Back to Journals » Clinical Interventions in Aging » Volume 20
Development and Testing a New Online Dynamic Nomogram for Contrast-Induced Acute Kidney Injury in Elderly Patients with ST-Segment Elevation Myocardial Infarction
Authors Jin J ![]() , Ding J, Zhang X
, Ding J, Zhang X ![]() , Wang L
, Wang L ![]() , Zhang X
, Zhang X ![]() , Li W
, Li W ![]() , Li S
, Li S ![]()
Received 23 May 2025
Accepted for publication 19 July 2025
Published 25 July 2025 Volume 2025:20 Pages 1085—1098
DOI https://doi.org/10.2147/CIA.S534736
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Zhi-Ying Wu
Jingkun Jin,1,* Jiahui Ding,1,* Xishen Zhang,1 Linsheng Wang,1 Xudong Zhang,1 Wenhua Li,1,2 Shanshan Li2
1The First School of Clinical Medicine, Xuzhou Medical University, Xuzhou, People’s Republic of China; 2Department of Cardiology, The Affiliated Hospital of Xuzhou Medical University, Xuzhou, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Wenhua Li; Shanshan Li, Email [email protected]; [email protected]
Background: ST-segment elevation myocardial infarction (STEMI), the most severe form of acute coronary syndrome (ACS), requires timely percutaneous coronary intervention (PCI) to restore coronary blood flow. However, contrast-induced acute kidney injury (CI-AKI), the third most common cause of hospital-acquired renal failure, remains a critical complication of PCI.
Objective: To develop a machine learning model predicting CI-AKI risk in elderly patients with STEMI patients using clinical features.
Methods: Data from 2120 elderly patients with STEMI treated with PCI at Xuzhou Medical University Affiliated Hospital (2019– 2023) were used for model development and testing. An external validation cohort, comprising 236 individuals, was derived from the Medical Information Mart for Intensive Care-IV (MIMIC-IV) database (2008– 2019). Lasso regression selected predictors, and nine Machine Learning (ML) algorithms were evaluated via Receiver Operating Characteristic (ROC) analysis. Overlapping top-ranked features from high-performing models (AUC > 0.8) informed a nomogram. Performance was assessed using AUC and decision curve analysis (DCA).
Results: The final model included five independent predictors: lymphocyte-to-monocyte ratio, diuretic use, residual cholesterol, serum creatinine, and blood urea nitrogen. This model was developed as a simple-to-use online dynamic nomogram. It demonstrated robust discrimination, with C-statistics of 0.782 in the testing dataset and 0.791 in the validation dataset. DCA confirmed its clinical utility across a wide range of risk thresholds.
Conclusion: A new online dynamic nomogram was developed to provide a practical tool for CI-AKI risk stratification in elderly STEMI patients, aiding personalized prevention strategies.
Keywords: contrast-induced acute kidney injury, ST-segment elevation myocardial infarction, remnant cholesterol, lymphocyte to monocyte ratio, elderly patients
Background
ST-segment elevation myocardial infarction (STEMI), the most severe manifestation of acute coronary syndrome (ACS), necessitates timely revascularization via percutaneous coronary intervention (PCI) to restore coronary blood flow and optimize clinical outcomes. A critical complication of PCI is contrast-induced acute kidney injury (CI-AKI), a reversible form of acute kidney injury occurring within 72 hours after intravascular contrast agent administration. CI-AKI ranks as the third most prevalent cause of hospital-acquired renal failure, surpassed only by hypoperfusion and nephrotoxic medications.1 In elderly STEMI patients, CI-AKI is associated with prolonged hospitalization, elevated healthcare costs, progression to end-stage renal disease, and increased mortality.2 While the pathophysiology of CI-AKI remains incompletely understood, proposed mechanisms include contrast-mediated renal ischemia, oxidative stress, and inflammatory cascades.3 Current prevention strategies are limited to hydration protocols, highlighting the urgent need for early identification of high-risk patients to mitigate irreversible renal damage.
Machine learning (ML), a subset of artificial intelligence (AI), has emerged as a transformative tool for analyzing complex medical datasets.4 Its capacity to discern nonlinear patterns in clinical variables enables the development of predictive models that outperform conventional statistical approaches in accuracy and generalizability. These models are increasingly deployed in critical care settings, including coronary care units (CCUs), to guide risk stratification and therapeutic decision-making. This study aims to develop an interpretable ML-based model leveraging routine clinical features to predict CI-AKI risk in elderly STEMI patients undergoing PCI, thereby facilitating personalized preventive interventions.
Existing clinical scoring systems and statistical models for CI-AKI risk assessment often lack generalizability and interpretability, especially in older STEMI patients undergoing PCI. They also do not fully utilize the predictive power of clinical data available through advanced computational methods. This gap highlights the urgent need for early identification of high-risk patients to mitigate irreversible kidney damage.
The aim of this study was to develop a machine-learning based interpretable model that uses clinical features to predict the risk of CI-AKI in elderly STEMI patients undergoing PCI, thereby facilitating personalized preventive interventions. By enabling personalized prevention strategies, the model aims to reduce kidney injury and improve clinical outcomes in this vulnerable population.
Materials and Methods
Study Population
This study retrospectively selected patients with STEMI who underwent PCI at the CCU of Xuzhou Medical University Affiliated Hospital from 2019 to 2023 and a validation cohort from the MIMIC-IV database who underwent PCI from 2008 to 2019.
Inclusion criteria: (1) Diagnosis of STEMI, confirmed by: Persistent chest discomfort and/or ischemic symptoms (>20 minutes at rest); Electrocardiographic evidence of ST-segment elevation (≥2 mm in contiguous chest leads or ≥1 mm in limb leads) corresponding to the infarct location, or new left bundle branch block; Elevated cardiac biomarkers (eg, troponin) confirming myocardial necrosis. (2) PCI treatment during hospitalization; (3) Complete clinical records; (4) Age ≥ 60 years.
Exclusion criteria: (1) Missing preoperative/postoperative renal function parameters including serum creatinine; (2) severe valvular heart disease necessitating surgical intervention; (3) Active systemic infection; (4) History of malignancies; (5) Severe hepatic dysfunction.
A total of 2120 patients from the Affiliated Hospital of Xuzhou Medical University and 236 patients from the MIMIC-IV database were ultimately included in this study. The flowchart outlining patient selection is provided in Figure 1.
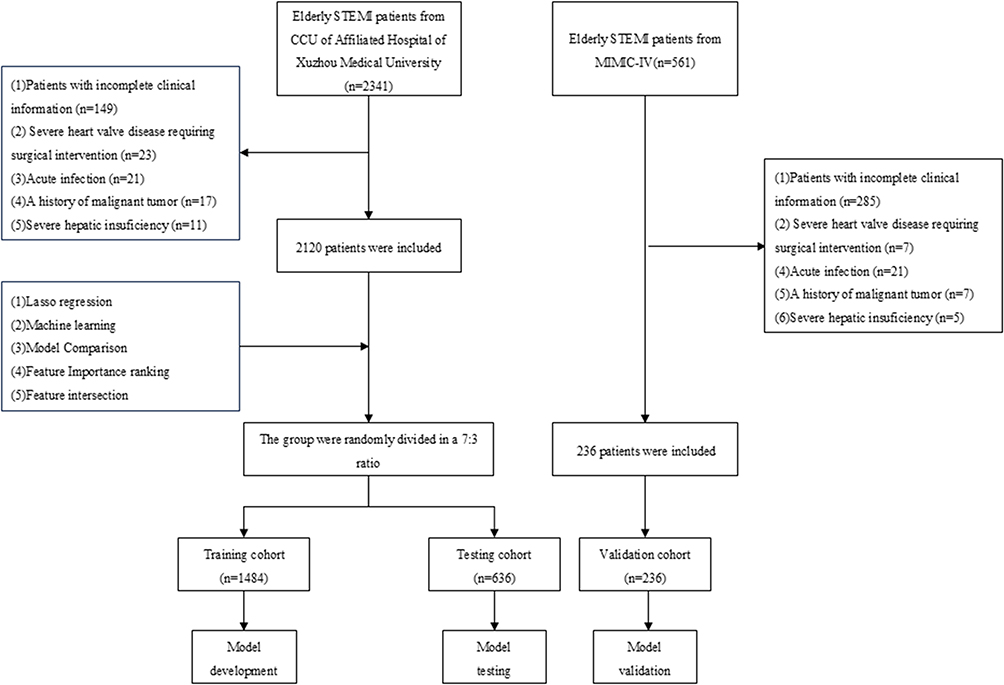 |
Figure 1 The flowchart describes the selection and statistical analysis of elderly patients undergoing PCI for ST-elevated acute myocardial infarction. |
Definition
CI-AKI is diagnosed when acute kidney injury (AKI) develops within 72 hours after contrast agent administration, following the exclusion of other causes of renal impairment. Diagnosis requires either a serum creatinine (Scr) increase of ≥0.3 mg/dL (26.5 μmol/L) or a rise to ≥1.5 times the baseline Scr level.5 Residual cholesterol acts as a significant indicator of cardiovascular disease risk. It denotes the cholesterol component present within lipoproteins that have a high triglyceride content, such as very-low-density lipoproteins (VLDL), intermediate-density lipoproteins (IDL), and chylomicrons.6 Residual cholesterol (RC) = total cholesterol (TC) – high density lipoprotein cholesterol (HDL-C) – low density lipoprotein cholesterol (LDL-C). The Mehran score, a validated risk stratification tool, categorizes patients into low-, moderate-, or high-risk groups based on clinical variables, enabling personalized risk assessment and management strategies.
Clinical and Laboratory Data Collection
Clinical data for patients from Xuzhou Medical University Affiliated Hospital were sourced from the institution’s electronic medical records. For patients in the MIMIC-IV database, the PostgreSQL database management system (version 14.5–1) and Navicat Premium database management tool (version 15) were used to access the MIMIC-IV database, with Structured Query Language (SQL) employed for data extraction. Data for all study subjects were collected at a point within 24 hours before the start of PCI in elderly STEMI patients, as close as possible to the actual start time of the PCI. Clinical data encompassed age, gender, smoking history, and additional demographic information; laboratory indices comprising white blood cell (WBC) count, red blood cell (RBC) count, hemoglobin, platelets, total bilirubin, albumin, glucose, creatinine, blood urea nitrogen (BUN), and others. RC and the lymphocyte-to-monocyte ratio (LMR), among other composite indices, were calculated. Variables with >30% missing data were excluded to preserve dataset integrity. For retained variables, missing data were imputed using the Multiple Imputation by Chained Equations (MICE) algorithm, ensuring robust handling of incomplete data.
Statistical Analysis
Patients from Xuzhou Medical University Affiliated Hospital were divided into training (70%) and testing (30%) cohorts, while the MIMIC-IV database cohort served as the external validation set. Continuous variables were presented as medians with interquartile ranges (IQRs) to summarize central tendency and dispersion, whereas categorical variables were expressed as frequencies and percentages. Differences between cohorts were analyzed using the Wilcoxon rank-sum test for continuous variables and Fisher’s exact test for categorical variables. Variables with statistically significant differences were incorporated into LASSO regression prior to the application of machine learning techniques to construct a model for predicting CI-AKI. The machine learning algorithms used encompass Extreme Gradient Boosting (XGBoost), Light Gradient Boosting Machine (LightGBM), Random Forest, Gradient Boosting Decision Trees (GBDT), Adaptive Boosting (AdaBoost), Gaussian Naive Bayes (GaussianNB), Multilayer Perceptron (MLP), Support Vector Machine (SVM), and k-Nearest Neighbors (KNN). Model performance was assessed using metrics such as the area under the receiver operating characteristic curve (AUROC), accuracy, sensitivity, and specificity. The optimal model was selected based on these criteria.
Variables from high-performing models were ranked by feature importance, and commonalities among top-ranked variables informed the final predictive model. Statistical analyses were performed using R (v4.2.3), Python (v3.11.4), and the Xsmart analytical platform (https://www.xsmartanalysis.com/). In accordance with the Transparent Reporting of a Multivariable Prediction Model for Individual Prognosis or Diagnosis (TRIPOD) guidelines, we systematically developed and validated the model to ensure methodological rigor and transparency. A P-value of less than 0.05 was considered statistically significant.
Results
Information Comparison
According to the CI-AKI diagnostic criteria, patients in the training set were stratified into non-CI-AKI (n =1182) and CI-AKI (n = 302) groups. Statistically significant differences were observed in a total of 51 variables, including age, smoking status, diastolic blood pressure (DBP), height, weight, and body mass index (BMI) (p < 0.05). The remaining indicators showed no significant differences (p > 0.05), with detailed results presented in Table 1.
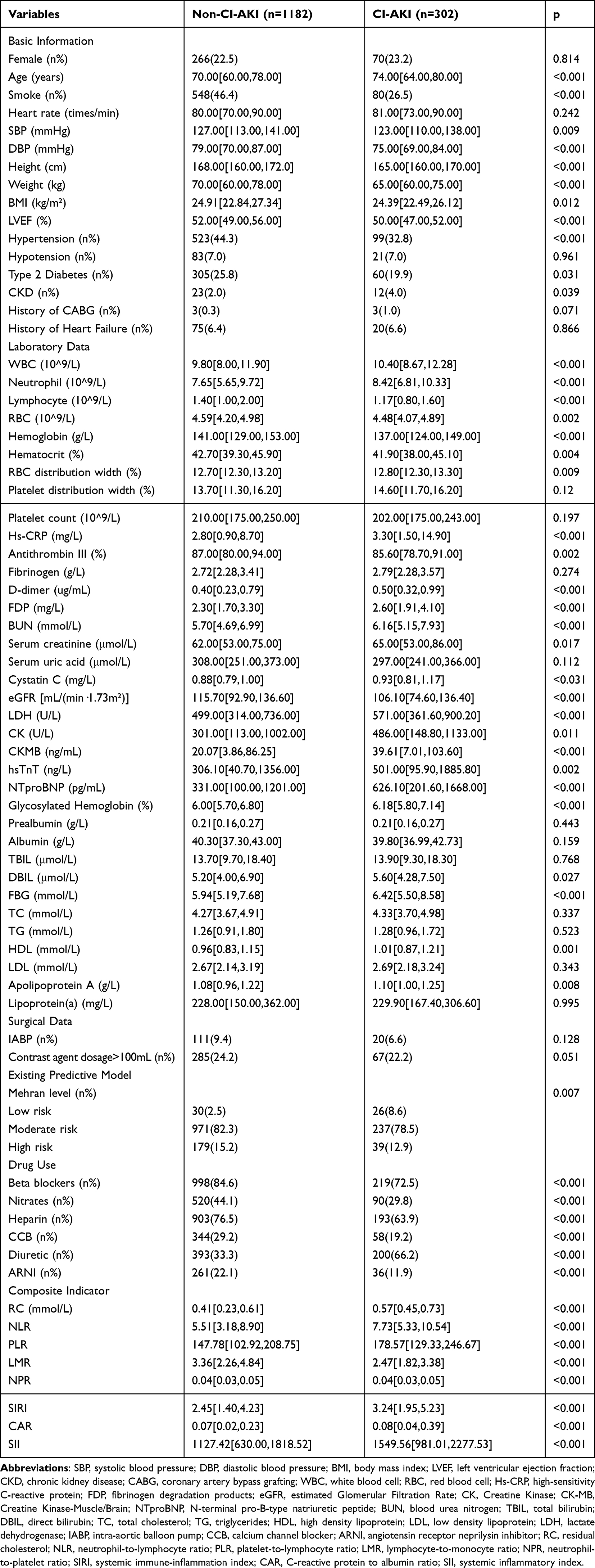 |
Table 1 The Comparison of Basic Information Between the Two Groups of Patients |
LASSO Clinical Feature Selection
We utilized 51 variables as independent predictors and conducted LASSO regression to model the occurrence of CI-AKI as the outcome. The optimal penalty coefficient λ was determined via 10-fold cross-validation, with the Lambda.1se value being 0.019. This process identified 18 predictive variables: age, height, hypertension, smoking, Mehran risk score, beta-blockers, nitrates, low molecular weight heparin, nicorandil, diuretics, high density lipoprotein, angiotensin receptor neprilysin inhibitor (ARNI), antithrombin III, BUN, creatinine, fasting blood glucose, LMR, and RC (Figure 2).
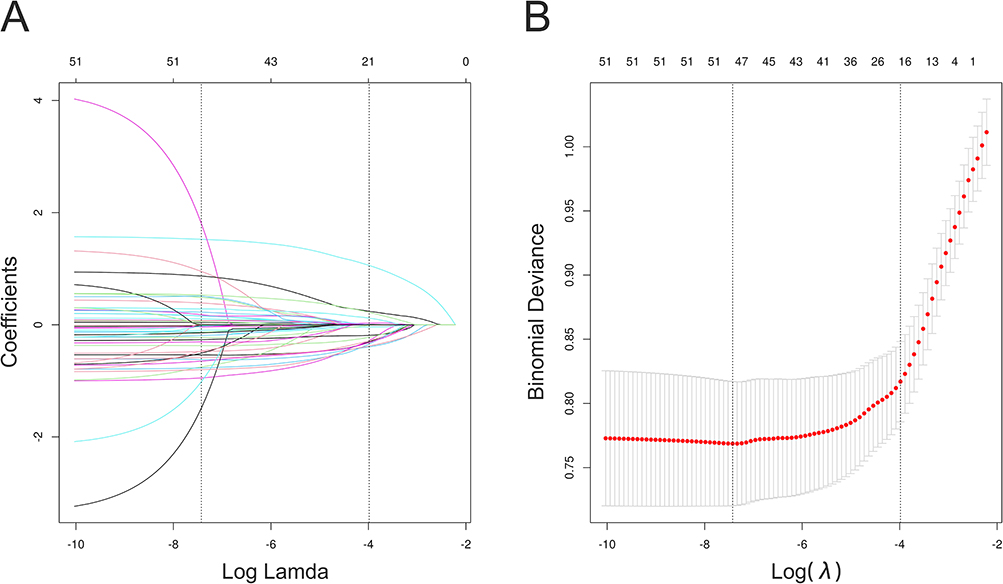 |
Figure 2 This is LASSO regression. (A)This graph shows the coefficient curve of the independent variable. (B)This graph shows the selection of the optimal independent variable by LASSO regression and 10-fold cross-validation. |
Analysis of Risk Factors for CI-AKI
After standardizing the 18 selected variables, nine machine learning algorithms were applied to develop predictive models. The following figures display the ROC curves for predicting CI-AKI for each model (Figure 3A). Table 2 outlines the performance of the nine machine learning algorithms on both training and validation dataset, including AUC, accuracy, sensitivity and specificity. The comparison of the AUC among nine machine learning models is depicted in the forest plot (Figure 3B). Models built using XGBoost, RandomForest, AdaBoost, and SVM had AUC scores above 0.8. Feature importance was ranked by four methods, and the top 10 intersecting features were selected (Figure 4).
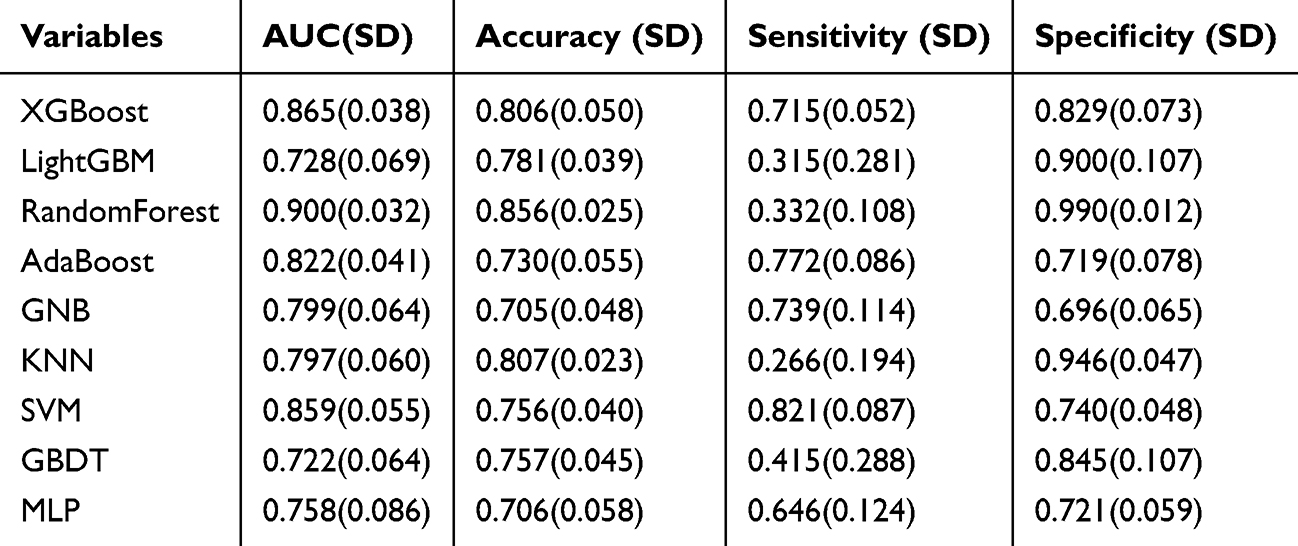 |
Table 2 Predictive Performance Comparison of the Nine Types of Machine Learning Algorithms |
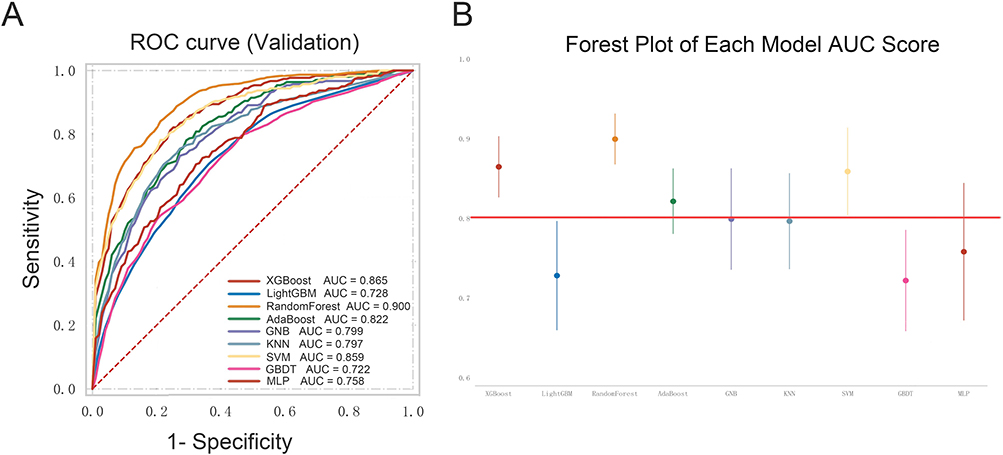 |
Figure 3 Prediction of CI-AKI based on selected variables using nine machine learning algorithms: ROC curves for validation set (A); and a forest plot of ROC-AUC across methods (B). Abbreviations: XGBoost, extreme gradient boosting; LightGBM, light gradient boosting machine; RF, random forest; GBDT, gradient boosting decision trees; AdaBoost, adaptive boosting; GNB, gaussian naive bayes; MLP, multilayer perceptron; SVM, support vector machine; KNN, k-nearest neighbors. |
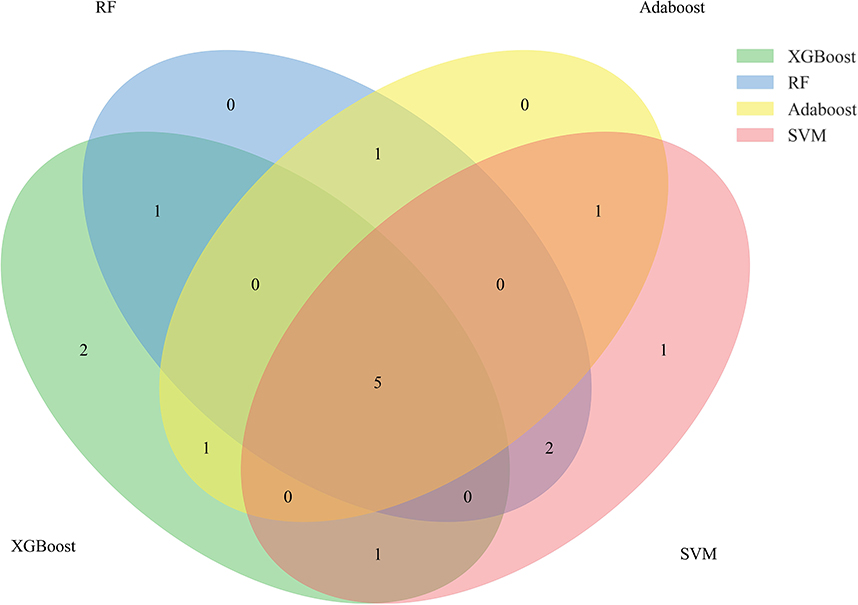 |
Figure 4 Venn diagram of the top 10 variables in four types of machine learning models. Abbreviations: XGBoost, extreme gradient boosting; AdaBoost, adaptive boosting; SVM, support vector machine; RF, Random Forest. |
Model Construction
The intersection of the top 10 most important variables across the four machine learning models identified five independent predictors of CI-AKI in STEMI patients post-PCI: LMR, diuretic use, RC, serum creatinine, and BUN (Table 3). These predictors were incorporated into a nomogram to visualize CI-AKI risk stratification (Figure 5).
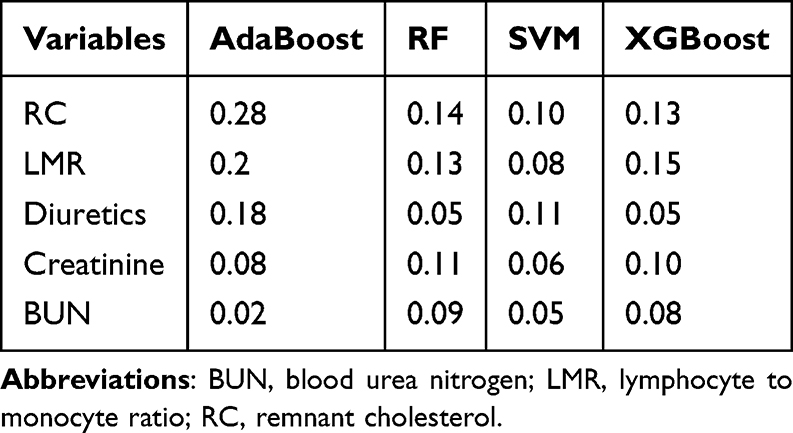 |
Table 3 The Importance of the Top 10 Variables in Four Well-Performing Models |
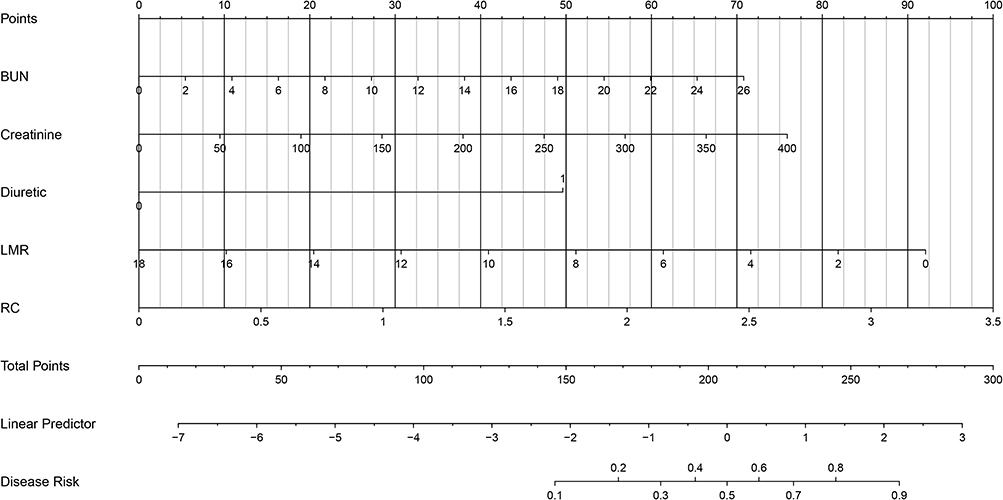 |
Figure 5 The nomogram of predictive model for CI-AKI after PCI in elderly patients with STEMI. Abbreviations: BUN, blood urea nitrogen; LMR, lymphocyte to monocyte ratio; RC, remnant cholesterol. |
In contrast to complex logistic regression models, the nomogram offers a simplified and clinically practical tool for risk stratification. Each of the five risk factors is assigned a point value, which users sum to calculate a total score. This total score corresponds to a vertical projection on the nomogram’s axis, directly translating to the predicted probability of CI-AKI. Higher scores indicate an elevated likelihood of CI-AKI development, enabling clinicians to tailor prevention strategies to individual patient profiles. The final model was developed as a simple-to-use nomogram, which is illustrated and available online (https://jjk0227.shinyapps.io/dynnomapp/) and presented in Figure 6.
 |
Figure 6 The online dynamic nomogram to predict CI-AKI After PCI in elderly patients with STEMI. Abbreviations: BUN, blood urea nitrogen; LMR, lymphocyte to monocyte ratio; RC, remnant cholesterol. |
Prediction Analysis
Internal validation demonstrated that the predictive model exhibits strong predictive performance (Figure 7A and B). The C-statistic values for the nomogram’s training and internal validation cohorts were 0.794 and 0.782, which were superior to the existing Mehran score of 0.632 and 0.588, indicating a high predictive value. As depicted in Figure 7D and E, the horizontal line on the decision curve analysis (DCA) curve signifies no intervention with zero net benefit, whereas the diagonal line represents intervention for all patients. The analysis revealed a broad range of high-risk threshold probabilities in both the modeling and validation cohorts, highlighting the model’s potential utility for guiding clinical decision-making. The calibration curves show that the model exhibits good fit and prediction accuracy on both the training set and the internal validation set. This consistency further confirms the reliability and generalizability of the model, making it highly practical for clinical applications (Figure 7G and H).
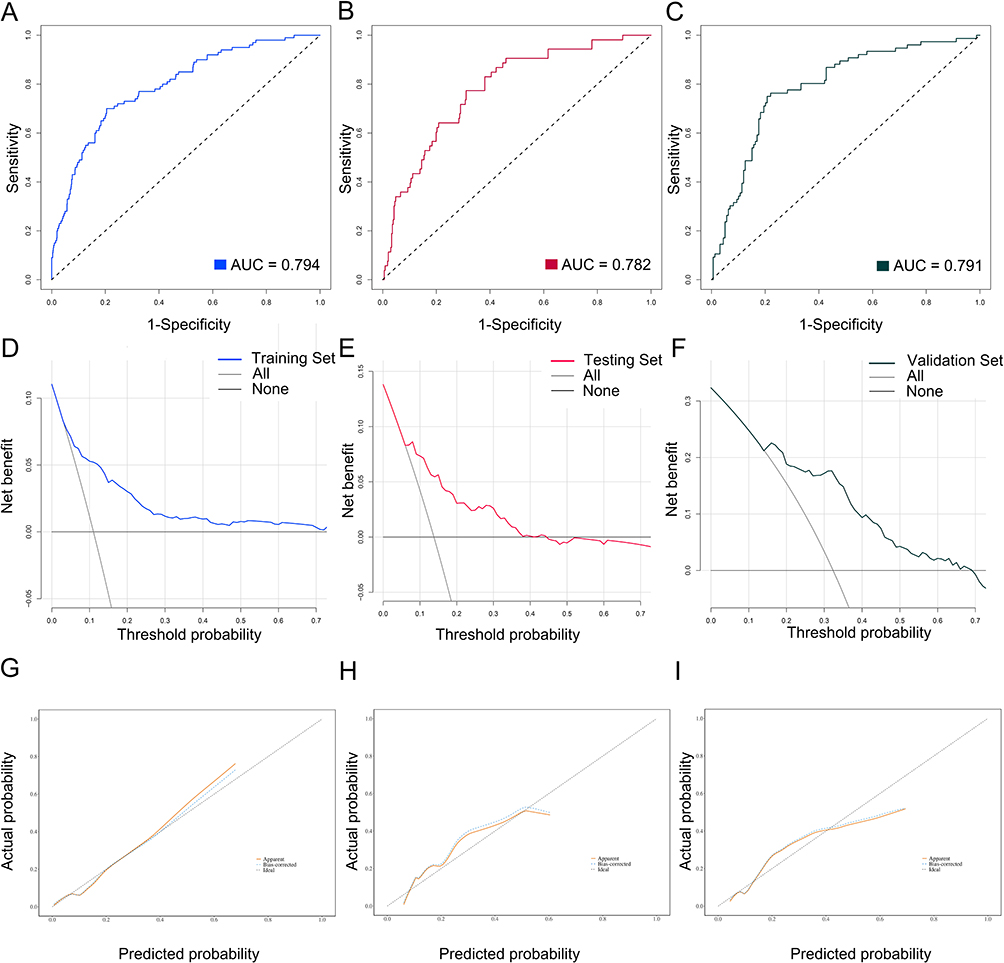 |
Figure 7 Illustrates ROC curves of the established predictive model for the occurrence of CI-AKI in elderly STEMI patients within the training (A), testing (B), and validation set (C); and the clinical decision-making benefits obtained within the training (D), testing (E), and validation set (F); and the calibration curves demonstrating the agreement between predicted and actual probabilities in the training (G), testing (H), and validation set (I). |
For external validation, C-statistics was 0.791 (Figure 7C), and the DCA curves (Figure 7F) indicated that the model more effectively predicted the clinical utility of CI-AKI risk within a probability threshold for risk ranging from 14% to 70%. In addition, the model also demonstrated good fit and predictive accuracy in calibration curve analysis on an external validation set. This further demonstrates the robustness and generalizability of the model on different datasets and enhances its potential for application in clinical practice (Figures 7I).
Discussion
In our research, we developed a cost-effective, interpretable machine learning model using data from the CCU of a leading tertiary hospital, with subsequent validation via a public database. The database incorporated diverse clinical variables, including demographics, lifestyle, past medical history, preoperative laboratory tests, intraoperative details, and medication usage. Among nine machine learning algorithms evaluated, models based on XGBoost, Random Forest, AdaBoost, and SVM demonstrated superior predictive accuracy, achieving cross-validation AUC scores above 0.80. Among these four models, BUN, LMR, RC, creatinine levels, and diuretic usage consistently ranked among the top 10 predictors of clinical significance. A nomogram integrating these five variables demonstrated potential to improve risk stratification for STEMI patients by accurately predicting CI-AKI. External validation confirmed the model’s robust performance, underscoring its translational potential for clinical decision-making.
The predictive model pinpointed several critical risk factors, encompassing preoperative RC, BUN, LMR, creatinine levels, and the utilization of diuretics. Baseline renal function markers such as creatinine and BUN demonstrated high predictive accuracy for CI-AKI, consistent with prior studies.7–9
Our study indicates that elevated residual cholesterol levels are associated with an increased risk of CI-AKI. These findings corroborate previous studies highlighting the role of cholesterol metabolism and inflammatory pathways in renal injury pathogenesis.10,11 The connection between cholesterol and the mechanisms of kidney damage has been a focal area of research.12
Residual cholesterol is particularly relevant for assessing residual cardiovascular risk in statin-treated patients with controlled LDL-C levels and has been closely linked to comorbidities such as coronary artery disease and diabetes mellitus.13–15 The study is the first to propose the role of RC in CI-AKI. Lipoproteins in RC are internalized by macrophages and other immune cells, forming foam cells. They induce the production of IL-6 and TNF-α via the PI3K/Akt and MAPK signaling pathways. This exacerbates vascular inflammation, oxidative stress, promoting atherosclerosis and renal ischemia, thereby elevating CI-AKI risk. Furthermore, RC regulates oxidized LDL receptors and NF-κB-dependent lectin-like receptors, enhancing TNF-α expression and foam cell formation.16 (2) STEMI is typically precipitated by thrombosis, induces a hypercoagulable state. RC not only upregulates PAI-1 to enhance platelet aggregation but also amplifies the coagulation cascade, reducing renal perfusion and oxygen, which amplifies CI-AKI risk.17
Furthermore, inflammatory processes play a critical role in the development of CI-AKI, and specific inflammatory biomarkers have been shown to forecast the occurrence of CI-AKI in patients with ACS following PCI. LMR, a novel inflammatory marker that has emerged in recent years, is defined as the ratio of lymphocyte count to monocyte count. It is considered to mirror the equilibrium between anti-inflammatory and pro-inflammatory immune reactions.18,19 A reduced LMR signifies pro-inflammatory dominance, increasing renal vulnerability to contrast-induced injury.20 Notably, elevated LMR levels are independently associated with a lower risk of postoperative AKI in aortic dissection patients.21
However, as previous research has noted, reliance on preoperative data alone is insufficient for outcome prediction. Our study assessed perioperative medication use and discovered that diuretic administration may reduce renal blood flow and impair tubular concentration capacity, thereby exacerbating renal stress and increasing the risk of CI-AKI.22,23 Additionally, diuretics may lead to electrolyte imbalances and acid-base disturbances, further compromising renal function.24
Unlike our previous studies, this study focused on elderly patients with STEMI, a subgroup at higher risk of CI-AKI due to age-related physiologic decline and complex revascularization protocols.25 An advanced machine learning algorithm was used to capture the complex nonlinear relationship between predictor variables and CI-AKI, whereas previous studies mainly relied on traditional statistical methods.26 In addition, this study used a larger sample size (N = 2120) and was externally validated through a public database (MIMIC-IV, 2008–2019), addressing the limitations of small sample sizes or single-center studies in previous studies.27 The developed online dynamic column-line diagram integrates key predictors into an intuitive interface, enabling clinicians to implement personalized prevention strategies at the bedside. This innovation not only enhances clinical utility, but also provides clinicians with a platform to calculate CI-AKI risk probabilities in real time, thus enabling timely interventions against modifiable risk factors to prevent or mitigate the occurrence of CI-AKI.
Limitations
First, the retrospective design of this study may introduce selection bias. Second, our ML algorithm model is somewhat constrained by specific mechanisms, necessitating further verification in real-world clinical settings. Additionally, the use of the MIMIC-IV database, a curated resource, presents inherent constraints, including potential data incompleteness. These limitations highlight the need for external validation with larger, more diverse cohorts to confirm the generalizability of our findings.
Future studies should prioritize establishing large, multicenter, and multi-ethnic cohorts to validate and refine the clinical risk prediction model, while concurrently identifying novel CI-AKI biomarkers to enhance the model’s predictive accuracy and clinical utility.
Clinical Perspectives
In the future we envision that our model can be seamlessly integrated into clinical workflows to further explore the correlation between intraoperative variables and outcome occurrences through multicenter and larger sample size studies and provide real-time risk stratification of older STEMI patients in clinical care, especially during PCI procedures. Early identification of high-risk individuals allows clinicians to make more informed decisions regarding contrast use, hydration strategies, and other preventive measures. This timely intervention may significantly reduce the incidence of CI-AKI and improve patient outcomes. We also further refine the patient types and assist clinicians in giving intraoperative as well as perioperative personalized treatment plans based on the patient’s underlying and individual needs.
Conclusion
This study developed and validated model to predict CI-AKI in elderly patients with STEMI, leveraging preoperative and intraoperative clinical variables. The model demonstrated robust predictive accuracy for identifying high-risk CI-AKI elderly patients and maintained strong performance in validation databases. To facilitate clinical translation, we designed an online dynamic nomogram clinically accessible nomogram that synthesizes key risk factors, enabling real-time risk stratification to support clinical decision-making. This tool advances personalized medicine by optimizing individualized risk prediction and therapeutic planning. We will further collect clinical patient data and refine the model to improve its predictive efficacy for better clinical treatment.
Ethic Approval
This study strictly followed the principles of the Declaration of Helsinki and was approved by the Ethics Committee of the Affiliated Hospital of Xuzhou Medical University (approval number: XYFY2022-KL122-01). Given the retrospective nature of the study, the medical records and data used were collected following routine medical procedures and privacy protection measures. All data were anonymized in the study and no personally identifiable information could be identified. The Ethics Committee concluded that the study would not pose additional risks or burdens to the participants and granted an exemption from the requirement for informed consent in accordance with relevant national laws and regulations as well as the institutional policy of Xuzhou Medical University. To comply with the relevant regulations, the author, Jingkun Jin, was certified by the Collaborative Institutional Training Initiative (CITI) and was authorized to access the MIMIC-IV database (ID: 13411060).
Acknowledgments
We thank the Xsmart Analysis Platform (https://www.xsmartanalysis.com/) for the analytical and visualization support provided in our research.
Funding
This study was supported by a grant from the Jiangsu Provincial Postgraduate Research Practice Innovation Project (No. SJCX25_1569).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Kilari S, Sharma A, Zhao C, et al. Identification of novel therapeutic targets for contrast induced acute kidney injury (CI-AKI): alpha blockers as a therapeutic strategy for CI-AKI. Transl Res. 2021;235:32–47. doi:10.1016/j.trsl.2021.03.005
2. Narula A, Mehran R, Weisz G, et al. Contrast-induced acute kidney injury after primary percutaneous coronary intervention: results from the HORIZONS-AMI substudy. Eur Heart J. 2014;35(23):1533–1540. doi:10.1093/eurheartj/ehu063
3. Yin WJ, Zhou LY, Li DY, et al. Protective effects of amlodipine pretreatment on contrast-induced acute kidney injury and overall survival in hypertensive patients. Front Pharmacol. 2020;11:44. doi:10.3389/fphar.2020.00044
4. Sau A, Pastika L, Sieliwonczyk E, et al. Artificial intelligence-enabled electrocardiogram for mortality and cardiovascular risk estimation: a model development and validation study. Lancet Digit Health. 2024;6(11):e791–e802. doi:10.1016/S2589-7500(24)00172-9
5. D CI-AKIC, Ponzo P, Risso A, et al. A prospective, multicenter, three-cohort study evaluating contrast-induced acute kidney injury (CI-AKI) in patients with cirrhosis. J Hepatol. 2024;80(1):62–72. doi:10.1016/j.jhep.2023.10.010
6. Zou Y, Lan J, Zhong Y, Yang S, Zhang H, Xie G. Association of remnant cholesterol with nonalcoholic fatty liver disease: a general population-based study. Lipids Health Dis. 2021;20:139. doi:10.1186/s12944-021-01573-y
7. González-Nicolás MÁ, González-Guerrero C, Goicoechea M, Boscá L, Valiño-Rivas L, Lázaro A. Biomarkers in contrast-induced acute kidney injury: towards a new perspective. Int J Mol Sci. 2024;25(6):3438. doi:10.3390/ijms25063438
8. Wang H, Gao T, Zhang R, et al. Neutrophil extracellular traps aggravate contrast-induced acute kidney injury by damaging glomeruli and peritubular capillaries. J Inflamm Res. 2023;16:5629–5646. doi:10.2147/JIR.S433110
9. Song L, Yao S, Zheng D, Xuan Y, Li W. Astaxanthin attenuates contrast-induced acute kidney injury in rats via ROS/NLRP3 inflammasome. Int Urol Nephrol. 2022;54(6):1355–1364. doi:10.1007/s11255-021-03015-1
10. Liu YH, Liu Y, Chen JY, et al. LDL cholesterol as a novel risk factor for contrast-induced acute kidney injury in patients undergoing percutaneous coronary intervention. Atherosclerosis. 2014;237(2):453–459. doi:10.1016/j.atherosclerosis.2014.10.022
11. Baum L, Ng MC, So WY, et al. Effect of hepatic lipase −514C->T polymorphism and its interactions with apolipoprotein C3 −482C->T and apolipoprotein E exon 4 polymorphisms on the risk of nephropathy in Chinese type 2 diabetic patients. Diabetes Care. 2005;28(7):1704–1709. doi:10.2337/diacare.28.7.1704
12. Zhang J, Wu Y, Zhang J, Zhang R, Wang Y, Liu F. ABCA1 deficiency-mediated glomerular cholesterol accumulation exacerbates glomerular endothelial injury and dysfunction in diabetic kidney disease. Metabolism. 2023;139:155377. doi:10.1016/j.metabol.2022.155377
13. Stürzebecher PE, Katzmann JL, Laufs U. What is ‘remnant cholesterol’? Eur Heart J. 2023;44(16):1446–1448. doi:10.1093/eurheartj/ehac783
14. Burnett JR, Hooper AJ, Hegele RA. Remnant cholesterol and atherosclerotic cardiovascular disease risk. J Am Coll Cardiol. 2020;76(23):2736–2739. doi:10.1016/j.jacc.2020.10.029
15. Quispe R, Martin SS, Michos ED, et al. Remnant cholesterol predicts cardiovascular disease beyond LDL and ApoB: a primary prevention study. Eur Heart J. 2021;42(42):4324–4332. doi:10.1093/eurheartj/ehab432
16. O’Hagan R, Berg AR, Hong CG, Parel PM, Mehta NN, Teague HL. Systemic consequences of abnormal cholesterol handling: interdependent pathways of inflammation and dyslipidemia. Front Immunol. 2022;13:972140. doi:10.3389/fimmu.2022.972140
17. Gowdak LHW. Atherosclerosis, inflammation, and genetics - and you thought it was just LDL-cholesterol. Arq Bras Cardiol. 2020;114(2):273–274. doi:10.36660/abc.20200038
18. Mandaliya H, Jones M, Oldmeadow C, Nordman II. Prognostic biomarkers in stage IV non-small cell lung cancer (NSCLC): neutrophil to lymphocyte ratio (NLR), lymphocyte to monocyte ratio (LMR), platelet to lymphocyte ratio (PLR) and advanced lung cancer inflammation index (ALI). Transl Lung Cancer Res. 2019;8(6):886–894. doi:10.21037/tlcr.2019.11.16
19. Yang X, Zhao S, Wang S, et al. Systemic inflammation indicators and risk of incident arrhythmias in 478,524 individuals: evidence from the UK Biobank cohort. BMC Med. 2023;21(1):76. doi:10.1186/s12916-023-02770-5
20. Jodeleit H, Milchram L, Soldo R, et al. Autoantibodies as diagnostic markers and potential drivers of inflammation in ulcerative colitis. PLOS ONE. 2020;15(2):e0228615. doi:10.1371/journal.pone.0228615
21. Chen W, Song X, Hong L, et al. The association between lymphocyte-monocyte ratio and postoperative acute kidney injury in patients with acute type A aortic dissection. J Cardiothorac Surg. 2022;17(1):60. doi:10.1186/s13019-022-01813-x
22. Marenzi G, Bartorelli AL. High urine output with matched hydration for CI-AKI prevention: “Salus Per Aquam” (Health Through Water). JACC Cardiovasc Interv. 2017;10(4):364–366. doi:10.1016/j.jcin.2016.12.269
23. Briguori C, Visconti G, Donahue M, et al. Renal guard system in high-risk patients for contrast-induced acute kidney injury. Am Heart J. 2016;173:67–76. doi:10.1016/j.ahj.2015.12.005
24. Putzu A, Boscolo Berto M, Belletti A, et al. Prevention of contrast-induced acute kidney injury by furosemide with matched hydration in patients undergoing interventional procedures: a systematic review and meta-analysis of randomized trials. JACC Cardiovasc Interv. 2017;10(4):355–363. doi:10.1016/j.jcin.2016.11.006
25. Ma K, Li J, Shen G, et al. Development and validation of a risk nomogram model for predicting contrast-induced acute kidney injury in patients with Non-ST-elevation acute coronary syndrome undergoing primary percutaneous coronary intervention. Clin Interv Aging. 2022;17:65–77. doi:10.2147/CIA.S349159
26. Zhu H, Shen Y, Wang G, Li Z, Qiu W. A predictive model for contrast-induced acute kidney injury after percutaneous coronary intervention in elderly patients with st-segment elevation myocardial infarction. Clin Interv Aging. 2023;18:453–465. doi:10.2147/CIA.S402408
27. Wang L, Xu Y, Zhang X, et al. The predictive value of SII combined with UHR for contrast-induced acute kidney injury in patients with acute myocardial infarction after percutaneous coronary intervention. J Inflamm Res. 2024;17:7005–7016. doi:10.2147/JIR.S482977
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Preprocedural SII Combined with High-Sensitivity C-Reactive Protein Predicts the Risk of Contrast-Induced Acute Kidney Injury in STEMI Patients Undergoing Percutaneous Coronary Intervention
Ma K, Qiu H, Zhu Y, Lu Y, Li W
Journal of Inflammation Research 2022, 15:3677-3687
Published Date: 25 June 2022
A Predictive Model for Contrast-Induced Acute Kidney Injury After Percutaneous Coronary Intervention in Elderly Patients with ST-Segment Elevation Myocardial Infarction
Qiu H, Zhu Y, Shen G, Wang Z, Li W
Clinical Interventions in Aging 2023, 18:453-465
Published Date: 22 March 2023
The Prognosis of Neutrophil-to-Lymphocyte Ratio and Lymphocyte-to-Monocyte Ratio in Elderly with Acute Ischemic Stroke
Wang J, Zhao Y, Lv C, Li F
Clinical Interventions in Aging 2024, 19:1715-1720
Published Date: 19 October 2024