Back to Journals » Cancer Management and Research » Volume 12
Development and Validation of a Model for Predicting Urethral Recurrence in Male Patients with Muscular Invasive Bladder Cancer After Radical Cystectomy Combined with Urinary Diversion
Authors Liu Z, Zhang X, Wu B, Zhao Y, Bai S ![]()
Received 12 May 2020
Accepted for publication 2 August 2020
Published 24 August 2020 Volume 2020:12 Pages 7649—7657
DOI https://doi.org/10.2147/CMAR.S261809
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Xueqiong Zhu
Zeqi Liu,1 Xuanyu Zhang,1 Bin Wu,1 Yueyang Zhao,2 Song Bai1
1Department of Urology, Shengjing Hospital of China Medical University, Shenyang, Liaoning 110004, People’s Republic of China; 2Department of Library and Statistics, Shengjing Hospital of China Medical University, Shenyang 110004, People’s Republic of China
Correspondence: Song Bai Email [email protected]
Purpose: Radical cystectomy (RC) is the primary treatment strategy for patients with muscular invasive bladder cancer (MIBC). However, the prognosis is poor and tumor recurrence is not rare, in particular, urethral recurrence (UR) in male patients who underwent RC combined with urinary diversion. Here, we have developed and validated a model for predicting UR in these patients.
Patients and Methods: The development cohort comprised 310 patients who underwent RC combined with urinary diversion at our center between 1 January 2007 and 31 December 2015. Clinicopathologic data of patients were comprehensively recorded. Multivariate Cox proportional hazard regression was used for building a predictive model with regression coefficients and backward stepwise selection applied by utilizing the likelihood ratio test with Akaike’s information criterion as the stopping rule. An independent cohort consisting of 131 consecutive patients treated from 1 January 2016 to 31 December 2017 was used for validation. The performance of this predictive model was assessed with respect to discrimination, calibration, and clinical usefulness.
Results: The predictors of this model included body mass index, history of transurethral resection of bladder tumor, tumor grade, tumor stage, and concomitant carcinoma in situ. In the validation cohort, the model showed good discrimination with a concordance index of 0.777 (95% CI, 0.618 to 0.937) and calibration. Decision curve analysis also demonstrated the clinical utility of the model.
Conclusion: The predictive model facilitated postoperative individualized prediction of UR in male patients with MIBC after RC combined with urinary diversion and it may therefore serve to improve follow-up strategies.
Keywords: male, muscle invasive bladder cancer, radical cystectomy, urethral recurrence, predictive model
Introduction
Bladder cancer (BC) is the ninth most common cancer type worldwide, showing an increasing trend of incidence. About 430,000 people are diagnosed with bladder cancer every year, with a higher incidence in males than females. The worldwide age-standardised incidence rates for men and women are 9.0 and 2.2 per 100,000 person/years, respectively.1 The mortality rate of BC ranks 13th among cancer-related deaths on a global scale,2 with a BC age-standardised mortality rate of 3.2 per 100,000 person/years for men vs 0.9 for women in 2012.1
BC is classified into non-muscle invasive bladder cancer (NMIBC) and muscle invasive bladder cancer (MIBC) according to depth of tumor invasiveness. While the proportion of MIBC is lower than that of NMIBC, accounting for only 25% BC, the prognosis of MIBC is poorer than NMIBC. The 5-year survival rates have been determined as ~60% for pT2, 45% for pT3, and 16% for pT4 disease.3
Radical cystectomy (RC) combined with urinary diversion or orthotopic substitution are the main treatment strategies for patients with MIBC.3 Despite advancements in treatment strategies, patients continue to have a high risk of recurrence and metastasis. In previous studies, the incidence of urethral recurrence (UR) was 1.3–13.7% after RC and three times higher in male than female patients.4 In male patients where BC invades the urethra or who has positive urethral surgical margin, total urethrectomy usually be performed simultaneously.5 Nevertheless, risk of UR remains existent for the rest of BC patients. In addition, risk of UR is higher in patients subjected to urinary diversion than those with orthotopic substitutions.6 Therefore, UR should be paid more attention on these patients.
Individualized prediction of UR for patients with BC following RC could aid in guiding treatment strategies and follow-up schedules. To our knowledge, no studies to date have addressed in predicting this issue. The aim of this study was to develop and validate a predictive model of UR for male patients with MIBC after RC combined with urinary diversion.
Patients and Methods
Patients
The development cohort of this study consisted of 310 male patients who underwent radical RC combined with urinary diversion at our hospital between January 1, 2007 and December 31, 2015. The validation cohort comprised 131 consecutive male patients from January 1, 2016 to December 31, 2017, who met the same inclusion and exclusion criteria. A detailed cohort flow chart is presented in Figure 1A and B. This study has been reported in line with the STROCSS criteria.7
 |
Figure 1 Flow chart of the study. (A) Development cohort (B) Validation cohort. |
Inclusion and Exclusion Criteria
Diagnosis of urothelial muscular invasive bladder cancer was confirmed by pathological examination. Male patients who underwent open or laparoscopic radial cystectomy combined with extracorporeal cutaneous ureterostomy or ileal conduit, and pelvic lymphadenectomy were included; Urethral margin status at time of surgery are negative. Patients with urothelial carcinoma invading urethra were excluded in addition to those with BC combined with upper urinary tract urothelial carcinoma or history of upper urinary tract urothelial carcinoma were excluded either.
Clinicopathological Data
We collected the following data: demographics (age, body mass index [BMI]), clinical data (Charlson Comorbidity Index [CCI], history of smoking, history of transurethral resection of bladder tumor [TURB] due to non-muscle-invasive bladder cancer, neoadjuvant chemotherapy, adjuvant chemotherapy, tumor grade, tumor stage, carcinoma in situ [CIS] in RC specimens, tumor multifocality, lymph metastasis, bladder neck or prostatic involvement, and urinary diversion type [cutaneous ureterostomy versus ileal conduit]).
The definition of CCI was based on that of Charlson et al.8 History of smoking was defined as patients who smoked continuously or cumulatively for six months or more during their lifetime.9 Patients who received TURB due to nonmuscle invasive bladder cancer at least once in the past were classified as those with history of TURB. Tumor stage was categorized according to the International Union Against Cancer TNM classification system10 and tumor grade according to the 2004 World Health Organization (WHO) classification system.11 Tumor multifocality was defined as two or more pathologically confirmed tumors present synchronously in the bladder. Lymph node metastasis refers to pathological staging. Cutaneous ureterostomy (CU) is achieved by connecting detached ureters to the skin surface.12 The basic technique of ileal bladder surgery is to obtain free ileum, anastomose with ureters on both sides and subsequently perform abdominal wall skin stoma at the distal end through which urine is discharged out of the body.13
UR was established based on pathologic evidence after surgery. UR time was defined as time from surgery to the time of UR confirmation via pathology. Preoperative neoadjuvant and postoperative chemotherapy both constitute GC (gemcitabine and cisplatin) regimens. Patients received gemcitabine (1,000 mg/m2) on days 1, 8, and 15 to which cisplatin (70 mg/m2) was added on day 2. Cycles were repeated every 21 days.14 Patients receiving chemotherapy were defined as patients who underwent at least one cycle of chemotherapy.
Follow-up regimen: oncological evaluations were performed regularly once every 3 months for the first 2 years after surgery and once every 6 months for the next 2 years, including assessment of symptoms, physical examination, urethral wash cytology, computerized tomography (CT) urogram, bone scan, and imaging of the chest, abdomen, and pelvis.
Statistical Analysis
Data were analyzed using SPSS 22.0 for Windows (IBM, Armonk, NY, USA), STATA 16.0. (Stata Corp., College Station, TX, USA), and R software (version 3.0.1; http://www.Rproject.org). The packages in R used in this study were RMS and glmnet. The reported statistical significance levels were two-sided, with p<0.05 considered statistically significant. Normality of continuous variables was determined using the Shapiro–Wilks test. Normally distributed continuous variables were presented as means ± standard deviation (SD) and non-normally distributed continuous variables as the median (interquartile range). The Cox proportional hazard regression model was applied for univariate analysis.
Multivariate Cox proportional hazard regression analysis was used for building a predictive nomogram with regression coefficients. Backward stepwise selection was applied by using the likelihood ratio test with Akaike’s information criterion as the stopping rule.15,16 The performance of this model was tested in an independent validation cohort. The Cox regression formula applied in the development cohort was used for the validation cohort, and the probability for each patient at specific time-points was calculated. To quantify the discrimination performance of this model, Harrell’s concordance index (c-index) was measured. A c-index of 0.5 indicates no discrimination, whereas 1.0 indicates perfect discrimination. Calibration plots were used to assess the calibration of this model. Perfect calibration is depicted by a slope on the 45-degree line. Decision curve analysis was performed to determine the clinical usefulness of this model by quantifying net benefits at different threshold probabilities in the validation cohort.
Results
Based on strict inclusion and exclusion criteria, 310 patients were included in the development cohort and 131 in the validation cohort. Overall, UR was diagnosed in 30 patients (9.68%) in the development cohort and 17 (12.98%) in the validation cohort.
Based on univariate analysis of the development cohort, history of TURB, tumor stage, tumor grade, CIS in RC specimens, tumor multifocality, neoadjuvant chemotherapy, and adjuvant chemotherapy were significantly associated with UR (Table 1). The multivariate Cox proportional hazard regression model was used for building a predictive model with regression coefficients. Backward stepwise selection (p < 0.1) was applied by using the likelihood ratio test with Akaike’s information criterion as the stopping rule. Five predictors of UR were identified in the final model (BMI, history of TURB, tumor stage, tumor grade, and tumor multifocality). On the basis of these results, we developed a nomogram for predicting UR in male patients with MIBC after RC combined with urinary diversion was generated (Table 2; Figure 2).
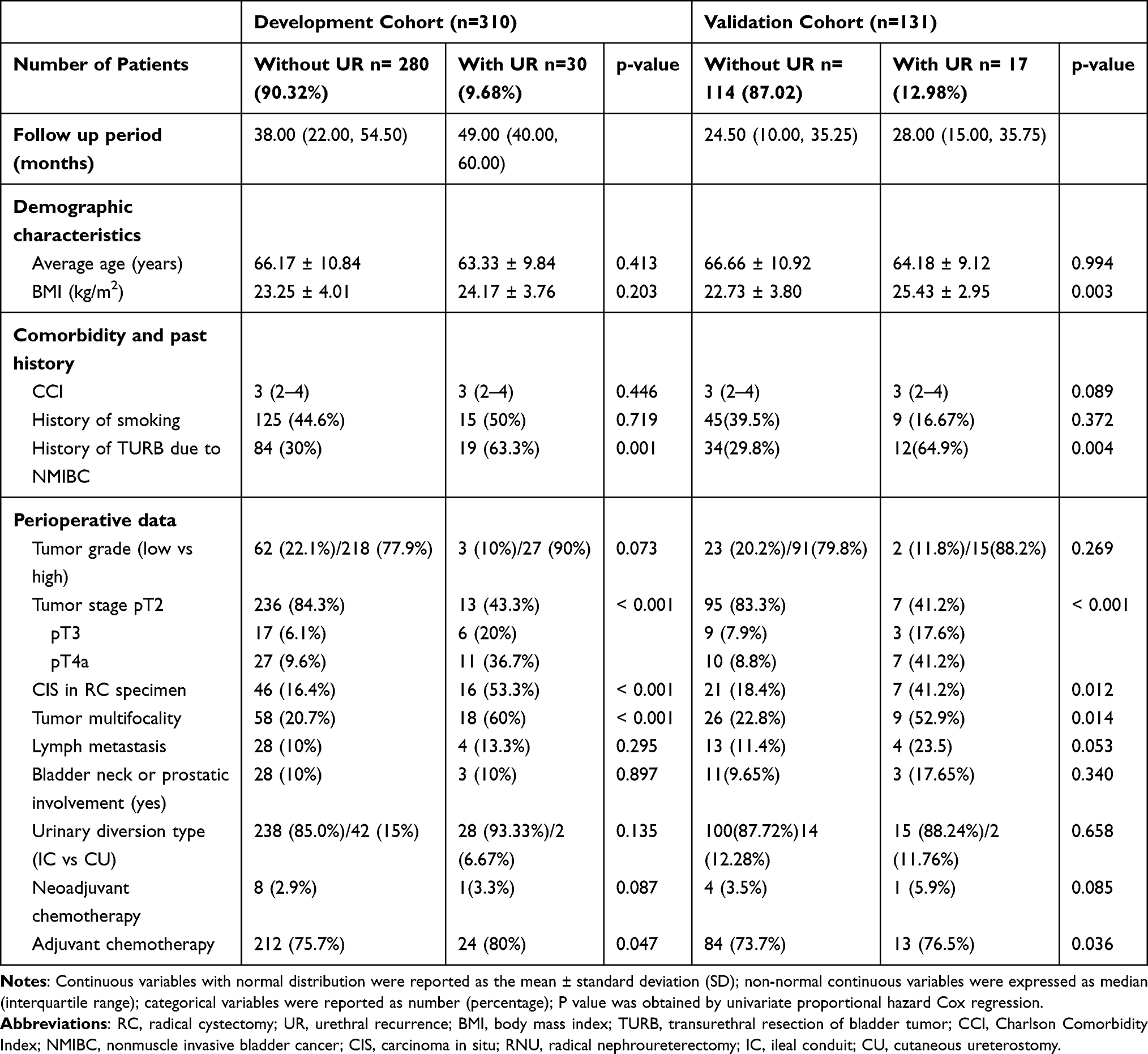 |
Table 1 Univariate Analysis of Patients in the Development and Validation Cohort |
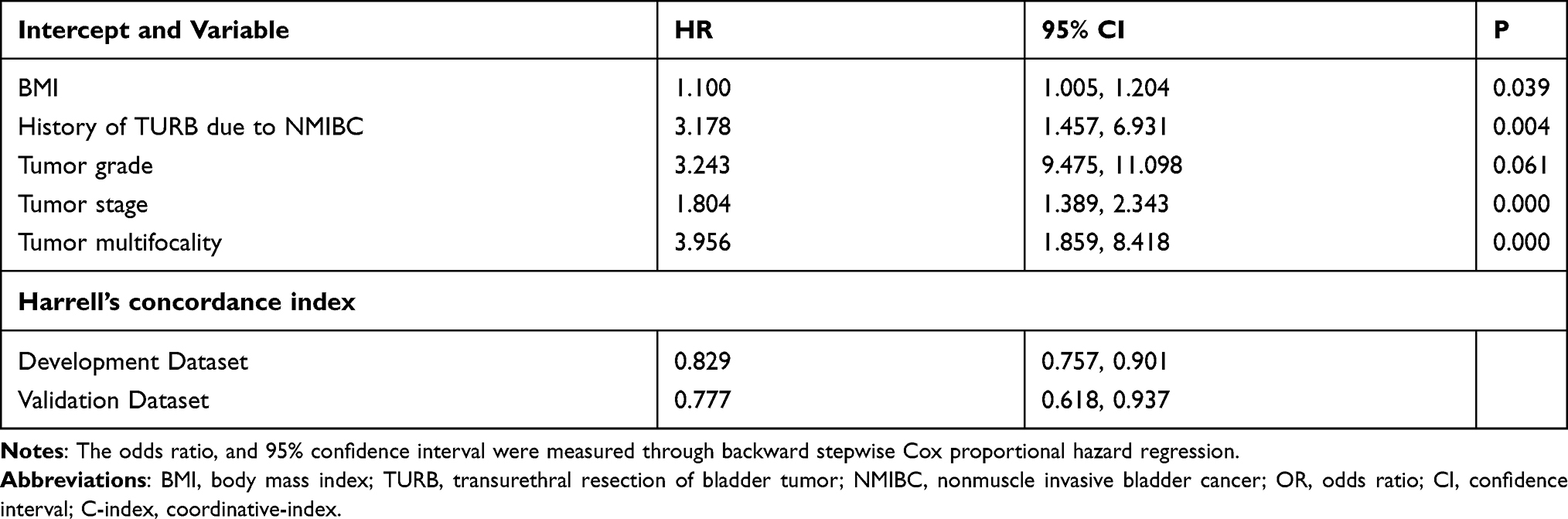 |
Table 2 Multivariate Cox Proportional Hazard Regression for UR |
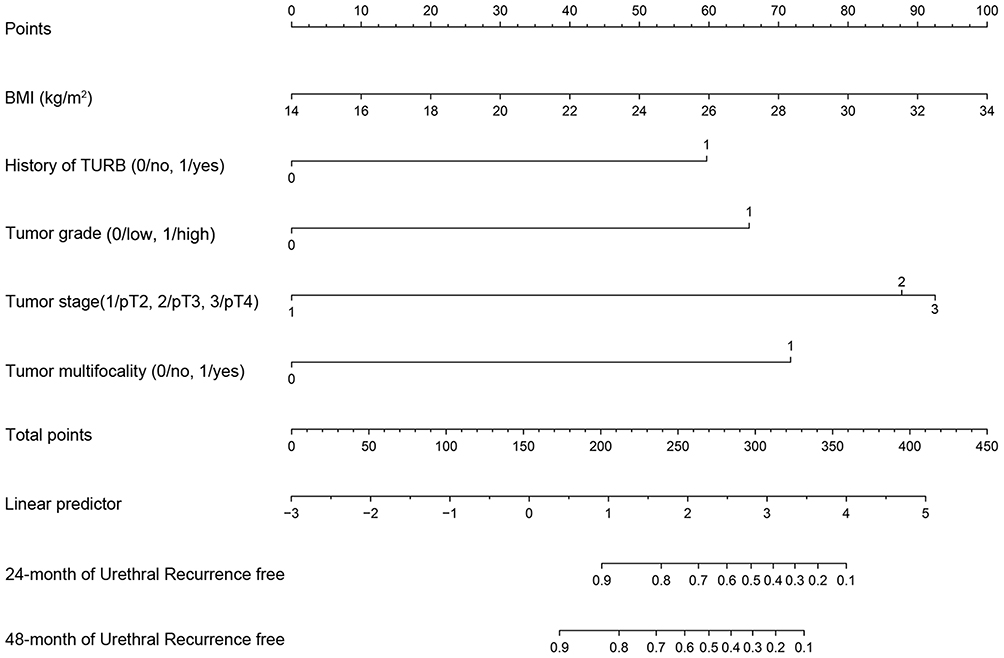 |
Figure 2 Nomogram of UR prediction in male MIBC patients after RC combined with urinary diversion. |
Each clinicopathologic feature corresponds to a specific point by drawing a line straight upward to the Points axis. The sum of the points located on the Total Points axis represents the probability of UR by drawing straight down to the risk axis. For example, considering a patient with the following features: BMI = 22 (40 points), T4 stage (93 points), history of TURB (60 points), tumor multifocality (72 points), and high-grade urothelium carcinoma (66 points), total points were 331, the probability of UR-free rate by month 24 was 25% and that by month 48 was 8% (details in Supplementary Figure 1). This calculated outcome could be used in decision making for follow-up or treatment guidance.
The discrimination efficiency of this model was qualified using the concordance index. The concordance index was determined as 0.829 (95% CI, 0.757 to 0.901) in the development cohort and 0.777 (95% CI, 0.618 to 0.937) in the validation cohort. Calibration plots revealed good calibration in the validation cohort (Figure 3A and B). In the decision curve analysis, the nomogram provided net benefits for the “treat all” or “treat none” strategy at a threshold probability of 5–45% at 24 months and 10–50% at 48 months, respectively. Within this range, net benefit was comparable (Figure 3C and D).
 |
Figure 3 Calibration and DCA in validation cohort. (A) Calibration at 24th month. (B) Calibration at 48th month. (C) DCA at 24th month. (D) DCA at 48th month. |
Discussion
Although RC is the main treatment strategy for patients with MIBC, prognosis remains poor, which carries serious psychological and living burdens. After RC, the incidence of UR is not rare, accounting for 1.3–13.7% of cases.4 UR mainly occurs within 24 months after RC,17,18 it highlighting the fact that UR is an important oncologic issue. In previous studies, the incidence of UR in males was reported to be higher than that in females (5.0% vs 1.4%).5 In addition, the UR rate in patients with urinary diversion was significantly higher than that in patients with OCD also.19,20 However, studies focusing on exploring the risk factors of UR in patients after RC are less and the conclusions are inconsistent. Furthermore, no study has investigated the prediction of UR in male patients with MIBC after RC combined with urinary diversion. Therefore, in this study, we developed and validated a model for predicting UR in male patients with MIBC after RC combined with urinary diversion.
In line with previous studies, the incidence of UR after RC was approximately 10% in this study. This model ultimately retained five predictors with good discrimination, calibration, and clinical net benefits, there were tumor stage, tumor grade, tumor multifocality, BMI, and history of TURB due to NMIBC.
This study identified tumor stage as a predictor of UR. In consistent with our findings, in a single center study on 287 patients, 11 had UR after RC, among which two patients had pT1, one had pT2, and eight had pT4 disease (p < 0.001). The results showed that higher tumor stage is an important risk factor of UR (P<0.001).20 Conversely, another study reported higher UR rate in low-stage than high-stage tumors.21 On the other hand, Kang Su Cho demonstrated that tumor stage is not an independent risk factor of UR.18 These discrepancies may be ascribed to that there are no pT1 stage patients and only male patient included in our study.
Tumor grade was additionally established as a predictor for UR. Patients with higher tumor grade have a higher incidence of UR than patients with a lower tumor grade. This may be because tumor cells are more prone to exfoliation in patients with a high tumor grade.22 However, in a retrospective review, including a total of 294 patients among whom 63 had low tumor and 230 had high tumor grades, tumor grade was not related to UR (p=0.635).18 These inconsistent findings may be due to the different inclusion criteria. For instance, we excluded patients with T1 tumor stage, distinct from the earlier study.
Another predictor of UR was tumor multifocality. According to previous reports, multifocality was a risk factor of UR.23,24 A study by Li et al21 disclosed significant differences between solitary and multifocal BC of UR (RR=2.93; 95% CI: [1.93,4.44]), the mechanism possibly is due to polycentric tumor growth. On the contrary, Stein and co-workers observed that the presence of tumor multifocality tended not to be associated with increased risk of UR (P = 0.06), however this finding was borderline statistically significant.6
An earlier population-based study showed that increasing BMI is a risk factor for BC.25 Moreover, overweight (BMI ≥ 24.9) was associated with shorter time to bladder tumor recurrence.26 However, no studies to date have shown an association between BMI and UR after RC. Our study indicated that BMI is a predictor of UR. At present, the biological mechanisms underlying obesity and tumor recurrence are unclear. Obesity is potentially related to inflammation of adipose tissue and stimulates the production and secretion of inflammatory molecules, which provide a microenvironment suitable for tumor growth.27
History of TURB due to NMIBC was another predictor of UR, possibly because tumor cells have a chance to implant and grow in the urethra during the process of TURB. However, no similar findings have been documented to date.
Combined CIS in RC specimens was not determined as a predictor of UR. In keeping with this finding, in a large-scale study involving 6,169 patients, HR of CIS for UR was 0.97 (p=0.88).4 However, in a large meta-analysis of 9,498 patients,21 BC patients with CIS showed a higher probability of developing UR than patients without CIS (RR = 3.09; 95% CI: [1.48, 6.47]), which may be attributed to the inclusion of female patients in this meta-analysis.
We further confirmed that lymph node metastasis is not a predictor of UR. In a meta-analysis of 9,498 patients, no significant differences in UR were observed between lymph node-positive and lymph node-negative cases (RR=0.57; 95% CI: [0.32, 1.02]).23 In general, positive lymph metastasis is an important predictor of prognosis, which is closely related with local and systemic recurrence. However, this may be less predictive for UR.28
Urinary diversion was not a predictor of UR. In our center, IC and CU were the main urinary diversion methods. Both of these two procedures are urinary diversion, and displayed no differences in UR predictive ability.
There was no model for predicting the urethral recurrence in male patients with bladder cancer after radical cystectomy. Simone et al found that age, pathologic tumor stage, lymph node density and extent of pelvic lymph node dissection were independent predictors of disease-free survival in patients with RC based on a predictive model with externally validation in multiple centers. The discrepancy might be due to different inclusion criteria and primary study endpoints.29
This study has a number of limitations that should be acknowledged. First, data were retrospectively collected from a single center. Second, the patients underwent OCD were excluded, so these patients were not suitable for this model. This study did not include patients with robotic assisted radical cystectomy (RARC), however, Simone et al found that disease-free survival (log-rank p= 0.746) was comparable between patients with RARC and open group in a cohort from a single-centre series using propensity score matched study.30 In addition, all the procedures of urinary diversion in this study were extracorporeal, however, Brassetti et al concluded that long-term oncologic outcomes after RARC with intracorporeal urinary diversion appeared similar to robotic series with extracorporeal diversion.31 Third, there was no either cytology examination before surgery or no urethral washing cytology examination in our routine follow-up schedule, which might be potential predictors of UR. Fourth, this study is temporal external validation, which tested a model from older data on newer data. Further multicenter prospective studies are warranted to validate this model. Nevertheless, this study was the first model for predicting UR for male patients with MIBC after RC combined with urinary diversion. It facilitated postoperative individualized prediction of UR and therefore serve to improve follow-up strategies.
Conclusion
The predictive model facilitated postoperative individualized prediction of UR in male patients with MIBC after RC combined with urinary diversion and it may therefore serve to improve follow-up strategies.
Ethics Statement
Ethical approval (Ethical Committee No. 2019PS032K) was provided by the Institutional Research and Ethics Committee of the Shengjing Hospital Affiliated China Medical University in Shenyang, China, on 21 February 2019. Informed consent from all participants was obtained. The clinical research registry UIN is CHiCTR1900022080. The study protocol conformed to the ethical guidelines of the Declaration of Helsinki. Research involving Human Participants and/or Animals:
The study involved Human Participants.
Acknowledgments
This study was financially supported (MC05) through the Shengjing Hospital Science and Technology Program. We give special thanks to all the teachers at the Department of Urology of Shengjing Hospital for their help and support.
Disclosure
The authors (Zeqi Liu, Xuanyu Zhang, Bin Wu, Yueyang Zhao, Song Bai) declare that they have no competing interests for this work. Song Bai certifies that all conflicts of interest, including specific financial interests, relationships and affiliations relevant to the subject matter or materials discussed in the manuscript (eg, employment/affiliation, grants or funding, consultancies, honoraria, stock ownership or options, expert testimony, royalties, or patents filed, received, or pending) are none. There was no role in this study of funding source.
References
1. Ferlay J, Soerjomataram I, Dikshit R, et al. Cancer incidence and mortality worldwide: sources, methods and major patterns in GLOBOCAN 2012. Int J Cancer. 2015;136(5):E359–E386. doi:10.1002/ijc.29210
2. Antoni S, Ferlay J, Soerjomataram I, Znaor A, Jemal A, Bray F. Bladder cancer incidence and mortality: a global overview and recent trends. Eur Urol. 2017;71:96–108. doi:10.1016/j.eururo.2016.06.010
3. Malkowicz SB, van Poppel H, Mickisch G, et al. Muscle-invasive urothelial carcinoma of the bladder. Urology. 2007;69:3–16. doi:10.1016/j.urology.2006.10.040
4. Fahmy O, Khairul-Asri MG, Schubert T, et al. Urethral recurrence after radical cystectomy for urothelial carcinoma: a systematic review and meta-analysis. Urol Oncol. 2018;36:54–59. doi:10.1016/j.urolonc.2017.11.007
5. Van Poppel H, Sorgeloose T. Radical cystectomy with or without urethrectomy? Crit Rev Oncol Hematol. 2003;47(2):141–145. doi:10.1016/S1040-8428(03)00077-5
6. Stein JP, Clark P, Miranda G, Cai J, Groshen S, Skinner DG. Urethral tumor recurrence following cystectomy and urinary diversion: clinical and patho- logical characteristics in 768 male patients. J Urol. 2005;173:1163–1168. doi:10.1097/01.ju.0000149679.56884.0f
7. Agha RA, Borrelli MR, Vella-Baldacchino M, Thavayogan R, Orgill DP. The STROCSS statement: strengthening the reporting of cohort studies in surgery. Int J Surg. 2017;46:198–202. doi:10.1016/j.ijsu.2017.08.586
8. Charlson ME, Pompei P, Ales KL, MacKenzie CR. A new method of classifying prognostic comorbidity in longitudinal studies: development and validation. J Chronic Dis. 1987;40:373–383. doi:10.1016/0021-9681(87)90171-8
9. Word Health Organization. Guidelines for controlling and monitoring the tobacco epidemic. Geneva: Tobacco or Health Programme, WHO; 1997.
10. TNM. classification of malignant tumor. In: Lh S, Gospodariowicz M, Wittekind C, editors. UICC International Union Against Cancer.
11. VEble JN, Sauter G, Epstein JI, et al. Pathology and Genetics of Tumours of the Urinary System and Male Genital Organs: World Health Organization Classification of Tumors. Lyon, France: IARC Press; 2004.
12. Furubayashi N, Negishi T, Kashiwagi E, Fukuda A, Nakamura M. Clinical outcome of transperitoneal ureterocutaneostomy using the transverse mesocolon. Mol Clin Oncol. 2013;1:721–725. doi:10.3892/mco.2013.117
13. Bricker EM. Bladder substitution after pelvic evisceration. Surg Clin North Am. 1950;30:1511–1521. doi:10.1016/S0039-6109(16)33147-4
14. von der Maase H, Hansen SW, Roberts JT, et al. Gemcitabine and cisplatin versus methotrexate, vinblastine, doxorubicin,and cisplatin in advanced or metastatic bladder cancer: results of a large, randomized, multinational, multicenter, phase III study. J Clin Oncol. 2000;18:3068–3077. doi:10.1200/JCO.2000.18.17.3068
15. Collins GS, Reitsma JB, Altman DG, Moons KG. Transparent reporting of a multivariable prediction model for individual prognosis or diagnosis (TRIPOD): the TRIPOD statement. BMJ. 2015;350:7594. doi:10.1136/bmj.g7594
16. Sauerbrei W, Boulesteix AL, Binder H. Stability investigations of multivariable regression models derived from low- and high-dimensional data. J Biopharm Stat. 2011;21:1206–1231. doi:10.1080/10543406.2011.629890
17. Chan Y, Fisher P, Tilki D, Evans CP. Urethral recurrence after cystectomy: current preventative measures, diagnosis and management. BJU Int. 2016;117:563–569. doi:10.1111/bju.13370
18. Cho KS, Seo JW, Park SJ, et al. The risk factor for urethral recurrence after radical cystectomy in patients with transitional cell carcinoma of the bladder. Urol Int. 2009;82:306. doi:10.1159/000209363
19. Djaladat H, Mitra AP, Miranda G, Skinner EC, Daneshmand S. Radical cystectomy and orthotopic urinary diversion in male patients with pT4a urothelial bladder carcinoma: oncological outcomes. Urol Int. 2013;20:1229. doi:10.1111/iju.12133
20. Balcı U, Dogantekin E, Özer K, Görgel SN, Girgin C, Dinçel Ç. Patterns, risks and outcomes of urethral recurrence after radical cystectomy for urothelial cancer; over 20 year single center experience. Int J Surg. 2015;13:148. doi:10.1016/j.ijsu.2014.12.006
21. Li X, Wang W, Zhu G, He W, Gou X. Risk factors, follow-up, and treatment of urethral recurrence following radical cystectomy and urinary diversion for bladder cancer: a meta-analysis of 9498 patients. Oncotarget. 2018;9:2782. doi:10.18632/oncotarget.23451
22. Yafi FA, Brimo F, Steinberg J, Aprikian AG, Tanguay S, Kassouf W. Prospective analysis of sensitivity and specificity of urinary cytology and other urinary biomarkers for bladder cancer. Urol Oncol. 2015;33:66–e25. doi:10.1016/j.urolonc.2014.06.008
23. Sherwood JB, Sagalowsky AI. The diagnosis and treatment of urethral recurrence after radical cystectomy. Urol Oncol. 2006;24:356. doi:10.1016/j.urolonc.2005.11.027
24. Chen ME, Pisters LL, Malpica A, Pettaway CA, Dinney CP. Risk of urethral, vaginal and cervical involvement in patients undergoing radical cystectomy for bladder cancer: results of a contemporary cystectomy series from MD Anderson Cancer Center. J Urol. 1997;157:2120–2123. doi:10.1016/S0022-5347(01)64691-3
25. Choi JB, Lee EJ, Han KD, Hong SH, Ha US. Estimating the impact of body mass index on bladder cancer risk: stratification by smoking status. Sci Rep. 2018;8:947. doi:10.1038/s41598-018-19531-7
26. Wyszynski A, Tanyos SA, Rees JR, et al. Body mass and smoking are modifiable risk factors for recurrent bladder cancer. Cancer. 2014;120:408. doi:10.1002/cncr.28394
27. Dirat BA, Bochet L, Escourrou G, Valet P, Muller C. Unraveling the obesity and breast cancer links: a role for cancer-associated adipocytes? Endocr Dev. 2010;19:45.
28. Dirat BA, Bochet L, Escourrou G, Valet P, Muller C. The relationship of local control to distant metastasis in muscle invasive bladder cancer. J Urol. 1995;154:2059–2063.
29. Simone G, Bianchi M, Giannarelli D, et al. Development and external validation of nomograms predicting disease-free and cancer-specific survival after radical cystectomy. World J Urol. 2015;33(10):1419–1428. doi:10.1007/s00345-014-1465-4
30. Simone G, Tuderti G, Misuraca L, et al. Perioperative and mid-term oncologic outcomes of robotic assisted radical cystectomy with totally intracorporeal neobladder: results of a propensity score matched comparison with open cohort from a single-centre series. Eur J Surg Oncol. 2018;44(9):1432–1438. doi:10.1016/j.ejso.2018.04.006
31. Brassetti A, Cacciamani G, Anceschi U, et al. Long-term oncologic outcomes of robot-assisted radical cystectomy (RARC) with totally intracorporeal urinary diversion (ICUD): a multi-center study. World J Urol. 2020;38(4):837–843. doi:10.1007/s00345-019-02842-3
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.