Back to Journals » Risk Management and Healthcare Policy » Volume 12
Developing a Hospital Disaster Risk Management Evaluation Model
Authors Abbasabadi Arab M ![]() , Khankeh HR
, Khankeh HR ![]() , Mosadeghrad AM, Farrokhi M
, Mosadeghrad AM, Farrokhi M
Received 12 May 2019
Accepted for publication 18 November 2019
Published 10 December 2019 Volume 2019:12 Pages 287—296
DOI https://doi.org/10.2147/RMHP.S215444
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Kent Rondeau
Masoumeh Abbasabadi Arab,1 Hamid Reza Khankeh,1 Ali Mohammad Mosadeghrad,2 Mehrdad Farrokhi1
1Health in Emergency and Disaster Research Center, University of Social Welfare and Rehabilitation Sciences, Tehran, Iran; 2Management and Economics School of Public Health, Tehran University of Medical Sciences, Tehran, Iran
Correspondence: Hamid Reza Khankeh
Health in Emergency and Disaster Research Center, University of Social Welfare and Rehabilitation Sciences, Kodakyar Street, Velenjak, Tehran, Iran
Tel +98 21 2218 0160
Fax +98 22 180 160
Email [email protected]
Purpose: Disasters are increasing worldwide and hospitals should be prepared to respond well to such disasters. An effective hospital disaster risk management program saves peoples’ lives, reduces damage to the hospital properties and assures hospital service continuity. This article aimed to develop and verify a Hospital Disaster Risk Management Evaluation model (HDRME).
Methods: A mixed-method explanatory sequential approach was used to develop and verify the HDRME model. The first draft of the HDRME model was introduced through a comprehensive literature review of major databases (i.e., PubMed, Scopus, Web of Science, and Science Direct), using appropriate keywords. Furthermore, 18 in-depth individual interviews were conducted with well-known experts in DRM to identify more HDRME constructs, sub-constructs, and standards. Then, three rounds of Delphi were conducted with 22 experts in hospital disaster risk management to verify the proposed model.
Results: The proposed HDRME consists of eight constructs, including seven enablers (management and leadership; risk assessment; planning; prevention and mitigation; preparedness; response, and recovery) and one result (key performance results). These constructs were further broken into 27 sub-constructs. The enablers and results scored 85% and 15% of the model’s total scores.
Conclusion: A comprehensive conceptual framework for the evaluation of hospital disaster risk management was introduced and verified. Standards and measurable elements can be embedded in this conceptual model to measure a hospital’s preparedness in disasters and accordingly, corrective actions can be taken to strengthen the hospitals’ responses to the disasters. However, the proposed model should be validated in a hospital setting through implementation.
Keywords: hospital, disaster, risk management, evaluation, model
Introduction
Disasters are inevitable and cause social and economic problems for the people and governments. About 315 natural disasters occurred in 2018 and Asia experienced the highest percentage of disasters (44%). Almost 68.5 million people were affected, and 11,804 deaths were reported, with an economic loss of US$131. 7 billion.1
International agreements have done for Disaster Risk Reduction and the building of resilience to disasters in the world.2 Three international frameworks for disaster risk reduction (DRR) are consist of: the Yokohama Strategy and Plan of Action for a Safer World, the Hyogo Framework for Action 2005–2015, and the Sendai Framework for Disaster Risk Reduction 2015–2030 (SFDRR). Disaster risk management (DRM) as a comprehensive all-hazard approach develops and implements strategies for each phase of the disaster life cycle (i.e. Prevention and mitigation, preparedness, response, and recovery).3,4
Hospitals play important roles in saving the lives and reducing the suffering of injured people during and after disasters. Hospitals are expected to create a safe environment for patients, visitors, and staff and provide health care services to disasters’ casualties. Hence, an effective hospital disaster risk management program should be planned and implemented. However, the Iranian hospital preparedness for disaster response is low and moderate.5–8
Evaluation is the regular review of program activity, output, and outcome, with an emphasis on lessons learned.3 The performance of hospitals’ DRM program should be measured and assessed and accordingly corrective actions should be planned and implemented. There is a persistent need for valid, reliable and comprehensive tools for DRM evaluation. Systematic review studies on hospital preparedness’s tools in the world have shown that these tools do not meet all dimensions that required for hospital preparedness.9–11 Also, despite advances in research, program and plan development in the field of hospital preparedness, there are no globally accepted standards for hospital DRM.3
There are many organization’ performance evaluation models in the world, which use systematic models. These models include a system of structural requirements, processes, and outcomes for health care organizations that include a number of primary and secondary dimensions.12 There are few models for the DRM conceptual framework. The traditional disaster life cycle consisted of four phases (i.e. Prevention and mitigation, preparedness, response and, recovery)13 which address the process of disaster risk management. Nirupama (2013) identified seven domains as key elements of a comprehensive disaster risk management: 1-Threat recognition, risk and vulnerability Identification; 2- Risk analysis and Assessment; 3- Risk control options, structural, non-structural, cost/benefit analysis; 4- Strategic planning, economic, political and institutional support considerations; 5- Response, recovery, reconstruction, rehabilitation; 6- Knowledge management, sustainable development; and 7- Resilience building, community participation.14,15 Zhong (2014) developed a hospital resilience conceptual framework consisted of four criteria, including redundancy, robustness, rapidity and, resourcefulness.16
A comprehensive and systemic conceptual framework for performance evaluation should be used to host DRM standards and measurement elements. A DRM evaluation model should consider the structures, processes and outputs/outcomes, which current DRM models have not addressed. However, other elements such as leadership, management commitment, funding, regulations, risk assessment, planning, information system and partnership with other organizations, etc. should also be considered in any attempt to evaluate a hospital’s DRM program.17–20 Therefore, this study aimed to develop and verify a comprehensive Hospital Disaster Risk Management Evaluation model (HDRM) which introduce constructs, sub-constructs, standards of DRM and evaluation tool for DRM hospitals.
Materials and Methods
A Mixed-method explanatory sequential approach was used in this study to develop and verify the HDRME model. First, a critical review on major databases including PubMed, Scopus, Web of Science, and Science Direct, using keywords including “evaluation models”, “hospital disaster risk management”,” disaster risk management model or framework”, “hospital Preparedness checklist”, “hospital preparedness tools” was conducted to identify the evaluation models, constructs and sub-constructs of DRM. In addition, for identifying international and national standards, a comparative study of Disaster Risk Management accreditation standards of 10 countries including USA, Canada, Australia, Malaysia, India, Turkey, Thailand, Egypt, Saudi Arabia, and Denmark was examined to extend the list of HDRME model constructs and sub-constructs. Furthermore, 18 in-depth individual interviews were conducted with well-known experts in DRM to identify more HDRME constructs, sub-constructs, standards, and measurable elements. Then, the research team developed the first draft of the HDRME model using the grounded theory.21
Finally, three rounds of a Delphi study were conducted to verify the proposed HDRME model. The Delphi study was performed between January and August 2018. Twenty- two experts in hospital disaster management participated in this Delphi study. Experts were professors in health in emergencies & disasters, the staff of the Emergency Department in the ministry of health and disaster management center in universities of medical sciences, Emergency Medicine Specialist and Secretary of the DRM committee in hospitals. Twenty- two experts completed the first round, and 21 experts completed the second and the third rounds. The Delphi panelists’ key demographic characteristics are presented in (Table 1).
 |
Table 1 The Demographic Characteristics of Delphi Panel Experts |
The proposed HDRME model’s constructs and sub-constructs were presented to the expert panel during the first round of the Delphi study and they were asked to comment on the model and its constructs and sub-constructs. They were also asked to comment on the rationality, comprehensiveness, suitability, and applicability of the proposed model in hospitals. Experts’ answers were reviewed and incorporated in the second draft of the model. The revised model was then, presented to the Delphi panelists in the second round. They were asked to give a score between 1 (very low) and 10 (very much) to the HDRME model’s constructs, sub-constructs, its logic and rationality, comprehensiveness, suitability, feasibility and applicability in the hospitals. A score of 70% and more (score 7 and 10) was considered as acceptable from the panelist’s side.22,23 The results of the second round were analyzed. The mean and standard deviation for each question were calculated and sent back to the Delphi panelists for the third round. They were asked to give a score between 1 and 10 to each question. The experts were also asked to give a weight to each construct of the HDRME model out of 100.
Results
The preliminary HDRME model consisted of nine constructs (management and leadership, risk assessment, planning, staff management, patient management, resource management, safety and security, incident management, and key performance results) and 38 sub-constructs (Figure 1). The Delphi experts in the first round agreed to keep constructs such as “management and leadership”, “risk assessment”, “planning”, and “key performance results in the HDRME model. However, about 81% of experts believed that it would be better to add the DRM cycle (i.e. Prevention and mitigation, preparedness, response, and recovery) to the proposed model. Thus, the DRM cycle constructs were substituted with the “staff management”, “patient management”, “resource management”, “safety and security”, and “incident management” in the HDRME model. For example, the sub-constructs of “staff management” and “resource management” were incorporated in the “preparedness”, “response” and “recovery” constructs; the sub-constructs of “patient management” was incorporated in the “response” and “recovery” constructs; the sub-constructs of the “safety and security” was merged in “prevention and mitigation”, and “response” constructs, and finally, the elements of “incident management” was merged in the “preparedness” and “response” constructs the HDRME model. The experts’ comments and suggestions were considered in the model for further development. As a result, the HDRME model was consisted of 8 constructs and 26 sub-constructs including “management and leadership”, “risk assessment”, “planning”, “prevention and mitigation”, “preparedness”, “response”, “recovery”, and “key performance results”. (Figure 2).
 |
Figure 1 The preliminary model of hospital disaster risk management evaluation model. |
 |
Figure 2 Conceptual framework of hospital disaster risk management evaluation (HDRME) model. |
The statistical result (mean scores and standard deviation) for the HDRME model, constructs and sub-constructs are presented in (Table 2). The second round Delphi results showed that the panelists did not agree with the comprehensiveness and the rationality of the “risk assessment” and “planning” constructs and they achieved a score less than 7. Experts provided some suggestions on how to improve these constructs. Their comments were considered in the model and the revised model with 8 constructs and 27 sub-constructs were presented to the experts for further comments. The findings of the third round showed that the Delphi experts were considered the proposed model valid, comprehensive, suitable, feasible and applicable to the hospitals. (Figure 3) shows the final HDRME model constructs and sub-constructs. The results of the model constructs’ weighting are presented in (Table 3). The “Key Performance results” and “risk assessment” constructs had the highest scores among the HDRME constructs. About 27 international standards were extracted from the comparative study of hospital DRM accreditation standards and interviewed by experts added 30 national standards (totally 57 standards).24 These standards added to construct and sub-constructs of HDRME model. Final checklists were determined by standards for each sub-constructs. (Figure 4) shows the relationship between the HDRME model and the standards.
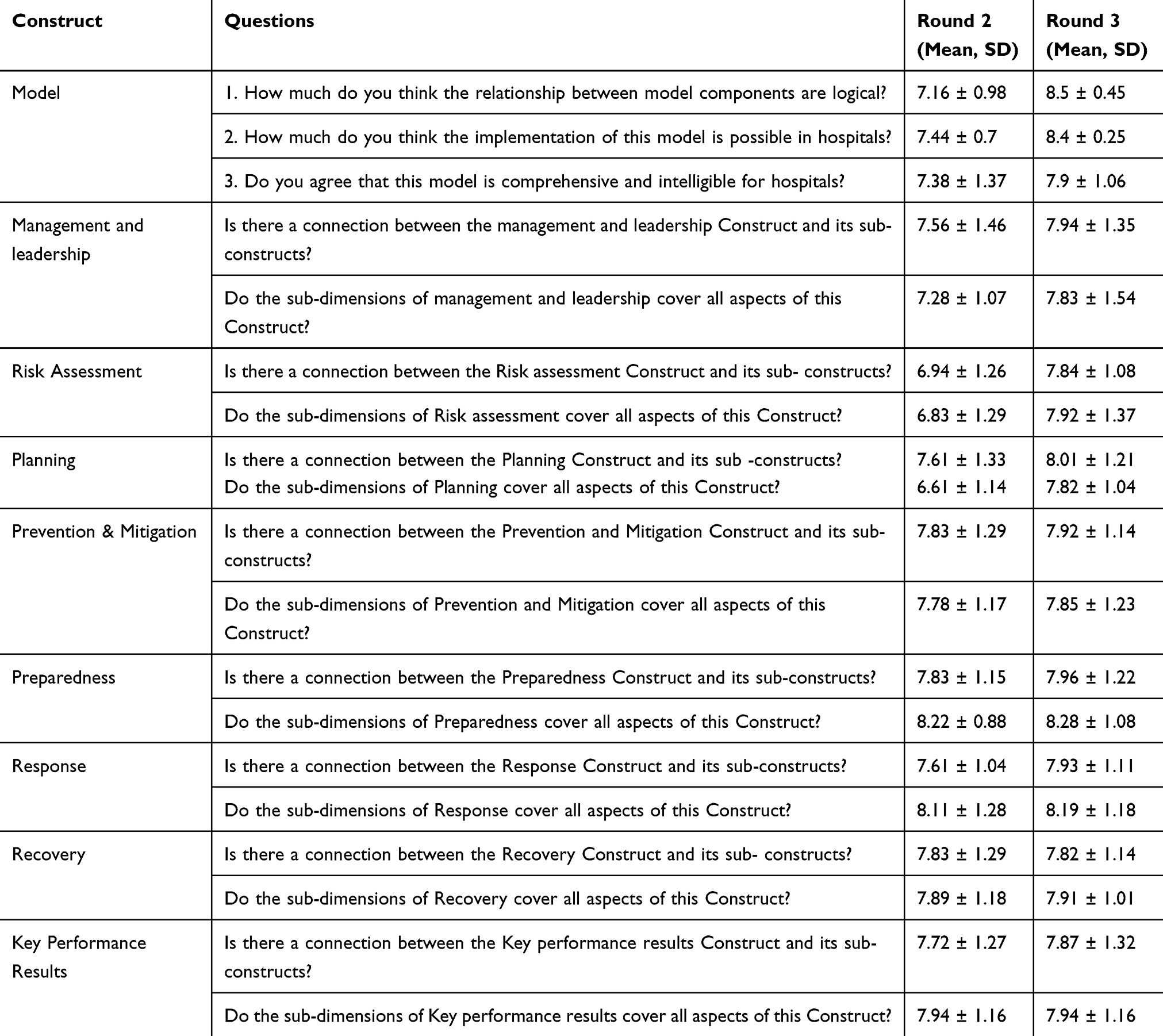 |
Table 2 The Statistical Result for HDRME Model, Construct and Sub-Construct of HDRME Model in Second and Third Round of Delphi Study |
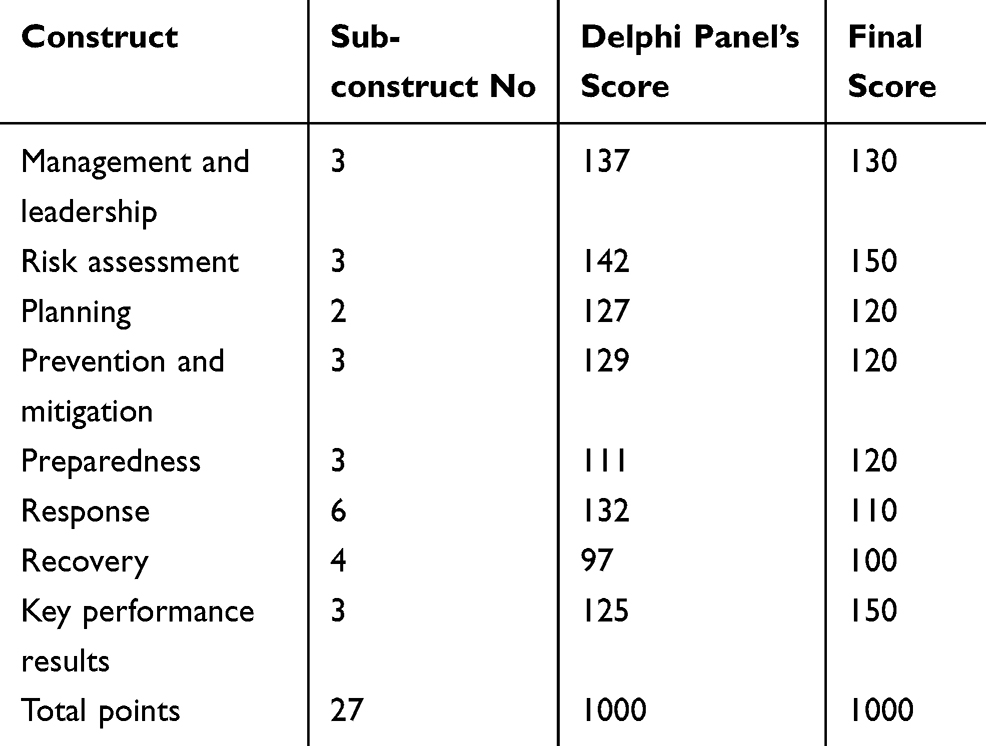 |
Table 3 Constructs and Score of HDRME Model |
 |
Figure 3 Final construct and sub-constructs of (HDRME) model. |
 |
Figure 4 The relationship between the HDRME model and the standards. |
Discussion
A comprehensive conceptual framework for hospital disaster risk management evaluation (HDRME) was introduced and verified in this study. The HDRME model has eight constructs of which seven are enablers (“Management and leadership”, “Risk assessment”, “Planning”, “Prevention and mitigation”, “Preparedness”, “Response”, and “Recovery”) and one is the result (“Key performance results”). These constructs were further broken into 27 sub-constructs. These constructs and sub-constructs cover the traditional DRM cycle and the elements of disaster risk management model introduced by Nirupama (2013) and the hospital resilience conceptual framework developed by Zhong (2014). (Table 4) shows the Comparison of HDRME model constructs with other DRM models.
 |
Table 4 The Comparison of HDRME Model Constructs with Other DRM Models |
The HDRME model can be defined as “an integrated system of principles, processes and best practices that provide a framework to improve hospital disaster preparedness”.
Management and leadership have critical roles in the DRM. Hospital managers’ commitment, involvement, and support, allocating resources to implement plans, and developing community involvement programs are important for the success of the DRM program. Senior managers should pay more attention to the prevention stage of the DRM and enhance the safety of the hospital environment. They must create a safe and sustainable environment for patients and staffs through developing guidelines and standards for various hospital departments and units. Hospitals need a well-established structure for the DRM such as the DRM committee, the incident command system (ICS) and the hospital command center (HCC). Furthermore, a good external relationship should be established with community relief organizations.25 A hospital’s capability to provide the best healthcare services to casualties during a disaster is dependent on its capability to effective coordination with other organization and service providers.26 One of the key elements of the Conceptual Framework of Healthcare Resilience Zhong & et al is “Emergency Leadership and coordination” that pay attention to hospital collaboration with other agencies.22 Initiating and developing a could help hospital managers to use their resources and technical assistance for disaster situation management.
Disaster planning starts with hazards vulnerability analysis and risk assessment to explore the most probable hazards in a hospital, prevent and mitigate the effects of the hazards on the hospital’s structural and non-structural elements.3 This key construct involves identifying the risks of natural and man-made hazards and recognizing vulnerable elements of the organization. Risk assessment, using quantitative or qualitative data, estimate the levels of the risk and develops plans. Risk assessment should not be limited only to the prevention and mitigation phase of the DRM cycle. It has to cover the whole disaster management cycle, including preparedness, response, and recovery, especially in cascade events.
Planning is also important in the DRM. Planning determines how managers establish a long-term vision, develop the values required for long-term success of the hospital, set DRM goals and objectives, and implements them via appropriate policies and action plans. A comprehensive hospital disaster plan should consider all hazards, all DRM phases, and all levels of the hospital. The hospital DRM plan should be implemented thoroughly and reviewed on a regular basis. Resources should be available to the lower managers and employees to implement the DRM plan.8 The plans must be exercise and revised if it was necessary.
The first stage of the disaster life cycle is related to the prevention and mitigation to reduce the severity of an event. It also includes actions that reduce potential physical damage to facilities during an event. Hence, at this stage, the safety of hospital’s structural and non-structural elements should be enhanced to reduce the effects of the hazards.
Preparedness is defined as the knowledge and capacities developed by governments, recovery organizations, communities and individuals to effectively anticipate, respond, and improve, likely effects, impending an Accidents or Dangerous Areas.27 It includes actions such as early warning systems, surge capacity, response strategies, disaster exercises, and training. Surge capacity is defined as the ability of an organization to expand rapidly and augment services in response to one or multiple disasters.28 The provision of support services plays a key role in the success of hospitals in disasters. Hospitals with more precise support provision plans were more successful in responding to disasters.20 Early warning system is the first component of every response plan.29 The Sendai Framework for Disaster Risk Reduction 2015–2030 (SFDRR), early warning system was considered as an important special goal.2 Staff training and exercises are crucial in enhancing hospital employees’ preparedness.
Response refers to the immediate and ongoing activities, programs and tasks, eg incident command system activation, casualties’ triage, and management, staff & volunteers’ management, resource management, information management, safety & security. Good pre-event planning, and efficient resource coordination and allocation are critical to the success of the response stage.17 Volunteers’ management in disasters including identifying, supervising and evaluating their performance, is also of great importance.
Recovery covers restoration, reconstruction, and improvement of facilities, livelihoods and living conditions of affected communities. Recovery was given a higher priority in the development of standards. In this dimension, business continuity of services had addressed only in the accreditation standards of the pioneering countries. Moreover, paying attention to the personnel and their mental recovery is one of the overlooked dimensions of sustainable development.
Key performance results measure the performance of the hospital in disasters in terms of the effects of the DRM on organization, employees, and the society using output, outcome and impact key performance indicators. A systematic review concluded that there is a lack of post-disaster evaluations.30 The Nirupama DRM model focuses on the consequences of DRM, including Resilience building, community participation, sustainable development and knowledge management.14
Weighting to model constructs was determined by national experts, with 85% devoted to enablers and 15% to results. Since in our country, we are still at the beginning of implementing DRM processes and it takes more time to achieve key performance results. The weight of each of constructs of HDRME model can be changed depending on status and importance in other countries.
Conclusion
The hospital disaster risk management evaluation model is a logical and systematic framework for evaluating the structures, processes and outputs/outcomes of a hospital disaster risk management. This study sets out to introduce and develop a comprehensive conceptual framework and a systemic approach to DRM and logic relation between key constructs. The HDRME can be used as a self-assessment framework by hospital managers to recognize their DRM strengths and weaknesses and accordingly apply corrective actions. It shows a clear picture of a hospital’s preparedness for disasters. It also can be used for comparing the DRM programs of various hospitals in a region.
Study Limitations and Implications for Future Research
A comprehensive HDRM model was developed using an intensive literature review and in-depth interviews and verified by DRM experts. However, the proposed model should be validated in a hospital setting through implementation.
Ethics Approval
This article was taken from a doctoral thesis and was approved by the University of Social Welfare and Rehabilitation Sciences Ethics Committee, with approval code IR.USWR.REC.1396.290.
Acknowledgments
The authors would like to thank the distinguished referees who contributed to the quality of this paper with their constructive comments. The authors also acknowledge Dr. Akbar Biglarian who was a member of the research team and the statistic co-supervisor, for their contributions to this work.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Centre for Research on the Epidemiologyof Disasters (CRED). CRED Crunch 54 - Disasters 2018: Year in Review. CRED; 2019.
2. UNISDR, U. Sendai framework for disaster risk reduction 2015–2030.
3. Ciottone GR, Biddinger PD, Darling RG, et al. Ciottone’s Disaster Medicine. Elsevier Health Sciences; 2015.
4. Schipper L, Pelling M. Disaster risk, climate change and international development: scope for, and challenges to, integration. Disasters. 2006;30(1):19–38. doi:10.1111/disa.2006.30.issue-1
5. Ardalan A, Kandi Keleh M, Saberinia A, et al. 2015 estimation of hospitals safety from disasters in I.R.Iran: the results from the assessment of 421 hospitals. PLoS One. 2016;11(9):e0161542. doi:10.1371/journal.pone.0161542
6. Asefzadeh S, Rajaee R, Ghamari F, et al. Preparedness of Iranian hospitals against disasters. Biotechnol Health Sci. 2016;3(3). doi:10.5812/bhs
7. Nasiripour A, Raisee P, Mahboubi M. Study of preparedness rate of marginal hospitals encounters crises. Health Manage J. 2007;10(28):41–48.
8. Djalali A, Castren M, Khankeh H, et al. Hospital disaster preparedness as measured by functional capacity: a comparison between Iran and Sweden. Prehosp Disaster Med. 2013;28(5):454–461. doi:10.1017/S1049023X13008807
9. Heidaranlu E, Ebadi A, Khankeh HR, Ardalan A Hospital disaster preparedness tools: a systematic review. PLoS Curr. 2015;7.
10. Nekoie-Moghadam M, Kurland L, Moosazadeh M, et al. Tools and checklists used for the evaluation of hospital disaster preparedness: a systematic review. Disaster Med Public Health Prep. 2016;10(5):781–788. doi:10.1017/dmp.2016.30
11. Tang R, Fitzgerald G, Hou X-Y, et al. Building an evaluation instrument for China’s hospital emergency preparedness: a systematic review of preparedness instruments. Disaster Med Public Health Prep. 2014;8(1):101–109. doi:10.1017/dmp.2014.10
12. Bahadori M, Izadi AR, Ghardashi F, Ravangard R, Hosseini SM. The evaluation of hospital performance in Iran: a systematic review article. Iran J Public Health. 2016;45(7):855.
13. Wallace WA, De Balogh F. Decision support systems for disaster management. Public Adm Rev. 1985;134–146. doi:10.2307/3135008
14. Nirupama N. Disaster Risk Management, in Encyclopedia of Natural Hazards. Springer; 2013:164–170.
15. Agrawal N. Natural Disasters and Risk Management in Canada: An Introduction. Vol. 49. Springer; 2018.
16. Zhong S, Clark M, Hou X-Y, et al. Development of hospital disaster resilience: conceptual framework and potential measurement. Emerg Med J. 2014;31(11):930–938. doi:10.1136/emermed-2012-202282
17. Khankeh HR, Khorasani-Zavareh D, Johanson E, et al. Disaster health-related challenges and requirements: a grounded theory study in Iran. Prehosp Disaster Med. 2011;26(3):151–158. doi:10.1017/S1049023X11006200
18. Zhong S, Clark M, Hou X-Y, et al. Progress and challenges of disaster health management in China: a scoping review. Glob Health Action. 2014;7:24986. doi:10.3402/gha.v7.24986
19. Barbera JA, Yeatts DJ, Macintyre AG. Challenge of hospital emergency preparedness: analysis and recommendations. Disaster Med Public Health Prep. 2009;3(S1):S74–S82. doi:10.1097/DMP.0b013e31819f754c
20. Wise RA. The creation of emergency health care standards for catastrophic events. Acad Emergency Med. 2006;13(11):1150–1152. doi:10.1197/acem.2006.13.issue-11
21. Strauss A, Corbin J. Basics of Qualitative Research Techniques. Thousand Oaks, CA: Sage publications; 1998.
22. Zhong S, Clark M, Hou X-Y, et al. Development of key indicators of hospital resilience: a modified Delphi study. J Health Serv Res Policy. 2015;20(2):74–82. doi:10.1177/1355819614561537
23. Wakai A, O’Sullivan R, Staunton P, et al. Development of key performance indicators for emergency departments in Ireland using an electronic modified-Delphi consensus approach. Eur J Emergency Med. 2013;20(2):109–114. doi:10.1097/MEJ.0b013e328351e5d8
24. Khankeh H, Mosadeghrad AM, Abbasabadi Arab M. Developing accreditation standards for disaster risk management: an approach for hospital preparedness improvement–editorial. J Mil Medi. 2019;20(6):574–576.
25. Adelaine SA, Shoaf K, Harvey C. An assessment of collaboration and disasters: a hospital perspective. Prehosp Disaster Med. 2016;31(2):121–125. doi:10.1017/S1049023X16000066
26. Adalja AA, Watson M, Bouri N, et al. Absorbing citywide patient surge during Hurricane Sandy: a case study in accommodating multiple hospital evacuations. Ann Emerg Med. 2014;64(1):66–73. doi:10.1016/j.annemergmed.2013.12.010
27. UNISDR, M. UNISDR Terminology for Disaster Risk Redution. Switzerland: United Nations International Strategy for Disaster Reduction (UNISDR) Geneva; 2009.
28. ASTM IS. Historical Standard: ASTM E2413-04 Standard Guide for Hospital Preparedness and Response. The American Society for Testing and Materials (ASTM); 2009.
29. Khankeh H, Masoumi G. National Hospital Disaster Risk Management Program Based on Accreditation Indicators.
30. Smith EC, Burkle FM, Aitken P, et al. Seven decades of disasters: a systematic review of the literature. Prehosp Disaster Med. 2018;33(4):418–423. doi:10.1017/S1049023X18000638
 © 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.