Back to Journals » Journal of Asthma and Allergy » Volume 19
Development and Internal Evaluation of a Clinical-Physiological Model for Predicting Methacholine-Defined Airway Hyperresponsiveness in Children Aged 0–3 Years
Authors Qin J, Liu S, Lin Y, Wang X, Zhao J, Liu F
Received 1 March 2026
Accepted for publication 12 June 2026
Published 17 June 2026 Volume 2026:19 602340
DOI https://doi.org/10.2147/JAA.S602340
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Luis Garcia-Marcos
Jiangjiao Qin,1,2 Sha Liu,1,2 Ying Lin,1,2 Xia Wang,1,2 Jing Zhao,1,2 Fangjun Liu1,2
1Department of Pulmonary Function, Children’s Hospital of Chongqing Medical University, Chongqing, People’s Republic of China; 2National Clinical Research Center for Children and Adolescents’ Health and Diseases; Ministry of Education Key Laboratory of Child Development and Disorders; Chongqing Key Laboratory of Pediatric Metabolism and Inflammatory Diseases, Children’s Hospital of Chongqing Medical University, Chongqing, People’s Republic of China
Correspondence: Fangjun Liu, Department of Pulmonary Function, Children’s Hospital of Chongqing Medical University, Chongqing, People’s Republic of China, Tel +86 15215048191, Fax +86 23-63631510, Email [email protected]
Purpose: Assessing airway hyperresponsiveness (AHR) in children aged 0– 3 years is crucial for early asthma diagnosis but is clinically challenging due to the safety risks and technical complexity of the methacholine challenge test (MCT). This study aimed to develop and internally evaluate a non-invasive, multidimensional nomogram to predict current methacholine-defined AHR in children aged 0– 3 years with suspected asthma.
Patients and Methods: We conducted a retrospective cohort study of children aged 0– 3 years with suspected asthma who underwent same-day tidal breathing pulmonary function testing, fractional exhaled nitric oxide (FeNO) measurement, and MCT. Clinical symptoms and atopic history were extracted from electronic medical records. Multivariable logistic regression was used to identify independent predictors of AHR. The model was internally evaluated using a single 70/30 random split into training and evaluation cohorts. Model performance was assessed by discrimination, calibration, and decision curve analysis and compared with machine-learning approaches.
Results: Seven independent predictors were identified: family history of asthma (OR = 3.90), presence of wheeze (OR = 3.85), history of allergy (OR = 2.34), history of rhinitis (OR = 1.69), FeNO (OR = 1.03), age (OR = 0.96), and TPTEF/TE (OR = 0.97). The model achieved an AUC of 0.81 (95% CI: 0.77– 0.85) in the training cohort and 0.76 (95% CI: 0.69– 0.84) in the evaluation cohort. At the optimal cutoff, the PPV and NPV were 0.89 and 0.39, respectively, in the evaluation cohort. SHAP analysis identified family history of asthma, wheeze, and FeNO as the most influential predictors.
Conclusion: We developed a clinical-physiological nomogram for predicting methacholine-defined AHR in children aged 0– 3 years. It serves as an adjunctive tool in tertiary care to identify patients with a high probability of AHR.
Keywords: methacholine challenge test, tidal breathing, exhaled nitric oxide, nomogram
Introduction
Airway hyperresponsiveness (AHR) is a key physiological feature of childhood asthma. In children aged 0–3 years, assessment of AHR may provide clinically relevant information during a period when respiratory phenotypes are still evolving. Longitudinal studies suggest that bronchial responsiveness can track from infancy into later childhood; however, its clinical relevance may change with age, and early-life AHR should not be considered equivalent to persistent asthma or later AHR.1–3
Several clinical tools have been developed to estimate future asthma risk in young children, including the Asthma Predictive Index and subsequent prediction models.4 These tools address prognosis rather than current airway responsiveness. In contrast, the present study focuses on estimating current methacholine-defined AHR in children aged 0–3 years who cannot reliably perform standard spirometry.
Direct assessment of AHR in this age group remains challenging because methacholine challenge testing requires sedation, close safety monitoring, and age-adapted clinical endpoints.5,6 FeNO measurement is also methodologically difficult because standard single-breath maneuvers are usually not feasible in young children; tidal-breathing FeNO techniques have therefore been applied in infants and young children, but the resulting values should not be interpreted using standard single-breath cutoffs.7 Our previous work showed that FeNO and tidal-breathing pulmonary function parameters are associated with current AHR status in this population.8 Therefore, this study aimed to develop and internally evaluate a clinical-physiological model integrating inflammatory, functional, and clinical factors to estimate the probability of current methacholine-defined AHR in children aged 0–3 years with suspected asthma, as an adjunctive probability-estimation tool prior to provocation testing.
Patients and Methods
Study Design and Participants
This retrospective cohort study was conducted at the Children’s Hospital of Chongqing Medical University and approved by the Research Ethics Committee (No. 2023–371), with waived additional informed consent due to its retrospective nature. Standard clinical consent for procedures (such as MCT) was obtained as part of routine care. We reviewed records of 7957 children who underwent tidal breathing pulmonary function testing (PFT) and methacholine challenge test (MCT) from January 2021 to June 2023. Children who did not complete PFT, MCT, and fractional exhaled nitric oxide (FeNO) measurements on the same day were excluded (n= 6,359), leaving 1,598 children. Further exclusions were applied for lower respiratory tract infection ≤4 weeks or upper respiratory tract infection ≤1 week prior, chest deformities, or confounding diagnoses (eg., nasal disease, congenital airway malformations, suspected gastroesophageal reflux; n=159), resulting in 1,439 children. Inclusion criteria were then applied: (1) aged 0–3 years (ie., from birth to <4 years of age); (2) clinical diagnosis of suspected asthma by a physician on at least two occasions; (3) met GINA 2024 criteria for children ≤5 years (eg., ≥3 exacerbations/year or symptoms persisting >10 days post-upper respiratory infection); (4) in clinical remission, with improvement after ≥2 months of low-dose inhaled corticosteroid (ICS) therapy and no exacerbations ≥4 weeks.9 Children failing to meet these criteria were excluded (n=621), yielding a final cohort of 818 children with suspected asthma. The present study is an extended analysis of an underlying cohort overlapping with our previous physiology-focused study.8 In the current analysis, additional clinical and atopic variables were incorporated to develop an integrated clinical-physiological prediction model. The dataset was randomly split into training (70%; n=572) and evaluation (30%; n=246) cohorts (Figure S1).
Clinical Data and Procedures
All tests were performed on sedated children (oral 10% chloral hydrate, 30–50 mg/kg). Clinical symptoms and history were extracted from electronic medical records. Wheeze was defined as a physician-documented high-pitched expiratory sound in the preceding 12 months; cough was caregiver-reported recurrent dry cough ≥3 times in the past week. To capture a more comprehensive clinical phenotype, we additionally collected data on four history-related variables. History of eczema and rhinitis were defined based on previous physician-documented diagnoses in the electronic medical records. Family history of asthma was defined as a confirmed diagnosis of asthma in a first-degree relative. History of allergy was determined by a history of adverse reactions to specific allergens or positive results in prior allergen-specific IgE or skin prick tests.
FeNO Measurement
FeNO was measured in parts per billion (ppb) using an offline tidal-breathing method under sedation with a Sunvou nitric oxide analyzer (CA2123), in accordance with pediatric ERS/ATS guidance.7,10 A mask was sealed over the nose and mouth, and at least five breaths were collected into a sampling bag after filtering ambient NO.
Tidal Breathing Pulmonary Function Test
Pulmonary Function Test: Parameters were measured using a Jaeger MasterScreenPaed device (CareFusion, San Diego, CA) on supine, sedated children, following ERS/ATS recommendations.11 A compliant mask (CY Xiamen Medical Equipment Co.Ltd. China) ensured airtight seal. After 5–8 regular breaths, end-inspiratory occlusion confirmed sealing. Data were recorded over 5 cycles (15–20 breaths each), accepted if no leakage and coefficient of variation (CV) for tidal volume (VT) ≤10%.
Methacholine Challenge Test
Preparation: Medications were withheld [Short-acting β2-agonists (SABA) ≥6 h, short-acting muscarinic antagonists (SAMA) ≥12 h, long-acting β2-agonists (LABA) ≥36 h, theophylline 12–24 h]; ICS and leukotriene modifiers continued per guidelines. Children with recent infections (≤4 weeks), baseline SpO2 <95%, or abnormal tidal indices (TPTEF/TE or VPTEF/VE ≤23%) were excluded for safety. During MCT, SpO2, heart rate, and respiratory movement were continuously monitored. After completion or termination of the test, bronchodilator treatment was administered, and vital signs were monitored until recovery to baseline.
Procedure: Continuous pulse oximetry (ChoiceMMed SN-type, Chaosi Medical Equipment Co., Ltd., China), heart rate, and respiratory movement monitoring occurred. Methacholine (0.5–16.0 mg/mL in 0.9% NaCl) was nebulized (Bai Ray, China; 5.5 L/min, 0.15 mL/min output, particle diameter 2.9 ± 1 μm) via mask for 1 min/dose.12 Tidal PFT repeated 30–60 s post-inhalation (2-min intervals). Testing ended at positive criteria or 16 mg/mL.
Positive Definition: ≥2 of: (1) auscultated expiratory wheezing; (2) ≥50% respiratory rate increase; (3) ≥5% SpO2 decrease, at ≤8 mg/mL.
Post-test Care: Bronchodilator was nebulized; vital signs monitored until baseline.
Statistical Analysis
Analyses were performed using R version 4.4.1. Missing data for clinical history variables were handled using multivariate imputation by chained equations under the missing-at-random assumption, with 20 imputed datasets. The dataset was randomly split into training (70%) and evaluation (30%) cohorts. Non-normal continuous variables were presented as M (P25-P75) and compared by Mann–Whitney U-test; categorical as n (%). Binary logistic regression with backward stepwise selection (excluding collinear variables) identified independent AHR predictors. Multicollinearity was evaluated using the variance inflation factor (VIF), with values <5 considered acceptable Performance was assessed via discrimination: area under the ROC curve (AUC); calibration: plots and Hosmer-Lemeshow test; clinical utility: decision curve analysis (DCA) for net benefit across thresholds. A complete-case sensitivity analysis using the non-imputed dataset was performed to assess the robustness of the primary imputation-based model. Internal model performance was additionally assessed using 500-resample bootstrap optimism correction on the full dataset. A nomogram was built from the multivariate model, assigning points per predictor; total scores yielded predicted AHR probability. Furthermore, the logistic model was compared against LASSO regression and Random Forest algorithms, with variable importance interpreted using SHAP values. P < 0.05 (two-sided) was significant.
Result
Characteristics of Participants
A total of 818 children with suspected asthma were included. The cohort was split into a training cohort (n = 572) and an evaluation cohort (n = 246).The detailed missing data profile and imputation summary are provided in Table S1. Baseline characteristics were well balanced between the two cohorts, with no significant differences observed across all variables (Table S2). In the training cohort (Table 1), 423 children (73.95%) were AHR-positive. Compared to the AHR-negative group, the positive group showed significantly higher FeNO levels (median 28.0 vs. 20.0 ppb, P < 0.001) and a higher prevalence of wheeze (60.28% vs. 24.83%, P < 0.001). Significant differences were also observed in clinical history, with the AHR-positive group having significantly higher rates of family history of asthma (47.52% vs. 18.12%), history of rhinitis (41.37% vs. 28.86%), and history of allergy (73.05% vs. 50.34%) (all P < 0.05).
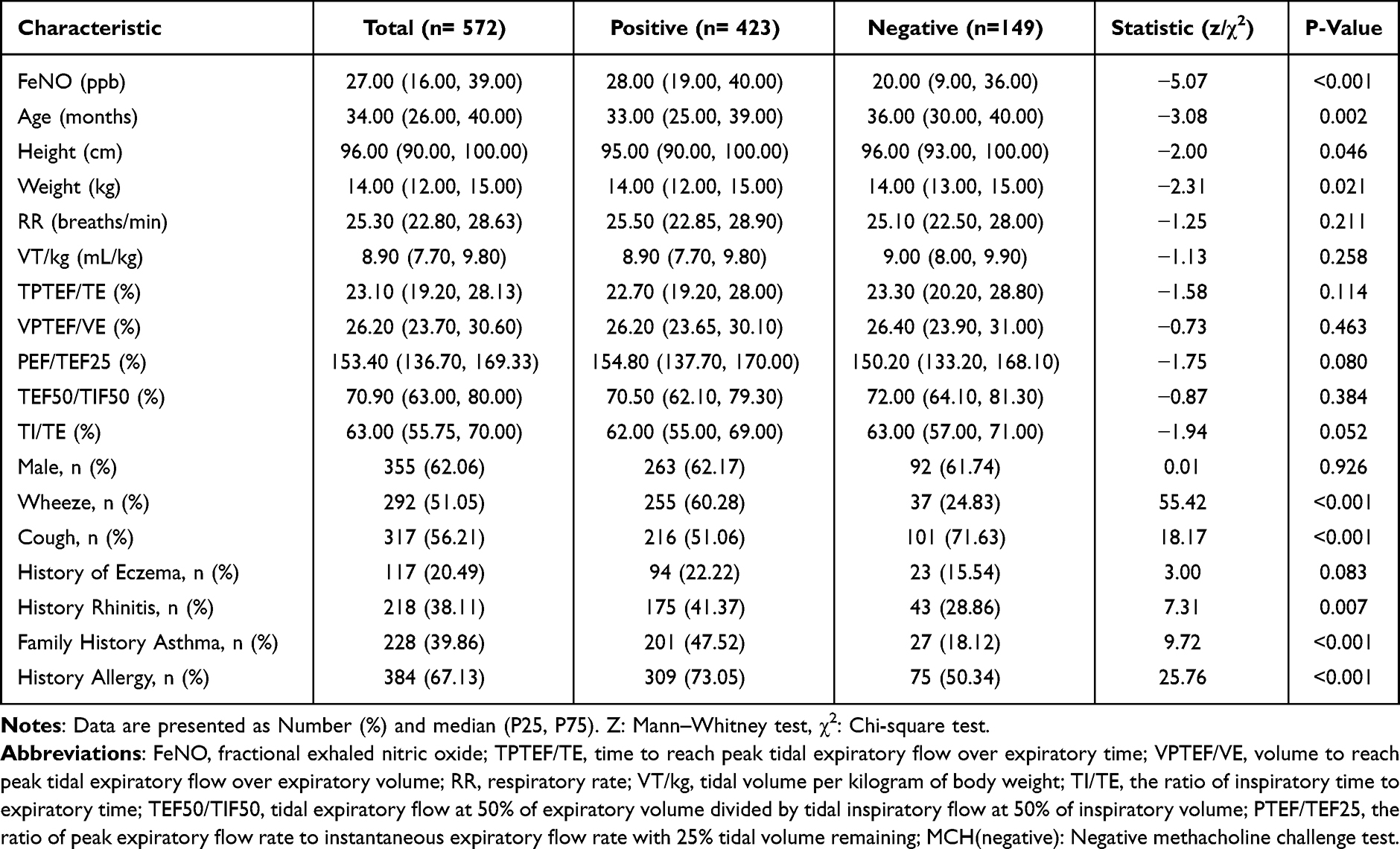 |
Table 1 Statistical Analysis of Basic Characteristics in the Training Cohort |
Independent Predictors of Airway Hyperresponsiveness
The multivariate logistic regression analysis identified several independent predictors for AHR. Among the clinical history factors, a family history of asthma showed the strongest association with AHR risk (OR = 3.90, 95% CI: 2.33–6.51, P < 0.001). Significant associations were also observed for a history of allergy (OR = 2.34, P < 0.001) and rhinitis (OR = 1.69, P = 0.029). Regarding symptom and physiological parameters, the presence of wheeze was associated with an increased likelihood of AHR (OR = 3.85, P < 0.001). Conversely, age (OR = 0.96, P = 0.006) and TPTEF/TE (OR = 0.97, P = 0.028) were negatively associated with AHR risk, alongside a significant contribution from FeNO levels (OR = 1.03, P < 0.001). Detailed regression coefficients and odds ratios for all included variables are presented in Table 2 and Table S3.
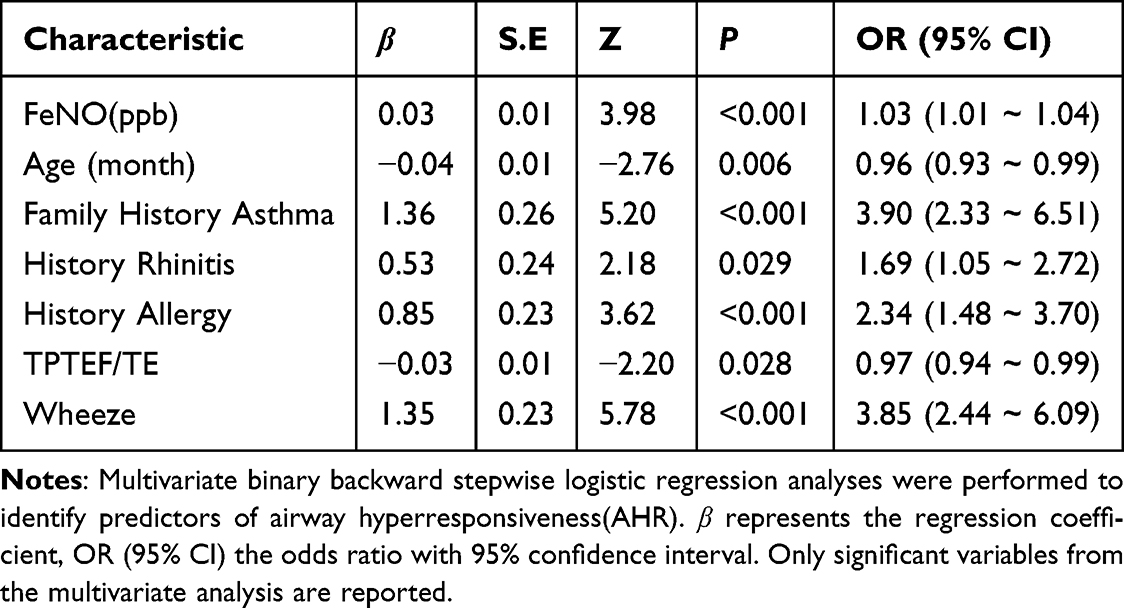 |
Table 2 Binary Backward Stepwise Logistic Regression Analysis of AHR |
Performance and Evaluation of the Predictive Model
The 7-parameter model achieved an AUC of 0.81 (95% CI: 0.77–0.85) in the training cohort and 0.76 (95% CI: 0.69–0.84) in the evaluation cohort (Table 3). A complete-case sensitivity analysis using the non-imputed dataset showed slightly attenuated but comparable discrimination, with an AUC of 0.77 (95% CI: 0.74–0.80) in the training cohort and 0.73 (95% CI: 0.69–0.78) in the evaluation cohort. In addition, 500-resample bootstrap optimism-corrected validation using the full dataset yielded a corrected C-index of 0.76. At the optimal cutoff of 0.762, the model yielded a specificity of 0.69 and an NPV of 0.39 in the evaluation set. Calibration curves and decision curve analyses are shown in Figure 1. The decision curve analysis suggested potential net benefit across a range of threshold probabilities (Figure 1A and C), while calibration curves indicated reasonable agreement between predicted and observed probabilities (Figure 1B and D). The corresponding nomogram is presented in Figure 2.
 |
Table 3 Discriminative Performance of the Nomogram for Predicting Methacholine-Defined AHR in Training and Evaluation Cohorts |
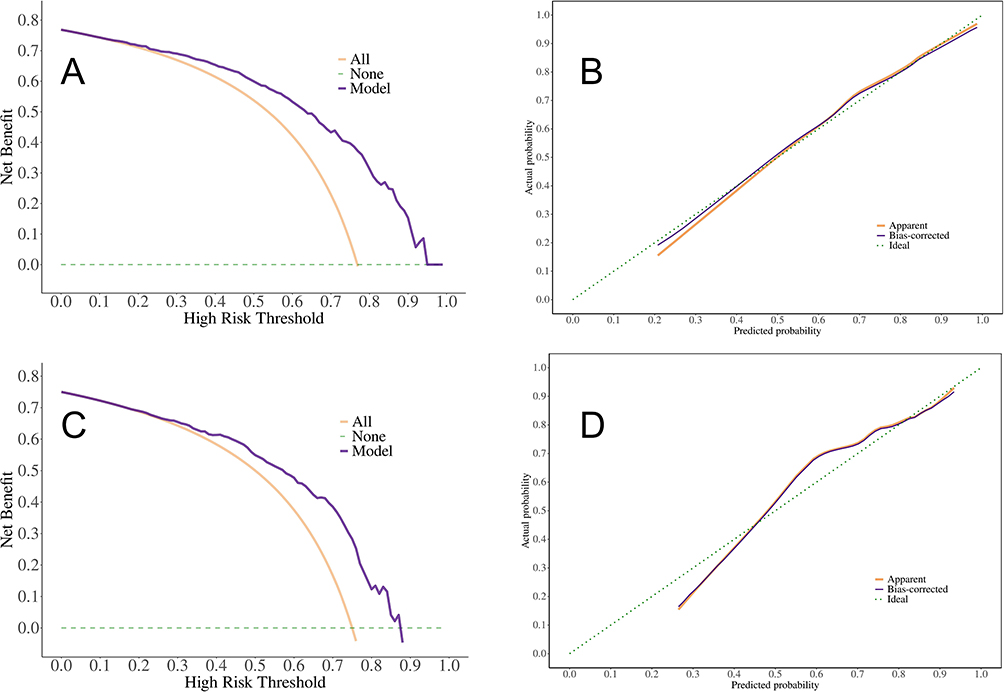 |
Figure 1 Decision curve analyses and calibration curves for the training and evaluation cohorts. Notes: (A) Decision curve analysis (DCA) in the training cohort. The Y-axis indicates net benefit. The solid line represents the clinical net benefit of using the prediction model across threshold probabilities. The grey dashed line assumes all patients are positive; the horizontal line assumes none are positive. The model showed potential net benefit across threshold probabilities of 0.25–0.8. (B) Calibration curve of the training cohort. The diagonal dashed line represents the ideal prediction. The red line indicates the apparent performance of the model on the training data, and the blue line shows the bias-corrected performance via bootstrap resampling (1,000 iterations). Hosmer–Lemeshow test: p=0.249. (C) Decision curve analysis in the evaluation cohort. (D) Calibration curve of the evaluation cohort, with similar annotation as in (B). Hosmer–Lemeshow test: p=0.241. |
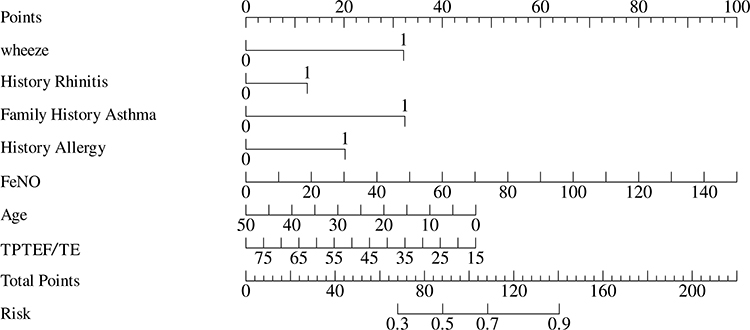 |
Figure 2 Nomogram for predicting airway hyperresponsiveness risk based on combined parameters. Notes: The nomogram integrates seven independent predictors (FeNO, Age, Family History of Asthma, History of Rhinitis, History of Allergy, TPTEF/TE, and Wheeze) to predict the risk of airway hyperresponsiveness (AHR). To use the nomogram, locate the value of each parameter on its respective axis, draw a vertical line upward to the Points axis to determine the score for that variable, and then sum the scores for all seven variables. Find the resulting Total Points on the bottom axis to obtain the individualized predicted probability of AHR. |
Machine Learning Model Comparison
In the evaluation cohort, the AUC of the 7-parameter logistic model (0.756) was comparable to LASSO (0.754) and Random Forest (0.792) (Table S4). SHAP analysis confirmed that family history of asthma, wheeze, and FeNO were the top three contributors to the AHR prediction (Figure S2).
Discussion
Our study developed a clinical-physiological model to estimate current methacholine-defined AHR in children aged 0–3 years with suspected asthma. The model integrates clinical, inflammatory, and tidal-breathing parameters and should be interpreted as an adjunctive probability-estimation tool rather than as an alternative to MCT.
Markers of atopic predisposition emerged as the strongest predictors of AHR. A family history of asthma, personal history of allergy, and history of rhinitis were each independently associated with increased AHR risk. These variables capture complementary aspects of inherited susceptibility13,14 and atopic phenotype,15,16 which may contribute to airway inflammation and heightened reactivity. Biologically, these historical markers represent a stable baseline of cumulative susceptibility anchored in epithelial barrier dysfunction.17 This impairment facilitates allergen penetration and triggers Type-2 inflammatory pathways, increasing susceptibility to persistent airway inflammation and heightened reactivity. By incorporating these variables, our model reflects underlying allergic and inflammatory vulnerability more effectively than cross-sectional physiological measurements alone.18
FeNO emerged as a relevant biomarker reflecting the inflammatory component of AHR. In our study, FeNO showed a statistically significant but modest association with methacholine-defined AHR (OR per 1 ppb increase = 1.03), consistent with evidence that airway inflammation contributes to, but does not solely determine, responsiveness to direct bronchoconstrictor stimuli.19 TPTEF/TE was retained as a tidal-breathing marker reflecting baseline airway mechanics rather than as a direct measure of airway obstruction.20,21 The combined inclusion of FeNO and TPTEF/TE allows the model to integrate inflammatory and functional information, consistent with previous studies linking FeNO to pediatric asthma-related phenotypes22 and supporting the combined use of pulmonary function parameters and FeNO for AHR assessment.23,24 This study builds on our previous work by adding clinical symptoms and atopic history to the model. Because the variables included in the model differ from those in our previous analysis, the role of TPTEF/TE should be interpreted cautiously and confirmed in external cohorts.
The inclusion of age and history of wheeze adds a critical temporal and phenotypic dimension to AHR risk assessment. In our study, increasing age (in months) was inversely associated with AHR, suggesting that airway hyperresponsiveness in the first three years of life is a dynamic and age-dependent phenotype rather than a fixed trait.25 This finding is consistent with longitudinal cohort studies showing that early-life airway responsiveness and wheezing symptoms may diminish with somatic growth and airway maturation, as increases in airway caliber reduce the mechanical consequences of bronchoconstriction.26 Wheeze emerged as a predictor of AHR, reflecting airflow limitation and dynamic airway narrowing that are core physiological features of airway hyperresponsiveness. Evidence from longitudinal cohorts indicates that early-life wheeze, particularly in the presence of atopy, is associated with persistent AHR, whereas isolated cough is largely nonspecific.27,28 Together with age, wheeze helps characterize the evolving clinical phenotype of AHR in early childhood.
Taken together, these findings clarify the intended role of the present model. Unlike prognostic tools that estimate future asthma risk, such as the Asthma Predictive Index,29 this model focuses on estimating the probability of current methacholine-defined AHR in children aged 0–3 years who cannot reliably perform standard spirometry. These approaches address different clinical questions and should not be directly compared. By integrating tidal-breathing parameters, FeNO, and atopic history, our nomogram provides an adjunctive probability-estimation tool for this specific population. For transparency and reproducibility, the web-based calculator is publicly available at: https://ahr-nomogramgit-qjj.streamlit.app/.
This study has several limitations. First, its retrospective, single-center design and the selected tertiary-care population of sedated children aged 0–3 years in clinical remission on ICS therapy limit generalizability to broader clinical settings. The high AHR positivity rate and low NPV in the evaluation cohort further indicate that the model is more suitable for identifying children with a higher probability of AHR than for general screening or AHR exclusion. Second, the MCT outcome was defined using age-adapted composite clinical endpoints rather than the conventional PC20-FEV1 criterion. Inter-rater reliability for auscultated wheeze and the incidence of minor or transient sedation-related adverse events could not be assessed retrospectively. Third, FeNO was measured using an offline tidal-breathing method under sedation and should not be directly compared with standard single-breath cutoffs; the absence of synchronized specific IgE or skin prick testing also limited detailed evaluation of atopic status. Finally, the use of backward stepwise selection may have affected predictor stability. Although bootstrap optimism correction supported the overall discrimination of the model, the contribution of individual tidal-breathing parameters and the generalizability of the model require prospective external validation.
In summary, this study developed and internally evaluated a clinical-physiological model for estimating the probability of current methacholine-defined AHR in children aged 0–3 years with suspected asthma. By integrating clinical, inflammatory, and tidal-breathing parameters, the model provides an exploratory adjunctive approach for identifying children with a higher probability of AHR in selected tertiary-care settings. Prospective external validation and further standardization of age-adapted MCT endpoints are required before broader clinical application.
Ethical Approval
This study was approved by the Research Ethics Committee of the Children’s Hospital of Chongqing Medical University (Approval No. 2023-371) and was conducted in accordance with the Declaration of Helsinki. Because this retrospective analysis used routinely collected clinical data, the requirement for additional informed consent for medical-record review was waived by the Ethics Committee. Standard clinical consent for procedures performed as part of routine care was obtained. Patient data were handled confidentially and analyzed in de-identified form.
Acknowledgments
Thank you to the Department of Respiratory Medicine, Children’s Hospital of Chongqing Medical University, for providing clinical and theoretical support.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Hallas HW, Chawes BL, Rasmussen MA. et al. Airway obstruction and bronchial reactivity from age 1 month until 13 years in children with asthma: a prospective birth cohort study. PLoS Med. 2019;16(1):e1002722. doi:10.1371/journal.pmed.1002722
2. Cox DW, Mullane D, Zhang GC, et al. Longitudinal assessment of airway responsiveness from 1 month to 18 years in the PIAF birth cohort. Eur Respir J. 2015;46(6):1654–9. doi:10.1183/13993003.00397-2015
3. Lajunen KT, Malmberg LP, Kalliola S, Kotaniemi-Syrjänen A, Pelkonen AS, Mäkelä MJ. Predictive value of childhood airway hyper-responsiveness to indirect stimuli: 10-year longitudinal study. Pediatr Allergy Immunol. 2020;31(7):767–773. doi:10.1111/pai.13248
4. Kothalawala DM, Kadalayil L, Weiss VBN, et al. Prediction models for childhood asthma: a systematic review. Pediatr Allergy Immunol. 2020;31(6):616–627. doi:10.1111/pai.13247
5. Stewart L, Miyazawa N, Covar R, et al. Wheeze is an unreliable endpoint for bronchial methacholine challenges in preschool children. Pediatr Allergy Immunol. 2022;33(4):e13767. doi:10.1111/pai.13767
6. Caussade S, Castro-Rodriguez JA, Contreras S, et al. Methacholine challenge test by wheezing and oxygen saturation in preschool children with asthma. Allergol Immunopathol. 2015;43(2):174–179. doi:10.1016/j.aller.2014.02.005
7. Baraldi E, de Jongste JC. European Respiratory Society/American Thoracic Society Task Force. Measurement of exhaled nitric oxide in children, 2001. Eur Respir J. 2002;20(1):223–237. doi:10.1183/09031936.02.00293102
8. Qin J, Liu F, Wang T, et al. Correlation between tidal breathing pulmonary function, exhaled nitric oxide and airway hyperresponsiveness in children aged 0–3 years with suspected asthma. Front Pediatr. 2025;13:1388951. doi:10.3389/fped.2025.1388951
9. Global Initiative for Asthma. Global Strategy for Asthma Management and Prevention. 2024. Available from: https://ginasthma.org/.
10. Daniel PF, Klug B, Valerius NH. Measurement of exhaled nitric oxide in young children during tidal breathing through a facemask. Pediatr Allergy Immunol. 2005;16(3):248–253. doi:10.1111/j.1399-3038.2005.00209.x
11. Bates JH, Schmalisch G, Filbrun D, Stocks J. Tidal breath analysis for infant pulmonary function testing. ERS/ATS Task Force on Standards for Infant Respiratory Function Testing. Eur Respir J. 2000;16(6):1180–1192.
12. Cockcroft DW, Davis BE, Smycniuk AJ. Development of a methacholine challenge method to minimize methacholine waste. Chest. 2003;124(4):1522–1525. doi:10.1378/chest.124.4.1522
13. Stick SM, Burton PR, Gurrin L, Sly PD, LeSouëf PN. Effects of maternal smoking during pregnancy and a family history of asthma on respiratory function in newborn infants. Lancet. 1996;348(9034):1060–1064. doi:10.1016/s0140-6736(96)04446-7
14. Postma DS, Boezen HM. Rationale for the Dutch hypothesis. Allergy and airway hyperresponsiveness as genetic factors and their interaction with environment in the development of asthma and COPD. Chest. 2004;126(2):96S–104S. doi:10.1378/chest.126.2_suppl_1.96S
15. Kelly KJ. Eosinophils and the Scope of Practice in Allergy/Immunology. J Allergy Clin Immunol Pract. 2018;6(5):1506–1507. doi:10.1016/j.jaip.2018.07.016
16. Liu Y, Sha J, Meng C, Zhu D. Mechanism of Lower Airway Hyperresponsiveness Induced by Allergic Rhinitis. J Immunol Res. 2022;2022:4351345. doi:10.1155/2022/4351345
17. Bradding P, Porsbjerg C, Côté A, Dahlén SE, Hallstrand TS, Brightling CE. Airway hyperresponsiveness in asthma: the role of the epithelium. J Allergy Clin Immunol. 2024;153(5):1181–1193. doi:10.1016/j.jaci.2024.02.011
18. Choi SH, Yoo Y, Yu J, Rhee CS, Min YG, Koh YY. Bronchial hyperresponsiveness in young children with allergic rhinitis and its risk factors. Allergy. 2007;62(9):1051–1056. doi:10.1111/j.1398-9995.2007.01403.x
19. Cockcroft DW, Davis BE. Mechanisms of airway hyperresponsiveness. J Allergy Clin Immunol. 2006;118(3):551–559. doi:10.1016/j.jaci.2006.07.012
20. Dweik RA, Boggs PB, Erzurum SC, et al. An official ATS clinical practice guideline: interpretation of exhaled nitric oxide levels (FENO) for clinical applications. Am J Respir Crit Care Med. 2011;184(5):602–615. doi:10.1164/rccm.9120-11ST
21. Lavizzari A, Zannin E, Ophorst M, et al. Tidal Breathing Measurements in Former Preterm Infants: a Retrospective Longitudinal Study. J Pediatr. 2021;230:112–118.e4. doi:10.1016/j.jpeds.2020.11.050
22. Brussee JE, Smit HA, Kerkhof M, et al. Exhaled nitric oxide in 4-year-old children: relationship with asthma and atopy. Eur Respir J. 2005;25(3):455–461. doi:10.1183/09031936.05.00079604
23. Yang H, Zhao X, Chen Z, et al. Innovative machine learning-based prediction of early airway hyperresponsiveness using baseline pulmonary function parameters. Front Med. 2025;12. doi:10.3389/fmed.2025.1611683
24. Bougard N, Nekoee H, Schleich F, et al. Assessment of diagnostic accuracy of lung function indices and FeNO for a positive methacholine challenge. Biochem Pharmacol. 2020;179:113981. doi:10.1016/j.bcp.2020.113981
25. Le Souëf PN. Validity of methods used to test airway responsiveness in children. Lancet. 1992;339(8804):1282–1284. doi:10.1016/0140-6736(92)91602-5
26. Martinez FD, Wright AL, Taussig LM, Holberg CJ, Halonen M, Morgan WJ. Asthma and wheezing in the first six years of life. N Engl J Med. 1995;332(3):133–138. doi:10.1056/NEJM199501193320301
27. Garden FL, Simpson JM, Mellis CM, Marks GB. CAPS Investigators. Change in the manifestations of asthma and asthma-related traits in childhood: a latent transition analysis. Eur Respir J. 2016;47(2):499–509. doi:10.1183/13993003.00284-2015
28. Määttä AM, Malmberg LP, Pelkonen AS, Mäkelä MJ. The link between early childhood lower airway symptoms, airway hyperresponsiveness, and school-age lung function. Ann Allergy Asthma Immunol. 2024;132(1):54–61.e5. doi:10.1016/j.anai.2023.10.006
29. Castro-Rodríguez JA, Holberg CJ, Wright AL, Martinez FD. A clinical index to define risk of asthma in young children with recurrent wheezing. Am J Respir Crit Care Med. 2000;162(4 Pt):1403–1406. doi:10.1164/ajrccm.162.4.9912111
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.