Back to Journals » Patient Preference and Adherence » Volume 20
Development and Preliminary Validation of a Dyadic Psychoeducational Intervention for Hemodialysis Patients and Caregivers Based on the Double ABC-X Model
Authors Zhang L ![]() , Zhang X, Tang W
, Zhang X, Tang W ![]() , Zou L, Chen Y, Zhou L
, Zou L, Chen Y, Zhou L
Received 23 January 2026
Accepted for publication 3 April 2026
Published 14 April 2026 Volume 2026:20 598462
DOI https://doi.org/10.2147/PPA.S598462
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Emma Veale
LiYuan Zhang,1,* XiaoHong Zhang,2,* Wen Tang,3 Li Zou,4 Yan Chen,5 LiJuan Zhou3
1Department of Neurosurgery, The Affiliated Taizhou People’s Hospital of Nanjing Medical University, Taizhou, Jiangsu, People’s Republic of China; 2Outpatient Department, The Affiliated Taizhou People’s Hospital of Nanjing Medical University, Taizhou, Jiangsu, People’s Republic of China; 3Nursing Department, The Affiliated Taizhou People’s Hospital of Nanjing Medical University, Taizhou, Jiangsu, People’s Republic of China; 4Endocrinology Department, The Affiliated Taizhou People’s Hospital of Nanjing Medical University, Taizhou, Jiangsu, People’s Republic of China; 5The Medical Insurance Administration Office, The Affiliated Taizhou People’s Hospital of Nanjing Medical University, Taizhou, Jiangsu, People’s Republic of China
*These authors contributed equally to this work
Correspondence: LiJuan Zhou, Email [email protected]
Objective: To develop and preliminarily validate a dyadic psychoeducational intervention program for maintenance hemodialysis (MHD) patients and their caregivers based on the Double ABC-X Model.
Methods: The intervention was constructed by integrating evidence from systematic reviews, cross-sectional survey data (200 MHD patient-caregiver dyads), and a two-round Delphi expert consultation (20 experts). The program, grounded in the Double ABC-X Model, comprised four core modules: (1) disease information provision, (2) social support enhancement, (3) coping strategy training, and (4) relaxation techniques. A pilot trial with three dyads was conducted to assess feasibility and refine the program. Effectiveness was not evaluated in this developmental study.
Results: The intervention was designed as a 4-week program with one 30– 40 minute session per week, delivered in face-to-face small groups during pre- or post-dialysis periods. It comprises 4 first-level, 22 second-level, and 10 third-level indicators, organized into four themes: “First Acquaintance”, “Deep Understanding”, “Co - Solution” and “Co - Experience”. Delphi results showed high expert authority (Cr=0.85– 0.86), significant Kendall’s concordance coefficient (P< 0.001), importance scores ≥ 4.35 (5-point scale), and low variation coefficients (≤ 0.12), indicating strong consensus.
Conclusion: This study developed a theory-driven, content-validated dyadic psychoeducational intervention for MHD patient-caregiver dyads. Future multicenter randomized controlled trials are needed to validate long-term efficacy.
Keywords: Delphi method, double ABC-X model, dyadic psychoeducational intervention, maintenance hemodialysis, program development
Background
Chronic kidney disease (CKD) is a major global health concern,1 with an estimated prevalence of 674 million in 2021.2 In China, approximately 120 million individuals are affected.3 End-stage renal disease (ESRD), the final stage of CKD, necessitates lifelong renal replacement therapy,4,5 with over 80% of patients receiving MHD.6 It is projected that by 2030, over 5.4 million patients worldwide will receive renal replacement therapy.7 MHD requires patients to attend dialysis sessions three times weekly, each lasting approximately four hours, alongside strict dietary, fluid, and medication regimens.8,9 These demands significantly impair patients’ quality of life (QoL) and mental health, with 50–95% experiencing anxiety and depression, a risk three to four times higher than the general population.4,10–12 Physical symptoms, cognitive dysfunction, and dependency further exacerbate psychological distress.13,14
Often termed “hidden patients,” caregivers experience significant stress, which impacts their well-being and patients’ treatment adherence.15 Compared to interventions targeting only patients or caregivers, dyadic interventions based on a family perspective that consider the mutual support between caregivers and patients are expected to benefit both parties.16 Empirical studies in chronic disease populations (particularly cardiovascular diseases) have shown that integrating psychoeducation for caregivers can produce bidirectional therapeutic effects: reducing caregiver burden while improving patient clinical outcomes.17,18 However, existing dyadic intervention studies have primarily focused on cancer,19 heart failure20 and stroke,21 with limited research on joint interventions for MHD patients and their caregivers. Unlike these conditions, MHD imposes a uniquely demanding routine—three weekly dialysis sessions, strict dietary controls, and ongoing vascular access management—creating persistent stress that affects both patients and caregivers in ways distinct from other chronic diseases. This highlights the need for a tailored dyadic psychoeducational intervention.
The Double ABC-X Model provides a robust framework for understanding dyadic stress and adaptation.22 It posits that family adaptation (xX) results from interactions among stressors (aA), resources (bB), perceptions (cC), and coping strategies (BC). This study based on the theoretical guidance of the Double ABC-X model and the results of systematic review4 and preliminary cross-sectional survey data, used the Delphi expert consultation method to construct a dyadic psychoeducational intervention program for MHD patients and caregivers to enhance coping, social support and psychosocial outcomes.
Methods
Delphi method was used to understand the attitude of experts towards the evaluation index system.23 This study was reported in accordance with the guidance for reporting intervention development studies in health research (GUIDED)24 and consolidated criteria for reporting reporting qualitative research (COREQ)25 to ensure transparency and integrity of the research process.
Formation of the Research Team
A multidisciplinary team of seven members was formed, including one chief nurse, two nursing postgraduate students, two hemodialysis specialist nurses, one chief physician of the hemodialysis center, and one clinical psychotherapist. Team members had extensive clinical experience in chronic kidney disease and clinical nursing. The chief nurse was responsible for overall project design and quality control; nursing postgraduates and specialist nurses were responsible for conducting systematic reviews to identify the latest evidence, drafting the initial intervention, designing expert consultation questionnaires, and performing statistical analysis; the chief physician and psychotherapist assisted in developing the initial draft based on clinical experience; the chief nurse, chief physician, and psychotherapist were responsible for inviting experts and summarizing their feedback. All team members held regular meetings to discuss and adjust the program.
Drafting the Initial Program
Theoretical Framework
This intervention program was constructed based on the Double ABC-X Model,22 which includes five core elements: stress accumulation (aA), family resources (bB), family cognition (cC), coping strategies (BC), and family adaptation (xX). The model explains the coping and adaptation process of family members facing crises, emphasizing that family adaptation is a complex process involving the interaction of resources and cognition, where the regulation of stress accumulation is crucial. During this process, the family system directly responds to the multidimensional demands of stressors, realizes the need to adjust internal structures to effectively cope with stressful events, and ultimately enhances family satisfaction and well-being.26 Based on our previous systematic review,4 this study designed the program around four core modules to strengthen the cognition and resources of MHD patient-caregiver dyads: (1) disease information provision; (2) social support enhancement; (3) coping strategy training; and (4) relaxation techniques.
Each module was designed to target specific elements of the Double ABC-X model. Disease information provision addresses the stressor (aA) by reducing uncertainty and enhancing knowledge about MHD. Social support enhancement strengthens family resources (bB) by expanding available support networks and facilitating emotional expression. Coping strategy training directly targets coping strategies (BC) by equipping dyads with problem-solving skills and adaptive coping techniques. Relaxation techniques further support coping (BC) by providing practical tools for emotional regulation. Together, these components aim to reshape family perception (cC) of the stressor and resources, ultimately promoting positive family adaptation (xX). This theoretical mapping is illustrated in Figure 1 and further detailed in the intervention description (Table 1).
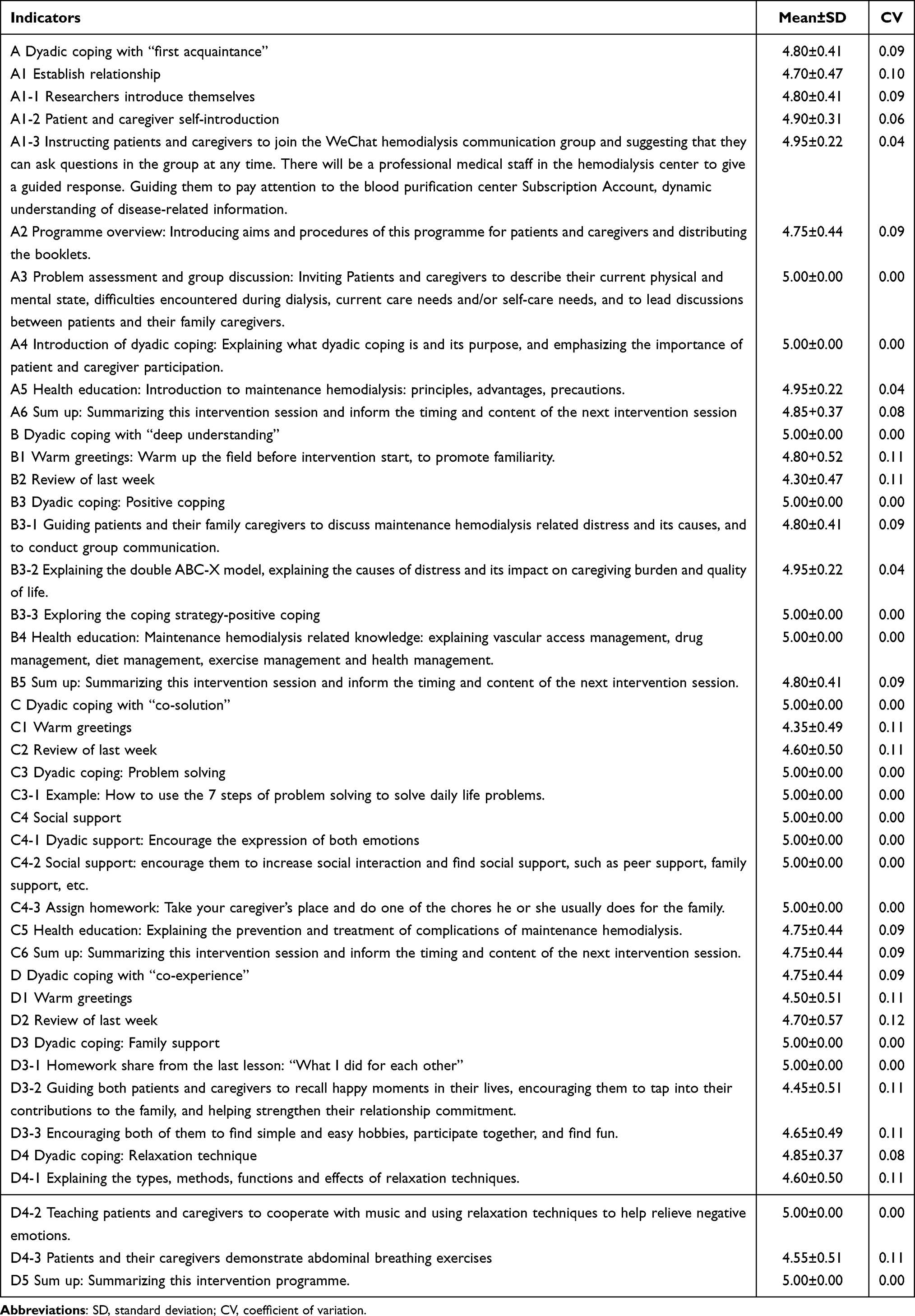 |
Table 1 Dyadic Psychoeducational Intervention Programs Based on the Double ABC-X Model |
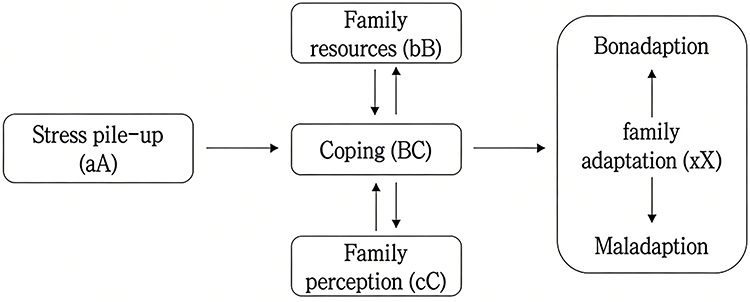 |
Figure 1 Double ABC-X Model of Family Stress and Adaptation: The model illustrates the core elements of family stress and adaptation, including stress pile-up (aA), family resources (bB), family perception (cC), coping strategies (BC), and family adaptation (xX). Family adaptation or maladaptation is determined by the interaction of these elements, rather than stressors alone; the family’s evaluation of stressors and utilization of resources to form coping strategies are the key determinants of adaptive outcomes. (aA) Addressed through disease information provision, which reduces uncertainty and knowledge gaps about MHD. (bB) Targeted through social support enhancement activities that strengthen available support networks. (cC) Influenced through problem assessment, group discussion, and cognitive reappraisal activities. (BC) Developed through coping strategy training and relaxation techniques. (xX) The hypothesized outcome of improved quality of life and reduced caregiver burden. The model provides the theoretical framework for the dyadic psychoeducational intervention program, with each session theme targeting specific model elements to promote adaptive coping and improve psychosocial outcomes for MHD patient-caregiver dyads. |
Literature Study
A systematic search was conducted in nine databases from inception to July 8, 2023, including five English databases (PubMed, Web of Science, CINAHL Complete, Cochrane Library, Embase) and four Chinese databases (CNKI, Wanfang, VIP, SinoMed). A combination of subject headings and free keywords was used for the search strategy (detailed PubMed strategy provided in Supplementary Table S1). Grey literature was retrieved from ProQuest Dissertations and Theses Global (PQDT Global) and Wanfang Degree Thesis Database, and references of included studies and relevant reviews were manually searched. Study selection was based on the PICOS framework, including studies that met the following criteria: 1) Population (P): hemodialysis patients aged ≥18 years. Caregivers were adult (≥18 years) family members (eg., spouses, children, siblings, other relatives) providing unpaid care (including physical, practical, or emotional support);27 2) Intervention (I): integrated psychoeducational interventions combining psychotherapeutic techniques (eg., cognitive reappraisal, behavioral activation, social support) with health education, aimed at improving psychological distress and/or quality of life in MHD patients;28 3) Comparison (C): usual care, blank control, placebo control, or waitlist control; 4) Outcomes (O): primary outcomes included psychological distress (eg., depression, anxiety, stress) and quality of life in MHD patients. Secondary outcomes included psychological distress and caregiving burden in family caregivers; 5) Study design (S): only randomized controlled trials were included, while study protocols, conference abstracts, reviews, and unpublished studies were excluded. A total of 14 studies were included, and indexes of related programs were preliminarily extracted to form an index entry pool of dyadic psychoeducational intervention programs for maintenance hemodialysis patients. This part of the study was registered on the International Prospective Register of Systematic Reviews (PROSPERO) in July 2023 (registration number: CRD42023440561).
Clinical Survey
The sample size was determined based on requirements for structural equation modeling (SEM).29 Following the widely recommended “5 or 10 cases per estimated parameter” rule (Boomsa, 1982),30 the proposed APIMeM model included 18 estimated parameters, requiring 90 or 180 dyads. To account for potential incomplete responses or missing data, we recruited 200 dyads. Hence a convenience sampling method was used to recruit 200 MHD patient-caregiver dyads from a tertiary hospital in Taizhou between October and November 2023. The inclusion criteria for patients were as follows: (i) meet the diagnostic criteria for CKD; (ii) MHD for more than 3 months; (iii) being aged ≥ 18 years; (iv) having a family caregiver as their partner in a dyad in this study. Family caregivers were included if they were: (i) being aged ≥ 18 years; (ii) responsible for the main care tasks of MHD patients. MHD dyads were excluded if: (i) either dyad member had a serious mental, visual, or hearing impairment that prevents normal communication; (ii) accompanied by serious diseases of vital organs. Surveys included a general information questionnaire, Emotion Regulation Scale (ERS),31 Medical Outcomes Study Social Support Survey (MOS-SSS),32 Problem Solving Inventory (PSI),33 Brief COPE Scale (BCS),34 Hospital Anxiety and Depression Scale (HADS),35 Zarit Caregiver Burden Interview (ZBI),36 and Kidney Disease Quality of Life 36-item Short Form (KDQOL-36™) (https://www.rand.org/health-care/surveys_tools/kdqol.html). Results showed that the average quality of life score for MHD patients was 66.54±14.55, significantly lower than the domestic norm.37 The average caregiver burden score was 41.21±14.51, indicating severe burden. Multivariate hierarchical regression analysis revealed that patients’ average monthly income, adaptive coping, and caregiver burden were independent risk factors for MHD patients’ quality of life; patients’ quality of life, social support, caregivers’ adaptive coping, and maladaptive coping were independent risk factors for caregiver burden. Actor-Partner Interdependence Model extended to Mediation (APIMeM) results showed that social support of both MHD patients and caregivers directly and positively predicted their own quality of life and caregiver burden, highlighting the important role of social support in improving patient quality of life and reducing caregiver burden. Additionally, adaptive coping of both patients and caregivers mediated the relationship between social support and patient quality of life, indicating that social support not only directly affects patient quality of life but also indirectly improves it by promoting positive coping strategies (detailed APIMeM provided in Supplementary Table S2). These findings further informed the program development.
Research Team Meetings
Guided by the Double ABC-X Model and referencing the systematic review,4 clinical survey results, and relevant literature, the seven team members discussed and revised the initial draft of the dyadic psychoeducational intervention program for MHD patients. The initial program included 4 first-level indicators, 10 second-level indicators, and 23 third-level indicators.
Expert Consultation
Designing the Expert Consultation Questionnaire
The expert consultation questionnaire consisted of four parts: 1) Instructions: briefly introduced the research purpose, background, status, existing problems, and instructions for completion. 2) Expert demographic information: included basic information about the experts, such as research field and years of experience. 3) Intervention program evaluation form: MHD patient dyadic psychoeducation expert opinion consultation form, using a 5-point scale from “not important” to “very important,” with encouragement for experts to provide specific suggestions or modifications in the “comments” Discussion) Expert authority self-assessment form: included familiarity with the topic and basis for judgment.
Selecting Experts
Selection criteria and procedures were based on guidelines for Delphi studies by Hasson.38 A consultation panel of 5–20 experts is considered scientific. Purposive sampling was used to select experts with extensive knowledge and experience in relevant fields. Inclusion criteria: ① experts in hemodialysis nursing, kidney disease management, nursing, nutrition, psychology, or related fields; ② bachelor’s degree or higher; ③ intermediate or higher professional title; ④ ≥5 years of work experience; ⑤ voluntary participation. Considering authority and accessibility, 20 experts were included. The process of gathering experts’ advice is independent and anonymous, ensuring that the experts will not discuss or exchange views.39 Through iterative multistage process, accurate and reliable data will eventually be obtained.
Conducting the Expert Consultation
Two rounds of expert consultation were conducted via WeChat in October–November 2023, each round limited to one week, with a two-week interval between rounds. Based on feedback from the first round, a revised questionnaire was sent for the second round. Results from the first round were attached to the second-round questionnaire to inform experts of modifications. As opinions converged in the second round, only two rounds were conducted.
Data Analysis
Mind maps were used to organize expert feedback. Key indicators included expert enthusiasm, authority, and coordination. The response rate was used to measure enthusiasm, with ≥70% indicating good participation. Expert authority (Cr) was calculated as the average of judgment basis (Ca) and familiarity (Cs), with Cr>0.70 indicating reliable opinions. Coordination was assessed using the coefficient of variation (CV) and Kendall’s coefficient of concordance, with CV>0.25 indicating disagreement and Kendall’s coefficient closer to 1 indicating better coordination (P<0.05 indicated significant agreement).
Ethics Considerations
The study design and procedures followed the Declaration of Helsinki and were approved by the Ethics Committee of Taizhou People’s Hospital, Jiangsu Province, China (KY2023-184-01). Written informed consent was obtained from each participant who agreed to participate in the study. Participants have the right to withdraw from the study at any time without any negative impact on their usual treatment, care, and other services.
Pilot Trial
After two rounds of Delphi expert consultation, a pilot trial was conducted with three MHD patient-caregiver dyads to assess the feasibility and acceptability of the intervention program. The purpose was to evaluate clarity, relevance, and practical delivery issues, rather than to test effectiveness. Two nursing postgraduates from the research team, both trained in the intervention protocol, delivered the four-session program. Feedback was collected through semi-structured interviews with each dyad after every session, exploring their understanding of the content, perceived relevance, and suggestions for improvement. Researchers also maintained observational notes during sessions to document engagement levels, interaction patterns, and any practical difficulties. Regarding structural feasibility indicators, all three dyads (100%) attended all four sessions, and no participants withdrew from the study, indicating acceptable adherence and retention. However, given the small sample size (n=3 dyads), these findings should be interpreted as preliminary indicators of feasibility rather than robust quantitative evidence.
Results
Expert Demographics
All 20 experts completed both rounds of consultation. They were from hospitals and universities in Jilin, Jiangsu, Zhejiang, and Hong Kong in China. There were 2 full professors, 7 associate professors, and 11 lecturers; 3 had PhDs, 8 had master’s degrees, and 9 had bachelor’s degrees; 10 were from hemodialysis nursing and medical fields, 5 from nursing management, and 5 from nursing research; average work experience was 18.10±10.06 years.
Expert Enthusiasm and Authority
The questionnaire response rate was 100% in both rounds. In the first round, 10 experts (50%) provided comments, and in the second round, 4 experts (20%) provided comments. The expert authority coefficients were 0.86 and 0.85 for the two rounds, with judgment coefficients of 0.94 and 0.92, and familiarity scores of 0.78 and 0.78, respectively.
Expert Coordination
Kendall’s coefficient of concordance was 0.147 (P<0.001) in the first round and 0.288 (P<0.001) in the second round, indicating moderate to acceptable consensus among experts. Details are shown in Table 2.
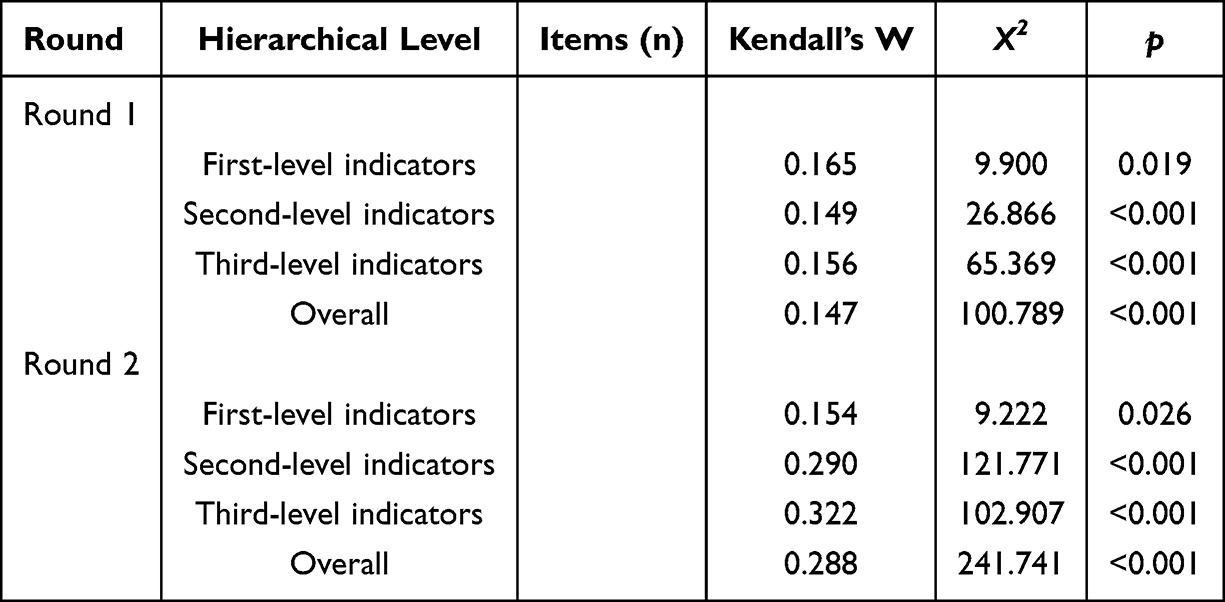 |
Table 2 Coordination Degree of Expert Opinions |
Expert Consultation Results
Based on suggestions from the first round, the team discussed and revised the content: 1) Adjustments: ① The experts suggested that the original theme names were not appropriate, lacked strong relevance to the intervention content, and were insufficiently distinctive, recommending revisions. After discussion within the research team, it was decided to retain the four themes but revise their names as follows: Theme 1 to “Dyadic Coping - First Acquaintance”; Theme 2 to “Dyadic Coping - Deep Understanding”; Theme 3 to “Dyadic Coping - Co-Solution”; Theme 4 to “Dyadic Coping - Co-Experience”. ② The experts pointed out that the original course sequence lacked logical flow, which could easily lead to memory loss or confusion among participants, and recommended a restructuring. In response to this feedback, we have reorganized the course order to enhance coherence and prevent potential misunderstandings. Additionally, the language used throughout has been refined to be clearer and more specific. ③ Based on feedback from multiple experts regarding the potential sensitivity of patient issues involving personal privacy, we have implemented two key changes: the question submission feature on the WeChat public platform has been set to anonymous, and a WeChat group has been established to facilitate patient discussions on non-private matters. 2) Additions: ① The experts noted that the course content lacked sufficient detail and was prone to cause confusion, recommending that we expand and better categorize the course modules. Following team discussions, we have systematically reorganized the curriculum under each theme. Additionally, a “Summary” session has been added at the end of each thematic unit to help participants consolidate key takeaways and inform them about the main content, schedule, and location of the next session. ② Based on expert recommendations to better understand the challenges faced by patients and caregivers during maintenance hemodialysis and provide corresponding coping strategies, the research team made the following revisions after discussion: in the “Problem Assessment and Group Discussion” session of Theme 1, we added an activity to
Invite patients and caregivers to describe their current physical and psychological states, difficulties encountered during dialysis, current nursing and/or self-care needs, and guide the patient-family caregiver dyads in discussion.
Within the “Dyadic Coping: Positive Coping” session of Theme 2, we incorporated content explaining the causes and impacts of these challenges, along with corresponding coping strategies. ③ In response to expert suggestions to enhance interaction among participants, the research team incorporated homework assignments and sharing sessions into the program after group discussions. Specifically, the following additions were made: In Theme 3, an “ Assign homework” was added: “ Take your caregiver’s place and do one of the chores he or she usually does for the family.” In Theme 4, a “Homework Sharing” session titled What I did for each other was introduced to facilitate discussion of these experiences. ④ experts observed that the relaxation techniques were limited to abdominal breathing exercises and recommended incorporating additional methods to allow participants to choose based on their preferences. In response, we have expanded the relaxation techniques component in Theme 4 by adding four new methods. The session now emphasizes detailed guidance on their practical application and includes live participant demonstrations.
The preliminarily revised dyadic psychoeducational intervention program was converted into a QR code using the Questionnaire Star platform and redistributed to all experts for the second round of consultation. During this round, several items received mean importance scores of 5.00 with zero standard deviation, indicating complete consensus among experts. This clustering likely reflects the rigorous pre-development process—including systematic review and clinical survey—which ensured that only evidence-based and clinically relevant items proceeded to expert evaluation. Additionally, the highly experienced expert panel (mean 18.1 years) and two-round revision process contributed to convergence on core intervention components. Expert opinions showed convergence toward consensus, allowing us to focus primarily on further refining and optimizing the program’s language to ensure greater clarity and precision.
Pilot Trial to Refine the Program
After two rounds of expert consultation, three MHD patient-caregiver dyads were recruited for a pilot trial. Based on feedback, further adjustments were made: ① During the intervention, some patients exhibited reluctance to communicate. To address this, the researchers adopted a proactive communication strategy during dialysis sessions. Through persistent yet respectful dialogue attempts, they actively listened to patients’ concerns regarding both treatment and daily life, providing individualized responses and support. This included clarifying medical questions, offering emotional guidance, and addressing practical needs. These efforts progressively fostered a trusting and understanding relationship between researchers and patients. ②During the intervention, some patients demonstrated limited interactivity, often remaining silent due to uncertainty in responding to questions. To address this, we modified the format of Theme 1 sessions from solely individual face-to-face interactions to a combination of individual and group face-to-face sessions. The revised format incorporates self-introductions among group members, ice-breaking activities to create a more relaxed atmosphere, and guided discussions to encourage active participation. ③ Both patients and caregivers tended to be reserved or hesitant in expressing their emotions toward each other. To address this, we incorporated demonstration videos illustrating emotional expression into the sessions. Additionally, we encouraged more outgoing individuals from the dyads to initiate emotional interactions first, thereby creating a supportive environment that motivated other participants to gradually engage in emotional expression.
Based on the feedback from two rounds of Delphi expert consultations and the practical outcomes of the pilot trial, the final dyadic psychoeducational intervention program for maintenance hemodialysis patients and their caregivers was developed. The intervention is designed to be delivered in the demonstration room of the hemodialysis center, targeting MHD patient-caregiver dyads. Sessions are scheduled during the pre- or post-dialysis periods, spanning 4 weeks with one session per week, each lasting 30–40 minutes. The format involves offline, face-to-face group sessions, with 6–10 patient-caregiver dyads per group. The specific intervention content, along with importance ratings and variation coefficients, is detailed in Table 1.
Discussion
Necessity of Developing a Dyadic Psychoeducational Intervention for MHD
Patients with chronic kidney disease (CKD) and their caregivers face multifaceted challenges—physiological, psychological, and social—throughout the disease management process. Although existing studies17,18 have confirmed the effectiveness of psychoeducational interventions in improving mental health among individuals with chronic conditions, research focusing specifically on dyadic interventions for maintenance hemodialysis (MHD) patients and their caregivers remains limited. Traditional single-focus intervention models often overlook the interactive dynamics between patients and caregivers. In contrast, dyadic interventions address disease-related stress more comprehensively by enhancing mutual collaboration and support between both parties. Evidence40 indicates that such dyadic interventions can significantly alleviate patients’ depressive symptoms while simultaneously reducing caregivers’ burden—a dual benefit unattainable through individual-focused approaches. Moreover, the long-term and complex nature of MHD treatment means that caregivers themselves are exposed to considerable psychological strain while providing support. Hejazi et al (2022) found that the psychological well-being of caregivers directly influences patients’ treatment adherence and quality of life.41 Therefore, developing a psychoeducational intervention tailored to patient-caregiver dyads not only helps improve psychosocial outcomes for patients but also provides essential support and resources for caregivers, creating a mutually beneficial situation.
The necessity of dyadic intervention is further reflected in its role in strengthening coping strategies and social support. Psychologist Lazarus42 defined coping strategies as behaviors that help individuals manage problems and stress. By integrating psychotherapeutic techniques focused on coping, dyadic interventions guide patients and caregivers to confront the disease proactively, resolve problems constructively, and reduce negative psychological experiences. Social support serves as a crucial resource for both patients and caregivers in dealing with illness-related stress. Dyadic interventions enhance the effective utilization of social support by fostering emotional expression and improving problem-solving abilities within the dyad. For instance, research by Zhu et al (2022) demonstrated that positive interactions between patients and caregivers significantly improved the quality of life for both and reduced disease-related stress.15
These findings provide a solid theoretical and practical foundation for the development of the present intervention program. Therefore, developing a psychoeducational intervention tailored to patient-caregiver dyads may help improve psychosocial outcomes for patients while also providing support and resources for caregivers, potentially creating mutual benefits.
Scientific Rigor of the Developed MHD Dyadic Psychoeducational Intervention
The development of this dyadic psychoeducational intervention followed a systematic process informed by multiple data sources. First, a cross-sectional survey identified factors associated with quality of life and caregiver burden, helping to define intervention targets. Second, an evidence-based review synthesized current literature on psychoeducational approaches in MHD populations. Third, a two-round Delphi expert consultation provided content validation, with high response rates and expert authority supporting the credibility of the process. Finally, a small pilot trial (n=3 dyads) offered preliminary feedback on feasibility and acceptability, though this was not an efficacy evaluation.
Feasibility of the Developed MHD Dyadic Psychoeducational Intervention
The feasibility of this intervention program is supported across theoretical, practical, and implementation dimensions. First, the program is grounded in the Double ABC-X model, which provides a robust theoretical framework. Within this model, social support is conceptualized as a family resource (bB), while anxiety and depression are viewed as reflections of family perception (cC). By strategically addressing these components, the intervention facilitates the development of adaptive coping strategies (BC), ultimately leading to improved quality of life (xX). Previous research[43 applying this model to dyadic interventions has demonstrated its effectiveness in enhancing patient-reported outcomes. Second, the program was developed in direct response to the actual needs of MHD patients and their caregivers. Findings from our situational survey revealed notably low patient quality of life and high caregiver burden, highlighting a strong interdependent relationship within the dyads. This interdependence supports the program’s dyadic approach, enabling synergistic intervention effects. Finally, the evidence-based methodology employed ensured that the intervention content, specific techniques, dosage, and delivery mode are all informed by current best evidence, supporting practicality and applicability in real-world clinical settings.
While the intervention content demonstrates strong feasibility, we acknowledge the logistical challenges of implementing a four-week, face-to-face group program in a busy clinical setting. Coordinating caregivers’ attendance—many of whom have work or family responsibilities—can be difficult. Drawing on our established rapport with patients and their caregivers through long-term dialysis care, we addressed this by scheduling sessions before or after dialysis based on individual preferences, with appointments confirmed in advance. We also provided light refreshments suitable for MHD patients to alleviate hunger after long dialysis hours—a small but meaningful gesture that fostered a supportive and welcoming atmosphere. These strategies improved adherence during the pilot and could be easily integrated into routine practice.
Cultural Context and Generalizability of the Developed MHD Dyadic Psychoeducational Intervention
This study was conducted entirely within a Chinese healthcare context, which may influence the applicability of findings to other settings. In China, family caregiving for older adults with chronic illness is strongly rooted in cultural norms of filial piety, and family involvement in dialysis care is typically high. Additionally, the hospital-based structure of dialysis delivery in China may differ from community-based or home dialysis models in other countries. These cultural and systemic factors may affect both the implementation and effectiveness of dyadic interventions. We therefore recommend that the program be adapted and tested in diverse cultural and healthcare contexts before broader dissemination.
Conclusion
This study developed a theory-driven, content-validated dyadic psychoeducational intervention for MHD patients and their caregivers. The program provides a structured foundation for future research. However, this study has several limitations. The pilot sample was small (n=3 dyads). Although adherence and retention were 100% in this small sample, the absence of structured feasibility metrics (eg., validated acceptability scales, fidelity checklists) limits the generalizability of these findings. Effectiveness was not evaluated. The intervention was developed and tested within a single cultural context (China), which may limit generalizability to other settings with different family structures, caregiving norms, or healthcare systems. Future research should include multicenter randomized controlled trials to evaluate effectiveness, incorporate quantitative feasibility outcomes, and explore cross-cultural adaptation and implementation strategies.
Abbreviations
MHD, Maintenance hemodialysis; CKD, Chronic kidney disease; DALYs, Disability-adjusted life years; ESRD, End-stage renal disease; QoL, Quality of life; MOS-SSS, Medical Outcomes Study Social Support Survey; BCS, Brief COPE Scale; HADS, Hospital Anxiety and Depression Scale; ZBI, Zarit Caregiver Burden Interview; KDQOL-36, Kidney Disease Quality of Life 36-item Short Form; ERS, Emotion Regulation Scale; APIMeM, Actor-Partner Interdependence Model extended to Mediation.
Data Sharing Statement
The authors are willing to permanently share data supporting the results and analysis presented in the paper after publication. The data can be used for scientific research beneficial to human health. The datasets generated during and/or analyzed during the current study are available from the corresponding author on reasonable request.
Ethics Approval and Consent to Participate
The study design and procedures followed the Declaration of Helsinki and were approved by the Ethics Committee of Taizhou People’s Hospital, Jiangsu Province, China (KY2023-184-01). Written informed consent was obtained from each participant who agreed to participate in the study. Participants have the right to withdraw from the study at any time without any negative impact on their usual treatment, care, and other services.
Acknowledgments
Thanks to all the experts who participated in the Delphi expert letter consultation for their efforts in this work.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was supported by the Taizhou Science and Technology Bureau of Jiangsu Province [Grant number TS202311], China.
Disclosure
The authors report there are no competing interests to declare.
References
1. Jones A. Anticoagulation in chronic kidney disease: current status and future perspectives. J Thromb Haemost. 2024;22(2):323–12. doi:10.1016/j.jtha.2023.09.020
2. GBD results. Institute for Health Metrics and Evaluation. 2021. Available from: https://vizhub.healthdata.org/gbd-results.
3. Zhang L, Chen Y, Tang W, Wang Q, Zou L, Zhou L. Effects of dyadic psychoeducational interventions for haemodialysis patients and their family caregivers: a randomised controlled trial. BMC Nurs. 2025;24(1):244. doi:10.1186/s12912-025-02835-1
4. Zhang L, Zou L, Zhou L. Effectiveness of psychoeducational interventions on psychological distress and health-related quality of life among patients with maintenance hemodialysis: a systematic review and meta-analysis. Ren Fail. 2024;46(1):2331613. doi:10.1080/0886022X.2024.2331613
5. Bhandari SK, Zhou H, Shaw SF, et al. Causes of death in end-stage kidney disease: comparison between the United States renal data system and a large integrated health care system. Am J Nephrol. 2022;53(1):32–40. doi:10.1159/000520466
6. Thurlow JS, Joshi M, Yan G, et al. Global epidemiology of end-stage kidney disease and disparities in kidney replacement therapy. Am J Nephrol. 2021;52(2):98–107. doi:10.1159/000514550
7. Chen J, Xiang J, Jie Y, et al. Expert consensus on clinical practice of injection safety in hemodialysis. Chinese Journal of Nursing. 2022;57(7):785–790.
8. Carswell C, Reid J, Walsh I, McAneney H, Lee JB, Noble H. Complex arts-based interventions for patients receiving haemodialysis: a realist review. Arts Health. 2021;13(2):107–133. doi:10.1080/17533015.2020.1744173
9. Bártolo A, Sousa H, Ribeiro O, Figueiredo D. Effectiveness of psychosocial interventions on the burden and quality of life of informal caregivers of hemodialysis patients: a systematic review. Disabil Rehabil. 2022;44(26):8176–8187. doi:10.1080/09638288.2021.2013961
10. Zhang Y, Niu J, Qin H, et al. Prevalence and correlates of depression among maintenance hemodialysis patients in Huhhot region,China:a cross-sectional study (Original in Chinese). Journal of Clinical Nephrology. 2022;22(7):574–583.
11. Al Naamani Z, Gormley K, Noble H, Santin O, Al Maqbali M. Fatigue, anxiety, depression and sleep quality in patients undergoing haemodialysis. BMC Nephrol. 2021;22(1):157. doi:10.1186/s12882-021-02349-3
12. Shirazian S, Grant CD, Aina O, Mattana J, Khorassani F, Ricardo AC. Depression in chronic kidney disease and end-stage renal disease: similarities and differences in diagnosis, epidemiology, and management. Kidney Int Rep. 2017;2(1):94–107. doi:10.1016/j.ekir.2016.09.005
13. Cohen SD, Cukor D, Kimmel PL. Anxiety in patients treated with hemodialysis. Clin J Am Soc Nephrol. 2016;11(12):2250. doi:10.2215/CJN.02590316
14. Al-Nashri F, Almutary H. Impact of anxiety and depression on the quality of life of haemodialysis patients. J Clin Nurs. 2022;31(1–2):220–230. doi:10.1111/jocn.15900
15. Zhu Z, Li P, Chai D, Luan W. Correlation between the frailty of elderly patients on regular haemodialysis and the quality of life of their family caregivers: a cross-sectional evaluation. J Multidiscip Healthc. 2022;15:2321–2330. doi:10.2147/JMDH.S384699
16. Pucciarelli G, Lommi M, Magwood GS, et al. Effectiveness of dyadic interventions to improve stroke patient-caregiver dyads’ outcomes after discharge: a systematic review and meta-analysis study. Eur J Cardiovasc Nurs. 2021;20(1):14–33. doi:10.1177/1474515120926069
17. Iovino P, Rebora P, Occhino G, et al. Effectiveness of motivational interviewing on health-service use and mortality: a secondary outcome analysis of the MOTIVATE-HF trial. ESC Heart Fail. 2021;8(4):2920–2927. doi:10.1002/ehf2.13373
18. Caggianelli G, Iovino P, Rebora P, et al. A motivational interviewing intervention improves physical symptoms in patients with heart failure: a secondary outcome analysis of the motivate-HF randomized controlled trial. J Pain Symptom Manage. 2022;63(2):221–229.e1. doi:10.1016/j.jpainsymman.2021.09.006
19. Chen X. The study of factors affecting self-perceived burden and dyadic coping for colorectal cancer patient-spousal caregiver dyads (Original in Chinese). Master’s thesis. Jiangnan University; 2025. doi:10.27169/d.cnki.gwqgu.2024.000625.
20. Chen S. Construction and Effect Evaluation of Dyadic Intervention Program of Mutuality in Patients with Chronic Heart Failure and Their Spouse Caregivers (Original in Chinese). Doctoral dissertation. Shandong University; 2023. doi:10.27272/d.cnki.gshdu.2022.000355.
21. Mou H, Wong MS, Chien WT. Effectiveness of dyadic psychoeducational intervention for stroke survivors and family caregivers on functional and psychosocial health: a systematic review and meta-analysis. Int J Nurs Stud. 2021;120:103969. doi:10.1016/j.ijnurstu.2021.103969
22. Mccubbin HI, Patterson JM. The family stress process: the double ABCX model of adjustment and adaptation. Marriage Fam Rev. 1983;6(1–2):7–37. doi:doi:10.1300/J002v06n01_02
23. Jones J, Hunter D. Consensus methods for medical and health services research. BMJ. 1995;311(7001):376–380. doi:10.1136/bmj.311.7001.376
24. Duncan E, O’Cathain A, Rousseau N, et al. Guidance for reporting intervention development studies in health research (GUIDED): an evidence-based consensus study. BMJ Open. 2020;10(4):e033516. doi:10.1136/bmjopen-2019-033516
25. Tong A, Sainsbury P, Craig J. Consolidated criteria for reporting qualitative research (COREQ): a 32-item checklist for interviews and focus groups. Int J Quality Health Care. 2007;19(6):349–357. doi:10.1093/intqhc/mzm042
26. Gilliss CL. Family nursing research, theory and practice. Image J Nurs Sch. 1991;23(1):19–22. doi:10.1111/j.1547-5069.1991.tb00629.x
27. Brodaty H, Donkin M. Family caregivers of people with dementia. Dialogues Clin Neurosci. 2009;11(2):217–228. doi:10.31887/DCNS.2009.11.2/hbrodaty
28. Rabelo JL, Cruz BF, Ferreira JDR, de M VB, Barbosa IG. Psychoeducation in bipolar disorder: a systematic review. World J Psychiatry. 2021;11(12):1407–1424. doi:10.5498/wjp.v11.i12.1407
29. Hubler O. Systems under indirect observations - causality - structure - prediction - joreskog,kg, wold,h. Kyklos. 1984;37(2):326–328.
30. Wolf EJ, Harrington KM, Clark SL, Miller MW. Sample size requirements for structural equation models: an evaluation of power, bias, and solution propriety. Educ Psychol Meas. 2013;76(6):913–934. doi:10.1177/0013164413495237
31. Wang LI, YiPing L, ZhongQuan L. Test of emotion regulation scale in adolescents (Original in Chinese). Chin J Clin Psychol. 2007;(3):236–238.
32. Y DSF, L DTF, Jean W. Psychometric testing of the Chinese version of the medical outcomes study social support survey (MOS-SSS-C). Res Nurs Health. 2004;27(2). doi:10.1002/nur.20008
33. Chan DW. Dimensionality and correlates of problem solving: the use of the problem solving inventory in the Chinese context. Behav Res Ther. 2001;39(7):859–875. doi:10.1016/s0005-7967(00)00082-6
34. Tang KNS, Chan CS, Ng J, Yip CH. Action type-based factorial structure of brief COPE among Hong Kong Chinese. J Psychopathol Behav Assess. 2016;38(4):631–644. doi:10.1007/s10862-016-9551-0
35. Leung CM, Ho S, Kan CS, Hung CH, Chen CN. Evaluation of the Chinese version of the hospital anxiety and depression scale. A cross-cultural perspective. Int J Psychosom. 1993;40(1–4):29–34.
36. Lu L, Lie W, Xiaoshi Y, Qiaolian F. Zarit caregiver burden interview: development, reliability and validity of the Chinese version. Psychiat Clin Neurosci. 2009;63(6). doi:10.1111/j.1440-1819.2009.02019.x
37. Yan H, Zhao L, Liu D, NingXiu L. Psychometric properties of SF - 36 and SF - 12 as measures of population health status survey (Original in Chinese). Modern Prevent Med. 2017;44(5):852–862.
38. Hasson F, Keeney S, McKenna H. Research guidelines for the Delphi survey technique. J Adv Nurs. 2000;32(4):1008–1015.
39. Black M, Matthews LR, Millington MJ. Using an adapted delphi process to develop a survey evaluating employability assessment in total and permanent disability insurance claims. Work. 2018;60(4):539–548. doi:10.3233/WOR-182761
40. Wang X, Zang L, Hui X, et al. Dyadic interventions for cancer patient-caregiver dyads: a systematic review and network meta-analysis. Int J Nurs Stud. 2025;161:104948. doi:10.1016/j.ijnurstu.2024.104948
41. Hejazi SS, Hosseini M, Ebadi A, Alavi Majd H. Development and psychometric properties evaluation of caregiver burden questionnaire in family caregivers of hemodialysis patients. BMC Nurs. 2022;21(1):246. doi:10.1186/s12912-022-01025-7
42. Lazarus R. Progress on a cognitive motivational relational theory of emotion. Am Psychol. 1991;46(8):819–834. doi:10.1037/0003-066X.46.8.819
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.