Back to Journals » HIV/AIDS - Research and Palliative Care » Volume 13
Determinants of the Community Knowledge and Attitude Towards HIV Prevention Methods in Majang Zone, Southwest Ethiopia
Authors Wondimu W ![]() , Asefa A
, Asefa A ![]() , Qanche Q
, Qanche Q ![]() , Nigussie T
, Nigussie T ![]() , Yosef T
, Yosef T ![]()
Received 29 October 2020
Accepted for publication 6 January 2021
Published 12 January 2021 Volume 2021:13 Pages 21—29
DOI https://doi.org/10.2147/HIV.S289379
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Bassel Sawaya
Wondimagegn Wondimu,1 Adane Asefa,1 Qaro Qanche,2 Tadesse Nigussie,3 Tewodros Yosef1
1Department of Epidemiology and Biostatistics, School of Public Health, College of Medicine and Health Sciences, Mizan-Tepi University, Mizan Aman, Ethiopia; 2Department of Public Health, School of Public Health, College of Medicine and Health Sciences, Mizan-Tepi University, Mizan Aman, Ethiopia; 3Department of Reproductive Health and Nutrition, School of Public Health, College of Medicine and Health Sciences, Mizan-Tepi University, Mizan Aman, Ethiopia
Correspondence: Wondimagegn Wondimu
Mizan-Tepi University, College of Medicine and Health Sciences, School of Public Health, Department of Epidemiology and Biostatistics, PO Box: 260, Mizan Aman, Ethiopia
Email [email protected]
Background: Although in Ethiopia there is a high burden of HIV/AIDS, the community knowledge and attitude towards HIV/AIDS prevention has not been investigated adequately. Thus, this study assessed the determinants of the community knowledge and attitude towards HIV/AIDS prevention in the Majang zone which is the zone with the highest HIV prevalence in Ethiopia.
Methods: A community-based cross-sectional study was conducted in the Majang zone, southwest Ethiopia from March 1st to May 31st, 2019 by including randomly selected 845 adults. Knowledge and attitude towards HIV prevention methods were dependent variables. The independent variables include socio-demographic characteristics and behavioral factors. A binary logistic regression was employed to determine the association using the odds ratio at 95% confidence intervals. A p-value of less than 5% was considered to declare the final significance.
Results: Of 845 respondents recruited, 772 participated yielding a 91.4% response rate. Not sharing contaminated sharp materials (63.4%), consistent condom use (61.2%), and abstinence (57.9%) were the prevention methods mentioned by majority of the respondents. Only two of five respondents (39.6%) had good HIV prevention knowledge. More than half [412 (53.4%)] of the respondents had a positive attitude towards HIV prevention. The independent determinants of HIV prevention knowledge were secondary educational status (AOR=1.84; 95% CI=1.04, 3.24), tertiary and above educational status (AOR=2.01; 95% CI=1.07, 3.75) and positive HIV prevention attitude (AOR=1.89; 95% CI=1.39, 2.57). Similarly, age of greater than 27 years (AOR=2.13; 95% CI=1.55, 2.95) and good HIV prevention knowledge (AOR=1.83; 95% CI=1.35, 2.48) were significantly associated with a positive HIV prevention attitude.
Conclusion: This study revealed insufficient HIV prevention knowledge and attitude in the community with the highest HIV prevalence. To achieve the goal of ending the HIV epidemic, health education should be considered using different innovative approaches especially by prioritizing young and less educated individuals.
Keywords: HIV/AIDS prevention, knowledge, attitude, Majang, Ethiopia
Introduction
The prevalence of Human Immunodeficiency Virus/Acquired Immune Deficiency Syndrome (HIV/AIDS) is not decreasing as expected and leads to a significant number of life loss. The pandemic of HIV/AIDS leads to 960, 000 deaths globally in 2019. In Eastern and Southern Africa, there were an estimated 300,000 AIDS-related deaths in the same year.1 In 2017, an estimated 613,000 people were living with HIV in Ethiopia; of whom 62% were females.2 The adult HIV prevalence in Ethiopia in 2016 was estimated to be 1.1%. There was substantial prevalence variation by region (6.6% in Gambella, 5.0% in Addis Ababa, and 0.7% in Southern Nations, Nationalities and Peoples’ (SNNPR) region). This indicates that the Gambella region had the highest share of HIV prevalence.3
Considering the fatal impact of HIV/AIDS’ prevalence, there is a great struggle globally to end its epidemic. In 2014, UNAIDS launched new targets named 90-90-90 to help end the AIDS epidemic.4–6 Ethiopia has adopted the global goal to attain the 90-90-90 targets: 90% of people living with HIV (PLHIV) know their status, 90% of PLHIV who know their status are on treatment (ART) and 90% of PLHIV on treatment have attained viral suppression. The country has developed a national prevention road map with different pillars to attain the global goal and combination of HIV prevention. Furthermore, the road map also specified the geographic priorities for intervention due to variation in the burden of the HIV infection by residence, and population groups.2
The goals set nationally and internationally can be achieved when the community, particularly those living in high prevalent areas, have adequate knowledge and a positive attitude towards HIV prevention methods. HIV prevention is a complex issue and having good knowledge and a positive attitude are essential for its success.7 In Eastern and Southern Africa, many people lack basic HIV related knowledge, and the level of negative attitude including stigma towards people living with HIV remain high.6
Although Ethiopia is among the countries with a high burden of HIV/AIDS, there is a gap of community-based study that investigated the knowledge and attitude towards HIV/AIDS prevention methods in the country. As per the knowledge of the authors, no published community-based study assessed the knowledge and attitude towards HIV prevention methods in Ethiopia. As a result, this study assessed the factors determining the knowledge and attitude of the community regarding HIV prevention methods in the Majang zone (Gambella region) which had the highest (3.5%) estimated HIV prevalence at the second administrative level (zonal level) in Ethiopia in 2017.8
Methods and Materials
Study Design, Setting, and Period
A community-based cross-sectional study was conducted in the Majang zone from March 1st to May 31st, 2019. Majang zone is found in Gambella regional state and it is among HIV high prevalent areas in Ethiopia.8 It is found 628 km from Addis Ababa, the capital of Ethiopia to the southwest direction. It has three woredas namely Godere, Mengeshi, and Meti. Based on the population projection done by the Central statistical agency (CSA) for 2014–2017, the zone had a total population of 79,041, of whom 40,896 were men.9
Sample Size Determination, Sampling Technique, and Study Population
The single population proportion formula was used by taking the following assumptions. The proportion of good knowledge about HIV prevention methods taken as 50% since there was no study conducted in a comparable setting. Moreover, a 95% confidence level and 5% margin of error were considered. The calculated sample size became 384. After using the design effect of 2 and adding 10% for non-response rate the final sample size was 845. The study population for this study were all randomly selected adults in the Majang zone and whose age was greater or equals to 18. To identify the calculated sample, first, we have selected 30% of Kebeles (the smallest administrative unit) from three woredas found in the Majang zone. Using a sampling frame obtained from the health post family folder registry, a systematic random sampling technique was employed to select the sampling unit (households) from the identified Kebeles. Then, the selected households’ eligible individual was selected by lottery method, if there were more than one eligible participant in the household.
Study Variables
Knowledge and attitude towards HIV prevention methods were dependent variables. The independent variables include socio-demographic characteristics (age, sex, marital status, occupation, educational status, and residence) and behavioral factors (history of alcohol drinking and chat chewing).
Data Collection Procedures and Quality Management
A structured questionnaire developed from different literatures was used. The internal validity of the questionnaire was checked by computing the Pearson correlation coefficient (r). The minimum calculated r (0.123) was significantly (p=0.001) higher than the critical value (0.071) with degree of freedom (df)=770 and two-sided α=0.05. This is suggestive of the validity of the questionnaire used. Nine BSc nurses collected the data with a close follow-up of three supervisors. The English version questionnaire was first translated into the Amharic language. Then, it was back-translated to English to check its consistency. The one-day training was given for the data collectors and supervisors concerning the objectives and data collection procedures. Pre-testing was conducted on 10% of the sample outside the selected Kebeles and some modifications were done on the study tool accordingly. Close supervision was conducted daily to ensure the completeness and consistency of the filled questionnaire.
Data Entry, Processing, and Analysis
The collected data were coded and entered using Epidata manager version 4.0.2.101, and cleaned and analyzed using SPSS version 21 statistical software. Summary statistics of the categorical independent variables were presented using frequency tables and proportions. The continuous variables were described using mean with standard deviation (SD) and median with interquartile range (IQR) depending on the suitability of the data. The participants were asked ten knowledge and thirteen attitude questions that were related to HIV prevention methods and further composited to categorize an individual whether he/she has good or poor knowledge and positive or negative attitude. Negatively worded knowledge and attitude questions were reverse scored.
The knowledge questions had three categories of responses (yes, no and I do not know) which further reduced to two categories (correct and incorrect answers). The response “I don’t know” was classified under an incorrect category. The correct answers were coded as 2 and incorrect answers were coded as 1. Thus, the maximum knowledge score was 20. Likewise, five-point scale attitude questions were used and each question (statement) had five categories (strongly disagree, disagree, neutral, agree, and strongly agree) coded from 1 to 5. The maximum attitude score that can be achieved by the respondents was 65. Participants who scored greater or equals to an average score of knowledge questions (10.8) were categorized as knowledgeable, otherwise not knowledgeable. Similarly, those who scored greater or equals to an average score of attitude questions (35.3) were categorized as having a positive attitude and otherwise negative attitude. A binary logistic regression was computed to determine the association between independent variables and outcome variables (knowledge and attitude) using the odds ratio at a 95% confidence level. Independent variables with p-values less than 25% were candidates for multivariable logistic regression. A p-value of less than 5% was considered as the level of significance for the final model. Regarding the model fitness, the Hosmer and Lemeshow analysis provided the p-value for knowledge and attitude as 10.8% and 62.9%, respectively, which indicate that the final models fit the data well.
Ethical Consideration
This study was conducted in accordance with the Declaration of Helsinki. Ethical approval was sought from the ethical review committee of Mizan-Tepi University and a cooperation letter was written to the respective government bodies of study areas and permission was obtained. Informed written consent was obtained from the study participants after interviewers explained the objectives, purposes, participants’ rights, and confidentiality of the study. The study participants were informed about their right to withdraw from the study at any time or to skip questions. Moreover, they were briefed that there will be no direct benefit or harm due to participation except taking some minutes for answering the questions. The participants were also informed that the information obtained from them will be kept confidential and merely used for research purposes.
Results
Socio-Demographic Characteristics
Of 845 respondents recruited, 772 participated in the study yielding a response rate of 91.4%. The median age of the study participants was 25 (±10 IQR) years and more than half (58.4%) of the respondents were in the age group of less than 27 years. More than two-thirds (67.7%) and more than half (54.8%) of the respondents were males and protestant religion followers, respectively. More than half (59.6%) and about three-fourths (75.5%) of the respondents had Majang ethnicity and rural residence, respectively (Table 1).
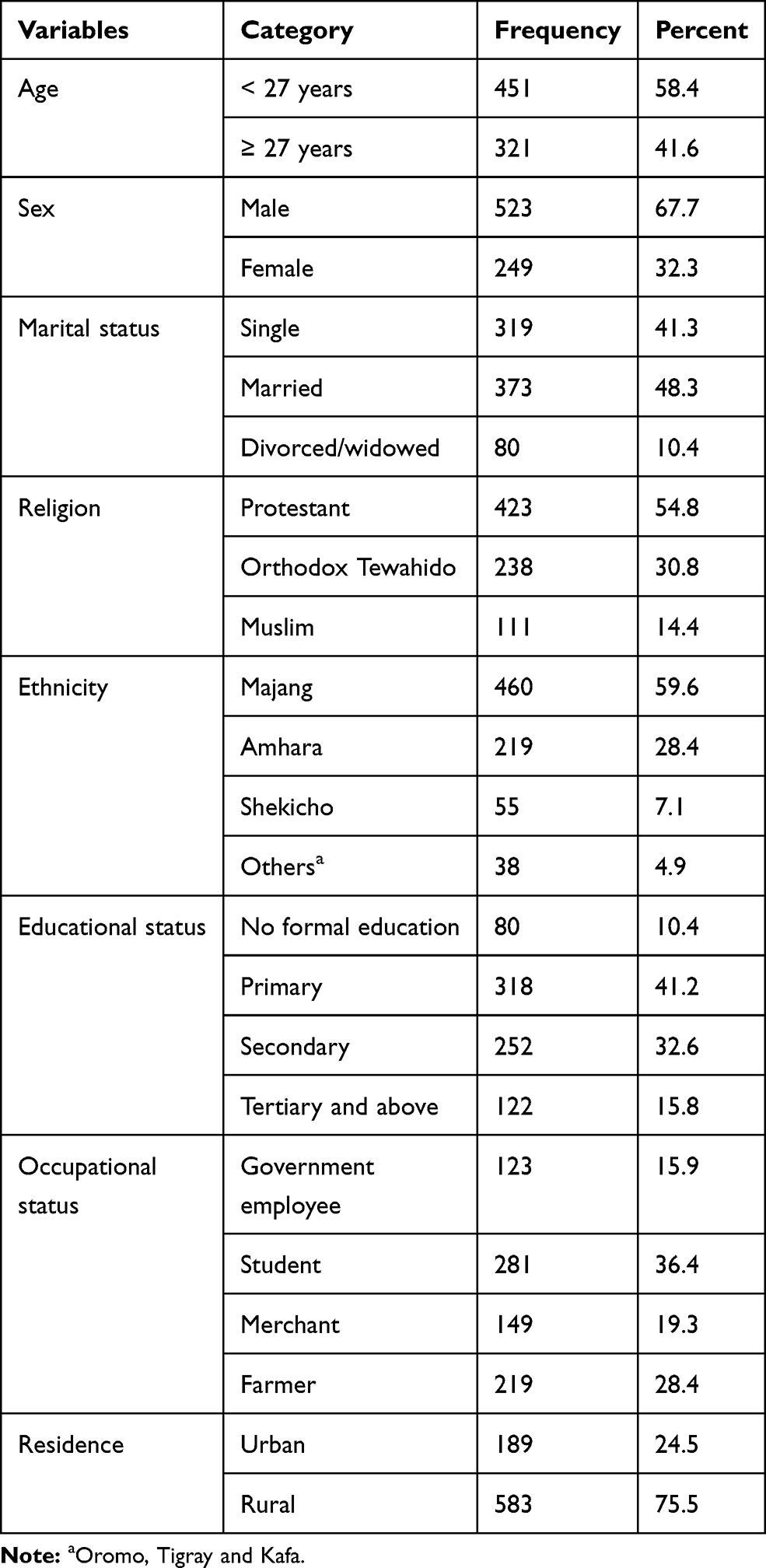 |
Table 1 Socio-Demographic Characteristics of the Respondents at Majang Zone, Southwest Ethiopia, 2019 |
Behavioral and Related Characteristics
More than a fourth (27.8%) of the respondents were alcohol drinkers. Of these more than half (58.1%) drink before sexual intercourse and one-third (33%) drink two to three times a week. Regarding chat chewing, more than three-fourths (77.2%) were not chewers (Table 2).
 |
Table 2 Behavioral and Related Characteristics of the Study Participants in Majang Zone, Southwest Ethiopia, 2019 |
Knowledge About HIV and Its Prevention Methods
Almost all (99.2%) and a very high proportion (98.1%) of the respondents had ever heard about HIV and think that HIV is preventable, respectively. Not sharing contaminated sharp materials (63.4%), consistent condom use (61.2%), and abstinence (57.9%) were the prevention methods mentioned by the majority of the respondents. The mean knowledge score of the study participants was 10.8 (±2.9 SD). In general, among the respondents, only 39.6% had good knowledge of HIV prevention methods (Tables 3 and 4).
 |
Table 3 Knowledge of Participants Regarding HIV Prevention Methods in Majang Zone, Southwest Ethiopia, 2019 |
 |
Table 4 Prevention Methods Mentioned by the Study Participants, Majang Zone, Southwest Ethiopia, 2019 |
Source of Information About HIV and Its Prevention Methods
Health professionals (92.6%) and faith-based organizations (39.9%) were the sources of information about HIV and its prevention methods for the majority of the study participants (Table 5).
 |
Table 5 Source of Information About HIV Prevention Methods as Mentioned by Respondents (n=757) |
Factors Associated with Knowledge of HIV Prevention Methods
The factors that were a candidate for multivariable logistic regression include sex, age group, educational status, and attitude towards HIV prevention method. In multivariable logistic regression the independent determinants of knowledge of HIV prevention methods were secondary educational status (AOR=1.84; 95% CI=1.04, 3.24), tertiary and above educational status (AOR=2.01; 95% CI=1.07, 3.75) and attitude towards HIV prevention methods (AOR=1.89; 95% CI=1.39, 2.57) (Table 6).
 |
Table 6 Bivariable and Multivariable Logistic Regression for Factors Affecting Knowledge of the Community Regarding HIV Prevention Methods in Majang Zone, Southwest Ethiopia, 2019 |
Attitude Towards HIV Prevention Methods
Among the total participants, 82 (10.6%) responded that they will not give a care if one of their family members has HIV. Similarly, half [385 (50%)] of the respondents reported that they will not keep the secret if a family member is infected with HIV. Moreover, 161 (20.9%) said that they will not buy food from a vendor who is living with HIV. A significant proportion [314 (40.7%)] of the participants agreed that sexual intercourse should only take place between married couples. About one-third of the participants [240 (31.1%)] replied that it is ashamed to buy or ask for condoms. The mean attitude score towards HIV preventive behavior was 35.3 (± 4.2 SD). More than half [412 (53.4%)] of the respondents had a positive attitude towards HIV prevention methods and 360 (46.6%) had negative attitudes.
Factors Associated with the Attitude of HIV Prevention Methods
At bivariable analysis, age group, marital status, occupational status, alcohol drinking, chat chewing, and knowledge of HIV prevention methods were statistically associated with a positive attitude towards HIV prevention methods and finally, age group (AOR=2.13; 95% CI=1.55, 2.95), and knowledge of HIV prevention methods (AOR=1.83; 95% CI=1.35, 2.48) were found to be significantly associated with a positive attitude towards HIV prevention methods (Table 7).
 |
Table 7 Factors Associated with the Attitude Towards HIV Prevention Methods in the Majang Zone, Southwest Ethiopia, 2019 |
Discussion
Knowledge of HIV prevention is a key to the successful prevention of HIV/AIDS. In this study, although a high proportion of the respondents had ever heard about HIV and think that HIV is preventable, only about 40% of respondents had good knowledge about HIV prevention methods and this is comparable with the finding of a study conducted in Peru where 41.5% of respondents had good knowledge about HIV prevention practices.10 This is a shocking figure and it can be considered as a ringing bell regarding the speed of progress towards ending the AIDS epidemic.4
Higher educational levels (secondary and, tertiary and above) were significantly associated with good knowledge in our study. The finding of a study conducted in Peru revealed a similar conclusion, where there was direct proportionality between the overall level of knowledge and educational level.10 This might be due to that individuals with higher educational levels will have a higher probability of getting information about HIV prevention methods from different sources and their ability to analyze the information they get. Similarly, the Ecuadorian study showed that participants with a higher level of education had good knowledge compared to those with primary education.11 The strength of the association is a bit higher compared to our finding and the difference might be attributable to the population difference between the Ecuadorian study and our study.
In the current study, a positive attitude was significantly associated with good knowledge. If peoples have a positive attitude towards HIV prevention methods, they may investigate them more and they will have good knowledge. Scholars recommend that for an individual to be successful and to have a better understanding of the issue, he/she should have a positive attitude about the issue.12
Regarding the attitude of the participants, half of them reported that they will not keep the secret of their HIV-positive family members. In addition, a considerable proportion of the respondents responded that they will not give a care if one of their family members has HIV and they will not buy food from a vendor who is living with HIV. These are supported by the finding from a countrywide survey and these findings support the continuity of discriminatory attitudes against HIV patients in Ethiopia still now.13 A significant proportion of the participants agreed that sexual intercourse should only take place between married couples. This is very important to prevent HIV by encouraging abstinence which is among the prevention methods mentioned by more than half of the respondents in the current study. Abstinence is among the highly promoted and effective HIV preventive behaviors considering its role in reducing the risk of other sexually transmitted infections and the crisis of premarital sexual intercourse.14–17 The overall magnitude of positive attitude towards HIV prevention methods was found to be 53.4% and this is comparable with the findings of studies from Goba and Hawassa towns.18,19
Respondents with the age of 27 years and above had 2 times increased odds of having a positive attitude towards HIV prevention methods. This may be explained in that an increase in age can be associated with increased knowledge about HIV and its prevention methods, which resulted in developing a positive attitude towards HIV prevention methods. Supporting this, the knowledge status was also significantly associated with attitude in our study. This finding was inconsistent with a study conducted in Brazil which revealed that there was no association between age and HIV preventive behavior.20 The discrepancy might be attributable to the difference in socio-demographic characteristics.
Knowledge plays a vital role in different action since it guides the underlying attitude of the behavior.21 In this study, respondents with good knowledge about HIV preventive behavior had two times increased odds of having a positive attitude towards HIV prevention methods. The more they know about the prevention, the better to develop a positive attitude towards HIV preventive behavior. This finding was supported by a study conducted in Cameroon which reported that respondents with medium and high levels of knowledge were more likely to display positive attitudes.22
Conclusion
This study revealed insufficient knowledge and attitude about HIV prevention methods among the community with the highest HIV prevalence. There were suggestive findings for the existence of discriminatory attitudes in the study. To achieve the goal of ending the HIV epidemic health education should be considered using different innovative approaches and especially by prioritizing young individuals and those with less education. Abstinence is a highly promoted behavior in Ethiopians’ culture to reduce premarital sex and it was also mentioned by many respondents as one of the HIV prevention method. Using this opportunity, it is possible to improve the HIV prevention knowledge and attitude of people which in turn can reduce the HIV burden in the country.
Abbreviations
AIDS, acquired immunodeficiency syndrome; AOR, adjusted odds ratio; ART, anti-retro viral therapy; CI, confidence interval; COR, crude odds ratio; HIV, human immunodeficiency virus; IQR, interquartile range; SD, standard deviation; SPSS, Statistical Package for Social Sciences; UNAIDS, The Joint United Nations Programme on HIV/AIDS.
Acknowledgments
The authors would like to acknowledge the staffs of the Majang zone health department, the study participants, data collectors, and the supervisors for the valuable roles they played in this study.
Disclosure
The authors have declared that no competing interests exist.
References
1. UNAIDS. Global AIDS update [Internet]; 2020 [
2. Federal HIV/AIDS Prevention and Control Office. HIV Prevention in Ethiopia: National Road Map 2018–2020. 2018:1–43
3. PEPFAR Ethiopia. Ethiopia country/regional operational plan (COP/ROP) 2017 strategic direction summary [Internet]. Addis Ababa; 2017 [
4. UNAIDS. 90-90-90An ambitious treatment target to help end the AIDS epidemic [Internet]; 2014 [
5. UNAIDS. 2017 Global HIV statistics [Internet]; 2018 [
6. UNAIDS. Global AIDS update 2019 [Internet]; 2019 [
7. Svanemyr J. Experiences and perception of youths towards HIV/AIDS prevention campaigns in Kibera Slums: Nairobi Kenya (thesis) [Internet]. University of Oslo; 2007. Available from: https://www.duo.uio.no/bitstream/handle/10852/30152/OceanicxOballa.pdf?sequence=2&isAllowed=y.
8. Mekdim Ethiopia National Association. HIV/AIDS was responsible for 17,181 deaths in Ethiopia in 2017 [Internet]; 2019 [
9. Federal Democratic Republic of Ethiopia Central Statistical Agency. Population projection of Ethiopia for all regions at wereda level from 2014–2017; 2013. Available from: http://www.csa.gov.et/ehioinfo-internal%3Fdownload%3D724:population-projection-of-eth.
10. Ugarte-gil C, Ponce M, Zamudio C, Canaza L, Samalvides F, Seas C. Knowledge about HIV prevention and transmission among recently diagnosed tuberculosis patients: a cross sectional study. BMC Public Health. 2015;13(1237).
11. Cabezas MC, Fornasini M, Dardenne N, Borja T, Albert A. A cross-sectional study to assess knowledge about HIV/AIDS transmission and prevention measures in company workers in Ecuador. BMC Public Health. 2013;13(139). doi:10.1186/1471-2458-13-139
12. Lowe J. Attitude before knowledge [Internet]; 2015 [
13. Central Statistical Agency (CSA) [Ethiopia] and ICF. Ethiopia Demographic and Health Survey 2016. Addis Ababa, Ethiopia, and Rockville, Maryland, USA; 2016.
14. Paul C, Fitzjohn J, Eberhart-Phillips J, Herbison P, Dickson N. Sexual abstinence at age 21 in New Zealand: the importance of religion. Soc Sci Med. 2000;51(1):1–10. doi:10.1016/S0277-9536(99)00425-6
15. Oladepo O, Fayemi MM. Perceptions about sexual abstinence and knowledge of HIV/AIDS prevention among in-school adolescents in a western Nigerian city. BMC Public Health. 2011;11(1):1–10. doi:10.1186/1471-2458-11-304
16. Erwinsyah E, Demartoto A, Supriyadi S. Early marriage in Jebres sub district of Surakarta city. Int J Multicult Multireligious Understanding. 2018;5(2):336–344. doi:10.18415/ijmmu.v5i2.396
17. Arini DP, Mohammad S. Teenage crisis school for students who become pregnant before marriage: social sciences postgraduate international seminar (SSPIS) [Internet]. Ahmad Dahlan University; 2014. Available from: http://eprints.usm.my/37779/1/sspis_2014_ms149_-_154.pdf.
18. Mohammed AY. Knowledge, attitude and practice on HIV/AIDS prevention among batu terara preparatory school students in Goba Town, Bale Zone, Southeast Ethiopia. Prim Health Care Open Access. 2015;05(01):1–6.
19. Mekonnen M, Behailu T, Wakgari N. Knowledge, attitude, and practice regarding HIV/AIDS among people with disability in Hawassa City, Southern Ethiopia. Adv Public Health. 2018;1–7.
20. Fontes MB, Campos Crivelaro R, Scartezini AM, et al. Determinant factors of knowledge, attitudes and practices regarding STD/AIDS and viral hepatitis among youths aged 18 to 29 years in Brazil. Cien Saude Colet. 2014;22(4):1343–1352. doi:10.1590/1413-81232017224.12852015
21. Fabrigar LR, Petty RE, Smith SM, Stephen L, Crites J. Understanding knowledge effects on attitude-behavior consistency: the role of relevance, complexity, and amount of knowledge. J Pers Soc Psychol. 2006;90(4):556–577. doi:10.1037/0022-3514.90.4.556
22. Nubed CK, Akoachere J-FTK. Knowledge, attitudes and practices regarding HIV/AIDS among senior secondary school students in Fako Division, South West Region, Cameroon. BMC Public Health. 2016;16(1):847. doi:10.1186/s12889-016-3516-9
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.