Back to Journals » Journal of Pain Research » Volume 18
Development and External Validation of a Nomogram for Predicting Pain Risk Post-Transperineal Prostate Biopsy Using Multi-Parameter Analysis
Authors Xu Y, Li X ![]() , Zhang Y, Xue P
, Zhang Y, Xue P
Received 27 June 2025
Accepted for publication 18 November 2025
Published 5 December 2025 Volume 2025:18 Pages 6545—6561
DOI https://doi.org/10.2147/JPR.S543761
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Jinlei Li
Yang Xu,1,* Xin Li,2,* Yang Zhang,1 Peng Xue1
1Department of Urology, The Affiliated Lianyungang Hospital of Xuzhou Medical University/The First People’s Hospital of Lianyungang, Lianyungang, Jiangsu, 222000, People’s Republic of China; 2Department of Urology, Zhengzhou University Affiliated Zhengzhou Central Hospital, Zhengzhou, HeNan, 450000, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Peng Xue, Department of Urology, The Affiliated Lianyungang Hospital of Xuzhou Medical University/The First People’s Hospital of Lianyungang, Lianyungang, Jiangsu, 222000, People’s Republic of China, Tel +86-0515-85605248, Email [email protected]
Purpose: To explore factors associated with moderate-to-severe pain (NRS > 4) in patients undergoing ultrasound-guided transperineal prostate biopsy (TPB), and to establish and validate a nomogram model for risk assessment.
Patients and Methods: This study included 520 patients who underwent ultrasound-guided TPB at the First People’s Hospital of Lianyungang City from September 2022 to December 2024. A training group (n = 400) and a validation group (n = 120) were established based on the admission time. Data collection included demographics, admission comorbidities, laboratory tests, imaging examinations, biopsy data, anxiety scores, and pain scores. Binary logistic regression was used to identify factors influencing moderate-to-severe pain (NRS > 4). A nomogram-based risk assessment model was constructed, with a validation model created to verify the training group. Additionally, a web-based dynamic nomogram risk assessment model was developed, and 120 patients from external hospitals were included for external validation.
Results: Univariate analysis identified factors with statistical significance. Based on binary Logistic regression analysis, prostate volume, anxiety score, history of diabetes, biopsy time, and number of biopsy needles were risk factors, while age was a protective factor (P < 0.05). The nomogram-based risk assessment model demonstrated favorable predictive accuracy, with an area under the receiver operating characteristic (ROC) curve (AUC) of 0.940 [95% CI: 0.914– 0.967] in the training group and 0.893 [95% CI: 0.834– 0.951] in the internal validation group. External validation further confirmed robust predictive capability (AUC = 0.888 [95% CI: 0.825– 0.951]). Additionally, decision curve analysis indicated clinically meaningful net benefits.
Conclusion: This nomogram-based risk stratification tool offers a robust framework for personalized perioperative pain management in patients undergoing TPB. Furthermore, external validation further supports the model’s applicability.
Keywords: biopsy, prostate tumor, cancer, pain, nomogram
Introduction
Prostate cancer (PCa) remains the second most common cancer and the fifth leading cause of cancer death among men globally according to GLOBOCAN 2020, with around 1,414,259 new cases of PCa, and 375,304 cancer-related deaths worldwide.1 Worldwide statistics revealed around 1,414,259 new cases, and 375,304 cancer-related deaths.1 In China, the age-standardized incidence rate (ASR) of PCa in 2020 was 10.2 per 100,000.1 Despite a prevalent occurrence worldwide, PCa has controversial detection methods and diagnostic technologies, depending mainly on transperineal and transrectal biopsies (TPB or TRB). Systematic TRB, ie, the gold standard, has been practiced globally for decades.2
Recent empirical evidence has demonstrated the superiority of TPB in minimizing the risk of infection,3 augmenting the accuracy of sampling in the anterior and apical zones of the prostate, reducing urethral trauma,4 and broadening peripheral zone sampling. Such type of mounting evidence is catalyzing a paradigm shift towards the adoption of TPB. A comprehensive assessment of TPB outcomes and patient comfort is deemed imperative given that over two million men in Europe and the United States undergo prostate biopsies annually.5
Effective pain management is crucial for TPB, directly impacting patient tolerance, procedural feasibility, and overall experience. Current clinical strategies, including local anesthesia, monitored anesthesia care (MAC), and various adjuncts, reflect a trend toward multimodal, personalized protocols. Although MAC with agents such as propofol offers complete analgesia—proving invaluable for highly anxious individuals or complex cases—its demand for specialized resources and personnel increases economic costs. Thus, well-optimized local anesthesia, involving perineal skin infiltration and targeted periprostatic nerve blockade (PNB), serves as the foundation and frequent first-line approach for most routine procedures. A key limitation of this approach, however, lies in the highly variable nature of pain response, underscoring the need to identify high-risk patients proactively.
Recent studies on pain mechanisms, despite a confirmed feasibility of TPB under local anesthesia, have identified severe pain and fear as major reasons for patients’ refusal, resulting in delayed necessary medical examinations. Moreover, many male patients experience significant discomfort during TPB,6 with about 1% requiring additional analgesia or general anesthesia for a repeat TPB.7,8 Therefore, despite its role as the first-line strategy, pain associated with TPB under local anesthesia remains a significant clinical issue, potentially affecting patient compliance and procedural success.9
While the clinical necessity for accurate pain prediction is unequivocal, predictive tools for procedural pain in urology remain sparse and limited. Prior research has developed models to predict postoperative pain following procedures such as cystoscopy or ureteral stent placement.10 However, these models lack generalizability to the specific context of intraoperative pain during TPB, which is the focus of the present investigation.
Previous research has documented various factors influencing pain during prostate biopsy, such as prostate volume, number of cores, and anesthesia protocols. However, these studies often face methodological constraints such as small sample sizes, single-center designs, and insufficient external validation. Furthermore, existing predictive models have largely overlooked psychological factors, particularly patient anxiety, which is a well-established modulator of procedural pain perception.11 It highlights the necessity for a comprehensive, validated predictive model, integrating both clinical and procedural factors, to accurately assess the risk of moderate-to-severe pain before biopsy. Therefore, this study constructed a nomogram reflecting the probability of moderate-to-severe pain during TPB specifically, with external validation, which is anticipated to facilitate early identification of high-risk individuals for moderate-to-severe pain, providing a reference for better strategic planning.
Materials and Methods
Patients and Data Collection
With approval obtained from the Independent Ethics Committee, and informed consent from all patients, between September 2022 and December 2024, this study retrospectively acquired eligible data from 600 individuals undergoing TPBs at Lianyungang City’s First People’s Hospital, Jiangsu, China. Patient selection was based on the following eligibility criteria:
Inclusion Criteria
a) Suspicious prostate nodules by digital rectal examination. b) Suspicious lesions by transrectal ultrasound (TRUS) or prostate MRI/CT. c) Serum total prostate-specific antigen (tPSA > 10 μg/L). d) A free-to-tPSA (f/tPSA) < 0.16, and/or prostate-specific antigen density > 0.15, and/or prostate-specific antigen velocity (PSAV) > 0.75 μg/(L·year) in case of blood tPSA levels ranging between 4–10 μg/L. e) Abnormal results in other PCa biomarkers, such as positive urinary PCa antigen 3 (PCA3). f) Diagnosis of PCa with evidence suggesting metastatic disease.
Exclusion Criteria
a) Acute infection phase or febrile phase of the urogenital system. b) Hypertensive crisis. c) Decompensated heart failure. d) Diseases with severe bleeding tendency. e) Severe immunosuppressive state. f) Poorly controlled or unstable comorbidities (eg, hypertension and diabetes). g) Contraindications for transrectal puncture in patients with severe internal or external hemorrhoids, perianal or rectal lesions, or anal stenosis. h) Presence of severe psychological disorders or patients uncooperative with the procedure. i) Study subjects lacking complete clinical information.
Following the exclusion of 80 patients (12 due to incomplete clinical records), a final cohort of 520 was enrolled. For constructing and internally validating a predictive model, participants were divided into the training group (n=400, September 2022 - May 2024) and the internal validation group (n=120, June 2024 - December 2024) based on their admission dates. To assess the external validity of the predictive model, an independent cohort consisting of 120 patients was collected from Huaian Second People’s Hospital between June 2024 and December 2024. TPBs were employed for all these participants during this period. The same eligibility criteria as applied in the training cohort were used for patient selection. The external validation cohort was utilized to evaluate the generalizability and predictive performance of the model we constructed.
Transperineal Biopsy Under Local Anesthesia
Patients were placed in the lithotomy position, and a high-frequency ultrasound probe was inserted transrectally. Subsequently, 20 mL of 1% lidocaine was administered locally via the perineum. First, based on the ultrasound image showing the prostate projection onto the perineum, skin and subcutaneous infiltration anesthesia (10 mL) was performed within approximately 0.5 cm of the peripheral prostate. Next, under real-time ultrasound guidance, lidocaine was injected around the bilateral neurovascular bundles of the prostate (5 mL per side, totaling 10 mL) using a puncture needle. Successful blockade was confirmed by the appearance of a hypoechoic fluid zone around the prostate and seminal vesicles on ultrasound imaging. After the onset of anesthesia, systematic and targeted biopsies were performed, guided by preoperative imaging findings (eg, suspicious MRI lesions) and a standard puncture protocol. Prostate dimensions, volume, and locations and sizes of abnormal echoes were documented during the procedure.
All anesthetic and biopsy procedures were performed by a single urologist. Relevant parameters (eg, duration, needle count) were recorded in real-time by a separate physician assisting throughout the procedure and subsequently entered into electronic medical records. This standardized data-collection procedure ensured consistency and accuracy of measurements.
Clinical Research Methodology
We conducted a comprehensive assessment of patients using a General Data Questionnaire, the State-Trait Anxiety Inventory (STAI), and the Numeric Rating Scale (NRS). The objectives were to investigate the correlation between various factors and the severity of postoperative pain experienced by patients following TPBs, and to construct a predictive model for this type of pain.
General Data Questionnaire: To identify factors influencing moderate-to-severe postoperative pain, we developed this questionnaire through an extensive literature review, discussions within our research team, and consultations with an expert panel. It consists of three sections: (1) Demographic data of age, education, and body mass index (BMI); (2) Disease-related details, such as prostate-specific antigen (PSA) levels, f/tPSA, prostate volume, Prostate Imaging Reporting and Data System (PI-RADS) scores, and International Prostate Symptom Score (IPSS); (3) Surgical particulars, covering operation duration, number of biopsy needles used, and pain scores.
STAI:12 This self-rating scale consists of 40 questions in two parts: (1) The State-Anxiety Inventory (S-AI, questions 1–20) to indicate transient experiences of unpleasant emotional states, such as tension, fear, anxiety, and nervousness, accompanied by heightened activity of the autonomic nervous system; and (2) The Trait-Anxiety Inventory (T-AI, questions 21–40) to describe the personality trait of relative stability, characterized by individual differences in anxiety disposition. Anxiety was then classified into three tiers of no (< 35), moderate (36–41), and severe (> 42) anxiety.13 During the study period, the STAI was routinely administered to all patients scheduled for the procedure as part of our institution’s standard preoperative nursing assessment, thereby minimizing selection bias.
NRS:14 This scale, with a range from 0 (no pain) to 10 (the most severe pain imaginable), was employed to quantify patients pain intensity. In this study, patients’ pain was assessed at five standardized time points: during insertion of the ultrasound probe into the rectum (NRS1), subcutaneous anesthesia (NRS2), layered infiltration anesthesia around the prostate capsule under ultrasound guidance (NRS3), each biopsy needle tissue sampling (NRS4), and 30 minutes postoperatively (NRS5). The highest pain score recorded at any stage was considered the primary pain outcome for analysis, categorizing patients into mild (≤4 points) and moderate-to-severe (>4 points) pain groups.
Statistical Analyses
SPSS 25.0 (25.0; SPSS, Inc., Chicago, IL) and the R 4.5.00 (R Foundation for Statistical Computing) were employed for analyses statistically. Categorical variables [frequencies (%)] were analyzed with the Chi-square (χ2) test; while continuous variables [M(P25, P75)] were assessed using the non-parametric Wilcoxon rank-sum test. A logistic regression analysis was utilized to pinpoint relevant factors. The identified factors were subsequently incorporated into the “rms” package (R 4.5.0) for the construction of a predictive nomogram risk assessment model.
Meanwhile, receiver operating characteristic (ROC) curves were generated to evaluate the predictive accuracy of this nomogram model in forecasting moderate-to-severe post-biopsy pain. A calibration curve was also plotted to assess the predictive consistency of this Model. The threshold of statistical significance was set to P < 0.05.
Results
Analysis of General Data Between Groups
Statistical tests revealed inter-group comparable baseline data (P > 0.05; Table 1), indicating inter-group comparability. Specifically, there was no significant inter-group difference in age, STAI, biopsy duration, number of biopsy needles, history of diabetes, and prostate volume (P > 0.05). Overall, the training group had an average age of 71.13±10.44 years, history of diabetes in 150 cases (37.5%), and anxiety score of 40.28±17.42; while those of the validation group were 72.72±10.22 years, history of diabetes in 38 cases (31.7%), and anxiety score of 41.83±16.96.
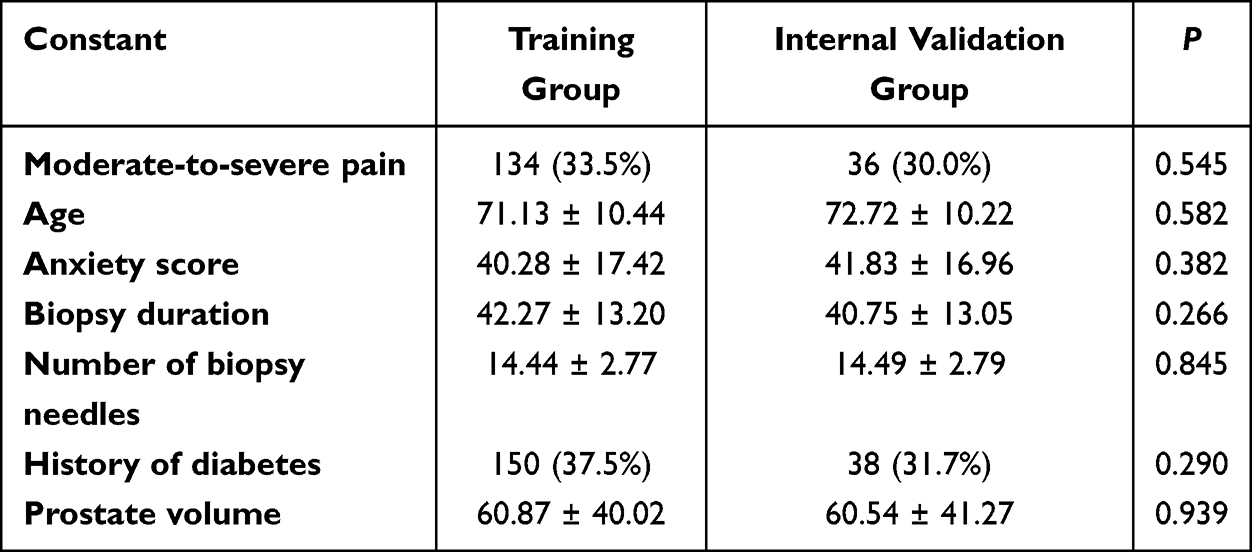 |
Table 1 Consistency Test of the Training and Validation Groups |
Univariate Analysis of Pain in Ultrasound-Guided TPB
Among the 400 patients in the training group, 134 experienced moderate-to-severe pain, while 266 patients only had mild pain. In Table 2, the pain in patients was mainly associated with differences in age, prostate volume, anxiety score, history of diabetes, biopsy history, biopsy time, Pi-RADS score, sleep quality and the number of biopsy needles (P < 0.05). However, there was no significant correlation with factors such as the patient’s education level, smoking history, long-term alcohol consumption history, digital rectal examination status, history of chronic diseases, PSA, and IPSS, with no statistical difference (P > 0.05).
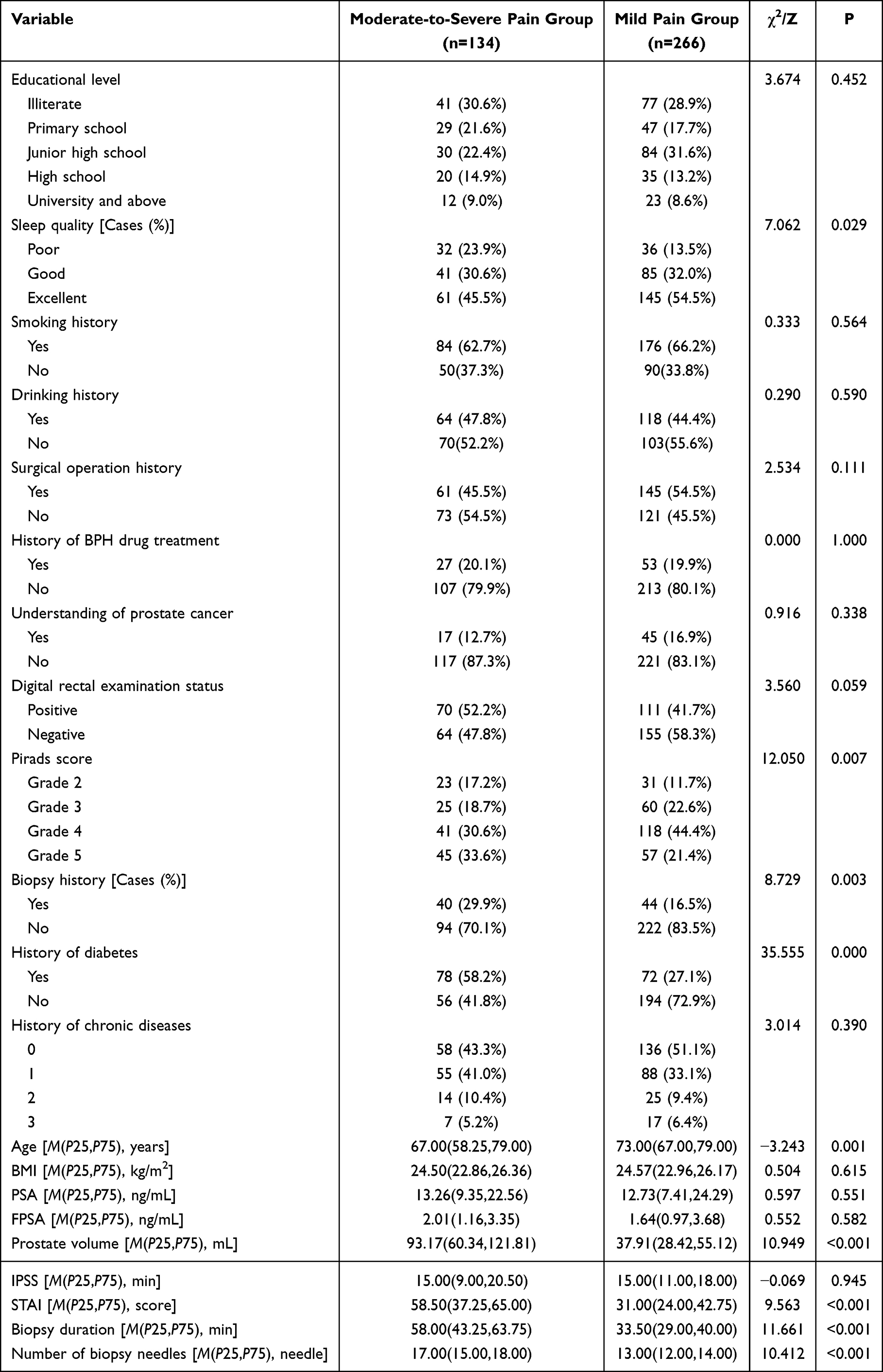 |
Table 2 Univariate Analysis of Moderate-to-Severe Pain Occurrence in Patients Undergoing Ultrasound-Guided TPB |
Logistic Regression Analysis of Factors Associated with Moderate-to-Severe Pain in Ultrasound-Guided TPB
A binary Logistic multivariate regression analysis method was used focusing on nine factors with statistical significance in the univariate analysis were independent variables, and the occurrence of moderate-to-severe pain in patients undergoing ultrasound-guided TPB as the dependent variable. As summarized in Table 3, the anxiety score (OR = 1.041, 95% CI [1.017, 1.065], P < 0.001), biopsy duration (OR = 1.084, 95% CI [1.048, 1.121], P < 0.001), number of biopsy needles (OR = 1.288, 95% CI [1.091, 1.520], P = 0.003), history of diabetes (OR = 4.436, 95% CI [2.101, 9.365], P < 0.001), and prostate volume (OR = 1.032, 95% CI [1.017,1.048], P < 0.001) were risk factors for moderate-to-severe pain; while age (OR = 0.911, 95% CI [0.877, 0.946], P < 0.001) might exert protective role.
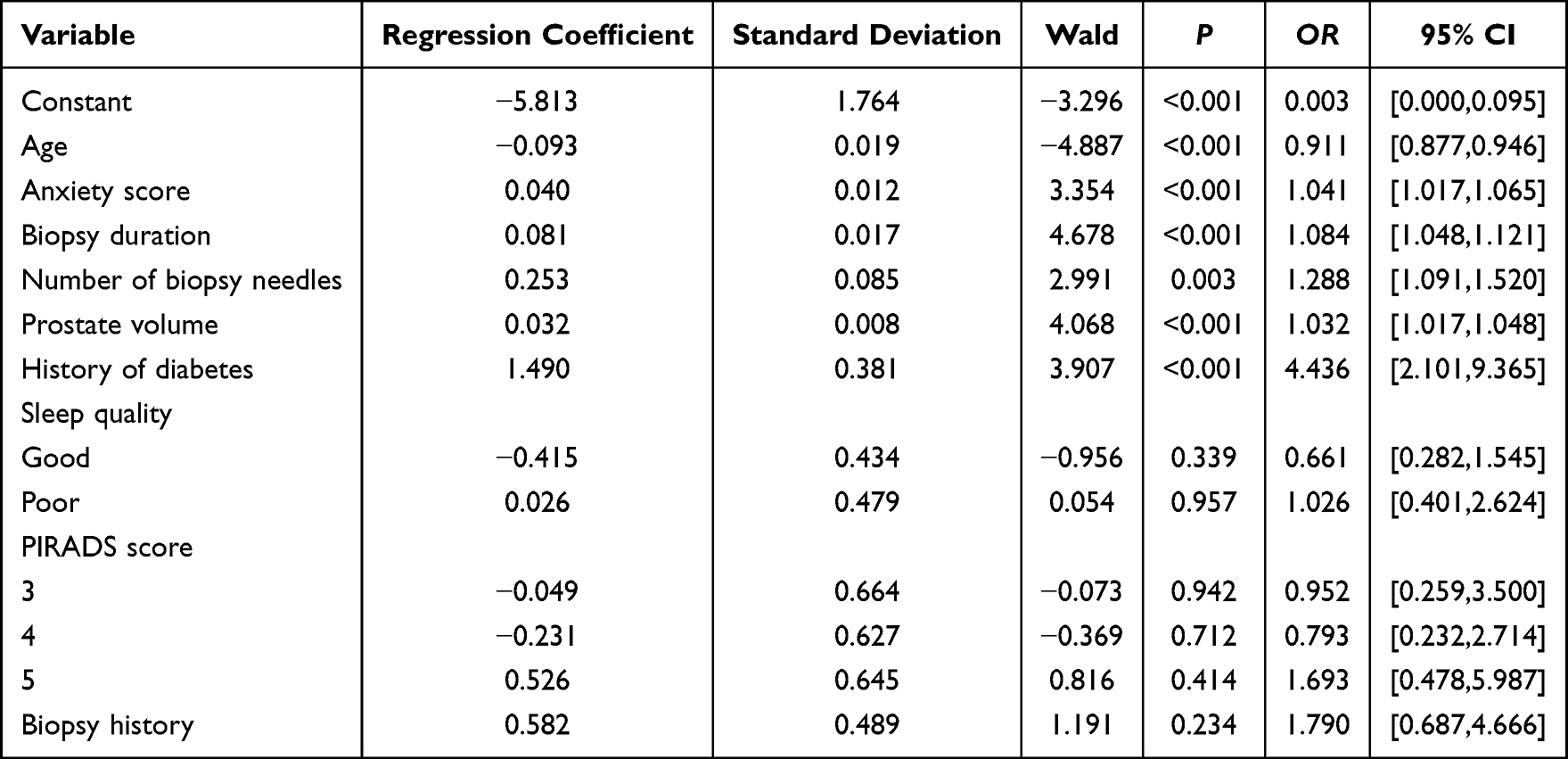 |
Table 3 Multivariate Analysis of Moderate-to-Severe Pain Occurrence in Patients Undergoing Ultrasound-Guided TPB |
Construction and Verification of the Nomogram Risk Assessment Model for Moderate-to-Severe Pain in Patients Undergoing Ultrasound-Guided TPB
Six statistically significant factors — age, anxiety score, biopsy duration, number of biopsy needles, history of diabetes, and prostate volume — were incorporated for modeling to predict moderate-to-severe pain in patients undergoing ultrasound-guided TPB (Figure 1A) To enhance clinical application, an online dynamic nomogram-based risk assessment model was developed and made available as a web-based tool (accessible at: https://pain-prediction-model.shinyapps.io/Pain-prediction-model/) (Figure 1B). This model is designed to provide clinicians with a user-friendly and intuitive platform for assessing the individualized risk of moderate-to-severe pain during biopsy procedures, thereby facilitating the development of personalized patient management strategies and treatment plans.
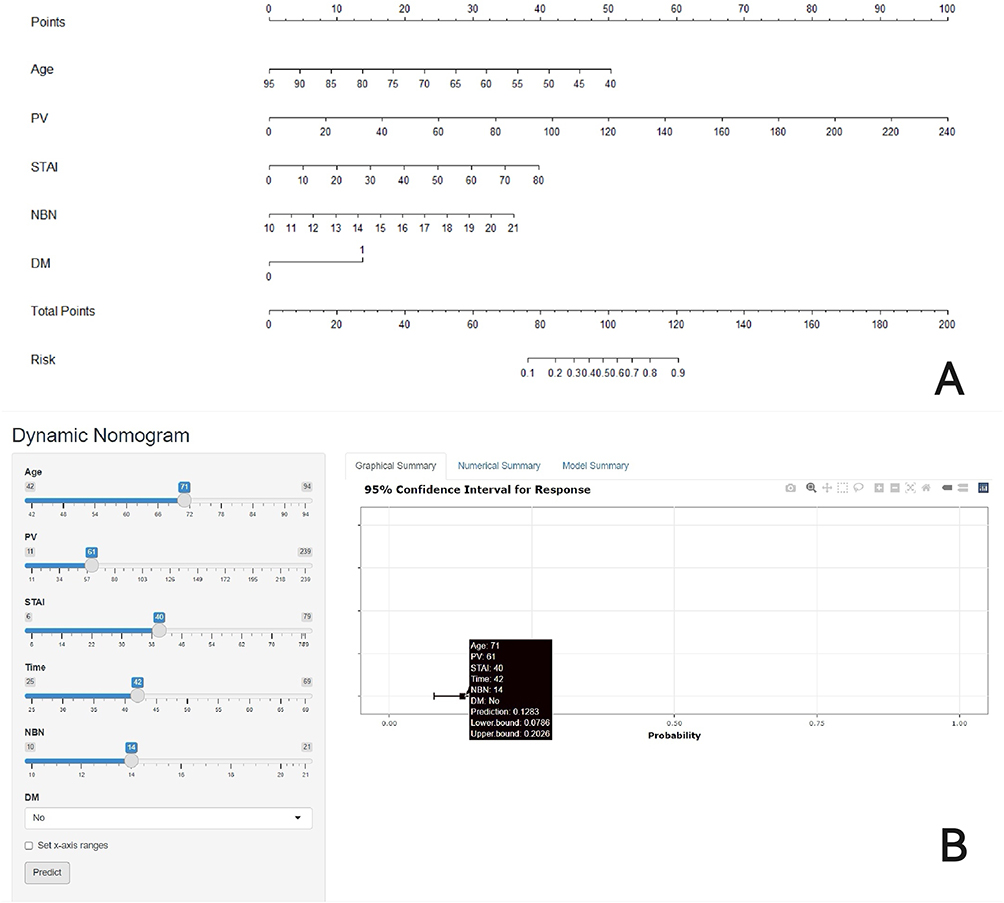 |
Figure 1 Nomogram Risk Assessment Model for moderate-to-severe pain occurrence in ultrasound-guided TPB (A) and example of the online predictive model for prostate biopsy pain (B). (A) The following six parameters were included in the development of the modeling group: Age (years), PV (prostate volume, mL), STAI (anxiety score), time (biopsy duration, min), NBN (number of biopsy needles), and DM (Diabetes mellitus). (B) The URL for the online risk assessment model is (https://pain-prediction-model.shinyapps.io/Pain-prediction-model/). The example shows a 71-year-old patient with specific biopsy parameters and a predicted probability of 12.83% for moderate-to-severe pain. |
The predictive performance of the model was evaluated through both internal and external validation. In the internal validation, the area under the ROC curve (AUC) was 0.940 [95% CI: 0.914–0.967] and AUC of 0.893 [95% CI: 0.834–0.954] in the training and internal validation cohort, respectively (Figures 2 and 3), with corresponding sensitivity of 80.6% and 91.7%, and specificity of 95.5% and 77.4%, respectively. In the external validation cohort of 120 patients, the model achieved an AUC of 0.888 [95% CI: 0.825–0.951] (sensitivity: 69.8%, and specificity: 96.1%) (Figure 4). The detailed performance metrics, including sensitivity, specificity, positive predictive value (PPV), and negative predictive value (NPV) at the optimal cutoff point, are summarized in Table 4. As a result, the risk assessment model exhibited strong discriminative ability and robust predictive performance across different patient cohorts.
 |
Table 4 Summary of Model Performance Metrics |
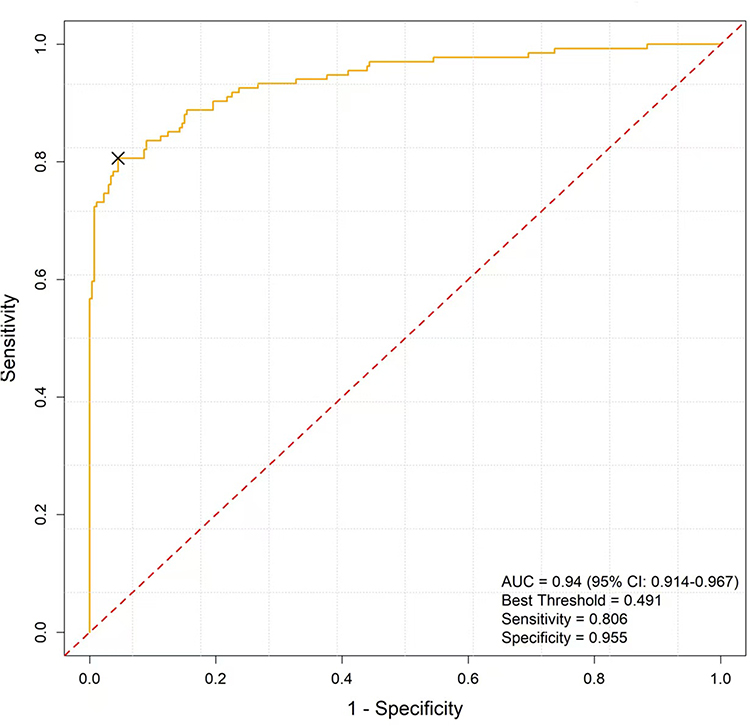 |
Figure 2 ROC Curve for the Training Group. The AUC was 0.940. The optimal cutoff point, determined by the maximum Youden index, is indicated by an “X” on the curve. |
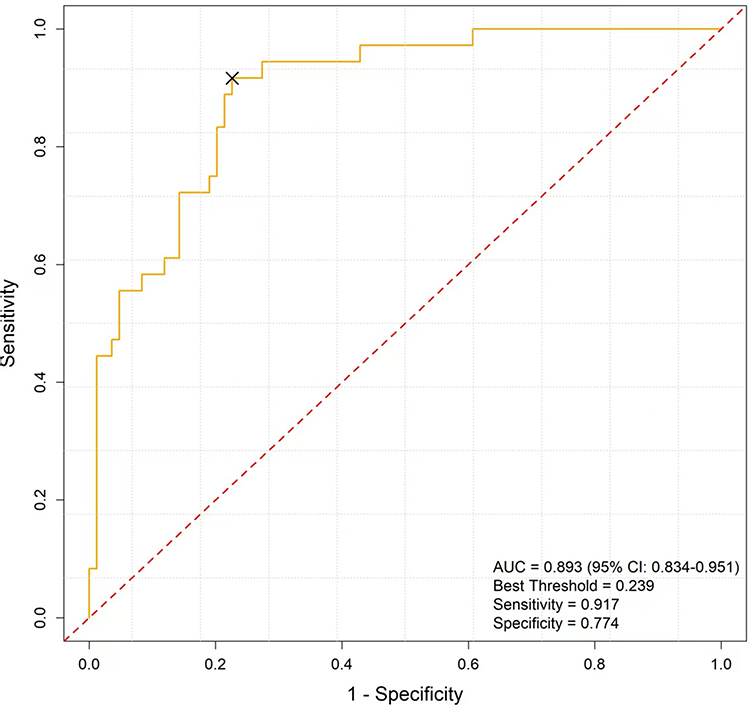 |
Figure 3 ROC Curve for the Internal Validation Group. The AUC was 0.893. The optimal cutoff point, determined by the maximum Youden index, is indicated by an “X” on the curve. |
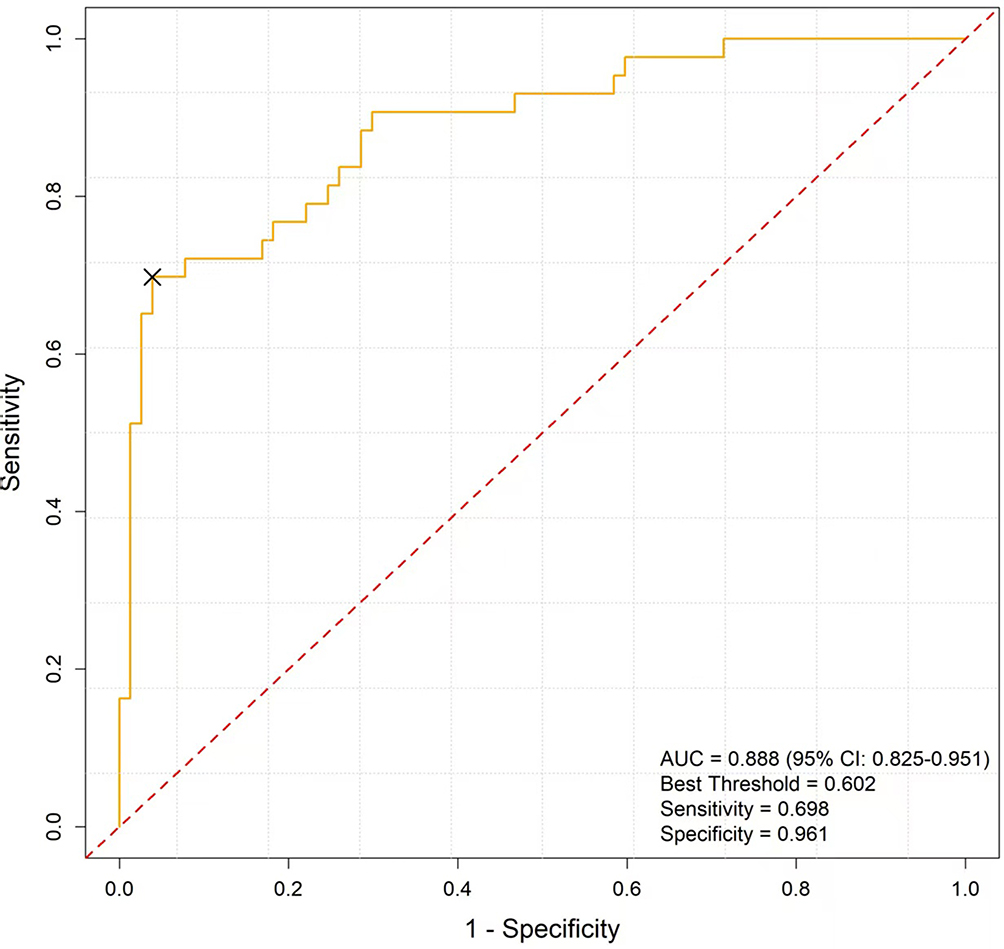 |
Figure 4 ROC Curve for the External Validation Group. The AUC was 0.888. The optimal cutoff point, determined by the maximum Youden index, is indicated by an “X” on the curve. |
For calibration performanceassessment,1,000 bootstrap resamples (B = 1,000) were applied to correct for potential bias. In the training cohort (Figure 5), the curve demonstrated excellent concordance between predicted and observed probabilities, with an average absolute error (Eavg) of 0.034 and a concordance index (C-index) of 0.940. Similarly, in the internal validation cohort (Figure 6), good calibration was observed, with an Eavg of 0.060 and a C-index of 0.893. In the external validation cohort (Figure 7), the calibration curve indicated satisfactory agreement, with an Eavg of 0.050 and a C-index of 0.888.
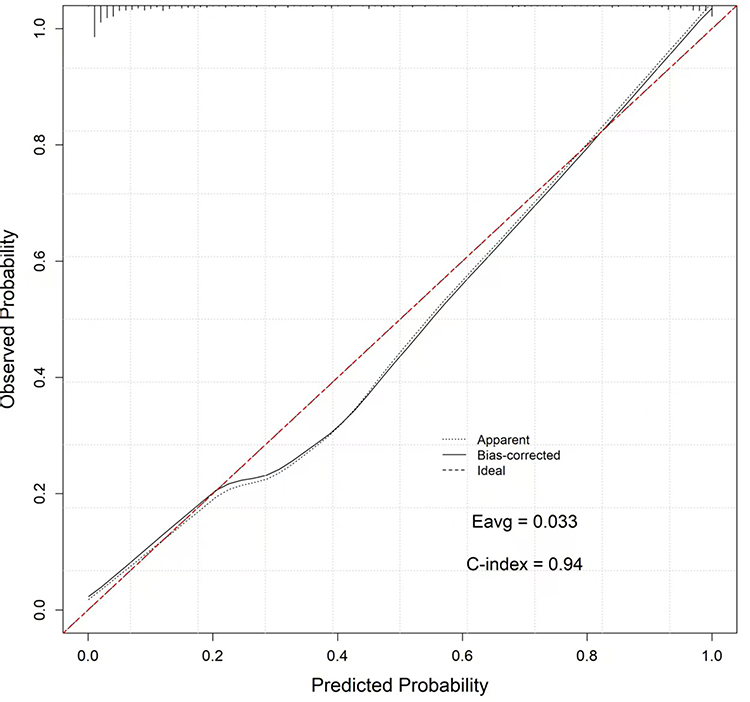 |
Figure 5 Calibration Curve for the Training Group. The curve illustrates the agreement between predicted and observed probabilities of moderate-to-severe pain. The average absolute error (Eavg) was 0.033, and the concordance index (C-index) was 0.940. The red dashed line represents the ideal reference line, while the blue line indicates the model’s performance after bootstrapping (n=1,000). |
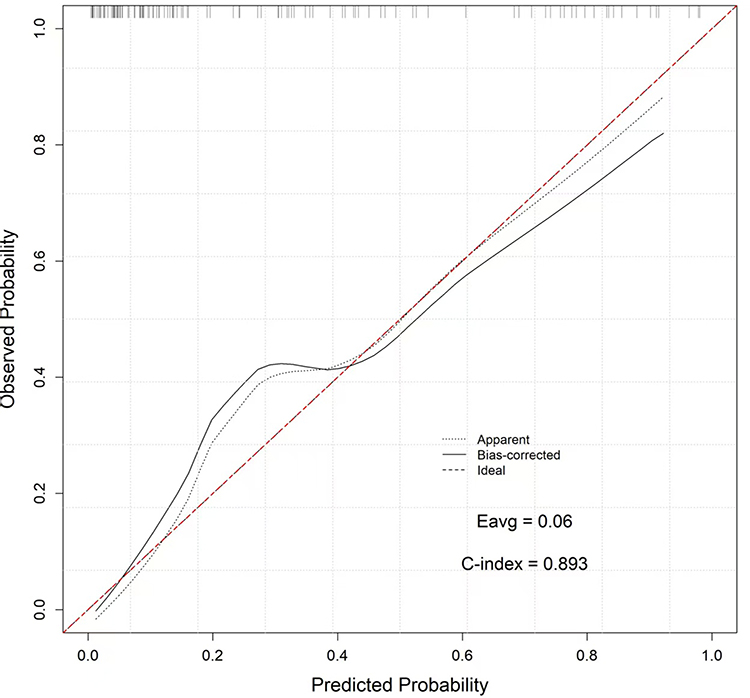 |
Figure 6 Calibration Curve for the Internal Validation Group. The curve shows the relationship between predicted probabilities and actual outcomes in the internal validation cohort. The Eavg was 0.060, and the C-index was 0.893. The red dashed line indicates the perfect prediction line, and the blue line reflects the model’s corrected calibration using 1,000 bootstrap resamples. |
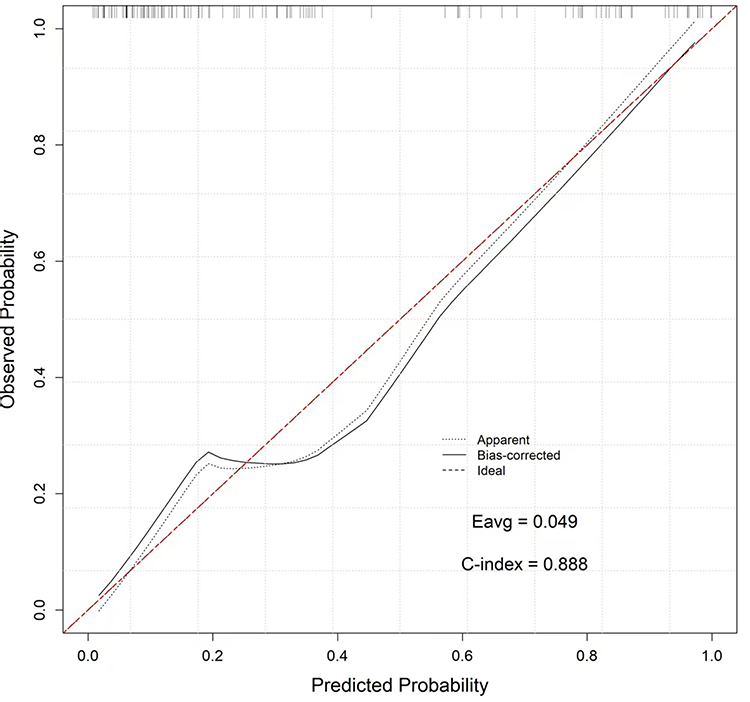 |
Figure 7 Calibration Curve for the External Validation Group. The calibration curve evaluates the model’s performance in an independent external validation cohort comprising 120 patients. The Eavg was 0.049, and the C-index was 0.888. The red dashed line stands for the ideal calibration, and the blue line demonstrates the model’s predictive accuracy after bias correction with 1,000 bootstrap iterations. |
Additionally, based on decision curve analysis (DCA), in the training cohort (Figure 8), the model demonstrated a higher net benefit across a wide range of threshold probabilities compared to the treat-all and treat-none strategies, indicating favorable clinical applicability. Similarly, the model consistently provided greater net benefit than the two comparator strategies, in the internal validation cohort (Figure 9), confirming its robustness and clinical usefulness. In addition, assessment based on the external validation cohort (Figure 10) observed a substantial net benefit advantage in this model, suggesting good generalizability and potential applicability to independent patient populations. Overall, the predictive model could effectively support clinical decision-making by offering consistent and meaningful net benefit across diverse threshold probabilities.
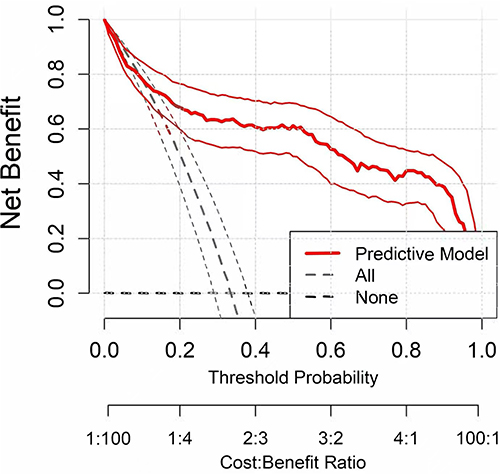 |
Figure 8 Clinical Net Benefit Curve (DCA) for the Training Group. The DCA for the training group shows that the predictive model (red curve) provides a greater net benefit across a wide range of threshold probabilities compared to the “treat-all” and “treat-none” strategies. The X-axis represents the threshold probability, and the Y-axis represents the net benefit. The analysis demonstrates that the model has favorable clinical utility for decision-making in the training group. |
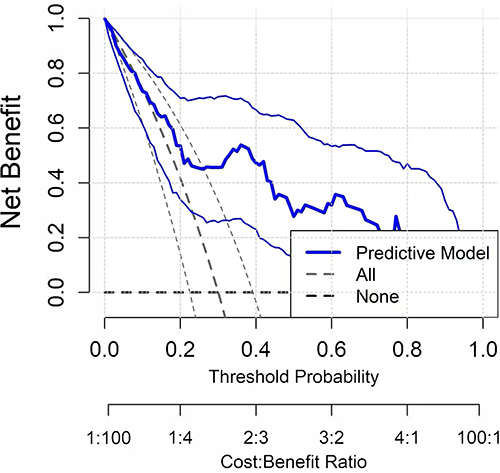 |
Figure 9 Clinical Net Benefit Curve (DCA) for the Internal Validation Group. The DCA for the internal validation group indicates that the predictive model (blue curve) consistently offers higher net benefit than the “treat-all” and “treat-none” strategies across various threshold probabilities. The findings confirm the robustness and clinical applicability of this model in an independent internal validation dataset. |
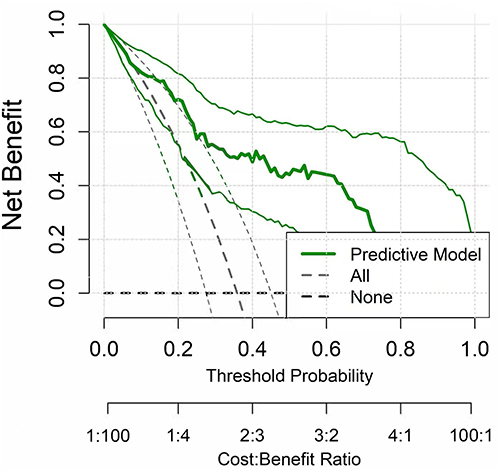 |
Figure 10 Clinical Net Benefit Curve (DCA) for the External Validation Group. The DCA for the external validation group demonstrates that the predictive model (green curve) maintains superior net benefit compared to the “treat-all” and “treat-none” strategies. These results suggest good generalizability of the model to external patient populations and support its potential utility in a broader clinical practice. |
Discussion
As the second most common male malignant tumors worldwide,1 PCa shows a continuous rise in its incidence rate in China, ranking the sixth place among male malignant tumors.15 Therefore, it underlines the importance of its early diagnosis and treatmentfor prolonging the lifespan of patients and improving their quality of life. Currently, TPB is considered the preferred option of biopsy for diagnosing PCa,16 which, however, may cause more pain compared to TRB as it requires passing through the skin and muscles until it reaches the prostate capsule.
Common procedures for local anesthesia in the process of prostate biopsy include intrarectal local anesthesia, perineal subcutaneous infiltration, pudendal nerve block, and periprostatic nerve block (PNB). PNB is currently considered the “gold standard” for alleviating pain during this biopsy.17 PNB involves injecting the anesthetic agent around the neurovascular bundles at the junction of the seminal vesicles and the prostate on both sides of the prostate base under the guidance of TRUS. In the clinical setting, some patients are still not satisfied with the pain control during TPB under PNB anesthesia, further compromising the progress of biopsy and subsequent diagnosis.
Presently, predictive tools for urological procedural pain are notably scarce. While recent studies have developed models to predict postoperative pain after interventions like cystoscopy or ureteral stent placement,10 these models are not generalizable to the distinct context of intraoperative pain encountered during TPB. This significant gap underscores the critical need for and urgency of developing tailored predictive models for TPB.
In this study, based on the enrollment of 520 patients with ultrasound-guided TPB, the occurrence of moderate-to-severe pain was found to be closely related to several influencing factors, including age, anxiety level, biopsy duration, number of biopsy needles, presence of diabetes, and prostate volume. Specifically, 134 (33.5%) of the 400 patients in the training group, and 36 (30.0%) of the 120 patients in the internal validation group suffered from moderate-to-severe pain. These findings were similar to those reported by Rodriguez and Terris,18 who reported that 30% of patients undergoing standard six-point biopsy protocol suffered from moderate-to-severe pain. Similarly, Zisman et al19 found in their pain assessment of 211 patients undergoing biopsy that 96% of patients felt discomfort after the biopsy, with 29% experiencing severe pain and discomfort.
Furthermore, our study revealed a protective role played by age in this context. Rodriguez and Terris18 also documented differences in pain perception between different age groups, and younger patients experienced more significant pain than older patients, supporting the potential effect of age in affecting patients’ pain perception. Despite this, there is still inconsistent research findings on the link between age and pain during TRB or TPB. Peyromaure M et al20 reported no correlation between age and pain or discomfort. Another study observed higher intraoperative prevalence of such pain in younger patients compared with older patients, which may be attributable to the psychological and physiological characteristics of young people. Young patients may have higher pain sensitivity and a lower pain threshold, resulting in higher sensitivity to acute pain during biopsy. In contrast, the elderly may have a certain natural protective effect against acute injury due to the reduction in the number of receptors and the increase in the threshold for pain transmission stimulation.
Moreover, the risk of experiencing moderate-to-severe pain would be increased by 1.065 times for every one-point increase in the patient’s anxiety score, highlighting the positive correlation between anxiety and pain perception. Indeed, prostate biopsy can cause significant psychological stress to patients, with approximately 20% of men reporting the feeling of anxiety or significant psychological tension before the biopsy.21 Some researchers also proposed a significant linear association between anxiety and pain perception, and that anxiety was an independent predictor of pain during prostate biopsy.22–24 Interventions for anxious patients, such as the use of anti-anxiety medications, can work to alleviate pain in gastrointestinal, breast, and bone marrow biopsies.25–27 Non-pharmacological interventions such as music therapy and behavioral adjustments have also been proven to effectively reduce patients’ anxiety and pain.28–32
In addition to psychological factors, diabetic patients also experienced significantly stronger pain perception during prostate biopsy. According to previous studies, diabetic patients have a higher sensitivity to pain, which may be explained by the increased excitability of peripheral nerves and the mechanism of pain amplification in the central nervous system.33–35
The number of biopsy needles and biopsy duration were significant risk factors. A notable pain correlation exists between surgical duration and the number of core samples. The number of core samples has been established as a predictor of pain in ultrasound-guided TRB.36 Conversely, Yasushi Nakai et al37 discovered that pain gradually accumulated from the first to the last sampling during ultrasound-guided TRB, forming the so-called pain accumulation effect. Compared to the number of samples taken, biopsy duration might have a more significant impact on pain perception, potentially resulting from increased perception of pain owing to an extended surgical duration. Prior opinion has more prominently emphasized a strong correlation between prostate biopsy duration and the pain caused by the surgery, rather than the number of samples taken. In this study, repeated biopsies were performed by penetrating the skin directly, without the use of sampling sleeves, possibly triggering prolonged duration surgically and aggravated pain perception in patients.
The prostate volume may also be a key factor causing patient pain. In our study, patients with larger prostate volumes experienced more severe pain during ultrasound-guided TPB. The average prostate volume and its interquartile range were 93.17 (60.34,121.81) mL and 37.91 (28.42,55.12) mL in the moderate-to-severe pain group and the mild pain group, respectively. Existing publication has demonstrated prostate volume as a predictive indicator of biopsy-related pain.38 A positive correlation has also been established between prostate volume and pain intensity by previous research.39 A study by Sonmez et al40 proposed a cutoff value of 61.6 mm3 (with both sensitivity and specificity at 83%), suggesting that patients with the prostate volume exceeding 61.6 mm3 may experience higher risk of pain during prostate biopsy.
In general, nomogram is a graphical tool for result visualization, which may assist clinical workers in analyzing the probability of the risk of a certain indicator more intuitively, and providing decision-making support. For example, Ceci F et al developed an innovative clinical nomogram for predicting positive PSA failure in gallium-68 prostate-specific membrane antigen positron emission tomography/computed tomography in different clinical settings., with proved accuracy in predicting positive scans.41
On the basis of six readily accessible clinical and procedural variables, this study successfully developed and externally validated a predictive nomogram for moderate-to-severe pain in patients undergoing ultrasound-guided TPB. The model demonstrated excellent discriminative ability across different cohorts, with AUCs consistently exceeding 0.88. Calibration curves revealed good concordance between predicted probabilities and observed outcomes; and DCA confirmed its substantial clinical net benefit across a broad range of threshold probabilities. Unlike previous studies that predominantly emphasized anatomical or procedural parameters, in our study, the constructed model uniquely integrated psychological factors (eg, anxiety scores), alongside procedural characteristics such as biopsy duration and the number of biopsy needles, contributing to enhancing its predictive accuracy and clinical applicability simultaneously.
The accurate preoperative prediction of severe pain following transurethral prostate biopsy holds significant potential for optimizing healthcare resource utilization and improving economic efficiency. Our model, validated by decision curve analysis, supports a risk threshold of ≥20% for initiating targeted analgesic interventions. This stratification facilitates a differentiated management approach: low-risk patients are suitable for streamlined ambulatory pathways, whereas high-risk patients receive preemptive, multi-modal analgesia. Such a strategy not only mitigates breakthrough pain but also reduces the demand for unscheduled rescue interventions and unplanned admissions, thereby alleviating clinical workload and improving bed turnover. Furthermore, by enhancing patient comfort and predictability, the model may directly contribute to higher patient satisfaction scores—a critical metric in value-based care systems. It may also accelerate the shift towards cost-effective outpatient procedures by increasing clinician confidence in managing post-discharge risks. The proposed economic benefits, however, require future validation through formal cost-effectiveness analyses.
The nomogram can be considered as a practical tool for pre-procedural risk stratification. In our study, the identification of high-risk patients based on this nomogram could facilitate the implementation of personalized perioperative strategies, including optimized anesthesia, targeted anxiety management, and procedural adjustments, ultimately improving patient experience and biopsy tolerance. Nevertheless, several limitations warrant consideration. First, the single-center retrospective design inherently carries the risk of selection bias. Our patient cohort originated from a single tertiary care institution, potentially reflecting specific local demographic patterns and clinical practices; therefore, generalizability may be limited. Second, the retrospective design might introduce potential selection biases. Third, pain assessment relied on subjective patient-reported outcomes (eg, questionnaire-based data collection), which might be disturbed by individual variability in pain perception and unmeasured psychological factors. Finally, this study did not account for potential seasonal variations that may influence patient-reported anxiety and pain, constituting an important direction for future research. Prospective multicenter studies involving independent populations, particularly those with diverse ethnic backgrounds or differing healthcare delivery systems (eg, across multiple countries or hospital types), are needed to further validate and refine this model. Additionally, the predictive performance can be enhanced potentially by integrating more detailed anesthesia variables and comprehensive psychological assessments.
Conclusion
In summary, we have developed and validated a nomogram that identifies key risk factors—including prostate volume, anxiety, and procedural variables—for pain after TPB. To facilitate clinical implementation, a risk threshold of ≥20% is recommended to trigger a multi-modal intervention strategy, such as pre-procedural anxiolytics, enhanced local nerve blocks, and prioritization by experienced operators. The promising performance of this tool warrants further prospective, multi-center studies to confirm its generalizability and cost-effectiveness before widespread adoption.
Abbreviations
PCa, Prostate Cancer; TP, Transperineal; TR, Transrectal; DRE, Digital Rectal Examination; TRUS, Transrectal Ultrasound; PSA, Prostate-Specific Antigen; tPSA, Total PSA; f/t PSA, Free-to-Total PSA Ratio; PSAD, PSA Density; PSAV, PSA Velocity; PCA3, Prostate Cancer Antigen 3; IPSS, International Prostate Symptom Score; Pi-RADS, Prostate Imaging Reporting and Data System; STAI, State-Trait Anxiety Inventory; NRS, Numeric Rating Scale; ROC, Receiver Operating Characteristic Curve; AUC, Area Under the Curve; DCA, Decision Curve Analysis; OR, Odds Ratio; CI, Confidence Interval; MAC, monitored anesthesia care; PNB, periprostatic nerve blockade.
Data Sharing Statement
All data generated or analyzed during this study are included in this published article.
Ethics Approval and Consent to Participate
This study was conducted in accordance with the Declaration of Helsinki and approved by the ethics committee of The First People’s Hospital of Lianyungang (KY-20230525001-01), and all subjects signed the informed consent.
Funding
This study had no funding support.
Disclosure
The authors declared no conflicts of interest in this work.
References
1. Sung H, Ferlay J, Siegel RL, et al. Global cancer statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2021;71(3):209–249. doi:10.3322/caac.21660
2. Xiang J, Yan H, Li J, Wang X, Chen H, Zheng X. Transperineal versus transrectal prostate biopsy in the diagnosis of prostate cancer: a systematic review and meta-analysis. World J Surg Oncol Feb. 2019;17(1):31. doi:10.1186/s12957-019-1573-0
3. Chung HS, Hwang EC, Yu HS. Prevalence of fluoroquinolone‐resistant rectal flora in patients undergoing transrectal ultrasound‐guided prostate needle biopsy: a prospective multicenter study. Int J Urol. 2018;25(3):278–283. doi:10.1111/iju.13511
4. Chang DTS, Challacombe B, Lawrentschuk N. Transperineal biopsy of the prostate—is this the future? Nat Rev Urol. 2013;10(12):690–702. doi:10.1038/nrurol.2013.195
5. Marra G, Zhuang J, Marquis A, et al. Pain in men undergoing transperineal free-hand multiparametric magnetic resonance imaging fusion targeted biopsies under local anesthesia: outcomes and predictors from a multicenter study of 1,008 patients. J Urol. 2020;204(6):1209–1215. doi:10.1097/ju.0000000000001234
6. Li M, Wang Z, Li H. Local anesthesia for transrectal ultrasound-guided biopsy of the prostate: a meta-analysis. Sci Rep. 2017;7(1):40421. doi:10.1038/srep40421
7. Kum F, Elhage O, Maliyil J, et al. Initial outcomes of local anaesthetic freehand transperineal prostate biopsies in the outpatient setting. BJU Int. 2020;125(2):244–252. doi:10.1111/bju.14620
8. Marra G, Marquis A, Tappero S. Transperineal free-hand mpMRI fusion-targeted biopsies under local anesthesia: technique and feasibility from a single-center prospective study. Urology. 2020;140:122–131. doi:10.1016/j.urology.2019.11.078
9. Tsugawa Y, Jena AB, Orav EJ. Age and sex of surgeons and mortality of older surgical patients: observational study. BMJ. 2018;361:k1343. doi:10.1136/bmj.k1343
10. Tasian GE, Harper JD, Al-Khalidi HR, et al. Development of prediction models for severe pain and urinary symptoms after ureteroscopy with ureteral stent placement: results from the stents study and initial validation of pain interference. J Urol. 2025;213(4):475–484. doi:10.1097/ju.0000000000004370
11. Castaño-Asins JR, Barceló-Soler A, Royuela-Colomer E, et al. Effectiveness of peri-operative psychological interventions for the reduction of postsurgical pain intensity, depression, anxiety and pain catastrophising: a systematic review and meta-analysis. Eur J Anaesthesiol. 2025;42(7):609–625. doi:10.1097/eja.0000000000002157
12. Gorsuch RL, Spielberger CD. Anxiety, threat, and awareness in verbal conditioning 1. J. Pers. 1966;34(3):336–347. doi:10.1111/j.1467-6494.1966.tb01718.x
13. Marteau TM, Bekker H. The development of a six‐item short‐form of the state scale of the Spielberger State—Trait Anxiety Inventory (STAI). Br J Clin Psychol. 1992;31(3):301–306. doi:10.1111/j.2044-8260.1992.tb00997.x
14. Ferreira-Valente MA, Pais-Ribeiro JL, Jensen MP. Validity of four pain intensity rating scales. Pain®. 2011;152(10):2399–2404. doi:10.1016/j.pain.2011.07.005
15. Chen W, Sun K, Zheng R, et al. Cancer incidence and mortality in China, 2014. Chin J Cancer Res. 2018;30(1):1–12. doi:10.21147/j.issn.1000-9604.2018.01.01
16. Lenfant L, Barret E, Rouprêt M, Rozet F, Ploussard G, Mozer P. Transperineal prostate biopsy is the new black: what are the next targets? Eur Urol. 2022;82(1):3–5. doi:10.1016/j.eururo.2022.01.046
17. Kim DK, Lee JY, Jung JH, et al. What is the most effective local anesthesia for transrectal ultrasonography-guided biopsy of the prostate? A systematic review and network meta-analysis of 47 randomized clinical trials. Sci Rep. 2019;9(1):4901. doi:10.1038/s41598-019-41412-w
18. Rodriguez LV, Terris MK. Risks and complications of transrectal ultrasound guided prostate needle biopsy: a prospective study and review of the literature. J Urol. 1998;160(6):2115–2120. doi:10.1016/S0022-5347(01)62255-9
19. Zisman A, Leibovici DAN, Kleinmann J, Siegel YI, Lindner A. The impact of prostate biopsy on patient well-being: a prospective study of pain, anxiety and erectile dysfunction. J Urol. 2001;165(2):445–454. doi:10.1097/00005392-200102000-00023
20. Peyromaure M, Ravery V, Messas A, Toublanc M, Boccon-Gibod L. Pain and morbidity of an extensive prostate 10-biopsy protocol: a prospective study in 289 patients. J Urol. 2002;167(1):218–221. doi:10.1016/S0022-5347(05)65416-X
21. Macefield RC, Metcalfe C, Lane JA. Impact of prostate cancer testing: an evaluation of the emotional consequences of a negative biopsy result. Br. J. Cancer. 2010;102(9):1335–1340. doi:10.1038/sj.bjc.6605648
22. Borghesi M, Ahmed H, Nam R. Complications after systematic, random, and image-guided prostate biopsy. Europ urol. 2017;71(3):353–365. doi:10.1016/j.eururo.2016.08.004
23. Tang J, Gibson SJ. A psychophysical evaluation of the relationship between trait anxiety, pain perception, and induced state anxiety. J Pain. 2005;6(9):612–619. doi:10.1016/j.jpain.2005.03.009
24. Rhudy JL, Meagher MW. Fear and anxiety: divergent effects on human pain thresholds. Pain. 2000;84(1):65–73. doi:10.1016/S0304-3959(99)00183-9
25. Van Vlymen JM, Sarego MM, White PF. Benzodiazepine premedication: can it improve outcome in patients undergoing breast biopsy procedures? Anesthesiology. 1999;90(3):740–745. doi:10.1097/00000542-199903000-00016
26. Milligan DW, Howard MR, Judd A. Premedication with lorazepam before bone marrow biopsy. J Clin Pathol. 1987;40(6):696–698. doi:10.1136/jcp.40.6.696
27. Eisenberg E, Konopniki M, Veitsman E, Kramskay R, Gaitini D, Baruch Y. Prevalence and characteristics of pain induced by percutaneous liver biopsy. Anesthesia Analg. 2003;96(5):1392–1397. doi:10.1213/01.ANE.0000060453.74744.17
28. Kyriakides R, Jones P, Geraghty R. Effect of music on outpatient urological procedures: a systematic review and meta-analysis from the European Association of Urology Section of Uro-Technology. J Urol. 2018;199(5):1319–1328. doi:10.1016/j.juro.2017.11.117
29. Lang EV, Berbaum KS, Faintuch S. Adjunctive self-hypnotic relaxation for outpatient medical procedures: a prospective randomized trial with women undergoing large core breast biopsy. Pain. 2006;126(1–3):155–164. doi:10.1016/j.pain.2006.06.035
30. Hole J, Hirsch M, Ball E, Meads C. Music as an aid for postoperative recovery in adults: a systematic review and meta-analysis. Lancet. 2015;386(10004):1659–1671. doi:10.1016/S0140-6736(15)60169-6
31. Bradt J, Dileo C, Magill L, Teague A. Music interventions for improving psychological and physical outcomes in cancer patients: reviews. Cochrane Database Syst Rev. 2016. doi:10.1002/14651858.CD006911.pub3
32. Weldon SM, Korkiakangas T, Bezemer J, Kneebone R. Music and communication in the operating theatre. J Adv Nurs. 2015;71(12):2763–2774. doi:10.1111/jan.12744
33. Burchiel KJ, Russell LC, Lee RP, Sima AAF. Spontaneous activity of primary afferent neurons in diabetic BB/Wistar rats: a possible mechanism of chronic diabetic neuropathic pain. Diabetes. 1985;34(11):1210–1217. doi:10.2337/diab.34.11.1210
34. Misawa S, Sakurai K, Shibuya K. Neuropathic pain is associated with increased nodal persistent Na+ currents in human diabetic neuropathy. J Peripheral Nerv Syst. 2009;14(4):279–284. doi:10.1111/j.1529-8027.2009.00239.x
35. Fischer TZ, Waxman SG. Neuropathic pain in diabetes—evidence for a central mechanism. Nat Rev Neurol. 2010;6(8):462–474. doi:10.1038/nrneurol.2010.90
36. De SM, D’armiento M, Di LG. The need to reduce patient discomfort during transrectal ultrasonography‐guided prostate biopsy: what do we know? BJU Int. 2005;96(7):977–983. doi:10.1111/j.1464-410X.2005.05736.x
37. Nakai Y, Tanaka N, Matsubara T. Effect of prolonged duration of transrectal ultrasound-guided biopsy of the prostate and pre-procedure anxiety on pain in patients without anesthesia. Res Rep Urol. 2021;Volume 13:111–120. doi:10.2147/RRU.S297703
38. Bastide C, Lechevallier E, Eghazarian C, Ortega JC, Coulange C. Tolerance of pain during transrectal ultrasound-guided biopsy of the prostate: risk factors. Prostate Cancer Prostatic Dis. 2003;6(3):239–244. doi:10.1038/sj.pcan.4500664
39. Yun TJ, Lee HJ, Kim SH. Prospective analysis on the relation between pain and prostate volume during transrectal prostate biopsy. Korean J Radiol. 2007;8(3):231–235. doi:10.3348/kjr.2007.8.3.231
40. Sonmez G, Tombul ST, Demirtas T, Demirtas A. Risk factors associated with pain in fusion prostate biopsy. Prostate Int. 2020;8(4):185–189. doi:10.1016/j.prnil.2020.05.004
41. Ceci F, Bianchi L, Borghesi M, et al. Prediction nomogram for (68)Ga-PSMA-11 PET/CT in different clinical settings of PSA failure after radical treatment for prostate cancer. Eur J Nucl Med Mol Imaging. 2020;47(1):136–146. doi:10.1007/s00259-019-04505-2
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.