Back to Journals » Patient Preference and Adherence » Volume 17
Determinants of Medication Non-Adherence Among the Elderly with Co-Existing Hypertension and Type 2 Diabetes Mellitus in Rural Areas of Udupi District in Karnataka, India
Authors K J ![]() , Rao M, YN S, Thunga G, N R, Sudhakar C, Sanatombi Devi E
, Rao M, YN S, Thunga G, N R, Sudhakar C, Sanatombi Devi E
Received 27 January 2023
Accepted for publication 8 June 2023
Published 13 July 2023 Volume 2023:17 Pages 1641—1656
DOI https://doi.org/10.2147/PPA.S380784
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Professor Qizhi (Cathy) Yao
Jeyalakshmi K,1 Mahadev Rao,2 Shashidhara YN,1 Girish Thunga,2 Ravishankar N,3 Christopher Sudhakar,4 Elsa Sanatombi Devi5
1Department of Community Health Nursing, Manipal College of Nursing, Manipal Academy of Higher Education, Manipal, Karnataka, India; 2Department of Pharmacy Practice, Manipal College of Pharmaceutical Sciences, Manipal Academy of Higher Education, Manipal, Karnataka, India; 3Department of Biostatistics, Vallabhbhai Patel Chest Institute, University of Delhi, Delhi, India; 4Department of Mental Health Nursing & Director - Quality, Manipal Academy of Higher Education, Manipal, Karnataka, India; 5Department of Medical Surgical Nursing, Manipal College of Nursing, Manipal Academy of Higher Education, Manipal, Karnataka, India
Correspondence: Elsa Sanatombi Devi, Department of Medical Surgical Nursing, Manipal College of Nursing, Manipal Academy of Higher Education, Manipal, Karnataka, India, Tel +91 8310769938, Fax +91 820 292 2572, Email [email protected]
Purpose: Medication adherence is a crucial component in the management of elderly with co-morbid chronic conditions. Hence, this study aimed to investigate the determinants of medication non-adherence among rural elderly with co-morbid chronic conditions of hypertension (HTN) and type 2 diabetes mellitus (T2DM) in India.
Patients and Methods: This cross-sectional study adopted the probability proportional to size (PPS) sampling technique to find the determinants of medication non-adherence among elderly residing in rural coverage areas of five randomly selected primary health centres (PHC) in Udupi district, Karnataka, India. A total of 360 elderly (72 samples from each cluster) who met the inclusion criteria and consented were interviewed using predesigned prevalidated and standardized or reliable tools. The data were coded and entered in SPSS version 16.0 and analyzed using both descriptive and inferential statistics.
Results: The study found that 55.6% (n=200) of rural elderly with co-morbid conditions HTN and T2DM were non-adherent to their medications and established Spearman correlation coefficient rank (r) value between undesirable person-related factors (r=− 0.444); good family support (including financial support) (r=0.185); poor accessibility to healthcare facility (r=− 0.209); detrimental medication-related factors including high cost of medication (r=− 0.237) were found to be significant at 0.05 level of confidence (p < 0.05). Further, the study depicted that the chi-square test (χ2) was identified to be significantly associated (p< 0.05) with a variable such as education, knowledge, number of illnesses and impairments, vision, memory, and physical impairments.
Conclusion: Medication adherence could be improved among rural elderly with co-morbid conditions by identifying and addressing the determinants at the earliest. Further, it is vital to identify the suitable intervention program to address these avoidable problems.
Keywords: drug compliance, factors, old age people, multiple chronic conditions
Introduction
Multiple chronic disease conditions are often called co-morbid chronic conditions or multi-morbidity and it has become common among young adults and elderly those who are receiving healthcare services at present days.1 Due to physiological changes among the elderly, they are more prone to get affected with multiple chronic disease conditions which may lead to frequent visits to hospital/doctors, and pharmacy than the younger population and it might subsequently result in polypharmacy.2–4
Co-existence of HTN and T2DM is very common across the globe and such combinations lead to a higher risk of getting cardiovascular and renal complications.5,6 Medication non-adherence or suboptimal adherence to the medications is a well-known factor that contributes to the poor control of blood pressure and glycaemic level.7,8
Medication adherence is a vital element in the treatment of many chronic illnesses to ensure therapeutic benefits for patients. However, it has always been a problem among people with medical illnesses, especially among the elderly.9 Suboptimal adherence to the medication might contribute to the occurrence of certain newer health problems or diseases, functional impairments, poor quality of life, frequent visits to the hospital and pharmacy, poor outcomes, and the increased average length of hospital stay, which further raises the overall healthcare, cost/expenditure, and service utilization.10–12
Medication adherence is complex, and the behaviour towards maintaining optimum adherence to the treatment regimen has been majorly influenced by the factors that are relating to healthcare providers, patients, the existing healthcare system, medication, and socioeconomic conditions.13–15 Person-related factors can be intentional or unintentional. Intentional behaviours are influenced by the patient’s level of satisfaction, beliefs, attitude towards the disease condition, adverse effects of medication, and expectations of improvement on health which results in an active decision to stop taking medication or modify the treatment regimen without the treating physician’s knowledge. Unintentional factors are such that influence the patients’ to possess inappropriate medication-taking behaviour due to their level of education and knowledge, diminishing cognitive ability, poor vision and hearing impairments, and other physical disabilities. Prescribing complex treatment regimens, lack of coordinated care among healthcare team members, and failing to establish a trustable relationship and good communication with the patients by the healthcare providers can lead to misunderstanding of treatment regimen and poor adherence to the medication. Unequal distribution of healthcare facilities in certain demographic areas can cause poor accessibility to the healthcare system which might further contribute to suboptimal treatment compliance by patients. The most significant medication-related factors are the cost, size, taste, and side effects of drugs. Reduced social and family support, financial constraints, and poor public transport facility are the socio-economic conditions that affect the medication adherence behaviour of a person.15–18
Medication adherence is an essential element of care for any group of patients, especially among older people as they are more vulnerable to following suboptimal adherence to the prescribed medications due to multi-morbidity, polypharmacy, and poor cognition which occur due to the physiological changes in their body.18–20 According to the evidence, medication non-adherence among elderly patients is more prevalent and the cost of medication, financial constraints, and beliefs in alternative therapies are the important factors to be considered while addressing this phenomenon.21–23
Multi-morbidity is also more prevalent among elderly residing in rural areas, and the overall prevalence of multi-morbidity was 48.8% which dyads (25%) being the most common form, followed by triads (15.2%) in India24 and they are more affected with the co-existence of HTN and diabetes mellitus.25 However, very few research studies have been conducted to explore the problems and factors associated with medication non-adherence among elderly with co-morbid chronic conditions in rural India. Hence, this unique study intended to investigate the determinants of medication non-adherence among rural elderly with co-morbid chronic conditions of HTN and T2DM in India with the view to develop a participant-tailored intervention program to manage their medications as non-adherence to the medication is believed to be the complex health behaviour with multifaceted determinants.26
Materials and Methods
Sample and Sampling Technique
The cross-sectional study was conducted from December 2019 to February 2021 using the Probability Proportional to Size (PPS) sampling technique. The study did not recruit the participants between April and August 2020 as there was a restriction from the institutional ethics committee to conduct the research studies due to the nationwide lockdown in India due to COVID spread. A total of 360 rural elderly with co-morbid HTN and diabetes mellitus were involved in the study. The sample size was calculated using a scientific method based on the pilot study report. The calculation was done to identify the probability of selection of each sampled cluster based on the primary survey report which was conducted by the investigators to identify the prevalence of elderly with co-morbid conditions of HTN and diabetes mellitus in rural coverage areas under seven selected PHCs in Udupi district, Karnataka, India.
As per Table 1, the clusters sampled for the study were the village coverage areas of selected PHCs which include Hirebettu (Cluster −1), Pernankila (Cluster −2), Kukkehalli and Peradoor (4), Kolalagiri (5), Pethri (6) and 72 individuals from five randomly selected clusters were sampled by using non–probability purposive sampling technique.
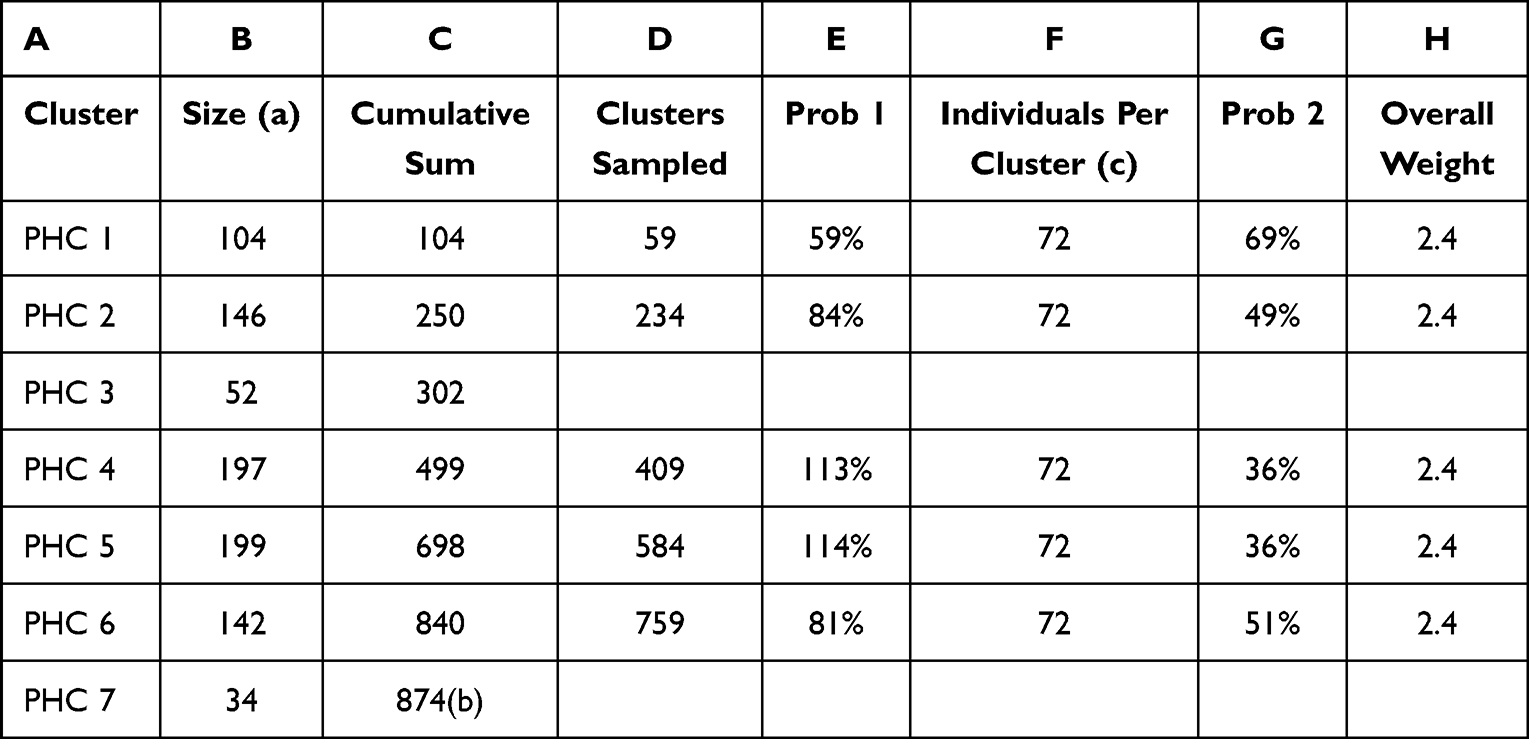 |
Table 1 Cal-Clusters Sampled (Probability of Selection for Each Sampled Cluster) |
Tools Used for the Study
Patient characteristics proforma is a tool which was used to understand the participants’ basic demographic and clinical proforma.
Hill-bone compliance scale was used to measure the medication non-adherence rate among elderly with co-morbid conditions of HTN and diabetes mellitus and it is a 14-items standardized tool for African American patients with high blood pressure. This tool was modified to the context for measuring the selected chronic conditions for the study after obtaining permission from the original author. The final modified scale had 9 items. Hence, the exact score of 9 is adherent and less than 9 is considered to be non-adherent. Reliability (r) of the original tool was 0.84 (n=341) and the reliability of the translated tool in the Kannada (official language of Karnataka state, India) version was (r=0.99; n=20) established in Indian settings before administering the questionnaire to the study participants.
Factors influencing medication adherence were assessed using a rating scale that consists of 25 items with three options such as “Always”, “Sometimes”, and “Never”. The determinants of medication adherence were grouped, and the final tool consists of four categories of factors which includes Undesirable person-related factors (Individual factors (9 items)), Good familial support including financial support (Familial factors (6 items)), Poor accessibility and availability of healthcare facility (Social factors (4 items)) and Detrimental medication-related factors including the high cost of medication (Medication-related factors (6 items)).
The person-related factors include the major elements of understanding the need/importance of taking regular medication/treatment, diet and exercise control, and nature of disease condition, forgetfulness, and unfavorable opinions about taking medication for their illness. Familial factors include the elements that are supportive (including financial support) to the patient to maintain compliance with their prescribed medication. Social factors focused on measuring the poor accessibility and availability of healthcare facilities. The medication-related factors assessed the detrimental elements, which include high cost of medication, side effects or adverse effects of the drug, disinclinations of taste and smell of drug, and polypharmacy that yielded to confusion about the medication regimen, time, and dose.
The positive items in the tools were scored as always −3; sometimes −2; never −1 and the negative items were scored in reverse order. This tool was developed by researchers based on an extensive literature review and reviewed by the subject experts. The translated tool in the Kannada (Local language) version was also tested for its reliability (r=0.74) before the administration to the study participants.
Ethical Consideration
The ethical clearance for the study was obtained (IEC Number: 487/2018) from the Institutional Ethical Committee of Kasturba Medical College and Kasturba Hospital, and the study was conducted following the Declaration of Helsinki. The study was also registered under the Clinical Trials Registry of India (CTRI Number: CTRI/2018/10/015962). The study included only the consented participants after signing an informed consent form.
Inclusion Criteria/Exclusion Criteria
The study included elderly aged 60 years and above residing in selected clusters and diagnosed and taking prescribed treatment for the co-morbid conditions of HTN and T2DM at least for 3 months based on the allopathic system of medicine.
The study excluded the elderly with chronic illnesses who had a previous experience of being part of any other project related to drug compliance and also elderly with any other major diagnosed co-morbid illness such as renal failure/kidney disease on dialysis treatment, and other illnesses such as cancer in any situ, TB, HIV/AIDS as their treatment regimen or strategies are varied and complex.
Data Collection
Administrative permissions were obtained from the District Health Office (DHO-Udupi district, Karnataka) and Medical Officer – In-charge from respective PHCs to gain co-operation to collect data from their rural coverage areas and to meet the elderly with co-morbid conditions of HTN and diabetes mellitus at their residential places or homes.
The pilot study was conducted on 40 elderly with co-morbid conditions of HTN and diabetes mellitus residing in selected clusters (eight samples from five village clusters), not involved in the study to understand the feasibility of using the methodology in the large-scale study. Data were obtained through a face-to-face interview by the primary investigator using standardized and pre-structured and pre-validated questionnaires after obtaining written informed consent from the elderly who met the inclusion sampling criteria. The quality of data was cross validated by other investigators of the study.
Precautionary Measures Taken to Prevent the Spread of COVID-19 During Data Collection
The study continued the data collection once the ethical committee permitted it to continue as per government guidelines. The strict adherence to the COVID appropriate behaviour such as wearing a mask, face shield, and hand gloves, social distancing, etc., was maintained, and the guidelines issued for conducting community-based research studies from the government of India were also followed throughout the study by the investigator.
The investigator was regularly screened in a phased manner for COVID and had an RT-PCR negative report before the interaction with the study participants. On the other hand, the study participants were screened for any COVID-like symptoms before the start of data collection. The elderly with co-morbid conditions who had symptoms and tested positive for COVID at the time of data collection were excluded from the study.
Analysis
The data were coded, entered, and analyzed by Statistical Package for the Social Sciences (SPSS) version 16. The entered data in SPSS were cross verified for their accuracy by performing a random check of the responses in the questionnaires and the data in the software.
Patient characteristics proforma and medication adherence scores of the elderly were analyzed using descriptive statistics and reported in terms of frequency (f) and percentage (%).
The Spearman correlation coefficient (r) test was chosen to compute the correlation between medication compliance and its influencing factors as the data were skewed. The chi square-test was computed to understand the association between the medication adherence and selected demographic variables, clinical variables, healthcare facility, medication-related variables, and knowledge variables to determine if a difference between these two data is due to chance or it is due to the relationship between the variables.
Results
The study included responses from all 360 participants and presented the findings below:
Sample Socio-Demographic Characteristics
The mean age of the study participants were 69 years (SD = 7.464) and almost 54.2% (195) of them were aged between 60 and 69 years; 61.9% (223) of them were female. Most of the participants were reported to have completed their primary (44.7% (161)) and secondary/higher secondary (29.7% (107)) school education. Two hundred and ninety-nine (83.1%) among 360 elderly participants were not employed and depended on their pension or family for their daily necessities including health and 185 (51.4%) elderly among 360 were the beneficiaries of various government pension schemes in India. For example, the Indira Gandhi National Widow Pension Scheme or Indira Gandhi National Old Age Pension Scheme and most (89.4% (322)) among them were receiving pensions lower than 1000 INR.
A limited amount of elderly with co-morbid illness are living alone (5.6% (20)) and with a spouse (17.2% (62)) and the remaining are residing with their family (278 (77.2%)). More than 60% of the study participants (230 (63.9%) have told that they belonged to below poverty line (BPL) card holders in India. Almost 61.9% (223) of the study participants were not enrolled in any insurance schemes. However, the remaining (137 (38.1%)) enrolled in one of the health insurance schemes that are available to them through private or government agencies including Ayushman Bharat, a newer initiative from the Government of India (Table 2).
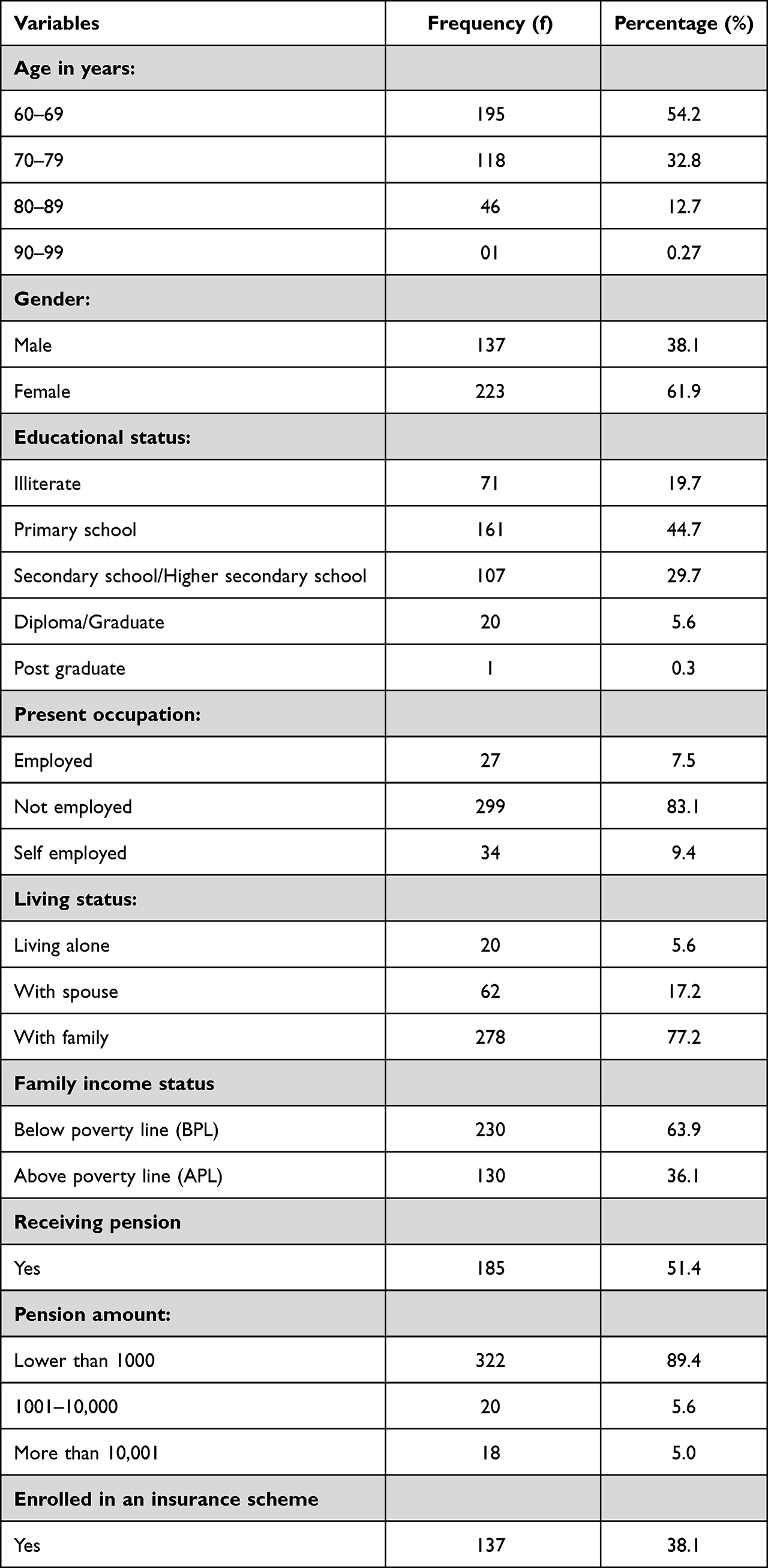 |
Table 2 Frequency and Percentage of Sample Socio-Demographic Characteristics (n=360) |
Prevalence of Medication Non-Adherence Among Elderly with Co-Morbid Chronic Illness
Among 360, more than 50% of the rural elderly (f=200; 55.6%) with co-morbid conditions of HTN and diabetes mellitus were non-adherent to their prescribed medications and the remaining 44.4% (f=157) of them were adherent to anti-hypertensive and anti-glycemic drugs.
Determinants of Medication Non-Adherence Among Elderly with Co-Morbid Chronic Illness
Relationship Between Medication Adherence with Its Influencing Factors
To find out the relationship between medication adherence and its influencing factors, the Spearman correlation coefficient (r) was chosen to perform as the data were skewed and it was computed between the exact score of medication compliance and its influencing factors, and the findings are presented in Table 3.
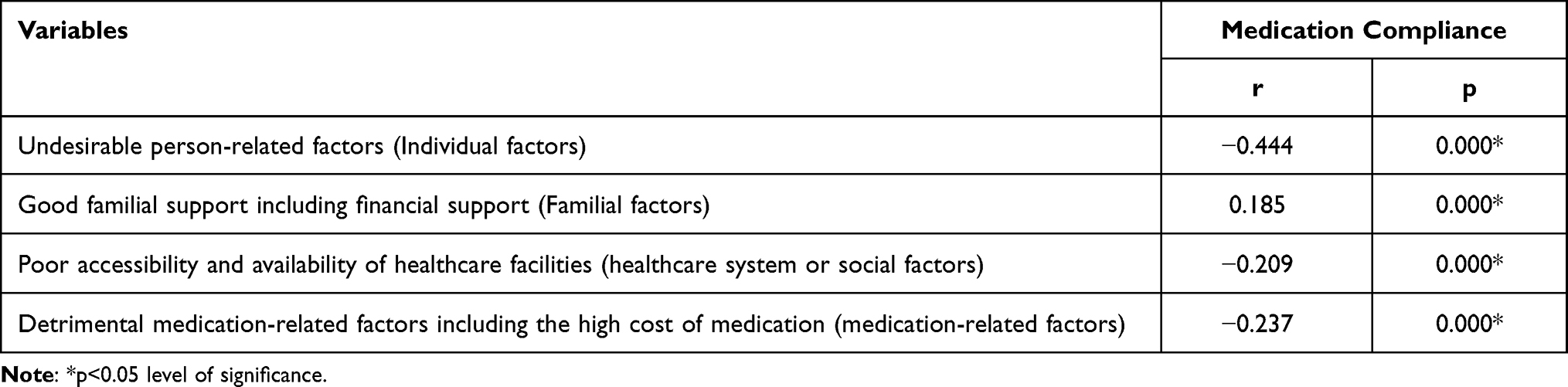 |
Table 3 Correlation Between Influencing Factors and Medication Compliance n=360 |
The results showed that the obtained “r” value between undesirable person-related factors (r= −0.444); good family support (including financial support) (r=0.185); poor accessibility to healthcare facility (r=−0.209); detrimental medication-related factors including high cost of medication (r= −0.237) were found to be significant at 0.05 level of confidence (p < 0.05).
The obtained Spearman correlation coefficient (r) value also showed that there is a weak to moderate negative correlation between the patients’ medication adherence and undesirable person-related factors, poor accessibility to the healthcare facility, and detrimental medication-related factors including the high cost of the medication. Hence, it could be interpreted as:
- When the undesirable person-related factors are decreased, there will be an increase in medication compliance among the elderly with the co-morbid illness of HTN and diabetes mellitus. The study denotes the person-related factors that are undesirable are poor understanding of the need for taking regular treatment, nature of disease condition, forgetfulness, the time factor, and various beliefs/opinions on consumption of medication for their illness.
- When there is improved availability and accessibility to healthcare facilities including hospitals and pharmacies, the medication non-adherence rate among the elderly with the co-morbid illness of HTN and T2DM will decrease.
- When there are reduced detrimental medication-related factors including high cost, there will be an increase in medication adherence rate among the elderly with the co-morbid illness of HTN and diabetes mellitus. The medication-related factors that are detrimental to hinder medication adherence among the elderly are the high cost of medication, fear about side effects or adverse effects of the drug, disinclinations of taste and smell of the drug, and polypharmacy that yield to confusion about the medication regimen, time and dose.
Further, the obtained Spearman correlation coefficient (r) value showed that there is a weak positive correlation between the patient’s medication adherence and good family support including financial support. Hence, it could be interpreted as good family support and financial assistance from family members will increase medication adherence among the elderly with co-morbid conditions of HTN and diabetes mellitus to a certain extent.
Association Between Medication Adherence and Selected Demographic Variables of Elderly with Co-Morbid Chronic Illness
Data Table 4 shows that the obtained chi-square value (χ2) is not found to have a significant association (p>0.05) between medication adherence and the selected socio-demographic variables such as age, gender, education, occupation, living status, family income status, receiving a pension, amount of pension and insurance facility.
 |
Table 4 Association Between Selected Socio-Demographic Variables and Medication Compliance of Elderly with Co-Morbid Conditions of HTN and Diabetes Mellitus n=360 |
The obtained chi-square test value (χ2) revealed that there is no significant association (p>0.05) between medication adherence and the clinical variable such as the absence of functional impairments, presence of hearing impairment, and duration of illnesses of HTN and diabetes mellitus. However, it is found to have a significant association with other notifiable clinical variables such as poor vision, memory impairment, physical disability, presence of more than one or multiple functional impairments, and other co-morbid illnesses (Table 5).
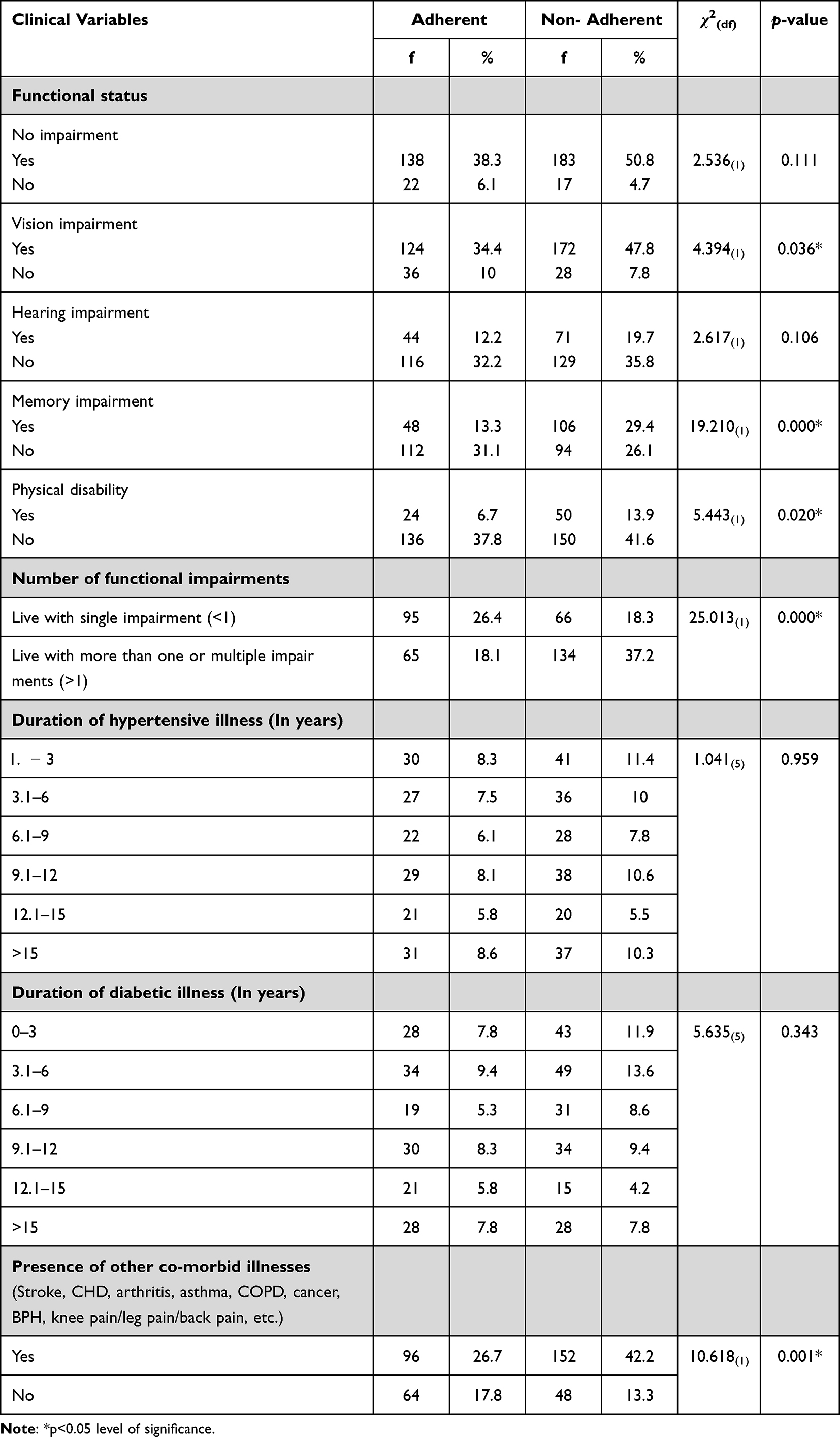 |
Table 5 Association Between Selected Clinical Variables and Medication Compliance of Elderly with Co-Morbid Conditions of HTN and Diabetes Mellitus n=360 |
The data in Table 6 show that the obtained chi-square value (χ2) is not found to have a significant association (p>0.05) between medication compliance and the treatment facility, number of prescribed drugs, and consumption of complementary therapies along with allopathic drugs.
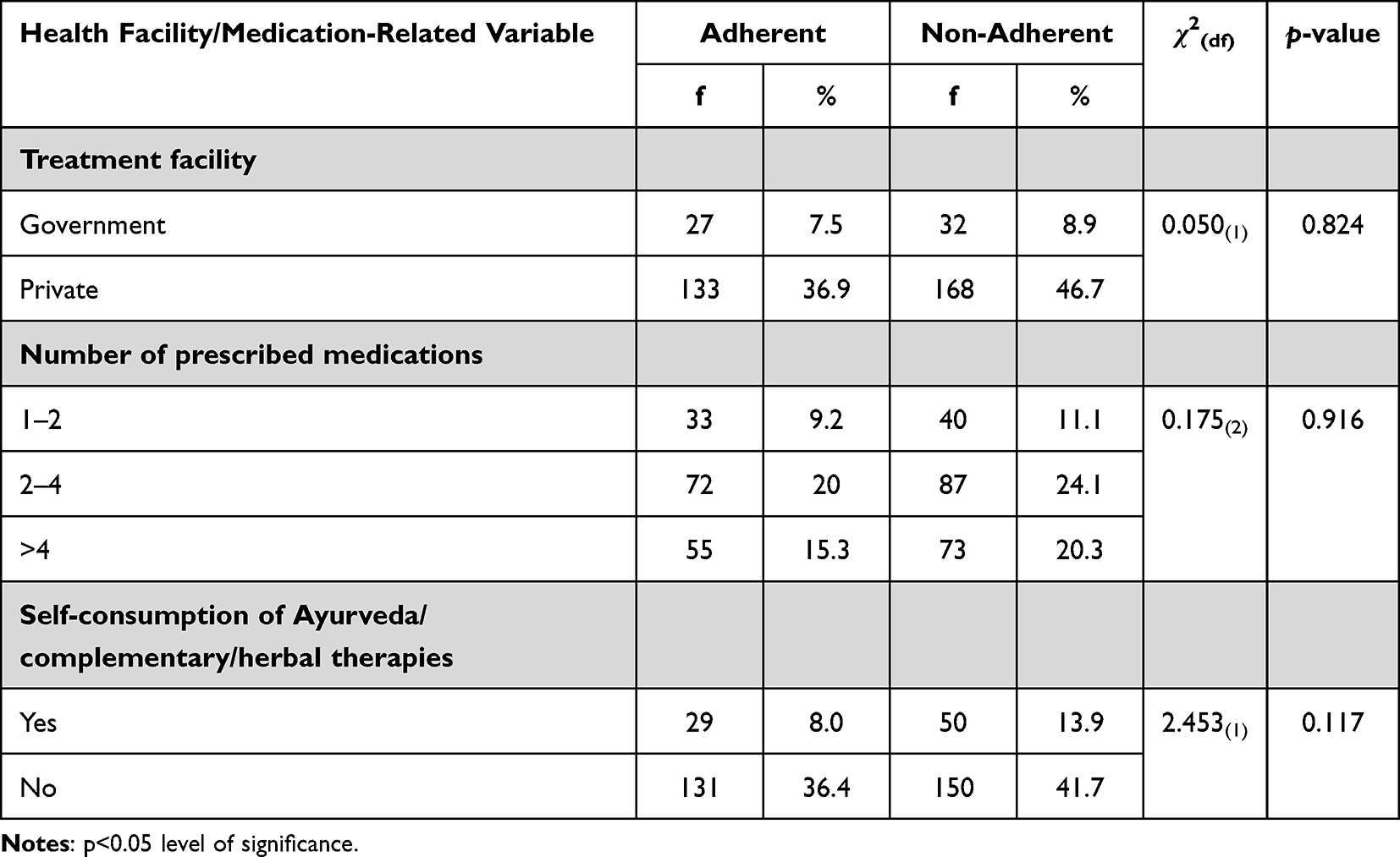 |
Table 6 Association Between Treatment Facility and Medication Related Variables and Medication Compliance of Elderly with Co-Morbid Conditions of HTN and Diabetes Mellitus n=360 |
The obtained chi-square value (χ2) is found to have a significant association (p<0.05) between medication adherence and knowledge about health conditions and their associated complications and knowledge of the importance of taking medications. It is not significantly associated with the awareness of how to take the medications (Table 7). Therefore, it could be interpreted as adherence to anti-hypertensive and anti-glycaemic drugs among the elderly with co-morbid conditions of HTN and diabetes mellitus could be dependent or influenced by the knowledge of disease conditions and their complications as well as the knowledge about the importance of consumption of regular medications. It is also revealed and interpreted that, medication compliance is independent of the patients’ awareness of how to take their medications.
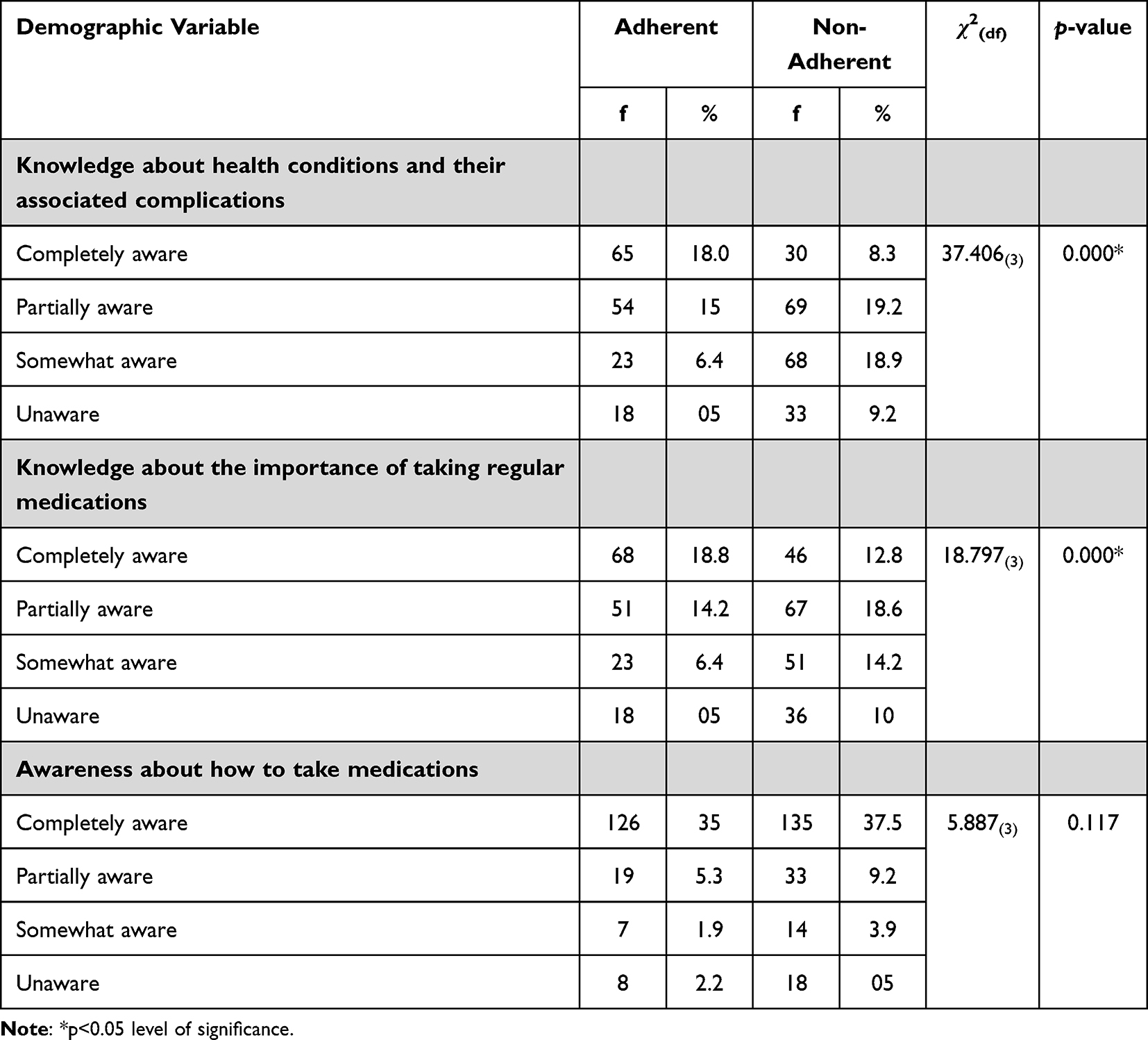 |
Table 7 Association Between Knowledge Related Variables and Medication Compliance of Elderly with Co-Morbid Conditions of HTN and Diabetes Mellitus n=360 |
Discussion
The present study aimed to find the determinants of medication non-adherence among elderly with co-morbid chronic conditions residing in rural areas and the study findings are discussed under the headings of medication non-adherence, determinants that are related to patients, healthcare providers, health system, medication, and socio-economic/familial conditions.
Medication Non-Adherence
In the present study, findings showed that 200 (55.6%) elderly with co-morbid conditions of HTN and diabetes mellitus among 360 are non-adherent to their physician-prescribed medications and other treatment regimens to control their blood pressure and glycaemic level. Similar results were reported in the studies that are done in other parts of India27–30 and this result is slightly higher than the study report presented from other countries.31 However, the present study result is contradicted by the hospital-based study which was done before the COVID pandemic in the same district of Karnataka state, India, and it shows a 16.9% difference in the non-adherence rate and higher adherence rate (61.4%) among elderly to anti-hypertensive medications.32 This difference must have occurred due to the pre and post-COVID data collection period, co-morbid status of the elderly, and the variations in the study settings.
Person-Related Factors
In the current study, 54.2% (f=195) of the elderly reported to be between the age group of 60 and 69 years, and 61.9% (f=223) of elderly with co-morbid conditions of HTN and diabetes mellitus are found to be female and this result is supported by the report given by Singh, et al29 However, Singh et al had presented the higher illiteracy rate in RS Pura health block in Jammu district in North‑West India than the present study (19.7%; f=71).
However, the chi-square test value between medication compliance among the elderly and age (χ2= 0.449); gender (χ2= 0.059); and educational status (χ2= 9.440; p=0.05) are found to be not statistically significant at 0.05 level of confidence and this result is inconsistent with the report from Srivalli and Pereira30 and Sheilini et al33 However, Sheilini et al had given a contrasting result in the perspective of educational status to the current study showing a significant association with medication adherence.
The study also presents the significant association between medication adherence and knowledge about health conditions (χ2= 37.406; p<0.05) and the importance of taking regular medications (χ2= 18.797; p<0.05) among elderly with co-morbid chronic conditions. The study reports presented by Morisky et al,34 Bosch-Lenders et al,35 Mekonnen and Gelayee36 support these findings, and augment the importance of the knowledge component in hiking the medication adherence rate.
In the present study, the chi-square test value shows the significant influence (p<0.05) of certain clinical variables such as poor memory (χ2=19.210) and vision (χ2=4.394), physical disability (χ2=5.443), presence of more than one functional impairment (χ2=25.013) and co-morbid chronic conditions (χ2=10.618). Many authors from their scientific evidence had proven that cognitive impairment or poor memory is a major determinant of medication non-adherence among the elderly, and interventions focusing on improving their cognitive ability among the elderly will improve their medication adherence level and it further protects them from detrimental effects.37–41 Scientists also have reported in their research findings that, older people can have multiple age-related problems such as impaired vision, physical disabilities, and multiple morbid conditions along with other psychosocial factors which might lead to poor adherence to their treatment regimen.9,18,42
On the whole, the undesirable person-related factors have a significant relationship (r=−0.444; p<0.05) with medication adherence among the elderly with chronic illness. According to this study, the undesirable individual factors are poor understanding of the need for taking regular treatment and the nature of the disease condition, forgetfulness, inappropriate drug-taking behaviour that includes wrong frequency and drug dose regimen, and the decision to stop taking medication by themselves and also the various beliefs/opinions on consumption of medication for their illness including home remedies. Most of the research findings have described the influence of person-related factors on medication adherence among elderly with chronic illness and also specified the importance of communication, patient–provider relationship, level of satisfaction, and physician-patient agreement on drug therapy.18,37–44
Healthcare System-Related Factors
Healthcare facilities in India are broadly classified into public and private. Public health facilities are sponsored by the government, whereas the treatment cost should be paid by the patient to the privately owned medical facility in India or it can be paid through availed insurance scheme by the patient to the affiliated hospitals/health facility.
In the present study, most of the rural elderly with co-morbid conditions of HTN and diabetes mellitus were taking treatment from a private facility (83.6%; f=301) and it does not have any significant association (χ2=0.50; p>0.05) with medication non-adherence. However, the poor accessibility and availability of healthcare facilities have a significant correlation (r=- 0.209; p<0.05) with medication adherence among them. In this study, healthcare facility factors such as non-availability of hospital/health centre/pharmacy within proximity of distance of patient residence, unavailability of physician prescribed medicines in the nearby available pharmacy, and poor transport facility to the medical care facility were considered. Brown and Bussell 44 Gordon et al,45 and Kennedy et al46 mentioned in their article that, inequitable distribution of the healthcare system plays a barrier to medication adherence by limiting the co-ordination between the patient access to care and the healthcare facility and higher cost of drug or prohibitive drug costs are also considered to be the contributing factors for poor medication adherence. Hence, it is vital to have equitable distribution, good accessibility to the healthcare system, and availability of prescribed medication at medical facilities/pharmacies at an affordable cost to improve the medication adherence rate among the elderly with chronic illness.
Medication-Related Factors
The majority of the rural elderly with co-morbid chronic conditions (24.1%; f=87) were taking two to four medications or more than four medications (20.3%; f=73) per day and are non-adherent to their anti-hypertensive and anti-glycaemic treatment regimen. However, the chi-square test value is found to be not significant (χ2=0.175; p>0.05) between the number of prescribed medications and medication adherence. In contrast, this phenomenon of interest was well described in a nationwide population-based study done by Kim et al47 and specified in their report that, the association between medication adherence and the total number of medications, and age demonstrated an inverted U-shape with a peak at three to four total medications and age 60–69 years and irrespective of age, the adherence rate was decreased significantly, when the total number of drugs was nine or more. Hence, the treating doctor should take appropriate measures to improve adherence based on the total number of medications and the age of the patient.
The present study finding depicts that the consumption of Ayurveda/complimentary/herbal therapies without the consultation of the treating doctor was found among the limited number of elderly (13.9%; f=50) with co-morbid chronic conditions and it is not statistically significant with the medication non-adherence (χ2= 2.453; p>0.05). In contrast, Cuffee et, al48 proved that usage of two or more home remedies was significantly related to low adherence (OR: 0.55, CI: 0.36–0.83, P=0 0.004).
Further, the detrimental medication-related factors including the high cost of medication were identified to be the most significant determinant (r=−0.237; p<0.05) of the medication non-adherence among elderly with chronic illness of HTN and diabetes mellitus. This study refers to the high cost of the drug, fear of adverse effects, drug odor and taste, and multiple prescribed drug regimens or polypharmacy as the unfavorable medication-related factors for drug adherence. The influence of these factors on medication adherence among the elderly has been proven by many other investigators and reiterates the importance of focused interventions on these factors to enhance medication adherence among the elderly.18,23,30,49–51
Socio-Economic and Family Conditions-Related Factors
A current study report shows that, most of the rural elderly who are non-adherent to their medication are found to be living with their family members (41.9%; f=151); belonged to below poverty line (37.2%; f=134); depend on their old age pension (28.3%; f=102); receiving pension less than INR 1000 (51.1%; f=184) and not enrolled in any insurance scheme (34.1%; f=123). However, these factors are not having a statistically significant association with the medication non-adherence (p>0.05).
Further, the findings of this study showed that there is a weak positive correlation between the patients’ medication compliance and good family support including financial support (r=0.185; p<0.05). The parameters which include better family financial conditions and funding for purchasing prescribed drugs, good family support towards following therapeutic diet and exercise regimen and providing remainder for taking prescribed medications to elderly, and caregiver confidence in caring for elderly in emergencies are the good family support-related factors in this study. Many evidence related to these factors confirm that there is a considerable decrease in the non-adherence rate among the elderly when there is a satisfactory socio-economic condition and family support which also enhances their quality of life among them.52–57
Limitations
This study did not establish the relationship between the level of treatment satisfaction and patient–provider communication and IPR and medication non-adherence among elderly with co-morbid conditions.
Conclusion
In summary, the present study findings displayed that, 55.6% of the elderly with co-morbid chronic conditions are non-adherent to their anti-hypertensive and anti-glycaemic drugs and established the significant relationship between medication non-adherence and the determinants related to the person, family and financial support, accessibility and availability of healthcare facility and medication including high-cost drugs and also depicted the strong evidence that, there are multiple determinants to medication non-adherence. Better understanding about these determinants will help the physician to decide on appropriate precautionary measures to prevent non-adherence of medication among elderly and also it helps policy makers to choose the right solution for addressing this preventable public health problem. Further studies on developing some patient-specific intervention program to improve medication adherence among elderly would be beneficial.
Abbreviations
HTN, hypertension; T2DM, type 2 diabetes mellitus; PHC, primary health centers; COVID, coronavirus disease.
Data Sharing Statement
All gathered or analyzed data are included in this article. The rating scale on factors influencing medication adherence is available to the first/corresponding author and will be shared upon reasonable request.
Acknowledgments
This study was self-financed and acknowledges the contribution of all Doctoral Advisory Committee (DAC) members for their valuable inputs for the conduct of this study. This article was copy-edited by Mr Prithvirajesh Kumar S K, Acquisition Editor, Manipal Universal Press, Manipal.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Rahman FI, Aziz F, Huque S, Ether SA. Medication understanding and health literacy among patients with multiple chronic conditions: a study conducted in Bangladesh. J Public Health Res. 2020;9(1):1792. PMID: 32607317; PMCID: PMC7315107. doi:10.4081/jphr.2020.1792
2. Bastani P, Bikineh P, Mehralian G, et al. Medication adherence among the elderly: applying grounded theory approach in a developing country. J Pharm Policy Pract. 2021;14(55):2–8. doi:10.1186/s40545-021-00340-9
3. Takane AK, Balignasay M-D, Nigg CR. Polypharmacy reviews among elderly populations project: assessing needs in patient-provider communication. Hawaii J Med Public Health. 2013;72(1):15–22. doi:10.1186/1472-6963-9-228
4. Huang AR, Mallet L, Rochefort CM, et al. Medication-related falls in the elderly: causative factors and preventive strategies. Drugs Aging. 2012;29(5):359–376. doi:10.2165/11599460-000000000-00000
5. Balogun WO, Salako BL. Co-occurrence of diabetes and hypertension: pattern and factors associated with order of diagnosis among Nigerians. Ann Ib Postgrad Med. 2011;9(2):90–94.
6. Shayakul C, Teeraboonchaikul R, Susomboon T, et al. Medication adherence, complementary medicine usage and progression of diabetic chronic kidney disease in Thais. Patient Prefer Adherence. 2022;16:467–477. doi:10.2147/PPA.S350867
7. Burnier M, Egan BM. Adherence in hypertension a review of prevalence, risk factors, impact, and management. Circ Res. 2019;124:1124–1140. doi:10.1161/CIRCRESAHA.118.313220
8. Polonsky WH, Henry RR. Poor medication adherence in type 2 diabetes: recognizing the scope of the problem and its key contributors. Patient Prefer Adherence. 2016;10:1299–1307. doi:10.2147/PPA.S106821
9. Yap AF, Thirumoorthy T, Kwan YH. Case report: medication adherence in the elderly. J Clin Gerontol Geriatr. 2016;7:64–67. doi:10.1016/j.jcgg.2015.05.001
10. Rolnick SJ, Pawloski PA, Hedblom BD, et al. Patient characteristics associated with medication adherence. Clin Med Res. 2013;11(2):54–65. doi:10.3121/cmr.2013.1113
11. Asefzadeh S, Asefzadeh M, Javadi H. Care management: adherence to therapies among patients at Bu-Alicina Clinic, Qazvin. Iran Pajouhesh Dar Pezeshki. 2005;10(6):343–348.
12. Brown MT, Bussell J, Dutta S, et al. Medication adherence: truth and consequences. Am J Med Sci. 2016;351(4):387–399. doi:10.1016/j.amjms.2016.01.010
13. Gellad WF, Grenard J, Elizabeth AM. A Review of Barriers to Medication Adherence: A Framework for Driving Policy Options. Santa Monica, CA: RAND Corporation; 2009.
14. Miller NH, Hill M, Kottke T, et al. The multilevel compliance challenge: recommendations for a call to action: a statement for healthcare professionals. Circulation. 1997;95:1085e90. doi:10.1161/01.CIR.95.4.1085
15. Sabate E. Adherence to Long-Term Therapies: Evidence for Action. Geneva: World Health Organization; 2003.
16. Neiman AB, Ruppar T, Ho M, et al. CDC grand rounds: improving medication adherence for chronic disease management — innovations and opportunities. Morb Mortal Wkly Rep. 2017;66(45):1248–1251. doi:10.15585/mmwr.mm6645a2
17. Sengstock D, Zimmerman J. Addressing polypharmacy & improving medication adherence in older adults. In: Current Diagnosis & Treatment: Geriatrics.
18. Jin H, Kim Y, Rhie SJ. Factors affecting medication adherence in elderly people. Patient Prefer Adherence. 2016;10:2117–2125. doi:10.2147/PPA.S118121
19. Huang J, Harry HX, Wang HHX, et al. Medication adherence among the older adults: challenges and recommendations. Hong Kong Med J. 2020;26:476–478. doi:10.12809/hkmj205108
20. Pasina L, Brucato AL, Falcone C, et al. Medication non-adherence among elderly patients newly discharged and receiving polypharmacy. Drugs Aging. 2014;31(4):283–289. PMID: 24604085. doi:10.1007/s40266-014-0163-7
21. Chung GC, Marottoli RA, Cooney LM, et al. Cost-related medication nonadherence among older adults: findings from a nationally representative sample. J Am Geriatr Soc. 2019;67(12):2463–2473. doi:10.1111/jgs.16141
22. Barry HE, Hughes CM. An update on medication use in older adults: a narrative review. Curr Epidemiol Rep. 2021;8(3):108–115. doi:10.1007/s40471-021-00274-5
23. Morgan SG, Lee A. Cost-related non-adherence to prescribed medicines among older adults: a cross-sectional analysis of a survey in 11 developed countries. BMJ Open. 2017;7:e014287. doi:10.1136/bmjopen-2016-014287
24. Kshatri JS, Palo SK, Bhoi T, et al. Prevalence and patterns of multimorbidity among rural elderly: findings of the AHSETS study. Front Public Health. 2020;8:582663. doi:10.3389/fpubh.2020.582663
25. Tripathy JP, Thakur JS, Jeet G, et al. Prevalence and determinants of comorbid diabetes and hypertension: evidence from non-communicable disease risk factor STEPS survey, India. Diabetes Metab Syndr. 2017;11: 1:S459–S465. doi:10.1016/j.dsx.2017.03.036
26. Easthall C. Medication non-adherence as a complex health behavior: there is more to it than just missed doses. J Am Geriatr Soc. 2019;67:12. 2439–2440. doi:10.1111/jgs.16143
27. Shruthi R, Jyothi R, Pundarikaksha HP, et al. A study of medication compliance in geriatric patients with chronic illnesses at a tertiary care hospital. J Clin Diagn Res. 2016;10:FC 40–3.
28. Punnapurath S, Vijayakumar P, Platty L, et al. A study of medication compliance in geriatric patients with chronic illness. J Fam Med Prim Care. 2021;10(4):1644–1648. doi:10.4103/jfmpc.jfmpc_1302_20
29. Singh P, Gupta RK, Jan R, et al. Adherence for medication among self-reporting rural elderly with diabetes and hypertension. J Med Soc. 2017;31:86–89. doi:10.4103/jms.jms_48_16
30. Srivalli BD, Pereira PA. study of medication compliance and medication safety among geriatric patients in rural areas. APIK J Int Med. 2020;8:65–72. doi:10.4103/AJIM.AJIM_4_19
31. Sinan O, Akyuz A. Effects of home visits on medication adherence of elderly individuals with diabetes and hypertension. East J Med. 2019;24(1):8–14. doi:10.5505/ejm.2019.71463
32. Sheilini M, Hande HM, Prabhu MM, et al. Antihypertensive prescription pattern, self-reported reasons for non adherence to antihypertensives and lifestyle practices among the elderly. JCDR. 2018;12:OC01–OC04. doi:10.7860/JCDR/2018/29729.11025
33. Sheilini M, Hande HM, Prabhu MM, et al. Impact of multimodal interventions on medication non adherence among elderly hypertensives: a randomized controlled study. Patient Prefer Adherence. 2019;13:549–559. doi:10.2147/PPA.S195446
34. Morisky DE, Ang A, Krousel-Wood M, et al. Predictive validity of a medication adherence measure in an outpatient setting. J Clin Hypertens. 2008;10(5):348–354. doi:10.1111/j.1751-7176.2008.07572.x
35. Bosch-Lenders D, Denny WHA, Henri H, et al. Factors associated with appropriate knowledge of the indications for prescribed drugs among community-dwelling older patients with polypharmacy. Age Ageing. 2016;45(3):402–408. doi:10.1093/ageing/afw045
36. Mekonnen GB, Gelayee DA. Low medication knowledge and adherence to oral chronic medications among patients attending community pharmacies: a cross-sectional study in a low-income country. Biomed Res Int. 2020;1–8. doi:10.1155/2020/4392058
37. Cho MH, Shin DW, Chang SA, et al. Association between cognitive impairment and poor antihypertensive medication adherence in elderly hypertensive patients without dementia. Sci Rep. 2018;8:11688. doi:10.1038/s41598-018-29974-7
38. Chudiak A, Uchmanowicz I, Mazur G. Relation between cognitive impairment and treatment adherence in elderly hypertensive patients. Clin Interv Aging. 2018;13:1409–1418. doi:10.2147/CIA.S162701
39. Campbell NL, Boustani MA, Skopeljia EN, et al. Medication adherence in older adults with cognitive impairment: a systematic evidence-based review. Am J Geriatr Pharmacother. 2012;10(3):165–177. doi:10.1016/j.amjopharm.2012.04.004
40. Smith D, Lovell J, Weller C, et al. A systematic review of medication non-adherence in persons with dementia or cognitive impairment. PLoS One. 2017;12(2):e0170651. doi:10.1371/journal.pone.0170651
41. Ma Y, He F, Liu S, et al. The association between the prevalence, medication adherence and control of hypertension and the prevalence of mild cognitive impairment in rural northern china: a cross-sectional study. Patient Prefer Adherence. 2022;16:493–502. doi:10.2147/PPA.S351588
42. Nikolaus T, Kruse W, Bach M, et al. Elderly patients’ problems with medication. An in-hospital and follow-up study. Eur J Clin Pharmacol. 1996;49(4):255–259. PMID: 8857069. doi:10.1007/BF00226324
43. Alfian S, Sukandar H, Arisanti N, et al. Complementary and alternative medicine use decreases adherence to prescribed medication in diabetes patients. Ann Trop Med Public Health. 2016;9(3):174–179. doi:10.4103/1755-6783.179108
44. Brown MT, Bussell JK. Medication adherence: WHO cares? Mayo Clin Proc. 2011;86(4):304–314. doi:10.4065/mcp.2010.0575
45. Gordon K, Smith F, Dhillon S. Effective chronic disease management: patients’ perspectives on medication-related problems. Patient Educ Couns. 2007;65(3):407–415. doi:10.1016/j.pec.2006.09.012
46. Kennedy J, Tuleu I, Mackay K. Unfilled prescriptions of medicare beneficiaries: prevalence, reasons, and types of medicines prescribed. J Manag Care Pharm. 2008;14(6):553–560. doi:10.18553/jmcp.2008.14.6.553
47. Kim J, Kwon D, Han EB, et al. Impact of number of medications and age on adherence to antihypertensive medications. Medicine. 2019;98: 49:e17825. doi:10.1097/MD.0000000000017825
48. Cuffee L, Rosal M, Hargraves L, et al. Does home remedy use contribute to medication non adherence among blacks with hypertension? Ethn Dis. 2020;30(3):451–458. doi:10.18865/ed.30.3.451
49. Krousel-Wood M, Joyce C, Holt E, et al. Predictors of decline in medication adherence: results from the cohort study of medication adherence among older adults. Hypertension. 2011;58(5):804–810. doi:10.1161/HYPERTENSIONAHA.111.176859
50. Osterberg L, Blaschke T. Adherence to medication. N Engl J Med. 2005;353(5):487–497. doi:10.1056/NEJMra050100
51. Smaje A, Weston-Clark M, Raj R, et al. Factors associated with medication adherence in older patients: a systematic review. Aging Med. 2018;1:254–266. doi:10.1002/agm2.12045
52. Lee H, Park JH, Floyd S, et al. Combined effect of income and medication adherence on mortality in newly treated hypertension: nationwide study of 16 million person‐years. J Am Heart Assoc. 2019;8:e013148. doi:10.1161/JAHA.119.013148
53. Osborn Y, Kripalani S, Goggins M, et al. Financial strain is associated with medication nonadherence and worse self-rated health among cardiovascular patients. J Health Care Poor Underserved. 2017;28(1):499–513. doi:10.1353/hpu.2017.0036
54. Manias E, Bucknall T, Hughes C, et al. Family involvement in managing medications of older patients across transitions of care: a systematic review. BMC Geriatr. 2019;19:95. doi:10.1186/s12877-019-1102-6
55. Kardas P, Lewek P, Matyjaszczyk M. Determinants of patient adherence: a review of systematic reviews. Front Pharmacol. 2013;4(91):1–16. doi:10.3389/fphar.2013.00091
56. Lozano-Hernández M, López-Rodríguez A, Leiva-Fernández F, et al. Social support, social context and nonadherence to treatment in young senior patients with multimorbidity and polypharmacy followed-up in primary care. MULTIPAP Study. PLoS One. 2020;15(6):e0235148. doi:10.1371/journal.pone.0235148
57. Wamala S, Merlo J, Bostrom G, et al. Socioeconomic disadvantage and primary non-adherence with medication in Sweden. Int J Qual Health Care. 2007;19(3):134–140. doi:10.1093/intqhc/mzm011
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.