Back to Journals » Journal of Multidisciplinary Healthcare » Volume 19
Development and Usability Evaluation of a Serious Game for Dietary Health Education in Gestational Diabetes Mellitus: A Mixed-Methods Study Based on the SGDA Framework
Authors Xie C, Xu Y, Huang F, Shi S, Liu C, Xiao J ![]() , Cai S
, Cai S
Received 8 November 2025
Accepted for publication 30 January 2026
Published 16 February 2026 Volume 2026:19 580073
DOI https://doi.org/10.2147/JMDH.S580073
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Krzysztof Laudanski
Chunying Xie,1 Yiyi Xu,2 Fangying Huang,3 Siqi Shi,1 Chen Liu,1 Jingjing Xiao,2 Shu Cai1
1School of Nursing, Guangdong Pharmaceutical University, Guangzhou, Guangdong Province, 510310, People’s Republic of China; 2Guangdong Women and Children Hospital, Guangzhou, Guangdong Province, 511442, People’s Republic of China; 3Obstetrics Department, The Third Affiliated Hospital of Guangzhou Medical University (Huangpu Campus), Guangzhou, Guangdong Province, 510150, People’s Republic of China
Correspondence: Shu Cai, School of Nursing, Guangdong Pharmaceutical University, Guangzhou, Guangdong Province, 510310, People’s Republic of China, Email [email protected]
Purpose: To develop a serious game for dietary health education in gestational diabetes mellitus (GDM) and conduct its usability evaluation, so as to provide a new auxiliary tool for dietary health education among GDM patients.
Patients and Methods: Guided by the Serious Game Design Assessment (SGDA) framework, the script of the serious game was formulated by integrating evidence and literature, and the content of the script was revised through expert group meetings. After optimizing the game script, cooperation with software engineers was carried out to complete the development of the serious game. GDM patients from the obstetric outpatient department were selected as research subjects using the convenience sampling method, and usability evaluation was conducted by adopting the think-aloud method and the System Usability Scale (SUS) respectively.
Results: A mini-program of the serious game for GDM dietary health education was developed, with modules including Food Matching Elimination, Glycemic Index (GI) Classification Master, Meal Preparation Game, Gestational Sugar Control Gourmet, and Nutritious Plate Challenge. In the think-aloud test, the effectiveness of 3 GDM patients in completing the target tasks was (87.5%, 75.0%, 87.5%) respectively. Two themes regarding the game user experience were extracted: 1) the game content has practical value; 2) users can obtain an interesting emotional experience. The total SUS score of the serious game assessed by 30 GDM patients was (79.50± 4.17), indicating that the serious game has good usability.
Conclusion: The serious game for GDM dietary health education has practicality and interest. It can help patients learn GDM-related dietary knowledge and can be used as an auxiliary tool for GDM dietary health education.
Keywords: gestational diabetes mellitus, diet, health education, serious game, usability evaluation
Introduction
Gestational Diabetes Mellitus (GDM) is a metabolic disorder characterized by glucose intolerance that first occurs during pregnancy.1 It not only increases the risk of adverse pregnancy outcomes but also raises the long-term probability of both mother and infant developing metabolic diseases.2 Currently, the incidence of GDM is on the rise globally as well as in China, with the average incidence rate in China being approximately 14.8%.3 With the adjustment of fertility policies and the improvement of living conditions, the proportions of advanced-age pregnant women and obese pregnant women have been continuously increasing,4 further increase the difficulty of GDM prevention and control. Therefore, enhancing the self-management ability of pregnant women with GDM has become a key factor in improving maternal and infant outcomes.
However, clinical studies have shown that GDM patients face problems such as low awareness of dietary knowledge, imbalanced dietary structure, and insufficient self-management ability.5–7 Current GDM health education mainly includes one-on-one outpatient consultations and group classes for pregnant women,8 typically covering GDM knowledge instruction, personalized dietary advice, self-monitoring of blood glucose, and guidance on physical activity during pregnancy. In addition, models such as family-centered empowerment education9 and self-family-environment empowered dietary management10 emphasize empowerment as the core, mobilizing family members to participate jointly in blood glucose control actions. Although the aforementioned interventions have achieved certain results, shortcomings remain in promoting the transformation of knowledge into skills and in sustaining long-term self-management. These mainly include: outpatient health education and group classes often involve one-way knowledge transmission, placing patients in a passive reception state where their active participation and subjective initiative are difficult to fully mobilize; while family-centered interventions often lack continuous guidance, focus more on family supervision rather than collaborative learning, and fail to adequately stimulate patients’ internal motivation.
In view of this, as a digital tool centered on educational goals, serious games demonstrate unique advantages in facilitating knowledge acquisition and skill transfer through mechanisms such as immersive interaction and progressive challenges.11 Among these, immersive interaction typically employs scenario simulation, role-playing, and instant feedback systems to integrate theoretical knowledge into game task design, embodying and contextualizing the learning process, thereby strengthening knowledge retention and promoting its transformation into skills for solving practical problems.12 The progressive challenge mechanism, on the other hand, continuously matches and elevates users’ ability levels by dynamically adjusting game difficulty, setting appropriate task goals, and providing staged rewards.13 Furthermore, game mechanics leverage users’ intrinsic pursuit of a sense of achievement and challenge. Through designs such as point accumulation, level unlocking, and immediate feedback, it reinforce positive behaviors and aid in the long-term maintenance of healthy eating habits.14,15 Previous studies have indicated that serious games developed for specific groups focusing on dietary nutrition can enhance users’ knowledge of dietary nutrition, thereby promoting their healthy eating behaviors.16 However, to date, no study has followed a structured game design framework to systematically design and develop a GDM dietary health education game. Although digital interventions have been gradually applied in the field of GDM management in recent years, the functional designs of existing digital tools in current research mostly focus on basic modules such as dietary plan recommendations, blood glucose logging, and nutrition calculations, lacking sufficient interactivity and entertainment.17 Moreover, these digital tools lack systematic and in-depth usability evaluations of themselves. Additionally, existing research on GDM dietary games primarily involves card-based elimination games conducted offline by healthcare professionals organizing groups of GDM patients,18 which cannot meet the need for convenient use in digital scenarios.
Based on this, this study designed a serious game for dietary health education applicable to GDM patients based on the SGDA framework. A mixed-methods research approach (combining the think-aloud method and the System Usability Scale) was adopted to conduct a comprehensive and in-depth usability evaluation. The aim is not only to provide a scientifically designed tool but also, through rigorous usability testing, to offer an effective and feasible auxiliary tool for dietary education among GDM patients.
Methods
Design of the Serious Game Script
Formulation of the Serious Game Script
This study adopted a user-centered approach in developing the serious game. The functional modules of the game were designed based on the preliminary qualitative interview results regarding GDM patients’ perceptions and needs for a dietary health education game mini-program, derived from previous research.19 Purposive sampling was used in this preliminary study to select 15 GDM patients for semi-structured in-depth interviews. Content analysis was applied to analyze the data, and four core themes were extracted: channels for obtaining dietary education information, attitudes towards electronic games, expectations for game mini-programs, and challenges of gamified health education. These themes clarified patients’ core needs, such as game interactivity, personalized dietary information, and realistic scenarios, providing direct basis for the design of game modules and content optimization.
The content of GDM - related dietary knowledge in the serious game script was developed in accordance with the evidence summaries on dietary management of gestational diabetes mellitus,20,21 as well as the sections on nutrition management in Dietary Guidelines for Chinese Residents (2022),22 Dietary Reference Intakes for Chinese Residents (2023 Edition),23 Guidelines for the Diagnosis and Treatment of Hyperglycemia in Pregnancy (2022) [Part 1],24 and Knowledge Book on Pregnancy Complicated with Diabetes.25
In terms of the design of game modules, the study was guided by the Serious Game Design Assessment (SGDA) framework.26 This framework comprises six core elements, namely purpose, content, narrative, mechanics, structure, and aesthetics. It emphasizes a purpose - based game system, where the core objective acts as the key driving force for game design elements and runs through all components of the framework.27
With the aim of realizing health education on dietary self - management for GDM patients, this study designed the serious game under the SGDA framework. The game starts with concise and clear guiding remarks on the homepage to provide users with clear directional guidance. Subsequently, users can sequentially access the core modules of the game: Food Matching Elimination, Glycemic Index (GI) Classification Master, Meal Preparation Game, Gestational Sugar - Control Gourmet, and Nutritious Meal Plate Challenge. The game concludes after the user completes all level - clearing tasks.
Expert Panel Meeting
The expert meeting method was adopted in this study, with the core focus on the design of the functional modules and content of the serious game mini - program. Obstetric medical and nursing experts with extensive experience in gestational diabetes mellitus management were selected for the meeting. The criteria for expert selection were as follows: (1) Clinical medical experts engaged in obstetrics and GDM management, with at least 10 years of medical experience, a bachelor’s degree or above, and an associate senior professional title or higher. (2) Clinical nursing experts specialized in GDM and obstetrics, with no less than 10 years of clinical nursing experience, a bachelor’s degree or above, and a senior nurse practitioner title or higher.
The topics discussed at the expert panel meeting included three aspects: (1) Was the design of the content in the serious game script scientific and appropriate? (2) What aspects of the game script needed to be revised, added, deleted, or paid special attention to? (3) What additional suggestions could be put forward for the design of the game script? Eventually, a total of 10 experts were invited to participate in this study, including associate chief physicians of obstetrics, associate chief physicians of clinical nutrition, diabetes specialist nurses, staff nurses, and software engineers. The average age of the experts was (37.40±6.08) years old, and their average working experience was (13.10±4.20) years. The individual authority coefficients of the experts in this panel meeting ranged from 0.70 to 0.93, with an overall authority coefficient of 0.80.
Based on the revision opinions put forward at the expert panel meeting, this study summarized the content requiring modification. The specific revisions were as follows: (1) Adjust the level structure of “Glycemic Index (GI) Classification Master” to include 2 levels, and strengthen the training of GI matching games focusing on fruits and grain - tuber products. (2) Add a “Dietary Nutrition Guidance” section to provide comprehensive and popular science - oriented articles on dietary knowledge. (3) Incorporate the “palm - size portion guide” for rapid food portion estimation into the “Nutritious Meal Plate Challenge”, so as to help players learn how to quickly assess the required food intake when dining out. (4) Add specialty dishes from different regions, allowing users to independently choose and combine ingredients according to their dietary preferences; incorporate ingredients of the same type of food from various regions into both the “restaurant ordering” session and the nutrition plans. (5) Enhance the design of GDM dietary education objectives: add progressive difficulty levels for level - clearing in the simulated “supermarket shopping”, “restaurant ordering” and “kitchen cooking” sessions; in the “Meal Preparation Game” session, add personalized nutrition guidance plans targeting different individuals, such as those with excessive weight gain or insufficient weight gain, when evaluating users’ dietary plans. (6) Remove the “Meat and Egg Matching Elimination” level and add a staple food classification and matching module instead. (7) Refine the game feedback prompts in the “kitchen cooking” session, which were revised to detailed feedback on the impacts of different cooking methods on the glycemic index of food. The information architecture of the revised serious game for GDM dietary health education is shown in Figure 1.
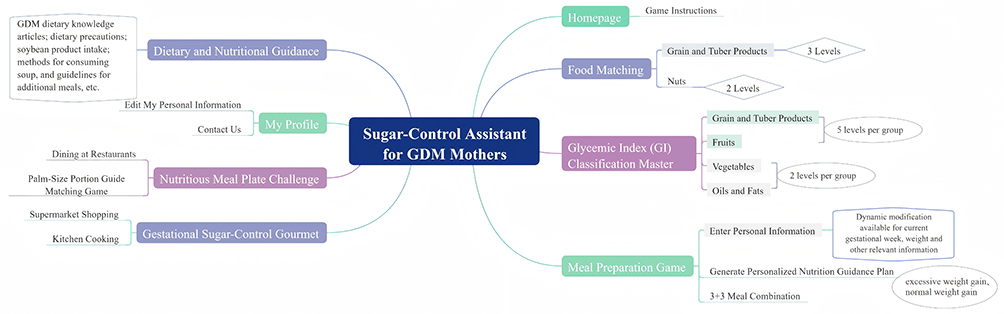 |
Figure 1 Information Architecture of the Serious Game for GDM Dietary Health Education. |
Development of the Serious Game
Development Process
Based on the revised script of the serious game for GDM dietary health education finalized at the expert panel meeting, a game development agreement was signed with a game developer to complete the production of the serious game. The researchers defined the intended functions and effects of the serious game, downloaded and categorized the food image library required for the game, formulated the game content and UI design, and compiled the game feedback prompts and game logic, which were then submitted to the software engineers. Multiple rounds of communication and confirmation were conducted with the software engineers during the process. Throughout the development phase, the researchers took charge of compiling the requirements document and game logic, while the technical team put forward professional optimization suggestions from the perspective of engineering implementation. Through repeated two - way communication and debugging, the technical feasibility and functional completeness of the requirements document were ensured. This serious game was developed as a WeChat Mini Program, which is compatible with both iOS and Android operating systems.
Design of the Dietary Game Module
Partial screenshots of the content of this module are shown in Figure 2.
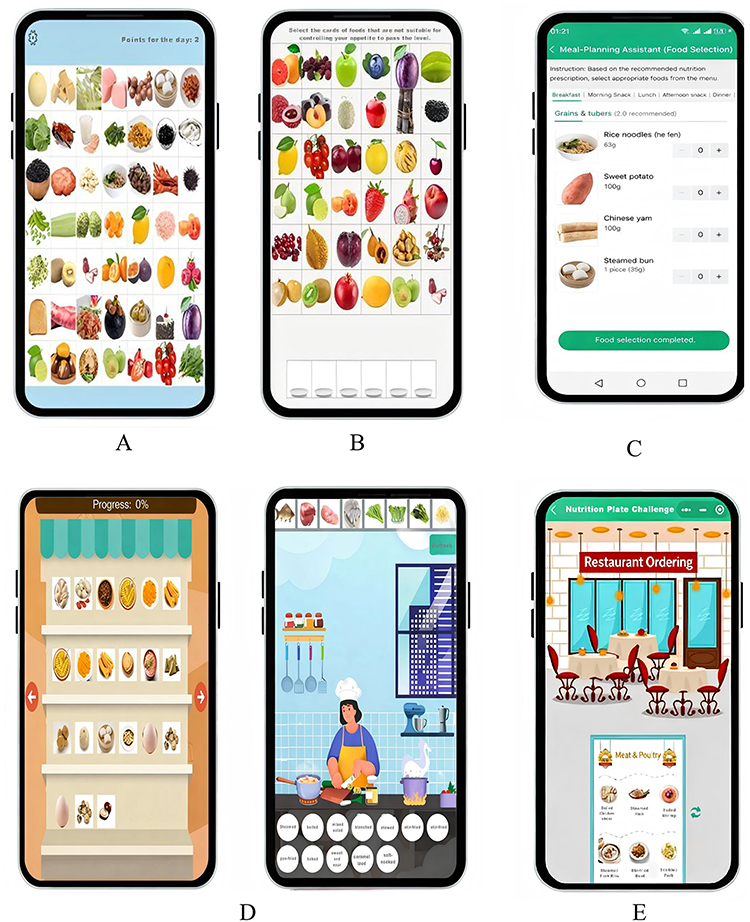 |
Figure 2 Dietary Game Module Design of the GDM Dietary Health Education Serious Game. Notes: (A) Food Matching Elimination. (B) Glycemic Index (GI) Classification Master. (C) Meal Preparation Game. (D) Gestational Sugar-Control Gourmet and Kitchen Cooking. (E) Nutritious Meal Plate Challenge. |
Food Matching Elimination Module
In accordance with the group standard Food Exchange Servings (T/CNSS 020—2023) issued by the Chinese Nutrition Society,28 foods are categorized into grain - tuber and miscellaneous bean products, vegetables, fruits, meat, eggs and aquatic products, nuts, soybean milk and its products, oils and seasonings.
Players are required to select foods of the same category from mixed food images. When three foods of the same category are selected and correctly classified, they will be eliminated, and new images will be automatically supplemented. Players can gain 2 points for each correct selection in each round. This module integrates education with entertainment; the difficulty of levels increases progressively, and the variety of foods becomes more abundant as the game proceeds.
Glycemic Index (GI) Classification Master Module
Users need to select foods with different glycemic indices that meet the requirements in the game. New foods are unlocked based on the player’s level - clearing progress. The content of each level is distinct, and the difficulty escalates gradually.
The initial level provides common low - GI foods such as oatmeal and high - GI foods like pancakes. After clearing this level, complex foods with glycemic indices that are harder to judge—such as mixed and processed foods—appear. Players must score points by correctly selecting appropriate foods in accordance with their knowledge and the game’s prompts. When a wrong selection is made, the system only gives a reminder without disclosing the correct answer. This urges players to master knowledge and classification of food glycemic indices through trial and error, thereby improving their judgment ability.
Meal Preparation Game
Players are required to input multiple items of personal health information in the game, including age and gestational week, and such data can be dynamically updated with prenatal examinations. Based on this information, the system generates a personalized nutrition guidance plan, which includes the daily required energy, the servings of various types of foods, suggestions on meal times and frequency, as well as recommended foods.
Meanwhile, targeted prompts on food selection are provided according to the player’s weight gain and prenatal examination results. Subsequently, players enter the meal preparation interface and complete the food selection for three daily meals and additional meals in line with the requirements of the nutrition guidance plan. After submitting the prepared meals, the serious game will provide specific feedback.
Gestational Sugar-Control Gourmet and Kitchen Cooking
Users purchase ingredients as guided by the system in a virtual supermarket scenario, adding foods from the shelves to the virtual shopping cart. After completing the purchase, they proceed to the kitchen to cook the ingredients and must select an appropriate cooking method. If an incorrect cooking method is chosen, the system will issue a reminder along with relevant suggestions.
Nutritious Meal Plate Challenge
Players act as pregnant women dining out and order food from a diverse menu in the restaurant. If an inappropriate food is ordered, the serious game will pop up a prompt, and the player must re - select until the correct choice is made.
Additionally, players need to complete a matching game for assessing the intake of different types of foods by applying the simple palm - size portion guide. Only after clearing this level can they proceed to the serving session.
Usability Evaluation of the Serious Game for GDM Dietary Health Education
Study Subjects
Convenience sampling was adopted in this study, and patients with GDM who visited The Third Affiliated Hospital of Guangzhou Medical University were selected as the research subjects. The inclusion criteria for the samples were as follows: (1) Aged 20 years or older; (2) Meeting the diagnostic criteria for GDM recommended in China’s Guidelines for the Diagnosis and Treatment of Hyperglycemia in Pregnancy (2022);24 (3) Proficient in using smartphones and WeChat Mini Programs; (4) No communication disorders. The exclusion criterion was having severe pregnancy-related complications or comorbidities that prevented completion of the test. This study was approved by the Ethics Committee of the Third Affiliated Hospital of Guangzhou Medical University (Ethics Review No. [2024] No. 121) and was conducted in accordance with the principles of the Declaration of Helsinki. All study subjects provided written informed consent forms, which included permission for the publication of anonymized responses and direct quotes, and all data were anonymized throughout the study to protect participants’ privacy.
Both qualitative and quantitative evaluation methods were employed for the usability assessment in this study. Specifically, the think - aloud testing was used for the qualitative evaluation, and a usability assessment scale was adopted for the quantitative evaluation. (1) In think - aloud research, Nielsen29 points out that selecting 3–5 subjects is appropriate. The final number of subjects is determined by factors such as the experimenter’s skills and experience, and the number of iterations in the design plan. Considering the qualitative research purpose of this study—to gain in - depth insights into users’ subjective experiences and operational processes—purposive sampling was ultimately used to select 3 patients with GDM from those visiting The Third Affiliated Hospital of Guangzhou Medical University for the think - aloud testing. This approach ensured information saturation while maintaining the feasibility of the study. (2) Relevant studies on sample sizes for usability testing indicate that 80% of usability problems can be identified when the number of test subjects reaches 10, and all problems can be covered when the number increases to 15.30 Eventually, 30 patients with GDM were selected to conduct the survey using the usability assessment scale.
Research Instruments and Evaluation Methods
General Information Questionnaire
A self-designed general information questionnaire was adopted in this study, which included information such as age, gestational week, and history of Gestational Diabetes Mellitus (GDM).
Qualitative Evaluation
The think-aloud method was used for qualitative evaluation in this study. Before the test, the researchers prepared a set of specific tasks for the participants, and elaborated on the test method, functional characteristics of the game, development background, application purposes, core objectives of the test, and implementation procedures, while obtaining the participants’ consent for audio recording. These tasks specifically include: a) Log in and register on the game Mini Program, and enter personal information such as obstetric history, family history, and oral glucose tolerance test (OGTT) results; b) Check the “Nutrition Guidance Plan” and read the personalized nutrition guidance plan; c) Enter the “Fun Games” section, read the game agreement, and browse the game level directory; d) Experience the “Food Matching Elimination” level; e) Experience the “Glycemic Index (GI) Classification Master” level; f) Experience the simulated game sessions of “Gestational Sugar-Control Gourmet” and “Nutritious Meal Plate Challenge”; g) Based on the “Nutrition Guidance Plan”, experience the “Meal Preparation Game” level and select and combine foods according to individual daily calorie requirements; h) View articles on GDM dietary knowledge in the “Nutrition Knowledge Guidance” section. During the test, the researchers encouraged the participants to adopt a mode of “thinking aloud while operating”, urging them to express their true inner feelings and thoughts in real time while experiencing the game Mini Program. Meanwhile, the researchers conducted written records of key information during the think-aloud test, including task completion status, completion time, and usability issues.
Quantitative Evaluation
The Chinese version of the System Usability Scale (SUS) was used for the survey.31 This scale consists of 10 Likert items, with a total score of 70 or above regarded as a passing score. Specifically, higher scores on odd - numbered items indicate that patients have a higher degree of approval for the content of the items; in contrast, higher scores on even - numbered items mean that patients have a stronger disagreement with the corresponding content.
Data Collection Methods
(1) Qualitative evaluation: The one-on-one test between researchers and participants was conducted in a quiet consulting room. The participants were clearly informed that the test process would be audio - recorded, and the test began only after their informed consent was obtained. (2) Quantitative evaluation: The researchers introduced the purpose and content of the game Mini Program test to GDM patients. After obtaining their informed consent, the patients were allowed to experience the game Mini Program. After completing all game levels, the participants took part in the evaluation survey and finished filling out the System Usability Scale.
Statistical Analysis
Qualitative Data
NVivo 12.0 software was used for coding, and the content analysis method32 was adopted for data analysis. The researchers transcribed the interview recordings into text. In the coding process, a combination of inductive and deductive methods was applied to sort out and refine the data word by word, and then summarize and form core themes.
Quantitative Data
SPSS 27.0 statistical software was employed to analyze the questionnaire data. Continuous variables were expressed as mean ± standard deviation, and categorical variables were presented as frequency (%).
Results
Qualitative Evaluation Results
Three GDM patients participated in the think-aloud test, and they were numbered P1, P2, and P3 respectively. All three patients basically completed the test tasks, with an average time required of 17.67 minutes. Their effectiveness in completing the target tasks was 87.5%, 75.0%, and 87.5% respectively, while their efficiency was 2.71 minutes per task, 3 minutes per task, and 2.29 minutes per task.
Among the participants, two were unsure how to fill in obstetric information in the “Personal Information” section, and one failed to select foods of the same category in the “Food Matching Elimination” section, requiring prompts from the researchers. One participant failed to read the game rule prompts clearly in the “Glycemic Index (GI) Classification Master” section, which resulted in the failure to clear this section. Additionally, one participant could not find the “Nutrition Knowledge Guidance” section. The expressions made by the participants during the test were coded, and two core themes were summarized through the content analysis method. Basic information of the participants is shown in Table 1.
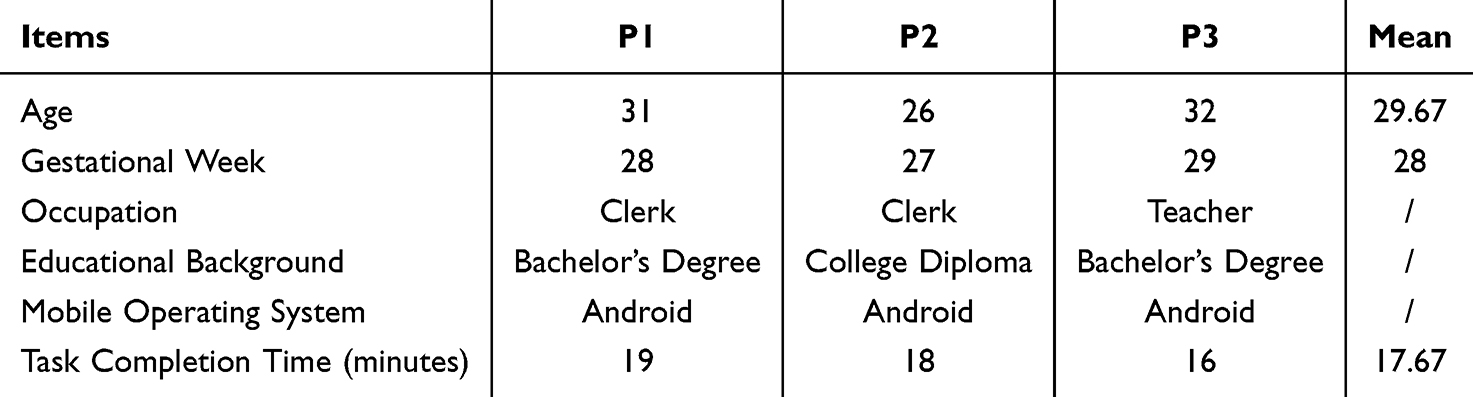 |
Table 1 Demographic Data and Test Task Duration of Participants |
Theme 1: The Game Content Possesses Practical Value
All three participants affirmed the positive significance of the serious game during the test tasks, and gave positive evaluations of its content. They believed the game was highly practical and facilitated better acquisition of relevant knowledge and skills.
P1: It turns out I can input the gestational week here. This is really convenient. I can also check the content of the relevant nutrition document here.
P2: While playing just now, I learned about the meat matching for lunch and dinner. I used to cook two types of meat separately, which was quite troublesome. It turns out I misunderstood the proper way. I think this game is really useful and helps me gain a much clearer understanding.
P3: This game is pretty good and really useful to me. If I can’t remember whether certain foods are suitable for me to eat, I can play this game for a quick reminder.
Theme 2: Access to Interesting Emotional Experiences
P1: This is my first time encountering a game designed for learning. Besides, the design is excellent—it’s quite similar to real menus, and it’s really entertaining.
P3: In terms of design, the game is clear and minimalist with reasonable categorization. It’s really fun to play. It will give me a reminder when I make a wrong match, and I can keep trying until I get it right. It’s not too difficult, and doesn’t take much time.
Quantitative Evaluation Results
General Information Survey Results
A total of 30 participants participated in the usability evaluation of this study. Their average age was (31.63±3.18) years, with an average gestational week of (25.83±1.37). The pre-pregnancy BMI was (24.40±3.82). Regarding educational background, 1 participant (3.3%) had an education level of senior high school or below, 26 participants (86.7%) had a college diploma or bachelor’s degree, and 3 participants (10%) had a master’s degree or above. Among them, 6 participants (20%) had a family history of diabetes, and 24 participants (80%) did not. In addition, 4 participants (13.3%) had a previous history of GDM, while 26 participants (86.7%) had no such history.
SUS Score Results
The survey results showed that the 30 participants gave favorable evaluations of the usability of the serious game, with the mean total SUS score being (79.50±4.17). The scores for each item are detailed in Table 2.
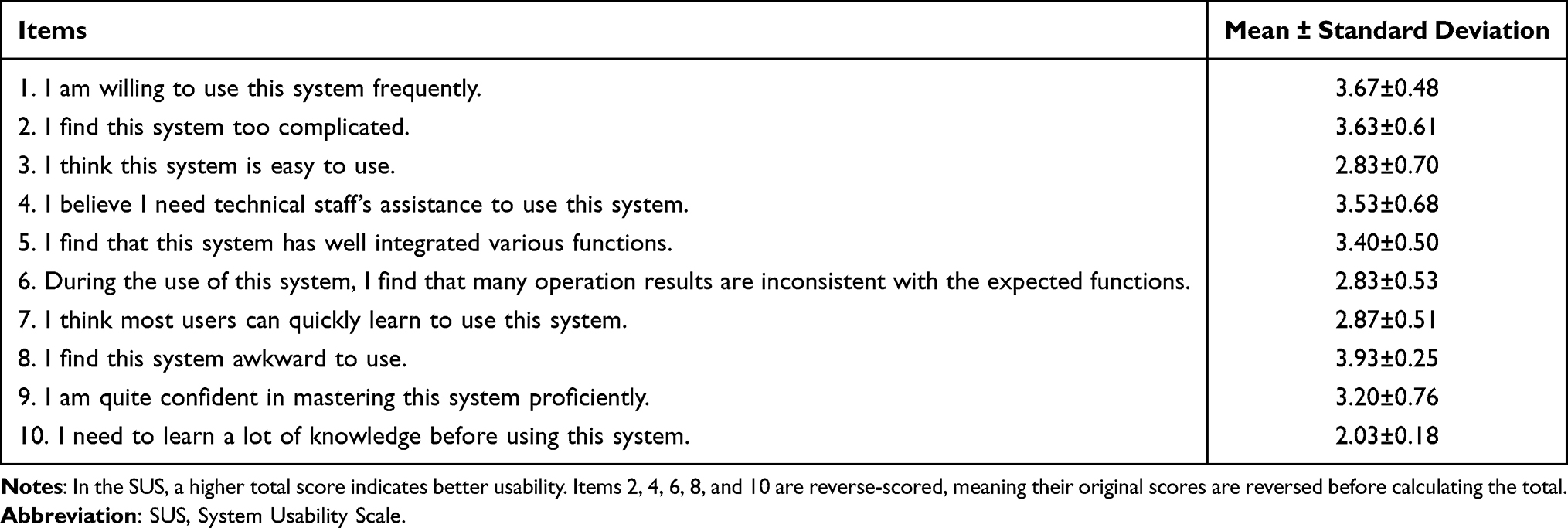 |
Table 2 Scores of Each Item in the SUS (n=30) |
Discussion
The Serious Game for GDM Dietary Health Education Features Rich and Scientific Content
Health education is a cost-effective and effective approach to modifying health behaviors.33 With the rapid advancement of mobile intelligent technologies, providing convenient and personalized dietary self-management education for pregnant women with GDM in a digital form has become a key research direction in the field of GDM nutritional intervention.34–36 However, studies have indicated that health management software for pregnancy currently available on mainstream application platforms generally suffers from poor quality.37
A study conducted by Dodd et al38 revealed that although mobile applications can help pregnant women improve their dietary quality during pregnancy, these applications are plagued by low adoption and usage rates. They suggested that integrating game-based strategies could enhance pregnant women’s acceptance and usage of such applications in the future. In addition, compared with traditional mobile applications, WeChat Mini Programs have distinct advantages in terms of usability, accessibility, and development costs, including simple operation, easy access and dissemination, as well as low development and maintenance costs.39 Therefore, based on clinical guidelines, evidence summaries and other literatures related to GDM dietary management, this study designed and developed a serious game Mini Program for dietary health education in a goal-oriented manner under the guidance of the SGDA framework. The script content was optimized through the expert meeting method to ensure its scientific validity and authority. In the script design, GDM dietary knowledge was integrated into interactive experiences. The game consists of five core modules, namely Food Matching Elimination, Glycemic Index Classification Master, Meal Preparation Game, Gestational Sugar-Control Gourmet, and Nutritious Meal Plate Challenge. It forms a comprehensive system of dietary management knowledge and skills, covering food classification, glycemic index judgment, meal preparation, cooking, and food selection when dining out. Meanwhile, expert opinions were incorporated to ensure the scientific validity and applicability of the game content, thus guaranteeing the rational design of the serious game for GDM dietary health education developed in this study.
The GDM Dietary Health Education Serious Game Combines Education with Entertainment and Boasts Good Usability
The guidelines on mobile health issued by the World Health Organization40 emphasize that usability evaluation should be conducted prior to assessing the effectiveness of mobile health interventions to ensure patients have a positive user experience. For this reason, this study adopted a mixed-methods research design, combining think-aloud testing with the SUS survey to comprehensively evaluate the usability of the serious game from both quantitative and qualitative perspectives, with the two types of data complementing and validating each other.
Quantitative results showed that the mean total SUS score was (79.50±4.17), which was higher than the generally recognized threshold for good usability, indicating that the game program developed in this study had favorable usability.41
Further analysis of the scores for each item revealed that Item 8 (an even-numbered item) and Item 1 (an odd-numbered item) received the highest scores, suggesting that users had a positive operational experience and strong willingness to accept the game. This was consistent with the qualitative evaluation from the think-aloud testing—participants commented that the game featured an innovative and user-friendly design with appropriate challenges, which could stimulate learning interest and provide a positive emotional experience, consistent with the findings of scholar Ren.42 This may be attributed to the study’s design choices, such as avoiding excessive medical terminology, providing sufficient game guidance, and adhering to the functional game framework; its design and functions aligned with patients’ needs, enabling it to deliver dietary education information while offering interactive experiences.
In addition, Item 10 obtained a relatively low score in the quantitative results, indicating that users perceived the need to learn a substantial amount of GDM dietary knowledge during use. This reflects the game’s core design concept of linking knowledge mastery to level clearance, ie, promoting players’ acquisition and application of knowledge through level challenges.43 The qualitative evaluation further validated this usability result: participants stated that the serious game was highly practical, helping them better remember dietary recommendations and providing a convenient way of learning, thereby enhancing GDM patients’ dietary knowledge to a certain extent, which was consistent with the findings of other studies.44,45 The reason for this may lie in the edutainment model adopted in this study, which integrates scientific knowledge into immersive experiences, thereby naturally stimulating patients’ learning interest and improving their concentration and engagement.46 In conclusion, the serious game developed in this study exhibited excellent usability and user experience. It can effectively support patients’ dietary education and management, and thus can be promoted as an auxiliary tool for dietary education among GDM patients.
Limitations of This Study
The participants in the usability evaluation of this study were all recruited from a single hospital. This may lead to limitations in the generalizability of the research results to the broader population of GDM patients due to regional and environmental constraints, making it difficult to fully reflect the differences in usage experiences and needs for the serious game among patients with diverse characteristics. In addition, this study lacked a follow-up assessment of users’ long-term usage behaviors and did not verify the actual intervention effect of the game on GDM patients’ dietary management by incorporating objective clinical indicators. Future studies could expand the sample scope, evaluate the actual effect of the game intervention through long-term follow-up combined with clinical indicators, so as to more comprehensively optimize the game design and verify its application value in GDM dietary management.
Conclusion
Guided by the SGDA framework, this study designed and developed a serious game for GDM dietary health education, and optimized the script content through the expert panel meeting method. The game encompasses five core functional modules, namely Food Matching Elimination, GI Classification Master, Meal Preparation Game, Gestational Sugar-Control Gourmet, Kitchen Cooking, and Nutritious Meal Plate Challenge. A mixed-methods research approach was adopted to conduct a usability evaluation of this serious game. Specifically, think-aloud testing and the System Usability Scale (SUS) were applied to systematically assess its usability. The results indicated that most participants recognized the game as highly interesting and practical. It integrates education with entertainment, enabling patients to learn GDM-related dietary knowledge effectively, and the participants expressed their willingness to use this game Mini Program.
Therefore, the serious game developed in this study can be integrated into existing GDM clinical management as an auxiliary tool for dietary guidance. After being incorporated into the health system for standardized promotion and maintenance, its application reliability and usability can be further improved. Meanwhile, the application value of the game can be extended to patients’ families; by encouraging spouses and other family members to participate, it can serve as a joint family learning tool, helping to build a family-level sugar control support environment. Future research needs to expand the sample coverage, conduct large-scale multi-center studies, and verify the long-term intervention effect of the game.
Ethics Approval and Consent to Participate
This work has been carried out in accordance with the Declaration of Helsinki (2000) of the World Medical Association. This study was approved by the Ethics Committee of the Third Affiliated Hospital of Guangzhou Medical University (Ethics Review No. [2024] No. 121). All study subjects provided written informed consent forms, which included permission for the publication of anonymized responses and direct quotes, and all data were anonymized throughout the study to protect participants’ privacy.
Author Contributions
All authors contributed to data analysis, drafting or revising the article, have agreed on the journal to which the article will be submitted, gave final approval of the version to be published, and agree to be accountable for all aspects of the work.
Funding
Guangzhou Health Science and Technology Project (No. 20231A011090);University-Industry-University Collaborative Innovation Fund of China (No. 2023HT018); College Students’ Innovation and Entrepreneurship Training Program (No. S202510573006).
Disclosure
The authors report no conflicts of interest in this work.
References
1. McIntyre HD, Catalano P, Zhang C, et al. Gestational diabetes mellitus. Nat Rev Dis Primers. 2019;5(1):47. doi:10.1038/s41572-019-0098-8
2. Mahmoud E, Elsayed AM, Elsayed B, et al. Association between gestational diabetes mellitus diagnostic criteria and adverse pregnancy outcomes-a systematic review and meta-analysis of adjusted effect sizes from studies using current diagnostic criteria. BMJ Open. 2024;14(11):e091258. doi:10.1136/bmjopen-2024-091258
3. Gao C, Sun X, Lu L, Liu F, Yuan J. Prevalence of gestational diabetes mellitus in mainland China: a systematic review and meta-analysis. J Diabetes Investig. 2019;10(1):154–12. doi:10.1111/jdi.12854
4. Juan J, Yang H. Prevalence, Prevention, and Lifestyle Intervention of Gestational Diabetes Mellitus in China. Int J Environ Res Public Health. 2020;17(24):9517. doi:10.3390/ijerph17249517
5. Weng HY, He Y, Han PP. Investigation on disease cognition, dietary and exercise status of pregnant women with gestational diabetes mellitus and analysis of intervention countermeasures. Maternal Child Health Care China. 2023;38(20):3980–3984.
6. Guo YH, Kou LH, Zhang Y, et al. Current status of medical nutrition therapy for gestational diabetes mellitus in China. Chin Nurs res. 2020;34(23):4267–4270.
7. Xiao GH, Wei H-Z, Deng H-Y, Xiao G-H, Zhang Y-C. A study on self - management behaviors of patients with gestational diabetes mellitus based on social cognitive theory. Neoplasma. 2023;70(1):1–14. doi:10.4149/neo_2022_220724N745
8. Shi WX, Guo M, Kong M, Zhang YP. Meta-analysis of the effect of one-day clinic for gestational diabetes mellitus on maternal blood glucose control and pregnancy outcomes. J Nurses Training. 2023;38(09):804–810.
9. Wang LX, Zheng MF, Qin SM. Effects of family - centered empowerment education combined with diversified management on pregnancy outcomes and breastfeeding efficacy of pregnant women with gestational diabetes mellitus. Maternal Child Health Care China. 2023;38(21):4264–4267.
10. Liu YY, Li HY, Zhang YX, et al. Application of SFEE dietary management intervention in patients with gestational diabetes mellitus. Chin Nurs res. 2023;37(12):2233–2238.
11. Maxim RI, Arnedo-Moreno J. Identifying Key Principles and Commonalities in Digital Serious Game Design Frameworks: scoping Review. JMIR Serious Games. 2025;13:e54075.
12. Aster A, Laupichler MC, Zimmer S, Raupach T. Game design elements of serious games in the education of medical and healthcare professions: a mixed-methods systematic review of underlying theories and teaching effectiveness. Adv Health Sci Educ Theory Pract. 2024;29(5):1825–1848. doi:10.1007/s10459-024-10327-1
13. DeSmet A, Shegog R, Van Ryckeghem D, Crombez G, De Bourdeaudhuij I. A Systematic Review and Meta-analysis of Interventions for Sexual Health Promotion Involving Serious Digital Games. Games Health J. 2015;4(2):78–90. doi:10.1089/g4h.2014.0110
14. Thomas TH, Sivakumar V, Babichenko D, Grieve V, Klem ML. Mapping Behavioral Health Serious Game Interventions for Adults With Chronic Illness: scoping Review. JMIR Serious Games. 2020;8(3):e18687. doi:10.2196/18687
15. Suleiman-Martos N, García-Lara RA, Martos-Cabrera MB, et al. Gamification for the Improvement of Diet, Nutritional Habits, and Body Composition in Children and Adolescents: a Systematic Review and Meta-Analysis. Nutrients. 2021;13(7):2478. doi:10.3390/nu13072478
16. Lamas S, Rebelo S, Da CS, et al. The Influence of Serious Games in the Promotion of Healthy Diet and Physical Activity Health: a Systematic Review. Nutrients. 2023;15(6):1399. doi:10.3390/nu15061399
17. Yang Q, Yang Y, Nie G, Lou J. The impact of mobile health interventions on maternal-neonatal outcomes in women with gestational diabetes mellitus: a systematic review and meta-analysis. Front Endocrinol. 2025;16:1707520. doi:10.3389/fendo.2025.1707520
18. Zhang RL, Wei Q, Xu YQ, et al. Application of visual game-based education in blood glucose management of pregnant women with gestational diabetes mellitus. Evidence-Based Nursing. 2025;11(24):5222–5225.
19. Xu YY, Huang FY, Cai S, et al. A qualitative study on the cognition and demand of patients with gestational diabetes mellitus for developing a mini program of dietary health education games. J Nurs Sci. 2024;39(16):86–89.
20. Wang SX, Chen YJ, Li SY, et al. Summary of the best evidence for dietary management of gestational diabetes mellitus. Chin J Clin Res. 2022;35(2):284–288.
21. Cao YN, Zhu YN, Wang NN, et al. Summary of evidence for dietary management of pregnant women with gestational diabetes mellitus. Chin J Nurs Educ. 2021;18(11):1040–1046.
22. Cao QM, Wang WJ, Zhang L, et al. Practice of balanced dietary patterns among Chinese residents: interpretation of the dietary guidelines for Chinese residents (2022). Food Mach. 2022;38(6):22–29. doi:10.13652/j.spjx.1003.5788.2022.60050
23. Chinese Nutrition Society. Releases the Dietary Reference Intakes for Chinese Residents (2023 Edition). Acta Nutrimenta Sinica. 2023;45(5):414.
24. The Obstetrics Group of Chinese Society of Obstetrics and Gynecology, Chinese Society of Perinatal Medicine, Professional Committee of Pregnancy Complicated with Diabetes of China Maternal and Child Health Association. Guidelines for the Diagnosis and Treatment of Hyperglycemia in Pregnancy (2022) [Part One]. Chin J Obstetric Gynecol. 2022;57(1):3–12.
25. Li YT. Knowledge Reader on Pregnancy Complicated with Diabetes. South China University of Technology Press; 2017.
26. Mitgutsch K, Alvarado N. Purposeful by design? A serious game design assessment framework.
27. Ma YM, Bernard Y, Francois C, Flore V. Design of serious games in industrial engineering education. J Higher Eng Educat Res. 2022;2022(6):80–85.
28. Chinese Nutrition Society. Interpretation of the Group Standard for Food Exchange Servings[EB/OL]; 2025.
29. Nielsen J. Estimating the number of subjects needed for a thinking aloud test. Int J Hum-Comput Stud. 1994;41(3):385–397. doi:10.1006/ijhc.1994.1065
30. Virzi RA. Refining the test phase of usability evaluation: how many subjects is enough? Hum Fact. 1992;34(4):457–468. doi:10.1177/001872089203400407
31. Wang Y, Lei T, Liu X. Chinese system usability scale: translation, revision, psychological measurement. Int J Hum Comput Interact. 2020;36(10):953–963. doi:10.1080/10447318.2019.1700644
32. Hsieh H, Shannon SE. Three approaches to qualitative content analysis. Qual Health Res. 2005;15(9):1277–1288. doi:10.1177/1049732305276687
33. Beard E, West R, Lorencatto F, et al. What do cost-effective health behaviour-change interventions contain? A comparison of six domains. PLoS One. 2019;14(4):e0213983. doi:10.1371/journal.pone.0213983
34. Hu MY. Application of feedback - based health education on APP platform combined with individualized dietary nursing in patients with gestational diabetes mellitus. Qingdao Medical Health. 2023;55(2):93–97.
35. Tumminia A, Vitacolonna E, Sciacca L, et al. “MySweetGestation”: a novel smartphone application for women with or at risk of diabetes during pregnancy. Diabet Res Clin Pract. 2019;158:107896. doi:10.1016/j.diabres.2019.107896
36. Al Hashmi I, Alsabti H, Al Omari O, Al Nasseri Y, Khalaf A. Development, feasibility and acceptability of a self-efficacy-enhancing smartphone application among pregnant women with gestational diabetes mellitus: single-arm pilot clinical trial. BMC Pregnancy Childbirth. 2022;22(1):358. doi:10.1186/s12884-022-04684-1
37. Kalhori SRN, Hemmat M, Noori T, Heydarian S, Katigari MR. Quality evaluation of English mobile applications for gestational diabetes: app review using Mobile Application Rating Scale (Mars). Curr Diabetes Rev. 2021;17(2):161–168. doi:10.2174/1573399816666200703181438
38. Dodd JM, Louise J, Cramp C, et al. Evaluation of a smartphone nutrition and physical activity application to provide lifestyle advice to pregnant women: the SNAPP randomised trial. Maternal and Child Nutrition. 2018;14(1):e12502. doi:10.1111/mcn.12502
39. Wu MH, Li J. Advantage analysis of WeChat Mini Programs and their application in enterprises. Electron Technol Softw Eng. 2019;2019(15):45–46.
40. Agarwal S, LeFevre AE, Lee J, et al. Guidelines for reporting of health interventions using mobile phones: mobile health (mHealth) evidence reporting and assessment (mERA) checklist. BMJ. 2016;352:i1174. doi:10.1136/bmj.i1174
41. Bangor A, Kortum P, Miller J. Determining what individual SUS scores mean: adding an adjective rating scale. J Usability Stud. 2009;4(3):114–123.
42. Ren JL, Ma KL, Zhang DY, et al. Development and application of a pulmonary rehabilitation health education game for patients with chronic obstructive pulmonary disease. Chin J Nurs. 2025;60(5):525–531.
43. Chen SY, Wang F. A study on the design of healthy diet APP based on gamification. Popular Literature and Art. 2020;2020(3):133–134.
44. Zhao Q, Niu ME, Han YX, et al. Development and evaluation of a serious game for guiding inhaler use in patients with chronic obstructive pulmonary disease. J Nurs Sci. 2023;38(23):98–102.
45. Wang L, Wu LP, Wang P, et al. Development and application of health education game software for children with type 1 diabetes mellitus. Chin J Nurs. 2020;55(11):1659–1664.
46. Ke WL. A study on the application of health education game mode in 140 middle - aged and young patients with type 2 diabetes mellitus. Chin J Typical Cases. 2024;18(4):105–108.
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.