")
Back to Journals » International Journal of Women's Health » Volume 15
Determinants of Menstrual Hygiene Among Adolescent School Girls in Indonesia
Authors Wihdaturrahmah, Chuemchit M
Received 12 December 2022
Accepted for publication 8 April 2023
Published 8 June 2023 Volume 2023:15 Pages 943—954
DOI https://doi.org/10.2147/IJWH.S400224
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Marleen van Gelder
Wihdaturrahmah,1 Montakarn Chuemchit1,2
1College of Public Health Sciences, Chulalongkorn University, Bangkok, Thailand; 2Excellent Center for Health and Social Sciences and Addiction Research, Chulalongkorn University, Bangkok, Thailand
Correspondence: Montakarn Chuemchit, College of Public Health Science, Chulalongkorn University, Bangkok, 10330, Thailand, Tel +66 898375096, Email [email protected]
Purpose: The aim of this study was to determine the prevalence of menstrual hygiene management (MHM) and its associated factors among adolescent girls in Tangerang District, Indonesia.
Methods: This study was a cross-sectional study of 409 female students aged 12– 15 years old from 3 junior high schools selected using multistage sampling. The data were collected through a self-reported questionnaire both online and offline that was administered from April to May 2022. Bivariate and multivariable analysis using binary logistic regression were performed to determine the factors and predictors between sociodemographic characteristics, menstruation variables, knowledge, attitude, enabling environment, and the practice on MHM.
Results: Our study revealed a prevalence of good MHM practices among 52.3% of students, as well as moderate knowledge (48.9%) and neutral attitudes (70.4%). With regard to water, sanitation, and hygiene (WASH) facilities at school, most girls reported access to hand washing soap, a hook, a mirror, and a covered bin, but at home, the least available facilities were a mirror and a covered bin. Significant predictors of healthy MHM practices were having reached grade 8 (AOR = 1.80, 95% CI = 1.10– 2.95), having ever received information about menstruation at school (AOR = 1.95, 95% CI = 1.19– 3.18), having a positive attitude (AOR = 4.21, 95% CI = 1.78– 9.96), having access to a private home toilet (AOR = 2.71, 95% CI = 1.36– 5.42), and having a home toilet with a covered bin (AOR = 2.15, 95% CI = 1.38– 3.37).
Conclusion: The girls in this study showed a high prevalence of good MHM practices, but access to WASH facilities at school and at home was still a challenge. Positive attitude was the most significant factor associated with good MHM among female students. Therefore, we suggest establishing menstruation-focused education related to attitudes, particularly sociocultural norms, myths, and misconceptions and WASH facilities provided at home.
Keywords: attitude, female students, knowledge, menstrual hygiene management, practice
Introduction
According to the World Health Organization adolescents represent over 16% of the world’s population, around 1.2 billion. This is a stage of rapid physical, cognitive, and psychosocial growth, including, for adolescent girls, menstruation and the beginning of their reproductive years. The menstrual cycle starts at an average age of 12 years; however, it can begin as early as eight and as late as fifteen.1 Bacterial infections are riskier during menstruation, so correct genital hygiene is imperative for young women; however, many adolescent girls neglect menstrual hygiene management (MHM). Adequate MHM means access to clean material to absorb menstrual blood, privacy to change materials, access to soap and water to clean the body, and safe and convenient facilities to dispose of menstrual materials.2
MHM is an essential right for girls and women worldwide, and indeed aligns with a number of the United Nation’s (UN) Sustainable Development Goals, including good health and well-being (goal 3), quality education (goal 4), gender equality (goal 5), and clean water and sanitation (goal 6). Additionally, MHM requires four key environmental elements: social support, knowledge and skills, facilities and services, and materials,3 where adequate facilities mean access to water, sanitation, and hygiene (WASH) accommodations.4,5
According to Joint Monitoring Program for Water, Sanitation, and Hygiene Report 2020, globally, drinking water coverage reached nearly seven in ten schools, 16% had limited service, and one-fifth of schools had no source of water at all.6 Regarding sanitation, 63% of schools had access to basic sanitation services, but nearly 20% of schools had limited or even no sanitation services; additionally, 57% of schools had basic hygiene service (soap and water provided), almost 20% had limited services, and 25% had no WASH facilities at all.6 Meanwhile, in Indonesia specifically, most schools, 73%, did not have access to basic sanitation services, roughly 60% did not have access to hygiene services, and one out of three schools did not have sex-segregated toilets.7 That is, approximately 43.5 million students in Indonesia lacked access to proper WASH facilities.7
In one previous study in Tangerang District, almost 80% of junior high schools had toilet facilities, but most school toilets lacked complete WASH facilities, and nearly half of schools did not have trash bins for disposing of used menstruation materials.8 The lack of these facilities made it uncomfortable for menstruating girls to control their menstrual flow at school.9 Moreover, 38% of schools provided menstruation materials, but nearly two-thirds of students reported having to pay for supplies. Thus, because of the lack of available and affordable self-care materials, the young women in that study did not regularly change their sanitary napkins at school.8 It can also be remarked that the insufficiency of systems and supply chains for hygiene facilities are the greatest MHM challenges.10
Irrespective of individual school facilities, many adolescent girls can find it challenging to manage menstruation hygienically because social norms and cultural practices do not include giving girls accurate or complete information about MHM prior to menarche.11 Girls are thus left to learn about menstruation from their mothers or other female relatives who likely also were not properly informed, and unsanitary MHM practices persist for generations.12 In one study among high school students, most of the girls knew that menstruation is a natural physiological process for women even before menarche, but almost 90% of the students answered incorrectly when asked what organ menstrual blood came from. Inaccurate knowledge passed around among adolescent girls or passed down to them likely results in such misconceptions.13 Therefore, knowledge is one of the most powerful means of spreading the practice of safe and healthy menstrual hygiene and preventing the spread of diseases related to menstruation.14
Culture and religion have highly negative effect, with growing myths on managing menstrual hygiene and links to longstanding perception that restricts the practices.15,16 For instance, in one previous study in Indonesia, almost all respondents had misconceptions about foods that could not be consumed and physical activities that were considered dangerous during menstruation, and such beliefs have harmful impacts on girls’ health and school performance.17 Another challenge is access to menstrual hygiene materials, where pocket money is an important predictor to determine whether girls would have good menstrual hygiene management.18
It can be said that many young women around the world would benefit from better knowledge about proper MHM with the aim of improving positive attitudes toward managing menstruation and ultimately toward spreading safer and more hygienic practices. There has been no published research that elaborates on young women’s sociocultural knowledge, attitudes, and practices related to menstruation management including food and activity restrictions and enabling factors (WASH facilities at school and at home, availability and affordability of menstrual materials) specifically in the Tangerang District of Indonesia. Thus, we aimed with this study to assess the state of menstrual hygiene management including the associated factors among a population of adolescent girls in Tangerang District, Indonesia.
Materials and Methods
Study Design and Setting
We conducted this cross-sectional study from April to May 2022 in Tangerang District, Indonesia. According to the Public Health District Office, there are 544 junior high schools in the district. However, we conducted the study at three specific junior high schools that were known to have inadequate WASH facilities and that had not been the recipients of any hygiene-related interventions (such as baseline and endline study, capacity training for teachers, and health campaign) from UNICEF.19 The three schools were located in different subdistricts across Tangerang: in Cikupa, Solear, and Mauk. The study was approved by the school health program adviser and the water supply and sanitation working group of Tangerang District.
Sample Size and Sampling Procedure
The total study population was 1264 female students aged 12–15 who attended one of the selected schools during the study period. The girls were chosen because they mostly experienced menarche is 10–15 years old. We calculated the study sample size by estimating a finite population with the prevalence of MHM practice (P = 0.64) from a previous study conducted in Indonesia,20 which produced 354 students as the sample size. Adding 10% to account for missing or incomplete data gave a total sample size of 390 female students, and the participants were selected through multistage sampling. We selected schools and subdistricts via purposive sampling from schools that had not participated in a 2019 UNICEF study on MHM in the study area based on the schools’ hygiene practices and WASH facilities. The next step was selecting the students based on the inclusion and exclusion criteria. The inclusion criteria were female student who had reached menarche, used WhatsApp as it is the main media communication used to share the information, and understood the online questionnaire, and girls were excluded who did not obtain a signed parents’ approval letter. Lastly, we used convenience sampling and probability proportional to size to select the appropriate number of students for each school as follows: JHS A = 150; JHS B = 117; and JHS C = 123.
Ethical Considerations
The study received written approval from the Institutional Review Board of the Faculty of Medicine and Health at University of Muhammadiyah Jakarta (certificate no. 062/PE/KE/FKK-UMJ/IV/2022). We also obtained permission letters from the principal of each junior high school and the related authorities before we began the data collection. Regarding the informed consent in this study, the students obtained signed approval from their parents or guardians and also signed informed consent documents themselves before they received the questionnaires. The students were also informed that they could withdraw their participation at any time. The present study was also conducted in accordance with the Declaration of Helsinki.
Data Collection
We used a structured self-administered questionnaire to collect the data for this study. The survey was based on standardized questions from the WHO and UNICEF Joint Monitoring Program, various institutional sources, and literature review.2,3,11,20–27 The questionnaire were initially constructed in English and then translated into Indonesian. Three research assistants with public health background supported the questionnaire administration. They were trained on the study protocols, study objectives, and the content of questionnaires. The questionnaire was structured in six sections based on the study objectives. First section was sociodemographic characteristics, which included age, education grade, religion, parent’s educational level, household income, and pocket money. Second section gathered information about source of information and variable on menstruation including age of menarche, duration of menstruation, source of information, and ever having gotten information at school. Third section was on knowledge of MHM with some variables including menstruation definition, organ releasing the menstrual blood, duration and interval of menstruation, and menstrual hygiene. Fourth section was on attitude towards MHM, which consisted of opinion, beliefs, sociocultural, myth/misconception regarding MHM. Next section was on enabling factors, which included WASH facilities, availability, and affordability of menstrual materials. Last section solicited information on MHM practices focusing on menstrual hygiene-related questions, but it was not limited to the type of menstrual materials used, the changing pads frequency, how to dispose the pads, how to clean the genitalia, and bathing during menses. Prior to data collection, we had obtained the necessary permissions from the schools’ authorities, then we coordinated the three schools’ personnel to obtain the students’ personal data (name, age, grade, and contact). Students who returned a parent’s signed approval letter and signed the informed consent document received the link to the questionnaire along with explanations of some questions via WhatsApp. However, because of some obstacles, the data collection was executed only fully online by student at JHS B. The surveys were completed fully offline by student at JHS C, and students at JHS A completed their surveys partly online and partly offline. The principal investigator and the research assistants checked over the data during the data collection for completeness and consistency. Since the online form was used, the incomplete answer was not able to be submitted.
Data Analysis
In the first analysis step, the data were input into Google Forms and exported to Microsoft Excel. We then used SPSS Statistics 22 (IBM, USA) to clean and analyze the data. Descriptive analysis presented the categorical data as frequencies and percentages and presented the continuous data as mean, median, standard deviation, minimum and maximum, frequency, and percentage. The knowledge variable consisted of 20 questions with true/false/not sure response. The correct answer was scored one (1) point, while incorrect and not sure answer was scored zero (0) point. The Bloom’s cut-off point was used to categorize the knowledge score into low level (less than 12), moderate (12–15), and high (16–20). For attitude variable, it consisted of 32 questions, which were measured by using Likert’s scale with three ranges (agree, neither agree nor disagree, and disagree). The scores were calculated by using median cut off point (68.00±7.09) to categorize into negative, neutral, and positive attitudes. Meanwhile, the MHM practices were categorized into poor and good practice. To identify this, the respondents who used sanitary pads were considered to have good practice of MHM, while other kinds of materials used were considered to have poor practice. If the respondents change menstrual products more than 4 times every 3–4 hr in a day, it was said to be good practice. On disposing techniques and its place, wrapping the pads in plastic and disposed into trash bin were considered to be good practice. Respondents who washed their hands with water and soap before and after changing the pads were said to have good practice, while those who washed their hands using water were said to have poor MHM. The respondents who bathed and washed their hair during menses and cleaned genitalia using only water were included as having good practice. Bivariate and multivariable analysis using binary logistic regression were performed to obtain the significant associated independent variables (sociodemographic characteristics, sources of information and variables on menstruation, knowledge, attitude, and enabling factors) that predicted the dichotomous dependent variable: poor or good MHM practices with values given 0 and 1, respectively. The results were presented with crude odds ratios (CORs), adjusted odds ratios (AORs), and 95% confidence intervals (CIs).
Results
A total of 409 junior high school female students completed the questionnaires. The mean age (±SD) of the adolescent girls was 13.77 (±0.96) years. A plurality of the girls (135, 33%) were age 14 and in grades 8 or 9 (134, 32.8%), and Islam was by far the dominant religion (387, 94.6%). The mothers of over half of the respondents had low education levels, but their fathers’ education levels were fairly evenly split: high, 50.9% versus low, 49.1%. Over three-fifths of respondents had a low family income (less than 4.230.000 IDR [±293.76 USD]), but just about all respondents (98.5%) reported receiving pocket money from their parents (Table 1).
 |
Table 1 Sociodemographic Characteristics of Adolescent Girls in Tangerang District (n = 409) |
Most of the girls (84.8%) had reached menarche between ages 12 and 15, with a mean age of 12 at time of menarche, and almost 75% students had menstruated for 5–7 days. Nearly 85% of students had ever been told about menstruation before menarche, and most girls (40.7%) reported their mothers as their main source of information about menstruation. However, 77% of the girls reported having ever gotten information about menstruation at school (Table 2).
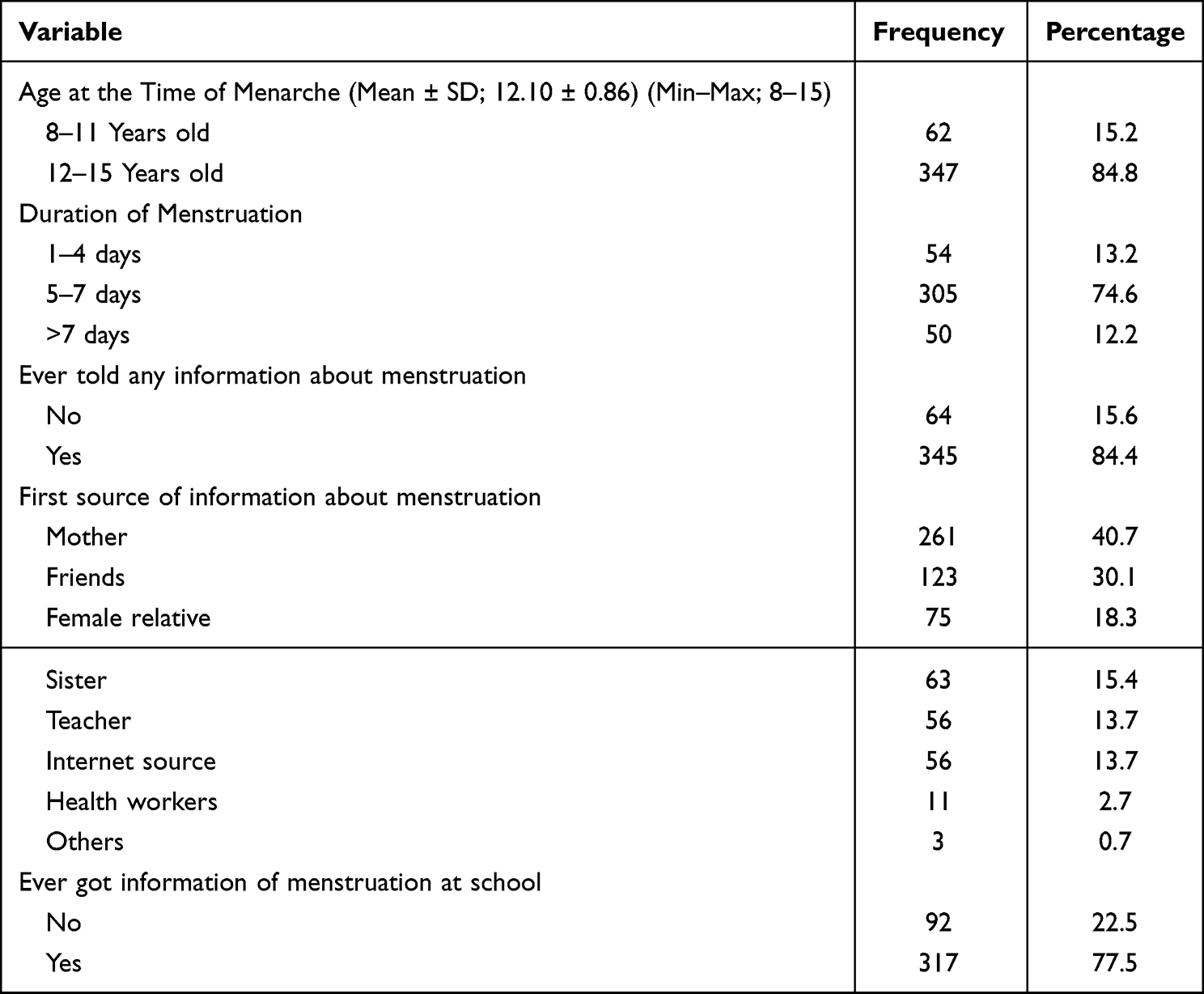 |
Table 2 Menstruation Variables Among Adolescent Girls in Tangerang District (n = 409) |
Among 409 junior high school female students aged 12–15 years who participated in this study, we identified good MHM practices in 52.3%, just over half. Nearly half of the girls had moderate knowledge about menstruation, and approximately 70% of them had neutral attitudes toward MHM practices (Table 3).
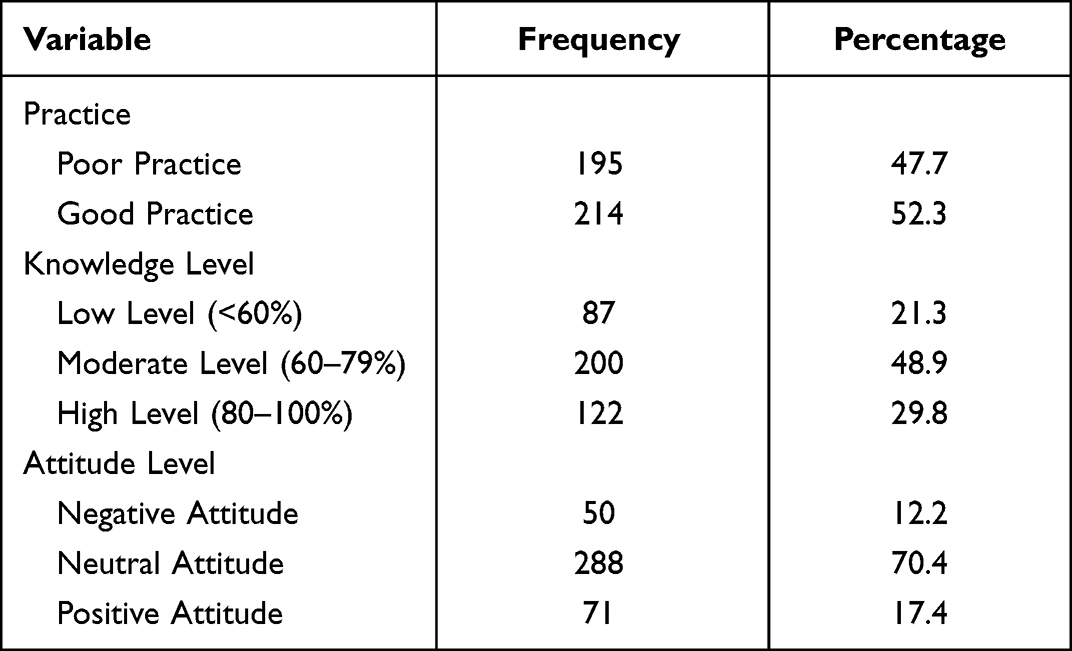 |
Table 3 Menstrual Hygiene Management Knowledge, Attitudes, and Practices Among Adolescent Girls in Tangerang District (n = 409) |
We considered three factors that enabled good MHM practices: WASH facilities at school and at home and available, affordable menstrual materials. From the survey, the girls reported that most of the schools had separate toilet facilities for male and female students, but only around 60% of the students stated that their school toilet was private. Over half of students said the school toilet is clean, but more than three-fifth reported that the school did not provide hand washing soap. In addition, 75.1% and 87.5% of students, respectively, reported no hook or no mirror next to the toilet. In contrast, the girls reported considerably higher percentages of washing soap, hooks, and mirrors present at home than at school. Lastly, less than a third of students stated that the school provided a covered bin in the toilet, which was lower than the 70% of homes with a covered bin in the toilet (Table 4).
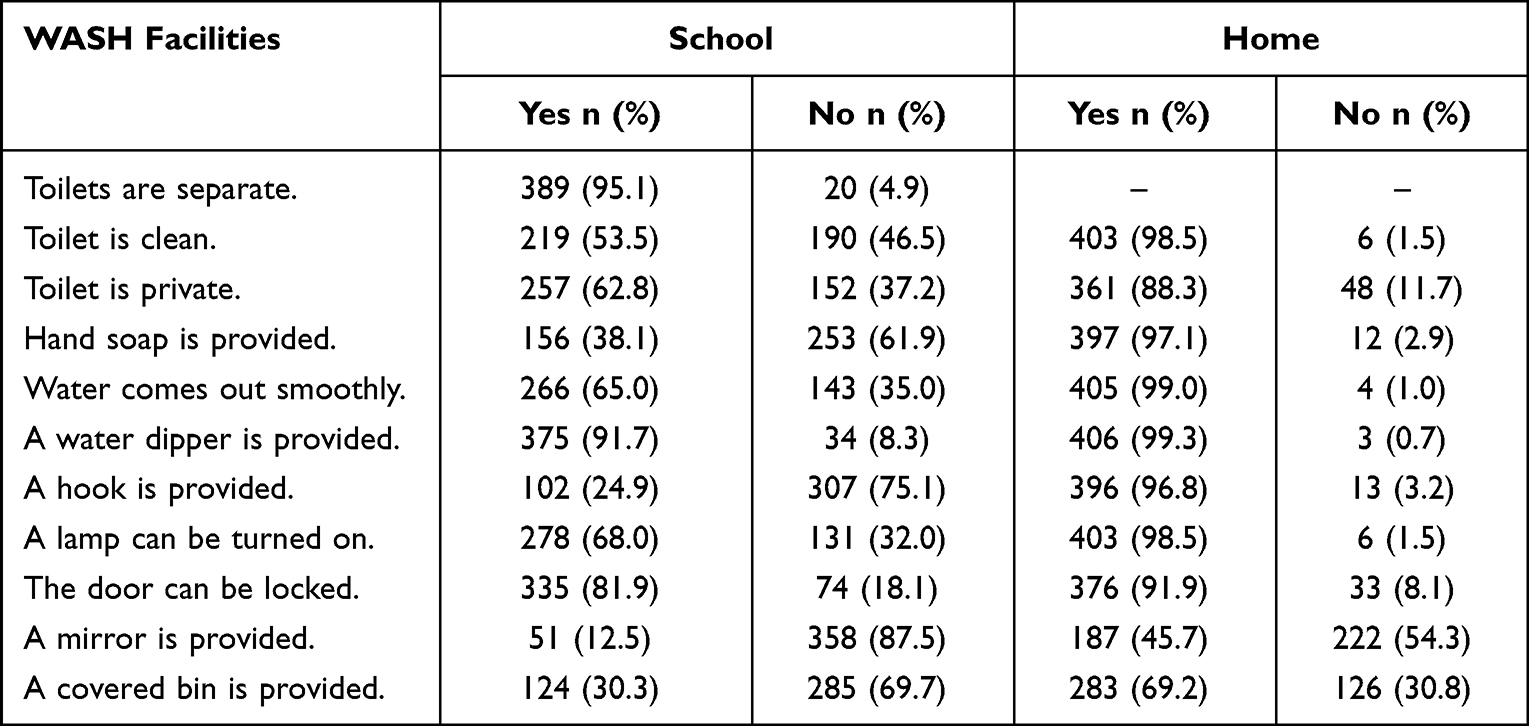 |
Table 4 WASH Facilities for Menstrual Hygiene Among Adolescent Girls in Tangerang District (n = 409) |
Nearly all of the girls, 90%, acquired their menstrual materials from their parents, which aligns with the fact that nearly 85% of the students reported no storage box for school-supplied sanitary napkins and that around 80% of students stated that commercial menstrual pads were not available at school. Over half of students purchased pads at school, but nearly all could afford to do so (Table 5).
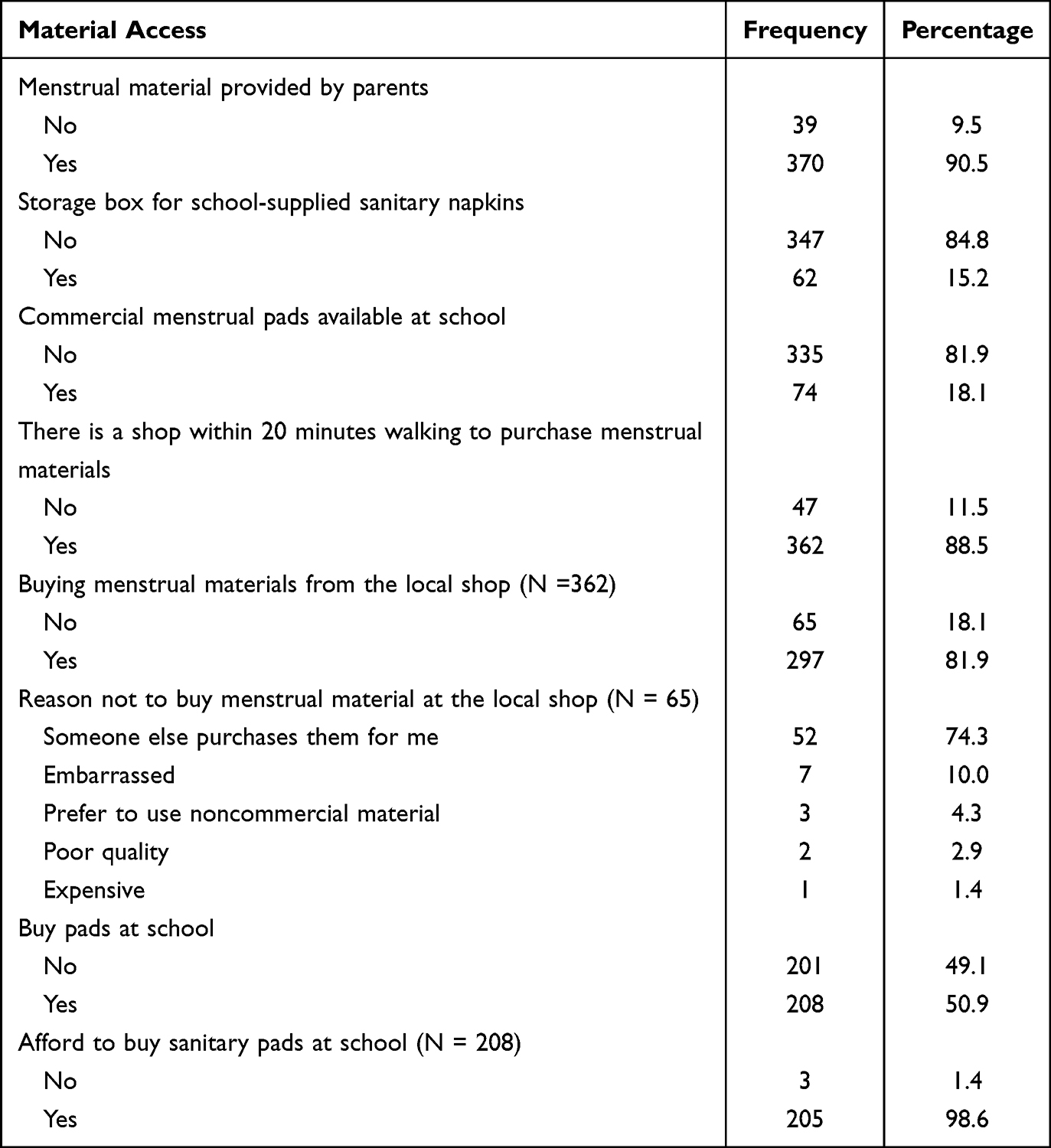 |
Table 5 Availability and Affordability of Menstrual Hygiene Materials Among Adolescent Girls in Tangerang District (n = 409) |
According to the multivariable analysis findings, school grade, having receiving information about menstruation at school, attitude, and two of the enabling factors (home toilet is private and home toilet has covered bin) maintained statistically significant associations with good MHM practices (P < 0.05 for all). The students in grade 8 were 1.8 times more likely to have good MHM practices than the students in grades 7 (95% CI = 1.10–2.95). The students who ever received information about menstruation at school were 1.95 times more likely to have good MHM practices than the students who did not (95% CI = 1.19–3.18). The students with positive attitudes were 4.21 times more likely to have good MHM practices than were students with a negative attitude (95% CI = 1.78–9.96). Students with private home toilets were 2.71 times more likely to have good MHM practices than were students with a shared home toilet (95% CI = 1.36–5.42). Finally, the students whose home toilet had a covered bin were 2.15 times more likely to have good MHM practices than were those whose toilets did not have a covered bin (95% CI = 1.38–3.37) (Table 6).
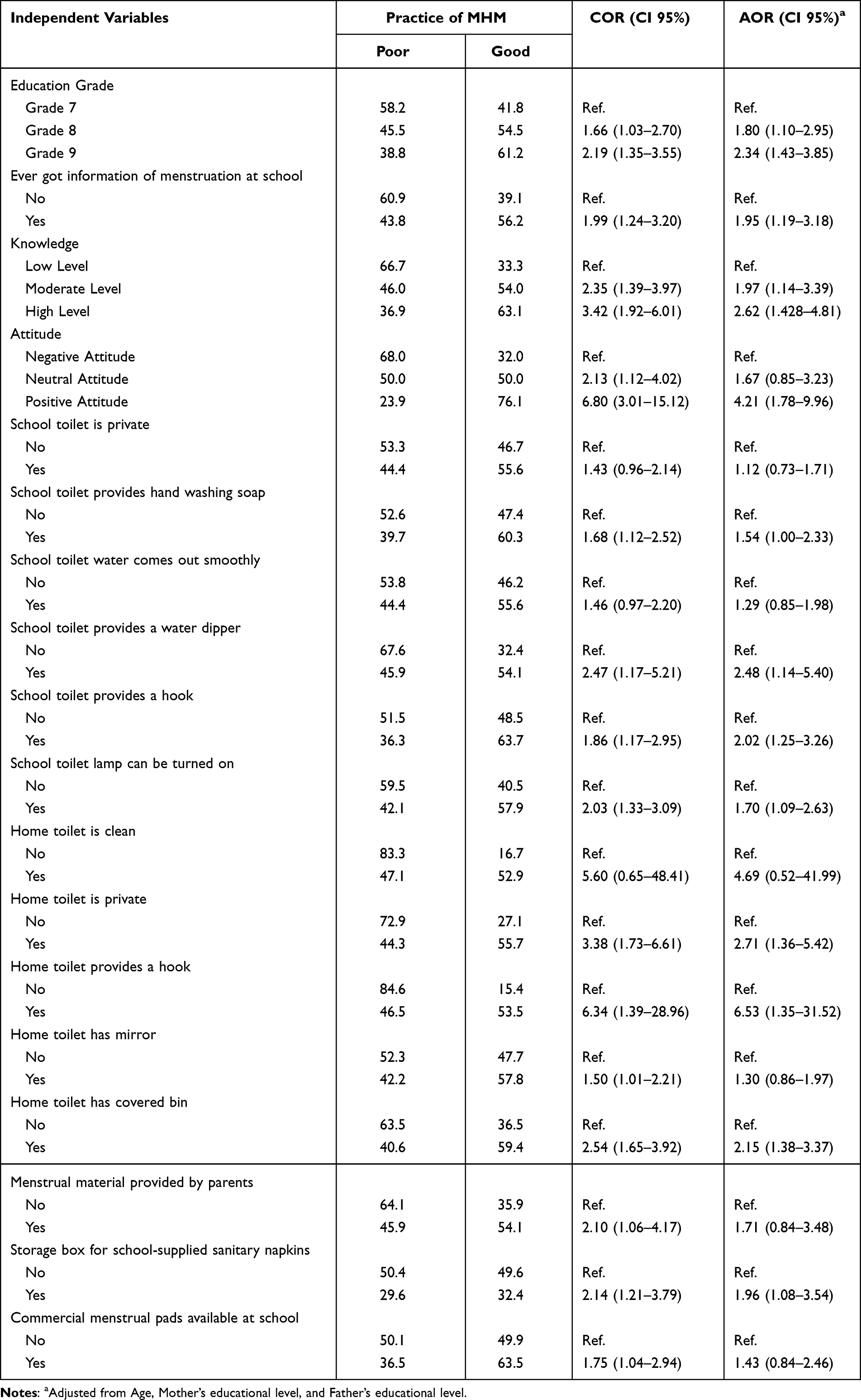 |
Table 6 Predictors of Menstrual Hygiene Among Adolescent Girls in Tangerang District (n = 409) |
Discussion
Among 409 junior high school female students aged 12–15 years old participating in this study, 52.3% of the girls reported good MHM practices on the self-reported questionnaire. This finding was quite lower than the finding of 61.4% prevalence of good menstrual hygiene from a study in northern Ghana among junior high schools.28 However, in a similar study conducted among junior high-school students in Makassar, Indonesia, the prevalence of good MHM practices was around 13% lower than the current finding.23 We suggest that one explanation for the difference between our study and that one was the differences in the students’ knowledge levels in the two studies: There were more girls with high levels of menstruation-related knowledge in this study than in the study in Makassar. Moreover, in that study, 30% more respondents reported low socioeconomic status than in our study, and 20% more respondents reported low maternal education levels than in this study.
In this study, the girls in grade 8 were statistically significantly more likely to practice good MHM than were the girls in grades 7 and 9, possibly because the eighth-grade girls had better knowledge about MHM. This finding aligns with the results from a study conducted in Bangladesh in which girls in grade 8 were more likely to perform well academically and in turn showed a higher likelihood of practicing good menstrual hygiene.29
Under 20% of the girls in this study had never been told anything about menstruation before the onset of menstruation, although mothers were the main source of menstruation information for 40% of the girls. This finding is similar to results from studies conducted in Indonesia, Myanmar, India, and Central Ethiopia,30–32 but in those studies, about 65% of students reported that their mothers had been their first sources of information about menstruation. A possible explanation for the discrepancy with our findings is the low education levels of the mothers in our study: 56.2% of our students reported low maternal education levels. With higher education levels, more mothers might become the most important source of information about menstruation for their daughters before menarche, which is supported by findings from a study in India.32
Additionally, 77% of the students in this study reported having ever received information about menstruation at school, and the students who had received information about menstruation at school were 1.9 times more likely to have good MHM practices than were the students who had not. This finding is consistent with results from a study in Ethiopia in which adolescent girls who received menstruation information at school were more likely to have good MHM practices.33,34 Meanwhile, girls in one study who did not receive any information at school before menarche were more likely to use unhygienic menstruation materials and to generally have unsanitary MHM practices.35 Some girls learn about menstruation somewhat indirectly, from science classes, physical and health education, and religious education, which discuss basic genital hygiene and the biological mechanism of menstruation.17 Having been exposed to information related to MHM and sexual and reproductive health then enhances these girls’ knowledge and confidence once it is time for them to manage their own menstrual hygiene.17,26,36 Notwithstanding these findings, we did find that 45% of the girls who received information about menstruation from school also showed poor MHM practices. This could have been because teachers themselves are not adequately prepared to discuss menstruation and MHM and school curricula do not incorporate the subject at all, which was one of the conclusions in a previous study conducted in Indonesia.17
Our study finding that attitude toward menstruation was significantly associated with the practice of MHM was consistent with other studies.21,30,31 Only 17% of the adolescent girls in our study reported positive attitudes toward menstruation, but, interestingly, we found similar proportions of poor and good MHM practices in the group of girls who had neutral attitudes toward menstruation. The percentage of positive attitudes in this study is slightly higher than the finding from a study conducted in northern Ghana,11 but in research in Nepal, roughly half of the adolescent girls had positive attitudes toward menstruation, markedly higher than our finding.37,38 A possible explanation is that most of the students in this study had only moderate knowledge about menstruation, which aligned with the 70% of students who also had neutral attitudes toward menstruation. These findings contrast with an earlier finding that attitude was significantly associated with knowledge such that adolescents who had more knowledge had more positive attitudes than those of adolescents who had less knowledge.39
Separately, we found that students whose home toilet was private were 2.7 times more likely to have good MHM practices than were students whose toilets were not private; similarly, students whose home toilet had a covered bin were 2.1 times more likely to have good MHM practices. About 12% of students reported that the toilet is not private at home and specifically that the toilet area was designed for the needs of the male members of the household, so that it was difficult for girls to practice safe MHM in clean and private facilities. In Indonesia, the men in the household do not engage in any efforts to support menstruation and never discuss the subject with any women in the household.40 Another possible reason for poor MHM practices at home is fear of being teased: In our study, 84 students reported having ever been teased about being on their period, and among those girls, 21 students had been teased by their family members. In brief, we identified—but did not elaborate on—a general lack of privacy at home for some of the girls in our study. This topic warrants a more in-depth study given the UNICEF guideline that privacy as a concept can be subjective and difficult to define.
Conclusion
With this study, we identified a rather high prevalence of healthy MHM practices among 409 adolescent girls in Tangerang District in Indonesia. The factors that affected the girls’ MHM practices were school grade, attitude toward menstruation, having ever received information on menstruation at school, and having a home toilet that was private and had a covered bin. Of these, attitude was the most significant factor: Adolescent girls in this study who reported positive attitudes toward menstruation also showed good menstrual hygiene practices. Therefore, we strongly suggest incorporating reproductive health education into school curricula, specifically sociocultural norms, myths and misconceptions, and general beliefs. Collaborative support from the health, education, and family sectors should establish adequate menstrual hygiene facilities that encourage young women to have healthy and safe menstrual hygiene practices.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Crawford BJ, Waldman EG. Period Poverty in a Pandemic: Harnessing Law to Achieve Menstrual Equity. Washington University Law Review, Forthcoming; 2020.
2. UNICEF. Guidance on Menstrual Health and Hygiene. UNICEF; 2019.
3. UNICEF. Guidance for Monitoring Menstrual Health and Hygiene (Version I). UNICEF; 2020.
4. Notoatmodjo S. Promosi Kesehatan Dan Perilaku Kesehatan. Rineka Cipta; 2012.
5. UNICEF. Strategy for Water, Sanitation and Hygiene 2016–2030. UNICEF; 2016.
6. World Health Organization. Progress on Drinking Water, Sanitation, and Hygiene in Schools: Special Focus on COVID-19. World Health Organization; 2020.
7. KEMENDIKBUD. Profil Sanitasi Sekolah [School Sanitation profile]; 2020. Available from: http://repositori.kemdikbud.go.id/22134/1/isi_FD54325B-2BC7-476F-8EDD-615705C2D5DE_.pdf.
8. Myriad. Manajemen Kebersihan Menstruasi Di Sekolah Menengah Pertama Dan Madrasah Tsanawiyah Di Kabupaten Tangerang Tahun 2019 [Management of Menstrual Hygiene in Junior High Schools and Madrasah Tsanawiyah in Tangerang Regency in 2019]. Myriad; 2019.
9. Asumah MN, Abubakari A, Gariba A. Schools preparedness for menstrual hygiene management: a descriptive cross-sectional study in the West Gonja Municipality, Savannah Region of Ghana. BMJ Open. 2022;12(4):e056526. doi:10.1136/bmjopen-2021-056526
10. Keatman T, Cavill S, Mahon T Menstrual Hygiene Management in Schools in South Asia. Synthesis Report; 2017.
11. Boakye-Yiadom A, Aladago DA, Beweleyir J, Mohammed HB, Salifu MF, Asaarik M. Assessing the knowledge, attitude and practice of menstrual hygiene management among junior high schools adolescent females in the Yendi Municipality in the Northern region of Ghana. ESJ. 2018;14:467. doi:10.19044/esj.2018.v14n36p467
12. Chandra-Mouli V, Patel SV. Mapping the knowledge and understanding of menarche, menstrual hygiene and menstrual health among adolescent girls in low-and middle-income countries. In: The Palgrave Handbook of Critical Menstruation Studies. Springer; 2020:609–636.
13. Mohammed S, Larsen-Reindorf RE. Menstrual knowledge, sociocultural restrictions, and barriers to menstrual hygiene management in Ghana: evidence from a multi-method survey among adolescent schoolgirls and schoolboys. PLoS One. 2020;15(10):e0241106. doi:10.1371/journal.pone.0241106
14. Dasgupta A, Sarkar M. Menstrual hygiene: how hygienic is the adolescent girl? Indian J Community Med. 2008;33(2):77. doi:10.4103/0970-0218.40872
15. Asumah MN, Abubakari A, Aninanya GA, Salisu WJ. Perceived factors influencing menstrual hygiene management among adolescent girls: a qualitative study in the West Gonja Municipality of the Savannah Region, Ghana. Pan Afr Med J. 2022;41:146. doi:10.11604/pamj.2022.41.146.33492
16. Maulingin-Gumbaketi E, Larkins S, Whittaker M, Rembeck G, Gunnarsson R, Redman-MacLaren M. Socio-cultural implications for women’s menstrual health in the Pacific Island Countries and Territories (PICTs): a scoping review. Reprod Health. 2022;19(1):128. doi:10.1186/s12978-022-01398-7
17. SMERU. Menstrual Hygiene Management (MHM): A Case Study of Primary and Junior High School Students in Indonesia. SMERU; 2019.
18. Asumah MN, Abubakari A, Aninanya GA. Determinants of menstrual hygiene management practices among schoolgirls: a cross-sectional study in the Savannah Region of Ghana. Infect Dis Obstet Gynecol. 2022;2022:1–10. doi:10.1155/2022/7007117
19. Profil Kesehatan Kabupaten Tangerang [Tangerang District Health Profile]; 2020.
20. Davis J, Macintyre A, Odagiri M, et al. Menstrual hygiene management and school absenteeism among adolescent students in Indonesia: evidence from a cross-sectional school-based survey. Trop Med Int Health. 2018;23(12):1350–1363. doi:10.1111/tmi.13159
21. Amanda D, Ariyanti F. Perilaku menstrual hygiene remaja: studi pada santriwati di pondok pesantren modern kota depok [Adolescent menstrual hygiene behavior: a study of female students at a modern Islamic boarding school in Depok]. J Publikasi Kesehat Masy Indones. 2020;7(2):1.
22. Caruso BA, Salinger A, Patrick M, Conrad A, Sinharoy S A review of measures and indicators for gender in WASH; 2021.
23. Hadi EN, Atiqa UD. Menstrual hygiene management of junior high school students in rural areas of Indonesia (study in Tinambung Sub-District, Polewali Mandar, West Sulawesi). J Int Dent Medical Res. 2021;14(3):1230–1235.
24. Hennegan J, Nansubuga A, Akullo A, Smith C, Schwab KJ. The Menstrual Practices Questionnaire (MPQ): development, elaboration, and implications for future research. Glob Health Action. 2020;13(1):1829402. doi:10.1080/16549716.2020.1829402
25. House SM, Therese C. Menstrual Hygiene Matters. WaterAid; 2012.
26. Kennedy E. Menstrual Hygiene Management in Indonesia: Understanding Practices, Determinants and Impacts Among Adolescent School Girls. Melbourne: Burnet Institute; 2015.
27. UNICEF. Menstrual Hygiene Management of Adolescent School Girls and Nuns: Knowledge, Attitude, and Practices Study in Bhutan. UNICEF; 2018.
28. Kumbeni MT, Otupiri E, Ziba FA. Menstrual hygiene among adolescent girls in junior high schools in rural northern Ghana. Pan Afr Med J. 2020;37:190. doi:10.11604/pamj.2020.37.190.19015
29. Ahmed MS, Yunus FM, Hossain MB, Sarker KK, Khan S. Association between menstrual hygiene management and school performance among the school-going girls in rural Bangladesh. Adolescents. 2021;1(3):335–347. doi:10.3390/adolescents1030025
30. Balqis M, Arya IFD, Ritonga MNA. Knowledge, attitude and practice of menstrual hygiene among high schools students in Jatinangor. Althea Med J. 2016;3(2):230–238. doi:10.15850/amj.v3n2.783
31. Htun NN, Laosee O, Rattanapan C. Factors that influence menstrual hygiene management in adolescent girls in Mudon Township, Mon State, Myanmar. J Health Sci Res. 2021;39(3):207–217.
32. Thakre SB, Thakre SS, Reddy M, Rathi N, Pathak K, Ughade S. Menstrual hygiene: knowledge and practice among adolescent school girls of Saoner, Nagpur district. J Clin Diagn Res. 2011;5(5):1027–1033.
33. Bulto GA. Knowledge on menstruation and practice of menstrual hygiene management among school adolescent girls in Central Ethiopia: a cross-sectional study. Risk Manag Healthc Policy. 2021;14:911–923. doi:10.2147/RMHP.S296670
34. Gultie TK. Practice of menstrual hygiene and associated factors among female Mehalmeda high school students in Amhara Regional State, Ethiopia. Sci J Public Health. 2014;2(3):189–195. doi:10.11648/j.sjph.20140203.18
35. Aniebue UU, Aniebue PN, Nwankwo TO. The impact of pre-menarcheal training on menstrual practices and hygiene of Nigerian school girls. Pan Afr Med J. 2009;2:9.
36. Shibeshi BY, Emiru AA, Asresie MB. Disparities in menstrual hygiene management between urban and rural schoolgirls in Northeast, Ethiopia. PLoS One. 2021;16(9):e0257853. doi:10.1371/journal.pone.0257853
37. Belbase D, Basnet A, Panthi MP, Gautam K, Aryal R. knowledge attitude and practices of menstrual hygiene among rural adolescent school girls of Kapilvastu District, Nepal. Int J Collab Res Intern Med Public Health. 2021;2(2):1.
38. Yadav RN, Joshi S, Poudel R, Pandeya P. Knowledge, attitude, and practice on menstrual hygiene management among school adolescents. J Nepal Health Res Counc. 2017;15(3):212–216. doi:10.3126/jnhrc.v15i3.18842
39. Srinivasan D, Agrawal T, Attokaran T, Fathima FN, Johnson AR. Awareness, perceptions and practices regarding menstruation and menstrual hygiene among students of a college in Bengaluru Urban district, South India: a cross sectional study. Int J Community Med Public Health. 2019;6(3):1126–1132. doi:10.18203/2394-6040.ijcmph20190597
40. O’Reilly K, Louis E. The toilet tripod: understanding successful sanitation in rural India. Health Place. 2014;29:43–51. doi:10.1016/j.healthplace.2014.05.007
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.