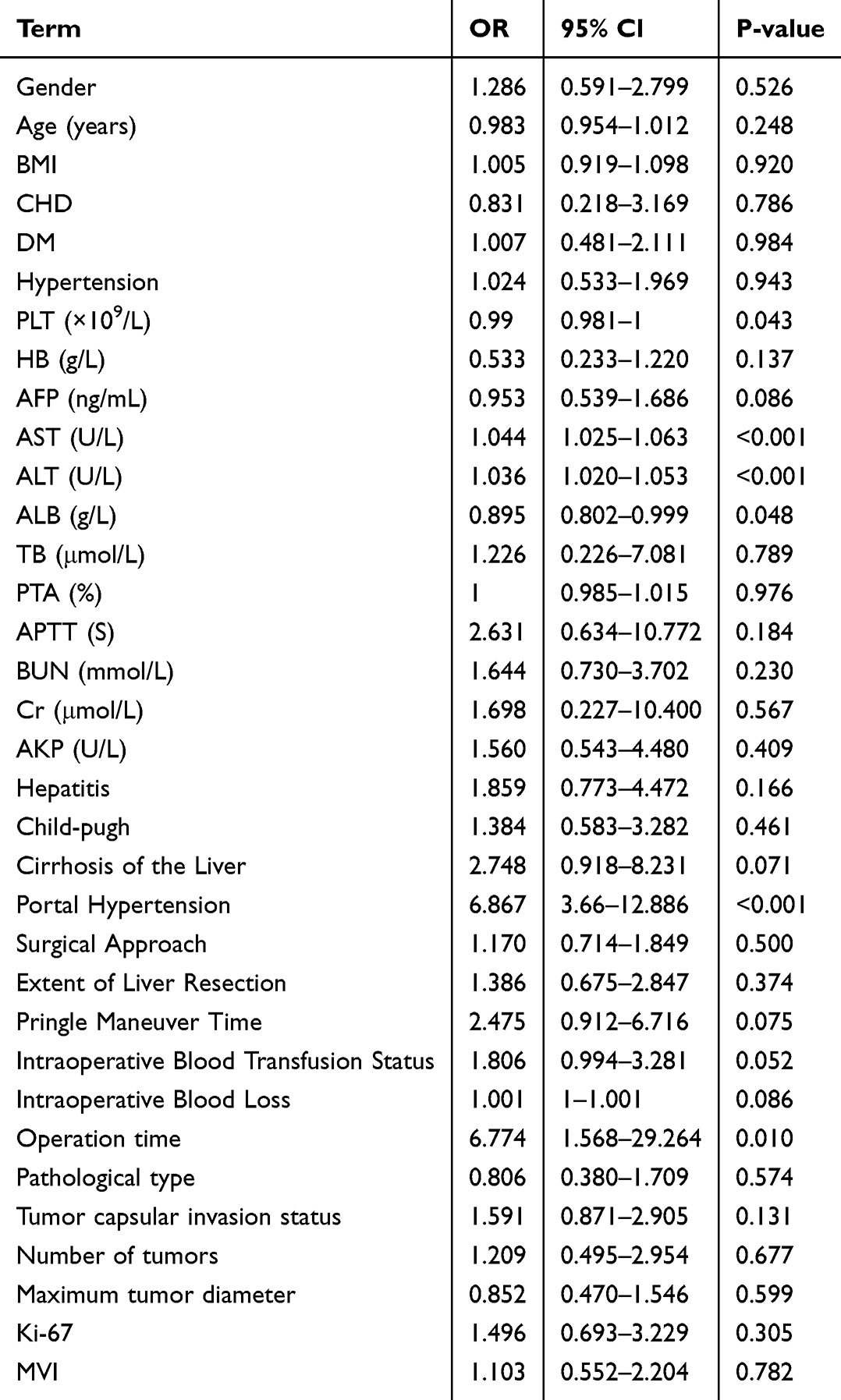 |
Table 2 Univariate Logistic Regression Analysis of Postoperative Massive Ascites |
Multivariate Analysis of Massive Ascites in Patients with HCC
Eleven variables in the univariate analysis were included in the multivariate binary logistic regression model. Multivariate analysis identified four independent risk factors for massive postoperative ascites: PLT (OR = 0.985, 95% CI: 0.973–0.996), AST (OR = 1.027, 95% CI: 1.001–1.054), portal hypertension (OR = 5.288, 95% CI: 2.535–11.033), and operative duration (OR = 5.011, 95% CI: 1.034–24.296). Detailed results are provided in Table 3.
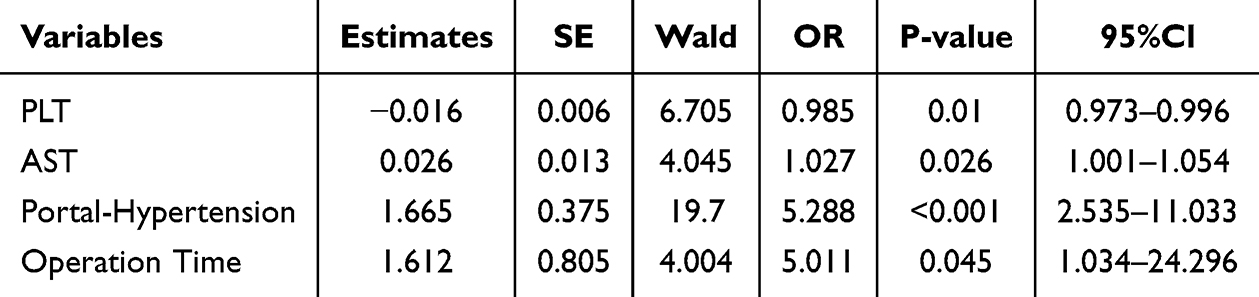 |
Table 3 Multivariate Logistic Regression Analysis of Postoperative Massive Ascites |
Establishment of the Nomogram Model for Predicting Postoperative Massive Ascites
Based on the independent predictors identified by multivariate logistic regression—PLT, AST, portal hypertension, and operative duration—we constructed a nomogram for predicting massive ascites (Figure 1).
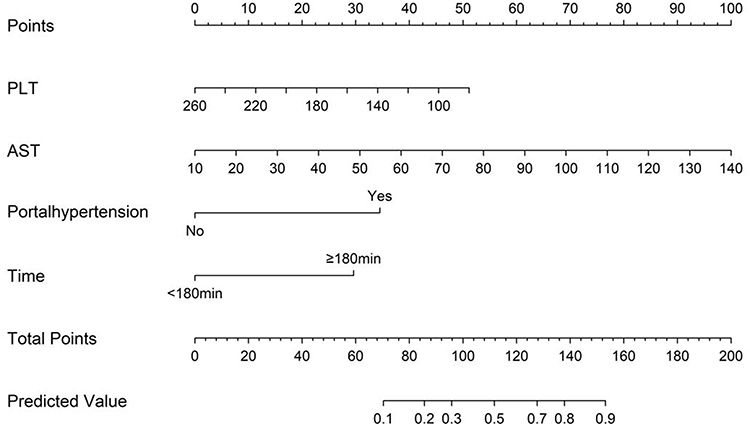 |
Figure 1 Nomogram for predicting massive ascites after hepatectomy. |
The predictive performance of the nomogram was evaluated using receiver operating characteristic (ROC) analysis. As shown in Figure 2, the model achieved an area under the curve (AUC) of 0.837 (95% CI: 0.781–0.892), indicating strong discriminative ability in stratifying the risk of postoperative massive ascites.
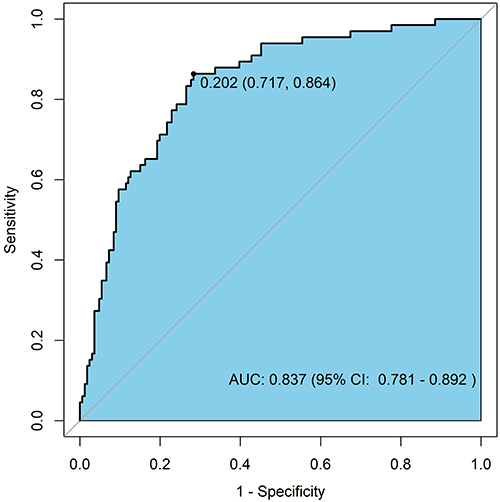 |
Figure 2 ROC curve of the nomogram for predicting postoperative massive ascites. |
The calibration of the nomogram was evaluated using a calibration curve (Figure 3) and the Hosmer–Lemeshow (HL) test. The HL test result (χ2 = 3.968, P = 0.860) indicated no significant deviation between predicted and observed outcomes, suggesting good model fit. Both the calibration plot and HL test confirmed that the nomogram is well-calibrated, with predicted probabilities closely aligning with actual event rates. This supports its reliability as a quantitative tool for individualized risk assessment of massive ascites.
 |
Figure 3 Calibration curve of the nomogram for predicting postoperative massive ascites. |
Decision curve analysis (DCA) was conducted to evaluate the clinical utility of the nomogram (Figure 4). The results indicated that the model provides a positive net benefit across a wide range of threshold probabilities, specifically from 0.00 to 0.71 and again from 0.86 to 0.93.
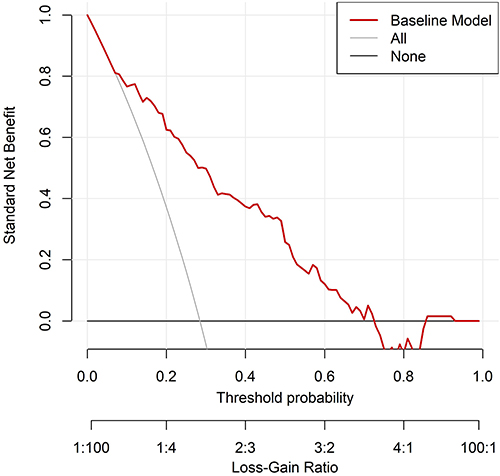 |
Figure 4 Decision curve analysis of the nomogram for postoperative massive ascites. |
The clinical impact curve (CIC) further supported these findings (Figure 5). At threshold probabilities above 0.4, the number of individuals classified as high-risk by the model closely aligned with the actual number of observed events, demonstrating high concordance between prediction and observation and confirming the model’s practical diagnostic value.
 |
Figure 5 Clinical impact curve of the nomogram for postoperative massive ascites. |
Discussion
The reported incidence of massive postoperative ascites varies considerably, ranging from 3.5% to 37% across studies,13–15 largely attributable to inconsistent diagnostic criteria. Some studies define it as a daily drainage volume exceeding 500 mL beyond the third postoperative day until drain removal,8,17 although this criterion does not account for variations in patient body weight. Ishizawa et al proposed an alternative definition based on a maximum daily drainage volume of >10 mL/kg of preoperative body weight.5,16 Nevertheless, daily drainage volumes can be influenced by multiple transient factors, such as tube patency, patient positioning, peritoneal lavage, and wound exudate. To improve reliability, our study defined massive ascites as either a maximum daily drainage volume >10 mL/kg of preoperative body weight or a cumulative drainage volume >1500 mL within the first postoperative week, thus integrating cumulative volume to mitigate the influence of transient or incidental factors. In this study, all patients received early postoperative oral intake and nutritional support, with no clinically significant changes in body weight. Therefore, admission body weight was uniformly used for ascites-related calculations. We analyzed preoperative, intraoperative, and postoperative variables from 232 patients who underwent hepatectomy for hepatocellular carcinoma. Multivariate analysis identified platelet count, aspartate aminotransferase level, portal hypertension, and operative time as independent risk factors for massive postoperative ascites. These factors were incorporated into a nomogram that demonstrated strong discriminative ability, with an area under the receiver operating characteristic curve (AUC) of 0.837. The nomogram also exhibited satisfactory calibration and clinical utility, supporting its use as a practical predictive tool.
The pathophysiology of postoperative ascites following hepatectomy in hepatocellular carcinoma (HCC) patients, though previously explored, remains incompletely understood. Impaired hepatic functional reserve is widely recognized as a pivotal contributor. Emerging evidence suggests that immune dysregulation, including the accumulation of myeloid‑derived suppressor cells (MDSCs), may also contribute to ascites formation and the immunosuppressive tumor microenvironment in HCC patients.19 In this study, the mean platelet count (PLT) was significantly lower in the massive ascites group than in the non-massive ascites group (121 × 109/L vs. 151 × 109/L). This difference may be partly explained by hypersplenism secondary to cirrhotic portal hypertension, a condition that also promotes ascites formation, which in turn may further accelerate platelet consumption.20 These observations align with our finding that portal hypertension constitutes an independent risk factor for postoperative ascites. Notably, platelet count remained significant in the multivariate regression, suggesting that thrombocytopenia alone cannot fully account for poor outcomes. Emerging evidence indicates that platelets may also facilitate HCC progression and liver fibrosis through the release of cytokines such as VEGF and TGF-β, thereby indirectly contributing to the pathophysiology of ascites.21
Furthermore, accumulating evidence has established preoperative thrombocytopenia as an independent predictor of postoperative complications and perioperative mortality in liver surgery, corroborating our findings.7,13,14,22–28 Aspartate aminotransferase (AST), a sensitive marker of hepatocellular injury, reflects the degree of hepatic inflammation and sinusoidal endothelial dysfunction. Elevated AST levels are associated with increased sinusoidal permeability, which facilitates the extravasation of albumin and fluid into the peritoneal space. This process may also promote intrahepatic fibrogenesis, thereby contributing to a self-sustaining cycle in ascites pathogenesis. Previous studies have consistently linked high preoperative AST levels with an increased risk of postoperative complications, including ascites,22 which aligns with our results. Preoperative portal hypertension not only exacerbates underlying hepatic dysfunction but also serves as a critical prognostic indicator of post-hepatectomy complications.8,29,30 Mechanistically, hepatectomy disrupts intrahepatic portosystemic shunts, leading to a sharp rise in sinusoidal and splanchnic vascular pressure, which in turn promotes fluid transudation. Additionally, portal hypertension stimulates hepatic lymph production beyond the drainage capacity of the thoracic duct, resulting in lymphatic leakage into the abdominal cavity31,32. It has also been suggested that this elevated venous pressure, combined with reduced colloid osmotic pressure due to impaired albumin synthesis, disrupts the Starling equilibrium, establishing a vicious cycle that perpetuates ascites accumulation.33 In line with these pathophysiological insights, the American Association for the Study of Liver Diseases guidelines recognize preoperative portal hypertension as a relative contraindication to hepatectomy, providing further support for our conclusions.34
Our findings suggest that the risk of massive postoperative ascites is not solely dependent on liver function parameters, but rather stems from the interplay of multiple determinants. Operative duration emerged as a significant risk factor in our analysis, consistent with previous reports.7,8 A large-scale national analysis of 21,443 hepatectomy cases demonstrated that procedures exceeding 3 hours may induce immunosuppression, tissue hypoperfusion, and infectious complications, thereby increasing postoperative morbidity and mortality.35
While some studies have reported associations between surgical approach and massive ascites incidence,36–38 we did not observe significant differences in this regard. Nevertheless, we speculate that as our institution’s experience with laparoscopic hepatectomy expands and surgical techniques continue to evolve, the physiological advantages of minimally invasive approaches—including preserved hepatic hemodynamics, reduced surgical trauma, and earlier recovery of oral intake—may become particularly beneficial for cirrhotic patients. These benefits could potentially translate into a substantial reduction in post-hepatectomy ascites risk with the accumulation of experience and technical refinement.
Based on our findings, preoperative thrombocytopenia, elevated aspartate aminotransferase (AST), prolonged operative time, and the presence of portal hypertension were identified as significant risk factors for massive postoperative ascites. Accordingly, we propose the following clinical recommendations. For patients with progressive preoperative thrombocytopenia, timely platelet transfusion should be considered to correct coagulation dysfunction. In cases of preoperative AST elevation or early signs of ascites, perioperative hepatoprotective therapy should be promptly initiated to facilitate AST normalization and prevent worsening of fluid accumulation. Intraoperatively, surgical efficiency should be optimized—through standardized hilar dissection and judicious inflow occlusion—and minimally invasive approaches should be prioritized when feasible to reduce operative duration. The strength of this study lies in the development of the first nomogram specifically designed to predict massive ascites following hepatectomy for hepatocellular carcinoma. We adopted a dual‑definition approach (maximum daily drainage volume >10 mL/kg or cumulative drainage >1500 mL within the first postoperative week), which improves reliability by mitigating transient or incidental factors. After internal validation using 1000 bootstrap samples, the model demonstrated acceptable predictive performance, with an AUC of 0.837 and a Hosmer‑Lemeshow test P value of 0.860. However, it should be regarded as a preliminary tool that requires external validation in larger, multicenter cohorts with standardized postoperative management before clinical application. Several limitations of this study should be acknowledged. Several limitations of this study should be acknowledged. First, its retrospective and single-center design introduces potential selection bias and unmeasured confounding, despite statistical adjustments. Second, the modest sample size (232 cases) limits the generalizability of the findings; external validation through multicenter prospective studies is warranted. Third, certain potential predictors of post-operative ascites—such as tumor diameter, indocyanine green retention rate at 15 minutes (ICG-R15), and liver stiffness measurement (LSM)—were not incorporated into the model. ICG-R15 and LSM were not routinely performed in all patients at our institution due to constraints including equipment availability, cost, and a lengthy procedural workflow, as well as the fact that many patients had small tumors amenable to local hepatectomy with minimal or no cirrhosis. Fourth, we did not systematically record or compare postoperative interventions such as diuretics and albumin administration between the two groups, which may have influenced the occurrence or severity of ascites and introduced confounding bias. Future prospective studies with standardized medication protocols and detailed documentation are needed to further validate our nomogram while controlling for these factors. Fifth, Excluding patients with postoperative bile leakage or hemorrhage may have introduced selection bias and could result in an underestimation of the overall incidence of massive ascites. Our findings should therefore be interpreted as applicable to patients without these complications; generalizability to those with bile leakage or hemorrhage remains to be determined. Finally, the lack of post-operative follow-up data precluded an assessment of the long-term prognostic impact of massive ascites on survival or recurrence.
Conclusion
In summary, massive ascites after hepatectomy for HCC results from a multifactorial interplay of perioperative variables. The proposed nomogram offers a preliminary approach to risk stratification that advances current knowledge by providing the first such tool using only routine clinical variables, though its clinical readiness requires confirmation through external validation in larger, prospective multicenter studies with standardized postoperative protocols.
Acknowledgments
We would like to thank Professors Wei Zhang and Lei Han for their guidance on the topic selection, revisions to the manuscript, and financial support for this paper. We also express our gratitude to all medical staff and patients who made contributions to this article. This work was supported by grants from the Independent Scientific Research Project of General Hospital of Northern Theater Command (ZZKY2024036), the Science and Technology Planning Project of Liaoning Province (2025-BS-0947), the Xingliao Talent Program (XLYC2412087) and the Shenyang Science and Technology Plan Project (24-214-3-25). This paper has been uploaded to ResearchSquare and europemc as a preprint:https://www.researchsquare.com/article/rs-8441964/v1-and,https://europepmc.org/article/ppr/ppr1153981.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was supported by the Independent Scientific Research Project of General Hospital of Northern Theater Command (ZZKY2024036), the Science and Technology Planning Project of Liaoning Province (2025-BS-0947), the Xingliao Talent Program (XLYC2412087), and the Shenyang Science and Technology Plan Project (24-214-3-25).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Bray F, Laversanne M, Sung H, et al. Global cancer statistics 2022: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2024;74:229–13. doi:10.3322/caac.21834
2. Zheng RS, Chen R, Han BF, et al. Cancer incidence and mortality in China, 2022. Chin J Oncol. 2024;46:221–231. doi:10.3760/cma.j.cn112152-20240119-00035
3. Younes M, Loubnane G, Sleiman C, Rizk S. Tocotrienol isoforms: the molecular mechanisms underlying their effects in cancer therapy and their implementation in clinical trials. J Integr Med. 2024;22:1–11. doi:10.1016/j.joim.2024.01.002
4. Sheta E, El-Kalla F, El-Gharib M, et al. Comparison of single-session transarterial chemoembolization combined with microwave ablation or radiofrequency ablation in the treatment of hepatocellular carcinoma: a randomized-controlled study. Eur J Gastroenterol Hepatol. 2016;28:1198–1203. doi:10.1080/08820139.2017.1407787
5. Torzilli G, Makuuchi M, Inoue K, et al. No-mortality liver resection for hepatocellular carcinoma in cirrhotic and noncirrhotic patients: is there a way? A prospective analysis of our approach. Arch Surg. 1999;134:984–992. doi:10.1001/archsurg.134.9.984
6. Taketomi A, Kitagawa D, Itoh S, et al. Trends in morbidity and mortality after hepatic resection for hepatocellular carcinoma: an institute’s experience with 625 patients. J Am Coll Surg. 2007;204:580–587. doi:10.1016/j.jamcollsurg.2007.01.035
7. Ishizawa T, Hasegawa K, Kokudo N, et al. Risk factors and management of ascites after liver resection to treat hepatocellular carcinoma. Arch Surg. 2009;144:46–51. doi:10.1001/archsurg.2008.511
8. Chan KM, Lee CF, Wu TJ, et al. Adverse outcomes in patients with postoperative ascites after liver resection for hepatocellular carcinoma. World J Surg. 2012;36:392–400. doi:10.1007/s00268-011-1367-1
9. Kudo M, Kitano M, Sakurai T, Nishida N. General rules for the clinical and pathological study of primary liver cancer, nationwide follow-up survey and clinical practice guidelines: the outstanding achievements of the liver cancer study group of Japan. Dig Dis. 2015;33:765–770. doi:10.1159/000439101
10. Okuda K, Ohtsuki T, Obata H, et al. Natural history of hepatocellular carcinoma and prognosis in relation to treatment. Study of 850 patients. Cancer. 1985;56:918–928. doi:10.1002/1097-0142(19850815)56:4
11. Tong C, Xu X, Liu C, Zhang T, Qu K. Assessment of liver volume variation to evaluate liver function. Front Med. 2012;6:421–427. doi:10.1007/s11684-012-0223-5
12. Ishii N, Harimoto N, Araki K, et al. Preoperative Mac-2 binding protein glycosylation isomer level predicts postoperative ascites in patients with hepatic resection for hepatocellular carcinoma. Hepatol Res. 2019;49:1398–1405. doi:10.1111/hepr.13412
13. Harimoto N, Araki K, Ishii N, et al. Predictors of postoperative ascites after hepatic resection in patients with hepatocellular carcinoma. Anticancer Res. 2020;40:4343–4349. doi:10.21873/anticanres.14437
14. Yoshikawa T, Nomi T, Hokuto D, et al. Risk factors for postoperative ascites in patients undergoing liver resection for hepatocellular carcinoma. World J Surg. 2017;41:2095–2100. doi:10.1007/s00268-017-4003-x
15. Zhou J, Sun H, Wang Z, et al. china liver cancer guidelines for the diagnosis and treatment of hepatocellular carcinoma (2024 Edition). Liver Cancer. 2024. doi:10.1159/000546574
16. Berardi G, Morise Z, Sposito C, et al. Development of a nomogram to predict outcome after liver resection for hepatocellular carcinoma in Child-Pugh B cirrhosis. J Hepatol. 2020;72:75–84. doi:10.1016/j.jhep.2019.08.032
17. Li JK, Huang HL, Zhu YH, et al. Research progress of imaging methods in the diagnosis of cirrhotic portal hypertension. Chin J Hepatol. 2021;29(12):1224–1228. doi:10.3760/cma.j.cn501113-20200116-00019
18. Belghiti J, Hiramatsu K, Benoist S, et al. Seven hundred forty-seven hepatectomies in the 1990s: an update to evaluate the actual risk of liver resection. J Am Coll Surg. 2000;191:38–46. doi:10.1016/s1072-7515(00)00261-1
19. Elwan N, Salem ML, Kobtan A, et al. High numbers of myeloid derived suppressor cells in peripheral blood and ascitic fluid of cirrhotic and HCC patients. Immunol Invest. 2018;47(2):169–180. doi:10.1080/08820139.2017.1407787
20. Aryal B, Yamakuchi M, Shimizu T, et al. Deciphering platelet kinetics in diagnostic and prognostic evaluation of hepatocellular carcinoma. Can J Gastroenterol Hepatol. 2018;2018:9142672. doi:10.1155/2018/9142672
21. Pavlovic N, Rani B, Gerwins P, Heindryckx F. Platelets as key factors in hepatocellular carcinoma. Cancers. 2019;11:1022. doi:10.3390/cancers11071022
22. Bennett JJ, Blumgart LH. Assessment of hepatic reserve prior to hepatic resection. J Hepatobiliary Pancreat Surg. 2005;12:10–15. doi:10.1007/s00534-004-0950-3
23. Kaneko K, Shirai Y, Wakai T, et al. Low preoperative platelet counts predict a high mortality after partial hepatectomy in patients with hepatocellular carcinoma. World J Gastroenterol. 2005;11:5888–5892. doi:10.3748/wjg.v11.i37.5888
24. Luo JC, Hwang SJ, Chang FY, et al. Simple blood tests can predict compensated liver cirrhosis in patients with chronic hepatitis C. Hepatogastroenterology. 2002;49:478–481.
25. Jarnagin WR, Gonen M, Fong Y, et al. Improvement in perioperative outcome after hepatic resection: analysis of 1803 consecutive cases over the past decade. Ann Surg. 2002;236:397–406. doi:10.1097/01.SLA.0000029003.66466.B3
26. Lu SN, Wang JH, Liu SL, et al. Thrombocytopenia as a surrogate for cirrhosis and a marker for the identification of patients at high-risk for hepatocellular carcinoma. Cancer. 2006;107:2212–2222. doi:10.1002/cncr.22242
27. Venkat R, Hannallah JR, Krouse RS, Maegawa FB. Preoperative thrombocytopenia and outcomes of hepatectomy for hepatocellular carcinoma. J Surg Res. 2016;201:498–505. doi:10.1016/j.jss.2015.08.038
28. Boleslawski E, Petrovai G, Truant S, et al. Hepatic venous pressure gradient in the assessment of portal hypertension before liver resection in patients with cirrhosis. Br J Surg. 2012;99:855–863. doi:10.1002/bjs.8753
29. Piano S, Tonon M, Angeli P. Management of ascites and hepatorenal syndrome. Hepatol Int. 2018;12(Suppl 1):122–134. doi:10.1007/s12072-017-9815-0
30. Rockey DC. Noninvasive assessment of liver fibrosis and portal hypertension with transient elastography. Gastroenterology. 2008;134:8–14. doi:10.1053/j.gastro.2007.11.053
31. Jeong J, Tanaka M, Iwakiri Y. Hepatic lymphatic vascular system in health and disease. J Hepatol. 2022;77:206–218. doi:10.1016/j.jhep.2022.01.025
32. Chung C, Iwakiri Y. The lymphatic vascular system in liver diseases: its role in ascites formation. Clin Mol Hepatol. 2013;19:99–104. doi:10.3350/cmh.2013.19.2.99
33. Kaplan DE, Ripoll C, Thiele M, et al. AASLD Practice Guidance on risk stratification and management of portal hypertension and varices in cirrhosis. Hepatology. 2024;79:1180–1211. doi:10.1097/HEP.0000000000000647
34. Singal AG, Llovet JM, Yarchoan M, et al. AASLD practice guidance on prevention, diagnosis, and treatment of hepatocellular carcinoma. Hepatology. 2023;78:1922–1965. doi:10.1097/HEP.0000000000000466
35. Chacon E, Eman P, Dugan A, et al. Effect of operative duration on infectious complications and mortality following hepatectomy. HPB. 2019;21:1727–1733. doi:10.1016/j.hpb.2019.05.001
36. El-Gendi A, El-Shafei M, El-Gendi S, Shawky A. Laparoscopic versus open hepatic resection for solitary hepatocellular carcinoma less than 5 cm in cirrhotic patients: a randomized controlled study. J Laparoendosc Adv Surg Tech A. 2018;28:302–310. doi:10.1089/lap.2017.0518
37. Belli G, Fantini C, D’Agostino A, et al. Laparoscopic versus open liver resection for hepatocellular carcinoma in patients with histologically proven cirrhosis: short- and middle-term results. Surg Endosc. 2007;21:2004–2011. doi:10.1007/s00464-007-9503-6
38. Kanazawa A, Tsukamoto T, Shimizu S, et al. Impact of laparoscopic liver resection for hepatocellular carcinoma with F4-liver cirrhosis. Surg Endosc. 2013;27:2592–2597. doi:10.1007/s00464-013-2795-9
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.