Back to Journals » Patient Preference and Adherence » Volume 20
Determinants of Baseline Ophthalmic Screening and Its Association with Long-Term Treatment Persistence in Patients with Rheumatic Diseases Initiating Hydroxychloroquine: A Nationwide Cohort Study
Authors Kim A ![]() , Park GU, Lee SG
, Park GU, Lee SG ![]()
Received 13 February 2026
Accepted for publication 10 May 2026
Published 18 May 2026 Volume 2026:20 603312
DOI https://doi.org/10.2147/PPA.S603312
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Johnny Chen
Aran Kim,1,2 Geun U Park,3 Seung-Geun Lee1,2
1Division of Rheumatology, Department of Internal Medicine, Pusan National University Hospital, Pusan National University School of Medicine, Busan, Republic of Korea; 2Biomedical Research Institute, Pusan National University Hospital, Busan, Republic of Korea; 3Department of Statistics, GN Co., Seoul, Republic of Korea
Correspondence: Seung-Geun Lee, Division of Rheumatology, Department of Internal Medicine, Pusan National University Hospital, Pusan National University School of Medicine, 179 Gudeok-Ro, Seo-Gu, Busan, 49241, Republic of Korea, Email [email protected]
Purpose: Hydroxychloroquine (HCQ) is a cornerstone therapy for various rheumatic diseases (RDs), but prolonged exposure carries a risk of irreversible retinal toxicity. Current guidelines recommend baseline ophthalmic screening to ensure safety and support treatment longevity. This study aimed to evaluate real-world adherence to baseline screening, identify its determinants, and assess its association with long-term HCQ treatment persistence.
Patients and Methods: We conducted a nationwide retrospective cohort study using the South Korean Health Insurance Review and Assessment Service (HIRA) database. Adult patients with RDs who initiated HCQ between 2014 and 2018 and maintained therapy for ≥ 30 consecutive days were included. Baseline ophthalmic screening was defined as fundoscopy or optical coherence tomography (OCT) performed within 12 months of HCQ initiation, a pragmatic window reflecting real-world clinical practice. Determinants of screening were identified using multivariable logistic regression, and the association between screening and HCQ persistence was analyzed using Cox proportional hazards models.
Results: Of the 19,876 patients included, only 32.5% underwent baseline screening. Independent predictors of higher screening rates included older age, female sex, treatment initiation at tertiary or general hospitals, a later initiation year, and a diagnosis of systemic lupus erythematosus, Sjögren’s syndrome, or Behçet’s disease. Conversely, concomitant use of conventional synthetic disease-modifying antirheumatic drugs or glucocorticoids predicted lower rates. During follow-up, baseline ophthalmic screening was independently associated with significantly improved HCQ persistence (adjusted HR for discontinuation: 0.91; 95% CI: 0.88– 0.94); this relationship held true specifically for patients undergoing baseline OCT (adjusted HR: 0.93; 95% CI: 0.88– 0.98).
Conclusion: These findings highlight the gap between guideline recommendations and real-world practice. The observed association between baseline ophthalmic screening, particularly utilizing OCT, and improved HCQ persistence suggests that such screening may potentially serve as an indicator of comprehensive clinical management within routine practice.
Keywords: hydroxychloroquine, rheumatic diseases, retinal diseases, optical coherence tomography, medication adherence
Introduction
Hydroxychloroquine (HCQ), a chloroquine analogue, is extensively used to manage a diverse spectrum of rheumatic and systemic autoimmune diseases owing to its immunomodulatory properties and favorable safety and tolerability profile.1 Although its mechanisms of action remain incompletely understood, HCQ functions by inhibiting Toll-like receptors 7 and 9, suppressing autophagy, and modulating inflammatory cytokine pathways. In particular, it serves as a therapeutic cornerstone in systemic lupus erythematosus (SLE) by preventing acute flares and controlling disease activity, while also offering potential disease-modifying effects in rheumatoid arthritis (RA). Accordingly, HCQ is utilized as long-term maintenance therapy for SLE and various other chronic rheumatic diseases to achieve sustained disease control and improve clinical outcomes.2,3
Despite these clinical benefits, long-term HCQ use necessitates caution due to the risk of retinal toxicity, which can result in irreversible visual impairment.4 The reported prevalence of HCQ-associated retinopathy among long-term users ranges from approximately 0.6% to 10.4%, varying by study population and screening methodology.5 HCQ accumulates in melanin-rich retinal pigment epithelium (RPE) cells, ultimately causing parafoveal photoreceptor damage and disrupting the RPE layer. Consequently, HCQ-induced retinopathy can be progressive and irreversible, affecting the outer retinal layers and potentially leading to permanent vision loss.4 Notably, once HCQ-induced retinopathy manifests, progression may continue even after therapy cessation.6 Given this risk, the American Academy of Ophthalmology (AAO) recommends a baseline funduscopic evaluation within the first year of therapy, supplemented by diagnostic imaging such as optical coherence tomography (OCT).7 Specifically, OCT serves as an indispensable, non-invasive tool for detecting early structural changes in HCQ-induced maculopathy, while advanced modalities such as OCT angiography can further delineate critical microvascular alterations prior to the onset of clinical symptoms.8
Despite these evidence-based recommendations, adherence to baseline ophthalmic screening in routine clinical practice remains suboptimal. A substantial proportion of patients initiate HCQ therapy without completing guideline-recommended baseline eye examinations,6,9,10 highlighting a persistent disparity between clinical guidelines and real-world practice. This gap is particularly critical in RDs, where long-term HCQ therapy is frequently required for disease control. However, determinants of baseline ophthalmic screening completion have not been systematically evaluated; identifying patients less likely to undergo assessment is essential for improving guideline compliance and optimizing early detection strategies. Furthermore, the impact of baseline screening on subsequent treatment adherence, specifically long-term HCQ persistence, remains undefined. To address these gaps, we aimed to identify patient- and healthcare system–level determinants of baseline ophthalmic screening among patients with RDs initiating HCQ. We further assessed the association between baseline ophthalmic screening and long-term HCQ treatment persistence.
Materials and Methods
Study Design, Data Source and Study Population
We conducted a nationwide, population-based retrospective cohort study using data from the South Korean Health Insurance Review and Assessment Service (HIRA). The HIRA database contains healthcare utilization records for nearly the entire South Korean population, including demographic data, diagnostic codes, procedures, and medication prescriptions derived from mandatory national health insurance claims.11 Due to its comprehensive coverage and high validity, this database is widely used in epidemiological and clinical research to examine disease patterns, treatment trends, and health outcomes.11
We included patients with RDs aged ≥18 years who initiated HCQ therapy between 2014 and 2018 and maintained treatment for at least 30 consecutive days. This 30-day minimum threshold was applied to exclude patients who received only transient trial prescriptions or immediately discontinued treatment due to early, non-ocular adverse events (eg, gastrointestinal intolerance), thereby allowing us to focus on a cohort that genuinely initiated maintenance therapy. We defined new users as those who had not received HCQ within the six months preceding the index date (the date of HCQ initiation). The study encompassed the following RDs: RA, SLE, Sjögren’s syndrome, systemic sclerosis, mixed connective tissue disease (MCTD), ankylosing spondylitis, psoriatic arthritis, antiphospholipid syndrome (APS), palindromic rheumatism, Behçet’s disease, polymyalgia rheumatica (PMR), idiopathic inflammatory myositis, systemic vasculitis, adult-onset Still’s disease (AOSD), and relapsing polychondritis. We identified each RD using International Classification of Diseases, Tenth Revision (ICD-10) diagnostic codes and corresponding registration codes from the Rare Intractable Disease Registration (RIDR) system. The RIDR is a South Korean national registry certifying patients with designated rare or intractable diseases for insurance support, providing a standardized framework for disease classification across healthcare institutions. We applied operational definitions for each RD based on ICD-10 and RIDR codes as previously reported;12–22 detailed definitions are provided in Supplementary Table 1. We excluded patients younger than 18 years, those lacking an RD diagnosis, and those prescribed HCQ for fewer than 30 days. Figure 1 depicts the study subject selection process.
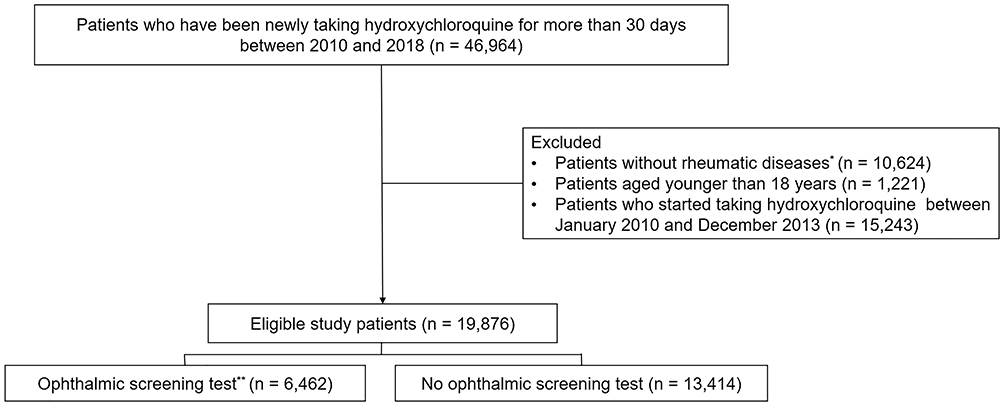 |
Figure 1 Flow chart of study patients. *Rheumatic diseases include rheumatoid arthritis, systemic lupus erythematosus, Sjögren’s syndrome, systemic sclerosis, mixed connective tissue disease, ankylosing spondylitis, psoriatic arthritis, antiphospholipid syndrome, palindromic rheumatism, Behçet’s disease, polymyalgia rheumatica, idiopathic inflammatory myositis, systemic vasculitis, adult-onset Still’s disease and relapsing polychondritis. **Perform fundoscopy or optical coherence tomography. |
This study was approved by the Institutional Review Board of Pusan National University Hospital (IRB No. 2306-029-128; approval date: July 3, 2023) and conducted in accordance with the principles of the Declaration of Helsinki. The requirement for informed consent was waived because the study utilized a publicly available, de-identified HIRA dataset.
Covariates
We extracted the following baseline demographic and clinical data at the index date: sex, age, hospital type and department of prescription, initiation year, starting dose, concomitant medications, and comorbidities. The main component codes for HCQ were 171701ATB, 171702ATB, 171703ATB, 171704ATB, and 171705ATB. Concomitant medications included conventional synthetic disease-modifying antirheumatic drugs (csDMARDs; methotrexate, sulfasalazine, leflunomide), immunosuppressants (azathioprine, tacrolimus, mycophenolate mofetil, cyclophosphamide), glucocorticoids, biological agents (etanercept, adalimumab, infliximab, golimumab, abatacept, tocilizumab, tofacitinib, baricitinib, belimumab, rituximab), and tamoxifen. We calculated the Charlson Comorbidity Index (CCI) by summing the weighted scores of relevant comorbid conditions, following established methods.23 Body weight and laboratory data were not available; therefore, weight-adjusted HCQ dose (mg/kg) could not be assessed.
Outcomes
Given the inherent limitations of claims-based data in differentiating screening from symptom-driven diagnostic testing, we conservatively defined baseline ophthalmic screening as the performance of a fundoscopic examination or OCT, modalities that are consistently coded and reproducible in the HIRA database. The primary outcome was the completion of a baseline ophthalmic screening examination within 12 months of HCQ initiation (the index date). While current AAO guidelines recommend baseline evaluation ideally before or shortly after treatment initiation, we adopted a pragmatic 12-month window to account for real-world delays in ophthalmologic referrals and appointment scheduling common in routine practice. We operationally defined baseline screening as the receipt of at least one of the following procedures: fundoscopic examination (HIRA EDI codes E660, E6670, E6674) or OCT (EDI code EZ796). Although clinical guidelines also recommend functional tests such as automated visual field (VF) testing, fundus autofluorescence (FAF), and multifocal electroretinography (mfERG), we focused on structural screening modalities (fundoscopy and OCT) as they are the most consistently captured and standardized procedural codes within the administrative database. We adopted this approach to ensure a reproducible assessment, as fundoscopy and OCT represent the most consistently captured and standardized procedural codes within the HIRA database. Furthermore, excluding modalities such as VF and FAF minimizes potential misclassification. While these tests are valuable components of a comprehensive baseline assessment, their clinical intent—whether for standardized baseline screening or for the diagnostic evaluation of pre-existing ocular conditions—is difficult to reliably differentiate using administrative claims data.
Additionally, we investigated HCQ persistence, defined as the duration from initiation to discontinuation of therapy.2 We defined discontinuation as a gap of > 60 days without a prescription refill. If HCQ was restarted within 60 days, we considered the treatment continuous. Follow-up continued until December 31, 2020. Specifically, we analyzed the impact of baseline ophthalmic screening on HCQ persistence.
Statistical Analyses
All statistical analyses were performed using an experienced biostatistician (GU Park), using SAS version 9.4 (SAS Institute, Cary, NC, USA); a p-value < 0.05 was considered statistically significant. We presented continuous and categorical variables as mean ± standard deviation and number (percentage), respectively. We compared groups using chi-square tests, Fisher’s exact tests, Student’s t-tests, or Mann–Whitney U-tests, as appropriate. We evaluated factors associated with baseline ophthalmic examination using logistic regression models. Multivariable logistic regression models verified independent associations, incorporating clinically relevant variables (eg, age, sex) and those with a p-value < 0.1 in the univariable analysis. Because comorbidity and the CCI were highly correlated, we constructed two separate multivariable models, each including one of these variables, to assess their associations with baseline screening completion. We evaluated factors associated with the risk of HCQ discontinuation using Cox proportional hazards regression models. We constructed multivariable Cox regression models similarly, including clinically relevant variables and those with a p-value < 0.1 in the univariable analysis.
Results
We included 19,876 patients who initiated HCQ between January 2014 and December 2018 (Figure 1). Table 1 summarizes baseline clinical and demographic data. Most patients were female (85.3%), and the mean age was 51.2 years. Notably, 69.3% initiated HCQ at general or tertiary hospitals, and 55.5% received prescriptions from rheumatologists. The mean starting HCQ dose was 284.6 mg. The most common RDs were RA (67.0%) followed by SS (19.6%), and SLE (19.4%). The majority of patients (73.9%) concomitantly received glucocorticoids. More than half of the cohort (55.5%) had hyperlipidemia, whereas > 30% had liver disease and hypertension (Table 1).
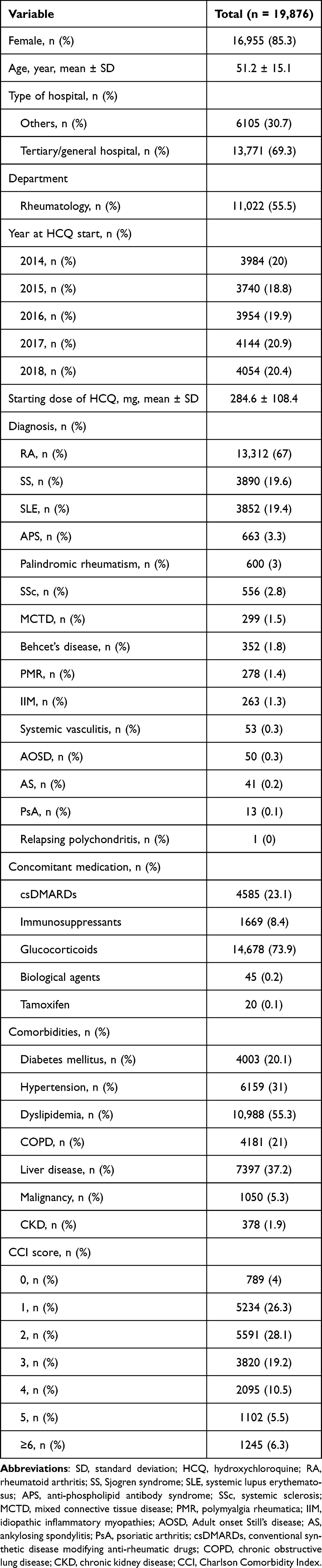 |
Table 1 Baseline Characteristics of Study Patients |
Overall, 32.5% of patients (n = 6456) completed at least one baseline ophthalmic examination (fundoscopy or OCT) within one year of initiating HCQ. Among screened patients, 6371 (32.1%) received fundoscopy and 2135 (10.7%) underwent OCT. Figure 2 details the frequency of baseline screening and OCT utilization across RD types. Patients with Behçet’s disease exhibited the highest screening rates (40.6%), followed by those with AS (39.0%), SS (38.7%), and SLE (37.4%). Conversely, patients with MCTD (26.8%) and palindromic rheumatism (22.7%) had the lowest rates. Additionally, OCT utilization was highest in SLE (15.6%), followed by PMR (14%), APS (12.5%), and AOSD (12%).
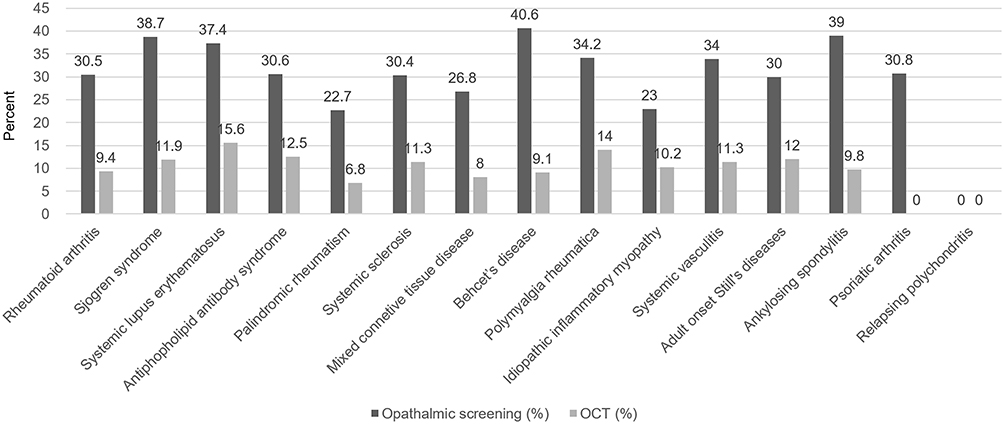 |
Figure 2 Frequency of baseline screening and optical coherence tomography utilization across rheumatic diseases types. |
Table 2 compares clinical characteristics stratified by baseline screening status. Compared with unscreened patients, those screened were significantly more likely to be female (p = 0.01) and older (p < 0.001). They were also more likely to initiate HCQ at tertiary or general hospitals (p < 0.001) and receive care from rheumatology departments (p < 0.001), though their mean starting dose was lower (p < 0.001). Additionally, screened patients had significantly higher comorbidity burdens and immunosuppressant use (p < 0.001); conversely, csDMARDs (p < 0.001) and glucocorticoid (p < 0.001) use was significantly lower. Screening rates varied significantly by underlying RD. Specifically, patients with SS (p < 0.001), SLE (p < 0.001), and Behçet’s disease (p = 0.001) were significantly more likely to undergo screening. In contrast, patients with RA (p < 0.001), palindromic rheumatism (p < 0.001), or MCTD (p = 0.032) were significantly less likely to be screened. Supplementary Table 2 compares clinical characteristics based on OCT performance; results were largely similar to the overall screening analysis.
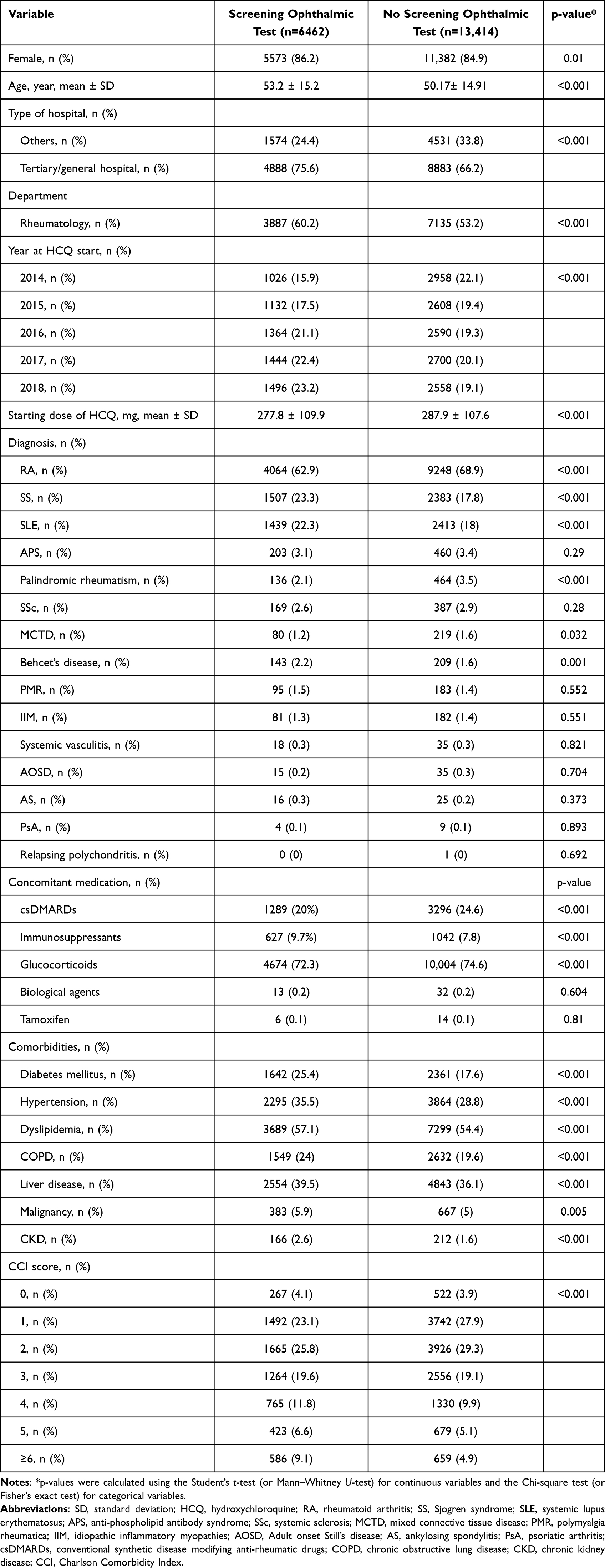 |
Table 2 Comparison of Clinical Parameters According to the Screening Ophthalmic Test Status |
Table 3 presents the results of logistic regression models evaluating predictors of baseline ophthalmic examination within 12 months of the index date. We constructed two multivariable models to account for potential confounding; findings were nearly identical. Independent predictors of increased screening likelihood included female sex (OR range, 1.14–1.15; p range, 0.002–0.003), older age (per 10-year increase; OR range, 1.14–1.15; p range, 0.002–0.003), prescription at tertiary/general hospitals (OR range, 1.40–1.41; p < 0.001), later initiation year (vs. 2014; ORs increasing from 1.21 to 1.53; all p < 0.001), starting dose ≤300 mg (OR range, 1.14–1.15; p < 0.001), and diagnoses of SS (OR range, 1.28–1.29; p < 0.001), SLE (OR range, 1.42–1.45; p < 0.001), or Behçet’s disease (OR range, 1.78–1.79; p < 0.001). Conversely, concomitant use of csDMARDs (OR range, 0.88–0.89; p range, 0.003–0.005) and glucocorticoids (OR, 0.92; p range, 0.023–0.032) was independently associated with a lower screening probability. Additionally, diabetes mellitus, hypertension, COPD, liver disease, and a CCI score ≥ 3 were significantly associated with an increased likelihood of screening.
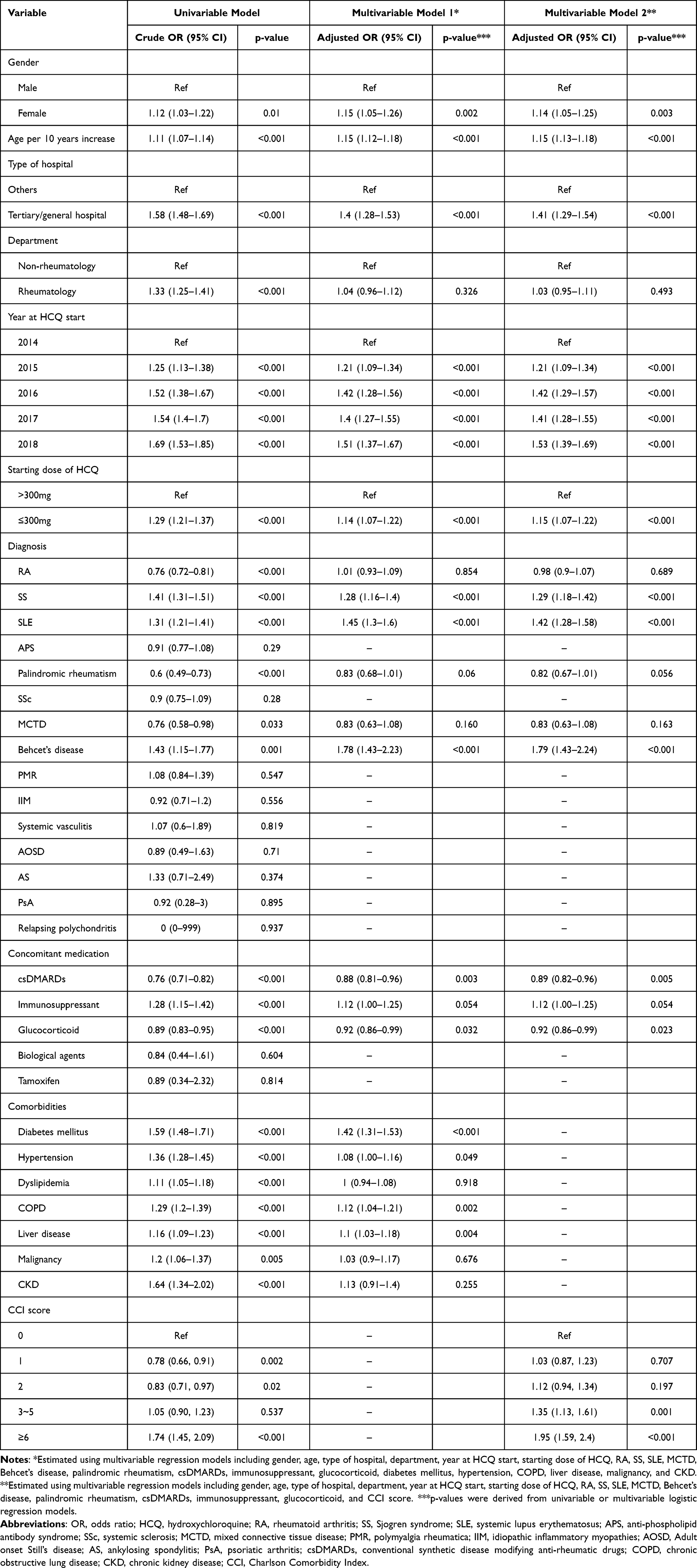 |
Table 3 Associated Factors for Undergoing Baseline Screening Ophthalmic Test Analyzed by Logistic Regression Models |
Supplementary Table 3 presents predictors of baseline OCT performance. After adjustment, older age, tertiary/general hospital setting, later initiation year, starting dose ≤300 mg, SLE diagnosis, and concomitant immunosuppressant use were independently associated with a higher probability of OCT; conversely, glucocorticoid use was associated with a lower likelihood.
During the study, 15,373 (77.3%) patients discontinued HCQ. Kaplan–Meier curves revealed that baseline ophthalmic screening was associated with significantly better HCQ persistence than unscreened patients (Figure 3). Additionally, patients who underwent baseline OCT demonstrated significantly greater HCQ persistence (Figure 3). Supplementary Table 4 shows results from univariable Cox regression models predicting HCQ discontinuation risk. After adjustment, baseline ophthalmic screening was significantly associated with a better HCQ treatment persistence (HR, 0.91, p < 0.001; Table 4). Multivariable models also revealed that screening OCT was associated with a decreased risk of HCQ withdrawal (HR, 0.93; p range, 0.006–0.007).
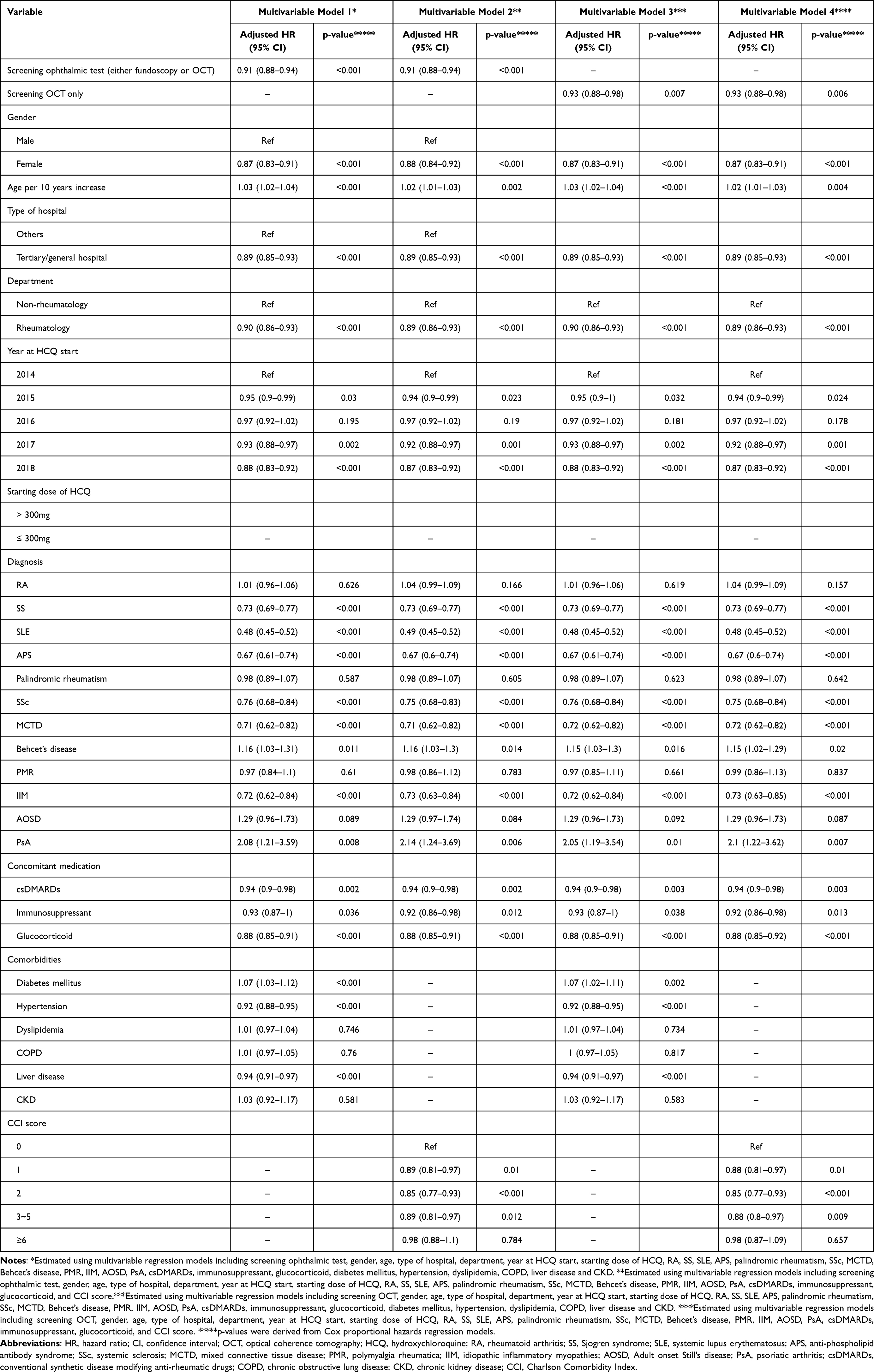 |
Table 4 Results of Multivariable Cox Regression Models for Predicting Risk of Hydroxychloroquine Discontinuation |
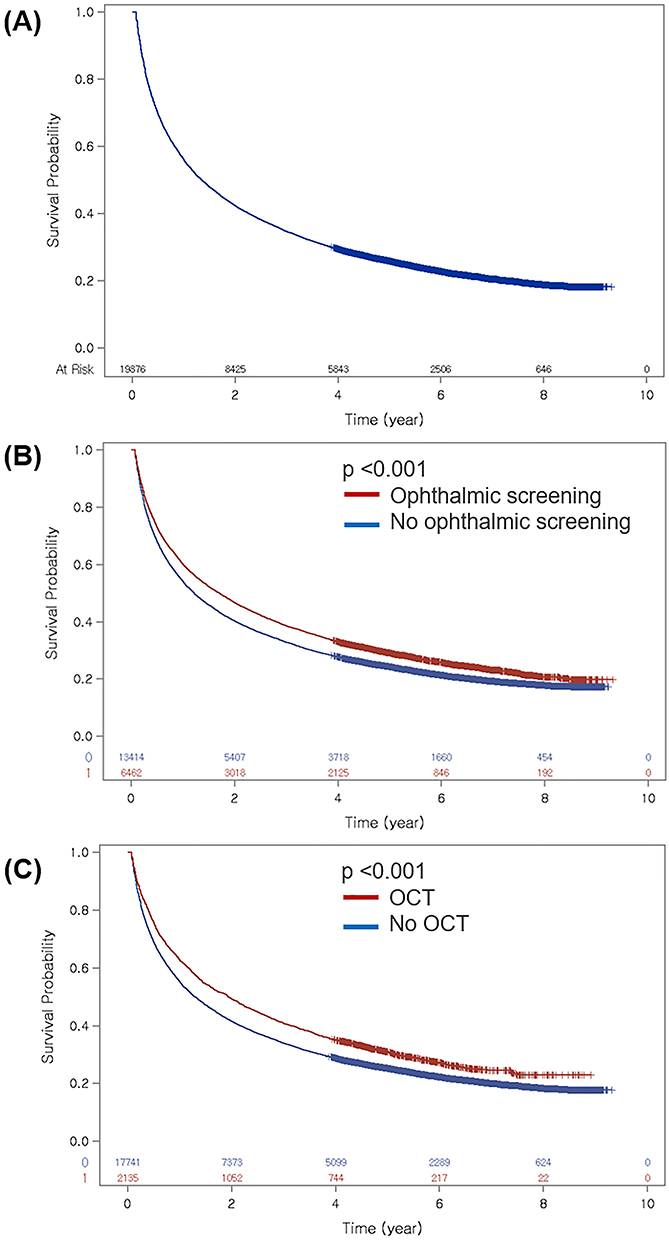 |
Figure 3 Persistence of hydroxychloroquine treatment. (A) Persistence of hydroxychloroquine in all study patients. (B) Comparison of hydroxychloroquine persistence according to baseline ophthalmic screening. (C) Comparison of hydroxychloroquine persistence according to baseline optical coherence tomography. |
Discussion
In this nationwide cohort study of Korean patients with RDs initiating HCQ, fewer than one-third completed a baseline ophthalmic screening examination within the first year of treatment. Despite established AAO recommendations advocating retinal evaluation prior to long-term HCQ use, our findings highlight a substantial disparity between guidelines and real-world care. We identified distinct determinants of adherence; older age, female sex, treatment initiation at tertiary or general hospitals, and a diagnosis of SLE, SS, or Behçet’s disease positively predicted baseline screening. Conversely, patients prescribed concomitant csDMARDs or corticosteroids were considerably less likely to be screened. A key finding was the association between baseline ophthalmic screening and improved long-term HCQ persistence.
The observed screening rate (32.5%) aligns with or falls slightly below the 30–60% range reported in prior research,6,24–26 underscoring a substantial gap between clinical guidelines and practice. Variability in reported rates likely reflects heterogeneity in healthcare systems, patient populations, screening definitions, and ophthalmologic service accessibility. Differences in study design and data sources, particularly the use of administrative claims versus clinical registries, may further contribute to these discrepancies. Collectively, however, evidence indicates that adherence to baseline screening recommendations remains suboptimal across diverse clinical settings. This global shortfall represents a systemic challenge in translating guideline recommendations into routine practice for patients on long-term HCQ therapy.
We identified several clinical and institutional determinants influencing baseline ophthalmic screening. Patients with SLE, SS, and Behçet’s disease were substantially more likely to be screened than those with RA. HCQ is recognized as an essential “anchor drug” in SLE, necessitating stricter adherence to safety monitoring protocols.25,27 In SS, higher screening rates—including the utilization of OCT—likely reflect the frequent need for ophthalmologic co-management due to chronic ocular symptoms such as dry eye. This established routine access to ophthalmic care inherently increases the likelihood of clinicians concurrently performing comprehensive baseline HCQ safety assessments, including structural imaging, during these visits. Similarly, the higher likelihood of screening in Behçet’s disease likely results from established protocols for monitoring disease-related ocular manifestations.28 In RA, where HCQ often serves as adjunctive therapy rather than a core disease-modifying agent, clinicians may perceive the risk of retinal toxicity as lower, contributing to reduced screening adherence. These findings, coupled with higher screening rates in tertiary and general hospitals, highlight the critical role of established referral systems and institutional protocols in improving compliance. Conversely, concomitant glucocorticoid or csDMARDs use predicted a lower screening probability, potentially due to “competing clinical demands” where clinicians prioritize immediate inflammatory control over preventive screening. Nevertheless, baseline evaluation remains vital in this subgroup given the need for prolonged HCQ therapy. Finally, older age and female sex independently predicted baseline screening. While this may partially reflect increased clinician vigilance toward older populations perceived to be at greater risk of ocular comorbidities, it is important to acknowledge a key limitation of claims-based data: the inability to determine the specific clinical indication for each exam. Older patients are inherently more likely to undergo ophthalmic evaluations for other common age-related conditions such as cataracts, glaucoma, or floaters. Therefore, some examinations and OCTs captured in this demographic may not have been specifically intended as HCQ baseline screening, potentially overestimating the true screening rate in this subgroup. Additionally, higher adherence among women aligns with their generally higher healthcare utilization and engagement in preventive care,29,30 increasing opportunities for screening completion.
We observed an association between lower absolute HCQ doses (≤ 300 mg) and higher screening rates. However, this finding must be interpreted with caution. Because HCQ dosing is typically determined according to body weight, absolute daily dose alone cannot accurately infer actual toxicity risk. The higher screening rates in the lower-dose group may partially reflect demographic factors; for instance, older patients and women generally have lower body weights and might therefore be prescribed lower fixed daily doses. Furthermore, lower doses are typically prescribed for maintenance in stable patients, providing a window for adherence to safety protocols, whereas higher doses are often required for acute flares, where the urgency of symptom control may overshadow preventive ophthalmic referrals. Importantly, the HIRA database lacks information on body weight, preventing the calculation of weight-based dosing (eg, <5 mg/kg). Therefore, we could not determine whether the lower doses represented appropriate weight-adjusted prescriptions or fixed dosing, which remains a limitation in interpreting this association. Furthermore, while the starting dose is reported as a continuous mean value in our baseline characteristics, HCQ is typically prescribed in fixed daily doses. The lack of a categorical dose distribution in Table 1 is a limitation arising from our retrospective data extraction and access constraints, although we addressed this in our outcome models by utilizing categorical dose thresholds.
A major finding was the independent association between baseline ophthalmic screening and improved long-term HCQ persistence. Patients completing any baseline screening had a 9% lower risk of discontinuation; this protective effect was consistently observed in those receiving OCT. Although the observational design precludes causal inference, the association between screening and persistence remained robust after adjusting for hospital type, prescribing department, and comorbidities. Rather than implying a direct causal effect of the screening procedure itself, this association likely positions baseline screening as a potential proxy for structured care pathways and active patient engagement. Several mechanisms may explain this association. First, baseline testing establishes a “safety reference point.” Retinal toxicity is a major concern for patients and physicians, often prompting premature withdrawal at the first sign of visual symptoms. A documented normal baseline—especially via objective imaging like OCT—provides the reassurance necessary to continue therapy, preventing unnecessary discontinuation due to non-specific visual changes.1,9,31 Second, the referral may function as a critical educational and engagement encounter. It reinforces the importance of HCQ as a long-term treatment and fosters a “healthy adherer” effect, reflecting that patients who proactively participate in safety monitoring are inherently more likely to adhere to their medication regimen.26 Our results suggest that integrating ophthalmic screening into the care pathway serves as a marker of comprehensive management that supports the therapeutic success of HCQ.
Several limitations warrant acknowledgment. First, we operationally defined screening using claims-based codes for fundoscopy and OCT performed within one year of HCQ initiation. Although guidelines recommend additional modalities (VF testing, FAF, mfERG), we excluded these from our definition. Although some claims-based studies have included VF, FAF, or mfERG,6,9,26 reliable identification of their screening intent remains limited in administrative databases because of inconsistent coding, heterogeneity in protocols, and difficulty distinguishing screening from symptom-driven evaluations.9,32,33 We therefore focused on structural screening modalities (fundoscopy, OCT) which are reliably captured in administrative data, although this may underestimate the true prevalence of comprehensive screening. Second, baseline screening was operationally defined as examinations performed within 12 months of HCQ initiation. It is important to consider that this 12-month window, while intended to reflect pragmatic delays in real-world clinical practice, may include a broader range of clinical encounters. For instance, examinations performed toward the end of this period could potentially represent delayed referrals, early routine monitoring, or evaluations prompted by incidental ocular symptoms rather than strict baseline assessment. While this definition allows for a comprehensive capture of initial safety surveillance, the possibility of including tests with varying clinical intents should be considered when interpreting these findings. Nevertheless, the consistent association observed suggests that early integration of ophthalmic care remains a significant factor in long-term treatment persistence. Third, claims data lack detailed clinical information (eg, baseline visual symptoms, pre-existing ocular disease, weight-based dosing, patient preferences) that may influence screening uptake and persistence. Although we adjusted for measured confounders, residual confounding from unmeasured factors cannot be excluded. Importantly, misclassification related to screening modality or timing is likely non-differential, tending to bias observed associations toward the null rather than spuriously exaggerating the protective effect. Fourth, our inclusion criterion required a minimum of 30 consecutive days of HCQ therapy. While this threshold successfully excluded transient users, 30 days does not fully represent the “long-term” exposure typically associated with retinal toxicity. Nevertheless, this pragmatic definition captures the critical initial window during which baseline screening decisions and referrals are typically made by prescribing physicians. Finally, as this study utilized data from a single-payer national health insurance system in South Korea, findings regarding healthcare utilization behaviors may have limited generalizability to countries with multi-payer or private insurance-based healthcare systems.
Conclusion
In summary, this nationwide cohort study found that fewer than one-third of patients with RDs initiating HCQ completed baseline ophthalmic screening within the first year, underscoring a substantial disparity between guidelines and practice. Screening uptake varied by demographics, healthcare setting, and underlying RD, suggesting that patient- and system-level factors contribute to adherence. Importantly, baseline ophthalmic screening—particularly utilizing objective imaging such as OCT—was independently associated with improved long-term HCQ persistence. These findings suggest that baseline ophthalmic screening may serve as a potential surrogate marker for comprehensive clinical management, which is closely associated with sustained HCQ therapy.
Funding
This study was supported by Biomedical Research Institute Grant (20230191), Pusan National University Hospital.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Ahn SJ, Kim JH. Causes and trends of late diagnosis in Korean patients with hydroxychloroquine retinopathy. Front Med. 2023;10:1238226. doi:10.3389/fmed.2023.1238226
2. Lee SG, Park EK, Park JH, Kweon SM, Kim YK, Kim GT. Compliance and persistence with hydroxychloroquine in South Korean patients with systemic lupus erythematosus. Lupus. 2018;27(5):753–18. doi:10.1177/0961203317742712
3. Nirk EL, Reggiori F, Mauthe M. Hydroxychloroquine in rheumatic autoimmune disorders and beyond. EMBO Mol Med. 2020;12(8):e12476. doi:10.15252/emmm.202012476
4. Ahn SJ, Lee BR. Hydroxychloroquine Retinopathy Update. J Rheum Dis. 2018;25(3). doi:10.4078/jrd.2018.25.3.153
5. Yusuf IH, Charbel Issa P, Ahn SJ. Hydroxychloroquine-induced retinal toxicity. Front Pharmacol. 2023;14:1196783. doi:10.3389/fphar.2023.1196783
6. Kato K, Shinoda K, Yokogawa N, Tajima T, Takahashi T, Kondo M. A real-world descriptive study of screening practices for hydroxychloroquine retinopathy in Japan using an insurance claims database. Sci Rep. 2025;15(1):12330. doi:10.1038/s41598-025-96579-2
7. Marmor MF, Kellner U, Lai TY, Melles RB, Mieler WF; American Academy of O. Recommendations on screening for chloroquine and hydroxychloroquine retinopathy (2016 Revision). Ophthalmology. 2016;123(6):1386–1394. doi:10.1016/j.ophtha.2016.01.058
8. Płatkowska B, Kal M, Biskup M. Optical coherence tomography angiography – use in ophthalmological practice. Med Stud. 2020;36(3):195–205. doi:10.5114/ms.2020.99541
9. Kim J, Kim KE, Kim JH, Ahn SJ. Practice patterns of screening for hydroxychloroquine retinopathy in South Korea. JAMA Network Open. 2023;6(5):e2314816. doi:10.1001/jamanetworkopen.2023.14816
10. Yen CY, Lee PH, Yen JC, Chen CC, Hu HY, Tseng PC. Current screening practice in patients under long-term hydroxychloroquine medication in Taiwan: a nationwide population-based cohort study. Medicine. 2019;98(14):e15122. doi:10.1097/MD.0000000000015122
11. Park JS, Lee CH. Clinical study using healthcare claims database. J Rheum Dis. 2021;28(3):119–125. doi:10.4078/jrd.2021.28.3.119
12. Won S, Cho SK, Kim D, et al. Update on the prevalence and incidence of rheumatoid arthritis in Korea and an analysis of medical care and drug utilization. Rheumatol Int. 2018;38(4):649–656. doi:10.1007/s00296-017-3925-9
13. Bae EH, Lim SY, Han KD, et al. Trend of prevalence and incidence of systemic lupus erythematosus in South Korea, 2005 to 2015: a nationwide population-based study. Korean J Intern Med. 2020;35(3):652–661. doi:10.3904/kjim.2018.303
14. Kim H, Cho SK, Kim JW, et al. An increased disease burden of autoimmune inflammatory rheumatic diseases in Korea. Semin Arthritis Rheum. 2020;50(3):526–533. doi:10.1016/j.semarthrit.2019.11.007
15. Bae KH, Hong JB, Choi YJ, et al. Association of congestive heart failure and death with ankylosing spondylitis: a nationwide longitudinal cohort study in Korea. J Korean Neurosurg Soc. 2019;62(2):217–224. doi:10.3340/jkns.2018.0110
16. Hwang JJ, Shin SH, Kim YJ, et al. Epidemiology of antiphospholipid syndrome in Korea: a nationwide population-based study. J Korean Med Sci. 2020;35(5):e35. doi:10.3346/jkms.2020.35.e35
17. Ahn JK, Hwang J, Seo GH. Incidence and risk of developing rheumatic diseases in 19,724 patients with palindromic rheumatism in South Korea: a nationwide population-based study. Joint Bone Spine. 2021;88(3):105128. doi:10.1016/j.jbspin.2020.105128
18. Lee YB, Lee JH, Lee SY, et al. Association between smoking and Behcet’s disease: a nationwide population-based study in Korea. J Eur Acad Dermatol Venereol. 2019;33(11):2114–2122. doi:10.1111/jdv.15708
19. Ahn SS, Han M, Yoo J, et al. Risk of cancers in antineutrophil cytoplasmic antibody-associated vasculitis: results from the Korea National Health Insurance Claims Database 2010–2018. J Clin Med. 2019;8(11). doi:10.3390/jcm8111871
20. Park SJ, Kim HJ, Park H, et al. Incidence, prevalence, mortality and causes of death in Takayasu Arteritis in Korea - A nationwide, population-based study. Int J Cardiol. 2017;235:100–104. doi:10.1016/j.ijcard.2017.02.086
21. Ji J, Dimitrijevic I, Sundquist J, Sundquist K, Zoller B. Risk of ocular manifestations in patients with giant cell arteritis: a nationwide study in Sweden. Scand J Rheumatol. 2017;46(6):484–489. doi:10.1080/03009742.2016.1266030
22. Nossent J, Raymond W, Keen H, Preen DB, Inderjeeth CA. Adult-onset still’s disease in Western Australia: epidemiology, comorbidity and long-term outcome. Int J Rheum Dis. 2022;25(11):1306–1314. doi:10.1111/1756-185X.14424
23. Charlson ME, Pompei P, Ales KL, MacKenzie CR. A new method of classifying prognostic comorbidity in longitudinal studies: development and validation. J Chronic Dis. 1987;40(5):373–383. doi:10.1016/0021-9681(87)90171-8
24. Nika M, Blachley TS, Edwards P, Lee PP, Stein JD. Regular examinations for toxic maculopathy in long-term chloroquine or hydroxychloroquine users. JAMA Ophthalmol. 2014;132(10):1199–1208. doi:10.1001/jamaophthalmol.2014.1720
25. Islam YFK, Stroman WR, Steigleman WA. Compliance with hydroxychloroquine screening guidelines at a large academic medical center. J Vitreoretin Dis. 2022;6(4):271–277. doi:10.1177/24741264221097806
26. Kim J, Jeong HC, Kwon HY, Kim YH, Ahn SJ. Demographic and clinical characteristics associated with screening practices for hydroxychloroquine retinopathy. Sci Rep. 2024;14(1):974. doi:10.1038/s41598-024-51667-7
27. Han JY, Cho SK, Sung YK. Epidemiology of systemic lupus erythematosus in Korea. J Rheum Dis. 2023;30(4):211–219. doi:10.4078/jrd.2023.0037
28. Zajac H, Turno-Krecicka A. Ocular manifestations of behcet’s disease: an update on diagnostic challenges and disease management. J Clin Med. 2021;10(21). doi:10.3390/jcm10215174
29. Golinelli D, Sanmarchi F, Guarducci G, et al. Gender differences in healthcare utilization across Europe: evidence from the European Health Interview Survey. Health Policy. 2025;162:105448. doi:10.1016/j.healthpol.2025.105448
30. Redondo-Sendino A, Guallar-Castillon P, Banegas JR, Rodriguez-Artalejo F. Gender differences in the utilization of health-care services among the older adult population of Spain. BMC Public Health. 2006;6:155. doi:10.1186/1471-2458-6-155
31. Eo DR, Lee MG, Ham DI, et al. Frequency and clinical characteristics of hydroxychloroquine retinopathy in Korean patients with rheumatologic diseases. J Korean Med Sci. 2017;32(3):522–527. doi:10.3346/jkms.2017.32.3.522
32. Ahn SJ. Real-world research on retinal diseases using health claims database: a narrative review. Diagnostics. 2024;14(14). doi:10.3390/diagnostics14141568
33. Stein JD, Lum F, Lee PP, Rich WL 3rd, Coleman AL. Use of health care claims data to study patients with ophthalmologic conditions. Ophthalmology. 2014;121(5):1134–1141. doi:10.1016/j.ophtha.2013.11.038
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.