Back to Journals » Infection and Drug Resistance » Volume 13
Determining Mycobacterium tuberculosis Drug Resistance and Risk Factors for Multidrug-Resistant Tuberculosis in Sputum Smear-Positive Tuberculosis Outpatients in Anhui Province, China, 2015–2016
Authors Yao S, Yan J ![]() , Li L, Ma D, Liu J, Wang Q, Wang A, Bao F, Zhang Z, Bao X
, Li L, Ma D, Liu J, Wang Q, Wang A, Bao F, Zhang Z, Bao X
Received 2 January 2020
Accepted for publication 26 March 2020
Published 9 April 2020 Volume 2020:13 Pages 1023—1032
DOI https://doi.org/10.2147/IDR.S244482
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Joachim Wink
Song Yao,1,* Junwei Yan,2,* Ling Li,1 Dongchun Ma,1 Jie Liu,1 Qing Wang,1 Aimin Wang,1 Fangjin Bao,1 Zekun Zhang,1 Xundi Bao1
1Tuberculosis Prevention and Treatment Institute of Anhui Province (Anhui Chest Hospital), Hefei 230022, Anhui, People’s Republic of China; 2Affiliated Psychological Hospital of Anhui Medical University, Hefei Fourth People’s Hospital, Anhui Metal Health Center, Hefei, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Junwei Yan No. 316, Huangshan Road, Hefei 230022, Anhui, People’s Republic of China
Tel/Fax +86-551-63658250
Email [email protected]
Background: Multidrug-resistant tuberculosis (MDR-TB) is currently a major problem in China. The prevention and treatment work for MDR-TB patients started late in Anhui province. To determine the prevalence of MDR-TB in sputum smear-positive TB patients (SSPTBPs) and analyze the risk factors for MDR-TB in Anhui province, we conducted an investigation of drug resistance among SSPTB outpatients from September 2015 to August 2016.
Methods: A stratified cluster-randomized sampling method was used to obtain a representative sample. It was estimated that 2290 new cases and 440 previously treated cases of SSPTBPs needed to be recruited from 40 survey sites. Isolates were tested for resistance to six first-line and second-line anti-TB drugs. Information from patient questionnaire survey was used to identify factors linked to MDR-TB.
Results: Finally, a total of 3047 SSPTBPs were recruited from 40 survey sites; of these, 2530 specimens were successfully cultured and had drug susceptibility testing done. The proportions of rifampin resistant (RR)-TB were 11.42% (289/2530, 95% CI: 10.18– 12.66%), 7.64% (163/2133, 95% CI: 6.38– 8.62%) and 31.74% (126/397, 95% CI: 27.38– 36.60%) in all cases, new cases and previously treated cases, respectively, and the proportions of confirmed MDR-TB were 7.63% (193/2530, 95% CI: 6.59– 8.66%), 4.97% (106/2133, 95% CI: 4.05– 5.89%) and 21.91% (87/397, 95% CI: 17.83– 26.00%), respectively. The ofloxacin resistance rate in previously treated SSPTBPs reached 21.66% (95% CI: 17.33– 26.75%). Patients who had received two or more anti-TB treatment courses were significantly associated with MDR-TB compared to patients who have received one anti-TB course.
Conclusion: MDR-TB prevalence was high among SSPTBPs in Anhui province, and past anti-TB treatment course was associated with MDR-TB.
Keywords: drug resistance, multidrug-resistant, Mycobacterium tuberculosis, tuberculosis
Background
Multidrug-resistant tuberculosis (MDR-TB) is a major problem in global TB control. In 2017, there were an estimated 558,000 new cases of rifampin (RIF) resistant TB (RR-TB), and 82% of which were MDR-TB.1 India, China and the Russian Federation accounted for almost half of the world’s cases of MDR/RR-TB, and there were about 58,000 new cases of MDR/RR-TB in China.1
Anhui province is located in the eastern part of mainland China, with a jurisdiction area of 140,100 square kilometers. At the end of 2017, the resident population was 62.548 million, and the per capita gross domestic product was 6200 dollars. Since 2004, a TB network monitoring system covering the whole province has been gradually established. 33,607 people with TB were reported in 2017, including 10,341 sputum smear-positive TB patients (SSPTBPs) (The data were obtained from the China TB network surveillance system).
The prevention and treatment work for MDR-TB patients started late in Anhui province. In 2012, the prevention and treatment of MDR-TB patients were carried out in Anqing, Fuyang and Ma’anshan city by relying on the Global Fund Program.2 After two years, the diagnosis and management of MDR-TB were officially launched in this province. When the Global Fund Program ended in 2016, the screening of MDR-TB patients was low with only 278 MDR-TB patients reported through the network. Historically, Anhui province participated in the 4 national TB epidemiological surveys. Since Anhui province was only a site in the national sample survey, and the sample size and sampling design mainly focused on the representativeness of TB prevalence in general, the obtained drug resistance results were not representative of the actual drug resistance level. In addition, a nationwide drug resistance baseline survey was conducted in 2007; these results showed MDR-TB prevalence rate in all TB patients, new TB patients and previously treated TB patients was 8.32% (401/3929), 5.71% (175/3037), and 25.64% (226/892), respectively.3 Since only 4 survey sites were set up in Anhui province, the results did not reflect the overall situation of Anhui province.
Domestic and foreign research reports indicated MDR-TB was closely related to a number of factors such as sociodemographic factors, economic level, and past anti-TB treatment courses,4–14 and these factors may differ by region or country. MDR-TB risk factors were not yet determined in Anhui province.15 The TB Prevention and Treatment Institute of Anhui province conducted a study to determine the prevalence of MDR-TB and analyzed the risk factors for MDR-TB in Anhui province.
Methods
In 2015, there were 86 TB clinics in Anhui province, covering 105 counties (districts) in 16 cities. It is estimated that in 2015, the prevalence of HIV among the entire population and TB patients in our province was 0.16% and 0.02% (102/35,550), which are all in a low epidemic situation. We did a prospective study from 2015 to 2016, and HIV was not test.
Sampling Method
(1) A stratified cluster sampling method was used to obtain a representative sample by referring to the monitoring program of the World Health Organization (WHO) Guidelines for surveillance of drug resistance in tuberculosis (Fourth Edition).16
2) We only chose sputum smear-positive specimens for culture, because the possibility of positive culture was very low for sputum smear-negative specimens, and subsequent drug sensitivity testing (DST) cannot be carried out.
3) The sample size is calculated according to the statistical requirements of the cross-sectional survey. Sample size formula: n= deff* (N*z^2 p(1-p))/(d^2 (N-1)+z^2 p(1-p)), where parameter N, the total number of SSPTBPs reported in the past year, was estimated according to the number in 2014 (N=11,151). The estimated resistance rate of RIF in new cases and previously treated cases was 0.07 (p=0.07), accuracy d=±1.4% and 0.3 (p=0.3), accuracy d=±6%, respectively, credibility was set to 95%, z=1.96, design effect deff=2.3,16 Then the sample size required for new cases of SSPTBPs is 2290, and the sample size required for previously treated cases is 440.
4) After comprehensive consideration of the sample size required for this survey, the time limit for completing the survey within one year and the number of TB patients actually diagnosed and treated at each survey site each year, 40 survey sites were finally selected. Then each survey site should recruit 57 new cases and 11 previously treated cases of SSPTBPs.
5) For stratified cluster sampling, the units of sampling are city-level or county-level (district-level) TB diagnosis and treatment units, mainly including city-level, county-level (district-level) disease prevention and control centers and TB designated hospitals.
6) Specific steps for sampling (Figure 1). Step 1 is to sort the administrative division code of TB prevention and control planning units in Anhui province. Step 2 is to collect the number of SSPTBPs registered and reported by all TB prevention and treatment planning implementation units in 2014, and list the cumulative number of SSPTBPs. Step 3 is to determine the sampling interval, which is equal to the cumulative number of SSPTBPs divided by the number of units to be sampled. Step 4 is to use the random number table to generate a random number, and the planning unit corresponding to the number of cumulative SSPTBPs is the first survey site. Step 5 is to determine the second to the 40th survey site (Figure 2) according to the same sampling interval. If the investigation site determined by random sampling cannot undertake the investigation due to special circumstances such as region, traffic or the number of patients, they can be replaced or supplemented downward in the prefecture-level cities under which the investigation sites belongs. In principle, the number of investigation sites replaced shall not exceed 5% of the total investigation sites.
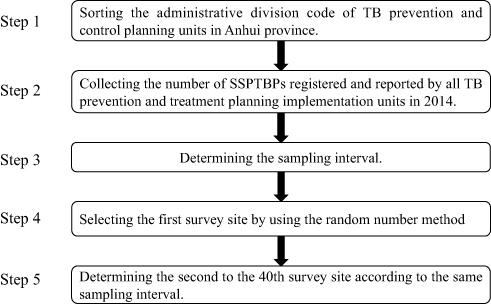 |
Figure 1 Specific steps for sampling. |
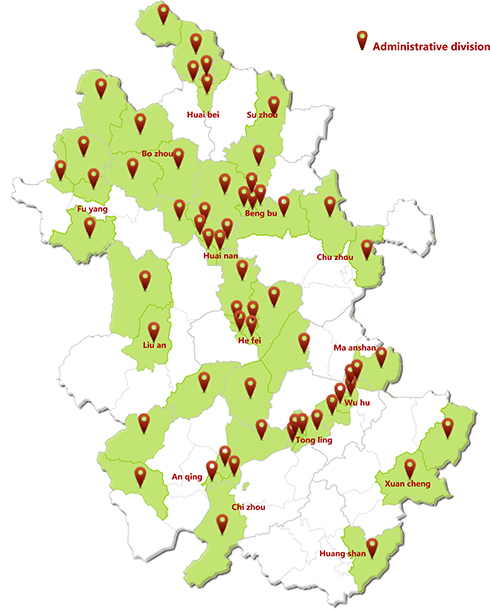 |
Figure 2 Layout of the county (district) administrative divisions covered by 40 survey sites. |
Case Inclusion Principles
The following principles were followed in the inclusion of cases at each investigation site: 1) During the investigation, new cases and previously treated cases should be included in the survey consecutively from the beginning to the end according to the registration time, and they could be stopped after reaching the specified number of samples. 2) The investigated cases were newly registered cases from September 15, 2015to August 31, 2016. 3) There was no age range limited for the included cases. 4) TB clinic doctors register and classify the TB patients by asking their medical history. New cases refer to TB patients who have not received any anti-TB treatment course or who received anti-TB treatment course for less than one month. Previously treated cases include four groups of patients: relapse, return after loss to follow-up, treatment failure and re-treatment patients not included in the previous three groups. Re-treatment patients not included in the previous three groups refer to the chronic TB patients treated repeatedly. Recurrence refers to patients with a clear history of anti-TB treatment. After completing the prescribed chemotherapy course, the doctor believed that it had been cured. At this time, the sputum smear was positive or the lesion of the TB patient had obvious activity. Return refers to patients with TB who had been treated for more than one month and whose treatment had been interrupted for more than or equal to two months, and then continued to seek treatment in a medical institution because of clinical symptoms related to TB. Initial treatment failure refers to the smear sputum was positive at the 5th month of anti-TB treatment course. 4) No examination fee was charged for the included patients.
Case Information Collection and the Definition of Variables
Two trained clinicians obtained signed informed consent from eligible participants. Once informed consent was obtained, a survey questionnaire was administered and completed by each participant to collect sociodemographic data and clinical records about past anti-TB treatment courses. When the respondent was a child younger than 18 years old, the investigator explained the purpose and the content of the investigation to the participant and the legal guardian; the legal guardian signed the informed consent form. Sociodemographic data including sex, age, educational status, and family income in 2014 were collected. Clinical data including household contact with TB patients, past anti-TB treatment courses, the number of anti-TB treatment courses, adverse drug reaction, duration of the first anti-TB treatment course, discontinuation of previous anti-TB treatment courses, and the number of discontinuation of previous anti-TB treatment courses were captured. After completing all the surveys at each survey site, investigators sealed all questionnaires and consent forms, and handed them to the survey coordinators.
One treatment course in “the number of anti-TB treatment courses” refers to one of the following conditions. First, including 6 months of treatment with the “2HRZE/4HR” (H, isoniazid, INH; R, rifampicin; Z, pyrazinamide; E, ethambutol, EMB) chemotherapy regimen, using “3HRZE/4HR” 6HRE chemotherapy regimen for 9 months, and the use of personalized treatment regimen. Second, within the same course of treatment, if the continuous treatment is stopped for no more than 2 months, it is considered as a course of treatment. Third, within the same course of treatment, the drug is discontinued for more than 2 months, and the treatment before the drug discontinuation is regarded as one treatment.
Bacteriological Examination
Three sputum specimens were obtained from each participant before starting TB treatment. Ziehl-Neelsen staining and smear microscopy for acid-fast bacilli was done on all specimens and the remainder of each specimen was stored at 4 degree Celsius. The best two specimens (highest smear positivity and if only one positive smear, the best smear-negative specimen) were selected for culture and the remainder of the smear-positive specimens stored at −20 degree Celsius. Positive specimens were cultured on lowenstein-jensen (LJ) medium with or without p-nitrobenzoic acid (PNB); growth of Mycobacterium TB (M. TB) was inhibited by PNB, while growth of non-TB Mycobacterium (NTM) was not affected. Positive cultures from each site were sent to provincial reference laboratories for DST.
DST was performed using the proportion method on LJ medium impregnated with INH, RIF, streptomycin (SM), EMB, ofloxacin (OFL) and kanamycin (KM). The concentrations of anti-TB drugs used were 0.2 μg/mL for INH, 40 μg/mL for RIF,2 μg/mL for EMB, 4 μg/mL for SM, 2 μg/mL for OFL, and 2 μg/mL for KM.17 After completion of all DSTs 10% strains were randomly selected for retesting.
Any drug-resistant TB was defined as resistance to any of the anti-TB drugs among the six drugs (INH, RIF, EMB, SM, OFL or KM). Poly-resistance was defined as resistance to two or more drugs excluding INH and RIF. MDR was defined as resistance to INH and RIF and RR were defined as resistant to RIF. XDR was defined as resistance to at least INH, RIF, OFL, and KM.
Statistical Analysis
The input of the original data was performed by two members of the Tuberculosis Prevention and Treatment Institute of Anhui Province using Epidata software (version 3.1), respectively. Consistency test was carried out on the two databases, and the inconsistent data were determined by the two staff members after checking the original data. Odds ratio (OR) value and 95% confidence intervals (CIs) were used to evaluate the MDR-TB related univariate risk factors. All variables in the univariate analysis were used in the logistic regression analysis modeling for survey data. All relevant variables were initially included in the model, and the forward method was used to select the final variables. The models were compared with the use of the maximum rescaled R2 statistic. P<0.05 was considered statistically significant. All statistical analyses were performed using SPSS software (version 16.0).
Results
Case Inclusion
A total of 3047 cases were recruited in the 40 survey sites, including 2502 new cases and 545 previously treated cases. Of these, 2330 (76.5%) were males, while 717 (23.5%) were females. The average age of all cases is 53.59 ± 19.63 years, with a range between 8 years and 96 years old.
Results of DST
Of the 3047 SSPTBPs cases, DST was not done in 517 (16.97%): 275/517 had negative cultures, in 141 NTM was cultured and 101 cultures were contaminated. Finally, 2530 specimens were successfully cultured. DST results are showed in Table 1. The proportions of RR-TB were 11.42% (289/2530, 95% CI: 10.18–12.66%), 7.64% (163/2133, 95% CI: 6.38–8.62%) and 31.74% (126/397,95% CI: 27.38–36.60%), respectively, in all cases, new cases and previously treated cases, and the proportion of MDR-TB was 7.63% (193/2530, 95% CI: 6.59–8.66%), 4.97% (106/2133, 95% CI: 4.05–5.89%) and 21.91% (87/397,95% CI: 17.83–26.00%). The drug resistance rate of previously treated cases to OFL reached 21.66% (17.33–26.75%).
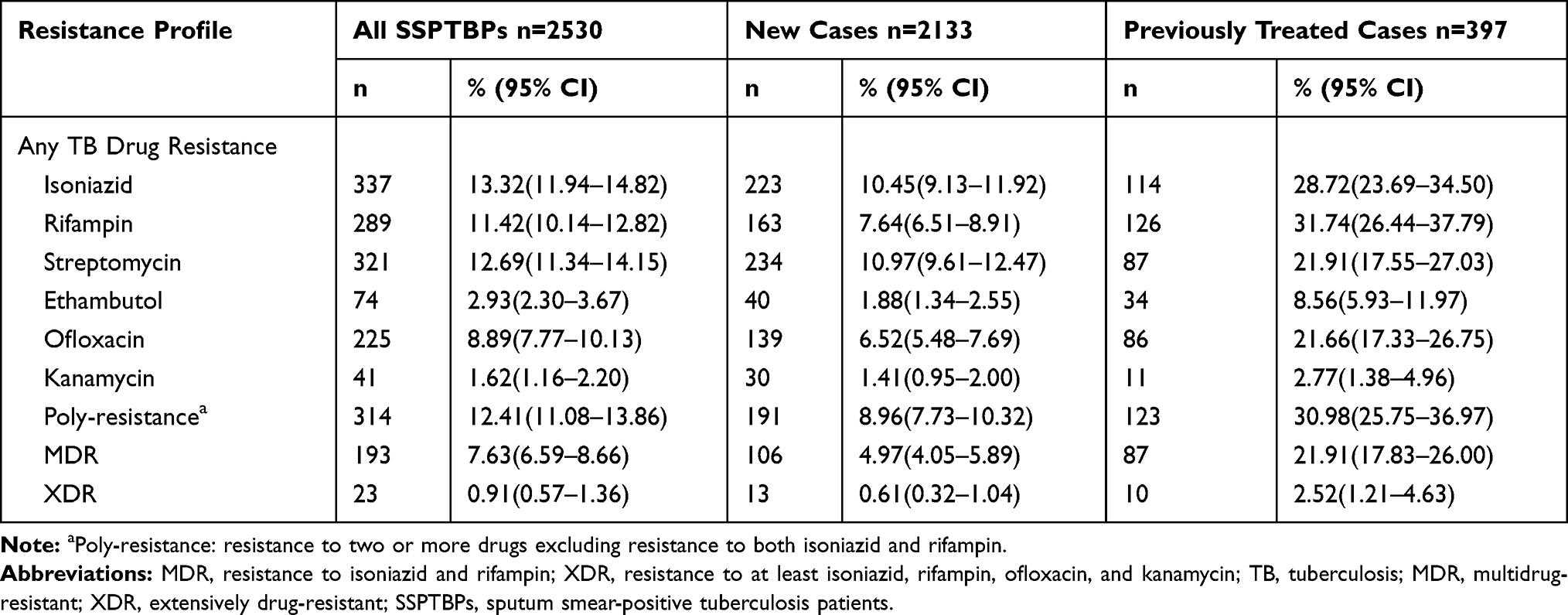 |
Table 1 Drug Resistance to First-Line and Second-Line Anti-Tuberculosis Drugs in Anhui, China, 2015–2016 |
Analysis of Risk Factors for MDR-TB in All Cases
Of the 2530 cases with DST results, 2529 had completed questionnaires. Table 2 shows the analysis results of risk factors for MDR-TB in all SSPTBPs. The univariate analysis results showed that household contact with TB patients, past anti-TB treatment courses, the number of anti-TB treatment courses, duration of the first anti-TB treatment courses, and number of interruptions to past anti-TB treatment courses were related to MDR-TB (P<0.05), while the other factors such as sex, age, educational status, household income in 2014, adverse drug reaction, and past anti-TB treatment interruption had no significant association with MDR-TB (P>0.05). Results of multivariate analysis showed only the number of anti-TB treatment courses was included in the model (P=0.004), and cases who received two or more anti-TB treatment courses had a significantly increased risk for developing MDR-TB compared with those who received one anti-TB treatment courses, respectively (OR=5.367, 95% CI=1.258–22.897, P<0.001; OR=13.143, 95% CI=3.487–49.534, P<0.001).
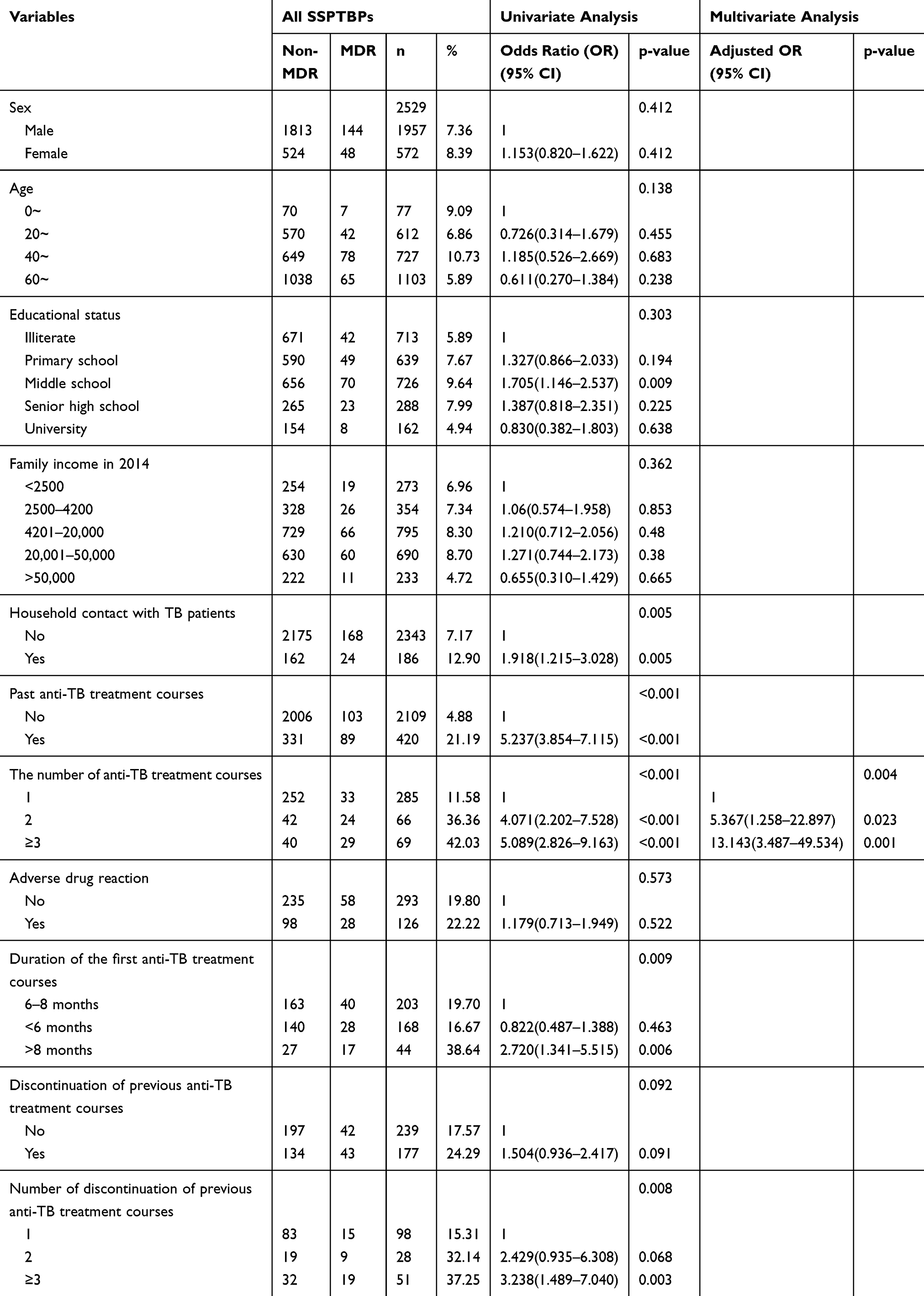 |
Table 2 Analysis of Risk Factors for Multidrug-Resistant Tuberculosis (MDR-TB) in All Cases |
Analysis of Risk Factors for MDR-TB in New Cases
Among the 2529 SSPTBPs with questionnaire, 2132 patients were new cases. Table 3 shows the analysis results of risk factors for MDR-TB in new cases. Univariate analysis did not find that age, sex and other factors were related to the generation of MDR-TB.
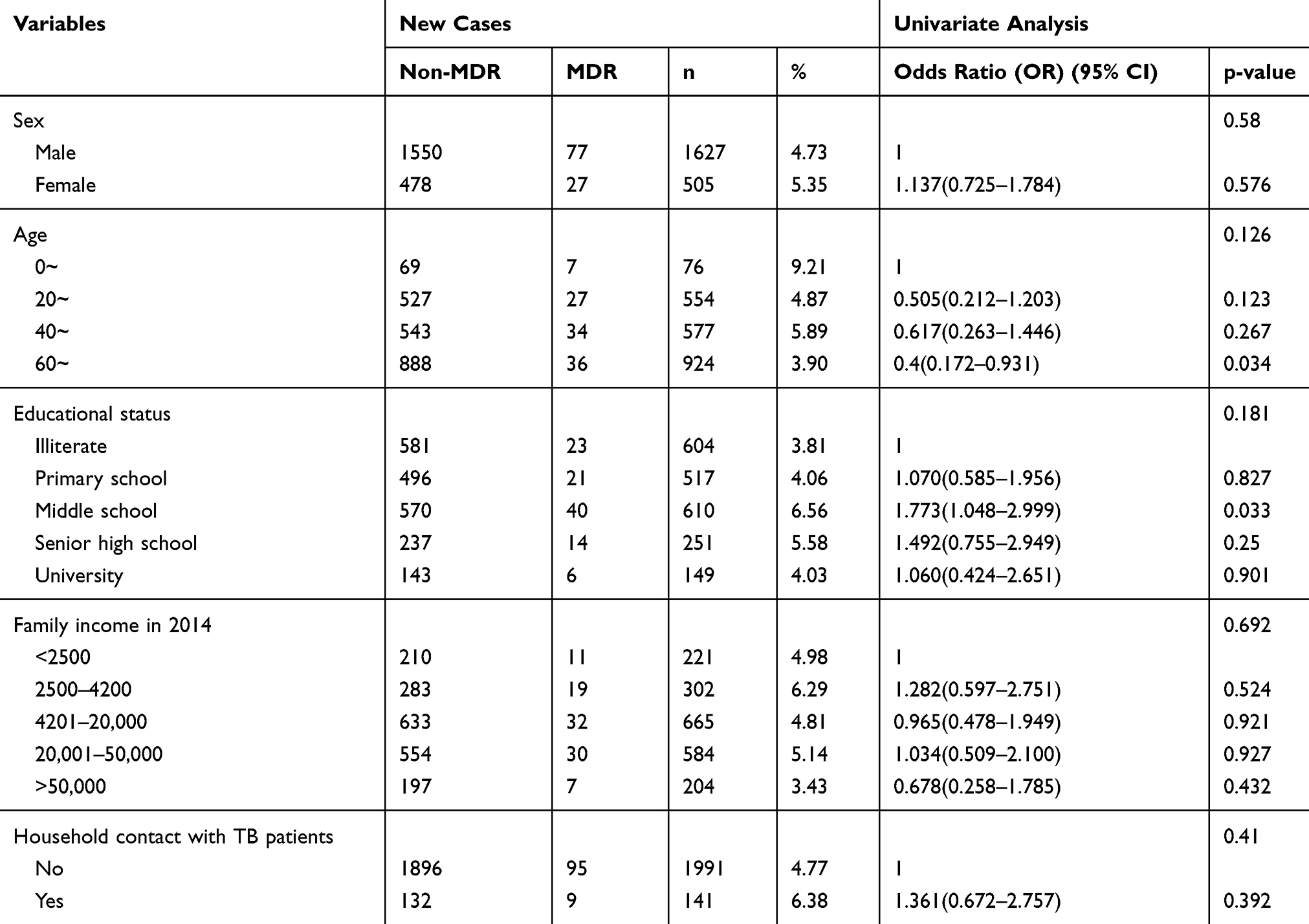 |
Table 3 Analysis of Risk Factors for Multidrug-Resistant Tuberculosis (MDR-TB) in New Cases |
Analysis of Risk Factors for MDR-TB in Previously Treated Cases
A total of 397 valid questionnaires for previously treated cases of SSPTBPs were collected, and Table 4 shows the analysis results of risk factors for MDR-TB. Univariate analysis showed that age, the number of anti-TB treatment courses, duration of the first anti-TB treatment courses, discontinuation of previous anti-TB treatment courses, and number of discontinuation of previous anti-TB treatment courses were significantly associated with MDR-TB (P<0.05). Factors such as sex, educational status and household income in 2014 were not related to MDR-TB. When all the above single variable was included in the logistic regression model, only the number of anti-TB treatment courses was included in the model (P=0.002). Subgroup analysis results show cases who received two or more anti-TB treatment courses had a significant association with MDR-TB compared with those who received one anti-TB treatment courses (OR=4.544, 95% CI=1.054–19.590, P=0.042; OR=11.100, 95% CI=2.913–42.300, P< 0.001).
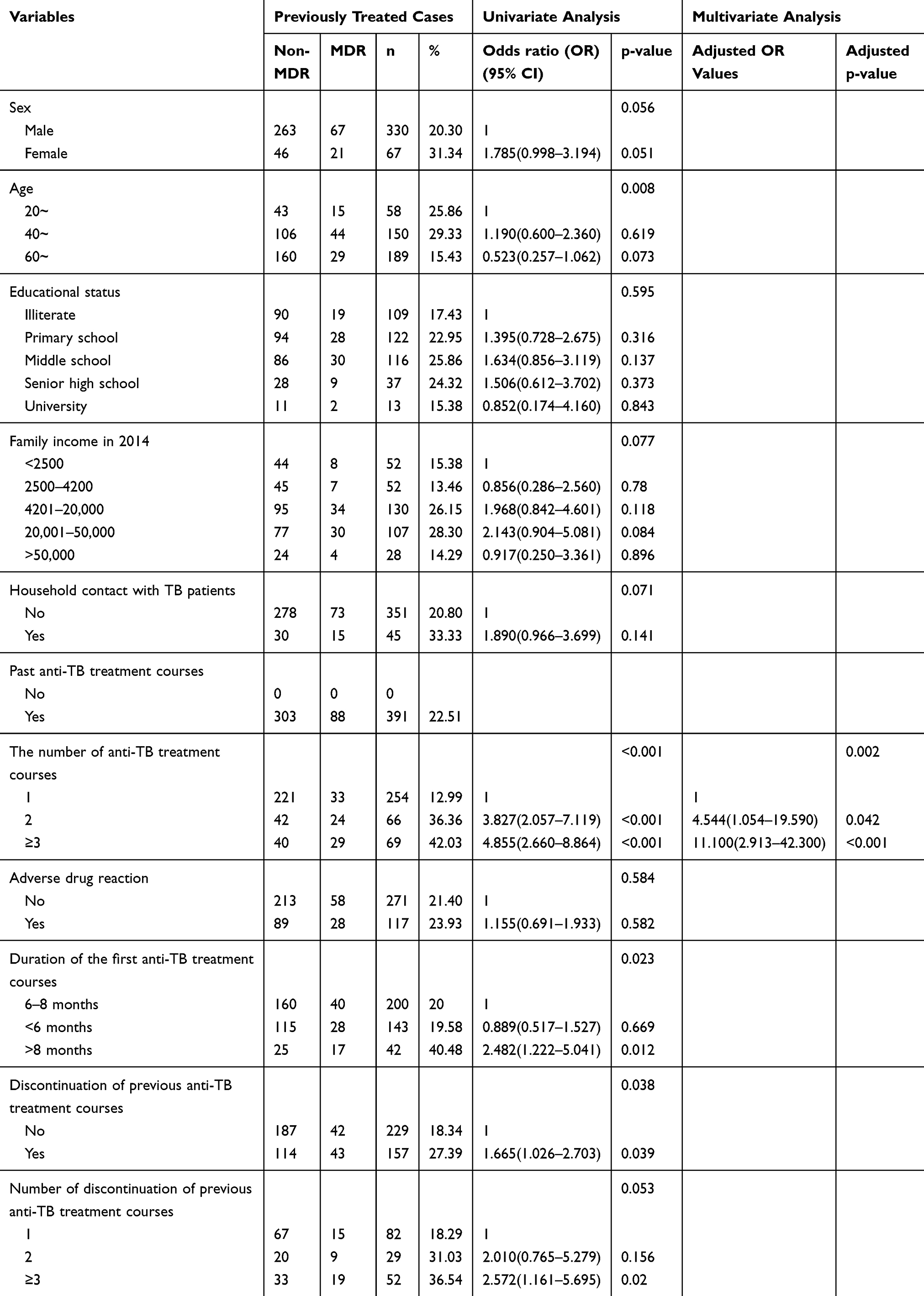 |
Table 4 Analysis of Risk Factors for Multidrug-Resistant Tuberculosis (MDR-TB) in Previously Treated Cases |
Discussion
In this study, the proportion of RR in SSPTBPs in Anhui Province was systematically sampled for the first time. Our results showed that the proportion of RR in new cases and previously treated cases was 7.64% (6.38–8.62%) and 31.74% (27.38–36.60%), respectively, which was higher than the national average of 7.1% (5.6–8.7%) and 24% (20–28%), and also above the global average of 4.1% (2.8–5.3%) and 19% (9.8–27%).18 The reasons for the high RR-TB prevalence in this study are not clear and further studies to determine possible reasons are needed. As in other studies, previously treated patients have a higher rate of RR-TB, but even new TB cases had a high rate of RR-TB.19 The reasons for this need to be explored.
Based on the prevalence of MDR-TB from this survey, we estimated that there are approximately 727 MDR-TB patients in Anhui Province in 2017: 451 patients were new cases, accounting for 62%, and 276 patients were previously treated cases, accounting for 38% (The estimation formula: M=Pn×Cn+Pr×Cr, M: total number of MDR-TB patients, Pn: the proportion of MDR-TB in new cases, which equals to 4.97% in this study, Pr: the proportion of MDR-TB in previously treated cases of SSPTBPs, which equals to 21.91%, Cn: the number of new cases in Anhui Province in 2017, which equals to 9071, Cr: the number of previously treated cases in Anhui Province in 2017, which equals to 1259.). However, only 310 MDR-TB patients were actually registered in Anhui Province in 2017, including 107 new cases, accounting for 34.5%, and 203 previously treated cases, accounting for 64.5%. This result suggested new and previously treated TB patients should have DST done so that an appropriate anti-TB treatment regimen can be started in all patients.
This study found that the drug resistance rate of previously treated patients to ofloxacin reached 21.66% (17.33–26.75%), much higher than the average level of 8.7% (6.1–11.2%) in China3 and 17% in Dalian city,7 and close to the WHO-reported rate of resistance to fluoroquinolones (FQs) in global MDR-TB patients (22%).1 High drug resistance of ofloxacin may be related to a number of factors. In China, FQs drugs are the preferred drug for undiagnosed respiratory bacterial infections,20 and readily available on the market. What’s more, excessive and premature use of ofloxacin in the anti-TB diagnostic treatment is also one of the reasons. FQs have been recommended as first-line drugs for the treatment of MDR-TB due to their high activity against M.tuberculosis. Unfortunately, poorly controlled use of FQs leads to the emergence of FQs resistance in M.tuberculosis, which might influence the therapeutic effect for MDR-TB patients.21 Thus, it is significant for us to accept that strict control of the use of FQs is important for the treatment of MDR-TB.
There are still several limitations in this study. First, the cases included in this survey are all SSPTBPs in the outpatient clinic of TB, rather than all TB patients in the population. Therefore, there are certain restrictions when the drug resistance results are extrapolated to all TB patients. Second, the factors affecting the production of MDR-TB are complex. Because the focus of this survey is to understand the prevalence of MDR-TB in Anhui Province, in order to ensure the feasibility of the survey, the influencing factors included in the questionnaire are not comprehensive enough. Foreign research mentioned HIV infection, drug use, and the economic burden and psychological factors of patients are not included in this survey. We will further discuss these factors and MDR-TB in the subsequent study.
Conclusion
The prevalence of MDR-TB was high among the SSPTBPs in Anhui Province, and past anti-TB treatment courses were associated with MDR-TB.
Abbreviations
CIs, Confidence intervals; EMB, Ethambutol; INH, Isoniazid; KM, Kanamycin; LJ, Lowenstein-jensen; MDR-TB, multidrug-resistant tuberculosis; MTB, Mycobacterium tuberculosis; NTM, Non-Mycobacterium tuberculosis; OFL, Ofloxacin; OR, Odds ratio; PNB, P-nitrobenzoic acid; RIF, Rifampin; RR-TB, Rifampin resistant tuberculosis; SM, Streptomycin; SSPTBPs, Sputum smear positive TB patients; WHO, World Health Organization.
Data Sharing Statement
The datasets used and analyzed during the current study are available from the corresponding author on reasonable request, and some of the data cannot be accessed due to patient confidentiality.
Ethics and Consent Statement
This protocol was approved by the Ethics Committee of Tuberculosis Prevention and Treatment Institute of Anhui Province (Anhui Chest Hospital) (Approval number: AHJF-IRB-SC-20150506). We confirmed that our study was conducted in accordance with the Declaration of Helsinki. All included patients signed the written informed consent form indicating their consent to participate in this survey. When the respondent is a child younger than 18 years old, the investigator explained the purpose and the content of the investigation to the respondent and its guardians face to face, and the guardians signed the written informed consent form after thorough consideration.
Acknowledgment
Song Yao and Junwei Yan are co-first authors for this study.
Funding
This study was granted by the “2015 Anhui Provincial Health Planning Commission Research Project (15tb010)”. The sponsors of this study had no role in study design, data collection, data analysis, data interpretation, and writing of the manuscript.
Disclosure
The authors declare that they have no competing interests in this work.
References
1. World Health Organization. Global Tuberculosis Report 2018. Geneva: World Health Organization; 2018.
2. Li L, Yao S, Zou Z, et al. Analysis on the effect evaluation of the global fund tuberculosis project on MDR-TB control in the pilot city of Anhui Province. Chin J Anti-Tuberc. 2017;39(7):728–731.
3. Zhao Y, Xu S, Wang L, et al. National survey of drug-resistant tuberculosis in China. N Engl J Med. 2012;366(23):2161–2170. doi:10.1056/NEJMoa1108789
4. Muchena G, Shambira G, Masuka N, et al. Determinants of multidrug resistance among previously treated tuberculosis patients in Zimbabwe, 2014. Int J Tuberc Lung Dis. 2017;21(11):1167–1172. doi:10.5588/ijtld.16.0826
5. Semunigus T, Tessema B, Eshetie S, et al. Smear positive pulmonary tuberculosis and associated factors among homeless individuals in Dessie and Debre Birhan towns, Northeast Ethiopia. Ann Clin Microbiol Antimicrob. 2016;15(1):50. doi:10.1186/s12941-016-0165-x
6. Shariff NM, Shah SA, Kamaludin F. Previous treatment, sputum-smear nonconversion, and suburban living: the risk factors of multidrug-resistant tuberculosis among Malaysians. Int J Mycobacteriol. 2016;5(1):51–58. doi:10.1016/j.ijmyco.2015.11.001
7. Lv X, Lu X, Shi X, et al. Prevalence and risk factors of multi-drug resistant tuberculosis in Dalian, China. J Int Med Res. 2017;45(6):1779–1786.
8. Luo D, Zhao J, Lin M, et al. Drug resistance in newly presenting and previously treated tuberculosis patients in Guangxi Province, People’s Republic of China. Asia Pac J Public Health. 2017;29(4):296–303.
9. Derseh D, Moges F, Tessema B. Smear positive pulmonary tuberculosis and associated risk factors among tuberculosis suspects attending spiritual holy water sites in Northwest Ethiopia. BMC Infect Dis. 2017;17(1):100. doi:10.1186/s12879-017-2211-5
10. Sinha P, Srivastava GN, Gupta A, et al. Association of risk factors and drug resistance pattern in tuberculosis patients in North India. J Glob Infect Dis. 2017;9(4):139–145. doi:10.4103/jgid.jgid_167_16
11. Khan MS, Hutchison C, Coker RJ. Risk factors that may be driving the emergence of drug resistance in tuberculosis patients treated in Yangon, Myanmar. PLoS One. 2017;12(6):e0177999. doi:10.1371/journal.pone.0177999
12. Worku J, Marjan G, Leila S, et al. Prevalence of and risk factors for multidrug-resistant tuberculosis in Iran and its neighboring countries: systematic review and meta-analysis. Rev Soc Bras Med Trop. 2017;50(3):287–295. doi:10.1590/0037-8682-0002-2017
13. Stosic M, Vukovic D, Babic D, et al. Risk factors for multidrug-resistant tuberculosis among tuberculosis patients in Serbia: a case-control study. BMC Public Health. 2018;18(1):1114. doi:10.1186/s12889-018-6021-5
14. Mesfin EA, Beyene D, Tesfaye A, et al. Drug-resistance patterns of Mycobacterium tuberculosis strains and associated risk factors among multi drug-resistant tuberculosis suspected patients from Ethiopia. PLoS One. 2018;13(6):e0197737. doi:10.1371/journal.pone.0197737
15. Yu S, Mei X, Yan X, et al. Case-control study on risk factors of multidrug-resistant tuberculosis in Anhui Province. J Dis Control. 2016;20(10):1026–1028.
16. World Health Organization. Guidelines for Surveillance of Drug Resistance in Tuberculosis.
17. World Health Organization. Guidelines for Drug Susceptibility Testing for Second-Line Anti-Tuberculosis Drugs for Dots-Plus. Geneva, Switzerland: WHO; 2001.
18. World Health Organization. Global Tuberculosis Report 2017. Geneva: World Health Organization; 2017.
19. Van Rie A, Warren R, Richardson M, et al. Classification of drug-resistant tuberculosis in an epidemic area. Lancet. 2000;356(9223):22–25. doi:10.1016/S0140-6736(00)02429-6
20. Chinese Medical Association Respiratory Diseases Branch. Guidelines for the diagnosis and treatment of adult adult community acquired pneumonia (2016 edition). Chin J Tuberc Res Dis. 2016;39(4):253–279.
21. Zhang Z, Lu J, Wang Y, et al. Prevalence and molecular characterization of fluoroquinolone-resistant Mycobacterium tuberculosis isolates in China. Antimicrob Agents Chemother. 2014;58(1):364–369. doi:10.1128/AAC.01228-13
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.