Back to Journals » Clinical Ophthalmology » Volume 17
Determining the Superiority of Vitrectomy vs Aflibercept for Treating Dense Diabetic Vitreous Hemorrhage: A Systematic Review and Meta-Analysis of Randomized Clinical Trials
Authors Quiroz-Reyes MA ![]() , Quiroz-Gonzalez EA, Quiroz-Gonzalez MA
, Quiroz-Gonzalez EA, Quiroz-Gonzalez MA ![]() , Lima-Gómez V
, Lima-Gómez V ![]()
Received 25 May 2023
Accepted for publication 4 August 2023
Published 15 August 2023 Volume 2023:17 Pages 2359—2370
DOI https://doi.org/10.2147/OPTH.S419478
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Scott Fraser
Miguel A Quiroz-Reyes,1 Erick Andrés Quiroz-Gonzalez,1,2 Miguel A Quiroz-Gonzalez,1 Virgilio Lima-Gómez3
1Retina Department, Oftalmologia Integral ABC, Mexico City, Mexico; 2Ophthalmology Department, Institute of Ophthalmology, Mexico City, Mexico; 3Retina Department, Juarez Hospital, Mexico City, Mexico
Correspondence: Miguel A Quiroz-Reyes, Retina Department, Oftalmologia Integral ABC, Paseo de las Palmas 735 suite 303, Lomas de Chapultepec, Mexico City, 11000, Mexico, Tel +525 5217 2732, Fax +525 55 1664 7190 ; +525 55 1664 7180, Email [email protected]
Abstract: This review aimed to systematically compare the efficacy and safety of intravitreal aflibercept (IVA) and vitrectomy for treating severe vitreous hemorrhage (VH) secondary to proliferative diabetic retinopathy (PDR). The review was conducted in accordance with PRISMA guidelines. A search strategy, including the MEDLINE, Embase, Cochrane Central Register of Controlled Trials, and US National Library of Medicine databases, was developed to identify randomized controlled trials (RCTs) that compared vitrectomy and IVA for managing VH due to PDR (participant age ≥ 18 years). The primary outcome measure was the difference in the mean visual acuity between the two treatment groups at 1, 6, and 24 months. Outcome measures included clearance of VH (in weeks), the incidence of recurrent VH, and the rate of complications. The studies were evaluated using the Cochrane Bias (ROB) tool. We identified 774 articles; six articles met the inclusion criteria, and two were ultimately included (n = 239 eyes). With or without PRP, IVA injections and vitrectomy were performed in 117 and 122 eyes, respectively. The mean BCVA at one month was significantly better in the vitrectomy group (MD=0.22, CI:0.10– 0.34, p=0.0003), but no difference was found at six months (MD=0.04, CI: − 0.04– 0.12, p=0.356). The incidence of recurrent VH was significantly higher in the IVA group (OR=5.05, CI:2.71– 9.42, p< 0.0001). The probability of recurrent VH was five times greater in the IVA group than that in the vitrectomy group. There were no significant differences in the overall proportions of intra- or postoperative complications (OR=0.64, CI: 0.09– 4.85, p=0.669). None of the studies had a low ROB in any of the seven domains. We conclude that IVA can be considered a viable treatment modality for diabetic VH in patients with a good follow-up. Vitrectomy initially provides better visual effect, faster VH recovery, and lower VH recurrence than IVA injections.
Keywords: aflibercept, anti-VEGF, intravitreal injection, proliferative diabetic retinopathy, vitrectomy
Introduction
Diabetic retinopathy (DR) is the leading cause of permanent visual impairment worldwide.1 Secondary consequences of DR in the eye include multiple vision-threatening complications such as diabetic macular edema (DME) and vitreous hemorrhage (VH) secondary to proliferative diabetic retinopathy (PDR).2 PDR is traditionally treated using panretinal photocoagulation (PRP).3 However, PRP can cause permanent vision loss in the peripheral visual field, reduce contrast sensitivity, and delay adaptation to darkness.2,4,5 Surgical treatment options for PDR include pars plana vitrectomy (PPV), which has been practiced since the 1970s. Although there have been improvements in instrumentation and surgical techniques, the frequency of performing vitrectomy has decreased over the years and is usually reserved for the most difficult cases.6 Newer treatment methods, such as antiangiogenic agents, are increasing in popularity as they have been found to be effective in stabilizing vision in PDR.7 Bevacizumab, ranibizumab, and aflibercept are the most commonly used intravitreal anti-vascular endothelial growth factors (anti-VEGF).7
The management of VH in PDR is difficult because of its recurrence and poor visual outcomes. Although surgical, laser and pharmacological procedures are currently used in clinical practice, no single treatment has been proven to be “1 and done”. Therefore, there is a need to identify new treatment methods that are effective in the long term. Several treatment modalities for diabetic VH have been investigated, including intravitreal aflibercept (IVA) injections. Aflibercept is a humanized recombinant fusion protein that binds to VEGF to exert inhibitory effects on VEGF receptors, thereby preventing endothelial proliferation, vascular permeability, and neovascularization. It binds to VEGF with a greater affinity than bevacizumab or ranibizumab8,9 and has been shown to be a promising anti-VEGF agent. In addition, IVA has been shown to be no worse than PRP in the treatment of PDR.10 Koshchynets et al reported a case demonstrating the efficacy of intravitreal aflibercept in combination with PRP for the regression of neovascularization and prevention of recurrent vitreous hemorrhage in a patient with severe type 1 diabetes having total vitreous hemorrhage.11 In a prospective study, Umanets et al, reported that intravitreal aflibercept resulted in the obliteration of neovascularization of epiretinal membranes (ERMs) and avoided intraoperative and postoperative bleeding during vitrectomy.12 The procedure resulted in a significant improvement in visual outcomes across all cases. Based on case studies and nonrandomized trials, aflibercept has shown efficacy and safety in the management of vitreous hemorrhage in diabetic eye diseases.
Some studies have compared the efficacy of IVA with that of vitrectomy in diabetic VH; however, most of the information presented in the literature is limited to uncontrolled clinical studies or retrospective case series. The results of such studies are inconclusive because of their high risk of bias. Therefore, it is necessary to assess the safety and efficacy of IVA, which can be achieved through a comprehensive meta-analysis. In this review, we sought to systematically establish the efficacy and safety profiles of IVA and vitrectomy in cases of VH secondary to DR to inform future studies with possible clinical benefits. To this end, this systematic review aimed to identify, appraise, and synthesize evidence on the safety and efficacy of two different treatment modalities for VH secondary to DR.
Methods
The present systematic review was conducted in accordance with the Preferred Reporting Items for Systematic Review and Meta-analyses (PRISMA) guidelines.13 A search strategy [see Appendix - I in the Supplementary File] was developed to identify all articles that reported vitrectomy and IVA as treatments for VH secondary to PDR.
Study Eligibility Criteria
Studies were selected for inclusion based on the prespecified Population, Intervention, Comparator, Outcomes (PICO) criteria (Table 1). Randomized controlled trials (RCTs) that reported the use of either vitrectomy or IVA to treat VH secondary to PDR were eligible for inclusion. Conference abstracts, animal studies, non-RCTs, and case series were excluded.
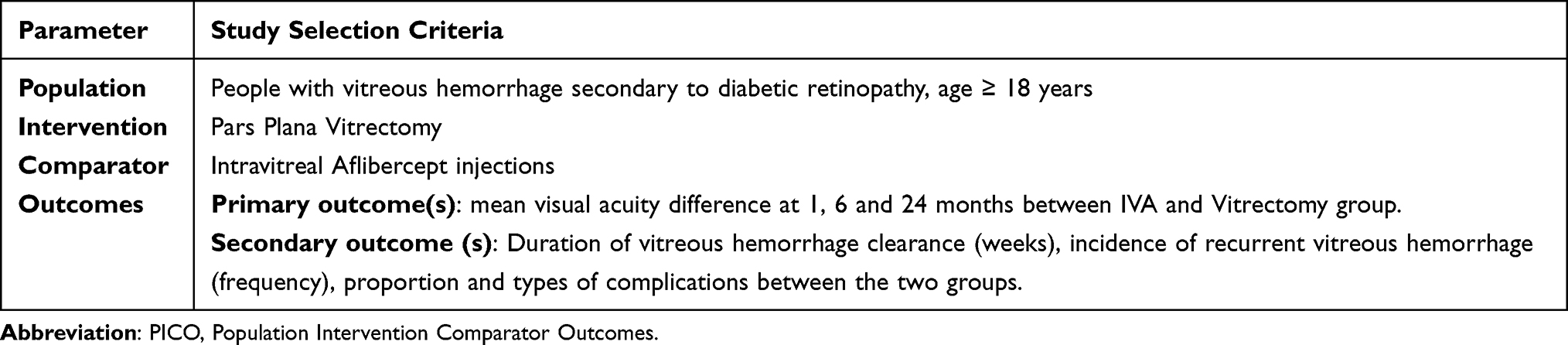 |
Table 1 PICO Criteria for the Inclusion of Studies |
Search Strategy
The following electronic bibliographic databases were searched: Medline, Embase, Cochrane Central Register of Controlled Trials, and the US National Library of Medicine. English keywords were used to identify studies in these databases published before November 25, 2022. The bibliographies of the included articles were also searched to identify relevant studies.
Data Extraction and Management
Two reviewers (MAQR and VLG) independently screened the titles and abstracts identified in the bibliographic search. Full-text reviews and data extraction were performed independently, and discrepancies were resolved by comparison with the inclusion criteria. Data were extracted using a standardized proforma and included study design, inclusion criteria, participant demographics (age, sex, and underlying conditions), intervention type, and outcome data. Additionally, the sample size, follow-up duration, time to VH resolution, incidence of recurrent VH, and reported complications were also extracted. The mean logMAR visual acuity at the baseline and follow-up visits was also determined.
Risk of Bias Assessment
The Cochrane Collaboration tool was used to assess the risk of bias (ROB) [see Appendix II for Supporting Information in the Supplementary File].14 This tool incorporates several domains that assess sampling methods, randomization, reporting bias, and detection bias. Two reviewers (MAQR and VLG) independently assessed the ROB in each RCT across the seven domains. Disagreements were resolved through consensus.
Measures of Treatment Effect
The primary outcome measure was the mean difference in the best-corrected visual acuity (BCVA) in logMAR units at 1, 6, and 24 months. The secondary outcome measures included the duration of VH clearance after treatment (weeks), recurrence of VH (frequency), and complications. Complications were defined as worsening conditions requiring adjunctive treatment or adverse effects after treatment. Data were reported across studies, with widely varying time points and outcome assessors. Therefore, the other outcome measures reported in the included studies were extracted and interpreted. The meta-analysis was performed using the R statistical package.
Results
The literature search yielded 774 articles, of which 6 were eligible for inclusion. A full-text review identified four articles to be excluded (one uncontrolled study,15 one study in which IVA was compared to sham treatment,16 and two studies in which IVA was compared with PRP)10,17, and ultimately, only two articles were included in the qualitative and quantitative synthesis. The PRISMA flowchart for the selection of studies is shown in Figure 1. The first study was conducted across 39 Diabetic Retinopathy Clinical Research (DRCR) Retina Network sites in the United States and Canada.18 The study recruited 205 participants between November 2016 and December 2017 and conducted final follow-up in January 2020. Another study was conducted at two eye centers, one each in Kuwait and Egypt.19 The study recruited 34 participants between March 2018 and July 2019.
 |
Figure 1 PRISMA flow chart outlining the article selection process. |
This meta-analysis included 239 eyes (one eye per participant). Among these, 117 eyes received IVA injections with or without panretinal photocoagulation (PRP) and 122 eyes received vitrectomy with or without PRP. The participants were randomly allocated to receive either IVA with or without PRP, or vitrectomy with or without PRP. Participants in the IVA group received three19 or four monthly doses of IVA injections18 (EYLEA; Regeneron Pharmaceutical Inc., Tarrytown, NY, USA) at a dose of 2 mg/0.05 mL. Seventeen participants in the IVA group received PRP in addition to IVA injections. PPV with or without PRP was performed in participants in the other group. The participants were followed up for two years in one study, and for nine months in another study. The characteristics of the included studies are summarized in Table 2.
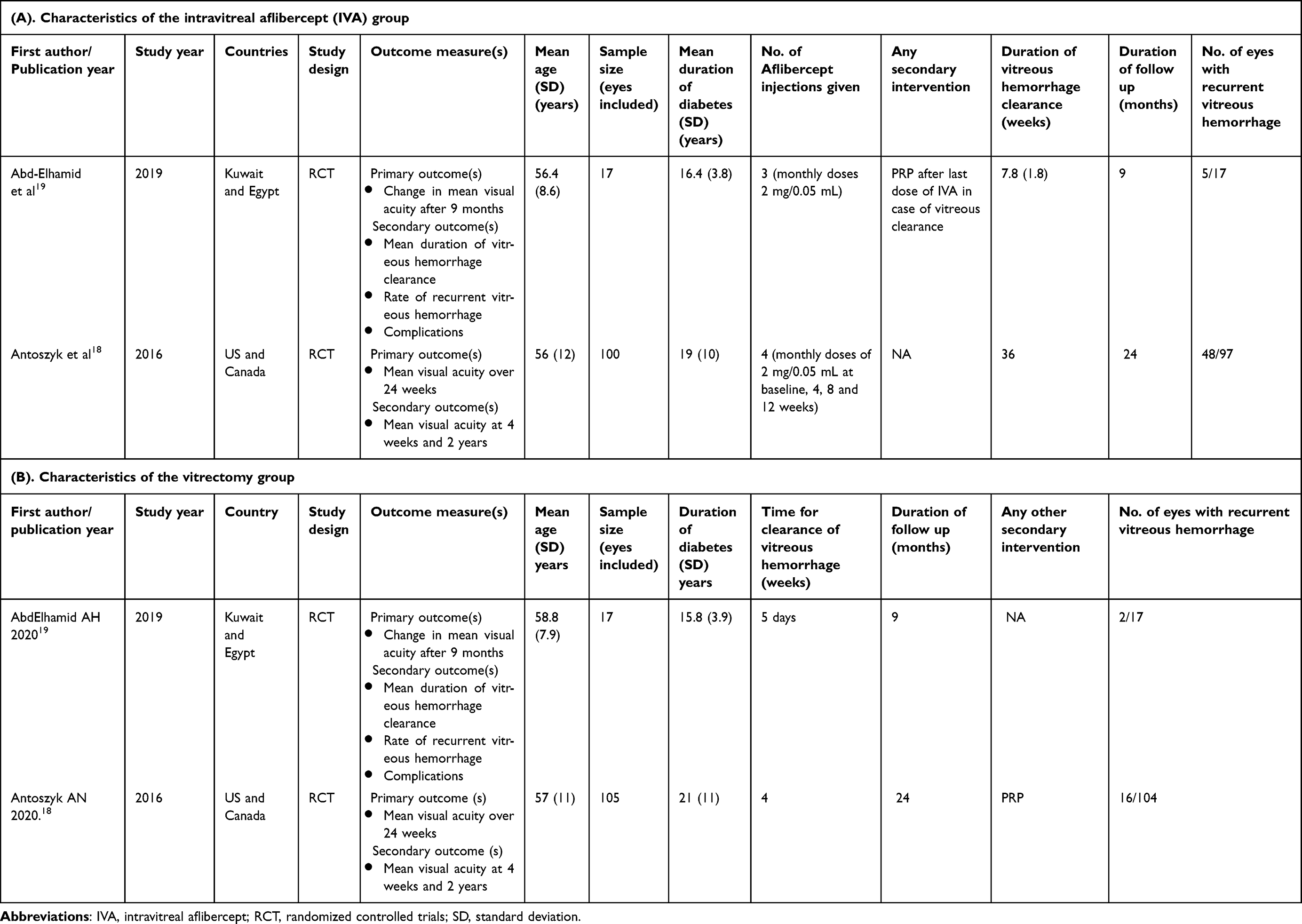 |
Table 2 Characteristics of the Included Studies |
Meta-Analysis of Best-Corrected Visual Acuity (BCVA) at 1 and 6 Months
The mean BCVA data were available at baseline and at 1, 3, 6, and 9 months from one study,19 and at baseline, 1 month (4 weeks), 6 months (24 weeks), and 2 years from the other study.18 The mean BCVA in the IVA group and the vitrectomy group in the two included studies at the 1-month and 6-month follow-ups were pooled to assess the difference between the two groups. The mean BCVA values at different follow-up times in the two included studies are shown in Table 3. The mean BCVA in the vitrectomy group was significantly better at one month than at six months (MD=0.22, CI:0.10–0.34, p=0.0003). There was no significant difference in BCVA between the two groups (MD=0.04, CI: −0.04–0.12, p=0.356). There was no heterogeneity between the groups at either 1 month (I2=0.00%, Q (df=1) =0.491, p=0.483) or 6 months (I2=0.00%, Q (df=1) =0.477, p=0.490). Forest plots for the mean difference in BCVA at the 1-month and 6-month follow-ups are shown in Figures 2 and 3, respectively. Similarly, no significant difference in mean visual acuity between the two groups was observed at 24 months in the Antoszyk et al18 study.
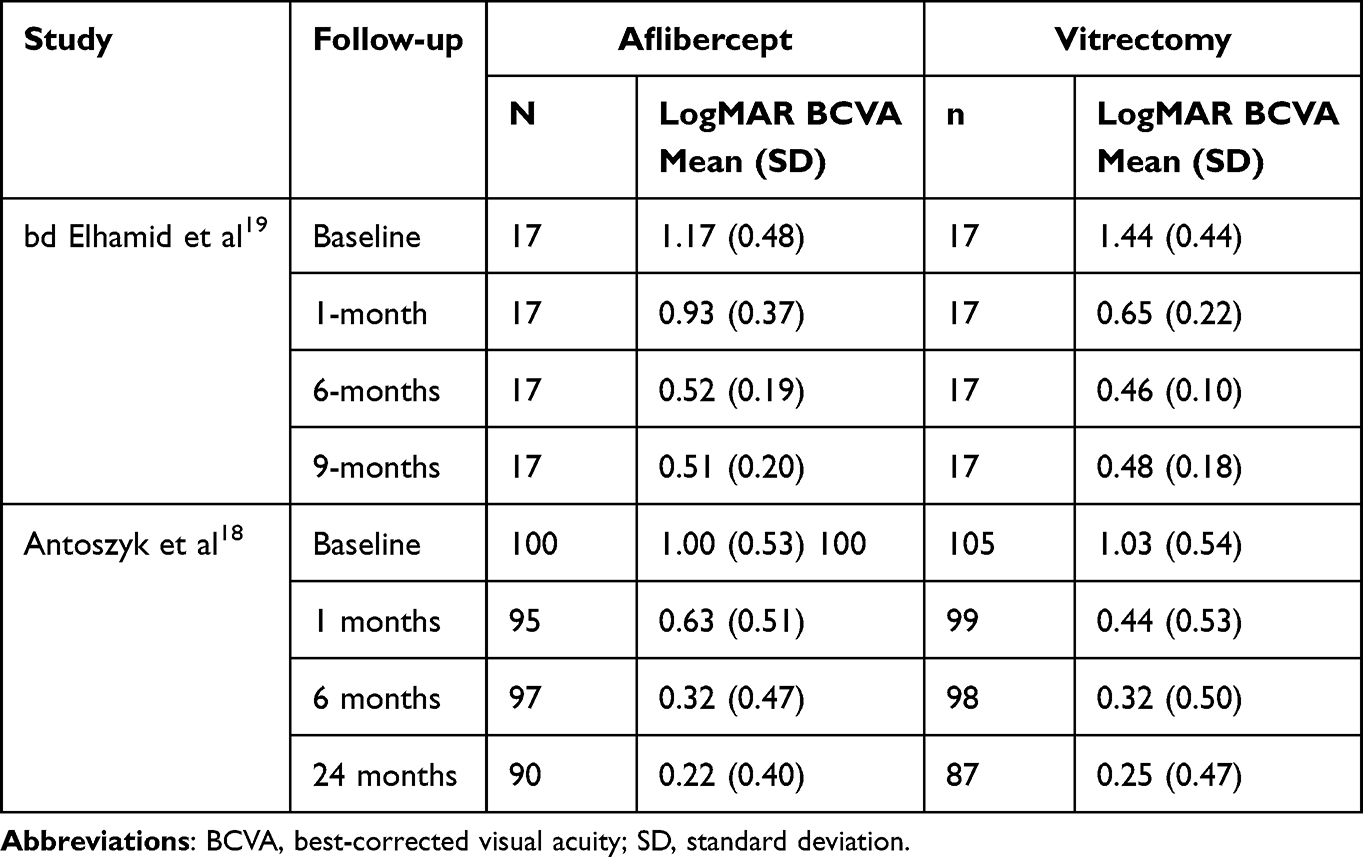 |
Table 3 Mean BCVA in the Aflibercept and Vitrectomy Groups at Different Follow-Up Visits |
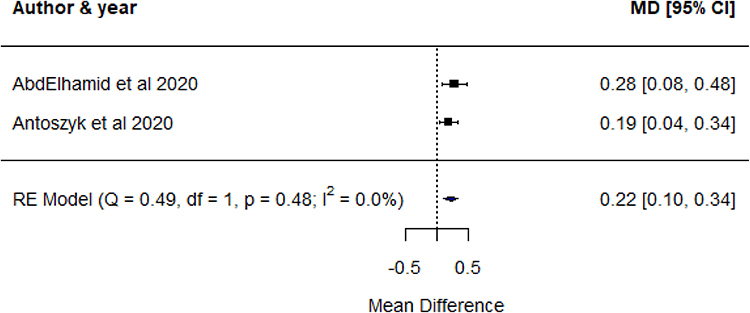 |
Figure 2 Mean difference in BCVA at 1-month follow-up visits. |
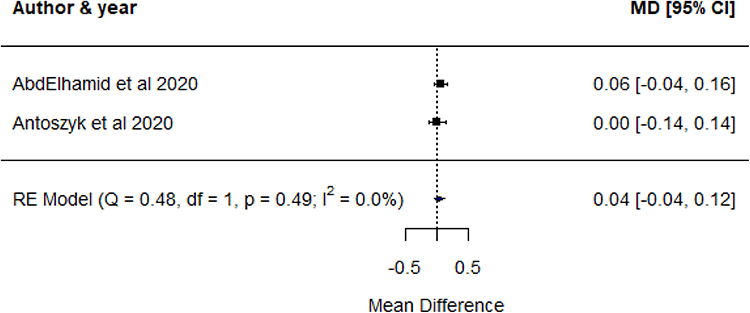 |
Figure 3 Mean difference BCVA at 6-month follow-up visits. |
Duration for Vitreous Hemorrhage Clearance
Abd Elhamid et al19 reported a mean duration of 7.8 weeks (SD ±1.8) in the aflibercept group and five days in the vitrectomy group. Similarly, in a secondary analysis of Glassman et al20 study reported the median time for the clearance of VH as 36 weeks (IQR, 24–52 weeks) in the aflibercept group and 4 weeks (IQR, 4–4 weeks) in the vitrectomy group. Both studies reported a significantly faster clearance of VH in the vitrectomy group than in the aflibercept group.
Incidence of Recurrent Vitreous Hemorrhage
The incidence of recurrent VH was reported in both included studies. The incidence of recurrent VH was significantly higher in the aflibercept group (odds ratio [OR]=5.05, CI:2.71–9.42, p<0.0001). The odds of recurrent VH were five times higher in the aflibercept group than in the vitrectomy group. There was no heterogeneity among the studies when assessing the incidence of recurrent VH (I2=0.00%, Q (df=1)=0.31, p=0.579). The pooled incidence of recurrent vitreous hemorrhage is shown in Figure 4.
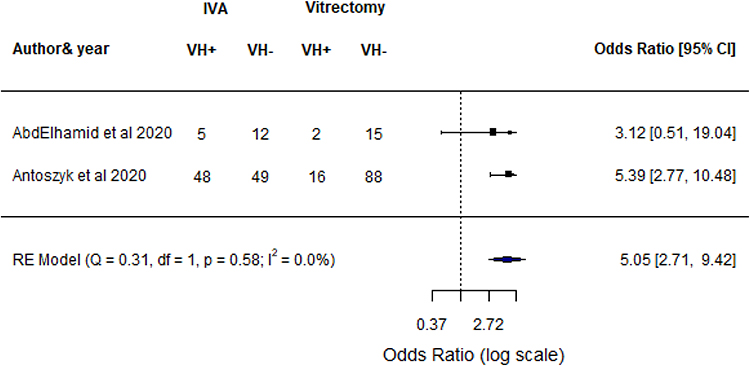 |
Figure 4 Pooled incidence of recurrent vitreous hemorrhage. |
Complications
Intraoperative or postoperative complications occurred in both the included studies. A summary of the ocular complications in the two studies is presented in Table 4. Cataracts in the phakic eyes were the most commonly reported complications in both groups. Other complications include new or worsened retinal detachment, tears, ERMs, and endophthalmitis. The overall proportion of intra- or postoperative complications was not significantly different between the groups (OR =0.64, CI:0.09–4.85, p=0.669). However, substantial heterogeneity was observed when estimating the pooled proportions of overall ocular complications between groups (I2=79.50%, Q (df=1) = 4.88, p =0.027). The odds ratios and proportions of ocular complications are shown in Figure 5.
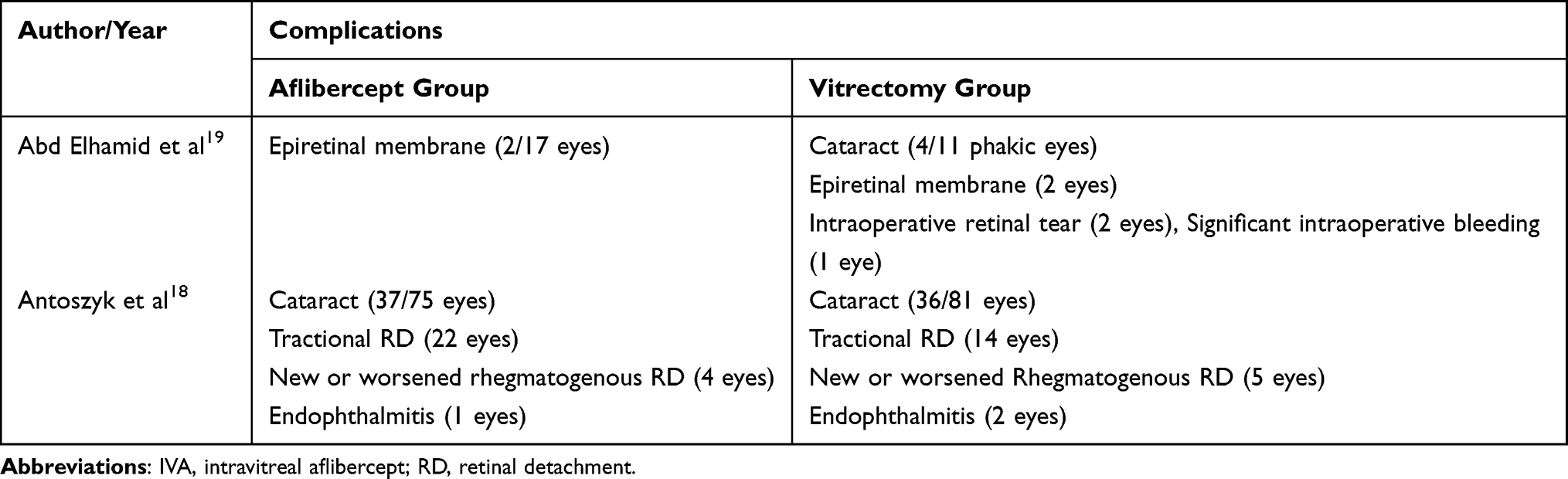 |
Table 4 Ocular Complications in the IVA and Vitrectomy Groups |
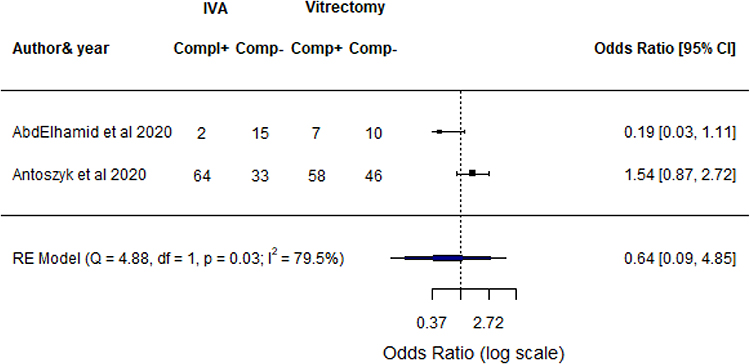 |
Figure 5 Proportions of ocular complications. |
Study Quality
Figure 6 summarizes the ROB assessments of the included studies. None of the studies was judged to have a low ROB in any of the seven domains. Antozsky et al18 were judged to have a low risk of bias across most domains (5/7 domains), while Abd Elhamid et al19 were judged to have a low risk of bias across only two domains.
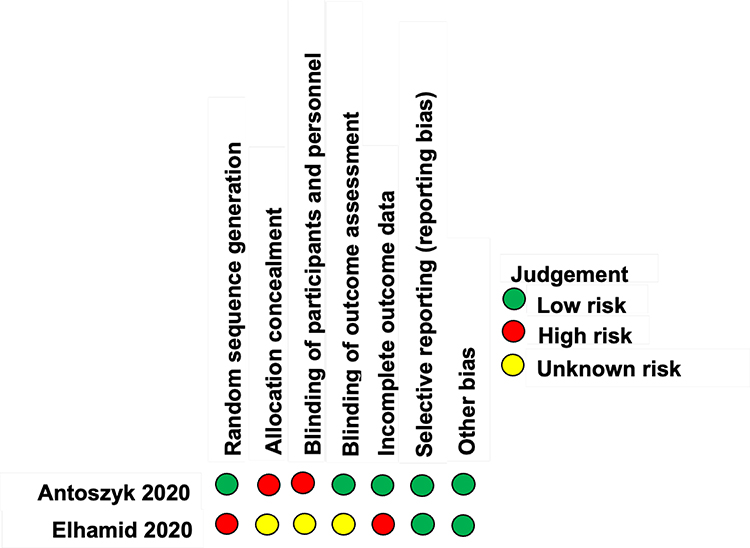 |
Figure 6 Risk of bias assessment of the included studies. |
Discussion
Vitrectomy and PRP have been widely used for the treatment of diabetic VH since the 1970s.6 However, the role of anti-VEGF agents, including IVA, has increased over the last few years.21 IVA is less invasive than vitrectomy. This makes IVA a good choice for the treatment of diabetic retinopathy.10 However, the potential benefits and safety of IVA in the treatment of VH are not clearly understood. Therefore, the aim of the present systematic review and meta-analysis was to identify a better functional approach between the two modalities of treatment for diabetic VH, that is, vitrectomy versus IVA.
The primary outcome measure of this review was the mean difference in visual acuity at 1, 6, and 24 months postintervention. Although the visual acuity outcome was better in the vitrectomy group in the early stages, there was no difference in the long-term recovery between the two interventions. The secondary outcome measures of the review were the duration of VH clearance and occurrence of recurrent VH postintervention. VH clearance was faster in the vitrectomy group than that in the IVA group. Similarly, the odds of recurrent VH were higher in the IVA group than those in the vitrectomy group. Historical observations have highlighted the association between intravitreal treatment and visual outcomes. Retinal thickness deviation, which indicates the deviation of central subfoveal thickness from normative values, has previously been shown to be strongly associated with visual outcomes in patients with diabetic macular edema undergoing intravitreal treatment.22
Previous studies have confirmed the beneficial effects of IVA in treating diabetic retinal disease, particularly DME. Chen et al23 reported that three monthly intravitreal aflibercept injections yielded benefits in nearly two-thirds of cases of DME resistant to bevacizumab or ranibizumab over a short-term follow-up. IVA has been observed to be safe and effective in submacular hemorrhage secondary to neovascular AMD,24 in resolving rubeosis iridis secondary to proliferative diabetic retinopathy with VH,25 and in macular edema secondary to central retinal vein occlusion.26 IVA has been tested in multiple retinal diseases; however, specific literature regarding its safety and efficacy in VH due to diabetic retinopathy is lacking. Therefore, in the current literature, only two studies with similar study protocols could be combined to compare the treatment outcomes after IVA and vitrectomy.
However, the safety of the two interventions was inconclusive because of the high heterogeneity in estimating the results.27 The proportions of intra- or postoperative ocular complications were not significantly different between the two groups. Cataracts in the phakic eyes were the most common complications that occurred in both the vitrectomy and IVA groups. The development of cataracts after vitrectomy is a well-known complication.28 Other complications noted in both groups were tractional retinal detachment (TRD), new or worsened rhegmatogenous RD, ERMs and endophthalmitis. Further RCTs on the safety of these two interventions are warranted to clearly understand the differences in complications between the two groups.
The results of this study have several potential clinical implications. Given the insignificant differences in complication rates between the two groups and the relatively lower invasiveness of IVA, it can be considered a good choice in terms of long-term visual outcomes. However, the frequent administration required to overcome recurrent VH, which has a higher incidence after IVA, may not make IVA an ideal choice for patients with poor follow-up. Since the incidence of recurrent VH and the duration of VH clearance were significantly better in the vitrectomy group, it should be considered superior to IVA in terms of these treatment outcomes. Therefore, in patients requiring faster recovery from the hemorrhage, particularly in one-eyed patients with VH in the better eye, vitrectomy can be considered a better treatment choice.
Risk of Bias Assessment
The two studies that examined the safety and efficacy of IVA for VH due to diabetic retinopathy had a high risk of performance bias. This is because surgical interventional studies on cases of profound visual loss secondary to diabetic retinopathy are likely to have inherent variability because of the seriousness of the disease; patient masking and clinician masking are usually difficult, as shared decision making is needed to determine the intervention applied.29 Additionally, patients are likely to decline newer treatment methods when given choice over an existing successful treatment method.30 This review included only RCTs for a stronger assessment, although non-RCTs and case series also provide information on unintended or long-term effects of an intervention.29,31
The strength of our meta-analysis was that we included only RCTs that offered the highest level of evidence. All noncontrolled trials were excluded. However, a major limitation of our review was the insufficient evidence available for its synthesis. Further RCTs are required to confirm the findings of the present study.
Conclusions
The present meta-analysis showed that intravitreal aflibercept can be a viable treatment modality for diabetic VH, given its similar long-term visual outcomes to vitrectomy in patients who maintain long-term follow-up visits. Nevertheless, vitrectomy provides a better initial visual outcome, faster recovery of VH, and lower recurrence of VH than IVA injections, and therefore shows superior surgical outcomes. However, there was no significant difference in the proportion of complications between the two modalities of treatments. The limited number of RCTs comparing these two interventions suggests the need for additional high-quality studies to confirm these findings.
Abbreviations
AMD, age-related macular degeneration; BCVA, best-corrected visual acuity; CI, confidence interval; DME, diabetic macular edema; DR, diabetic retinopathy; DRCR, Diabetic Retinopathy Clinical Research; IVA, intravitreal aflibercept; LogMAR, logarithm of the minimum angle of resolution; MD, median deviation; PRP, panretinal photocoagulation; PDR, proliferative diabetic retinopathy; PICO, Population, Intervention, Comparator, Outcomes; OR, odds ratio; PPV, pars plana vitrectomy; PRISMA: Preferred Reporting Items for Systematic Reviews and Meta-Analysis; RCTs, randomized controlled trials; RD, retinal detachment; ROB, Risk of Bias; VEGF, vascular endothelial growth factor; TRD, tractional retinal detachment; VH; vitreous hemorrhage.
Summary Statement
The management of vitreous hemorrhage in proliferative diabetic retinopathy is difficult because of its recurrence and poor visual outcomes. This systematic review compared the safety and efficacy of intravitreal aflibercept versus vitrectomy for the treatment of this condition by synthesizing evidence on the safety of the two different treatment modalities.
Data Sharing Statement
The datasets used in this study are included in the main article. Figures from this study may be released via a written application to the Photographic Laboratory and Clinical Archives at Oftalmologia Integral ABC, Medical and Surgical Assistance Institution (Nonprofit Organization), Av. Paseo de las Palmas 735 suite 303, Lomas de Chapultepec, Mexico City 11000, Mexico and the corresponding author upon request.
Ethics Approval and Consent to Participate
This study adhered to the tenets of the Declaration of Helsinki and received full approval from the appropriate research ethics committee, institutional review committee, and institutional teaching department (the institutions did not provide reference numbers for systematic reviews and meta-analyses).
Institutional Review Board Statement
This study was conducted in the Retina Department of the Oftalmologia Integral ABC Institution in Mexico City, Mexico. The Institutional Review Board approved the study’s institutional guidelines. No reference numbers were provided for the systematic review and meta-analysis.
Acknowledgments
We express our deep appreciation to the technical staff of the Retina Department of Oftalmologia Integral ABC (Nonprofit Medical and Surgical Organization) affiliated with The Postgraduate Division Studies at the National Autonomous University of Mexico. Mexico City, Mexico
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis, and interpretation, or in all these areas, took part in drafting, revising, or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Disclosure
The authors declare no conflicts of interest.
References
1. Burton MJ, Ramke J, Marques AP, et al. The Lancet global health commission on global eye health: vision beyond 2020. Lancet Glob Health. 2021;9(4):e489–e551. doi:10.1016/S2214-109X(20)30488-5
2. Group ETDRSR. Fundus photographic risk factors for progression of diabetic retinopathy: ETDRS report number 12. Ophthalmology. 1991;98(5):823–833. doi:10.1016/S0161-6420(13)38014-2
3. Riaskoff S. Photocoagulation treatment of proliferative diabetic retinopathy. Ophthalmology. 1981;88(7):583–600.
4. Lövestam‐Adrian M, Svendenius N, Agardh E. Contrast sensitivity and visual recovery time in diabetic patients treated with panretinal photocoagulation. Acta Ophthalmol Scand. 2000;78(6):672–676. doi:10.1034/j.1600-0420.2000.078006672.x
5. Group ETDRSR. Early photocoagulation for diabetic retinopathy: ETDRS report number 9. Ophthalmology. 1991;98(5):766–785. doi:10.1016/S0161-6420(13)38011-7
6. Smiddy WE, Flynn HW Jr. Vitrectomy in the management of diabetic retinopathy. Surv Ophthalmol. 1999;43(6):491–507. doi:10.1016/s0039-6257(99)00036-3
7. Gong D, Hall N, Elze T, et al. Temporal trends in the treatment of proliferative diabetic retinopathy: an AAO IRIS® registry analysis. Ophthalmol Sci. 2021;1(3):100037. doi:10.1016/j.xops.2021.100037
8. Papadopoulos N, Martin J, Ruan Q, et al. Binding and neutralization of vascular endothelial growth factor (VEGF) and related ligands by VEGF Trap, ranibizumab and bevacizumab. Angiogenesis. 2012;15:171–185. doi:10.1007/s10456-011-9249-6
9. Stewart MW, Rosenfeld PJ. Predicted biological activity of intravitreal VEGF Trap. Br J Ophthalmol. 2008;92(5):667–668. doi:10.1136/bjo.2007.134874
10. Sivaprasad S, Prevost AT, Vasconcelos JC, et al. Clinical efficacy of intravitreal aflibercept versus panretinal photocoagulation for best corrected visual acuity in patients with proliferative diabetic retinopathy at 52 weeks (CLARITY): a multicentre, single-blinded, randomised, controlled, phase 2b, non-inferiority trial. Lancet. 2017;389(10085):2193–2203.
11. Koshchynets O, Vadiuk R. Managing proliferative diabetic retinopathy in a patient with vitreous hemorrhage: a case report. Clinical Trials. 2022;8:11.
12. Umanets N, Korol A, Vit V, Zavodnaya V, Pasyechnikova N. Peculiarities of vitrectomy and morphologic changes in the epiretinal membrane after intravitreal aflibercept in patients with severe proliferative diabetic retinopathy. Retin Cases Brief Rep. 2017;11(2):114–118. doi:10.1097/ICB.0000000000000306
13. Moher D, Shamseer L, Clarke M, et al. Preferred reporting items for systematic review and meta-analysis protocols (PRISMA-P) 2015 statement. Syst Rev. 2015;4(1):1–9. doi:10.1186/2046-4053-4-1
14. Higgins JP, Altman DG, Gøtzsche PC, et al. The Cochrane Collaboration’s tool for assessing risk of bias in randomised trials. BMJ. 2011;343:d5928–d5928. doi:10.1136/bmj.d5928
15. Mansour AM, Ashraf M, El Jawhari KM, et al. Intravitreal ziv-aflibercept in diabetic vitreous hemorrhage. Int J Retina Vitr. 2020;6(1):1–4. doi:10.1186/s40942-019-0204-9
16. Maturi RK, Glassman AR, Josic K, et al. Effect of intravitreous anti–vascular endothelial growth factor vs sham treatment for prevention of vision-threatening complications of diabetic retinopathy: the protocol w randomized clinical trial. JAMA Ophthalmol. 2021;139(7):701–712. doi:10.1001/jamaophthalmol.2021.0606
17. Nicholson L, Crosby-Nwaobi R, Vasconcelos JC, et al. Mechanistic evaluation of panretinal photocoagulation versus aflibercept in proliferative diabetic retinopathy: CLARITY substudy. Invest Ophthalmol Vis Sci. 2018;59(10):4277–4284. doi:10.1167/iovs.17-23509
18. Antoszyk AN, Glassman AR, Beaulieu WT, et al. Effect of intravitreous aflibercept vs vitrectomy with panretinal photocoagulation on visual acuity in patients with vitreous hemorrhage from proliferative diabetic retinopathy: a randomized clinical trial. JAMA. 2020;324(23):2383–2395. doi:10.1001/jama.2020.23027
19. Abd Elhamid AH, Mohamed AAEA, Khattab AM. Intravitreal Aflibercept injection with Panretinal photocoagulation versus early Vitrectomy for diabetic vitreous hemorrhage: randomized clinical trial. BMC Ophthalmol. 2020;20(1):1–9. doi:10.1186/s12886-020-01401-4
20. Glassman AR, Beaulieu WT, Maguire MG, et al. Visual acuity, vitreous hemorrhage, and other ocular outcomes after vitrectomy vs aflibercept for vitreous hemorrhage due to diabetic retinopathy: a secondary analysis of a randomized clinical trial. JAMA Ophthalmol. 2021;139(7):725–733. doi:10.1001/jamaophthalmol.2021.1110
21. Salam A, Mathew R, Sivaprasad S. Treatment of proliferative diabetic retinopathy with anti‐VEGF agents. Acta Ophthalmol. 2011;89(5):405–411. doi:10.1111/j.1755-3768.2010.02079.x
22. Marolo P, Borrelli E, Gelormini F, et al. Retinal thickness deviation: a new OCT parameter for assessing diabetic macular edema. J Clin Med. 2023;12(12):3976. doi:10.3390/jcm12123976
23. Chen -Y-Y, Chang P-Y, Wang J-K. Intravitreal aflibercept for patients with diabetic macular edema refractory to bevacizumab or ranibizumab: analysis of response to aflibercept. Asia Pac J Ophthalmol. 2017;6(3):250–255. doi:10.22608/APO.2016186
24. Kim JH, Kim CG, Lee DW, et al. Intravitreal aflibercept for submacular hemorrhage secondary to neovascular age-related macular degeneration and polypoidal choroidal vasculopathy. Graefes Arch Clin Exp Ophthalmol. 2020;258:107–116. doi:10.1007/s00417-019-04474-0
25. Weng S-W, Huang T-L, Chang P-Y. Intravitreal aflibercept for rubeosis iridis secondary to proliferative diabetic retinopathy. Acta Ophthalmol. 2015;30(4):201–203.
26. Heier JS, Clark WL, Boyer DS, et al. Intravitreal aflibercept injection for macular edema due to central retinal vein occlusion: two-year results from the COPERNICUS study. Ophthalmology. 2014;121(7):1414–20. e1. doi:10.1016/j.ophtha.2014.01.027
27. Imrey PB. Limitations of meta-analyses of studies with high heterogeneity. JAMA Netw Open. 2020;3(1):e1919325–e. doi:10.1001/jamanetworkopen.2019.19325
28. Hsuan JD, Brown NA, Bron AJ, Patel CK, Rosen PH. Posterior subcapsular and nuclear cataract after vitrectomy. J Cataract Refract Surg. 2001;27(3):437–444. doi:10.1016/S0886-3350(00)00585-X
29. McLeod RS. Issues in surgical randomized controlled trials. World J Surg. 1999;23:1210–1214. doi:10.1007/s002689900649
30. Howard L, Thornicroft G. Patient preference randomised controlled trials in mental health research. Br J Psychiatry. 2006;188(4):303–304. doi:10.1192/bjp.188.4.303
31. Song JW, Chung KC. Observational studies: cohort and case-control studies. Plast Reconstr Surg. 2010;126(6):2234. doi:10.1097/PRS.0b013e3181f44abc
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Clinical Features and Vitreous Biomarkers of Early-Onset Type 2 Diabetes Mellitus Complicated with Proliferative Diabetic Retinopathy
Ke D, Hong Y, Jiang X, Sun X
Diabetes, Metabolic Syndrome and Obesity 2022, 15:1293-1303
Published Date: 26 April 2022
Hypotony Maculopathy Related to Anti-VEGF Intravitreal Injection
Lima-Fontes M, Godinho G, Cunha AM, Madeira C, Falcão M, Falcão-Reis F, Carneiro Â
International Medical Case Reports Journal 2022, 15:517-520
Published Date: 19 September 2022
Clinical Characteristics and Surgical Outcomes of Complications of Proliferative Diabetic Retinopathy in Young versus Older Patients with Type 2 Diabetes
Zhang M, Xu G, Ruan L, Huang X, Zhang T
Diabetes, Metabolic Syndrome and Obesity 2023, 16:37-45
Published Date: 11 January 2023
Analysis of Risk Factors for Revitrectomy in Eyes with Diabetic Vitreous Hemorrhage
Guo H, Li W, Wang K, Nie Z, Zhang X, Bai S, Duan N, Li X, Hu B
Diabetes, Metabolic Syndrome and Obesity 2023, 16:2865-2874
Published Date: 19 September 2023
Changes in Aqueous Humor Cytokine Profile Following Intravitreal Brolucizumab Injection
Ruamviboonsuk V, Kongwattananon W, Chuaypen N
Clinical Ophthalmology 2025, 19:427-437
Published Date: 11 February 2025