Back to Journals » Journal of Inflammation Research » Volume 19
Development and Validation of a Nomogram Based on Advanced Lung Cancer Inflammation Index for Predicting Overall Survival in Non-Surgical Esophageal Squamous Cell Carcinoma
Authors Liu C, Li H, Li H, Liu L, Liang J, Zhao Y, Shen S
Received 16 October 2025
Accepted for publication 11 February 2026
Published 23 February 2026 Volume 2026:19 572783
DOI https://doi.org/10.2147/JIR.S572783
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Subhasis Chattopadhyay
Changjiang Liu,1,* Huiqing Li,2,* Hua Li,3,* Lei Liu,1 Jia Liang,4 Yan Zhao,5 Supeng Shen4
1Department of Thoracic Surgery, The Fourth Hospital of Hebei Medical University, Shijiazhuang, Hebei, 050011, People’s Republic of China; 2Department of Oncology, People’s Hospital of Wei County, Handan, Hebei, 056899, People’s Republic of China; 3Second Department of Surgery, The Sixth People’s Hospital of Hengshui, Hengshui, Hebei, 053203, People’s Republic of China; 4Laboratory of Pathology, Hebei Cancer Institute, The Fourth Hospital of Hebei Medical University, Shijiazhuang, Hebei, 050011, People’s Republic of China; 5Department of Radiotherapy, The Fourth Hospital of Hebei Medical University, Shijiazhuang, Hebei, 050011, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Yan Zhao, Department of Radiation Oncology, The Fourth Hospital of Hebei Medical University, 12 Jiankang Road, Shijiazhuang, Hebei, 050011, People’s Republic of China, Email [email protected] Supeng Shen, Laboratory of Pathology, Hebei Cancer Institute, The Fourth Hospital of Hebei Medical University, 12 Jiankang Road, Shijiazhuang, Hebei, 050011, People’s Republic of China, Email [email protected]
Purpose: Despite advancements in multidisciplinary treatment strategies, long-term survival of esophageal squamous cell carcinoma (ESCC) patients remain suboptimal. Identifying novel prognostic biomarkers is essential for individualized treatment and surveillance approaches. The Advanced Lung Cancer Inflammation Index (ALI), an integrative biomarker reflecting nutritional, inflammatory, and immune status, has emerged as a potential predictor of prognosis. However, its association with overall survival (OS) in non-surgical ESCC patients remains poorly understood. This study aims to evaluate the prognostic value of ALI in ESCC patients undergoing radical radiotherapy and to develop a predictive nomogram to support clinical decision-making.
Patients and Methods: We retrospectively analyzed pre-radiotherapy ALI values of 266 ESCC patients treated from January 2017 to October 2022. A restricted cubic spline (RCS) model explored the link between continuous ALI levels and survival risk. Univariate and multivariate Cox proportional hazards models were used to identify independent predictors of OS, and a nomogram was constructed to predict 1 - year, 3 - year, and 5 - year OS probabilities.
Results: RCS analysis stratified patients into low (≤ 227.5), medium (227.5– 570.4), and high (> 570.4) ALI risk groups. Kaplan-Meier curves showed significant differences among the three groups, with lower ALI values associated with poorer prognosis (P = 0.0057). Multivariate analysis confirmed that ALI, radiation dose, T stage, and N stage were independent predictors of OS. A forest plot precisely quantified each variable’s prognostic contribution. The developed nomogram exhibited moderate to high predictive accuracy, as reflected by the area under the time-dependent ROC curves. Decision curve analysis (DCA) indicated a net clinical benefit at 1 - year, 3 - year, and 5 - year time points.
Conclusion: ALI is an independent prognostic factor for overall survival in non-surgical ESCC patients treated with radical radiotherapy. The ALI-based nomogram demonstrates good predictive performance and may serve as a useful tool for personalized risk stratification and clinical management.
Keywords: esophageal squamous cell carcinoma, (ESCC), prognosis, survival, advanced lung cancer inflammation index
Introduction
Esophageal cancer ranks eleventh in global cancer incidence and seventh in cancer-related mortality. In 2022, it accounted for 2.6% of all new cancer cases and 4.6% of cancer-related deaths worldwide.1 Approximately 90% of esophageal cancer cases in China are histologically classified as esophageal squamous cell carcinoma (ESCC).2 In the Chinese population, esophageal cancer is the sixth most commonly diagnosed malignancy and the fourth leading cause of cancer-related death, with a five-year survival rate ranging from 10% to 30% following diagnosis.1 Despite ongoing advancements in multidisciplinary comprehensive treatment strategies, long-term survival outcomes remain suboptimal. Furthermore, esophageal cancer therapies may lead to various complications that significantly impair patients’ quality of life.3 Therefore, identifying novel prognostic biomarkers is essential to enable more individualized treatment approaches and improved monitoring strategies for better clinical outcomes.
Accumulating evidence indicates that nutritional status, systemic inflammation, and immune function are closely linked to prognosis in various malignancies.4,5 Due to tumor-induced dysphagia, malnutrition is highly prevalent among esophageal cancer patients and may be further aggravated by treatment-related adverse effects such as nausea and vomiting. Studies have shown that malnutrition significantly influences the prognosis of patients with malignant tumors.4,6 Moreover, systemic inflammation plays a pivotal role in tumorigenesis and disease progression, profoundly affecting survival outcomes.7,8 Previous investigations have demonstrated that biomarkers including the neutrophil-to-lymphocyte ratio (NLR), Glasgow Prognostic Score (GPS), systemic immune-inflammation index (SII), and C-reactive protein-albumin-lymphocyte index (CALLY) are associated with clinical outcomes across multiple cancer types.9–11 Additionally, immune status has emerged as a critical predictor of therapeutic response and survival in oncology.12 The Advanced Lung Cancer Inflammation Index (ALI), a recently proposed biomarker, has been validated as a predictor of survival in non-small cell lung cancer.13 As a composite indicator integrating nutritional, inflammatory, and immune parameters, ALI provides a more comprehensive assessment. Subsequent studies have also revealed its prognostic value in other non-pulmonary malignancies, including gastrointestinal, hepatocellular and cervical cancers.14–16 Two retrospective studies have analyzed the relationship between ALI and survival in esophageal cancer patients, however, both included only those who underwent surgical treatment. The association between ALI and overall survival (OS) in non-surgical esophageal cancer patients remains uncertain and warrants further investigation. This study aims to evaluate the correlation between ALI and prognosis, develop and validate a nomogram model based on ALI for predicting overall survival, assess its prognostic utility, and provide insights for clinical decision-making in ESCC patients undergoing radical radiotherapy.
Materials and Methods
Study Population
This retrospective analysis included 266 patients with ESCC who received definitive radiotherapy between January 2017 and October 2022 at the Fourth Hospital of Hebei Medical University, Shijiazhuang, Hebei Province, China.Inclusion criteria were as follows: (I) age ≥18 years; (II) histologically or pathologically confirmed ESCC; (III) Eastern Cooperative Oncology Group performance status (ECOG PS) ≤1; (IV) no prior anti-tumor treatment; (V) clinical stage T2-T4 according to the 8th edition of the American Joint Committee on Cancer (AJCC) TNM staging system, with patients either deemed ineligible for surgery or having refused surgical intervention; (VI) receipt of intensity-modulated radiotherapy (IMRT) delivering a total dose of ≥50 Gy; (VII) chemotherapy regimen determined based on patient’s general condition, tumor characteristics, and personal preferences, including concurrent chemoradiotherapy or sequential chemotherapy following radiotherapy. Exclusion criteria were: (I) cervical esophageal cancer; (II) presence of distant organ metastases; (III) history of concurrent malignancies; (IV) incomplete clinical or follow-up data. Tumor staging was determined using barium esophagography, contrast-enhanced chest computed tomography (CT), electronic gastroscopy, endoscopic ultrasound, and/or positron emission tomography (PET), in accordance with the 8th edition of the AJCC TNM staging system. The research flow chart is shown in Figure 1. This study was conducted in compliance with the Declaration of Helsinki, adhered to the RECORD guidelines, and approved by the Ethics Committee of the Fourth Hospital of Hebei Medical University (Approval Number: 20240214). Written informed consent was obtained from all participants.
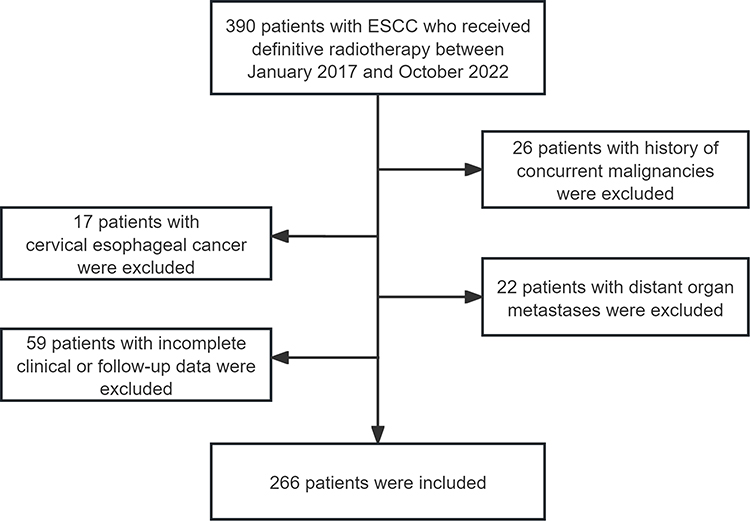 |
Figure 1 Flow chart of this study. |
Data Collection and Variables
Patient demographics and clinical characteristics collected included sex, age, body mass index (BMI), tumor location, T stage, N stage, TNM stage, radiation dose, receipt of chemotherapy, and pre-treatment peripheral blood parameters. The neutrophil-to-lymphocyte ratio (NLR) was calculated as neutrophil count divided by lymphocyte count. The ALI was defined as BMI multiplied by serum albumin level, divided by NLR.
Treatment
Patients were positioned and scanned using a CT simulator with a slice thickness of 3 mm. IMRT was delivered at a fraction dose of 1.8–2.0 Gy, five fractions per week, to a total dose of ≥50 Gy. Target volumes—including gross tumor volume (GTV), clinical target volume (CTV), and planning target volume (PTV)—were delineated using a treatment planning system (TPS) with 6-MV X-rays, incorporating information from CT simulation, barium esophagography, electronic gastroscopy, and/or PET. Dose constraints for organs at risk (OARs) adhered to established protocols: mean lung dose <13 Gy, V20 ≤30%, V30≤20%; mean heart dose ≤30 Gy, V30 ≤40%, V40 ≤30%; and maximum spinal cord dose <45 Gy. Chemotherapy was determined based on patient’s general condition, tumor characteristics, and personal preferences.Patients receiving chemotherapy were treated with either concurrent or sequential approaches. The chemotherapy drugs included paclitaxel, cisplatin, carboplatin, docetaxel, fluorouracil, S-1, capecitabine, and oxaliplatin. The most commonly used regimens were TP (paclitaxel 135–175 mg/m2 on day 1 plus cisplatin 75 mg/m2 on day 1) and PF (5-fluorouracil 750–1000 mg/m2 on days 1–4 plus cisplatin 75 mg/m2 on day 1), typically administered every three weeks when given concurrently.
Follow-Up
Follow-up evaluations were scheduled every 3 months during the first 2 years, every 6 months from years 3 to 5, and annually thereafter at our institution. Follow-up was conducted through outpatient clinic visits or telephone interviews, with a final follow-up cutoff date of April 2025. Overall survival (OS) was defined as the interval from the initiation of radiotherapy to the date of death from any cause or last follow-up, whichever occurred first.
Statistical Analysis
Intergroup comparisons were performed using chi-square tests or Fisher’s exact test, as appropriate. To evaluate the association between the continuous variable ALI and patient survival risk, a restricted cubic spline (RCS) model was applied. Based on the RCS analysis, patients were stratified into three risk groups according to ALI levels: low (≤227.5), medium (227.5–570.4), and high (>570.4). Kaplan-Meier survival curves and Log rank tests were used to compare time-to-event outcomes across groups. A nomogram was developed based on multivariate Cox proportional hazards regression to predict 1-, 3-, and 5-year overall survival probabilities. Forest plots derived from multivariate analysis were utilized to quantify the independent prognostic contributions of various factors. Model discrimination was evaluated using time-dependent receiver operating characteristic (ROC) curves. Decision curve analysis (DCA) was conducted to assess the clinical applicability and net benefit of the predictive model. A two-sided P-value <0.05 was considered statistically significant. All statistical analyses were carried out using R software (version 4.2.1).
Results
Patient Characteristics
This retrospective study included 266 patients with ESCC. Table 1 summarizes the association between ALI and baseline clinical characteristics. The median age was 66 years (range: 41–85 years). According to the AJCC 8th edition TNM staging system, 76 (28.6%), 115 (43.2%), and 75 (28.2%) patients were classified as stage T2, T3, and T4, respectively; while 63 (23.7%), 136 (51.1%), 54 (20.3%), and 13 (4.9%) were classified as stage N0, N1, N2, and N3, respectively. Chemotherapy was administered in 156 patients (58.6%), including 117 who received concurrent chemotherapy and 39 who received sequential chemotherapy. The median radiation dose was 6003 cGy (interquartile range [IQR]: 6000–6180 cGy). The median ALI value was 341.39 (IQR: 224.47–479.89).
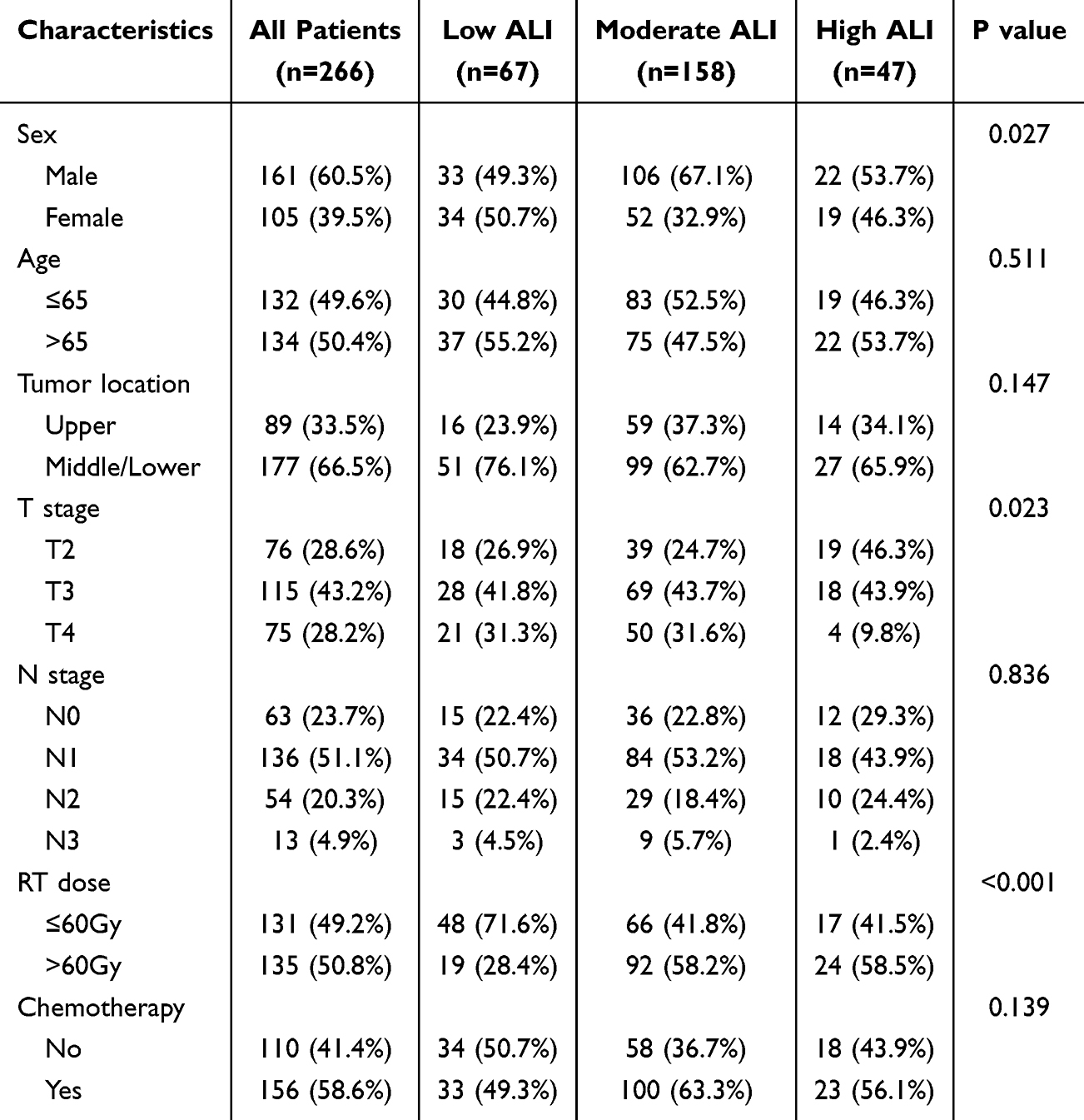 |
Table 1 Relationships Between ALI and Characteristics in ESCC Patients |
Association Between ALI and Overall Survival in ESCC Patients
The median follow-up time was 28.5 months (range, 2.2–86.6 months). Prior to categorical analysis, restricted cubic splines were used to examine the relationship between the continuous ALI variable and survival risk. The results indicated a nonlinear association between ALI and prognosis (Figure 2). Based on these findings, patients were categorized into three groups by ALI thresholds: low ALI (≤227.5), medium ALI (227.5–570.4), and high ALI (>570.4). The median OS for the entire cohort was 26.3 months (95% CI: 22.2–30.4), with 1-year, 3-year, and 5-year OS rates of 75.9%, 37.6%, and 28.3%, respectively. In the low ALI group, the median OS was 13.7 months (95% CI: 4.3–23.1), with 1-, 3-, and 5-year OS rates of 59.7%, 29.9%, and 23.9%, respectively. For the medium ALI group, median OS was 25.1 months (95% CI: 19.8–30.4), and 1-, 3-, and 5-year OS rates were 79.1%, 36.1%, and 27.9%, respectively. Patients in the high ALI group had a median OS of 41.6 months (95% CI: 26.5–56.6), with 1-, 3-, and 5-year OS rates of 90.2%, 55.9%, and 36.1%, respectively. Kaplan-Meier survival analysis revealed significant differences among the three groups, with lower ALI associated with poorer survival outcomes (Log rank test, P = 0.0057; Figure 3).
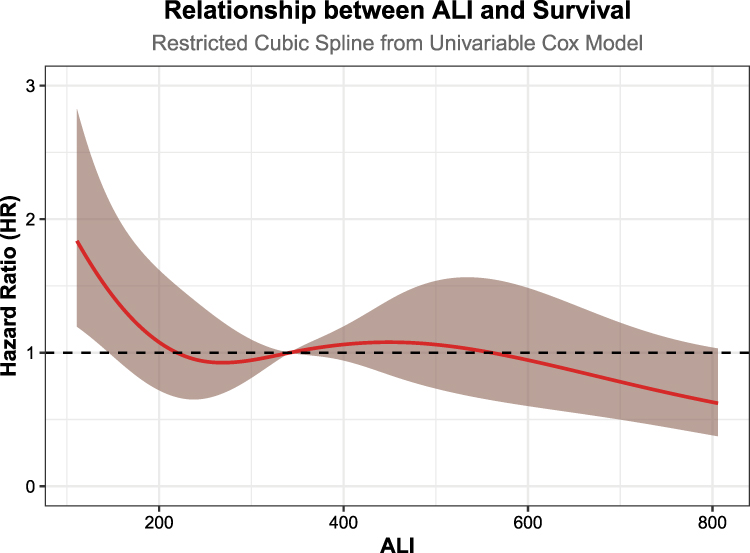 |
Figure 2 Restricted cubic spline (RCS) shows the relationship between ALI and overall survival in ESCC patients. |
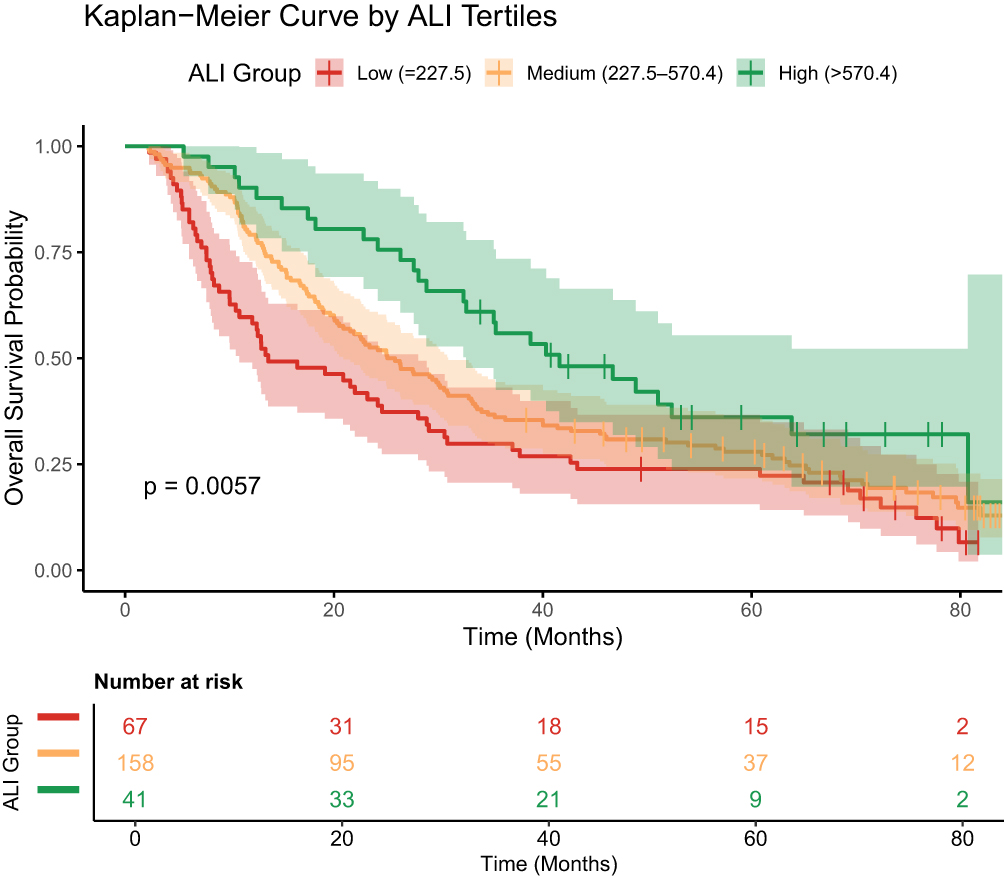 |
Figure 3 Kaplan-Meier curves of overall survival based on ALI in ESCC patients undergoing radical radiotherapy. |
Univariable and Multivariable Analyses
In our retrospective analysis, we conducted univariate and multivariate analyses to identify potential predictors of OS in patients with esophageal cancer. In the univariate analysis, ALI, radiation dose, T stage, and N stage were significantly associated with OS (Table 2). When these variables were included in the multivariate analysis, all remained independently and significantly associated with OS. The forest plot from the multivariate analysis illustrated the independent contribution of each factor to survival outcomes (Figure 4). Notably, advanced T stage (T3 vs T2: HR = 1.44; T4 vs T2: HR = 1.64) and N stage (N2 vs N0: HR = 2.00; N3 vs N0: HR = 3.66) were identified as significant risk factors for poorer survival. Importantly, continuous variable analysis demonstrated that higher radiotherapy dose (per 1 Gy increase: HR = 0.90, P = 0.002) and higher ALI value (per 100-unit increase: HR = 0.93, P = 0.044) were associated with improved OS. Although the hazard ratios were close to 1.0, the statistically significant P-values suggested that even small changes in these parameters may have clinically meaningful and sustained effects on prognosis.
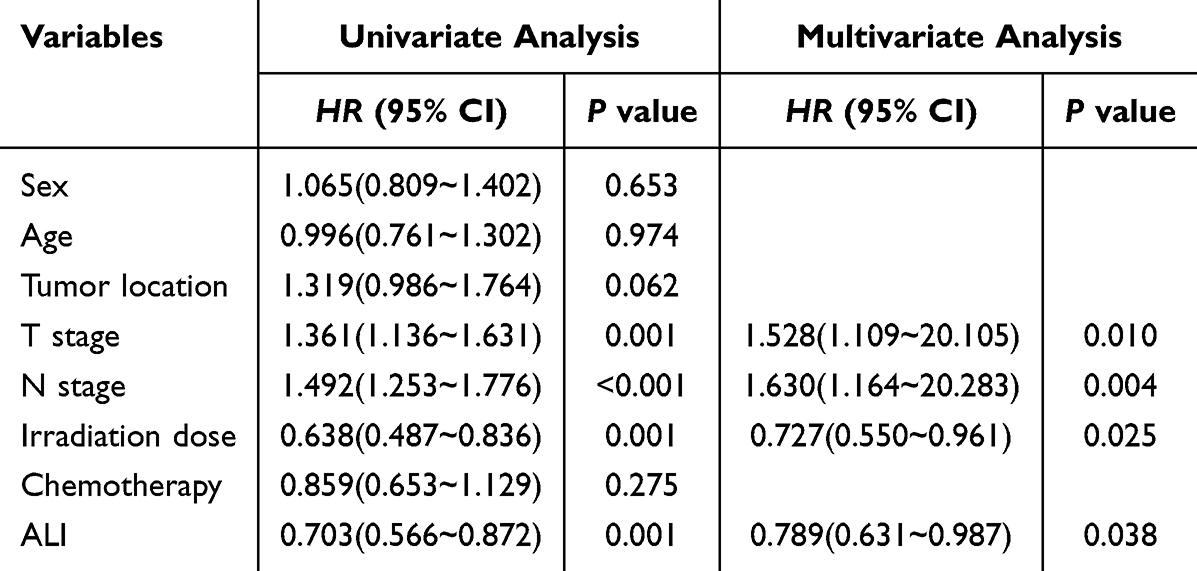 |
Table 2 Univariate and Multivariate Analyses of Prognostic Factors for OS in ESCC Patients |
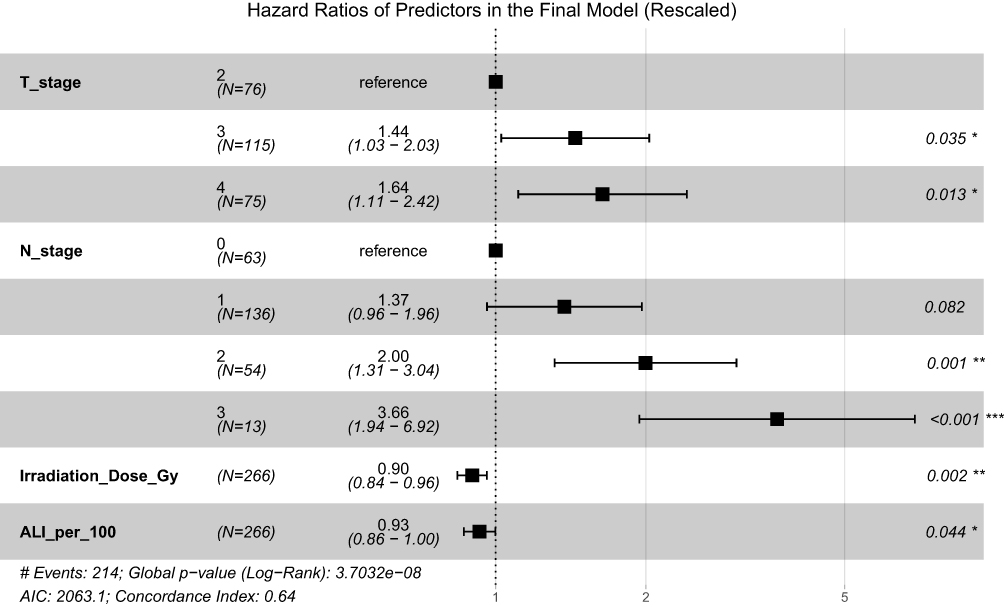 |
Figure 4 The forest plot from the multivariate analysis quantifying the independent contribution of each factor to survival outcomes. *p < 0.05; **p < 0.01; ***p < 0.001. |
Nomogram Model Based on ALI
To develop a quantitative tool for predicting prognosis in patients with esophageal cancer, we constructed a nomogram model. This prediction model, derived from multivariate Cox regression results and incorporating ALI, T stage, N stage, and radiation dose, was designed to estimate 1-year, 3-year, and 5-year OS probabilities. The nomogram assigns point scores based on ALI, radiation dose, T stage, and N stage, with higher total scores corresponding to worse survival outcomes (Figure 5).
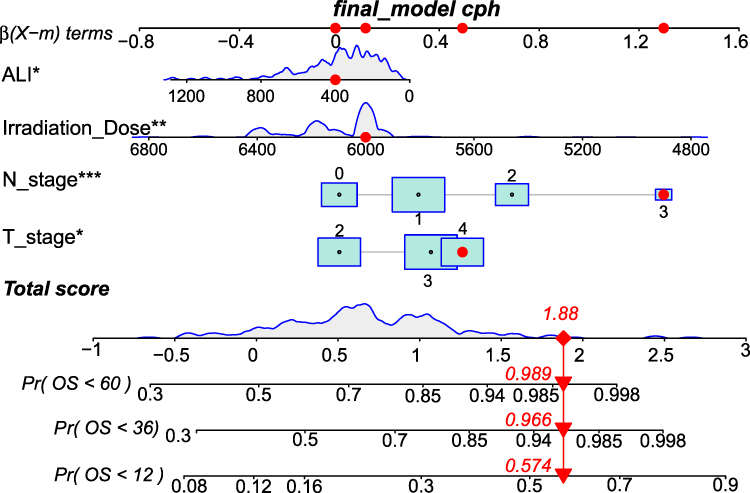 |
Figure 5 Prognostic nomogram based on ALI for predicting prognosis in patients with ESCC. *p < 0.05; **p < 0.01; ***p < 0.001. |
We evaluated the model’s discriminative performance using time-dependent receiver operating characteristic (ROC) curves. The results indicated moderate to high predictive accuracy, with area under the curve (AUC) values of 0.69, 0.71, and 0.67 for 1-year, 3-year, and 5-year mortality predictions, respectively (Figure 6). These findings confirm that the model maintains stable and effective discrimination between high- and low-risk patients across short-, medium-, and long-term follow-up periods. Furthermore, decision curve analysis (DCA) demonstrated favorable clinical utility. At 1-year, 3-year, and 5-year time points, the model showed a wide range of threshold probabilities (Figure 7), indicating that its use is likely to provide net clinical benefit across a broad spectrum of clinical decision-making scenarios.
 |
Figure 6 Time-dependent ROC curve for evaluating the the model’s discriminative performance. |
 |
Figure 7 Decision curve analysis (DCA) of the nomogram for the 1-year, 3-year and 5-year survival prediction of ESCC patients. |
Discussion
Despite ongoing advances in diagnostic techniques and therapeutic strategies, the prognosis of esophageal cancer remains suboptimal.17 Currently, patient stratification primarily relies on the TNM staging system, which guides treatment decisions. However, this system has inherent limitations, as it focuses exclusively on tumor-related characteristics and does not account for host-related factors—such as immune status, systemic inflammation, and nutritional condition—that may influence clinical outcomes. Even among patients with identical TNM stages, considerable heterogeneity in prognosis is observed.18 Therefore, there is a pressing need for more reliable biomarkers to improve prognostic stratification and enable more precise assessment of tumor behavior. Emerging evidence highlights the important roles of nutritional status, inflammatory responses, and immune function in cancer progression.19 The previous study by our research group analyzed the impact of different combination regimens of radiotherapy and chemotherapy on survival,20 while the present study analyzed survival prognostic factors from an alternative perspective perspective. In this cohort of patients with esophageal cancer undergoing definitive radiotherapy, those with lower ALI values exhibited significantly lower 1-year, 3-year, and 5-year OS rates compared to those with higher ALI values (p < 0.05).
ALI, a novel biomarker introduced in recent years, integrates nutritional status, inflammatory markers, and immune function. Lower ALI values are commonly associated with poorer nutritional status and/or more heightened systemic inflammation. It was initially established as an independent predictor of poor prognosis in advanced non-small cell lung cancer.13 Subsequent studies have consistently demonstrated its significant prognostic value across multiple malignancies.16,21–25 A large cohort study involving 10,137 elderly individuals revealed that ALI serves as a nutritional-inflammatory prognostic indicator, exhibiting a significant inverse correlation with colon cancer risk in older adults. These findings suggest that ALI may represent a promising non-invasive biomarker for risk stratification, particularly within high-risk subgroups such as unmarried women, drinkers, and those with low body mass index (BMI).22 Pang et al reported that postoperative low ALI levels in gastric cancer patients were an independent risk factor for reduced overall survival.23 Yu et al found that pretreatment ALI was an independent prognostic factor in cervical cancer patients undergoing radiotherapy, and a nomogram based on ALI may assist in identifying individuals at risk of adverse outcomes.16 Currently, evidence regarding the association between ALI and prognosis in esophageal cancer remains limited. Tan et al reported that both the L3 skeletal muscle index (L3SMI) and ALI were clinical indicators that could potentially be used to independently predict the prognosis of elderly esophageal cancer patients and demonstrated good predictive value.24 Another retrospective analysis indicated that modified ALI (mALI) was associated with the oncological prognosis of esophageal cancer patients undergoing radical resection and may function as a useful prognostic indicator.25 However, both studies exclusively included patients who underwent surgical intervention. To the best of our knowledge, there are no published reports on the relationship between ALI and survival outcomes in esophageal cancer patients receiving non-surgical treatment. In this study, restricted cubic spline (RCS) curve analysis revealed nonlinear associations between ALI and prognosis, rather than a simple linear relationship. This observation provided a methodological foundation for subsequent categorization of ALI using the tertiles approach, ensuring rational stratification. Kaplan-Meier and Cox regression analyses further confirmed the association between ALI and clinical outcomes in esophageal cancer patients, establishing ALI as an independent prognostic factor for overall survival. The results showed that 1-year, 3-year, and 5-year overall survival rates were significantly lower in patients with low ALI, which is consistent with findings from previous studies.
The TNM staging system is a widely accepted method for cancer prognosis prediction;26 however, considerable prognostic heterogeneity persists even among patients within the same stage. Nomogram-based prognostic models provide a valuable tool for individualized outcome prediction.27 In this study, based on multivariate Cox regression analysis, a nomogram incorporating ALI, radiation dose, T stage, and N stage was developed to predict 1-year, 3-year, and 5-year OS (OS) in patients with ESCC. The model’s predictive performance was validated using time-dependent receiver operating characteristic (ROC) curves, demonstrating moderate to high discriminative accuracy in distinguishing high-risk from low-risk patients. Furthermore, decision curve analysis (DCA) confirmed the clinical utility of the model, indicating a substantial net benefit across a range of clinically relevant threshold probabilities. By integrating ALI and other prognostic factors beyond conventional TNM staging, this nomogram enhances the precision of survival prediction in ESCC patients, enabling earlier identification of high-risk individuals earlier and facilitating tailored therapeutic strategies. To the best of our knowledge, this is the first prognostic nomogram to incorporate both ALI and tumor stage specifically for ESCC patients undergoing definitive radiotherapy, offering more refined survival prediction compared to TNM staging alone.
Concurrent chemoradiotherapy is the standard of care for patients with inoperable esophageal cancer. Current guidelines recommend identical radiation doses for both squamous cell carcinoma and adenocarcinoma, with a conventional total dose of 50.4 Gy. Nevertheless, local recurrence after definitive chemoradiotherapy remains high, occurring in 40–60% of cases.28 Despite numerous clinical trials evaluating the role of dose intensification in chemoradiotherapy, conclusive evidence remains lacking. Several studies, including the INT 0123 trial29 and the ARTDECO study,30 have shown no significant improvement in therapeutic outcomes with higher radiation doses. However, preclinical and theoretical evidence suggests that esophageal squamous cell carcinoma may be more radiosensitive than adenocarcinoma, potentially resulting in better responses to concurrent chemoradiotherapy.31 Some data indicate that dose escalation may improve survival specifically in patients with inoperable ESCC.32,33 This analysis identified higher radiation dose as a protective factor, associated with a significant reduction in death risk (HR = 0.90, P = 0.002). It is important to note, however, that this model reflects statistical associations rather than causal relationships. Clinically, higher-dose radiotherapy may be preferentially administered to younger, physically robust patients who tolerate chemoradiotherapy better and have a more favorable prognosis, which may confound the observed outcomes. From a therapeutic perspective, unrestricted dose escalation does not yield proportionally greater benefits. Beyond a certain threshold, improvements in local control plateau, while the risk of treatment-related toxicities increases substantially. Therefore, the optimal radiation dose for inoperable ESCC requires further investigation.
The findings of this study should be interpreted within the context of several limitations. First, the retrospective design and limited sample size may introduce selection and information bias. Second, all patients were enrolled from a single center and were of Chinese ethnicity. Given the known variations in esophageal cancer presentation across different ethnic and geographic populations, the generalizability of these results to other populations may be restricted. External validation in larger, multicenter cohorts with diverse demographic and clinical characteristics is warranted. Third, discrepancies in the definition of ALI thresholds across studies may partially limit the applicability of the findings. Furthermore, this study assessed only baseline values of BMI, albumin, neutrophil, and lymphocyte counts. Dynamic monitoring of these parameters may offer a more accurate assessment of the association between ALI and overall survival in patients with esophageal cancer.
Conclusion
ALI can serve as an independent prognostic indicator in patients with esophageal squamous cell carcinoma (ESCC) undergoing radical radiotherapy. The study revealed that, compared with patients with higher ALI values, those with lower ALI levels exhibited significantly lower 1-year, 3-year, and 5-year overall survival rates, indicating a poorer prognosis. To the best of our knowledge, this is the first prognostic nomogram incorporating ALI, T stage, N stage, and radiation dose specifically developed for ESCC patients treated with radical radiotherapy. This nomogram model provides more comprehensive clinical information than the conventional TNM staging system and may assist clinicians in making more precise and individualized treatment decisions. These findings require validation through future prospective studies.
Abbreviations
ESCC, esophageal squamous cell carcinoma; ALI, Advanced Lung Cancer Inflammation Index; OS, overall survival; RCS, restricted cubic spline; NLR, neutrophil-to-lymphocyte ratio; GPS, Glasgow Prognostic Score, SII, systemic immune-inflammation index; CALLY, C-reactive protein-albumin-lymphocyte index; ECOG PS, Eastern Cooperative Oncology Group performance status; IMRT, intensity-modulated radiotherapy; CT, computed tomography; PET, positron emission tomography; AJCC, American Joint Committee on Cancer; BMI, body mass index; GTV, gross tumor volume; CTV, clinical target volume; PTV, planning target volume; TPS, treatment planning system; OARs, organs at risk; ROC, receiver operating characteristic; DCA, Decision curve analysis; AUC, area under the curve; IQR, interquartile range; SIB, simultaneous integrated boost; HD-RT, high-dose radiotherapy; LD-RT, low-dose radiotherapy.
Data Sharing Statement
The datasets used and/or analyzed during the current study are available from the corresponding author upon reasonable request.
Acknowledgments
We are particularly grateful to all the people who have given us help on our article.
Author Contributions
All authors made a significant contribution to the work reported, with differing roles: CJL was primarily responsible for conceptualization, data curation, formal analysis, funding acquisition, resource management, software development, and writing (original draft, review, and editing). HQL and HL mainly contributed to data curation, formal analysis, investigation, resources, software, validation, visualization, and writing (original draft). LL and JL were primarily involved in investigation, resources, software, visualization, and writing (original draft). YZ and SPS led the conceptualization, data curation, funding acquisition, investigation, methodology, project administration, resources, supervision, validation, and writing (review and editing). All authors gave final approval of the version to be published, have agreed on the journal to which the article has been submitted, and agree to be accountable for all aspects of the work.
Funding
This study was supported by Hebei Natural Science Foundation (H2022206326) and Health Commission of Hebei Province (Grant No. 20230109).
Disclosure
All authors declare that they have no conflicts of interest in this work.
References
1. Bray F, Laversanne M, Sung H, et al. Global cancer statistics 2022: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2024;74(3):229–12. doi:10.3322/caac.21834
2. Morgan E, Soerjomataram I, Rumgay H, et al. The global landscape of esophageal squamous cell carcinoma and esophageal adenocarcinoma incidence and mortality in 2020 and projections to 2040: new estimates from globocan 2020. Gastroenterology. 2022;163(3):649–658.e2. doi:10.1053/j.gastro.2022.05.054
3. Sun L, Xu F, Xu X, Liu C. The correlation between common postoperative complications and quality of life, serum tumor markers, and prognosis in patients with esophageal cancer. Transl Cancer Res. 2022;11(1):217–226. doi:10.21037/tcr-21-2562
4. de Pinho NB, Martucci RB, Rodrigues VD, et al. High prevalence of malnutrition and nutrition impact symptoms in older patients with cancer: results of a Brazilian multicenter study. Cancer. 2020;126(1):156–164. doi:10.1002/cncr.32437
5. Kennel KB, Bozlar M, De Valk AF, Greten FR. Cancer-associated fibroblasts in inflammation and antitumor immunity. Clin Cancer Res. 2023;29(6):1009–1016. doi:10.1158/1078-0432.CCR-22-1031
6. Yin L, Chong F, Huo Z, Li N, Liu J, Xu H. GLIM-defined malnutrition and overall survival in cancer patients: a meta-analysis. J Parenter Enteral Nutr. 2023;47(2):207–219. doi:10.1002/jpen.2463
7. Winther-Larsen A, Aggerholm-Pedersen N, Sandfeld-Paulsen B. Inflammation-scores as prognostic markers of overall survival in lung cancer: a register-based study of 6,210 Danish lung cancer patients. BMC Cancer. 2022;22(1):63. doi:10.1186/s12885-021-09108-5
8. Moiseenko FV, Krasavina MA, Agranov IR, et al. Prognostic model integrating histology, systemic inflammation, and recurrence status predicts immunotherapy response in advanced non-small-cell lung cancer patients. Biol Direct. 2025;20(1):78. doi:10.1186/s13062-025-00674-3
9. Gu X, Han X, Shen Y, et al. Prognostic value of systemic inflammation response index in cancer patients treated with PD-1/PD-L1 immune checkpoint inhibitors: a meta-analysis. Ann Med. 2024;56(1):2413415. doi:10.1080/07853890.2024.2413415
10. Tian BW, Yang YF, Yang CC, et al. Systemic immune-inflammation index predicts prognosis of cancer immunotherapy: systemic review and meta-analysis. Immunotherapy. 2022;14(18):1481–1496. doi:10.2217/imt-2022-0133
11. Müller L, Hahn F, Mähringer-Kunz A, et al. Immunonutritive scoring for patients with hepatocellular carcinoma undergoing transarterial chemoembolization: evaluation of the CALLY index. Cancers. 2021;13(19):5018. doi:10.3390/cancers13195018
12. Bakkerus L, Subtil B, Bontkes HJ, et al. Exploring immune status in peripheral blood and tumor tissue in association with survival in patients with multi-organ metastatic colorectal cancer. Oncoimmunology. 2024;13(1):2361971. doi:10.1080/2162402X.2024.2361971
13. Jafri SH, Shi R, Mills G. Advance lung cancer inflammation index (ALI) at diagnosis is a prognostic marker in patients with metastatic non-small cell lung cancer (NSCLC): a retrospective review. BMC Cancer. 2013;13:158. doi:10.1186/1471-2407-13-158
14. Pang HY, Chen XF, Yan MH, et al. Clinical significance of the advanced lung cancer inflammation index in gastrointestinal cancer patients: a systematic review and meta-analysis. Front Oncol. 2023;13. doi:10.3389/fonc.2023.1021672
15. Yuan W, Zhao H, Wang S. Association between preoperative advanced lung cancer inflammation index and recurrence of hepatocellular carcinoma after curative resection. Adv Clin Exp Med. 2025;34(4):573–583. doi:10.17219/acem/188424
16. Yu Q, Sun Y, Zhang S, et al. Predictive value of advanced lung cancer inflammation index and development of a nomogram for prognosis in patients with cervical cancer treated with radiotherapy. J Inflamm Res. 2025;18:5371–5382. doi:10.2147/JIR.S501513
17. Then EO, Lopez M, Saleem S, et al. Esophageal cancer: an updated surveillance epidemiology and end results database analysis. World J Oncol. 2020;11(2):55–64. doi:10.14740/wjon1254
18. Reeh M, Nentwich MF, von Loga K, et al. An attempt at validation of the Seventh edition of the classification by the International Union Against Cancer for esophageal carcinoma. Ann Thorac Surg. 2012;93(3):890–896. doi:10.1016/j.athoracsur.2011.11.035
19. Pang H, Zhang W, Liang X, et al. Prognostic score system using preoperative inflammatory, nutritional and tumor markers to predict prognosis for gastric cancer: a two-center cohort study. Adv Ther. 2021;38(9):4917–4934. doi:10.1007/s12325-021-01870-z
20. Zhao Y, Li H, Li H, Zhang Z, Wen J, Li J. First-line induction or consolidation chemotherapy combined with concurrent chemoradiotherapy for esophageal squamous cell carcinoma. J Gastrointest Oncol. 2024;15(6):2389–2399. doi:10.21037/jgo-24-599
21. Li Q, Ma F, Tsilimigras DI, et al. The value of the Advanced Lung Cancer Inflammation Index (ALI) in assessing the prognosis of patients with hepatocellular carcinoma treated with camrelizumab: a retrospective cohort study. Ann Transl Med. 2022;10(22):1233. doi:10.21037/atm-22-5099
22. Zhong H, Chen Y, Wu W, et al. Advanced lung cancer inflammation index as a new predictor for colon cancer in elderly patients: an NHANES-based study. Front Nutr. 2025;12:1642913. doi:10.3389/fnut.2025.1642913
23. Pang H, Dai L, Chen L, et al. Prognostic value of the advanced lung cancer inflammation index in patients with gastric cancer after radical gastrectomy: a propensity-score matching cohort study and meta-analysis. BMC Cancer. 2024;24(1):583. doi:10.1186/s12885-024-12349-9
24. Tan X, Peng H, Gu P, Chen M, Wang Y. Prognostic significance of the L3 skeletal muscle index and advanced lung cancer inflammation index in elderly patients with esophageal cancer. Cancer Manag Res. 2021;13:3133–3143. doi:10.2147/CMAR.S304996
25. Yamamoto S, Aoyama T, Maezawa Y, et al. The usefulness of the modified advanced lung cancer inflammation index (Mali) as a prognostic factor in patients with esophageal cancer who have undergone curative resection. In Vivo. 2025;39(4):2176–2185. doi:10.21873/invivo.14013
26. Li J, Zhao Y, Li C, et al. The revision of 8th edition TNM stage criteria is more accurate in prediction postoperative survival for SCLC patients. Int J Surg. 2017;48:83–85. doi:10.1016/j.ijsu.2017.09.072
27. Gong J, Wang Q, Zhao L. A longitudinal CT-based subregional radiomics nomogram for predicting local recurrence-free survival in esophageal squamous cell carcinoma treated with definitive chemoradiotherapy: a multicenter study. Int J Radiat Oncol Biol Phys. 2025;123(1):e649. doi:10.1016/j.ijrobp.2025.06.2966
28. Pennathur A, Gibson MK, Jobe BA, et al. Oesophageal carcinoma. The Lancet. 2013;381(9864):400–412. doi:10.1016/S0140-6736(12)60643-6
29. Minsky BD, Pajak TF, Ginsberg RJ, et al. INT 0123 (Radiation Therapy Oncology Group 94-05) Phase III trial of combined-modality therapy for esophageal cancer: high-dose versus standard-dose radiation therapy. J Clin Oncol. 2002;20(5):1167–1174. doi:10.1200/JCO.2002.20.5.1167
30. Hulshof MCCM, Geijsen ED, Rozema T, et al. Randomized study on dose escalation in definitive chemoradiation for patients with locally advanced esophageal cancer (ARTDECO Study). J Clin Oncol. 2021;39(25):2816–2824. doi:10.1200/JCO.20.03697
31. Hu K, Wang W, Liu X, Meng Q, Zhang F. Comparison of treatment outcomes between squamous cell carcinoma and adenocarcinoma of cervix after definitive radiotherapy or concurrent chemoradiotherapy. Radiat Oncol. 2018;13(1):249. doi:10.1186/s13014-018-1197-5
32. Liou Y, Lan TL, Lan CC. A meta-analysis and review of radiation dose escalation in definitive radiation therapy between squamous cell carcinoma and adenocarcinoma of esophageal cancer. Cancers. 2024;16(3):658. doi:10.3390/cancers16030658
33. Shen PC, Chuang WK, Dai YH, et al. Identification of a suitable subgroup for radiation dose escalation in definitive concurrent chemoradiation therapy for nonmetastatic esophageal squamous cell carcinoma. JCO Precis Oncol. 2024;8:e2400555. doi:10.1200/PO-24-00555
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.