Back to Journals » Patient Preference and Adherence » Volume 17
Developing a Culturally Appropriate Tool to Support Self-Care in Migrants with Type 2 Diabetes – A Co-Design Study
Authors Pettersson S ![]() , Klompstra L
, Klompstra L ![]() , Jirwe M, Jaarsma T
, Jirwe M, Jaarsma T ![]()
Received 18 July 2023
Accepted for publication 8 September 2023
Published 13 October 2023 Volume 2023:17 Pages 2557—2567
DOI https://doi.org/10.2147/PPA.S426908
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Johnny Chen
Sara Pettersson,1 Leonie Klompstra,1 Maria Jirwe,2 Tiny Jaarsma1
1Linkoping University, Department of Health, Medicine and Caring Sciences, Linkoping, Sweden; 2Red Cross University College, Department of Health Sciences, Huddinge, Sweden
Correspondence: Sara Pettersson, Linköping University, Department of Health, Medicine and Caring Sciences, SE 601 74, Norrköping, Sweden, Tel +4611363635, Fax +4611125448, Email [email protected]
Introduction: Migrants, especially from the Middle East, experience poorer health outcomes and face greater difficulties in accessing healthcare compared to native populations and there is a need for culturally appropriate education for this vulnerable group. The purpose of this study is to describe the process of developing a culturally appropriate tool to support self-care in migrants with type 2 diabetes.
Methods: In this Co-design study, a tool for supporting self-care in migrants with type 2 diabetes was developed. Migrant patients with type 2 diabetes, healthcare providers and researchers participated in the process, which was based on six elements; engage, plan, explore, develop, decide and change. From February 2021 to December 2022, idea groups were conducted, and a tool was developed through brainstorming, prioritizing and prototyping.
Results: In total, 14 migrant patients, ten health care providers and four researchers participated in the Co-design process. The patients wished to receive information about type 2 diabetes self-care behaviour in their own languages. The healthcare providers asked for clear instructions on where to guide their patients regarding reliable information about diabetes in the patient’s own language. All participants agreed that information can be presented in different formats, either: text (paper or online), audio-visual via recorded videos and/or lectures and pictures.
Discussion: The Co-design process led to several important insights and experiences related to the importance of diverse cultural backgrounds. When conducting a Co-design study with end-users as stakeholders, it is significant that the stakeholders have a diverse background in experiences, both as patients as well as those who deliver or implement the health service. In this study it was of great importance to include patients with diverse backgrounds regarding; gender, age, health literacy, occupation, years living in Sweden and duration of diabetes.
Keywords: type 2 diabetes, self-care, culture, patient education, primary healthcare
Introduction
The global prevalence of diabetes has been increasing over recent decades, from 108 million people with the disease in 1980 (NCD 2016) to an estimated 783 million in 2045, and the majority suffer from type 2 diabetes.1 Type 2 diabetes increases the risk of developing several serious health problems, which leads to personal suffering, reduced quality of life, increased mortality and high medical costs for the individual and society2 (IDF 2019). Individuals with diabetes are also more likely to have serious complications from COVID-19.3–6 While type 2 diabetes is a significant health concern, its associated complications can be averted or postponed through proper self-care practices. Therefore, effective self-care, coupled with maintaining optimal glycemic control, stands as the fundamental cornerstone of treatment for individuals diagnosed with type 2 diabetes.7
According to the middle-range theory of self-care in chronic illness8 self-care can be defined as “a process of maintaining health by promoting health practices and managing illness”. Self-care can be seen as an overarching concept, built on three aspects: self-care maintenance, self-care monitoring and self-care management, where self-care maintenance is defined as behaviours that patients with a chronic illness implement to maintain physical and emotional stability. These behaviours can be entirely self-determined or reflect recommendations from a healthcare provider. Self-care monitoring refers to the process of being observant of symptoms and signs of changes. Self-care management is defined as the patients’ response to symptoms and signs of changes if they occur.8
Self-care in patients with type 2 diabetes entails many decisions in daily life related to diet, physical activity, medication and blood glucose monitoring9 and demands both knowledge and skills.10
Migration can have a significant impact on the health of individuals, particularly those who are living with chronic conditions or develop a chronic condition, such as diabetes, after migrating. Migrants with type 2 diabetes face unique challenges related to language barriers, cultural differences and access to healthcare. At the same time, global migration is increasing and today about 281 million people worldwide are migrants.11
The increasing prevalence of type 2 diabetes among migrants in Europe is well documented and forms challenges for many European countries.12–14 Migrants include foreign-born people who have moved to another country, either voluntarily as immigrants or involuntarily as refugees.15 Today, Sweden, like many other European countries, is a multicultural society15 and over the last decade, migration to Sweden predominately includes migrants of non-European origin, especially refugees from the Middle East.16
Country of birth is an independent risk factor for developing type 2 diabetes and people from the Middle East who migrate to Nordic countries have a higher prevalence of diabetes, compared to the native population. This emphasizes the impact migration may have on health outcomes, indicating complex interplay between genetic susceptibility, cultural shifts, lifestyle modifications, and environmental factors.17,18 Poor glycaemic control is lower in migrants from the Middle East who receive diabetes care in countries with a different culture than their own.19–21 Culture is one of the factors influencing self-care in chronic illness, like diabetes.22 Culture consists of knowledge, values, beliefs, assumptions, perspectives, attitudes, norms and the customs people experience when participating in a society or a certain group23 thus the type of healthcare required may look different for people with another cultural background than the native population.24
Diabetes healthcare often contributes to inequalities between the native population and people with other cultural backgrounds.12 Factors that could attribute to those inequalities includes cultural barriers to accessing healthcare, linguistic and cultural differences, varying health literacy levels, and awareness of diabetes management practices.25 Since research shows the benefits of culturally appropriate diabetes education compared to conventional diabetes education, educational models should be addressing the unique needs of individuals with diabetes from various cultural backgrounds, to be able to reduce disparities in diabetes healthcare.24,26 Culturally appropriate health education is defined as health education tailored to cultural or religious beliefs and linguistic and literacy skills.26 However, diabetes patient education needs to be developed, where culture is taken into consideration by culturally competent healthcare providers to improve self-care in multicultural societies.24,27 There is a need for targeted diabetes education programs for migrants from the Middle East who have migrated to Europe.28 One way to support migrants with their diabetes self-care, is by developing a culturally appropriate tool that addresses the needs of individuals with diabetes from cultural backgrounds.26 Thus, the purpose of this study is to describe the process of developing a culturally appropriate tool to support self-care in migrants with type 2 diabetes.
Research Design
This Co-design study29,30 aims to develop a culturally appropriate tool to support self-care in migrants with type 2 diabetes. Co-design centres around stakeholders working together to design services and/or care pathways.30 A core methodological approach in these methods involves the experiences of future users in the design process, focusing on both understanding and improving a person’s experiences of a service,30 see Figure 1.
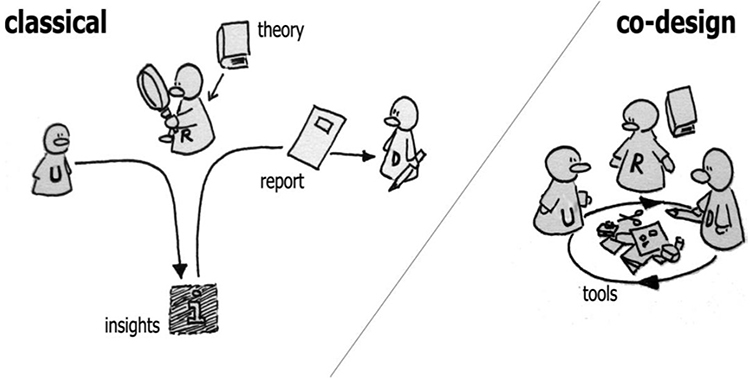 |
Figure 1 Classical roles of users, researchers, and designers in the design process (on the left) and how they merge in the Co-designing process (on the right) (Sanders & Stappers 2008). The users in this study were the participants in idea groups: health care providers, working in diabetes health care at a primary health care center and migrant patients, born in the Middle East, with type 2 diabetes. The designer and researcher came from the research team. |
Methodology
Procedure
The study was conducted between February 2021 to December 2022 with idea groups collecting data through brainstorming, prioritizing, and prototyping. Idea groups are a tool that can be used to brainstorm ideas for improvement and implementation in clinical practice. Prototyping can be used to test the functionality of new products and is a useful way to engage and stimulate creativity among the stakeholders participating in idea groups.29
Stakeholders and Participants
Stakeholders in this Co-design study included migrant patients born in the Middle East with type 2 diabetes, healthcare providers working with diabetes patients at a healthcare center and researchers. Participants in the idea groups included migrant patients and health care providers, see Table 1. The researchers consisted of three nurses and one healthcare professional, of which one had expertise in diabetes, two in chronic disease and one in cultural competence. Two of them were migrants themselves (not from the Middle East). Recruitment was performed by using convenience sampling. The sampling of patients was guided to achieve variation regarding gender, age, health literacy, years living in Sweden and duration of diabetes. The patients were identified by a diabetes nurse in electronic patient files at a primary healthcare center in south-east Sweden. Eligible patients received a written invitation and information about the study. After showing interest in participating in the study they were contacted by the first author (SP) who invited them to an idea group. All healthcare providers working in diabetes care at a primary health care center in a migrant-dense area were invited to participate.
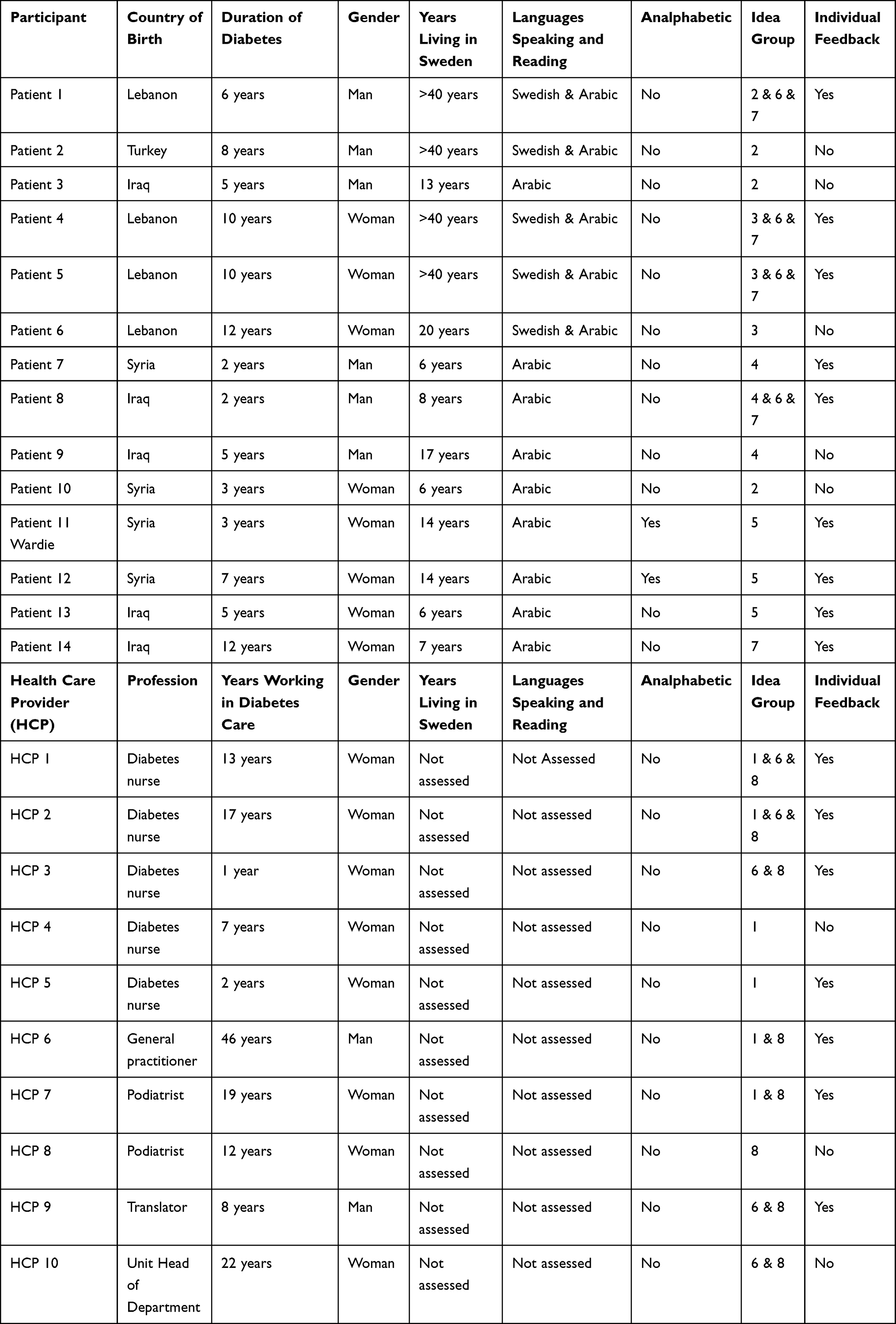 |
Table 1 Socio-Demographic Data for Participants in the Co-Design Process |
Data Collection
The Co-design process was based on six elements; engage, plan, explore, develop, decide and change29 see Table 2.
- Engage was achieved by establishing and maintaining relationships with stakeholders to understand and improve healthcare services.
- Plan involved the goal for the Co-design process, which was made before idea groups were formed. The goal, proposed by the research team: “To develop a culturally appropriate tool to support self-care in migrants with type 2 diabetes” was introduced to the participants and ideas on how to achieve and implement the goal in clinical practice were discussed during idea groups.
- Explore centred around participants’ experience of healthcare service, patient and healthcare responsibility and the patients’ needs in self-care education, which was performed during idea groups. In addition, ideas for improvement to support self-care in migrants with type 2 diabetes were discussed. Each idea group was based on prepared questions regarding participants’ experiences of migrant patients’ needs in diabetes healthcare and possible solutions to support self-care in migrants with type 2 diabetes.
- Develop focused on the summarized field notes from previous idea groups, which were discussed with the aim of improving the ideas and solutions. The develop phase continued with the research team discussing possible ideas for a culturally appropriate tool to support self-care in migrants with type 2 diabetes. These ideas were discussed and prioritized by participants in additional idea groups.
- Decide covered what tool should be developed and was undertaken by the research group by reviewing the list of improvements that were high value for both patients and healthcare providers, before they were presented to patients and healthcare providers for feedback.
 |
Table 2 The Co-Design Process Based on Six Elements; Engage, Plan, Explore, Develop, Decide and Change (Boyd H, 2010) |
Ethical Approval
This study was conducted according to the principles of the Declaration of Helsinki and in accordance with the Medical Research Involving Human Subjects Act in Sweden, approved by Regionala etikprövningsnämnden in Linköping (Dnr: 2020-00736.). Written, informed consent was obtained from all participants with clarification that they could terminate their participation at any time, without an explanation and without any effect on their care.
Results
In total, 14 patients, ten health care providers and four researchers participated in the Co-design process. A total of eight idea groups were carried out with the aim of collecting data through brainstorming, prioritizing and prototyping, see Figure 2.
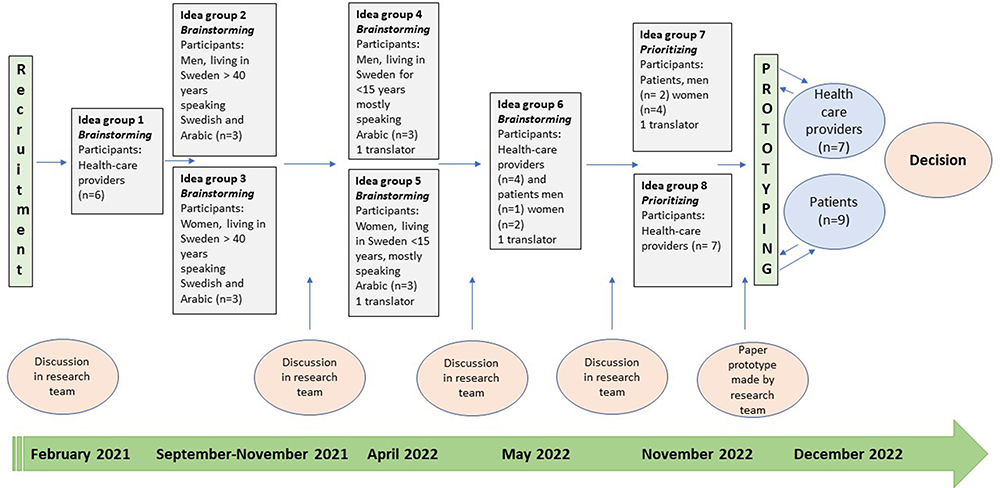 |
Figure 2 Timeline of the Co-design process including eight idea groups with migrant patients with type 2 diabetes and health care providers. The process contains idea groups with brainstorming, discussions in research team and prioritizing and prototyping. |
Plan and Explore
Brainstorming
The first idea group, idea group 1, consisted solely of healthcare providers, either a nurse, general practitioner or podiatrist working in diabetes care at a primary healthcare center. A following four idea groups - idea groups 2–5 - were held with patients, with a translator when needed. Groups 1–5 began with a short presentation by the research group and an introduction to self-care behaviour regarding type 2 diabetes. Implementing a user-centered design, scenarios, and personas facilitated the discussion.31 Two scenarios were used where the first represented a patient performing adequate self-care and the second scenario showed a patient with lack of self-care. The participants were asked to share their experiences about the responsibility of healthcare versus the patient themselves for various self-care aspects and what patients need help with. Finally, participants were encouraged to discuss their thoughts on a type of tool to support self-care in migrants with type 2 diabetes. Throughout all idea groups, two people from the research team were in attendance, one appointed as the facilitator while the other took field notes.
Needs
In idea group 1 (healthcare providers only), participants discussed the importance of patient knowledge about diabetes and self-care and that patients need support in their self-care as well as information about Swedish healthcare in general. They pointed out the importance of healthcare providers providing person-centered care, for example, advising on diet and cooking is linked to culture. Healthcare providers also discussed the importance of helping patients to accept their illness (to minimize denial and shame in the patient) and to involve patients’ relatives in self-care. Further, healthcare providers said it would be valuable for patients to receive written information and thus have the possibility to read the information several times.
In idea groups 2–5, (patients only), the patients emphasized their own responsibility for self-care and to take the information provided by healthcare providers. Some patients explain they were searching online for information about diabetes in their own languages. Patients discussed the lack of knowledge of suitable food. They all agreed they had to take responsibility for their own diet, but they experienced difficulty to eat “Swedish” food and wanted more information about what to eat as well as what not to eat. Additionally, they discussed their own responsibility for physical activity and the difficulties of being physically active. They all discussed how they were advised to walk 30 minutes every day but wanted other suggestions for physical activities. Patients stated their need for information about diabetes in their own language, both written and oral. Furthermore, patients felt that their family and friends do not understand self-care related to diabetes, especially with regards to diet, and would appreciate information about diabetes for friends and relatives, since they experienced that diabetes is not seen as a life-threatening disease in certain cultural groups. In addition, patients wanted to be able to monitor their blood sugar at home, while at the same time they needed help with interpretation of the blood values.
Possible Solutions
The healthcare providers (idea group 1) suggested the possibility for patients to receive information in their native language, provide tools and to involve relatives to support patients about illness and treatment to support self-care. Possible tools could be a brochure or technical aids like a mobile app or website, with information about diabetes in the patients’ own language.
The patients (idea group 2–5) thought that information via technical aids, for example a mobile app, could be a good option. In one of the idea groups, two women who were analphabetic attended and explained that they used their mobile phone to listen to information and watch recorded videos.
Develop
A joint idea group (idea group 6) was conducted where healthcare providers, patients and researchers attended. The focus for this idea group was to summarize what had been discussed during previous idea groups (idea group 1–5) and encourage participants to submit ideas to support self-care. Patients reported that they expected to get information from nurses but claimed that information is only a small part of learning self-care and patients must work very hard to maintain self-care. Some patients wanted group education, while others preferred more consultations with their nurse or doctor. Group education was not seen as ideal, as these are often scheduled during working hours. Furthermore, there were patients that could not read or write but agreed that a mobile app would work well; listening to and/or reading about diabetes was a good idea, but also a picture book was discussed.
Healthcare providers said there is a lot of good information about diabetes online, but there is no consensus about where to refer patients to read about diabetes and self-care in their own language. The healthcare providers agreed it would be convenient to gather information in one place, either online or in brochure form and a picture book would be a great addition. However, they also commented that healthcare probably needs to be more person-centered and offer several ways of providing information to patients.
When idea groups (1–6) were completed, the research team met and discussed how the tool needs to provide information and four perspectives were identified: Patient, family and friends, primary healthcare center and the community, see Figure 3. Both patients and healthcare providers agreed that the information source could be in different formats, either: text (paper or online) and audio-visual information via lectures or pictures. Possible ideas discussed in the team were: development of a brochure, a picture book, a mobile app, a website, information about diabetes in Arabic at 1177.se32 and oral presentations in public areas.
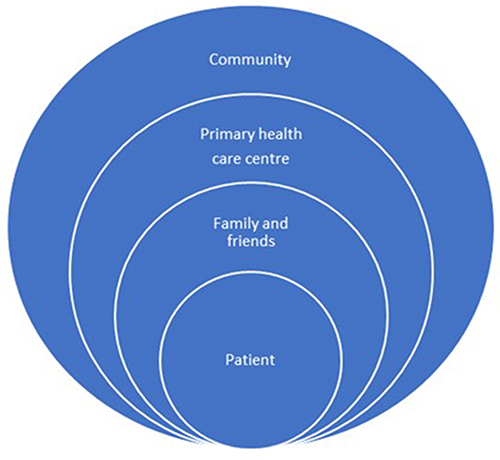 |
Figure 3 Four perspectives for providing information and to support self-care in migrants with type 2 diabetes. |
Decide
Prioritizing
During idea groups 7 and 8, patients and healthcare providers met separately with the researchers. According to the four identified perspectives - patient, family and friends, primary healthcare center and the community - the research team decided to prioritize the first three perspectives for the upcoming tool.
Possible ideas for a tool were summarized by the research team after reviewing the list for improvements that were of high value for both patients and health care providers and introduced to participants. Consequently, participants discussed and prioritized what ideas/tool they preferred. Patients liked the idea of a mobile app with recorded information about diabetes in Arabic and they also liked the idea of lectures about diabetes in Arabic, in a public area. The healthcare providers understood that a lot of good information already exists, but they would prefer to gather this information in one place, such as 1177.se - the Swedish national website that provides information about illnesses, care and health, which is well-known and trusted in Sweden.32 During further discussions within the research team, a decision was made that a digital platform will be developed that is possible to use in a mobile phone as well as a computer or other online devices.
Prototyping
A description of the digital platform, a paper prototype, was developed based on suggestions from the idea groups and relevant literature to identify culturally appropriate education, knowledge and guidelines for diabetes,21,24,26,27,33 see Figure 4. The paper prototype was sent for evaluation to the participants (patients and healthcare providers), who were asked to comment on the layout as well as the content. The participants found the prototype to be in accordance with their suggestions. The digital platform will be in Arabic and Swedish and contain links to existing evidence-based websites with information about diabetes, diabetes-related complications and self-care, knowledge about diabetes and suggestions for diet, physical activity, medication treatment, blood glucose-values and other self-care activities such as foot care. The links will contain both text and recorded videos to watch or listen to and will predominantly be in Arabic although some information will be in Swedish. In addition, the platform will contain links to the Swedish national website 1177.se, the Swedish Diabetes organisation and other relevant contacts supporting diabetes self-care behaviour.
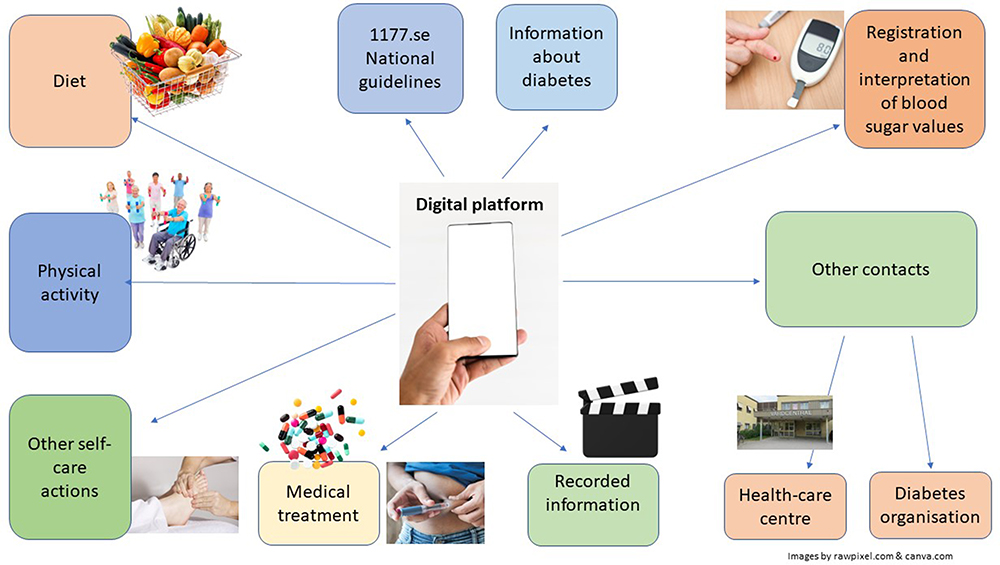 |
Figure 4 Paper prototype of a culturally appropriate tool, developed in the Co-design process. |
Discussion
In total, 28 stakeholders including migrant patients with type 2 diabetes, healthcare providers and researchers worked on a Co-design process29,30 and developed a digital platform tool that can be used on a mobile phone as well as a computer or other online devices.
The Co-design process led to several important insights/experiences related to the importance of diverse cultural backgrounds. When conducting a Co-design study with end-users as stakeholders, it is significant that the stakeholders have a diverse background in experiences, both as patients as well as those who deliver or implement the health service.34 In the initial phase of this study, only two idea groups to brainstorm were planned: one with healthcare providers and one with patients. However, the study concluded with five idea groups brainstorming to achieve the aim of including patients with diverse backgrounds regarding, gender, age, health literacy, occupation, years living in Sweden and duration of diabetes. In addition, two patients who had limited reading skills were included in idea groups. By using scenarios during the idea groups, a valuable basis for the exchange of ideas and thoughts in the groups was provided.31
As previously noted, the first element Engage, can be critical in a Co-design process.29 When recruitment for idea groups in this study was about to start, physical groups at the clinic were no longer allowed due to the COVID-19 pandemic. Online groups were proposed as an alternative, but the patients only wanted to join if the idea groups were held physically at the primary healthcare center, which is why this study was put on hold until physical idea groups were possible. In addition, double the number of patients were invited to each idea group since there was a drop-out of around 50% for each group.
When performing a Co-design study in vulnerable populations, there are three critical issues to be considered.35 The first issue is to have a clear epistemological starting point behind the decision to apply Co-design. In this study, the epistemological starting point was that migrants from the Middle East, have a high prevalence of type 2 diabetes,17 low self-care, low knowledge and poor glycaemic control21 and that there is a lack of culturally appropriate patient education about diabetes. Thus, a tool to support self-care in this vulnerable group as culturally appropriate diabetes education is needed.24,26
The second issue for researchers to consider is how the Co-design process will be planned, applied and adapted to engage the participants through the design process.35 In this study, the importance of each participant’s experiences was emphasized in this process, and they were engaged through continuous feedback about the process, which made it easier to plan, apply and adapt the Co-design process.
The third issue to consider is what kind of outcomes after the Co-design process can be predicted and created and how these can be used.35 This paper prototype of a tool, based on collected data from idea groups regarding needs and solutions, will be developed, tested and hopefully implemented in healthcare to support self-care in migrants born in the Middle East with type 2 diabetes. To simply collect data of experiences from patients is not enough - the result should be implemented in care.36 Thus, the last element of the process will be implemented as a Change in diabetes healthcare.
Initially, there seemed to be no clear consensus about the tool to be developed. Healthcare providers preferred to gather information about diabetes in Arabic in the form of a website they can use at a computer while working in diabetes care. Meanwhile, patients wanted a tool to use on their mobile phone. Healthcare providers also preferred the use of an existing, government-supported web site 1177.se.32 However, this web site is not currently language specific and was not viewed as appropriate by the patients.
Conclusion
By the process of this Co-design, a paper prototype of a culturally appropriate digital platform, to support self-care in migrant patients from the Middle East with type 2 diabetes, was developed. This digital platform will not only gather information in Arabic about diabetes by containing links to existing evidence-based websites with information about diabetes, diabetes-related complications and self-care. It will also guide patients to the Swedish national website 1177.se32, the Swedish Diabetes organization and other relevant contacts supporting diabetes self-care behaviour. One way to support migrants with their diabetes self-care, is by developing a culturally appropriate tool that addresses the needs of individuals with diabetes from cultural backgrounds.26 It will now be technically developed and tested for usability and feasibility among stakeholders (ie, migrant patients from the Middle East and healthcare providers working at a primary healthcare center). This platform will be accessible via computers as well as mobile phones.
Data Sharing Statement
Data are available from the corresponding author upon reasonable request.
Ethical Approval and Considerations
The study has been conducted according to the principles of the Declaration of Helsinki and in accordance with the Medical Research Involving Human Subjects Act in Sweden, approved by Regionala etikprövningsnämnden in Linköping. Ethical approval was received, Dnr: 2020-02042).
Acknowledgments
Thanks to the migrant patients and the health care providers at the studied Primary Health Care Center, who made it possible to carry out this study.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Disclosure
The authors declare that they have no conflicts of interest in this work.
References
1. Sun H, Saeedi P, Karuranga S, et al. IDF diabetes atlas: global, regional and country-level diabetes prevalence estimates for 2021 and projections for 2045. Diabetes Res Clin Pract. 2022;183:109119. doi:10.1016/j.diabres.2021.109119
2. Baena-Díez JM, Peñafiel J, Subirana I, et al. Risk of cause-specific death in individuals with diabetes: a competing risks analysis. Diabetes Care. 2016;39(11):1987–1995. doi:10.2337/dc16-0614
3. Rajpal A, Rahimi L, Ismail-Beigi F. Factors leading to high morbidity and mortality of COVID-19 in patients with type 2 diabetes. J Diabetes. 2020;12(12):895–908. doi:10.1111/1753-0407.13085
4. Huang I, Lim MA, Pranata R. Diabetes mellitus is associated with increased mortality and severity of disease in COVID-19 pneumonia - A systematic review, meta-analysis, and meta-regression. Diabetes Metab Syndr. 2020;14(4):395–403. doi:10.1016/j.dsx.2020.04.018
5. Mantovani A, Byrne CD, Zheng MH, Targher G. Diabetes as a risk factor for greater COVID-19 severity and in-hospital death: a meta-analysis of observational studies. Nutr Metab Cardiovasc Dis. 2020;30(8):1236–1248. doi:10.1016/j.numecd.2020.05.014
6. Kumar A, Arora A, Sharma P, et al. Is diabetes mellitus associated with mortality and severity of COVID-19? A meta-analysis. Diabetes Metab Syndr. 2020;14(4):535–545. doi:10.1016/j.dsx.2020.04.044
7. Testa R, Bonfigli AR, Genovese S, Ceriello A. Focus on migrants with type 2 diabetes mellitus in European Countries. Intern Emerg Med. 2016;11(3):319–326.
8. Riegel B, Jaarsma T, Strömberg A. A middle-range theory of self-care of chronic illness. Adv Nurs Sci. 2012;35(3):194–204. doi:10.1097/ANS.0b013e318261b1ba
9. Powers MA, Bardsley JK, Cypress M, et al. Diabetes self-management education and support in adults with type 2 diabetes: a consensus report of the American Diabetes Association, the Association of Diabetes Care & Education Specialists, the Academy of Nutrition and Dietetics, the American Academy of Family Physicians, the American Academy of PAs, the American Association of Nurse practitioners, and the American Pharmacists Association. Diabetes Care. 2020;43(7):1636–1649. doi:10.2337/dci20-0023
10. Beck J, Greenwood DA, Blanton L, et al. 2017 national standards for diabetes self-management education and support. Diabetes Care. 2017;40(10):1409–1419. doi:10.2337/dci17-0025
11. International Organization for Migration. World Migration Report 2022: Chapter 2 Migration and Migrants: A Global Overview. Available from: https://publications.iom.int/books/world-migration-report-2022-chapter-2.
12. Goff LM. Ethnicity and Type 2 diabetes in the UK. Diabet Med. 2019;36(8):927–938. doi:10.1111/dme.13895
13. Meeks KA, Freitas-Da-Silva D, Adeyemo A, et al. Disparities in type 2 diabetes prevalence among ethnic minority groups resident in Europe: a systematic review and meta-analysis. Intern Emerg Med. 2016;11(3):327–340. doi:10.1007/s11739-015-1302-9
14. Montesi L, Caletti MT, Marchesini G. Diabetes in migrants and ethnic minorities in a changing World. World J Diabetes. 2016;7(3):34–44. doi:10.4239/wjd.v7.i3.34
15. IOM IOfM. Who is a migrant?; 2020. Available from: http://www.iom.int/who-is-a-migrant.
16. Statistics Sweden. Från Finland till Afghanistan–invandring och utvandring för födda i olika länder sedan 1970 [From Finland to Afghanistan – immigration and emigration since 1970 for persons born in different countries]. Örebro: SCB; 2016. Swedish. Available from: https://www.scb.se/en/finding-statistics/statistics-by-subject-area/population/population-projections/demographic-analysis-demog/pong/publications/from-finland-to-afghanistan--immigration-and-emigration-since-1970-for-persons-born-in-different-countries/.
17. Andersen GS, Kamper-Jørgensen Z, Carstensen B, Norredam M, Bygbjerg IC, Jørgensen ME. Diabetes among migrants in Denmark: incidence, mortality, and prevalence based on a longitudinal register study of the entire Danish population. Diabetes Res Clin Pract. 2016;122:9–16. doi:10.1016/j.diabres.2016.09.020
18. Elinder LS, Hakimi S, Lager A, Patterson E. Global region of birth is an independent risk factor for type 2 diabetes in Stockholm, Sweden. Eur J Public Health. 2017;27(3):447–453. doi:10.1093/eurpub/ckw207
19. Pettersson S, Jaarsma T, Hedgärd K, Klompstra L. Self-care in migrants with type 2 diabetes, during the COVID-19 pandemic. J Nurs Scholarsh. 2022;55(1):167–177. doi:10.1111/jnu.12842
20. Bennet L, Groop L, Lindblad U, Agardh CD, Franks PW. Ethnicity is an independent risk indicator when estimating diabetes risk with FINDRISC scores: a cross sectional study comparing immigrants from the Middle East and native Swedes. Prim Care Diabetes. 2014;8(3):231–238. doi:10.1016/j.pcd.2014.01.002
21. Pettersson S, Hadziabdic E, Marklund H, Hjelm K. Lower knowledge about diabetes among foreign‐born compared to Swedish‐born persons with diabetes—A descriptive study. Nursing Open. 2019;6(2):367–376. doi:10.1002/nop2.217
22. Jaarsma T, Cameron J, Riegel B, Stromberg A. Factors Related to Self-Care in Heart Failure Patients According to the Middle-Range Theory of Self-Care of Chronic Illness: a Literature Update. Curr Heart Fail Rep. 2017;14(2):71–77. doi:10.1007/s11897-017-0324-1
23. Hammell KRW. Occupation, bien-être et culture: la théorie et l’humilité culturelle [Occupation, well-being, and culture: Theory and cultural humility]. Can J Occup Ther. 2013;80(4):224–234. French.
24. Hadziabdic E, Pettersson S, Marklund H, Hjelm K. Development of a group-based diabetes education model for migrants with type 2 diabetes, living in Sweden. Prim Health Care Res Dev. 2020;21:e50. doi:10.1017/s1463423620000493
25. Wilson C, Alam R, Latif S, Knighting K, Williamson S, Beaver K. Patient access to healthcare services and optimisation of self-management for ethnic minority populations living with diabetes: a systematic review. Health Soc Care Community. 2012;20(1):1–19. doi:10.1111/j.1365-2524.2011.01017.x
26. Creamer J, Attridge M, Ramsden M, Cannings-John R, Hawthorne K. Culturally appropriate health education for Type 2 diabetes in ethnic minority groups: an updated Cochrane Review of randomized controlled trials. Diabet Med. 2016;33(2):169–183. doi:10.1111/dme.12865
27. Pettersson S, Holstein J, Jirwe M, Jaarsma T, Klompstra L. Cultural competence in healthcare professionals, specialised in diabetes, working in primary healthcare-A descriptive study. Health Soc Care Community. 2022;30(3):e717–e726. doi:10.1111/hsc.13442
28. Alzubaidi H, Sulieman H, Mc Namara K, Samorinha C, Browning C. The relationship between diabetes distress, medication taking, glycaemic control and self-management. Int J Clin Pharm. 2022;44(1):127–137. doi:10.1007/s11096-021-01322-2
29. Boyd H, McKernon S, Old A. Health Service Co-Design: Working with Patients to Improve Healthcare Services. Auckland: Waitemata District Health Board; 2010.
30. Sanders EBN, Stappers PJ. Co-creation and the new landscapes of design. CoDesign. 2008;4(1):5–18. doi:10.1080/15710880701875068
31. Carroll JM. Five reasons for scenario-based design. Interact Comput. 2000;13(1):43–60. doi:10.1016/s0953-5438(00)00023-0
32. 1177.se. This is 1177. Available from: https://www.1177.se/en/Ostergotland/other-languages/other-languages/soka-vard/det-har-ar-1177/.
33. Welfare SNBoHa. Swedish Guidelines for Diabetes Care [In Swedish: nationella riktlinjer för diabetesvården 2018: stöd för styrning och ledning]. Swedish National Board of Health and Welfare; 2018. Available from: https://www.socialstyrelsen.se/globalassets/sharepoint-dokument/artikelkatalog/nationella-riktlinjer/2018-10-25.pdf.
34. Mulvale G, Moll S, Miatello A, et al. Codesigning health and other public services with vulnerable and disadvantaged populations: insights from an international collaboration. Health Expect. 2019;22(3):284–297. doi:10.1111/hex.12864
35. Moll S, Wyndham-West M, Mulvale G, et al. Are you really doing ‘codesign’? Critical reflections when working with vulnerable populations. BMJ Open. 2020;10(11):e038339. doi:10.1136/bmjopen-2020-038339
36. Coulter A, Entwistle VA, Eccles A, Ryan S, Shepperd S, Perera R. Personalised care planning for adults with chronic or long-term health conditions. Cochrane Database Syst Rev. 2015;2015(3):Cd010523. doi:10.1002/14651858.CD010523.pub2
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Maintenance of Self-Care Activities During COVID-19 Lockdown in Patients with Type 2 Diabetes That Received a Comprehensive Care Program Training
García Ulloa AC, Tron-Gómez MS, Díaz-Pineda M, Hernández-Juárez D, Landa-Anell MV, Melgarejo-Hernández MA, Hernández-Jiménez S
Diabetes, Metabolic Syndrome and Obesity 2022, 15:2857-2865
Published Date: 19 September 2022