Back to Journals » Infection and Drug Resistance » Volume 15
Detection of Mycobacterium tuberculosis Rifampicin Resistance Conferred by Borderline rpoB Mutations: Xpert MTB/RIF is Superior to Phenotypic Drug Susceptibility Testing
Authors Xia H, Song Y, Zheng Y, Wang S, Zhao B, He W, Liu D, Ou X, Zhou Y, Zhao Y
Received 13 January 2022
Accepted for publication 12 March 2022
Published 29 March 2022 Volume 2022:15 Pages 1345—1352
DOI https://doi.org/10.2147/IDR.S358301
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Héctor Mora-Montes
Hui Xia,1 Yuanyuan Song,1 Yang Zheng,1 Shengfen Wang,1 Bing Zhao,1 Wencong He,1 Dongxin Liu,2 Xichao Ou,1 Yang Zhou,1 Yanlin Zhao1
1National Center for Tuberculosis Control and Prevention, Chinese Center for Disease Control and Prevention, Beijing, People’s Republic of China; 2Institute of Hepatology, National Clinical Research Center for Infectious Disease, Shenzhen Third People’s Hospital, Shenzhen, People’s Republic of China
Correspondence: Yanlin Zhao, National Center for Tuberculosis Control and Prevention, Chinese Center for Disease Control and Prevention, No. 155, Changbai Road, Changping District, Beijing, People’s Republic of China, Tel +86 10-58900517, Email [email protected]
Objective: To compare the ability of detection of borderline rifampicin resistance in Mycobacterium tuberculosis between molecular assay and phenotypic drug susceptibility tests.
Methods: Fifty-seven isolates with His445Leu, Asp435Tyr, Leu452Pro, Leu430Pro, His445Asn, Ile491Phe, and His445Ser mutations in rpoB gene identified by whole-genome sequencing conferring borderline rifampicin resistance were included. Molecular-based Xpert MTB/RIF, phenotypic Löwenstein–Jensen (L-J) medium-based drug susceptibility test (DST) with a critical concentration of 40.0μg/mL and minimal inhibitory concentration (MIC) assay were performed to detect borderline rifampicin resistance.
Results: When using Xpert MTB/RIF, 48/57 (84.2%) isolates exhibited resistance to rifampicin. 25/57 (43.9%) and 33/57 (57.9%) isolates showed rifampicin resistance by L-J medium-based DST with 4 and 6 weeks of incubation, respectively. 30/57 (52.6%) and 40/57 (70.2%) strains were resistant to rifampicin by MIC method at cutoff values of 1.0 and 0.5μg/mL, respectively. The detection rate of rifampicin resistance of Xpert MTB/RIF was significantly higher than that of phenotypic methods (p < 0.001). Of the 57 isolates with borderline rpoB mutations, 5 (8.8%) had MICs of 0.25 or 0.12μg/mL, 22 (38.6%) had MICs of 0.5μg/mL or 1.0μg/mL, and 30 (52.6%) other isolates showed MICs ≥ 2.0μg/mL.
Conclusion: Molecular-based Xpert MTB/RIF showed superior ability to detect borderline rifampicin resistance over phenotypic DST methods. Extending the incubation time of L-J DST or lowering the cutoff value of the MIC method can improve borderline rifampicin resistance detection.
Keywords: Mycobacterium tuberculosis, rifampicin, borderline resistance, phenotypic drug susceptibility test
Introduction
China is one of the high-burden countries for tuberculosis and multidrug-resistant/rifampicin-resistant tuberculosis (MDR/RR-TB). There were an estimated 842,000 (717,000–978,000) cases of TB in 20201 and 65,000 (49,000–83,000) MDR/RR-TB cases in 20192 in China. Compared with the estimated MDR/RR-TB number in 2019 in China, the proportion of laboratory-confirmed MDR/RR-TB cases was only 28.1%,2 indicating a large gap in the detection of MDR/RR-TB. In recent years, China’s molecular testing capabilities have been strengthened. Variable diagnostic algorithms were implemented in different areas depending on the available diagnostic tools. Xpert MTB/RIF is provided as an initial diagnostic tool in approximately half of county-level tuberculosis care providers. Smear microscopy, culture or molecular-based tuberculosis detection assays, such as the Loop-mediated isothermal amplification assay, are used as initial tests in other peripheral laboratories, followed by specimen referral and rifampicin detection either by genotypic assay, such as line probe assay, or phenotypic drug susceptibility testing (DST) in an intermediate level laboratory. Molecular- based assays, especially Xpert MTB/RIF, are not universally accessible to every patient, however, for a variety of reasons, such as cost constraints, unavailability of tools, delays in specimen transport, and understanding the role of rapid determination of resistance of the doctors. Therefore, the traditional phenotypic DST is still widely used in the detection of rifampicin resistance in China. Rapid liquid culture systems such as the Mycobacteria Growth Indicator Tube (MGIT) 960 system fail to detect strains with borderline rifampicin resistance,3,4 most of which are conferred by WHO-defined borderline rpoB resistance mutations, eg His445Leu, Asp435Tyr, Leu452Pro, Leu430Pro, His445Asn, Ile491Phe, and His445Ser.5 Thus, if only phenotypic drug susceptibility testing methods are used, a patient infected with a strain with borderline rpoB mutation might be classified as rifampicin-susceptible, followed by standard rifampicin-based therapy, and then eventually treatment failure or relapse. The rifampicin resistance detection critical concentration for MGIT 960 and Middle brook 7H10 proportion DST had been reduced to 0.5μg/mL.6 Additional data on L-J medium-based DST at the current critical concentration (40.0μg/mL) to detect borderline rifampicin resistance requires clarification, especially in China, where the L-J medium-based DST is still a widely used DST method. With the application of whole-genome sequencing technology, the prevalence of Mycobacterium tuberculosis with borderline rpoB mutations in different settings has been reported. In china, borderline rpoB mutations accounted for 20.4% of the total rpoB mutations detected.7 Regarding the higher prevalence of borderline rpoB mutations and commonly used phenotypic DSTs in China, the ability of L-J medium-based DST to detect borderline rifampicin resistance conferred by specific mutations was explored in comparison with molecular based Xpert MTB/RIF.
Materials and Methods
Studied Isolates
Among 4922 Mycobacterium tuberculosis isolates with qualified genome sequencing results collected from 70 counties, 84 strains exhibited borderline rpoB resistance. 62 strains (73.8%) had a single borderline mutation and the other 22 strains (26.2%) had a combined mutation. 62 strains with a single borderline mutation were subcultured and 5 failed to culture, so 57 strains with 7 single borderline rpoB mutations (His445Leu, Asp435Tyr, Leu452Pro, Leu430Pro, His445Asn, Ile491Phe, and His445Ser) were finally included for analysis.
Whole Genome Sequencing
Genomic DNA was extracted using the cetyltrimethylammonium bromide (CTAB) method.8 2×150 paired-end (PE) DNA whole-genome sequencing was performed using Illumina HiSeq 2500 (Illumina, Inc., San Diego, CA). Rifampicin-related mutations were detected using the online “TB Profiler” tool.
Xpert MTB/RIF Testing
The Xpert MTB/RIF assay was performed using a 100-fold dilution of the 1.0 McFarland standard suspension. The procedure was according to the instruction of Xpert MTB/RIF. The target region is 426–453 of the rifampicin resistance determining region (RRDR) of the rpoB gene.
Solid L-J Medium-Based Proportion Susceptibility Testing
The rifampicin susceptibility test on solid L-J medium was performed according to the critical concentration of 40.0μg/mL recommended by WHO.6 Stored isolates were subcultured on L-J medium prior to DST. Susceptibility testing was performed with fresh Mycobacterium tuberculosis inoculates within 2–3 weeks’ growth. Susceptibility results were interpreted at 4- and 6- week incubation, respectively. A reference Mycobacterium tuberculosis strain H37Rv (ATCC 27294) was included in each test batch as a control.
Minimal Inhibitory Concentration Test
Fresh subcultures were tested for MIC using commercial microdilution plates (Thermo Fisher, Scientific Inc., USA) with rifampicin concentrations ranging from 0.03 to 2.0 μg/mL. Mycobacterium tuberculosis growth in drug containing wells was assessed visually using the Vizion instrument compared to growth in drug-free control wells on days 14–21. A reference Mycobacterium tuberculosis strain H37Rv (ATCC 27294) was included in each test batch as a control. Categories of rifampicin resistance were made based on the proposed breakpoint by Clinical Laboratory and Standards Institute (CLSI) at >1.0μg/mL9 and >0.5μg/mL.
Ethics Approval
The present study did not involve identifiable human subject data or interventional procedures. Therefore, ethics approval of the present study was waived by the Ethical Committees of the Chinese Center for Disease Control and Prevention.
Statistical Analysis
Descriptive data analysis was carried out. Categorical variables were summarized by presenting the frequency and proportion. The frequencies of categorical variables were compared using Pearson or Fisher’s exact test when appropriate. The data were analyzed using IBM SPSS software, version 22.0.
Results
Characteristics of Strains with Borderline rpoB Mutations
57 isolates with borderline rpoB mutations, consisting of 3 (5.2%) Asp435Tyr, 9 (15.8%) His445Asn, 4 (7.0%) His445Leu, 2 (3.5%) His445Ser, 3 (5.3%) Ile491Phe, 18 (31.6%) Leu430Pro and 18 (31.6%) Leu452Pro, were successfully retrieved. 51 isolates (89.5%) were Lineage 2 and 6 (10.5%) were lineage 4. Isoniazid resistance-related mutations or Indels in katG, ahpC or fabG1 were found in 43 strains (75.4%).
Comparison of Categorical Results Between Xpert MTB/RIF, L-J Medium-Based DST and MIC Methods
Of the 57 isolates, 48 (84.2%) were identified resistant to rifampicin by Xpert MTB/RIF. Only 25/57 (43.9%) and 33/57 (57.9%) strains exhibited resistance to rifampicin by solid L-J medium-based DST with 4- and 6- week incubation, respectively. 30/57 (52.6%) and 40/57 (70.2%) strains were resistant to rifampicin with MIC method at cutoff value of 1.0 and 0.5μg/mL, respectively. The detection rate of borderline rifampicin resistance by each method was significant (х2=23.98, p<0.001). The resistance rate detected by Xpert MTB/RIF was significantly higher than other methods (p<0.001) (Table 1).
 |
Table 1 Ability to Detect Borderline Resistance by Xpert MTB/RIF and Phenotypic Drug Susceptibility Testing |
As shown in Table 2, although the majority of resistance was detected by Xpert MTB/RIF, all 3 isolates with Ile491Phe mutation out of RRDR, 3 Leu452Pro, 1 His445Asn, 1 His445Leu and 1Leu430Pro mutation in RRDR were missed. Most of the Leu430Pro mutation was missed by phenotypic L-J DST and MIC method. For the Leu452Pro mutation, only half of the resistance was detected with the L-J DST after 4 weeks of incubation.
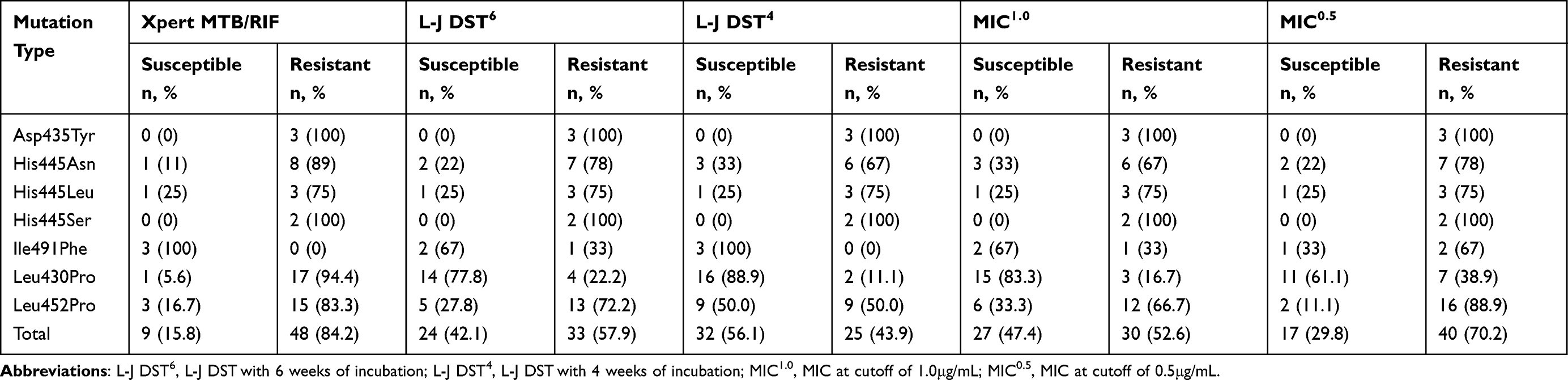 |
Table 2 Ability to Detect Borderline Resistance by Xpert MTB/RIF and Phenotypic Drug Susceptibility Testing Stratified by Different Borderline rpoB Mutations |
MIC Distribution Stratified by Different Borderline rpoB Mutations
The distribution of MICs was further analyzed to explore associations with various rpoB mutations. The MIC ranged from 0.12 to >2.0μg/mL. Among 57 strains, 5 strais (8.8%) had MICs of 0.25 or 0.12μg/mL, 22 strains (38.6%) had MICs of 0.5 or 1.0μg/mL, and the other 30 strains (52.6%) had MICs ≥2.0μg/mL. Notably, among strains with Leu430Pro or Leu452Pro mutations, 15/18 (83.3%) and 12/18 (66.7%) had MIC values within the range of one or two dilutions of the breakpoint of 1.0 or 0.5μg/mL. All inconsistent results between Xpert MTB/RIF and L-J DST with 6-week incubation to detect resistance conferred by Leu430Pro or Leu452Pro mutations were attributed to low MIC values (≤2.0μg/mL) (Figure 1).
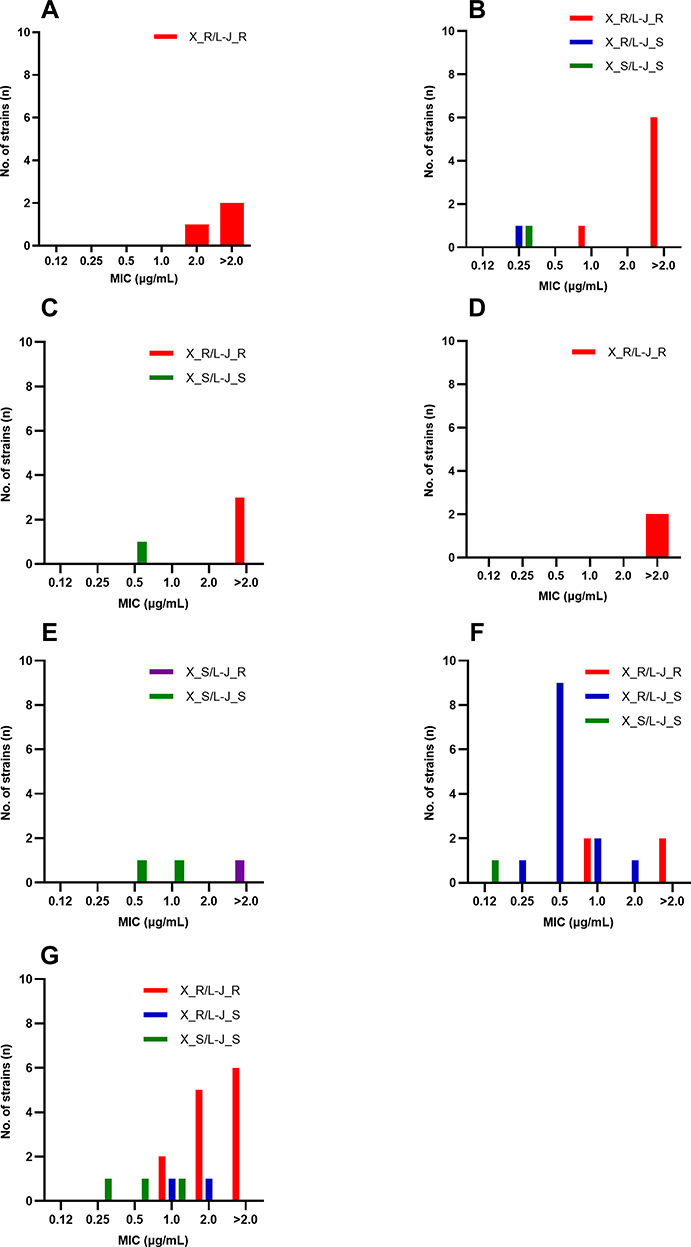 |
Figure 1 MIC distribution stratified by different borderline rpoB mutations, Asp435Tyr (A), His445Asn (B), His445Leu (C), His445Ser (D), Ile491Phe (E), Leu430Pro (F), Leu452Pro (G). X_R/L-J_R is colored in red; X_R/L-J_S is colored in blue; X_S/L-J_S is colored in green; X_S/L-J_R is colored in purple. Abbreviations: X_R/L-J_R, Xpert MTB/RIF resistant/L-J DST resistant strains; X_R/L-J_S, Xpert MTB/RIF resistant/L-J DST sensitive strains; X_S/L-J_S, Xpert MTB/RIF sensitive/L-J DST sensitive strains; X_S/L-J_R, Xpert MTB/RIF sensitive/L-J DST resistant strains. |
Discussion
Borderline rpoB resistance has been proven to be associated with significantly poor clinical response to treatment. Previous studies have shown that the proportion of borderline rpoB mutations in rifampicin-resistant Mycobacterium tuberculosis isolates, ranging from 3.3% to 13.1%.3,10–12 The reported proportion of 20.4% in china7 is higher than other countries. This study provided evidence that only 43.9% of rifampicin resistance conferred by borderline mutation was detected by L-J medium-based DST at the critical concentration of 40.0μg/mL6 with 4-week incubation. The detection rate increased to 57.9% as the incubation time was extended to six weeks. The MIC method detected more rifampicin resistance at the cutoff value of 1.0μg/mL recommended by CLSI9 and a lower breakpoint of 0.5μg/mL, but significantly lower than the 84.2% of the molecular-based Xpert MTB/RIF. The use of molecular-based assays as initial testing of tuberculosis samples will allow detection of more cases falsely susceptible to rifampicin by phenotypic DST. Phenotypic susceptibility test, especially L-J medium-based susceptibility testing will miss approximately 50% of borderline rifampicin resistance, leading to delays in timely and correct tuberculosis treatment adaptation or initiation, particularly when molecular-based assays are not widely available under field program conditions. When molecular and phenotypic drug susceptibility testing is performed sequentially or in parallel, inconsistent results are always presented, leaving clinicians confused about the results. The MIC method can explain some of the discrepancies between genotypic and phenotypic methods based on MIC values, particularly for strains with MIC values at or close to the breakpoint currently used by L-J DST. Therefore, molecular-based assays such as Xpert MTB/RIF can provide more accurate result in borderline rifampicin resistance and should be scaled up to increase their accessibility to patients in China.
Borderline mutations are always associated with low levels of rifampicin resistance and slightly elevated MICs below the critical concentration of current DST systems.13–17 In this study, 48.2% of the strains had MIC values equal to or lower than 2.0μg/mL, especially the Leu430Pro and Leu452Pro mutations, of which 88.9% and 66.7% of the strains had MIC values equal to or lower than 2.0μg/mL, respectively. Other mutations showed variable MIC values. Reduced the breakpoint of the MIC method from the current 1.0μg/mL to 0.5μg/mL can detect more borderline resistance, which is similar to the case of the MGIT 960 system, whose critical concentration has been reduced from the initial 1.0μg/mL to the current 0.5μg/mL by WHO5 to address more discrepancy between genotypic assays and the MGIT 960 system. The present findings suggest that the current cutoff value of 1.0μg/mL is also not suitable for the detection of borderline resistance to rifampicin by the MIC method. On egg-based L-J medium, the tested drug concentrations are not directly related to the actual MIC due to the high degradation and absorption of antimicrobial agents. As a result, drug concentrations are used that are significantly higher than those used in other media, such as Middlebrook-based solid and liquid media. Therefore, the critical concentration in L-J media is more difficult to determine. More research on appropriate breakpoint for L-J medium-based susceptibility testing is required in the future.
The mutations missed by the liquid MGIT 960 system were mostly located at the extreme ends of the rpoB resistance hot spot (Leu430Pro and Leu452Pro) or outside this core region (Ile491Phe). This study also showed that rifampicin-resistant isolates conferred by Ile491Phe or Leu430Pro mutation were more likely to be missed by L-J medium-based DST and MIC method with current drug breakpoint. Leu430Pro mutation accounted for 25% of the mutations associated with cases producing discordant susceptibility results between Xpert MTB/RIF and MIC method, followed by Leu452Pro (17.3%), His445Leu (9.6%) and Asp435Tyr (6.7%) in a large hospital in China.18 Resistance caused by borderline mutations might be due to fitness costs and a partial reduction in the binding affinity of rifampicin to the rpoB protein.13 An average delay of 7.2 days for positive results on the MGIT 960 system for strains with borderline mutations provided evidence that mutations conferring low levels of resistance are associated with delayed growth in MGIT.13 In this study, some strains failed to obtain resistance results after 4 weeks of incubation, but converted to resistance after an additional two weeks of incubation on L-J medium also supports that slow growth due to specific mutations may be one of the factors responsible for the false susceptible result in the phenotypic DST. Liquid broth medium provides more nutrients than solid L-J medium, so growth delay may be less affected in liquid medium, which may be the reason of the significant higher borderline resistance detected by MIC method compared to L-J DST with 4-week incubation. MIC method with a reduced breakpoint (0.5μg/mL) detected more borderline rpoB resistance than L-J DST at 4 and 6 weeks of incubation, reminding us that the currently recommended critical concentration is not suitable for borderline rifampicin resistance detection. Prolonged incubation period can improve borderline rifampicin resistance detection, but also result in further delays in diagnosis. Therefore, further studies should be carried out to explore suitable critical concentrations for L-J DST and MIC method. Xpert MTB/RIF missed some borderline rpoB resistance in this study. False-negative rifampicin susceptibility results may occur due to hetero resistance,19,20 or the presence of mutations outside of the rifampicin resistance-determining region (RRDR) (eg, rpoB Ile491Phe),21 and the Leu452Pro mutation sub-optimally identified using Xpert MTB/RIF.22
Few studies had examined the performance of borderline mutations detection by L-J medium-based DST.23–25 This study provided evidence of the ability of phenotypic L-J medium-based susceptibility testing and MIC method to detect borderline resistance conferred by seven mutations in the rpoB gene compared to the WHO recommended Xpert MTB/RIF. The main limitation is the low number of strains for certain mutations, such as Asp435Tyr, His445Ser and Ile491Phe. Future studies should increase the number of strains with these mutation classes. Another limitation is that the appropriate critical concentration on the L-J medium was not further explored.
Conclusion
Compared to phenotypic L-J medium-based susceptibility testing and MIC method at current breakpoints, the molecular-based Xpert MTB/RIF showed superior ability to detect borderline rifampicin resistance. Extending the incubation time of L-J medium-based DST to 6 weeks or reducing the critical concentration of MIC method to 0.5μg/mL can improve the borderline rifampicin resistance detection. Molecular based assays such as Xpert MTB/RIF should be rapidly scaled up to improve their accessibility to patients in China.
Acknowledgments
The study was financed by the National Science and Technology Major Project of China and Tuberculosis Control and Prevention Project (228711).
Disclosure
The authors report no conflicts of interest in this work.
References
1. World Health Organization. Global Tuberculosis Report 2021. World Health Organization; 2021.
2. World Health Organization. Global Tuberculosis Report 2020. World Health Organization; 2020.
3. Ocheretina O, Escuyer VE, Mabou MM, et al. Correlation between genotypic and phenotypic testing for resistance to rifampin in Mycobacterium tuberculosis clinical isolates in Haiti: investigation of cases with discrepant susceptibility results. PLoS One. 2014;9(3):e90569. doi:10.1371/journal.pone.0090569
4. Rafael LL, Raquel MS, Rogelio FA, Miroslava FP, Alejandra-Isabel JG, Paola RTS. Discordant results between genotypic and phenotypic assays (Xpert MTB/RIF vs. BACTEC MGIT 960 system) for detection of RIF-resistant Mycobacterium tuberculosis isolates in a high burden region. Infect Genet Evol. 2021;96:105142. doi:10.1016/j.meegid.2021.105142.
5. World Health Organization. Technical report on critical concentrations for drug susceptibility testing of isoniazid and the Rifamycins (Rifampicin, Rifabutin and Rifapentine). Geneva: World Health Organization; 2021.
6. World Health Organization. Technical manual for drug susceptibility testing of medicines used in the treatment of tuberculosis. World Health Organization; 2018.
7. Liu D, Huang F, Zhang G, et al. Whole-genome sequencing for surveillance of tuberculosis drug resistance and determination of resistance level in China. Clin Microbiol Infect. 2021;21(6):534–536. doi: 10.1016/j.cmi.2021.09.014
8. van Soolingen D, Hermans PW, de Haas PE, Soll DR, van Embden JD. Occurrence and stability of insertion sequences in Mycobacterium tuberculosis complex strains: evaluation of an insertion sequence-dependent DNA polymorphism as a tool in the epidemiology of tuberculosis. J Clin Microbiol. 1991;29(11):2578–2586. doi:10.1128/jcm.29.11.2578-2586.1991
9. Clinical and Laboratory Standards Institute. Performance Standards for Susceptibility Testing of Mycobacteria, Nocardia, Spp., and Other Aerobic Actinomycetes.
10. Jo KW, Lee S, Kang MR, Sung H, Kim MN, Shim TS. Frequency and type of disputed rpoB mutations in Mycobacterium tuberculosis isolates from South Korea. Tuberc Respir Dis. 2017;80(3):270–276. doi:10.4046/trd.2017.80.3.270
11. Van Deun A, Aung KJM, Bola V, et al. Rifampin drug resistance tests for tuberculosis: challenging the gold standard. J Clin Microbiol. 2013;51(8):2633–2640. doi:10.1128/JCM.00553-13
12. Mvelase NR, Pillay M, Sibanda W, Ngozo JN, Brust JCM, Mlisana KP. rpoB mutations causing discordant rifampicin susceptibility in Mycobacterium tuberculosis: retrospective analysis of prevalence, phenotypic, genotypic, and treatment outcomes. Open Forum Infect Dis. 2019;6(4):ofz065. doi:10.1093/ofid/ofz065
13. Miotto P, Cabibbe AM, Borroni E, Degano M, Cirillo DM. Role of disputed mutations in the rpoB Gene in interpretation of automated liquid MGIT culture results for Rifampin susceptibility testing of Mycobacterium tuberculosis. J Clin Microbiol. 2018;56(5):e01599–17. doi:10.1128/JCM.01599-17
14. Hu P, Zhang H, Fleming J, et al. Retrospective analysis of false-positive and disputed Rifampin resistance Xpert MTB/RIF assay results in clinical samples from a referral hospital in Hunan, China. J Clin Microbiol. 2019;57(4):e01707–18. doi:10.1128/JCM.01707-18
15. Berrada ZL, Lin SYG, Rodwell TC, et al. Rifabutin and rifampin resistance levels and associated rpoB mutations in clinical isolates of Mycobacterium tuberculosis complex. Diagn Microbiol Infect Dis. 2016;85(2):177–181. doi:10.1016/j.diagmicrobio.2016.01.019
16. Van Deun A, Barrera L, Bastian I, et al. Mycobacterium tuberculosis strains with highly discordant rifampin susceptibility test results. J Clin Microbiol. 2009;47(11):3501–3506. doi:10.1128/JCM.01209-09
17. Lin WH, Lee WT, Tsai HY, Jou R. Disputed rpoB mutations in Mycobacterium tuberculosis and tuberculosis treatment outcomes. Antimicrob Agents Chemother. 2021;65(7). doi:10.1128/AAC.01573-20
18. Huo F, Ma Y, Liu R, et al. Interpretation of discordant rifampicin susceptibility test results obtained using genexpert vs phenotypic drug susceptibility testing. Open Forum Infect Dis. 2020;7(8):ofaa279. doi:10.1093/ofid/ofaa279
19. Blakemore R, Story E, Helb D, et al. Evaluation of the analytical performance of the Xpert MTB/RIF assay. J Clin Microbiol. 2010;48(7):2495–2501. doi:10.1128/JCM.00128-10
20. Zetola NM, Shin SS, Tumedi KA, et al. Mixed Mycobacterium tuberculosis complex infections and false-negative results for rifampin resistance by Genexpert MTB/RIF are associated with poor clinical outcomes. J Clin Microbiol. 2014;52(7):2422–2429. doi:10.1128/JCM.02489-13
21. Sanchez-Padilla E, Merker M, Beckert P, et al. Detection of drug-resistant tuberculosis by Xpert MTB/RIF in Swaziland. N Engl J Med. 2015;372(12):1181–1182. doi:10.1056/NEJMc1413930
22. Rufai SB, Kumar P, Singh A, Prajapati S, Balooni V, Singh S. Comparison of Xpert MTB/RIF with line probe assay for detection of rifampin-monoresistant Mycobacterium tuberculosis. J Clin Microbiol. 2014;52(6):1846–1852. doi:10.1128/JCM.03005-13
23. Vincent V, Rigouts L, Nduwamahoro E, et al. The TDR tuberculosis strain bank: a resource for basic science, tool development and diagnostic services. Int J Tuberc Lung Dis. 2012;16(1):24–31. doi:10.5588/ijtld.11.0223
24. Andres S, Hillemann D, Rüsch-Gerdes S, Richter E. Occurrence of rpoB mutations in isoniazid-resistant but rifampin-susceptible Mycobacterium tuberculosis isolates from Germany. Antimicrob Agents Chemother. 2014;58(1):590–592. doi:10.1128/AAC.01752-13
25. Rigouts L, Gumusboga M, de Rijk WB, et al. Rifampin resistance missed in automated liquid culture system for Mycobacterium tuberculosis isolates with specific rpoB mutations. J Clin Microbiol. 2013;51(8):2641–2645. doi:10.1128/JCM.02741-12
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.