Back to Journals » International Journal of Chronic Obstructive Pulmonary Disease » Volume 20
Development and Psychometric Evaluation of an Instrument to Assess Physical Activity Participation Behavior Among Chinese Patients with Chronic Obstructive Pulmonary Disease
Authors Liao Y ![]() , Wang H, Zhan Y, Liu Y, Wang W, Ke H, Lan F, Zhi Q, Li W, Yu J
, Wang H, Zhan Y, Liu Y, Wang W, Ke H, Lan F, Zhi Q, Li W, Yu J
Received 8 December 2024
Accepted for publication 17 April 2025
Published 30 April 2025 Volume 2025:20 Pages 1321—1334
DOI https://doi.org/10.2147/COPD.S511061
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Richard Russell
Yuanyu Liao,1,2,* Huan Wang,3,* Yuxin Zhan,3 Yunfang Liu,4 Weiwei Wang,5 Hui Ke,6 Fenfen Lan,2 Qiongge Zhi,2 Wang Li,2 Jiaohua Yu1
1Department of Nursing, Union Hospital, Tongji Medical College, Huazhong University of Science and Technology, Wuhan, Hubei, People’s Republic of China; 2School of Nursing, Tongji Medical College, Huazhong University of Science and Technology, Wuhan, Hubei, People’s Republic of China; 3Department of Neurosurgery, Union Hospital, Tongji Medical College, Huazhong University of Science and Technology, Wuhan, Hubei, People’s Republic of China; 4Department of Thoracic Surgery, Union Hospital, Tongji Medical College, Huazhong University of Science and Technology, Wuhan, Hubei, People’s Republic of China; 5Department of Gastrointestinal Surgery, Union Hospital, Tongji Medical College, Huazhong University of Science and Technology, Wuhan, Hubei, People’s Republic of China; 6Department of Wound Care Center, Union Hospital, Tongji Medical College, Huazhong University of Science and Technology, Wuhan, Hubei, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Jiaohua Yu, Department of Nursing, Union Hospital, Tongji Medical College, Huazhong University of Science and Technology, 1277 Jiefang Avenue, Wuhan, Hubei, 430022, People’s Republic of China, Email [email protected]
Purpose: This study aimed to develop and evaluate a psychometrically reliable tool specifically designed to assess physical activity participation behavior in COPD patients in China.
Patients and Methods: Using the Motivation-Opportunity-Ability (MOA) model as a framework, a scale was developed and evaluated through literature and guideline reviews, qualitative research, interdisciplinary expert consultations (n=21), and a pilot trial (n=50). A sample of COPD patients diagnosed over a year was randomly divided into two groups for exploratory factor analysis (EFA) and confirmatory factor analysis (CFA) to test the factor structure. The scale’s content validity, internal consistency and test-retest reliability were further assessed.
Results: 433 COPD patients from four hospitals in a city in China participated in this study. The final scale included 32 items and demonstrated good internal consistency, with a Cronbach’s α of 0.956 and a test-retest reliability of 0.777. The EFA identified four dimensions, with factor loadings ranging from 0.530 to 0.799, explaining 60.338% of the total variance: Motivation (5 items), Opportunity (12 items), Ability (9 items), and Behavior (6 items). The CFA confirmed that the four-dimensional model fit the data well: χ²/df = 1.891, standardized root mean residual (SRMR) = 0.0497, root mean square error of approximation (RMSEA) = 0.064, comparative fit index (CFI) = 0.927, Tucker-Lewis index (TLI) = 0.921.
Conclusion: The Physical Activity Participation Behavior Scale for COPD patients demonstrated good reliability and validity and can be used to assess physical activity participation in individuals with COPD.
Keywords: COPD, instrument, reliability, validity
Introduction
Chronic Obstructive Pulmonary Disease (COPD) is currently one of the top three leading causes of death globally. In China, the overall prevalence rate is 8.6%, with a higher rate of 13.7% in individuals aged 40 and above. The total number of COPD patients is nearly 100 million, with more than 27.0% of those aged 60 and above affected. Annually, 5 to 11 million people are disabled due to COPD.1 COPD patients typically experience symptoms such as dyspnea, shortness of breath, cough, and sputum production. Dyspnea contributes to inactivity, reduced physical fitness, impaired cardiovascular function, muscle wasting, social isolation, and depression. A sedentary lifestyle exacerbates dyspnea, leading to further inactivity, immobility, and premature death, thereby creating a vicious cycle of physical decline.2
The BMJ Best Practice guidelines recommend that all COPD patients engage in physical activity (PA).3 In 1985, Caspersen et al defined physical activity as any bodily movement produced by skeletal muscles that requires energy expenditure, including sports, household chores, recreational activities, and occupational tasks.4 Since then, the issue of physical activity participation has garnered extensive global attention and research. Physical activity is traditionally categorized by type, intensity, and duration. It has been shown to significantly improve the quality of life and prognosis for patients, with exercise training being a structured, planned, and repetitive form of physical activity.4 As such, physical activity includes not only structured exercise programs, such as pulmonary rehabilitation, but also everyday physical tasks. However, the 2024 Global Initiative for Chronic Obstructive Lung Disease (GOLD) guidelines indicate that COPD patients still face significant challenges in promoting and maintaining physical activity. Incorporating regular exercise into daily life is especially difficult, with dyspnea serving as a major barrier.2
There is no consistent definition of physical activity participation behavior in COPD patients. A clear definition would facilitate a more accurate assessment of participation levels in physical activity. Lee’s research team defined physical activity participation in COPD patients based on activity habits, weekly frequency, and duration.5 A protocol for a systematic review included several factors for assessing behavior change in community-dwelling COPD patients, including physical activity participation, sedentary time, daily steps, dyspnea perception, functional capacity, quality of life, exercise capacity, adverse events, and adherence to interventions.6 COPD patients frequently experience “kinesiophobia”, or an irrational fear of movement due to dyspnea, leading them to avoid activities associated with breathlessness or compensate by reducing activity intensity.7 Therefore, addressing exercise-related fear should be a key focus when promoting physical activity in COPD patients. Additionally, a best-evidence summary from China indicates that COPD patients’ physical activity should include: pre-activity risk and intensity assessments, the development of exercise prescriptions incorporating aerobic, resistance, balance, and flexibility training, and flexible adjustments to activity duration and intensity for elderly, frail, sedentary, stable, or acutely exacerbated COPD patients, as well as those who are obese or underweight. It also emphasizes selecting appropriate activity settings to ensure safety and effectiveness, using behavior change techniques to increase activity, and evaluating the efficacy and quality of interventions.8 In conclusion, we propose that physical activity participation behavior in COPD patients involves the intensity and duration of activities such as self-care, household chores, transportation, occupational tasks, and exercise, influenced by factors including disease, psychological state, and environment.9 It also encompasses specific lifestyle elements related to physical activity, such as activity planning, safety management, communication, and quality control.
It is important to note that there is currently no comprehensive standard for assessing the physical activity participation behavior of patients with COPD. Numerous studies have utilized activity monitors, such as pedometers and accelerometers, to objectively measure and provide feedback on COPD patients’ daily steps or energy expenditure.10–14 However, these devices are associated with costs and can be affected by factors such as low battery, signal interference, improper placement, or device detachment, resulting in data inaccuracies or omissions. Other studies have used generic tools, including the International Physical Activity Questionnaire-Short Form (IPAQ-SF),15–17 the International Physical Activity Questionnaire (IPAQ),18,19 the Physical Activity Scale for the Elderly (PASE),20 the Short Questionnaire to Assess Health-Enhancing Physical Activity (SQUASH),21 and the Yale Physical Activity Survey (YPAS),22 to subjectively evaluate the physical activity levels of COPD patients. However, these tools do not fully consider the unique physiological and behavioral characteristics of COPD patients. Furthermore, they only provide data on activity frequency, duration, and intensity for the past week or year, which limits their ability to sensitively, accurately, and comprehensively capture COPD patients’ physical activity participation behavior. The research team led by Koreny employed the PROactive Physical Activity in COPD (C-PPAC) instrument to assess activity levels, difficulty, and overall experience over the past week.23 However, this tool lacks an evaluation of activity types such as self-care, resistance training, balance, and the safety of participation. Amorim et al applied the London Chest Activity of Daily Living (LCADL) scale to assess impairments in COPD patients’ ability to perform personal care, household tasks, physical activities, and leisure activities but did not explore the underlying causes of participation behavior.24 Therefore, there is a clear need for reliable, theoretically driven instruments to measure the physical activity participation behavior of COPD patients and to regularly assess their activity levels to enhance the effectiveness of related interventions.
To address this need, we developed a scale specifically for COPD patients based on the Motivation, Opportunity, and Ability (MOA) model. Proposed by MacInnis et al in 1991,25 this model has a robust theoretical framework for understanding behavior change and has been applied in recent years to explain a variety of complex behaviors.26,27 The MOA model posits that motivation directly influences behavior, while ability and opportunity moderate this relationship.28 In this study, the four core components of the MOA model were defined as follows: motivation—the internal drivers and direct influences that prompt COPD patients to engage in physical activity, including their willingness, interest, and desire; opportunity—the external, objective components of the environment that COPD patients perceive as facilitating or hindering their physical activity participation; ability—the internal capacity that affects the quality and quantity of physical activity participation, such as the mastery of specific skills; and behavior—the intensity and duration of COPD patients’ direct engagement in physical activity under the influence of both internal and external stimuli, as well as related lifestyle behaviors.
The initial development of this scale involved reviewing relevant guidelines and existing literature,29–31 synthesizing the results of qualitative studies on 17 COPD patients,32 and conducting group discussions to create the initial 41-item scale. After three rounds of expert review by 21 specialists, consensus was reached. The scale was further refined through a pilot trial and cognitive interviews to improve clarity and accuracy, resulting in a preliminary 38-item scale. This tool addresses the lack of specificity in generic modules by capturing aspects unique to COPD, such as related symptoms and psychological factors. In this paper, we describe the development process and further validate its reliability and validity in a sample of Chinese COPD patients. Our assessment tool will be instrumental in guiding the development and evaluation of future interventions aimed at improving the quality of life for COPD patients and reducing premature mortality.
Materials and Methods
Study Design
This methodological study was designed and reported following the COSMIN Study Design checklist for Patient-reported outcome measurement instruments.33
Participants
Participants were recruited from June 1, 2024, to September 30, 2024, at three large tertiary hospitals and one general tertiary hospital in Wuhan, Hubei Province, China, including both outpatient and inpatient departments. The inclusion criteria were: (1) a diagnosis of COPD based on the 2024 GOLD criteria,2 with a diagnosis duration of at least one year; (2) age ≥18 years; (3) clear consciousness and ability to articulate thoughts; and (4) voluntary participation with informed consent. Exclusion criteria included: (1) concurrent heart, liver, kidney, or other organ failure, or any life-threatening disease; (2) severe cognitive impairment, communication disorders, or psychiatric conditions; and (3) severely impaired functional status requiring full dependency on care.
Scale Development
From December 2023 to May 2024, 21 experts in respiratory medicine, nursing, rehabilitation, clinical psychology, and physical therapy were invited to participate via email, letters, and WeChat, based on the following criteria: (1) a minimum of a bachelor’s degree or intermediate professional title; (2) at least 10 years of experience in the relevant fields; and (3) familiarity with questionnaire development, with a willingness to participate under informed consent. The experts, aged between 34 and 60 years (mean 44.71±7.52), consisted of 6 with doctoral degrees, 7 with master’s degrees, and 8 with bachelor’s degrees. They represented nine cities from Hubei, Jiangsu, Beijing, Guangdong, Fujian, Shandong, and Hainan provinces. Regarding professional settings, 17 were from medical institutions, 3 from academic institutions, and 1 from a research institute. Concerning professional titles, 3 held senior positions, 10 held associate senior positions, and 8 held intermediate-level titles. Their areas of expertise included clinical respiratory medicine (n=3), clinical respiratory nursing (n=4), nursing management (n=6), nursing psychology (n=3), rehabilitation nursing (n=2), chronic disease management (n=2), and physical therapy (n=1). Their years of experience ranged from 10 to 41 years (mean 21.57±9.21).
Following the first round of expert consultation, several adjustments were made: (1) After group discussion, four items were deleted, and seven items were merged. For example, the items “I feel that receiving health education resources during hospitalization promoted my activity” and “I feel that receiving guidance from healthcare staff before discharge promoted my activity” were merged, as two experts deemed them similar in meaning. Items for which deletion was suggested by only a few experts were modified to better align with the intended measurement goals. For instance, the item “I feel that transportation promotes my activity” was revised to “Choosing walking, cycling, or other active modes of transportation has enhanced my physical activity” after an expert suggested it reflected inactivity. (2) Thirteen items were descriptively modified, and 1 new dimension and 13 additional items were added. For example, the item “I participate in activities because I know their importance” was revised to “The desire to alleviate dyspnea”, based on expert feedback for more specific symptom-related descriptions. Additionally, the item “The aim is to reduce fatigue” was added. A new “Behavior” dimension was recommended to capture both structured exercise programs and daily activity patterns. Based on a literature review, group discussions, and informal expert interviews, 3 items (B1, B2, B3) were added. Following the second round of consultation, four items were deleted, one was merged, and four were reworded to clarify meaning. In the third round, two additional items were revised. After three rounds of expert consultations, the ratings of the importance of all remaining items became stable and consistent. The final scale consists of 38 items across four dimensions: Motivation (7 items), Opportunity (13 items), Ability (10 items), and Behavior (8 items).
A pilot test of the Chinese version of the questionnaire was conducted with 50 participants. The Chinese-language paper questionnaire was introduced to assess whether each item was easy to understand and complete, and to determine how long it took to complete the questionnaire. Additionally, cognitive interviews were conducted with 12 representative participants. The interview questions included: (1) Were any questions difficult to understand or answer? (2) Were any questions unclear, and should the wording be revised? How should they be modified? (3) Were any questions missing? All participants completed the questionnaire within 12 minutes (average time: 7.38 minutes), and the response rate was 100%.
Data Collection
The appropriate sample size should be 5–10 times the number of items,34 and considering exploratory factor analysis (EFA) and confirmatory factor analysis (CFA) splitting, the total sample size should be 10–20 times the number of items. Therefore, a minimum of 380 participants was required. To account for a refusal rate of over 10%, the sample size was increased to at least 418. The survey was administered by five graduate students from the research team. Before data collection, group discussions and unified training were conducted, and the survey plan was revised. Each Likert scale item was set to have equidistant response options, with the midpoint representing a “neutral” stance, to minimize potential data loss and bias.35 Participants were selected based on strict adherence to inclusion and exclusion criteria during the survey. A standardized Chinese script was used to introduce the background, objectives, significance, risk control measures, and instructions for completing the questionnaire to COPD patients. Following their consent, informed consent forms were provided. Chinese-language paper questionnaires were distributed on-site, and participants were required to complete them independently. Immediate assistance was provided to address any questions raised by patients. For those unable to complete it alone, such as elderly participants, the surveyor assisted by reading the items aloud. Questionnaires were collected and checked for completeness, with missing items being completed on-site. Invalid questionnaires with patterned responses were excluded. A follow-up survey was conducted one week later to assess test-retest reliability. Once the target sample size was reached, further invitations were discontinued. The one-week interval minimized potential behavioral changes and dropout rates. The data were entered by two graduate students and were subjected to logical and consistency checks to ensure accuracy.
The present study recruited 471 participants, excluding invalid and missing samples, resulting in 433 valid responses, yielding a response rate of 91.93%. The complete sample was randomly divided into two subsamples: Sample 1 (n=214) was used for item reduction, reliability testing, and EFA to structure the model, while Sample 2 (n=219) was used for CFA to validate the model. Demographic data, including age, gender, residence, marital status, living conditions, and educational background, were collected. Participants were required to complete a revised 38-item questionnaire. Each item employed a 5-point Likert scale, with options ranging from “Strongly Disagree” to “Strongly Agree”, scored from 1 to 5. For the motivation dimension, the total score ranged from 7 to 35, with higher scores indicating stronger motivation for engaging in physical activity. For the opportunity dimension, scores ranged from 13 to 65, with higher scores reflecting greater opportunities for physical activity participation. For the capability dimension, scores ranged from 10 to 50, with higher scores indicating stronger skills or confidence in engaging in physical activity. For the behavior dimension, scores ranged from 8 to 40, with higher scores indicating more proactive involvement in physical activities. The average time to complete the questionnaire was between 5 and 15 minutes. Upon successful submission of the responses, participants were provided with health education counseling.
Data Analysis
IBM SPSS Statistics V.26 and IBM SPSS Amos V.26 were employed for item analysis, reliability testing, EFA, and CFA.
Item analysis was conducted, and items were excluded if: (1) the first round questionnaires were ranked by their total scores, and participants in the top 27% (high-score group) and bottom 27% (low-score group) were identified. An independent samples t-test was performed, revealing no statistical difference between the two groups; (2) the correlation coefficient between an item and the total score was below 0.30, or (3) the Cronbach’s alpha of the corresponding dimension significantly increased upon exclusion of the item.36
Content validity indices were calculated based on expert ratings of the scale items: the Scale-level Content Validity Index (S-CVI) and the Item-level Content Validity Index (I-CVI). The S-CVI was computed as the mean inter-expert agreement for the entire scale. A scale was considered to have adequate content validity if S-CVI ≥ 0.90 and I-CVI ≥ 0.78.37
Before factor analysis, the Kaiser-Meyer-Olkin (KMO) measure and Bartlett’s test of sphericity were used to assess the suitability of the data for factor analysis.36 A KMO value exceeding 0.80 and a significant Bartlett’s test indicated appropriate conditions for factor analysis. EFA was then conducted on Sample 1 using rotated principal component factor analysis to explore the factor structure. Factors were retained based on two criteria: (1) eigenvalues greater than 1 and (2) factor loadings greater than 0.50. CFA was performed on Sample 2 to further validate the factor structure identified in the EFA. Model fit was evaluated using several indices: relative χ² (χ²/df) < 3, standardized root mean residual (SRMR) < 0.05, root mean square error of approximation (RMSEA) < 0.08, and comparative fit index (CFI) and Tucker-Lewis index (TLI) ≥ 0.90.38
Reliability was assessed using Cronbach’s α coefficient and test-retest reliability, with Cronbach’s α > 0.80 considered indicative of good reliability.39 Test-retest reliability of the full scale and its subscales was evaluated using the intraclass correlation coefficient (ICC) based on a two-way mixed model. ICC values of 0.40–0.59, 0.60–0.74, and ≥ 0.75 were categorized as fair, good, and excellent, respectively.40
Results
Sample Characteristics
The characteristics of the participants are summarized in Table 1. The mean age of the participants was 70.31 ± 8.63 years, with an average duration of diagnosis of 6.74 ± 6.75 years. The majority were male (81.8%), resided in urban areas (62.6%), were married (89.4%), and lived with their spouses (79.0%). The predominant educational level was middle school (32.8%), and most participants were covered by urban-rural resident medical insurance (31.6%). A significant proportion were in a stable disease phase (60.5%) and had been hospitalized 1 to 3 times due to exacerbations in the past year (85.2%). Nearly 40% had never smoked (39.7%), and more than half had 1 to 2 comorbidities (52.0%).
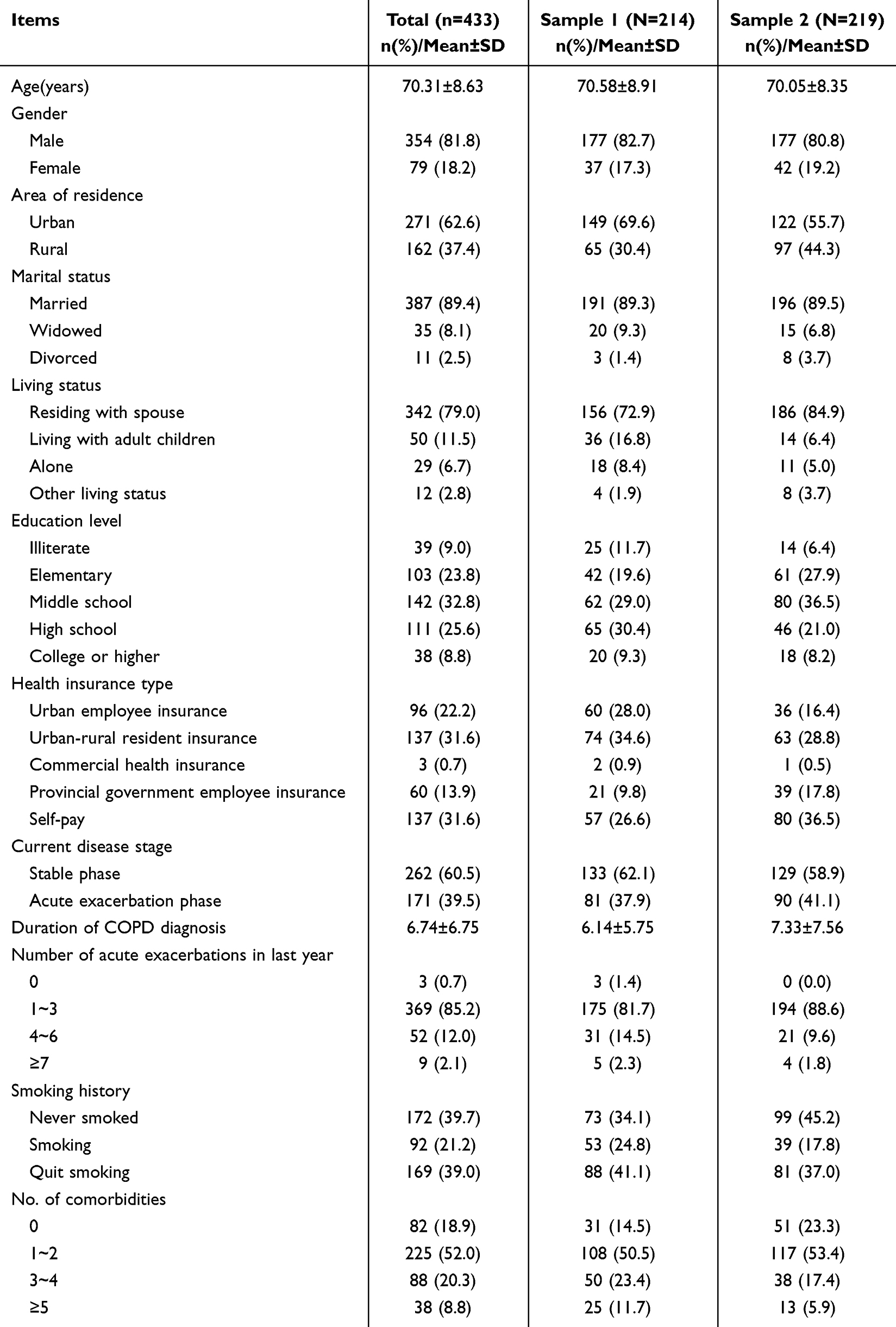 |
Table 1 General Characteristics of Participants (n=433) |
Item Analysis
The 214 questionnaires were ranked in ascending order based on total scores. Two groups were then established: individuals with scores ≤100 were classified in the low-score group, and those with scores ≥123 were classified in the high-score group. An independent samples t-tests indicated that one item (O1: “I experience increased activity during professional duties”) had a cutoff value <3, with a p-value > 0.05. After removing this item, significant differences were observed in the scores of the remaining items between the high- and low-score groups (t = 3.529 to 15.693, all p ≤ 0.001), demonstrating strong discriminative power. Another item (M6: “The confidence and belief in achieving personal goals”) showed a correlation with the total score <0.3. Following its removal, the correlation coefficient (r) ranged from 0.303 to 0.770, with all p-values <0.001, reflecting high homogeneity. Removal of four items (M7, A10, B7, B8) led to a significant increase in Cronbach’s α for the corresponding dimensions. Following group discussions, six items were removed, leaving 32 items in the final scale.
Structural Validity Assessment
EFA was conducted on the first half of the sample (N=214) to explore the basic factor structure of the 32-item scale. The KMO test yielded a value of 0.926, confirming good sampling adequacy. Bartlett’s test of sphericity (χ² = 4546.159, p < 0.001) indicated sufficient inter-item correlations to perform the EFA. Four factors were identified, accounting for 60.338% of the total variance. All factor loadings were > 0.5, with no cross-loadings observed, as detailed in Table 2. Based on the MOA model, the four factors were designated as Motivation (5 items), Opportunity (12 items), Ability (9 items), and Behavior (6 items).
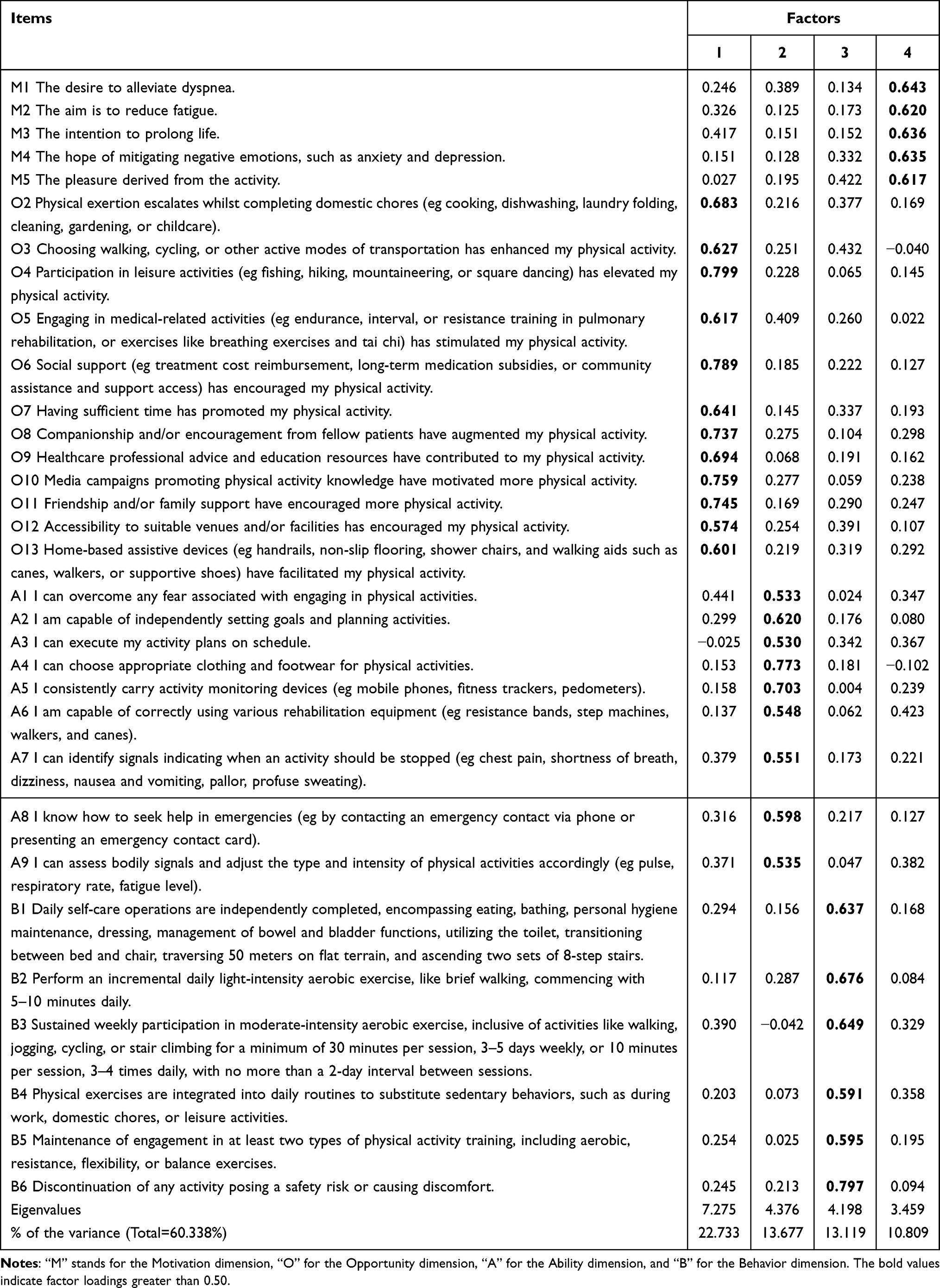 |
Table 2 Exploratory Factor Analysis Results (n=214) |
CFA was conducted on the second half of the sample (N=219) to validate the four-factor structure identified through EFA. The standardized factor loadings for the four dimensions (Motivation, Opportunity, Ability, and Behavior) ranged from 0.715 to 0.910 (Figure 1). Fit indices were as follows: χ²/df = 1.891 < 3, SRMR = 0.0497 < 0.05, RMSEA = 0.064 < 0.08, CFI = 0.927 > 0.90, and TLI = 0.921 > 0.90, indicating an excellent model fit.
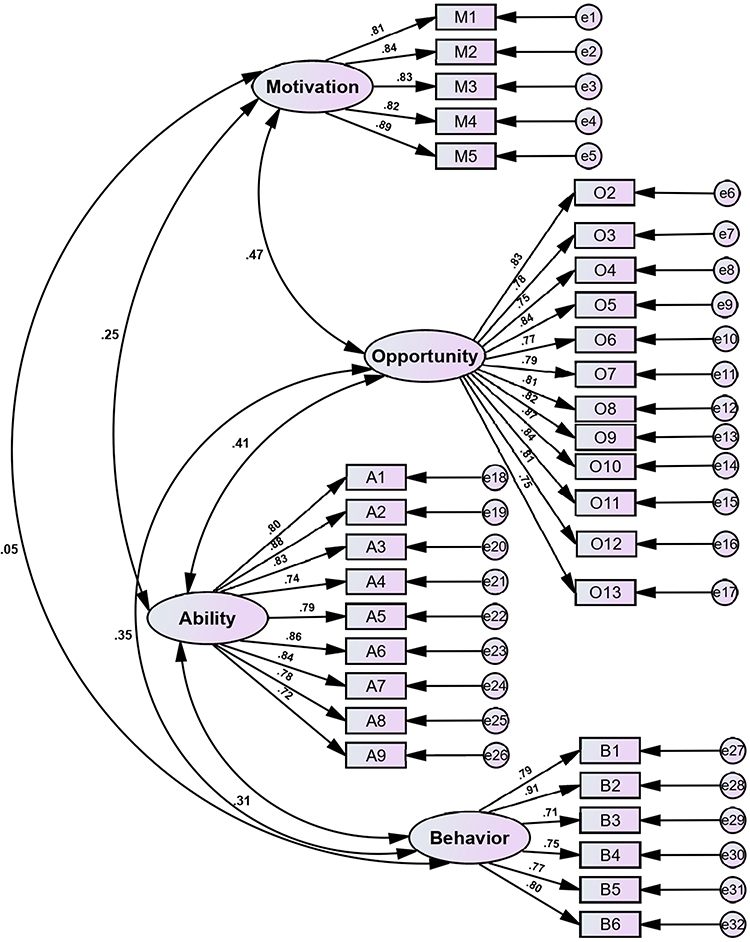 |
Figure 1 Confirmatory factor analysis results. |
Content Validity
The expert judgment coefficients (Ca) for the three rounds of consultation were 0.929, 0.935, and 0.940, respectively. The familiarity coefficients (Cs) were 0.848, 0.850, and 0.870, with authority coefficients (Cr) of 0.888, 0.893, and 0.905, indicating a high level of expert authority. The Kendall W concordance coefficients for the three rounds of expert consultation were 0.200 (χ² = 168.274), 0.248 (χ² = 207.912), and 0.263 (χ² = 194.354), all with p < 0.001, suggesting good agreement among the experts. The average importance scores for the items in each round ranged from 3.05 to 4.86, 3.45 to 4.90, and 4.10 to 4.95, with coefficients of variation (CV) of 0.07 to 0.46, 0.06 to 0.35, and 0.05 to 0.18, respectively. The percentage of maximum scores ranged from 19.05% to 85.71%, 20.00% to 90.00%, and 30.00% to 95.00%. After three rounds of consultation, there was a high degree of consensus regarding the importance of the 38 retained items. The final scale showed an average S-CVI of 0.992, with I-CVI ranging from 0.950 to 1.000, indicating strong content validity.
Reliability
The Cronbach’s alpha coefficient for the overall scale was 0.956, and the alpha coefficients for the four dimensions ranged from 0.826 to 0.945. The removal of individual items did not lead to a noticeable increase in alpha values. The test-retest reliability for the overall scale was 0.777, with values for the individual dimensions ranging from 0.707 to 0.742, as presented in Table 3. During the first assessment, some patients were either hospitalized or attending outpatient appointments and completed a paper questionnaire in person, after which they received health education on physical activity. For the second assessment, patients who had already been discharged were surveyed via telephone follow-up. Changes in the patient’s health status, psychological condition, and the measurement environment or method may have slightly reduced the test-retest reliability, as patient behavior may fluctuate over a week. Despite the good internal consistency of the scale’s items, the test-retest reliability showed a slight decrease. However, the overall scale’s test-retest reliability remained above 0.75, indicating an excellent level of reliability.40
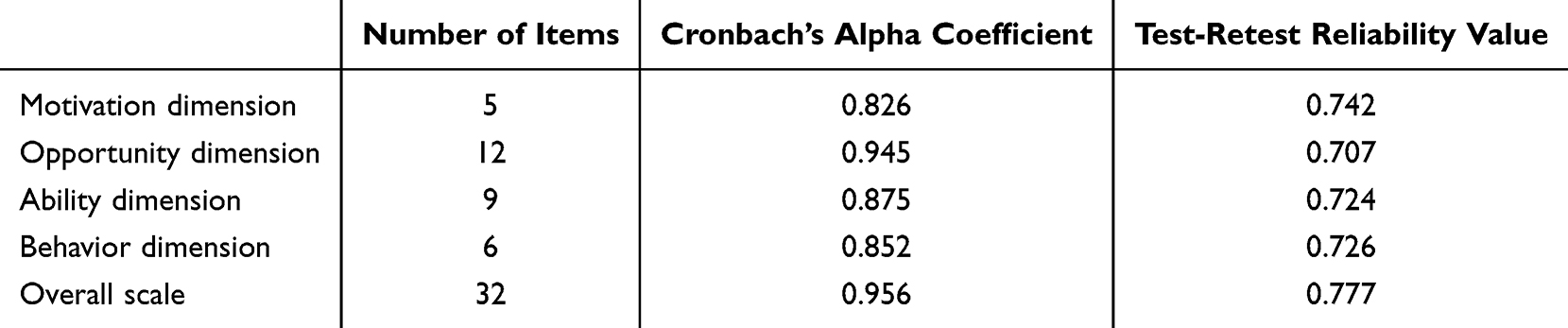 |
Table 3 Reliability Analysis Results |
Discussion
In this study, a new scale was developed based on the MOA model, which served as the theoretical framework. The scale incorporated four key dimensions: motivation, opportunity, ability, and behavior. A systematic evaluation was conducted using guidelines, literature review, qualitative analysis, group discussions, expert consultations, and a pilot test. Furthermore, the scale’s psychometric properties were assessed in a large sample of COPD patients, with a focus on factor structure. The theoretically grounded four-factor scale demonstrated strong psychometric properties, and subsequent EFA and CFA confirmed its reliability and validity from both theoretical and statistical perspectives. The results offer new insights into the conceptualization and structure of physical activity participation behaviors in COPD patients, indicating that the 32-item scale effectively measures physical activity participation levels and can inform the development of future interventions. By addressing each specific dimension and item, the scale can improve the physical activity participation behaviors of COPD patients and serve as a key outcome measure for evaluating the effectiveness of various interventions.
The scale was designed based on the MOA model, which emphasizes the direct influence of motivation on behavior while recognizing the moderating roles of opportunity and ability. The final scale comprises four dimensions: motivation, opportunity, ability, and behavior related to physical activity participation in COPD patients, consistent with the theoretical framework of the MOA model. The motivation dimension assesses an individual’s intrinsic drive to engage in physical activity, focusing on the impact of self-efficacy and the expectation of symptom improvement and life extension—findings that have been previously reported.41 The opportunity dimension evaluates the external environmental support for physical activity, particularly the availability of social support and environmental resources. Recent studies have confirmed the relationship between urban environments and increased physical activity participation among COPD patients.42 The ability dimension highlights the specific skills and confidence necessary for physical activity, addressing psychological barriers, goal-setting, safety concerns, and adjustments to activity levels. Research by Blondeel et al has illustrated the correlation between activity capacity and walking intensity.43 Several theoretical models, such as the Physical Activity-related Health Competence (PAHCO) model,44 emphasize that ability is a key factor influencing physical activity behavior. Finally, the behavior dimension focuses on the type, frequency, intensity, and safety management of physical activity during both leisure and non-leisure periods. While the MOA model aligns with the Capability, Opportunity, Motivation–behavior (COM-B) framework,45 which examines the interaction between motivation, opportunity, ability, and behavior, the motivation dimension in the MOA model places particular emphasis on the central role of intrinsic motivation in initiating behavior.
Apart from the opportunity domain, several items in the other domains overlap with those in the C-PPAC instrument,23 which is a patient-completed tool. Additionally, the motivation domain shares similarities with the Behavioral Regulations in Exercise Questionnaire-2 (BREQ-2).46 However, our 32-item instrument includes more items than both the C-PPAC and BREQ-2, providing a more comprehensive measure of physical activity participation behavior, incorporating both psychological and environmental factors. Despite the increased number of items, the scale demonstrated strong psychometric performance, with a completion time of under 15 minutes, which is considered acceptable A shorter version of the scale may be considered for future use. The theoretically guided development process enabled a thorough evaluation of all aspects of the scale, which will be beneficial for the creation of more effective prevention strategies.
The key components in the development of the scale included extensive involvement from both patients and healthcare providers.47 Input from patients, key informants, respiratory physicians, head nurses, nurses, and experts in rehabilitation, psychology, and physical therapy enabled the incorporation of the most common themes across all COPD participants. These themes were consistent with those found in the literature,48,49 helping to identify potential gaps in research on physical activity management for COPD patients. Additionally, experts recommended including specific topics (eg home activity aids) as well as symptoms (eg dyspnea and fatigue) and psychological aspects (eg anxiety and depression) relevant to COPD patients in our scale. To address the lack of expert consultation in the development stages of some existing measurement tools,50 we involved patients and multidisciplinary experts from the early stages of tool development, specifically seeking their insights on each dimension and item’s content, format, relevance, and clarity. Feedback received during the pre-testing phase enabled our team to revise the scale, preparing it for final validation in the cohort of COPD patients in China.
Our study demonstrated that the scale exhibited good reliability and structural validity. The Cronbach’s alpha coefficient for the total scale showed strong internal consistency, with all four dimensions exceeding 0.8, indicating excellent internal consistency.51 Our results suggested that all items on the scale consistently measured the same theme and aligned well with it. According to Hair et al’s research,36 the factors extracted in the EFA were reliable, as the factor loadings of all items exceeded 0.5, and the total explained variance was at least 60.338%. The EFA identified a four-factor structure, which was further confirmed by CFA showing good model fit, indicating that each dimension represented its respective concept.52 CFA results indicated that the standardized factor loadings of all items were greater than the recommended value of 0.5, and were statistically significant, suggesting good structural validity. These findings provide strong evidence for the scale’s satisfactory internal consistency and structural validity.
Given the challenges clinicians face in identifying reduced levels of physical activity in COPD patients, as well as the lack of comprehensive assessment methods among healthcare professionals,53 the design of this scale meets a critical clinical need. Its content is closely aligned with patients’ real-life conditions and is easy to understand and complete. This facilitates a rapid and accurate assessment of COPD patients’ physical activity participation, providing strong support for the development of personalized intervention strategies. In addition, the scale’s simplicity and efficiency ensure its ease of implementation and widespread use in clinical settings, thus enhancing the management of physical activity participation in COPD patients. Future studies will continue to evaluate the scale’s effectiveness across different clinical settings and refine it based on real-world feedback to provide more precise and effective strategies for managing physical activity for patients.
However, this study also had some limitations. First, the sample was recruited from a city in China between June and September 2024, with approximately 80% of the sample being male, predominantly elderly Asians. The results may therefore be subject to seasonal and climate-related biases and may not be representative of other regions or populations. Further research is needed to test the scale’s reliability and validity across more diverse seasons, healthcare systems, and populations (eg women and younger adults). Second, the scale’s assessment relied on self-reported data, which may be susceptible to social desirability bias. Future studies might consider combining this with more objective assessment methods, such as accelerometers for accurate measurement of physical activity.54 Additionally, future research should conduct more comprehensive psychological testing, covering construct, criterion, and cross-cultural validity, to confirm its robust psychometric properties.
Conclusion
In this study, a comprehensive four-factor scale for assessing physical activity participation behavior in patients with COPD was developed based on the MOA model. The 32-item scale exhibited strong psychometric properties, providing reliable and valid information regarding physical activity participation behavior in COPD patients. The results suggested that the scale could serve as an effective tool for evaluating physical activity participation in future research, as well as guiding interventions and outcome assessments for COPD patients by healthcare professionals.
Abbreviations
BREQ-2, behavioral regulations in exercise questionnaire-2; CFA, confirmatory factor analysis; CFI, comparative fit index; COM-B, capability, opportunity, motivation–behavior; COPD, chronic obstructive pulmonary disease; C-PPAC, PROactive physical activity in COPD; CV, coefficients of variation; EFA, exploratory factor analysis; GOLD, global initiative for chronic obstructive lung disease; ICC, intraclass correlation coefficient; I-CVI, item-level content validity index; IPAQ, international physical activity questionnaire; KMO, Kaiser-Meyer-Olkin; LCADL, London chest activity of daily living; MOA, motivation-opportunity-ability; PA, physical activity; PAHCO, physical activity-related health competence; PASE, physical activity scale for the elderly; RMSEA, root mean square error of approximation; S-CVI, scale-level content validity index; SQUASH, short questionnaire to assess health-enhancing physical activity; SRMR, standardized root mean residual; TLI, Tucker-Lewis index; YPAS, Yale physical activity survey.
Data Sharing Statement
The data that support the findings of this study are available from the corresponding author, JY, upon reasonable request.
Ethics Approval and Informed Consent
The study follows the principles outlined in the Declaration of Helsinki. Before its initiation, the research protocol was submitted for approval to the Ethics Committee of Tongji Medical College, Huazhong University of Science and Technology. Submitted materials included study design, questionnaire content, data collection methods, informed consent forms, participant recruitment procedures, and risk assessments. The committee assessed the ethical, safety, and scientific integrity of the study and approved it (approval number: [2023] Lun Shen Zi [S133]). All participants provided written informed consent before participation. In addition, the study was conducted anonymously, and data was securely stored by designated personnel to protect participants’ privacy and enhance the reliability of the results.
Acknowledgments
We would like to express our gratitude to all the participants who generously dedicated their time to this study by completing the questionnaire, as well as to the healthcare professionals who assisted with recruitment.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
The research received funding from two sources: Sponsor 1, the School of Nursing at Tongji Medical College, Huazhong University of Science and Technology, via the 2023 Independent Innovation Fund (ZZCX2023X003); and Sponsor 2, the Hubei Province Finance Department’s 2024 Research Program (08.01.24011). Both grants were awarded to the corresponding author, Jiaohua Yu. Sponsor 1 subsidized the study design, data collection, and analysis; whereas Sponsor 2 funded the manuscript publication and preparation.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Wang C, Xu J, Yang L, et al. Prevalence and risk factors of chronic obstructive pulmonary disease in China (the China Pulmonary health [CPH] study): a national cross-sectional study. Lancet. 2018;391(10131):1706–1717. doi:10.1016/S0140-6736(18)30841-9
2. Global Initiative for Chronic Obstructive Lung Disease. Global strategy for the diagnosis, management, and prevention of chronic obstructive pulmonary disease (2024 report); 2023. Available from: https://goldcopd.org/.
3. BMJ Best Practice. Chronic Obstructive Pulmonary Disease (COPD); 2024. Available from: https://bestpractice.bmj.com/topics/en-gb/7/prevention.
4. Caspersen CJ, Powell KE, Christenson GM. Physical activity, exercise, and physical fitness: definitions and distinctions for health-related research. Public Health Rep. 1985;100(2):126–131.
5. Lee YH, Huang YP, Pan SL. Physical activity and the risk of chronic obstructive pulmonary disease: a longitudinal follow-up study in Taiwan. Am J Med Sci. 2024;368(1):55–60. doi:10.1016/j.amjms.2024.03.013
6. Hanrahan C, Broderick J, O’Connor TM, McVeigh JG. Behaviour change and physical activity interventions for physical activity engagement in community dwelling adults with chronic obstructive pulmonary disease: protocol for a systematic review. HRB Open Res. 2022;4:110. doi:10.12688/hrbopenres.13399.2
7. Saka S, Gurses HN, Bayram M. Effect of inspiratory muscle training on dyspnea-related kinesiophobia in chronic obstructive pulmonary disease: a randomized controlled trial. Complement Ther Clin Pract. 2021;44:101418. doi:10.1016/j.ctcp.2021.101418
8. Xiang X, Huang L. Summary of the best evidence for physical activity in patients with chronic obstructive pulmonary disease. Chin J Health Manage. 2022;16(11):798–804. doi:10.3760/cma.j.cn115624-20220617-00463
9. Samitz G, Egger M, Zwahlen M. Domains of physical activity and all-cause mortality: systematic review and dose-response meta-analysis of cohort studies. Int J Epidemiol. 2011;40(5):1382–1400. doi:10.1093/ije/dyr112
10. Ichinose M, Minakata Y, Motegi T, et al. A non-interventional, cross-sectional study to evaluate factors relating to daily step counts and physical activity in Japanese patients with chronic obstructive pulmonary disease: STEP COPD. Int J Chron Obstruct Pulmon Dis. 2020;15:3385–3396. doi:10.2147/COPD.S277782
11. Yoshida M, Hiramoto T, Moriwaki A, Osoreda H, Iwanaga T, Inoue H. Impact of extrapulmonary comorbidities on physical activity in chronic obstructive pulmonary disease in Japan: a cross-sectional study. PLoS One. 2022;17(7):e0270836. doi:10.1371/journal.pone.0270836
12. Hirata RP, Dala Pola DC, Schneider LP, et al. Tossing and turning: association of sleep quantity-quality with physical activity in COPD. ERJ Open Res. 2020;6(4):00370–2020. doi:10.1183/23120541.00370-2020
13. Neale CD, Christensen PE, Dall C, Ulrik CS, Godtfredsen N, Hansen H. Sleep quality and self-reported symptoms of anxiety and depression are associated with physical activity in patients with severe COPD. Int J Environ Res Public Health. 2022;19(24):16804. doi:10.3390/ijerph192416804
14. Hoaas H, Zanaboni P, Hjalmarsen A, et al. Seasonal variations in objectively assessed physical activity among people with COPD in two Nordic countries and Australia: a cross-sectional study. Int J Chron Obstruct Pulmon Dis. 2019;14:1219–1228. doi:10.2147/COPD.S194622
15. Barbolla Benito P, Peces-Barba Romero G. Self-reported walking and associated factors in the Spanish population with chronic obstructive pulmonary disease. BMC Pulm Med. 2018;18(1):166. doi:10.1186/s12890-018-0731-4
16. Wang J, Bai C, Zhang Z, Chen O. The relationship between dyspnea-related kinesiophobia and physical activity in people with COPD: cross-sectional survey and mediated moderation analysis. Heart Lung. 2023;59:95–101. doi:10.1016/j.hrtlng.2023.02.007
17. Tödt K, Skargren E, Jakobsson P, Theander K, Unosson M. Factors associated with low physical activity in patients with chronic obstructive pulmonary disease: a cross-sectional study. Scand J Caring Sci. 2015;29(4):697–707. doi:10.1111/scs.12200
18. van Buul AR, Kasteleyn MJ, Chavannes NH, Taube C. Physical activity in the morning and afternoon is lower in patients with chronic obstructive pulmonary disease with morning symptoms. Respir Res. 2018;19(1):49. doi:10.1186/s12931-018-0749-4
19. Mendoza L, de Oca MM, López Varela MV, et al. Physical activity levels and associated factors in a Latin American COPD population of patients. The LASSYC Study. COPD. 2021;18(4):393–400. doi:10.1080/15412555.2021.1937090
20. Dragnich AG, Yee N, Gylys-Colwell I, et al. Sociodemographic characteristics and physical activity in patients with COPD: a 3-month cohort study. COPD. 2021;18(3):265–271. doi:10.1080/15412555.2021.1920902
21. van Buul A R, Kasteleyn M J, Poberezhets V, et al. Factors associated with physical activity among COPD patients with mild or moderate airflow obstruction. Monaldi Arch Chest Dis. 2021;92(1):
22. Esteban C, Antón-Ladislao A, Aramburu A, et al. Physical activity and sedentary behaviour in patients admitted with COPD: associated factors. Respir Med Res. 2023;84:101052. doi:10.1016/j.resmer.2023.101052
23. Koreny M, Arbillaga-Etxarri A, Bosch de Basea M, et al. Urban environment and physical activity and capacity in patients with chronic obstructive pulmonary disease. Environ Res. 2022;214(Pt 2):113956. doi:10.1016/j.envres.2022.113956
24. Amorim PB, Stelmach R, Carvalho CR, Fernandes FL, Carvalho-Pinto RM, Cukier A. Barriers associated with reduced physical activity in COPD patients. J Bras Pneumol. 2014;40(5):504–512. doi:10.1590/S1806-37132014000500006
25. MacInnis D, Moorman C, Jaworsk BJ. Enhancing consumers ‘motivation, ability and opportunity to process brand information from ads: conceptual framework and managerial implications. J Mark. 1991;55(55):32–53. doi:10.2307/1251955
26. Zong X, Fukushige A. Motivation, opportunity, and ability of Chinese tourists to stay at green hotels in Thailand. J China Tour. 2023;20(2):241–260. doi:10.1080/19388160.2023.2190187
27. Wang D, Zhan C. Why not blow the whistle on health care insurance fraud? Evidence from Jiangsu province, China. Risk Manag Healthc Policy. 2022;15:1897–1915. doi:10.2147/RMHP.S379300
28. Chen Z. Formation, development and core concepts of the MOA model. Research on Library Science. 2013;(13):53–57. doi:10.15941/j.cnki.issn1001-0424.2013.13.017
29. Burge AT, Cox NS, Abramson MJ, Holland AE. Interventions for promoting physical activity in people with chronic obstructive pulmonary disease (COPD). Cochrane Database Syst Rev. 2020;4(4):CD012626. doi:10.1002/14651858.CD012626.pub2
30. NICE. Physical activity: exercise referral schemes; 2014. Available from: https://www.nice.org.uk/guidance/ph54/chapter/Update-information.
31. NICE. Chronic obstructive pulmonary disease in adults; 2023. Available from: https://www.nice.org.uk/guidance/qs10.
32. Liao Y, Yu J, Zhan Y, et al. Motivating factors for physical activity participation among individuals with chronic obstructive pulmonary disease: a qualitative study applying the motivation, opportunity, and ability model. PLoS One. 2024;19(6):e0306494. doi:10.1371/journal.pone.0306494
33. Mokkink LB, Prinsen CAC, Patrick DL, et al. COSMIN study design checklist for patient-reported outcome measurement instruments; 2019. Available from: https://www.cosmin.nl/wp-content/uploads/COSMIN-study-designing-checklist_final.pdf.
34. Kline RB. Principles and Practice of Structural Equation Modeling.
35. Westland JC. Information loss and bias in Likert survey responses. PLoS One. 2022;17(7):e0271949. doi:10.1371/journal.pone.0271949
36. Hair JF, Babin BJ, Anderson RE, Black WC. Multivariate Data Analysis.
37. Polit DF, Beck CT. The content validity index: are you sure you know what’s being reported? Critique and recommendations. Res Nurs Health. 2006;29(5):489–497. doi:10.1002/nur.20147
38. Pituch KA, Stevens JP. Applied Multivariate Statistics for the Social Sciences.
39. Kline PA. Handbook of Test Construction.
40. Cicchetti DV. Guidelines, criteria, and rules of thumb for evaluating normed and standardized assessment instruments in psychology. Psychol Assess. 1994;6(4):284–290. doi:10.1037/1040-3590.6.4.284
41. Aljama C, Granados G, Ramon M, et al. Motivation and confidence about physical activity in chronic obstructive pulmonary disease patients: health benefits matter to patients. Respiration. 2024;103(7):378–387. doi:10.1159/000539206
42. Guimarães Paiva L, Oliveira TMD, Souza NB, et al. Exploring the impact of the environment on physical activity in patients with chronic obstructive pulmonary disease (EPCOT)-A comparative analysis between suggested and free walking: protocol study. PLoS One. 2024;19(8):e0306045. doi:10.1371/journal.pone.0306045
43. Blondeel A, Hermans F, Breuls S, et al. Factors associated to physical activity in patients with COPD: an ecological approach. Respir Med. 2023;219:107424. doi:10.1016/j.rmed.2023.107424
44. Carl JA, Geidl W, Schuler M, et al. Towards a better understanding of physical activity in people with COPD: predicting physical activity after pulmonary rehabilitation using an integrative competence model. Chron Respir Dis. 2021;18:1479973121994781. doi:10.1177/1479973121994781
45. Midthun WR, Benzo MV, Ridgeway JL, Benzo RP. Understanding the patient experience of home-based pulmonary rehabilitation with health coaching for COPD: a qualitative interview study. Chronic Obstr Pulm Dis. 2023;10(3):224–233. doi:10.15326/jcopdf.2022.0384
46. Cho HL, Tung HH, Lin MS, Hsu WC, Lee CP. Self-determined motivation and exercise behaviour in COPD patients. Int J Nurs Pract. 2017;23(3):1–9. doi:10.1111/ijn.12530
47. Poureslami I, Shum J, Kopec J, et al. Development and pretesting of a new functional-based health literacy measurement tool for chronic obstructive pulmonary disease (COPD) and asthma management. Int J Chron Obstruct Pulmon Dis. 2020;15:613–625. doi:10.2147/COPD.S234418
48. Tian J, Zhou F, Zhang XG, et al. Experience of physical activity in patients with COPD: a systematic review and qualitative meta-synthesis. Geriatr Nurs. 2022;47:211–219. doi:10.1016/j.gerinurse.2022.07.013
49. Xiang X, Huang L, Fang Y, Cai S, Zhang M. Physical activity and chronic obstructive pulmonary disease: a scoping review. BMC Pulm Med. 2022;22(1):301. doi:10.1186/s12890-022-02099-4
50. Garrod R, Bestall JC, Paul EA, Wedzicha JA, Jones PW. Development and validation of a standardized measure of activity of daily living in patients with severe COPD: the London Chest Activity of Daily Living scale (LCADL). RespirMed. 2000;94(6):589–596. doi:10.1053/rmed.2000.0786
51. Spitzer RL, Endicott J, Robins E. Research diagnostic criteria: rationale and reliability. Arch Gen Psychiatry. 1978;35(6):773–782. doi:10.1001/archpsyc.1978.01770300115013
52. Tinsley HEA, Tinsley DJ. Uses of factor analysis in counseling psychology research. J Couns. 1987;34(4):414–424.
53. Lahham A, Burge AT, McDonald CF, Holland AE. How do healthcare professionals perceive physical activity prescription for community-dwelling people with COPD in Australia? A qualitative study. BMJ Open. 2020;10(8):e35524. doi:10.1136/bmjopen-2019-035524
54. Soler-Cataluña JJ, Puente Maestu L, Román Rodríguez M, et al. Validation of the Spanish activity questionnaire in COPD (SAQ-COPD) in patients with chronic obstructive pulmonary disease. Int J Chron Obstruct Pulmon Dis. 2022;17:2835–2846. doi:10.2147/COPD.S381427
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.