Back to Journals » Journal of Multidisciplinary Healthcare » Volume 18
Development and Implementation of a Clinical Decision Support System to Enhance Efficiency and Accuracy in Medication Prescription Review in a Tertiary Care Hospital: A Retrospective Hospital CDSS Register Study
Authors Lin M, He Y, He P, Jiang H, Luo H, Dai H ![]() , Yu L
, Yu L ![]()
Received 11 November 2024
Accepted for publication 14 February 2025
Published 21 February 2025 Volume 2025:18 Pages 1043—1051
DOI https://doi.org/10.2147/JMDH.S505889
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr David C. Mohr
Meili Lin,1 Yi He,1 Ping He,1 Hongyan Jiang,1 Huan Luo,1 Haibin Dai,1,2 Lingyan Yu1,2
1Department of Pharmacy, Second Affiliated Hospital, Zhejiang University School of Medicine, Hangzhou, Zhejiang Province, People’s Republic of China; 2Research Center for Clinical Pharmacy, Zhejiang University, Hangzhou, Zhejiang Province, People’s Republic of China
Correspondence: Haibin Dai; Lingyan Yu, Department of Pharmacy, Second Affiliated Hospital, Zhejiang University School of Medicine, 88th Jiefang Road, Hangzhou, Zhejiang, People’s Republic of China, Email [email protected]; [email protected]
Background: The integration of Clinical Decision Support Systems (CDSSs) into the prescription review process is expected to mitigate medication errors and increase patient safety. This study aimed to quantify the impact of integrating the CDSS into the prescription review process.
Methods: This retrospective study was conducted by pharmacists at a 3200-bed tertiary hospital in China, leveraging data from the Hospital Information System and CDSS software across two distinct periods: August 2021 to July 2022 (preimplementation) and August 2022 to July 2023 (postimplementation). The chi-square test was used to compare the proportions of medication alerts and patients receiving alerts, both overall and per ward, before and after implementation. The chi-square test was also used to assess the significance of differences in medication alert deviations and pharmacist interventions between the two groups.
Results: During the pre- and postimplementation periods, 5,170,765 and 5,804,595 medication orders were prescribed, respectively. Among these, 130,286 (2.52%) and 133,562 (2.30%) prescriptions triggered alerts, indicating a significant reduction in the alert rate of 0.22% (aHR=0.911, 95% CI 0.904– 0.918; P< 0.001). Difference in the distribution of the top ten medication alert categories was observed between the two periods. In the pre- and postimplementation groups, 208,356 and 218,165 patients were prescribed medication, respectively. Among them, 63,219 (30.34%) and 61,258 (28.08%) patients received alerts, respectively, showing a significant reduction of 2.26% (aHR=0.896, 95% CI 0.885– 0.908; P< 0.001). Among the clinical wards, 66.09% (76 out of 115) showed significant differences in the proportion of patients receiving alerts between the pre- and postimplementation periods (P< 0.05). Specifically, 45.22% (52 out of 115) of these wards experienced a decrease in the proportion of patients receiving alerts, whereas a smaller percentage, 20.87% (24 out of 115), experienced an increase.
Conclusion: CDSSs are invaluable tools for hospital pharmacists and physicians, assisting in the complex task of prescription review.
Keywords: CDSS, prescription review, medication alerts, patient safety
Introduction
Prescribing medication is a fundamental but risky part of healthcare, with high potential for error. Approximately 50% of hospital inpatients were exposed to at least one prescription error during their stay.1 Medication errors are common in hospitals and other healthcare settings and threaten patient safety.2,3 These errors range from incorrect dosages and incorrect medications to treatments that interact dangerously with existing conditions.4,5 Medication misuse contributes to adverse drug events (ADEs), which might lead to increased morbidity, mortality, and healthcare costs.6–8 These errors often result from human factors, systemic issues, and communication breakdowns.9,10 Addressing these challenges requires systematic and evidence-based approaches. A multifaceted approach is needed, including improving medication management systems, enhancing healthcare professional training, and implementing strong safety protocols.11
Clinical decision support systems (CDSSs) were initially designed more than 50 years ago to enhance optimal problem-solving and decision-making capabilities.12 In the past two decades, the CDSS has evolved to support healthcare professionals by delivering real-time, patient-specific information and recommendations. These sophisticated systems analyze a wide array of patient medical data, including demographics, diagnoses, laboratory results, and current medications, to pinpoint potential issues such as drug‒drug interactions, drug‒disease contraindications, and inappropriate dosing.13,14 By harnessing advanced algorithms and clinical knowledge databases, the CDSS could effectively flag potential problems and propose alternative treatment options. This not only reduces the risk of ADEs but also significantly improves patient care.15,16
Despite their potential benefits, the integration of the CDSS presents substantial challenges, particularly concerning fatigue and data quality concerns. Research has indicated a median of 3 alerts per patient per hospital stay, with only approximately 4 out of 100 patients experiencing a change in practice.17 The inundation of excessive and often trivial alerts can lead to clinicians becoming desensitized and succumbing to alert fatigue. This may inadvertently result in the overlooking of crucial warnings.18 Consequently, the precision of CDSS recommendations is critically dependent on the quality and completeness of the input data, as well as the system’s ability to accurately interpret complex clinical scenarios.19,20
In our hospital, commercial CDSS software was integrated into the hospital’s information system in July 2020. Over two years, the system had a high rate of irrelevant medication alerts, affecting the prescription review process. The clinical pharmacists Lingyan Yu and Pin He led efforts to optimize the triggering sensitivity of the CDSS. They worked with a clinical medication knowledge database and an evaluation system. This database includes a basic knowledge base, drug data, manuals, references, and constantly updated rules for rational drug use. To improve audit rules, drug information was preprocessed for standardization, including deduplication, cleaning, normalization, coding, and translation. Customized rules promoting rational drug use were added to the system, including 1,946 drug-related rule sets with 161,608 individual rules, 111 administrative rules, 24 analytical rule sets with 59 rules, and 90 regime-relative rules. These rules were categorized and ranked from grade 5 to grade 8. Grade 8 was for strictly prohibited orders, determined by a rules-formulating committee, involving drug contraindications and incompatibilities. Grade 7 was for rule testing by the pharmacists. Grades 5 and 6 triggered alerts to remind prescribers and pharmacists, promoting rational medication use.
In this article, we outline the CDSS-guided prescription process (as shown in Figure 1). When a medication order is placed, the system activates rules related to the prescribed drugs. If a 5- or 6-grade alert is triggered, a pop-up window immediately notifies the prescriber, who can either adjust the prescription or override the alert by selecting a reason from a dropdown menu. Orders triggering an 8-grade alert are blocked and must be modified to prevent the prescription of critically irrational medications. Once nurses execute prescriptions, pharmacists can review them in the whole-scope system. The CDSS automatically analyzes prescriptions, with red lights indicating inappropriateness and necessitating intervention by a qualified pharmacist.
 |
Figure 1 Workflow of the prescription and review process guided by CDSS data analysis. |
This study aimed to evaluate the effectiveness of integrating CDSS software into the prescription review process and the role of pharmacists in this collaboration. The goal was to enhance pharmacy operations by identifying areas for improvement in current protocols. Our mission was to continuously improve pharmacy practices by addressing and correcting deficiencies, thereby ensuring high-quality patient care.
Methods
Study Setting
This study was conducted at the Second Affiliated Hospital, Zhejiang University School of Medicine, a tertiary care hospital in eastern China, with 3200 licensed beds.
Study Design
This retrospective study involved a prescription review center established in August 2022. The center was staffed by nine senior pharmacists, who were certified in prescription review, and fourteen clinical pharmacists, all of whom were trained in clinical pharmacy. They worked in shifts, with four on duty daily, to provide drug recommendations and address drug-related issues.
In the comprehensive review system, prescriptions deemed irrational were flagged with a red-light indicator. Double-clicking a flagged prescription revealed a pop-up with detailed error notes and treatment suggestions, enabling efficient pharmacist review. When uncertain, pharmacists could right-click to access a context menu, allowing them to assess prescription appropriateness and communicate with prescribers to prevent errors (as shown in Figure 2).
 |
Figure 2 Interface of the whole-scope prescription review system. In the whole-scope prescription review system, all of the patients’ prescriptions, including oral, intravenous, and topical medications, were indexed and displayed on a computer screen. The Clinical Decision Support Systems (CDSS) automatically assessed the appropriateness of the medications, and prescriptions deemed irrational were flagged with a red-light indicator. The patient’s profile, including sex, age, weight, body surface area, allergies, diagnoses, renal function, and abnormal laboratory test results, was presented on the lower part of the screen for pharmacists to review. Additionally, the pharmacists could right-click to access the patients’ database to determine whether advanced intervention was necessary. |
The period from August 2021 to July 2022 was the preimplementation group, and August 2022 to July 2023 was the postimplementation group. The inclusion criteria were as follows: (1) all new prescriptions issued during the study period and (2) all inpatients admitted during the implementation phase. The exclusion criterion included wards that were temporarily open in only one group, excluding them from the analysis of differences in wards with patients who received alerts in the pre- and postimplementation groups.
Data Collection
Data encompassing the total volume of new prescriptions dispensed, the aggregate patient population, and the total patient count within each ward were collected from the Hospital Information System by an information technology engineer. The number of specific prescriptions that triggered medication alerts, the number of patients who received alert notifications, the number of patients receiving alerts within each ward, and the top ten medication alert categories were compiled via CDSS software for the periods before and after the system’s implementation. Additionally, the interventions initiated by the pharmacists were meticulously recorded and summarized for both the pre- and postimplementation groups.
Analysis
All the statistical analyses were conducted via SPSS version 23.0. The chi-square test was employed to assess the differences in the proportions of medication alerts and the proportions of patients who received alerts, both overall and within each ward, between the preimplementation group and the postimplementation group. Additionally, the chi-square test was used to evaluate the significance of variations in the types of medication alert deviations and the interventions made by pharmacists between the two groups. A p value <0.05 was established as the threshold for statistical significance.
Results
Proportions of Medication Alerts
In the comparative analysis between the preimplementation and postimplementation phases, our study examined a substantial volume of medication orders. During the preimplementation period, a total of 5,170,765 medication orders were prescribed, resulting in 130,286 medication alerts being triggered, which accounted for 2.52% of the total orders. In contrast, after the implementation of the enhanced prescription review process, which was assisted by pharmacists and supported by the CDSS database, 5,804,595 medication orders were recorded, with 133,562 alerts triggered, reflecting a 2.30% rate. This shift represented a notable reduction in the frequency of medication alerts. The observed decrease in the percentage of alerts, 0.22%, was statistically significant (aHR =0.911, 95% CI 0.904–0.918; P<0.001), indicating that the interventions and refinements to the CDSS software had a positive effect on the prescription review process, as shown in Table 1.
 |
Table 1 The Proportions of Medication Alerts in the Pre- and Postimplementation Groups |
Top ten Categories of Medication Alerts
There was a notable difference in the percentage of alerts for inadequate usage and dosage, with 30.38% before stratification compared with 23.43% after stratification, indicating a statistically significant reduction (aHR=0.701, 95% CI 0.689–0.714; P<0.001). The percentage of alerts for untreated indications was greater after stratification, with 27.10% before and 29.84% after stratification, indicating a significant increase (aHR=1.144, 95% CI 1.125–1.163; P<0.001). The number of alerts for drug duplication increased significantly, from 9.95% to 12.90% (aHR=1.341, 95% CI 1.309–1.374; P<0.001).There was a significant decrease in alerts for drug-drug interactions, from 7.26% to 5.09% (aHR=0.684, 95% CI 0.663–0.707; P<0.001). A significant reduction in incompatibility alerts was observed, dropping from 6.86% to 3.10% (aHR=0.435, 95% CI 0.419–0.452; P<0.001). The number of alerts for inappropriate administration routes significantly decreased, from 5.46% to 2.64% (aHR=0.470, 95% CI 0.451–0.489; P<0.001). There was a significant increase in alerts regarding renal adjustment, from 5.30% to 11.97% (aHR=2.427, 95% CI 2.357–2.500; P<0.001). A slight but statistically significant difference was noted in treatment duration, with a decrease from 2.75% to 2.61% (aHR=0.946, 95% CI 0.902–0.992; P=0.021). The number of alerts for contraindications increased significantly, from 2.73% to 3.54% (aHR=1.304, 95% CI 1.248–1.363; P<0.001). There was a substantial increase in alerts for inappropriate medication regimens, from 1.68% to 4.38% (aHR=2.677, 95% CI 2.547–2.814; P<0.001) (Table 2).
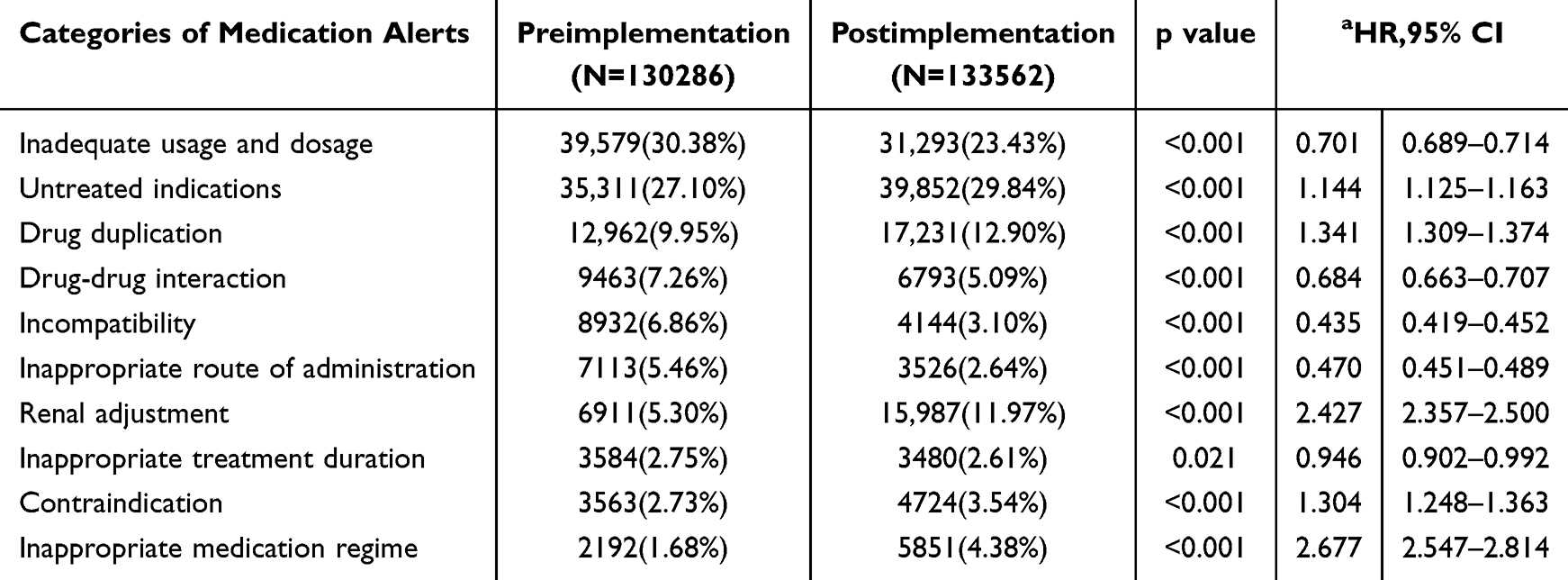 |
Table 2 The Top ten Categories of Medication Alerts Triggered in the Pre- and Postimplementation Groups |
Proportions of Patients Who Received Alerts and Interventions
In the preimplementation group, a total of 208,356 patients were prescribed medication, 63,219 (30.34%) of whom received medication alerts. In contrast, the postimplementation group consisted of 218,165 patients, with 61,258 (28.08%) receiving alerts. The difference in the percentage of patients receiving alerts between the two groups was statistically significant, with a 2.26% decrease after implementation (aHR=0.896, 95% CI 0.885–0.908; P<0.001), as detailed in Table 3.
 |
Table 3 The Proportions of Patients Who Received Alerts and Interventions in the Pre- and Postimplementation Groups |
Additionally, the pharmacists carried out advanced interventions in 4598 (2.21%) patients in the preimplementation group and in 4765 (2.18%) patients in the postimplementation group. A slight decrease in the percentage of advanced interventions postimplementation was also noted, as shown in Table 3.
Clinical Wards with Patients Who Received Alerts in the Pre- and Postimplementation Groups
The data collected and analyzed from clinical wards, as depicted in Figure 3, revealed significant changes in the proportions of patients receiving alerts. In the preimplementation group, a substantial majority of the wards, 66.09% (76 out of 115), presented a statistically significant difference in the proportion of patients with alerts (P < 0.05). Among these wards, 45.22% (52 out of 115) experienced a reduction in the proportion of patients receiving alerts, whereas a smaller percentage, 20.87% (24 out of 115), experienced an increase.
 |
Figure 3 Performance of clinical wards in terms of the patients who received alerts in the pre- and postimplementation groups. |
Discussion
In this study, we presented the integration of the CDSS into hospital prescription review processes. This integration significantly bolstered the efficiency of the review process by automating the detection of common errors, thereby enabling clinicians to devote more attention to more complex cases.21,22 Consistent with other studies, the medication alerts generated by the CDSS were meticulously categorized into various types on the basis of detailed drug-related issues. These issues include improper usage and dosage, untreated indications, drug duplication, drug‒drug interactions, incompatibility, etc.14 Several studies have highlighted that such improper medication use is a crucial factor contributing to adverse drug events (ADEs) in emergency departments.23 The implementation of the CDSS may serve as an effective strategy to mitigate these risks substantially. Particularly in outpatient care settings or settings with limited resources, the CDSS can offer vital support to healthcare providers during consultations. Studies have shown that prescriptions are both safe and appropriate, which could markedly increase patient safety and reduce the risk of adverse drug events.24
One of the key concerns regarding the use of the CDSS is the phenomenon of alert fatigue. Clinicians might become desensitized to the large volume of alerts generated by the system, which could result in important warnings being overlooked.25 In line with other studies, our study placed significant emphasis on refining CDSS rules to identify high-risk prescription errors effectively.26,27 We quantified the impact of pharmacists in fine-tuning the CDSS protocols, observing a notable reduction in alert rates and a strategic shift in the categorization of medication alerts. This finding indicated that the CDSS has evolved to more accurately pinpoint clinically significant issues while effectively filtering out less critical alerts.28 This dynamic shift highlights the importance of tailoring interventions to specific contexts and the ongoing need to refine CDSS rules in alignment with local clinical practices and the unique characteristics of patient populations.29 Moreover, the accuracy of CDSS recommendations is highly contingent upon the quality and completeness of the input data, as well as the system’s ability to correctly interpret complex clinical scenarios.30 There is also a pressing need for ongoing updates and maintenance to ensure that the system’s knowledge base remains up-to-date with the latest medical research and guidelines. As technology continues to advance, the future of the CDSS in hospital prescription review seems to be promising. The development of more sophisticated algorithms, the integration of artificial intelligence and machine learning, and the enhancement of user interfaces are supposed to improve the specificity and relevance of system-generated alerts.31,32 Moreover, the potential for personalized medicine, where the CDSS can take an individual’s genetic profile and other unique characteristics into account, offers a new frontier in optimizing medication therapy.
This study had several limitations. First, it was conducted in a single tertiary care hospital, which limits the generalizability of the findings. The results may not be applicable to other hospitals, especially those with different patient populations, healthcare systems, or CDSS implementations. Second, the study lacked data on patient outcomes. While it effectively quantifies the impact of integrating a Clinical Decision Support System (CDSS) on prescription errors and alert rates, it does not provide information on how these changes are translated into actual patient health outcomes. Third, the study relied on the interventions of pharmacists, which introduces the potential for biases in decision-making. Pharmacists may have varying levels of experience, training, and familiarity with the CDSS, leading to inconsistencies in their responses to alerts and interventions.
Despite these limitations, the study has several strengths. The robust methodology and large sample size provided a solid foundation for the findings. The significant reduction in medication alerts and the notable difference in the distribution of medication alert categories demonstrated the effectiveness of the CDSS in enhancing the prescription review process. The active involvement of pharmacists in refining the CDSS rules further enhanced the practicality and clinical relevance of the study.
Future research endeavors should aim to address the limitations identified in this study. Conducting multicenter studies is imperative to increase the generalizability of the findings and ensure that the results are applicable across diverse healthcare settings. Furthermore, future studies should incorporate comprehensive data on patient outcomes. This will enable a thorough assessment of the clinical significance of CDSS implementations, thereby providing a more holistic view of their impact on patient care.
The integration of artificial intelligence and machine learning into the CDSS represents a promising avenue for improvement. These technologies have the potential to further refine the prescription review process, offering more precise and personalized medication recommendations that are tailored to individual patient needs. As technology continues to evolve, it is crucial to persistently refine the CDSS. This will help minimize alert fatigue among clinicians and maximize the system’s benefits in enhancing patient safety and healthcare efficiency. By doing so, we can optimize the use of the CDSS to improve the overall quality of healthcare delivery.
Conclusion
CDSS constitute an invaluable asset in the armamentarium of hospital pharmacists and physicians, facilitating the intricate process of prescription review. Although there are challenges that need to be surmounted, the ongoing evolution and refinement of these systems hold the promise of substantially enhancing patient safety and the caliber of health care settings.
Data Sharing Statement
The data associated with our study have not been deposited into a publicly available repository.
Ethical Approval
This study was conducted in accordance with the principles of the Declaration of Helsinki. The study protocol was reviewed by the medical ethics committee of the Second Affiliated Hospital, Zhejiang University School of Medicine, China (Approval NO.2024--0081). This committee provided a waiver for obtaining informed consent on January 22, 2024. No sensitive information that allowed the identification of individuals was transferred to the research team. All individual patient information was deidentified.
Funding
No specific funding was received for this research.
Disclosure
The authors declare that they have no conflicts of interest related to this work.
References
1. Lewis PJ, Dornan T, Taylor D, Tully MP, Wass V, Ashcroft DM. Prevalence, Incidence and Nature of Prescribing Errors in Hospital Inpatients. Drug Safety. 2009;32(5):379–389. doi:10.2165/00002018-200932050-00002
2. England E, Deakin CD, Nolan JP, et al. Patient safety incidents and medication errors during a clinical trial: experience from a pre-hospital randomized controlled trial of emergency medication administration. Eur J Clin Pharmacol. 2020;76(10):1355–1362. doi:10.1007/s00228-020-02887-z
3. Vogelsmeier A, Jacobs A, Owen C, Mosa ASM, Subramanian R. Medication Identification Device to Reduce Medication Errors in Nursing Homes: a Controlled Pilot Study. J Gerontol Nurs. 2022;48(4):5–11. doi:10.3928/00989134-20220304-01
4. Wittich CM, Burkle CM, Lanier WL. Medication errors: an overview for clinicians. Mayo Clin Proc. 2014;89(8):1116–1125. doi:10.1016/j.mayocp.2014.05.007
5. Valencia Quintero AF, Amariles P, Rojas Henao N, Granados J. Medication errors in pediatrics. Andes Pediatr. 2021;92(2):288–297. doi:10.32641/andespediatr.v92i2.1357
6. Assiri GA, Shebl NA, Mahmoud MA, et al. What is the epidemiology of medication errors, error-related adverse events and risk factors for errors in adults managed in community care contexts? A systematic review of the international literature. BMJ Open. 2018;8(5):e019101. doi:10.1136/bmjopen-2017-019101
7. Slight SP, Tolley CL, Bates DW, et al. Medication errors and adverse drug events in a UK hospital during the optimisation of electronic prescriptions: a prospective observational study. Lancet Digit Health. 2019;1(8):e403–e412. doi:10.1016/s2589-7500(19)30158-x
8. Tully MP, Buchan IE. Prescribing errors during hospital inpatient care: factors influencing identification by pharmacists. Pharm World Sci. 2009;31(6):682–688. doi:10.1007/s11096-009-9332-x
9. Marcin JP, Lieng MK, Mouzoon J, et al. Telemedicine vs Telephone Consultations and Medication Prescribing Errors Among Referring Physicians: a Cluster Randomized Crossover Trial. JAMA Network Open. 2024;7(2):e240275. doi:10.1001/jamanetworkopen.2024.0275
10. Carroll AR, Johnson JA, Stassun JC, Greevy RA, Mixon AS, Williams DJ. Health Literacy-Informed Communication to Reduce Discharge Medication Errors in Hospitalized Children: a Randomized Clinical Trial. JAMA Network Open. 2024;7(1):e2350969. doi:10.1001/jamanetworkopen.2023.50969
11. Heed J, Klein S, Slee A, Watson N, Husband A, Slight SP. An e-Delphi study to obtain expert consensus on the level of risk associated with preventable e-prescribing events. Br J Clin Pharmacol. 2022;88(7):3351–3359. doi:10.1111/bcp.15284
12. Ledley RS, Lusted LB. Reasoning foundations of medical diagnosis; symbolic logic, probability, and value theory aid our understanding of how physicians reason. Science. 1959;130(3366):9–21. doi:10.1126/science.130.3366.9
13. Skalafouris C, Blanc AL, Grosgurin O, et al. Development and retrospective evaluation of a clinical decision support system for the efficient detection of drug-related problems by clinical pharmacists. Int J Clin Pharm. 2023;45(2):406–413. doi:10.1007/s11096-022-01505-5
14. Quintens C, De Rijdt T, Van Nieuwenhuyse T, et al. Development and implementation of ”Check of Medication Appropriateness” (CMA): advanced pharmacotherapy-related clinical rules to support medication surveillance. BMC Med Inform Decis Mak. 2019;19(1):29. doi:10.1186/s12911-019-0748-5
15. Huibers CJA, Sallevelt B, Heij J, et al. Hospital physicians’ and older patients’ agreement with individualised STOPP/START-based medication optimisation recommendations in a clinical trial setting. Eur Geriatr Med. 2022;13(3):541–552. doi:10.1007/s41999-022-00633-5
16. Armando LG, Miglio G, de Cosmo P, Cena C. Clinical decision support systems to improve drug prescription and therapy optimisation in clinical practice: a scoping review. BMJ Health Care Inform. 2023;30(1):100683. doi:10.1136/bmjhci-2022-100683
17. Thorakkattil SA, Parakkal SA, Mohammed Salim KT, et al. Improving patient safety and access to healthcare: the role of pharmacist-managed clinics in optimizing therapeutic outcomes. Explor Res Clin Soc Pharm. 2024;16:100527. doi:10.1016/j.rcsop.2024.100527
18. Slight SP, Seger DL, Franz C, Wong A, Bates DW. The national cost of adverse drug events resulting from inappropriate medication-related alert overrides in the United States. J Am Med Inform Assoc. 2018;25(9):1183–1188. doi:10.1093/jamia/ocy066
19. Damoiseaux-Volman BA, Medlock S, van der Meulen DM, et al. Clinical validation of clinical decision support systems for medication review: a scoping review. Br J Clin Pharmacol. 2022;88(5):2035–2051. doi:10.1111/bcp.15160
20. Levivien C, Cavagna P, Grah A, et al. Assessment of a hybrid decision support system using machine learning with artificial intelligence to safely rule out prescriptions from medication review in daily practice. Int J Clin Pharm. 2022;44(2):459–465. doi:10.1007/s11096-021-01366-4
21. Corny J, Rajkumar A, Martin O, et al. A machine learning-based clinical decision support system to identify prescriptions with a high risk of medication error. J Am Med Inform Assoc. 2020;27(11):1688–1694. doi:10.1093/jamia/ocaa154
22. Sutton RT, Pincock D, Baumgart DC, Sadowski DC, Fedorak RN, Kroeker KI. An overview of clinical decision support systems: benefits, risks, and strategies for success. NPJ Digit Med. 2020;3(1):17. doi:10.1038/s41746-020-0221-y
23. Hajesmaeel Gohari S, Bahaadinbeigy K, Tajoddini S, S RNK. Effect of Computerized Physician Order Entry and Clinical Decision Support System on Adverse Drug Events Prevention in the Emergency Department: a Systematic Review. J Pharm Technol. 2021;37(1):53–61. doi:10.1177/8755122520958160
24. McKie PM, Kor DJ, Cook DA, et al. Computerized Advisory Decision Support for Cardiovascular Diseases in Primary Care: a Cluster Randomized Trial. Am J Med. 2020;133(6):750–756.e2. doi:10.1016/j.amjmed.2019.10.039
25. Kennedy EE, Bowles KH. Human Factors Considerations in Transitions in Care Clinical Decision Support System Implementation Studies. AMIA Annu Symp Proc. 2021;2021:621–630. doi:10.1197/jamia.M2932
26. Bouet J, Potier A, Michel B, et al. Clinical risk assessment of modelled situations in a pharmaceutical decision support system: a modified e-Delphi exploratory study. Int J Clin Pharm. 2024;46(3):727–735. doi:10.1007/s11096-023-01698-3
27. Changulani T, Mustafa MZ, Ahuja S, James A, Agarwal PK. Minimising prescription errors-a quality improvement project in the ophthalmology department in a tertiary referral hospital. Int Ophthalmol. 2021;41(9):3041–3046. doi:10.1007/s10792-021-01866-2
28. Sallevelt B, Huibers CJA, Heij J, et al. Frequency and Acceptance of Clinical Decision Support System-Generated STOPP/START Signals for Hospitalised Older Patients with Polypharmacy and Multimorbidity. Drugs Aging. 2022;39(1):59–73. doi:10.1007/s40266-021-00904-z
29. Linkens A, Milosevic V, van Nie N, et al. Control in the Hospital by Extensive Clinical rules for Unplanned hospitalizations in older Patients (CHECkUP); study design of a multicentre randomized study. BMC Geriatr. 2022;22(1):36. doi:10.1186/s12877-021-02723-8
30. Westerbeek L, Ploegmakers KJ, de Bruijn G-J, et al. Barriers and facilitators influencing medication-related CDSS acceptance according to clinicians: a systematic review. Int J Med Inform. 2021;152:104506. doi:10.1016/j.ijmedinf.2021.104506
31. Moja L, Polo Friz H, Capobussi M, et al. Effectiveness of a Hospital-Based Computerized Decision Support System on Clinician Recommendations and Patient Outcomes: a Randomized Clinical Trial. JAMA Network Open. 2019;2(12):e1917094. doi:10.1001/jamanetworkopen.2019.17094
32. Yoshimura Y, Matsumoto A, Momosaki R. Pharmacotherapy and the Role of Pharmacists in Rehabilitation Medicine. Prog Rehabil Med. 2022;7:20220025. doi:10.2490/prm.20220025
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.