Back to Journals » Journal of Multidisciplinary Healthcare » Volume 19
Determinants Associated with Psychological Well-Being Among Children and Adolescents with Acute Lymphoblastic Leukemia Undergoing Chemotherapy
Authors Alya FP ![]() , Hendrawati S
, Hendrawati S ![]() , Yuliar TP, Nurhayati S, Mediani HS
, Yuliar TP, Nurhayati S, Mediani HS ![]()
Received 1 October 2025
Accepted for publication 21 January 2026
Published 2 February 2026 Volume 2026:19 570849
DOI https://doi.org/10.2147/JMDH.S570849
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Jagdish Khubchandani
Fania Putri Alya,1,2 Sri Hendrawati,3 Triliana Purwadesi Yuliar,4 Sri Nurhayati,5 Henny Suzana Mediani3
1Posgraduated Nursing Program, Faculty of Nursing, Universitas Padjadjaran, Sumedang, West Java, Indonesia; 2Faculty of Health Science, Universitas Bhakti Kencana, Bandung, West Java, Indonesia; 3Department of Pediatric Nursing, Faculty of Nursing, Universitas Padjadjaran, Sumedang, West Java, Indonesia; 4Pediatric Nurse, Nursing Department, Hasan Sadikin Provincial General Hospital, Bandung, West Java, Indonesia; 5Pediatric Nurse, Nursing Department, Al-Islam Hospital, Bandung, West Java, Indonesia
Correspondence: Henny Suzana Mediani, Department of Pediatric Nursing, Faculty of Nursing, Universitas Padjadjaran, Sumedang, West Java, Indonesia, Fax +62227795596, Email [email protected]
Background: Psychological well-being (PWB) plays a vital role in quality of life and psychological resilience, particularly in children undergoing intensive treatments such as chemotherapy. Children with acute lymphoblastic leukemia (ALL), especially during school age and adolescence, often experience emotional and physical stress related to fear, anxiety, and uncertainty about disease prognosis and long-term outcomes.
Purpose: This study aimed to identify factors associated with PWB among children with ALL undergoing chemotherapy.
Methods: A cross-sectional study was conducted among 66 children aged 8– 18 years with ALL undergoing chemotherapy, recruited via convenience sampling. Data were collected using a checklist, the Children’s Worlds Psychological Well-Being Scale (CW-PWBS), a family support questionnaire, and the Children’s Hope Scale (CHS). Data analysis included univariate analysis, bivariate analysis using Pearson and Spearman’s rho, and multivariate analysis using ordinal logistic regression.
Results: Most respondents (51.1%) had high PWB, whereas almost half (48.9%) had low PWB. Factors associated with PWB include age at diagnosis (p=0.015; r=− 0.298), duration of therapy (p=0.002; r=0.371), family support (p=0.004; r=0.347), and hope (p< 0.001; r=0.519). The results of multivariate analysis showed that the factor most associated with PWB in children aged 8– 18 years with ALL undergoing chemotherapy was family support (OR=11.36; 95% CI=1.540– 83.86; p=0.017).
Conclusion: Nearly half of children with ALL undergoing chemotherapy still experience low PWB. Age at diagnosis, therapy duration, family support, and hope are essential predictors influencing PWB, with family support as the most dominant predictor. These findings highlight the critical role of pediatric nurses in providing holistic, family-centered care, with an emphasis on psychosocial support to enhance PWB among children undergoing chemotherapy.
Keywords: acute lymphoblastic leukemia, children, family support, hope, psychological well-being
Introduction
The threat of cancer continues to increase as the number of sufferers increases, not only in adults but also in children.1 WHO estimates that ±400,000 children and adolescents aged 0–19 years are diagnosed with cancer every year.2 Based on data documented in the Indonesian Pediatric Center Registry (2022), there were 3834 new cases of childhood cancer detected during the 2021–2022 period.3 The most common childhood cancers are ALL (Acute Lymphoblastic Leukemia), retinoblastoma, osteosarcoma, brain cancer, lymphoma, neuroblastoma, and Wilms’ tumor.4–7
Chemotherapy is also an effective method for treating childhood cancer. While it has therapeutic effects that can inhibit the growth of cancer cells, chemotherapy can also cause potentially dangerous side effects and require treatment.8,9 However, the effects of chemotherapy treatment are not only physical, but also have severe psychological and social impacts related to a decrease in the quality of life and psychological well-being of patients undergoing it.10–12 Previous studies reported that approximately 14% of children with ALL experience anxiety with severity varying from mild to severe.12 In addition, 21% of them experienced depression, and 30% faced distress.12 In the context of the psychosocial dimension, children with cancer have significant concerns related to feelings of isolation.13
Psychological well-being (PWB) is a state where individuals can accept themselves in both positive and negative aspects, have healthy relationships with others, direct themselves, control their environment, and have clear life goals.14 According to Ryff (2013), psychological well-being is defined based on the extent to which a person has a goal in his life, whether they are aware of their potential, the quality of their relationships with other people, and the extent to which they are responsible for their own life.15 Children with cancer undergoing chemotherapy have a higher risk of experiencing depressive symptoms, withdrawing from their environment, and losing hope, so they have low levels of PWB. PWB levels can also influence how well children with cancer adhere to their treatment.16,17 Previous study has concluded that low PWB can be a barrier to medication adherence.16–18 Therefore, it is important to pay attention to the factors causing low levels of PWB in children with chronic diseases because this helps in developing more effective interventions to improve children’s quality of life.19
Several factors influence the PWB of children with chronic diseases.20 Several previous studies stated that predictors that influence PWB in children with cancer that have not been widely studied, especially in Indonesia, include age at diagnosis, phase of therapy, and duration of treatment.19–25 Age at diagnosis can influence PWB, where younger children have a limited understanding of the disease and its treatment process, leading to anxiety and uncertainty in undergoing painful and challenging treatment.17,19,20,25 There are also factors in the therapy phase that can cause severe side effects that not only affect the child physically, but also harm the child’s PWB.20,23,24 In addition, the duration of therapy or the length of cancer treatment is often a long process, and it is not always clear how long it will last. Uncertainty regarding treatment duration and outcomes can create anxiety and stress in both patients and their families, which can ultimately affect PWB.17,20,26
Family support and hope are other factors that may influence PWB in children with cancer, but research on them is still limited.13,20,27 Support from family, including parents and siblings, as well as from wider social networks, can significantly influence children’s PWB.20,28,29 The role of parents during chemotherapy treatment of children with ALL is crucial. Family support can provide positive emotions, emotional support, and a sense of appreciation, which can help improve PWB.17,27 In addition, hope is an essential element in preventing psychological disorders and increasing positive well-being in cancer patients of all ages.23 Life expectancy of children with psychiatric disorders is shorter than that of those who can overcome the condition. Therefore, it is vital to assess the hope of childhood cancer survivors to better understand their responses to stress and difficulties after surviving the disease.23,30
Based on this explanation, this research is vital to identify PWB factors in children with ALL, as it is the most common type of cancer in children. This study was conducted on children with ALL aged 8–18 years, who experience significant physical, emotional, and social changes that can influence PWB.31 School-aged children entering adolescence are typically cognitively mature enough to understand questions about PWB.32,33 According to Erik Erikson’s developmental theory, children in this age range are in the stages of industry vs inferiority and identity vs identity confusion, during which they begin to develop a sense of self-identity and seek social acceptance.34 Therefore, children with chronic illnesses and undergoing intensive treatment such as chemotherapy can have a significant impact on psychological development at this age.35 This study addresses an important gap in the literature by specifically examining psychological well-being and its associated clinical and psychosocial factors in children with ALL. Unlike previous studies that have predominantly focused on quality of life, this research focuses on psychological well-being and clarifies the factors most strongly associated with PWB.
Materials and Methods
Study Design
This study is quantitative, employing a cross-sectional design and multivariate analysis to examine factors influencing PWB among children aged 8–18 years with ALL undergoing chemotherapy. The independent variables: age of diagnosis, phase of therapy, duration of treatment, family support, and hope. In addition, the dependent variable, or the variable of interest in this study, was PWB. This study was conducted at two of the referral hospitals in West Java, Indonesia.
Sample and Setting
The population was 79 pediatric patients aged 8–18 years with ALL undergoing chemotherapy. The sampling technique used in this study was convenience sampling of pediatric patients with ALL aged 8–18 years undergoing chemotherapy. The choice of convenience sampling was based on the researcher’s ability to reach subjects and the availability of participants. The sample size for this study was calculated using the Slovin Formula, which is used to determine the appropriate sample size in research.36 A total of 66 patients were ultimately enrolled in the study, which met the sample size calculated using the Slovin formula. With a total population of 79 pediatric patients, the required sample size was determined using this formula, and a final sample of 66 participants corresponds to an estimated margin of error of approximately 5%.
The sample in this study had the following inclusion criteria: (1) children aged 8–18 years with acute lymphoblastic leukemia; (2) undergoing chemotherapy treatment; (3) in the induction, consolidation, and maintenance phases; (4) patients undergoing treatment and being awaited by their parents; (5) parents/guardians signed an informed consent form to participate as respondents. In addition, the exclusion criteria included: (1) children with intellectual disability, (2) children who were unable to communicate verbally, (3) children with unstable physical or hemodynamic conditions, and did not allow for data collection.
Instrument
This study used several instruments to measure independent and dependent variables. Therefore, each variable has its own measurement instrument. The instruments used in this study are: (1) Checklist sheet, (2) The Children’s Worlds Psychological Well-Being Scale (CW-PWBS) developed by Borualogo and Casas32 In the Indonesian version, (3) Family support questionnaire developed by Nursalam (2017) in Hermono,29 (4) Children Hope Scale adapted by Silfiasari and Varlina37 in the Indonesian version. The three questionnaires used in this study were valid and reliable. The analysis results showed that the Indonesian version of the CW-PWBS was valid (CFI> 0.950, RMSEA < 0.05, SRMR < 0.05) and reliable (α = 0.809), with retest reliability ranging from 0.384 to 0.737.32 The family support questionnaire was valid, with an r count of 0.359–0.989, and reliable, with an α value> 0.6.29 Likewise, the Children Hope Scale (CHS) was valid, with an r count of 0.71–0.88, and reliable, with an α value of 0.90.37 Thus, all instruments were shown to be valid and reliable and therefore suitable for use in this study.
Data Collection
Data collection was conducted over two months (October - November 2024) following submission of a research permit application and receipt of Ethical Clearance. Next, the researcher coordinated with the head of the children’s ward at the relevant hospital to take research samples from children with ALL aged 8–18 years who were undergoing chemotherapy.
During data collection, the researcher first explained the research objectives, benefits, and procedures to parents and children. Then, the researcher provided the child and the child’s parents with an informed consent form and allowed them time to consider their willingness. If the patient and parents agreed to participate, the parents were asked to sign the consent form. Subsequently, the researcher collected data by administering checklist sheets and questionnaires to the children, visiting each respondent in the treatment room individually. For younger children, such as those aged 8–12 years, completing the questionnaire was accompanied and guided directly by the researcher.
Meanwhile, adolescents aged 13–18 completed the questionnaires themselves but were still accompanied by the researcher. The researcher also collected data using a pediatric chemotherapy monitoring form on age at diagnosis, phase of therapy, and duration of treatment. Once all the required data was complete, the researcher proceeded to the data processing stage.
Data Analysis
In this study, data analysis methods included univariate, bivariate, and multivariate. Univariate analysis presents frequency distribution tables and measures of central tendency. Bivariate analyses were performed using Pearson correlation to examine the relationships between age at diagnosis, family support, hope, and PWB, as these variables were normally distributed. For the variables of phase and duration of therapy, Spearman’s rho was used because the data were not normally distributed, as indicated by a Kolmogorov–Smirnov p<0.05. Multivariate analysis was performed using a binary logistic regression test with a backward approach. This method can identify confounding variables by examining a 10% change in the OR.
Ethical Consideration
This research has obtained ethical approval from the Research Ethics Committee of dr. Hasan Sadikin General Hospital, Bandung, with number DP.04.03/D.XIV.6.5/464/2024 in accordance with the guidelines of the Declaration of Helsinki. This study adheres to the ethical principle of anonymity, whereby the researcher will not include respondents’ names and will record only their initials on the data collection sheet. Confidentiality principles are also applied, whereby the researcher guarantees the confidentiality of respondents’ data by not disseminating it and by storing it only in the researcher’s personal database, accessible only to the researcher. Furthermore, Beneficence and Non-Maleficence are also used in this study to maintain the comfort of respondents, both physically, psychologically, and socially, by conducting atraumatic research.
Results
Characteristic of the Study
According to Table 1, most respondents were aged 8–12 years (56.1%) and were male (59.1%). The most common type of ALL was ALL-HR (89.4%). In addition, the majority of respondents were diagnosed at school age (66.7%), and most were currently in the maintenance phase of therapy (51.5%). Furthermore, most respondents had undergone treatment for ≤2 years (75.8%).
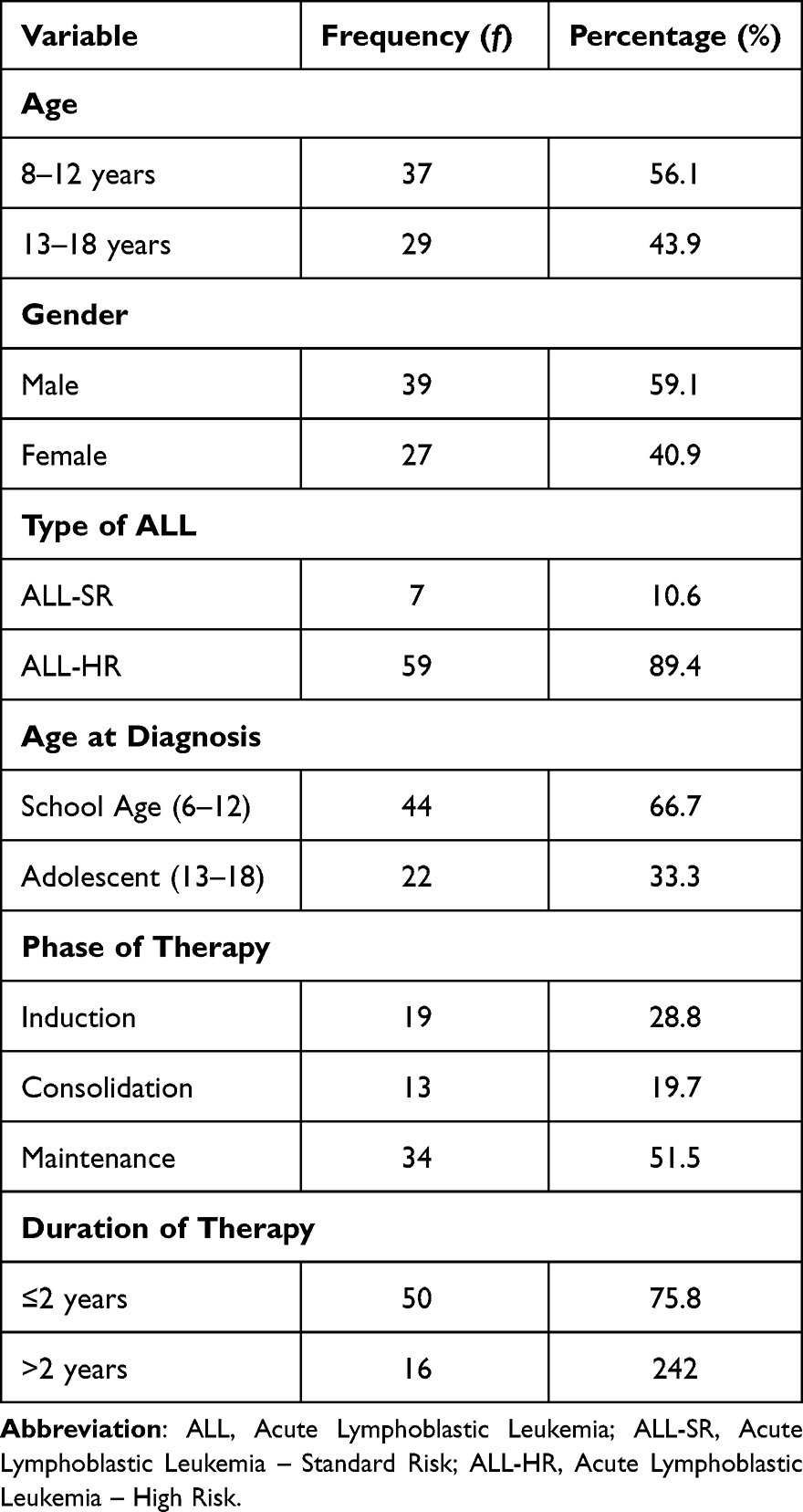 |
Table 1 Demographic Characteristics (n=66) |
PWB of Children Aged 8–18 Years with ALL Undergoing Chemotherapy
Most respondents reported a high level of PWB (51.1%). However, nearly half (48.5%) still experienced low PWB. Regarding family support, most respondents (81.8%) reported high levels, whereas a smaller proportion (18.2%) reported low levels. In addition, more than half of the respondents (54.5%) reported high hope, whereas 45.5% reported low hope. Among school-aged children (8–12 years), 34.8% reported high levels of PWB, compared to 16.7% among adolescents (13–18 years). In contrast, a higher proportion of adolescents reported low PWB (27.3%) compared to school-aged children (21.2%). These findings suggest that adolescents may experience greater psychological challenges, potentially related to the impact of cancer treatment (see Table 2).
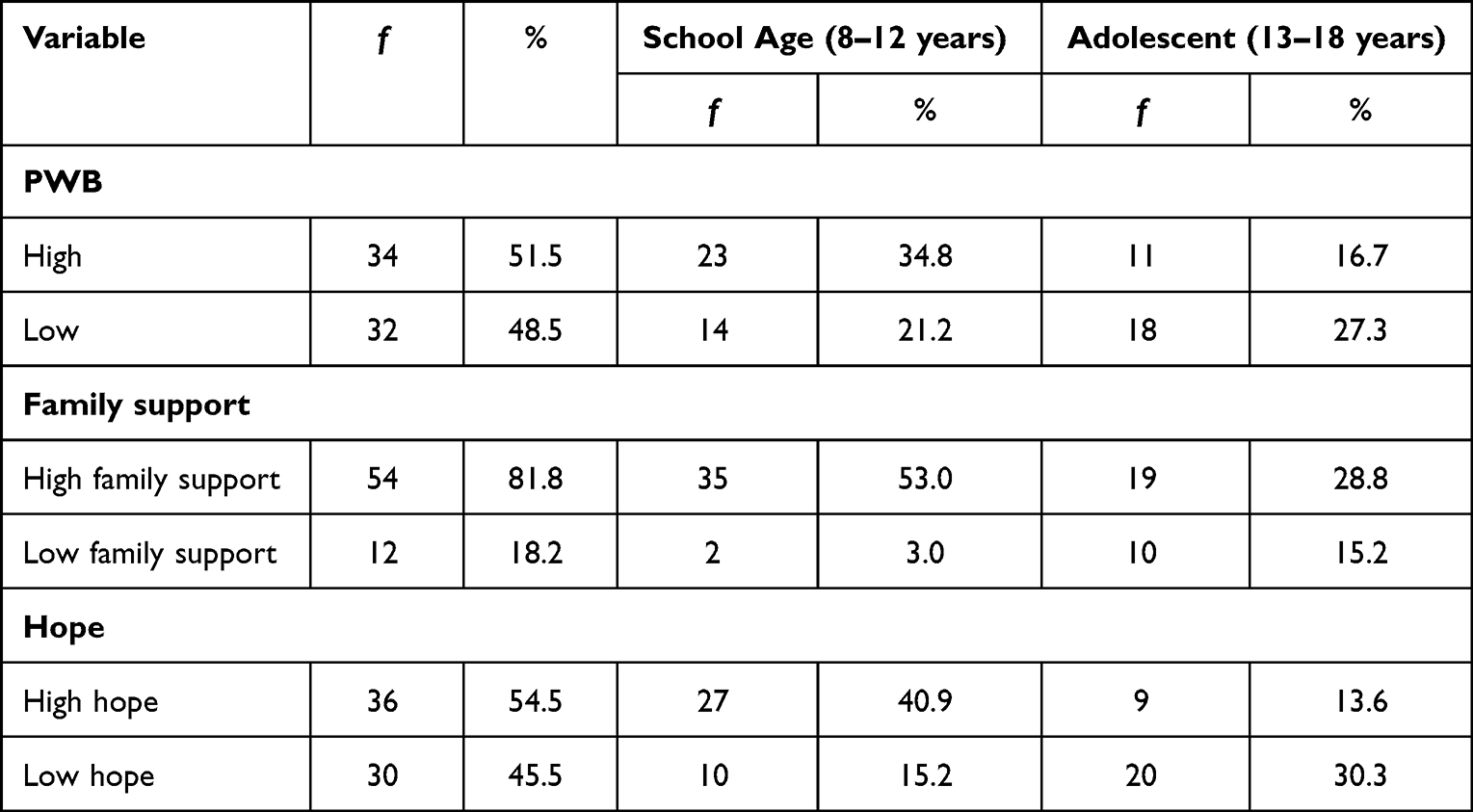 |
Table 2 PWB Levels, Family Support, and Expectations by Age Group (n=66) |
Relationship Between Independent Variables with PWB Among Children Aged 8–18 Years with ALL Undergoing Chemotherapy
Based on the crosstabulation results, Table 3 presents the bivariate analysis of the relationships between the independent variables and PWB. The findings indicate that several factors were significantly associated with PWB in children with cancer, such as age at diagnosis, which was significantly associated with PWB (p = 0.015, r = −0.298). Duration of therapy also showed a significant association with PWB (p = 0.002, r = 0.371), where the results showed that children who had undergone chemotherapy for a shorter duration (≤2 years) reported higher levels of PWB compared to those who had a longer duration of therapy (>2 years). Family support was significantly associated with PWB (p = 0.004, r = 0.347), indicating that higher levels of family support were associated with better PWB. In addition, hope showed a strong and significant association with PWB (p < 0.001, r = 0.519), with higher levels of hope associated with better PWB. In contrast, the therapy phase was not significantly associated with PWB (p = 0.155) and showed a very weak negative correlation (r = −0.177) (see Table 3).
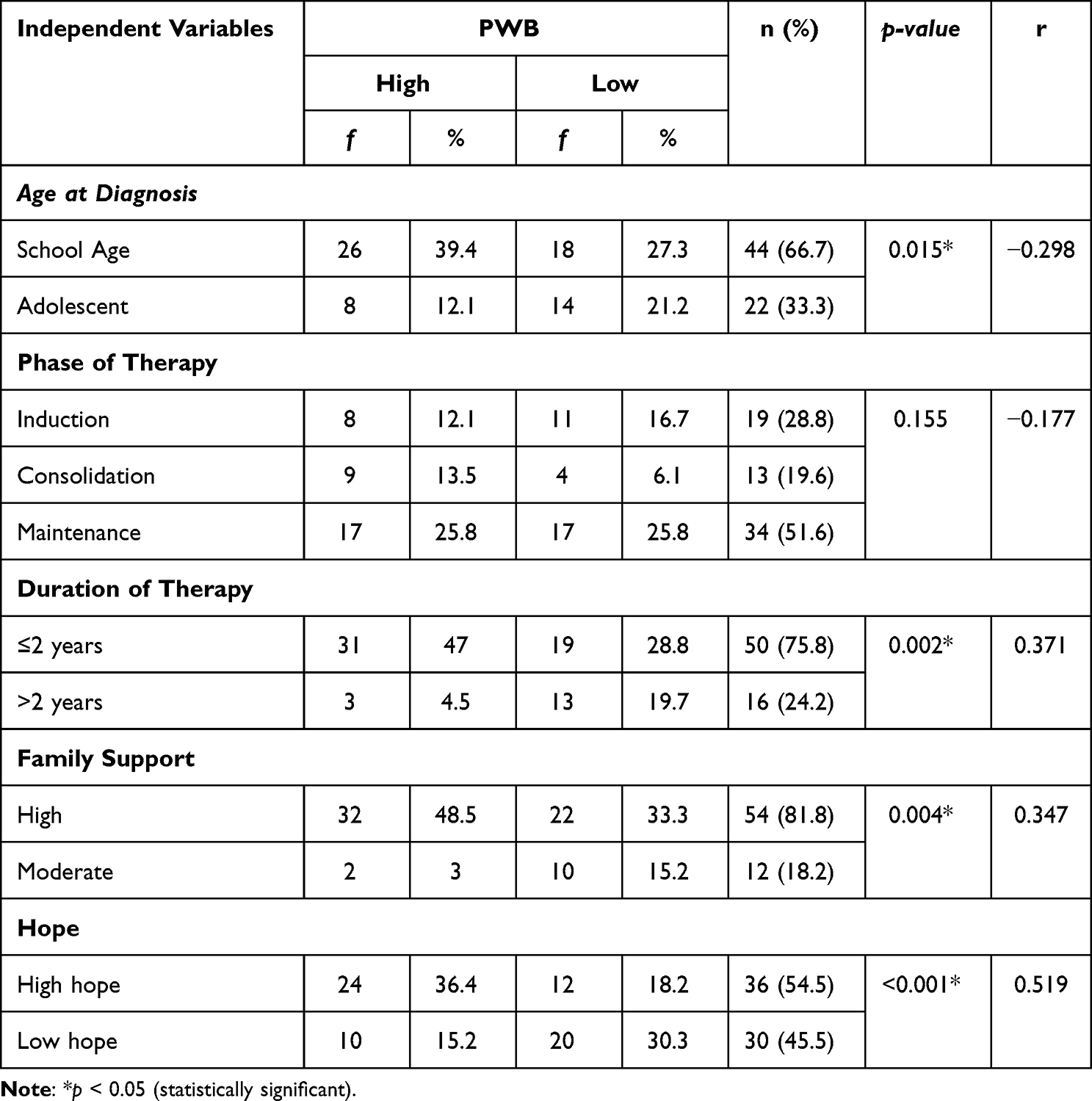 |
Table 3 The Relationship Between Independent Variables and PWB of Children Aged 8–18 Years with ALL (n=66) |
Predictors of PWB Among Children Aged 8–18 Years with ALL Undergoing Chemotherapy
The final multivariate analysis, presented in Table 4, shows the results of the logistic regression used to identify the strongest predictors of PWB. The study identified four predictors associated with PWB: therapy phase, therapy duration, family support, and hope. This model accounted for 46.2% of the variance in PWB among children aged 8–18 years with ALL, with the remaining 53.8% attributable to factors not examined in this study (see Table 4).
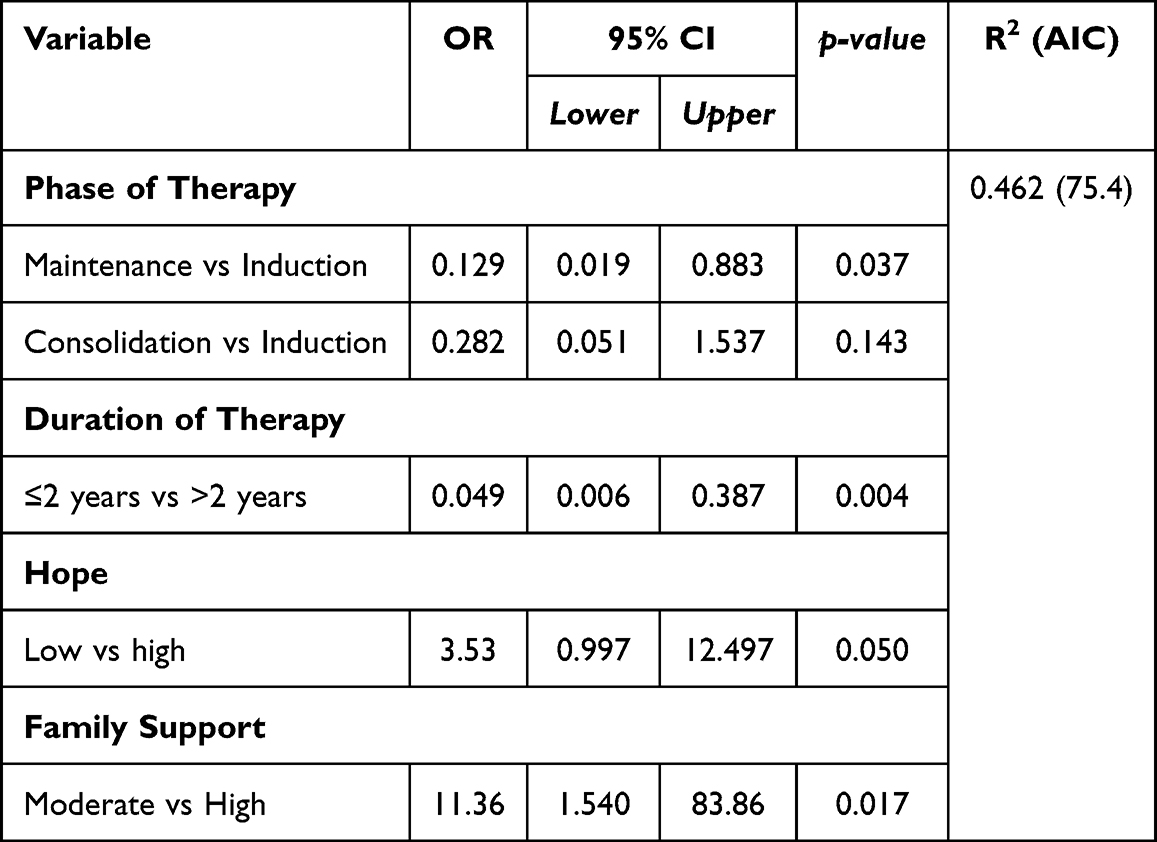 |
Table 4 Analysis of Factors Most Related to PWB of Children Aged 8–18 Years with ALL (n=66) |
Among the identified predictors, family support emerged as the strongest predictor of PWB (OR = 11.36; 95% CI = 1.540–83.86; p = 0.017). This indicates that children with high family support were 11.36 times more likely to have high PWB compared to those with low or moderate family support. Hope was the second strongest predictor (OR = 3.53; 95% CI = 0.997–12.497; p = 0.050), indicating that children with high hope were 3.53 times more likely to report high PWB than those with low hope. Regarding therapy phase, children in the maintenance phase had significantly lower odds of achieving high PWB compared to those in the induction phase (OR = 0.129; 95% CI = 0.019–0.883; p = 0.037). In contrast, the consolidation phase was not significantly associated with PWB compared with the induction phase (OR = 0.282; 95% CI = 0.051–1.537; p = 0.143). Children with a therapy duration of ≤2 years had significantly lower odds of low psychological well-being than those with a therapy duration>2 years (OR = 0.049; 95% CI = 0.006–0.387; p = 0.004). (see Table 4).
Discussion
Children’s PWB should be a key concern for both healthcare professionals and parents. Children who have good levels of PWB can help them cope with stress, anxiety, and uncertainty associated with their medical condition.17,25,38 Conversely, when children with cancer have low levels of PWB, they are at risk of experiencing barriers to adherence to treatment for children with cancer.17,39
Based on the research results, the majority (51.5%) of respondents had high levels of PWB. However, almost half (48.5%) of respondents, namely children with ALL aged 8–18 years, had low levels of PWB. High levels of PWB (39.4%) predominated among school-age children, whereas low levels (21.2%) were observed among adolescents. Low levels of PWB can vary across age groups and are higher in adolescents. School-age children may be unable to express their physical and psychological symptoms adequately. Conversely, adolescents are more likely to express their anxieties about treatment, death, and difficulties in adjusting to school life, as well as experiencing depressed mood, compared to younger children. Thus, adolescents are more likely to be diagnosed with lower PWB levels.22
Each child with cancer undergoing chemotherapy faces different physical and psychological challenges, depending on their age at diagnosis and their psychosocial development at that time. Age at diagnosis has significant implications for a child’s PWB.19 The findings of this research showed that most respondents were diagnosed at school age (6–12 years). Differences in children’s age characteristics are also examined in this study by comparing age at diagnosis between school-age children and adolescents. This factor significantly influences how children face, understand, and manage health conditions. The average age at diagnosis of respondents was 11.5 ± 2.78 years, with an age range of 7 to 16 years. The majority of diagnoses in this study occurred at age 9 years. Similar to previous studies, the majority of ALL cases were diagnosed in children, with a significant number between ages 5 and 9 years.40 The analysis results showed a significant relationship between age at diagnosis and PWB (p=0.015). The developmental stages of school-age children with leukemia are characterized by emotional, psychological, and social challenges influenced by the child’s illness and treatment.17,39,41 Children diagnosed with ALL during adolescence appear to show better psychological adaptation than children diagnosed at a younger age. Children diagnosed at a younger age may experience confusion and fear due to their limited understanding of the disease and medical procedures, which can impact their PWB.17,25
Furthermore, the majority of respondents were in the maintenance therapy phase. Although this phase is considered less physically demanding, the psychological challenges faced by children and adolescents undergoing treatment in the maintenance phase remain significant.42 Although this study found that the majority of respondents were in the maintenance phase, the analysis showed no significant relationship between the phase of therapy and PWB. The negative correlation identified between the therapy phase and the PWB of children with ALL indicates a tendency that the more prolonged or more intensive the therapy phase, the lower the level of PWB reported by the children. Even though children in the maintenance phase are expected to experience physical improvement and reduced symptoms, their psychological conditions varied. Some individuals reported better psychological functioning (high PWB), whereas others remained distressed or experienced a decline in PWB (low PWB). The chemotherapy phase is closely related to the PWB of children with leukemia. Previous studies have reported that the initial phases of chemotherapy, such as the induction phase, have the most significant impact on the PWB of children with cancer.17 This phase, which often involves more intensive treatment and more severe side effects, can pose a variety of emotional and psychological challenges for children.
Another predictor examined in this study was the duration of therapy. Most respondents (75.8%) had undergone chemotherapy for ≤2 years. The results showed a significant association between therapy duration and PWB. Children who had undergone chemotherapy for a shorter duration (≤2 years) reported higher levels of PWB compared to those who had a longer duration of therapy (>2 years). This finding suggests that prolonged treatment duration may increase psychological burden in children with ALL. Long-term exposure to chemotherapy, ongoing hospital visits, treatment-related side effects, and uncertainty about recovery can contribute to emotional distress, anxiety, and feelings of loss of control. Consequently, children undergoing longer courses of therapy may experience lower psychological well-being over time. This highlights the importance of providing continuous psychosocial support, particularly for children undergoing prolonged treatment.21,24
Family support is a significant predictor influencing PWB in children with ALL. In this study, family support was the most significant predictor influencing PWB in children with ALL aged 8–18 years. The analysis yielded an odds ratio (OR) of 11.36 (p = 0.017), indicating that children with ALL undergoing chemotherapy who receive high family support have 11.36 times higher odds of having better PWB than those with lower family support. This finding is also supported by research showing that respondents with high levels of family support predominantly reported high PWB (Table 3). Conversely, those who only received moderate levels of family support, 10 out of 12 respondents, had low levels of PWB. This indicates that family support has a very significant effect on PWB levels in children with ALL undergoing chemotherapy. This is supported by previous studies that stated that high family support is consistent with better levels of PWB in children with cancer.43
Family support influences the PWB of children with chronic illnesses such as cancer because various aspects of family functioning are closely related to the psychological health and well-being of children.44 This suggests that emotional support and positive interactions within the family can help children cope with the challenges posed by chronic illness, thereby improving their overall well-being.44 Family support is a very important factor for children who are struggling with their illness and can motivate them to undergo chemotherapy treatment.45 Family is the best friend for cancer patients in facing the battle with their disease.45 Lack of family support in cancer patients can result in depression and anxiety, which is three times more likely to result in non-adherence to treatment compared to patients who have good support.45 Family support has significant implications for PWB in children with cancer because the family is the primary source of love, attention, and emotional stability for children.46 When children face significant challenges such as a cancer diagnosis and undergo intense medical treatment, the emotional support provided by family members can help them cope with the anxiety, fear, and feelings of helplessness that often arise during the treatment process.46
The final predictor that showed a significant association with PWB was hope (OR = 3.53; 95% CI = 0.997–12.497; p = 0.050). This finding suggests that higher hope is associated with better PWB, with children who reported high hope having 3.53 times the odds of better PWB than those with lower hope. Overall, hope appears to play an essential role in the PWB of children with ALL undergoing chemotherapy. Hope can serve as a coping mechanism that helps children overcome the emotional and psychological difficulties that arise from a diagnosis of a chronic disease like cancer.47 It is also associated with feeling happier, more independent, and more optimistic about the future.48,49 Higher levels of hope correlate with better health-related quality of life, suggesting that fostering hope is critical to improving psychological outcomes in pediatric cancer patients.47 Although the majority of respondents in this study had high levels of hope, nearly half still had low levels of hope. This could be due to several physical and psychological factors related to the treatment process.16,17 Poor physical condition can affect a child’s perception of their situation.16,17 Uncertainty about the future, particularly regarding treatment outcomes and the possibility of disease recurrence, can also lead to a lack of optimism in children. Anxiety about recovery or concerns about the long-term effects of treatment often undermines their self-confidence and prevents them from feeling adequately well.16,17
The final results of this study found that family support is a major factor in determining the level of PWB in children with ALL undergoing chemotherapy for several fundamental reasons. First, cancer treatment in children involves not only medical aspects but also significantly impacts their emotional and PWB. In this context, the family has a critical role in providing an environment full of emotional and practical support.50 When children feel supported and loved by their families, they are better able to cope with the stress and strain that comes with intensive and challenging care.50,51 Second, the family is the primary source of emotional stability for children who face uncertainty and fear related to the cancer diagnosis and the treatment they undergo.50,52 Strong family support not only provides a sense of physical security but can also increase a child’s optimism and hope for recovery.53
Overall, research on PWB in children with cancer undergoing chemotherapy emphasizes the importance of holistic support encompassing emotional, social, and cognitive aspects to help them navigate the challenging treatment journey. Nurses play a critical role in implementing interventions to improve children’s PWB.54 As healthcare professionals who frequently interact directly with patients, nurses can provide ongoing emotional and psychological support and help children manage the challenges that arise during cancer treatment.54 Psychosocial programs implemented by nurses designed to support the mental and emotional well-being of children with cancer can help improve their PWB.54 The program includes play therapy, group support, and counseling sessions that provide space for children to express themselves and understand their condition.54,55 Appropriate support and effective interventions can have a significant positive impact, enabling them to achieve better psychological well-being despite challenging circumstances.
Implications for Practice
The study results indicate that family support, age at diagnosis, duration of therapy, and hope significantly influence the PWB of children with ALL. In pediatric nursing, nurses need to involve families in treatment planning, provide clear information about the stages and side effects of therapy, and implement a family-centered care approach to enhance family support. Strategies such as play therapy, group support, and counseling should be tailored to the child’s age to facilitate self-expression and emotion regulation. In addition, nurses need to monitor the child’s emotional condition throughout therapy, provide ongoing support to reduce stress, and encourage the child’s hope by celebrating each progress achieved. At the healthcare level, hospitals are advised to develop intervention programs that account for children’s age, provide education and counseling for children and families, and organize family support programs, such as counseling sessions and support groups. Hospitals should also create a supportive environment with recreational programs or art therapy to increase children’s motivation and hope during treatment. This approach is expected to improve the child’s overall psychological well-being during therapy.
Strengths and Limitations of This Study
This study has several limitations that should be acknowledged. First, the sample size was relatively small, involving only 66 children with ALL from two hospitals in Bandung, which may not fully represent the broader pediatric oncology populations across different regions or healthcare settings. Nevertheless, the study provides a significant contribution to understanding the PWB of children with ALL undergoing chemotherapy. With a primary focus on an in-depth assessment of PWB, the findings are valid and relevant, particularly in highlighting the crucial role of family support in enhancing children’s PWB. These results provide a valuable foundation for future research, which is recommended to include larger and randomized samples to enhance representativeness. In addition, the findings have practical relevance for pediatric nursing practice, supporting the development of family-centered and psychosocial interventions to improve the psychological well-being of children with ALL throughout their chemotherapy.
Conclusion
Based on the study results, the majority of respondents reported high PWB, although 48.5% still reported low PWB. Factors associated with PWB levels among children with ALL aged 8–18 years identified in this study include age at diagnosis, duration of therapy, family support, and hope. Four predictors were identified as influencing PWB: therapy phase, therapy duration, hope, and family support; family support emerged as the strongest predictor. The family’s provision of positive support can boost children’s motivation and strengthen their connection to the social environment. Consistent family support throughout the treatment process enhances children’s psychological resilience and enables them to maintain a positive attitude, thereby contributing to higher PWB levels. These findings have important implications for pediatric oncology nursing practice, emphasizing the integration of family-centered and psychosocial care into routine nursing interventions. Nurses play a crucial role in assessing PWB, involving families, and fostering hope as part of holistic care. Enhancing PWB during treatment may support better long-term emotional adjustment in children with ALL. Future research is recommended to develop targeted psychosocial and family-based interventions and to examine long-term outcomes using larger and more diverse samples.
Acknowledgments
All authors thank Universitas Padjadjaran for facilitating the database for us and funding in this study.
Disclosure
The authors report no conflicts of interest in this research.
References
1. Van Der Plas E, Erdman L, Nieman BJ, et al. Characterizing neurocognitive late effects in childhood leukemia survivors using a combination of neuropsychological and cognitive neuroscience measures. Child Neuropsychol. 2018;24(8):999–12. doi:10.1080/09297049.2017.1386170
2. World Health Organization. Cancer in children [Internet]. World Health Organization; 2025. Available from: https://www.who.int/news-room/fact-sheets/detail/cancer-in-children.
3. Indonesian Pediatric Cancer Registry. Ada 3.834 Kasus Baru Kanker Anak di Indonesia pada 2021–2022 [Internet]. Data Indonesia; 2023. Available from: https://dataindonesia.id/kesehatan/detail/ada-3834-kasus-baru-kanker-anak-di-indonesia-pada-20212022.
4. American Cancer Society. Types of Cancer That Develop in Children; 2024.
5. Erdmann F, Frederiksen LE, Bonaventure A, et al. Childhood cancer: survival, treatment modalities, late effects and improvements over time. Cancer Epidemiol. 2021;71(PB):101733. doi:10.1016/j.canep.2020.101733
6. National Cancer Institute. Childhood Cancer [Internet]. 2024. Available from: https://www.cancer.gov/types/childhood-cancers.
7. World Health Organization. CureAll framework: WHO global initiative for childhood cancer [Internet]. World Health Organization; 2021. Available from: https://www.who.int/publications/i/item/9789240025271.
8. Herfiana S, Arifah S. Dampak Fisiologis Kemoterapi Pada Anak Dengan Leukemia di Rumah Sakit. J Ber Ilmu Keperawatan. 2019;12(1):1–6. doi:10.23917/bik.v12i1.10583
9. Hockenberry MJ, Wilson D, Rodgers CC. Wong’s Essentials of Pediatric Nursing. Vol. 5.
10. Ridha R, Mardhiyah A, Hidayati NO. Dampak kemoterapi pada anak penderita kanker di rumah cinta bandung. J Keperawatan Aisyiyah. 2017;4(6):Hal33–39.
11. Kızılocak H, Okcu F. Late effects of therapy in childhood acute lymphoblastic leukemia survivors. Turkish J Haematol. 2019;36(1):1–11.
12. Anestin AS, Lippé S, Robaey P, et al. Psychological risk in long-term survivors of childhood acute lymphoblastic leukemia and its association with functional health status: a PETALE cohort study. Pediatr Blood Cancer. 2018;65(11):1–10. doi:10.1002/pbc.27356
13. Li HCW, Chung OKJ, Chiu SY. The impact of cancer on children’s physical, emotional, and psychosocial well-being. Cancer Nurs. 2010;33(1):47–54. doi:10.1097/NCC.0b013e3181aaf0fa
14. Yosep I, Mardhiyah A, Sriati A. Mindfulness intervention for improving psychological wellbeing among students during COVID-19 pandemic: a scoping review. J Multidiscip Healthc. 2023;16(May):1425–37.
15. Ryff CD. Psychological well-being revisited: advances in the science and practice of eudaimonia. Psychother Psychosom. 2013;83(1):10–28. doi:10.1159/000353263
16. Taverna L, Bellavere M, Tremolada M, et al. Oncological children and well-being: occupational performance and hrqol change after fine motor skills stimulation activities. Pediatr Rep. 2021;13(3):383–400. doi:10.3390/pediatric13030046
17. Tremolada M, Taverna L, Chiavetta IT, Bonichini S, Putti MC, Biffi A. Psychological wellbeing in adolescents with leukaemia: a comparative study with typical development peers. Int J Environ Res Public Health. 2020;17(2):567. doi:10.3390/ijerph17020567
18. Zhong D, Xiang Q, Liu Y, et al. Medication adherence in leukemia children receiving home-based treatment and its related factors. Hematol. 2023;28(1). doi:10.1080/16078454.2023.2227490
19. Tremolada M, Taverna L, Bonichini S, Pillon M, Biffi A. Psychological well-being, cognitive functioning, and quality of life in 205 adolescent and young adult childhood cancer survivors compared to healthy peers. Front Psychol. 2022;13(May):1–10. doi:10.3389/fpsyg.2022.860729
20. Alya FP, Hendrawati S, Mediani HS. Factors associated with psychological well-being among children under 18 years old with cancer: a scoping review. Psychol Res Behav Manag. 2025;18(January):39–53. doi:10.2147/PRBM.S488905
21. Sherief LM, Kamal NM, Abdalrahman HM, et al. Psychological impact of chemotherapy for childhood acute lymphoblastic Leukemia on patients and their parents. Med. 2015;94(51):1–6.
22. Heo J, Park JE, Noh OK, Shin Y. Psychiatric disorders among children with acute lymphoblastic leukemia in South Korea: a nationwide population-based longitudinal study. J Int Med Res. 2022;50(1). doi:10.1177/03000605221075223
23. Ho LLK, Li WHC, Cheung AT, et al. Relationships among hope, psychological well-being and health-related quality of life in childhood cancer survivors. J Health Psychol. 2021;26(10):1528–1537. doi:10.1177/1359105319882742
24. Cheung AT, Li WHC, Ho LLK, et al. Impact of brain tumor and its treatment on the physical and psychological well-being, and quality of life amongst pediatric brain tumor survivors. Eur J Oncol Nurs. 2019;41(January):104–109. doi:10.1016/j.ejon.2019.06.003
25. Yallop K, McDowell H, Koziol-McLain J, Reed PW. Self-reported psychosocial wellbeing of adolescent childhood cancer survivors. Eur J Oncol Nur. 2013;17(6):711–719. doi:10.1016/j.ejon.2013.06.007
26. Liu W, Cheung YT, Brinkman TM, et al. Behavioral symptoms and psychiatric disorders in child and adolescent long-term survivors of childhood acute lymphoblastic leukemia treated with chemotherapy only. Psychooncology. 2018;27(6):1597–1607. doi:10.1002/pon.4699
27. Neville AR, Moothathamby N, Naganathan M, Huynh E, Moola FJ. “A place to call our own”: the impact of camp experiences on the psychosocial wellbeing of children and youth affected by cancer – a narrative review. Complement Ther Clin Prac. 2019;36(March):18–28. doi:10.1016/j.ctcp.2019.04.007
28. Muskat B, Jones H, Lucchetta S, Shama W, Zupanec S, Greenblatt A. The experiences of parents of pediatric patients with acute lymphoblastic leukemia, 2 months after completion of treatment. J Pediatr Oncol Nurs. 2017;34(5):358–366. doi:10.1177/1043454217703594
29. Hermono T, Maria L, Hariyanti TB. Hubungan Dukungan Keluarga Dengan Tingkat Kecemasan Pada Anak Penderita Kanker yang Menjalani Kemoterapi di Irna 4 RSUD dr. Saiful Anwar Malang. J Ilm Keperawatan. 2022;8(2):270–282.
30. Gheihman G, Zimmermann C, Deckert A, et al. Depression and hopelessness in patients with acute leukemia: the psychological impact of an acute and life-threatening disorder. Psychooncology. 2016;25(8):979–989. doi:10.1002/pon.3940
31. Liddle I, Carter GFA. Emotional and psychological well-being in children: the development and validation of the Stirling Children’s Well-being scale. Educ Psychol Pract. 2015;31(2):174–185. doi:10.1080/02667363.2015.1008409
32. Borualogo IS, Casas F. The children’s worlds psychological well-being scale: adaptation and fit in the Indonesian context. Cogent Psychol. 2022;9(1). doi:10.1080/23311908.2022.2053377
33. Stavraki M, García-Márquez R, Bajo M, Callejas-Albiñana AI, Paredes B, Díaz D. Brief version of the Ryff Psychological Well-being scales for children and adolescents: evidence of validity. Psicothema. 2022;34(2):316–322. doi:10.7334/psicothema2021.235
34. Orenstein GA, Lewis L. Eriksons stages of psychosocial development. StatPearls Publishing; 2022.
35. Boris P, Kovács KE, Nagy BE. The comparative study of chronically ill and healthy children and adolescents in the light of their general mental health. Sci Rep. 2024;14(1):1–15. doi:10.1038/s41598-024-57442-y
36. Sugiyono. Metodologi Penelitian Kuantitatif. Bandung: Alfabeta; 2019.
37. Varlina AP. Adaptation of the Indonesian version of the children’s hope scale. KnE Soc Sci. 2024;2024:263–271.
38. Ho LLK, Li WHC, Ho KY, et al. Comparing the impact of cancer and treatment-related effects on psychological well-being and quality of life between Hong Kong survivors of childhood solid tumors and leukemia. Cancer Nurs. 2019;43(6):446–454. doi:10.1097/NCC.0000000000000736
39. Dinsmore E, Rosengarten L. The psychological, psychosocial and emotional wellbeing of children and young people with leukaemia. Br J Nurs. 2022;31(20):1020–1028. doi:10.12968/bjon.2022.31.20.1020
40. Hossain MJ, Xie L, McCahan SM. Characterization of pediatric acute lymphoblastic leukemia survival patterns by age at diagnosis. J Cancer Epidemiol. 2014;2014:1–9. doi:10.1155/2014/865979
41. Ghaffar R, Ali A, Sarwar H. Psychological well-being and care giver burden of parents having child with leukemia. J Ther Rehabil Sci. 2023;105–116.
42. Steur LMH, Kaspers GJL, van Someren EJW, et al. The impact of maintenance therapy on sleep-wake rhythms and cancer-related fatigue in pediatric acute lymphoblastic leukemia. Support Care Cancer. 2020;28(12):5983–5993.
43. Ionio C, Bigoni F, Sacchi M, et al. Exploring the effects of cancer as a traumatic event on italian adolescents and young adults: investigating psychological well-being, identity construction and coping strategies. Pediatr Rep. 2023;15(1):254–262. doi:10.3390/pediatric15010021
44. Leeman J, Crandell JL, Lee A, Bai J, Sandelowski M, Knafl K. Family functioning and the well-being of children with chronic conditions: a meta-analysis. Res Nurs Health. 2016;39(4):229–243. doi:10.1002/nur.21725
45. Firdaus AM, Nuryani R, Wulan Lindasari S. Hubungan Resiliensi dengan Dukungan Keluarga Pada Remaja dengan Leukemia yang Menjalani Kemoterapi. J Keperawatan Florence Nightingale. 2024;7(1):124–130. doi:10.52774/jkfn.v7i1.156
46. Triwahyuni F, Anggraeni LD, Hidayah AJ. Gambaran Dukungan Keluarga Pada Anak dengan Leukemia di Yayasan Kasih Anak Kanker Indonesia. J Pubnurs Sci. 2024;02(03):87–91.
47. Koyu HO, Algül G, Altay N, Kilicarslan E. The effect of psychological resilience and spiritual well-being on the experience of hope in parents of children with cancer. J Pediatr Nurs. 2024;76:e34–41. doi:10.1016/j.pedn.2024.01.016
48. Griggs S, Walker RK. The role of hope for adolescents with a chronic illness: an integrative review. J Pediatr Nurs. 2016;31(4):404–421. doi:10.1016/j.pedn.2016.02.011
49. Germann JN, Leonard D, Stuenzi TJ, Pop RB, Stewart SM, Leavey PJ. Hoping is coping: a guiding theoretical framework for promoting coping and adjustment following pediatric cancer diagnosis. J Pediatr Psychol. 2014;40(9):846–855. doi:10.1093/jpepsy/jsv027
50. Cetin N. Examining the role of post-treatment family support in pediatric and adolescent cancer survivors: a systematic review. J Adolesc Young Adult Oncol. 2023;12(1):1–8. doi:10.1089/jayao.2021.0179
51. Van Schoors M, Caes L, Knoble NB, Goubert L, Verhofstadt LL, Alderfer MA. Systematic review: associations between family functioning and child adjustment after pediatric cancer diagnosis: a meta-analysis. J Pediatr Psychol. 2017;42(1):6–18. doi:10.1093/jpepsy/jsw070
52. Park M, Suh EE, Yu SY. Uncertainty and nursing needs of parents with pediatric cancer patients in different treatment phases: a cross-sectional study. Int J Environ Res Public Health. 2021;18(8):4253.
53. Reshetnikov A, Gevandova M, Prisyazhnaya N, Vyatkina N. The role of parents in their child’s cancer diagnosis, treatment, rehabilitation, and socialization. Indian J Pediatr. 2024;91(1):30–34. doi:10.1007/s12098-022-04387-7
54. Semenenko E, Banerjee S, Olver I, Ashinze P. Review of psychological interventions in patients with cancer. Support Care Cancer. 2023;31(4). doi:10.1007/s00520-023-07675-w
55. Chotolli MR, Luize PB. Non-pharmacological approaches to control pediatric cancer pain: nursing team view. Rev Dor. 2015;16(2):109–113. doi:10.5935/1806-0013.20150021
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.