Back to Journals » Psychology Research and Behavior Management » Volume 15
Development and Psychometric Properties of the Caregiver Burden Scale in Polish Caregivers of Stroke Patients
Authors Jaracz K ![]() , Grabowska-Fudala B
, Grabowska-Fudala B ![]() , Kleka P
, Kleka P ![]() , Tomczak M
, Tomczak M ![]() , Smelkowska A
, Smelkowska A ![]() , Pawlicka A
, Pawlicka A ![]() , Górna K
, Górna K
Received 20 November 2021
Accepted for publication 11 February 2022
Published 15 March 2022 Volume 2022:15 Pages 665—675
DOI https://doi.org/10.2147/PRBM.S348972
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Igor Elman
Krystyna Jaracz,1 Barbara Grabowska-Fudala,1 Paweł Kleka,2 Maciej Tomczak,3 Anna Smelkowska,1 Aleksandra Pawlicka,4 Krystyna Górna5
1Department of Neurological Nursing, Poznan University of Medical Sciences, Poznań, Poland; 2Faculty of Psychology and Cognitive Sciences, Adam Mickiewicz University, Poznań, Poland; 3Department of Psychology, Poznan University of Physical Education, Poznań, Poland; 4Independent Researcher, Bydgoszcz, Poland; 5Department of Psychiatric Nursing, Poznan University of Medical Sciences, Poznań, Poland
Correspondence: Krystyna Jaracz, Department of Neurological Nursing, Poznan University of Medical Sciences, Poznań, Poland, Tel + 48 618612267, Email [email protected]
Purpose: Most stroke patients require long-term care of their family members. Excessive care burden entails several negative consequences; therefore, the severity of the burden should be periodically assessed. For this purpose, valid multidimensional measures are needed. Our study, which is a part of a larger research project, aims to translate and evaluate the psychometric properties of the Polish Caregiver Burden Scale (CBS) in relation to construct validity and internal consistency in caregivers of the patients after stroke.
Patients and Methods: The sample of this cross-sectional observational study consisted of 366 informal caregivers to consecutive first-ever stroke survivors. The five-factor Polish CBS and the Hospital Anxiety and Depression Scale (HADS) were administered during the home visits at three to six months after patients’ hospitalisation. Exploratory (EFA), confirmatory (CFA) factor analyses and a net analysis were performed to investigate the internal structure and a factorial construct validity of the CBS. Correlation analyses between the CBS and the HADS were carried out to examine convergent validity. Cronbach’s alpha and item-total correlation were applied to assess internal consistency.
Results: Three out of five factors identified by EFA were similar to the original indices of the CBS, while the remaining two deviated from the original structure of the CBS. The CFA five-factor model represented an acceptable fit (confirmatory fit index, CFI = 0.96, root mean square error, RMSEA = 0.04) but only after a modification. All subscale scores of the CBS were positively correlated with the HADS, supporting the convergent validity. Cronbach’s alpha coefficients for the overall scale (0.92) and all subscales (0.72– 0.87) except one (0.69) and item-total correlation results indicated good internal consistency.
Conclusion: The Polish version of the CBS showed acceptable internal consistency and good convergent validity. Factorial validity and structural integrity were partially supported. The interrelationships between the CBS subdomains, their partial mutual contamination, and the scale’s non-orthogonal structure should be considered when interpreting the results of further studies using this version of the scale.
Keywords: stroke, caregiver burden, reliability, validity
Introduction
Despite a decline in global stroke incidence and mortality rates since the 1990s, the absolute number of new stroke cases, stroke survivors and people who remained disabled after stroke has almost doubled during the recent decades.1 In European countries, the above trend has been projected to increase by 27% between 2017 and 2047, mainly because of population ageing and the improvement in survival rates.2 For that reason, stroke is and will continue to be a major concern of public health, a source of high demands for long-term care, and a potential cause of caregiver burden for patients’ families and other informal carers.
After being discharged from an acute hospital or inpatient rehabilitation setting, most stroke patients return to their homes where they are cared for by their immediate family members, usually female spouses.3 This is also the case in Poland, where the cultural tradition, moral obligations and religious beliefs motivate families to take responsibility for their chronically ill, disabled and elderly relatives.4,5 The fact is, however, that a waste majority of caregivers, including those who assume the caregiving role suddenly, such as family caregivers to stroke patients, do not receive any professional training, while the support from formal care service is far insufficient.6–8 As a consequence, especially when the carer’s own resources are also limited, and the care demands are too high, a feeling of multifaceted strain or burden arises.9,10 This, in turn, leads to deterioration of physical and mental health, diminished quality of life, burnout syndrome, and lowering the caring potential of carers.11,12 Therefore, it is important to evaluate the caregiver burden, its severity, trajectory and determinants to identify the high-risk persons and assess the effectiveness of planned interventions aimed at assuaging the burden of caring. For these purposes, reliable and valid assessment tools are needed.
There are several instruments to measure the caregiving related consequences in conditions with a sudden onset, such as stroke, spinal cord injury, or amputation.13,14 However, only two of these were developed within the Western cultural background and were originally validated in the caregivers of stroke survivors;15,16 only one of them was designed as a multi-dimensional measure.16 This is the Caregiver Burden Scale (CBS), developed by Swedish researchers, as a modified version of the Oremark’s “ABS-A Next of Kin Load Scale for caregivers of chronic patients”. The original target population of the CBS were caregivers to stroke patients.16 The scale has five dimensions dealing with several aspects of subjective burden, including the caregiver’s health, physical exhaustion, emotional strain, social isolation, and environmental situation. The original CBS has satisfactory validity and reliability and currently is one of the most used tools measuring the burden imposed on the caregivers of the people after stroke. However, the scale has not been comprehensively analysed in this respect in Poland, yet.
Therefore, the present study aimed at developing and, particularly, at evaluating the psychometric properties of the Polish Caregiver Burden Scale, focusing on the construct validity and internal consistency in caregivers of patients after stroke. To the best of the authors’ knowledge, this has been the first non-English CBS validation study among informal carers of stroke survivors.
Materials and Methods
Design and Participants
This study is a part of a larger long-term project on the impact of stroke on stroke survivors and their caregivers, conducted in the Department of Nursing at the University of Medical Sciences in Poznan, Poland. A few studies were carried out within this project, and the results were demonstrated in other works.17–20 The participants of these studies constituted a study sample in the present work. All subjects were adult primary caregivers of consecutively admitted patients due to the first-ever stroke to stroke units in two multi-profile hospitals in Poznan (Wielkopolska region). They were recruited from family members or otherwise closely related persons who declared their direct involvement in the patient’s care at home. People who were simultaneously caring for other chronically ill persons and those who were professional or paid caregivers were not included. More details concerning the study participants can be found elsewhere.17–20 During the hospitalisation, the caregivers had been informed about the planned follow-up home visit for face to face interviews at 3 to 6 months after discharge. All the caregivers in the database, ie those who fulfilled the inclusion criteria and agreed to take part in the follow-up examination before the patient’s discharge from the acute hospital (n = 576), were attempted to contact by telephone or personally 3 to 6 months later. As a result, 526 were reached, of whom 366 were visited for the personal interview. One hundred and fifty participants dropped out for the following reasons: death of the patient, between discharge and the follow-up investigation (70 patients), patients being transferred to a long-term care institution (39 patients), refusal of further participation (20 caregivers), discontinuation of providing the care (1 caregiver), too long distance for the researchers to the participants’ current place of living to visit them at home (30), inability to determine the participants’ current location, despite several attempts (50 participants). Eventually, the analysis included 63.54% of the initial sample. The number of caregivers who were invited but refused to enter the study at the very beginning, ie during the patient’s hospitalisation, were not recorded.
Instruments
The Caregiver’s Burden Scale was designed by Elmståhl et al16 as a new measure for the assessment of the subjective caregiver burden. It has 22-items and five indices, ie dimensions or subscales extracted by the exploratory factor analysis: General strain (8 items), Isolation (3 items), Disappointment (5 items), Emotional involvement (3 items), and Environment (3 items). Each item is scored on a scale from 1 to 4 (not at all, seldom, sometimes, often). The subscale and total scores are calculated as a mean of the item scores on each subscale and the entire scale, respectively. The possible scores range from 1 to 4, with the higher scores indicating greater caregiver burden. The psychometric properties of the original CBS were examined in family caregivers to 150 patients with stroke or dementia, and to another 23 stroke patients. The results proved good construct validity, adequate internal consistency for all subscales (Cronbach’s α = 0.70–0.87), except for the Environment (α = 0.53), and excellent test – retest stability for all subscales (Cohen’s kappa = 0.89–1), except for the Environment (kappa = 0.53).16
The Polish language version of the instrument was developed after obtaining written consent from the leading developer of the CBS, with the attached original questionnaire, scoring instruction and formal permission to translate it into Polish and use it in the research. In the first step of the translation and cultural adaptation process, the English version was independently translated by two native Poles with a good knowledge of English. Then, the two versions were compared and consolidated into one preliminary Polish version. Afterwards, the preliminary version was translated back into English by another two Polish language professionals who had an excellent command of English. Then, an expert committee (three nurse researchers and translators) was involved in reaching a consensus on the results of all these versions. In the end, after some corrections and adjustments in the preliminary version, the final Polish version was accepted.
Additionally to the CBS, the participants completed the Hospital Anxiety and Depression Scale. This scale enables the measurement of psychological distress in terms of depression (seven items) and anxiety (seven items). Each item is scored on a scale of 0–3, with subscale scores ranging from 0 to 21.21
Sociodemographic and clinical data of patients and caregivers were obtained from medical records and semi-structured interviews. The patients’ functional state was assessed using the Barthel Index (BI, the modified 20 point version).22 There were no missing data in any questionnaires used, including the CBS. This was possible because all the data had been collected by the same two experienced researchers (B. G-F and A.S) during personal interviews at the participants’ homes, where any ambiguities that arose while completing the questionnaires were clarified on the spot.
Statistical Analysis
Descriptive statistics were used to describe the study sample, and they were presented as percentages, means, standard deviations (SDs), and ranges. The psychometric properties of the CBS were examined in relation to selected aspects of validity and reliability. The factorial construct validity, convergent validity and internal consistency were examined.
Factorial validity was assessed by means of the Exploratory Factor Analysis (EFS) and the Confirmatory Factor Analysis (CFA). EFA (with minimum residuals solution and Oblimin method for rotation) was applied to scrutinize the factor structure of the scale on the data collected in the Polish sample. CFA was conducted with ML estimator to confirm the original five-factor model. The following goodness-of-fit statistics were examined: χ2, χ2/df ratio, Root Mean Square Error of Approximation (RMSA), Standardised Root Mean Square Error of Residual (SRMR), Nonformed Fit Index (NNFI) and Comparative Fit Index (CFI). It was assumed that the values χ2/df ≤ 3, RMSA 0.05–0.08, SRMR 0.05–0.08, NNFI ≥ 0.90, and CFI > 0.90 indicate an acceptable fit of a model to the data.23 Supplementary to the factor analyses, a network analysis was performed in order to examine the relationships between the scale items descriptively.24
Convergent validity was investigated by correlation analysis between CBS and HADS. Since psychological distress and perceived caregiver burden are closely related concepts, relatively robust correlations between these two scales were expected.9,25
Internal consistency was evaluated with the help of the Cronbach’s alpha coefficient. Values exceeding 0.7 were considered as acceptable.26 The item-total correlation was also analysed. A value > 0.30 was deemed as indicating that the individual item correlates well with the scale and measures the same construct as the other items.25 Multicollinearity was examined using the inter- item correlation analysis and the Variance Inflation Factor (VIF). VIF values not exceeding 3 were considered as acceptable.27
Data were analysed using the Statistica 13 Package (StatSoft, Poland) and with the lavaan package in R, Version 4.0.2.28,29
Ethical Consideration
The study was approved by the Bioethics Committee at the University of Medical Sciences in Poznań (no.1365/05; 32/10; 283/12). All candidates for the study were informed about the study, and those who agreed to participate gave their informed written consent. The study was performed in accordance with the Helsinki Declaration and the principles of good clinical practice, with respect for the rights and dignity of participants.
Results
Participants
The caregiver’s sample consisted of 366 people with a mean age of 54.45 years. The majority were women (81.7%), and 56.6% were spouses of the patients. The average time spent on caregiving was 9.24 hours per day. The patient’s sample included 169 (46.2%) women and 197 men with a mean age of 66.4 years (Table 1). Half of them (n = 185; 50.6%) had moderate or severe dependency in ADL (< 10 BI points). The mean BI score was 12.72 (SD = 6.67).
 |
Table 1 Characteristics of the Caregivers and the Patients |
Factorial Construct Validity
Large values of the Bartlett test (chi2 (df 231) = 3780.747; p < 0.001) and the Kaiser – Meyer – Olkin measure (KMO = 0.92) indicated the existence of relationships between the test items that could be attributed to latent factors and showed that the data were suitable for EFA. The results of EFA with the assumed five-factor solution are given in Table 2. The obtained structure deviated, to some extent, from the theoretical assumptions. Three factors, ie factor 2 (orig. Isolation), 4 (orig. Emotional involvement), and 5 (orig. Environment), most strongly recreated the structure of the CBS. All items loaded on their originally constructed subscales, except for item EI2, which cross-loaded on factor 1 (orig. General strain).
 |
Table 2 Exploratory Factor Loadings of Items in CBS with Five Factors |
Regarding factor 3 (orig. Disappointment), two items (D1 and D2) loaded on their original factor, another two (D4 and D5) loaded strongly on factor 1 (org. General strain), and one item (D3) loaded weakly on factor 1 (General strain) and additionally on factor 2 (org. Isolation). This shows that the Disappointment subscale reproduced the original structure most poorly.
Factor 1 (orig. General strain), in turn, gathered loadings from the Disappointment and Emotional involvement subscales, but simultaneously items from that very factor loaded on other factors. Item GS1 loaded equivalently on factor 5, item GS2 on factor 3, item GS5 loaded strongly on factor 2 and cross-loaded on factor 3. Nevertheless, all items belonging to the General strain subscale were present in their original factor 1; however, two items (GS5 and GS8) had low loadings. The total cumulative variance explained by these five factors amounted to 41.4%.
The CFA was carried out in two stages. A comparison was made of a one-factor model with the five-factor model consistent with the original assumptions in the first stage. The second model differed significantly from the one-factor model (chi2 (10) = 322.9; p < 0.001); however, the fit statistics were not satisfactory (χ2/df = 3.641, RMSEA = 0.084, 90% CI (0.078–0.0916); SRMR = 0.066, = 0.898, CFI = 0.856). Therefore, based on the modification indices, four paths for residual correlations in the second stage of the analysis were freed. These concerned relationships of item GS1 with the three items in the Environment subscale and correlations between D1 and D2 in the Disappointment subscale. The modified model showed an adequate fit to the data (Figure 1), and this was significantly better in comparison to the model without error correlations (chi2 (4) = 190.5; p < 0.001). As displayed in Figure 1, strong and moderate correlations between the subscales can be attributed to the relationships between the individual items.
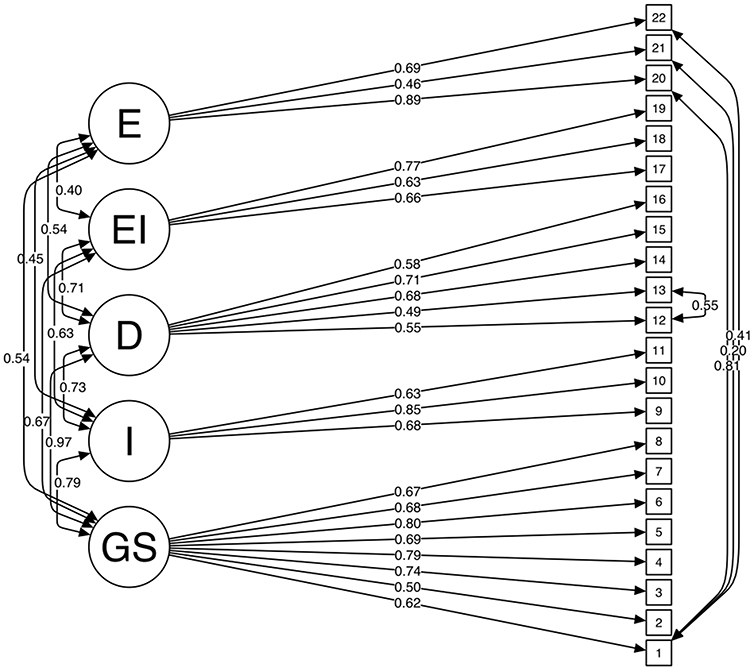 |
Figure 1 The result of the CFA of the final five-factor model with residual correlations. Fit measures: chi square (df 194) = 505.2, p = 0.001), chi square/df = 2.6, 1, RMSEA = 0.066, 90% CI (0.059–0.073); SRMR = 0.053, NNFI = 0.898, CFI = 0.915. Abbreviations: GS, General strain; I, Isolation; D, Disappointment; EI, Emotional involvement; E, Environment. Note: The items are numbered according to their order in the original subscales of the CBS. |
This is also shown in Figure 2, presenting the results of the net analysis. The network of mutual relationships between the items indicates distinct dimensions for the Isolation and Environment subscales only. Emotional involvement and Disappointment are not so homogeneous, and each of them seems to be divided into two subgroups. Some items in the General strain are associated with the items of the other subscales, except GS7, which is not related meaningfully enough (<0.13) to any other items, and GS3, GS5, and GS8, which are linked only to the items of their intended subscale. Such a structure of interrelationships revealed by the partial correlations analysis confirms the scale structure disturbances in relation to the original model revealed by the EFA.
 |
Figure 2 A network plot presenting the partial correlations between the Caregiver Burden Scale items. Abbreviations: GS, General strain; I, Isolation; D, Disappointment; EI, Emotional involvement; E, Environment. Notes: Blue lines indicate positive correlations, whilst red lines indicate negative correlations. The thickness of lines connecting the nodes is proportional to the strength of the relationships (partial correlation coefficients) between the CBS items (represented by circles). The range of relationships: 0.10–0.53. The items are numbered according to their order in the original subscales of the CBS. |
Convergent Validity
The CBS total and subscale scores positively correlated with the HADS scores (r = between 0.22 and 0.59) (Table 3).
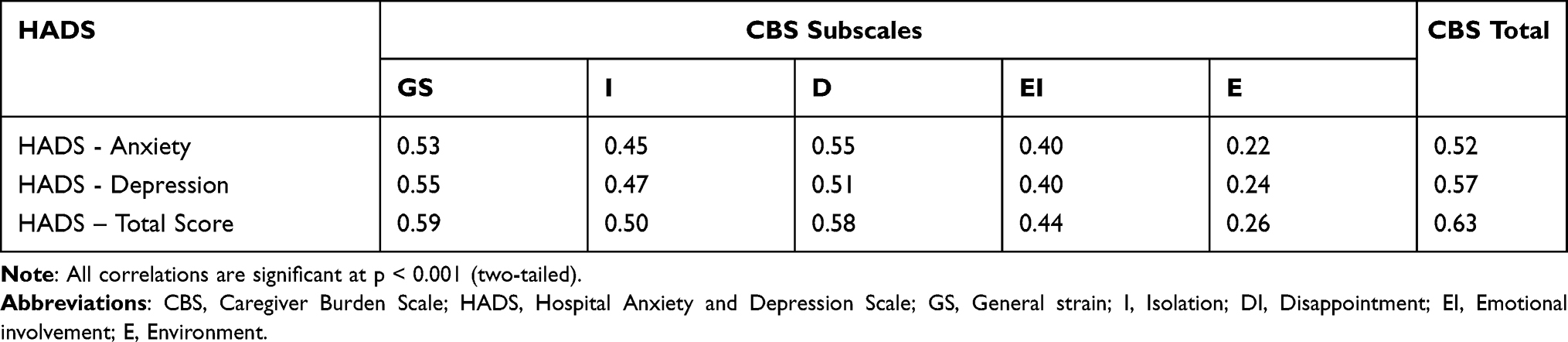 |
Table 3 Pearson Correlation Coefficients Between CBS and HADS Scores in Caregivers of Stroke Patients |
Internal Consistency Reliability
The Cronbach’s alpha coefficient for the overall scale was 0.923, and for the subscales it ranged from 0.726 to 0.875 demonstrating acceptable values, except for the Environment subscale where it was slightly lower (0.697). When individual items were deleted, α remained stable The item-total correlations were all positive and higher than 0.32, supporting the internal consistency of the scale (Table 4). The internal correlations between the different subscales according to the Pearson’s coefficient were all significant and ranged between 0.31 (Emotional involvement vs Environment) to 0.76 (General strain vs Disappointment). The item-item correlations were also positive and ranged from 0.04 (D2 vs E2) to 0.67 (GS4 vs GS6), with this latter being lower than the individual correlations between each of these two items and the total score (0.76 and 0.78, respectively). The VIF statistics ranged between 1.52 (GS2) - 2.70 (GS6), which met the criterion of the VIF < 3 threshold.
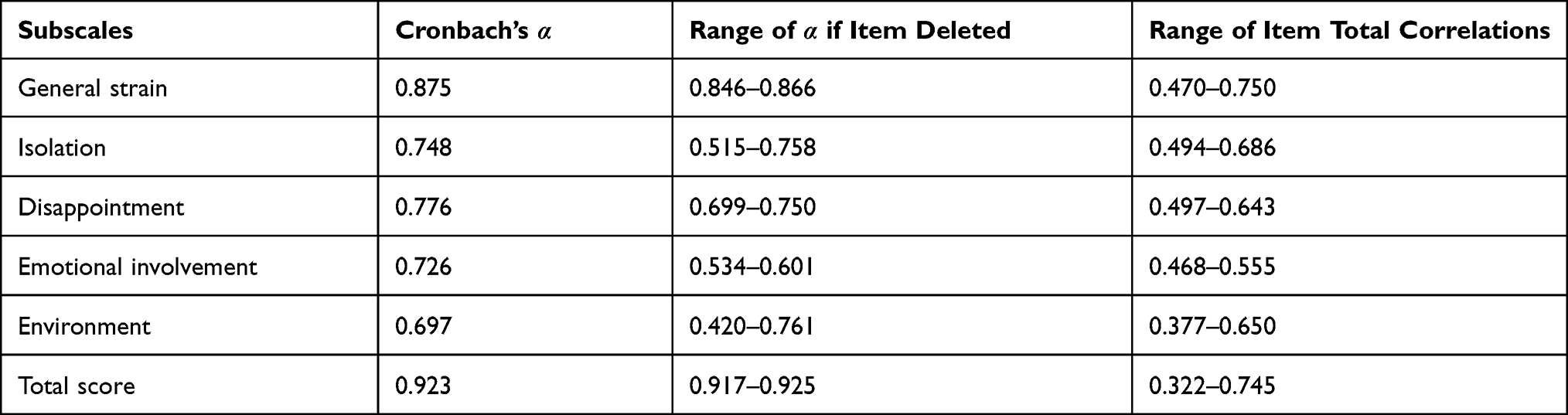 |
Table 4 Reliability Analyses of the Caregiver Burden Scale |
Discussion
The study aimed to evaluate the validity and reliability of the Polish language Caregiver Burden Scale in a sample of 366 caregivers of stroke patients. Since in Poland acute stroke, and post-hospital stroke care varies depending on the region,30 the caregivers’ experiences may also differ. Therefore, the findings were interpreted in the context of the study population.
The results partially confirmed the factorial structure of the scale. Three factors identified by EFA were similar to the original indices, and factor loading distribution on these factors supported the original names of the subscales (Emotional involvement, Environment and Isolation), assigned by the authors according to the items with the highest loadings.16
However, the remaining two factors, ie General strain and, in particular, Disappointment deviated from the authorial version of the instrument. Some items loaded or cross-loaded on factors other than their intended ones or had low factor loadings. For example, item D4 concerning physical tiredness, belonging to the Disappointment subscale, loaded on the General strain, on which other items concerning tiredness (GS4 and GS6) are originally located. Further, item D3 pertaining to loneliness and isolation (Do you feel lonely and isolated because of your relative’s problem?) loaded both on the General strain and the Isolation subscales, but the loadings were weak. These findings may indicate a lack of clear conceptual separateness of the factors, a partial overlap of their content or semantic similarities of some items.31 The similarities between the General strain and Disappointment factors were previously noted by Elmståhl et al32 in their study on caregiver burden among caregivers to persons from the general elderly population in Sweden. The above explanation may be additionally supported by the results of the net analysis that also showed a rather problematic structural integrity of the General strain and Disappointment subscales.
Further exploration of the factorial structure through the CFA showed that the five-factor model had a significant advantage of fitting to the data over the one-factor model, which confirms the reasonableness of extracting theoretically justified subscales within the CBS. However, the model required some modification to reach an acceptable fit to the data (CFI > 0.90, RMSEA < 0.08). By analysing the items for which the error correlations have been added, one can assume a partial content or conceptual overlap, and consequently shared measurement errors.33 The results of the EFA also seem to reflect this same problem (see item GS1).
Comparing the results with Iranian study findings showed that the Persian version of CBS for assessing burden among caregivers to patients with spinal cord injury, in general, supported the original model of the scale (CFI = 0.96, RMSEA = 0.04); however, low factor loadings (< 0.30) for two items (GS3 and E2) indicated the need for their modification.34 On the contrary, the Turkish validation study in caregivers of haemodialysis patients found a five-factor model fully acceptable (CFI = 0.96, RMSEA = 0.07).35 The findings of the present study could not be compared with other validation studies from European countries because there are no such reports, even though, as it has already been mentioned, the CBS is one of the most frequently used caregiver burden measure not only in observational, but also in clinical research.36–39
Referring to other aspects of construct validity, as expected, positive relationships were found between caregiver burden and emotional distress in terms of anxiety and depression, with the highest correlation between the HADS and the Strain and Disappointment subscales and the lowest with the Environmental subdomain. These findings are in line with the Iranian validation study demonstrating a similar pattern of correlations between the CBS and the Beck Depression Inventory.34 Other studies with the CBS also showed comparable results.40,41 All these data together confirm the convergent validity of the CBS.
Regarding reliability, the results obtained showed good internal consistency for four out of five subscales, where the Cronbach’s alphas reached the value above 0.70, which is consistent with the results of the English version of the scale (see the Methods section). A slightly lower coefficient for the Environment subdomain in this study is probably due to relatively weak correlations between the item E2 “do you worry about not taking care of your relative in a proper way” and the remaining two items (0.27 and 0.41, see also Figure 2). It can be accounted for by the fact that there is a lack of systematic procedures for post-discharge care in Poland, which in turn may result in varied knowledge in this area, and different experiences among individual caregivers. A small number of items in this subscale may also play a role. The Iranian authors, reporting alpha = 0.559 for the Environment subscale, came to similar conclusions.34 However, attention is drawn to the very high Cronbach’s alpha coefficient for the total scale, which might indicate that some items, as they currently stand, may be redundant,42 which seems to correspond to the results of the EFA and its interpretation (see Discussion, par. 2). Commenting on other results of the analyses that showed moderate and high correlation between the subscales, it can be concluded that the CBS subdomains are not independent of each other. This finding justified using the oblimin rotation method in EFA in the study.
The present study has some implications for the understanding of the overall burden and its measurement. Assuming that caregiver burden is a complex, multidimensional phenomenon and caregiving experiences are shaped by country-specific cultural peculiarities, family traditions, and societal changes over time43,44 the burden’s measures, which reflect the underlying latent construct, are also tied to these conditions. Our results that only partially confirmed the construct validity of the CBS seems to mirror this problem. Thus, as the construct and its understanding may vary depending on circumstances, the existing measures should be refined accordingly.
This is especially important when the measurement results are to be used to develop effective intervention programs aimed at mitigating the caregiver burden and consequently its personal, social and, less frequently evaluated, economic costs. The latter is regarded as a loss of productivity, informal care’s monetary value, and care-related expenditure. Depending on the country, the total economic cost is calculated differently, and thus it ranges from 10,635 € up to 24,000 € annually per caregiver of stroke patients.45,46 In the USA, the total economic costs of caregiver burden attributable to stroke were projected to increase from 30.5 billion dollars in 2015 to 66.3 in 2023.47 In the above context and given the need for further up–to–date research on caregiving,47 using psychometrically sound tools is of importance.
Limitations
The study has several limitations that should be taken into account. Firstly, only selected aspects of validity and reliability were examined. Due to a cross-sectional design, the repeatability of the measure administered on different occasions was not assessed. Secondly, the study lacked face validity analyses with the participation of the persons from the target population. Only an expert panel was involved. On the other hand, thanks to the presence of the experienced researchers, any doubts or ambiguities that arose while completing the CBS questionnaire could be clarified on the spot. However, it should be admitted that the frequency of these ambiguities and whether they repeatedly concerned specific questions were not recorded, and that might have been a source of valuable information. Thirdly, because of a limited number of participants, the measurement invariance of the CBS across gender was not examined, which would be important given cultural differences in social roles depending on gender.48 Fourthly, due to a consecutive sampling procedure applied and a relatively large dropout rate, the selection and recruitment bias cannot be ruled out, which threatens the generalizability of the results and indicates that its utility in various settings and other than caregivers of stroke patients populations require further investigation.
With these limitations in mind, the authors hope that the study extends the existing knowledge on psychometric properties of the CBS and broadens the field for further research as they agree with the belief of D.L. Streiner et al25 that construct validity is a continual task of seeing how the scale performs in a variety of situations.
Conclusion
The Polish version of the CBS showed acceptable internal consistency and good convergent validity of the CBS evaluating the burden in caregivers to stroke patients. Factorial validity and structural integrity were partially supported. Some deviations from the original factor structure of the scale do not preclude its use on the subscale levels. However, the interrelationships between the subdomains, partial mutual contamination, and the non – orthogonal structure should be considered when interpreting study results. Further research on the scale validity and conceptual clarity in different Polish and international samples are needed.
Acknowledgments
We would like to express our gratitude to Prof. Solve Elmståhl, Lund University, Sweden, for his kind permission to translate the Caregiver Burden Scale into Polish and to use it in our research. A part of this study was supported by a Polish Ministry of Science and Higher Education grant (number N404 073 32/2200).
Disclosure
No conflicts of interest for this work have been declared by the authors.
References
1. Krishnamurthi R, Ikeda T, Feigin VL. Global, regional and country-specific burden of ischaemic stroke, intracerebral haemorrhage and subarachnoid haemorrhage: a systematic analysis of the global burden of disease study 2017. Neuroepidemiology. 2020;54(2):171–179. doi:10.1159/000506396
2. Wafa HA, Wolfe CDA, Emmett E, Roth GA, Johnson CO, Wang Y. Burden of stroke in Europe: thirty-year projections of incidence, prevalence, deaths, and disability-adjusted life years. Stroke. 2020;51(8):2418–2427. doi:10.1161/STROKEAHA.120.029606
3. Han B, Haley WE. Family caregiving for patients with stroke review and analysis. Stroke. 1999;30(7):1478–1485. doi:10.1161/01.str.30.7.1478
4. Alber J, Köhler U. Health and Care in an Enlarged Europe (Report). Luxemburg: Office for Official Publications of the European Communities; 2004.
5. United Nations Economic Commission for Europe. The challenging roles of informal carers. UNECE policy brief on aging No. 22; 2019. Available from: https://unece.org/DAM/pau/age/Policy_briefs/ECE_WG1_31.pdf.
6. Di Rosa M, Kofahl C, McKee K, et al. A typology of caregiving situations and service use in family carers of older people in six European countries: the EUROFAMCARE study. GeroPsych. 2011;24(1):5–18. doi:10.1024/1662-9647/a000031
7. Camak DJ. Addressing the burden of stroke caregivers: a literature review. J Clin Nurs. 2015;24(17–18):2376–2382. doi:10.1111/jocn.12884
8. Chen L, Xiao LD, Chamberlain D, Newman P. Enablers and barriers in hospital-to-home transitional care for stroke survivors and caregivers: a systematic review. J Clin Nurs. 2021;30(19–20):2786–2807. doi:10.1111/jocn.15807
9. Liu Z, Heffernan C, Tan J. Caregiver burden: a concept analysis. Int J Nurs Sci. 2020;7(4):438–445. doi:10.1016/j.ijnss.2020.07.012
10. Lindt N, Van Berkel J, Mulder BC. Determinants of overburdening among informal carers: a systematic review. BMC Geriatr. 2020;20(1):304. doi:10.1186/s12877-020-01708-3
11. Gérain P, Zech E. Informal caregiver burnout? Development of a theoretical framework to understand the impact of caregiving. Front Psychol. 2019;31(10):1748. doi:10.3389/fpsyg.2019.01748
12. Revenson TA, Griva K, Luszczynska A, et al. Caregiving in the Illness Context. Palgrave Macmillan; 2016.
13. Visser-Meily JM, Post MWM, Riphagen II, Lindeman E. Measures used to assess burden among caregivers of stroke patients: a review. Clin Rehabil. 2004;18(6):601–623. doi:10.1191/0269215504cr776oa
14. Scholten EWM, Hillebregt CF, Ketelaar M, Visser-Meily JMA, Post MWM. Measures used to assess impact of providing care among informal caregivers of persons with stroke, spinal cord injury, or amputation: a systematic review. Disabil Rehabil. 2021;43(6):746–772. doi:10.1080/09638288.2019.1641847
15. Bakas T, Champion V. Development and psychometric testing of the Bakas caregiving outcomes scale. Nurs Res. 1999;48(5):250–259. doi:10.1097/00006199-199909000-00005
16. Elmståhl S, Malmberg B, Annerstedt L. Caregiver’s burden of patients 3 years after stroke assessed by a novel caregiver burden scale. Arch Phys Med Rehabil. 1996;77(2):177–182. doi:10.1016/S0003-9993(96)90164-1
17. Jaracz K, Grabowska-Fudala B, Górna K, Kozubski W. Caregiving burden and its determinants in Polish caregivers of stroke survivors. Arch Med Sci. 2014;10(5):941–950. doi:10.5114/AOMS.2014.46214
18. Jaracz K, Grabowska-Fudala B, Górna K, Jaracz J, Moczko J, Kozubski W. Burden in caregivers of long-term stroke survivors: prevalence and determinants at 6 months and 5 years after stroke. Patient Educ Couns. 2015;98(8):1011–1016. doi:10.1016/J.PEC.2015.04.008
19. Grabowska-Fudala B, Jaracz K, Górna K, et al. Depressive symptoms in stroke patients treated and non-treated with intravenous thrombolytic therapy: a 1-year follow-up study. J Neurol. 2018;265(8):1891–1899. doi:10.1007/s00415-018-8938-0
20. Smelkowska A. Jakość Życia, Potrzeby i Obciążenie Opiekunów Chorych po Udarze Mózgu [Eng. Quality of Life, Needs and Burden among Caregivers of Stroke Patients] [unpublished dissertation]. Poznan University of Medical Sciences; 2019.
21. Zigmond AS, Snaith RP. The hospital anxiety and depression scale. Acta Psychiatr Scand. 1983;67(6):361–370. doi:10.1111/j.1600-0447.1983.tb09716.x
22. Wade DT, Hewer RL. Functional abilities after stroke: measurement, natural history and prognosis. J Neurol Neurosurg Psychiatry. 1987;50(2):177–182. doi:10.1136/jnnp.50.2.177
23. Pituch KA, Stevens JP. Applied Multivariate Statistics for the Social Sciences: Analyses with SAS and IBM’s SPSS.
24. Kossakowski JJ, Epskamp S, Kieffer JM, van Borkulo CD, Rhemtulla M, Borsboom D. The application of a network approach to Health-Related Quality of Life (HRQoL): introducing a new method for assessing HRQoL in healthy adults and cancer patients. Qual Life Res. 2016;25(4):781–792. doi:10.1007/s11136-015-1127-z
25. Streiner DL, Norman GR, Cairney J. Health Measurement Scales: A Practical Guide to Their Development and Use.
26. Hays RD, Anderson R, Revicki D. Psychometric considerations in evaluating health-related quality of life measures. Qual Life Res. 1993;2(6):441–449. doi:10.1007/BF00422218
27. Hair JF, Black WC, Babin BJ, Anderson RE. An Multivariate Data Analysis. Pearson Education Limited; 2009.
28. Rosseel Y. Lavaan: an R package for structural equation modeling. J Stat Softw. 2012;48(2):11–36. doi:10.18637/jss.v048.i02
29. Team RC. R: a language and environment for statistical computing. R Foundation for Statistical Computing; 2020. Available from: https://www.r-project.org/.
30. Maluchnik M, Ryglewicz D, Sienkiewicz-Jarosz H, et al. Differences in acute ischaemic stroke care in Poland: analysis of claims database of National Health Fund in 2017. Polish J Neurol Neurosurg. 2020;(5):449–455. doi:10.5603/PJNNS.a2020.0066
31. Worthington RL, Whittaker TA. Scale development research: a content analysis and recommendations for best practices. Couns Psychol. 2006;34(6):806–838. doi:10.1177/0011000006288127
32. Elmståhl S, Dahlrup B, Ekström H, Nordell E. The association between medical diagnosis and caregiver burden: a cross-sectional study of recipients of informal support and caregivers from the general population study ‘Good Aging in Skåne’, Sweden. Aging Clin Exp Res. 2018;30(9):1023–1032. doi:10.1007/s40520-017-0870-0
33. Byrne BM. Structural Equation Modeling with AMOS: Basic Concepts, Applications, and Programming, Second Edition.
34. Farajzadeh A, Akbarfahimi M, Maroufizadeh S, Rostami HR, Kohan AH. Psychometric properties of Persian version of the Caregiver Burden Scale in Iranian caregivers of patients with spinal cord injury. Disabil Rehabil. 2018;40(3):367–372. doi:10.1080/09638288.2016.1258738
35. Cil Akinci A, Pinar R. Validity and reliability of Turkish caregiver burden scale among family caregivers of haemodialysis patients. J Clin Nurs. 2014;23(3–4):352–360. doi:10.1111/j.1365-2702.2012.04235.x
36. Ford GA, Bhakta BB, Cozens A, et al. Safety and efficacy of co-careldopa as an add-on therapy to occupational and physical therapy in patients after stroke (DARS): a randomised, double-blind, placebo-controlled trial. Lancet Neurol. 2019;18(6):530–538. doi:10.1016/S1474-4422(19)30147-4
37. Eriksson GM, Kamwesiga JT, Guidetti S. The everyday life situation of caregivers to family members who have had a stroke and received the rehabilitation intervention F@ce in Uganda. Arch Public Health. 2021;79(1):100. doi:10.1186/s13690-021-00618-z
38. Simpson GK, Anderson MI, Daher M, Jones KF, Morey P. Testing a model of resilience in family members of relatives with traumatic brain injury vs spinal cord injury: multigroup analysis. Arch Phys Med Rehabil. 2021;102(12):2325-2334. doi:10.1016/j.apmr.2021.06.016
39. Caap-Ahlgren M, Dehlin O. Factors of importance to the caregiver burden experienced by family caregivers of Parkinson’s disease patients. Aging Clin Exp Res. 2002;14(5):371–377. doi:10.1007/BF03324464
40. Ågren S, Evangelista L, Strömberg A. Do partners of patients with chronic heart failure experience caregiver burden? Eur J Cardiovasc Nurs. 2010;9(4):254–262. doi:10.1016/j.ejcnurse.2010.03.001
41. Pudelewicz A, Talarska D, Bączyk G. Burden of caregivers of patients with Alzheimer’s disease. Scand J Caring Sci. 2019;33(2):336–341. doi:10.1111/scs.12626
42. Tavakol M, Dennick R. Making sense of Cronbach’s alpha. Int J Med Educ. 2011;2:53–55. doi:10.5116/ijme.4dfb.8dfd
43. Ożegalska-Łukasik N. Redefining and elderly caregiving in the 21st century China and Poland. In: Joanna W, editor. China - Central and Eastern Europe Cross-Cultural Dialogue Society, Business and Education in Transition. Jagiellonian University Press; 2016:47–62. Available from: https://www.cambridge.org/core/product/370C1D24F2C72FABBBBDA2995C5361AF.
44. Chakrabarti S. Cultural aspects of caregiver burden in psychiatric disorders. World J Psychiatry. 2013;3(4):85–92. doi:10.5498/wjp.v3.i4.85
45. Albrecht D, Wollensak T, Ernst C, Becker C, Hautzinger M, Pfeiffer K. Costs of informal care in a sample of German geriatric stroke survivors. Eur J Ageing. 2015;13(1):49–61. doi:10.1007/s10433-015-0356-x
46. Barral M, Rabier H, Termoz A, et al. Patients’ productivity losses and informal care costs related to ischemic stroke: a French population-based study. Eur J Neurol. 2021;28(2):548–557. doi:10.1111/ene.14585
47. Dunbar SB, Khavjou OA, Bakas T, et al. Projected costs of informal caregiving for cardiovascular disease: 2015 to 2035: a policy statement from the American Heart Association. Circulation. 2018;137(19):e558–e577. doi:10.1161/CIR.0000000000000570
48. Zygouri I, Cowdell F, Ploumis A, Gouva M, Mantzoukas S. Gendered experiences of providing informal care for older people: a systematic review and thematic synthesis. BMC Health Serv Res. 2021;21(1):730. doi:10.1186/s12913-021-06736-2
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.