Back to Journals » OncoTargets and Therapy » Volume 8
Detection of epidermal growth factor receptor mutation in plasma as a biomarker in Chinese patients with early-stage non-small cell lung cancer
Authors Guo K, Zhang Z, Han L, Han J, Wang J, Zhou Y, Liu H, Tong L, Li X, Yan X
Received 12 August 2015
Accepted for publication 14 October 2015
Published 6 November 2015 Volume 2015:8 Pages 3289—3296
DOI https://doi.org/10.2147/OTT.S94297
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr William C. Cho
Kai Guo,1,* ZhiPei Zhang,1,* Lu Han,2,* Jing Han,3 Jian Wang,1 YongAn Zhou,1 HongGang Liu,1 LiPing Tong,1 XiaoFei Li,1 XiaoLong Yan1
1Department of Thoracic Surgery, Tangdu Hospital, 2Department of Ultrasound, Xijing Hospital, 3Department of Ophthalmology, Tangdu Hospital, The Fourth Military Medical University, Xi’an, People’s Republic of China
*These authors contributed equally to this work
Purpose: This preplanned exploratory analysis was conducted to reveal the true status of correlation between tissue and plasma detection for early-stage non-small cell lung cancer (NSCLC) epidermal growth factor receptor (EGFR) mutations, knowing that specific subgroups of NSCLC patients may be potential candidates for EGFR mutation analysis by using plasma samples.
Materials and methods: Tissue samples were surgically resected from 198 patients with stage I–IV NSCLC, where stage IA to IIIA accounted for 92.4%. EGFR mutations in all these tissues were positive. Paired plasma EGFR mutations were detected by real-time polymerase chain reaction; concentration of cell-free DNA (cfDNA) in plasma was measured by ultraviolet spectrophotometry.
Results: EGFR-activating mutation was detected in 34 plasma samples, and their mutation types were matched with that in tissue. The sensitivity of EGFR mutation for the 198 paired tissue and plasma samples was 17.2%. The sensitivity positively correlated with disease stage and negatively correlated with tumor differentiation. The sensitivity of stage IA, IB, IIA, IIB, and IIIA was 1.6%, 7.9%, 11.1%, 20%, and 33.3%, respectively; the sensitivity of high differentiation was 0% versus 36.8% for poor differentiation. There was no correlation between plasma cfDNA concentration and patient characteristics.
Conclusion: We recommend using plasma cfDNA as a biomarker in stage IIIA or poorly differentiated tumors for gene diagnosis, especially in patients whose tissue samples cannot be obtained by surgery. Plasma samples can really reflect the patients’ EGFR mutation types and may contain comprehensive genotypic information that comes from different parts of the tumor than tissue specimens. The concentration of plasma cfDNA does not vary with patient characteristics.
Keywords: EGFR mutations, NSCLC, plasma, early stage, ARMS, targeted therapy
Introduction
Lung cancer is the most common cause of cancer-related death in both men and women worldwide,1 and 80%–90% of all lung cancers are non-small cell lung cancer (NSCLC).2 Currently, patients with NSCLC are generally treated with curative intent using surgery, chemotherapy, and radiation therapy, or a combined modality approach. However, the 5-year relative survival rate for NSCLC is only approximately 15%,3 although this status is being changed by molecular targeting treatment. Tyrosine kinase inhibitors (TKIs) are representative molecular targeting drugs. Epidermal growth factor receptor (EGFR)-activating mutations have significant impact on the clinical treatment of NSCLC patients using EGFR-TKIs.4–6 The Iressa Pan-Asia Study showed that objective response rate % and progression-free survival (PFS) of EGFR-TKI therapy reach up to 71.2% and 9.8 months, respectively, which is significantly higher than chemotherapy, whose objective response rate % and PFS is only 47.3% and 6.4 months, respectively.7 Several studies well demonstrated that PFS was increased significantly in TKI-treated patients with EGFR-positive NSCLC.8–10
EGFR mutation detection using tissue samples from NSCLC patients is regarded as the gold standard in the prediction of TKI treatment responses and prognoses. However, it is sometimes difficult to collect tumor tissues for biomarker analysis,11 and therefore great interest in using surrogate samples such as serum and plasma samples has been aroused. The biological mechanism underlying the increased release of cell-free DNA (cfDNA) remains to be fully understood. Several reviews detailed the biology and mechanism of DNA release into circulation.12–14 Elements of apoptosis and necrosis, especially of large tumors, and the possibility of active release of cfDNA from tumors have been reported.15 The detection of EGFR mutations in plasma may provide a noninvasive and surrogate source of genotypic information that might provide dynamic monitoring to facilitate clinical decision-making at the time of diagnosis and in the later course of disease, especially in TKI-treated patients. Recently, Mok et al16 have confirmed that dynamic changes in the cfDNA EGFR mutation status relative to the baseline may predict clinical outcomes of patients using EGFR-TKIs.16
Although a series of previous studies have shown that the use of plasma to detect EGFR mutations is feasible in the advanced stage of the disease, the reported sensitivity varied considerably. Brevet et al17 showed that the sensitivity and specificity, respectively, were 44% and 85% in stage III–IV NSCLC versus 100% and 89% in stage IIIB–IV, as reported by He et al.18 However, studies about plasma EGFR mutation detection in early-stage NSCLC are rarely reported. Zhao et al assessed plasma EGFR mutations in stage I–IV patients by mutation-enriched polymerase chain reaction (PCR) and reported an overall sensitivity of 36% versus 45.9% for stage IA–IIIA.19 On the contrary, Ren et al20 showed that the sensitivity was 0 in stage IA–IIIA patients using direct sequencing, indicating that direct sequencing is not sensitive enough to detect a very low level of EGFR mutation in plasma of early stage. So, both of the two studies were vulnerable in assessing plasma EGFR mutations in the early-stage NSCLC patients.
The frequently used methods for EGFR mutation detection in plasma include direct sequencing, Scorpion-amplification-refractory mutation system (ARMS), denaturing high-performance liquid chromatography, multiplex PCR, and digital droplet PCR. The Scorpion-ARMS method is highly sensitive and fast for detection of known mutations.21 In addition, it is easy and simple to operate. Goto et al22 reported a sensitivity of 43.1% and a specificity of 100% with the Scorpion-ARMS method in a Japanese subgroup of patients from the Iressa Pan-ASia Study. A recent first-line, single-arm study on gefitinib reported a concordance rate of 94.3%, sensitivity of 65.7%, and specificity of 99.8% using the Scorpion-ARMS method.23 However, the aforementioned studies used different detection methods and therefore lacked standardization. It is notable that few studies have reported on early-stage (IA–IIIA) patients and the correlation between sensitivity and patient characteristics.
In the present study, we used the Scorpion-ARMS method to explore the mutation status in the plasma of NSCLC patients whose tissue EGFR mutations were positive, in an attempt to provide credible experimental data for clinical screening of specific subgroups of early-stage patients who may be the best candidates for EGFR mutation analysis using blood cfDNA for diagnosis and dynamic monitoring of cfDNA and prediction of TKI resistance. In addition, we also attempted to use plasma EGFR mutation detection to assess the prognosis of early-stage NSCLC patients.
Materials and methods
Patients and materials
Included in this study were 198 NSCLC patients who had not received radiotherapy, chemotherapy, or targeted therapy previously and had been diagnosed and treated at the Department of Thoracic Surgery of Tangdu Hospital of the Fourth Military Medical University (Xi’an, People’s Republic of China) between February 2014 and June 2015. Our study was approved by the Review Board of the said university. Written informed consent was obtained from all patients before any study-related procedure, including the provision of samples for biomarker testing.
Tissue samples
All tissue samples were obtained by various operations in the Department of Thoracic Surgery of Tangdu Hospital. All tumor samples were evaluated histologically by pathologists from Tangdu Hospital to confirm the NSCLC diagnosis. A part of stage IV patients who had metastasis were treated by surgical resection, aiming to obtain tumor by surgery for pathological diagnosis. According to manufacturer’s protocol, DNA was extracted from fresh tumor samples using an Amoy Tissue DNA Extraction Kit (Amoy Diagnostics Corporation, Xiamen, People’s Republic of China). Then Human EGFR Mutation Detection Kit (Amoy Diagnostics Corporation) and real-time PCR (Agilent StrataGene Mx3000P, Palo Alto, CA, USA) was used for EGFR mutation detection (including G719X in exon 18, deletions mutations in exon 19, T790M mutation in exon 20, exon 20 insertions, and L858R in exon 21, L861Q and S768I). All tissue EGFR detections of the 198 NSCLC patients were positive.
Plasma samples
Blood samples were collected 1 day before the operation and prepared in an anticoagulant-treated (ethylenediaminetetraacetic acid) tube for analysis within 4 hours after sampling.24 For each patient, a 5 mL blood sample was needed; it was centrifuged (Sigma Laborzentrifugen 3–30K, Osterode am Harz, Germany) at 825× g for 15 minutes and then the 2 mL supernatant, or plasma, was moved in a sterile tube and stored at −80°C until use. Paired plasma samples were collected from the 198 patients whose tissue mutations were positive.
cfDNA extraction
cfDNA was extracted from 2 mL plasma using an Amoy plasma/serum DNA Extraction Kit (Amoy Diagnostics Corporation) according to manufacturer’s protocol. The concentration and purity of the extracted DNA were determined using a spectrophotometer (DU800 UV/VIS Spectrophotometer, Beckman Coulter, Pasadena, CA USA). The extracted DNA was stored at −20°C until use.
Real-time PCR analysis for EGFR mutation
The Scorpion-ARMS method is highly sensitive and fast,21 and can be validated to detect a mutant as low as 1.0%.25 cfDNA (45 μL) was used for EGFR mutation detection using a Human EGFR Mutation Detection Kit (Amoy Diagnostics Corporation) by real-time PCR (Agilent StrataGene Mx3000P) according to manufacturer’s protocol. The PCR reaction included three stages: first stage, 1 cycle at 95°C for 5 minutes; second stage, 15 cycles at 95°C for 25 seconds, 64°C for 20 seconds, 72°C for 20 seconds; third stage, 31 cycles at 93°C for 25 seconds, 60°C for 35 seconds, 72°C for 20 seconds. The real-time PCR result of plasma mutation was read and analyzed by two professional investigators. Any disagreement between the two investigators was resolved by discussion with a third observer. Experimental data were obtained and recorded independently by the investigators who were blinded to the clinical data until statistical analysis.
Statistical analysis
SPSS software (version 22.0, IBM Software, Armonk, NY, USA) was used to analyze the data. The chi-square test or Fisher’s exact test was used to assess the relationship between the presence of EGFR mutations in plasma with NSCLC and patient characteristics. One-way analysis of variance was used to assess the relationship between the concentration of cfDNA and patients characteristics. A P-value of less than 0.05 was considered to be statistically significant.
Results
Patient characteristics and the results of subgroup sensitivity analysis
A total of 198 patients were enrolled into our study between February 2014 and June 2015 at the Department of Thoracic Surgery of Tangdu Hospital. The patients were composed of 86 men and 112 women ranging in age from 36 to 78 years. The initial clinical records of the 198 patients were reviewed by the investigators, showing 52 smokers and 146 never-smokers. A person who smoked more than 100 cigarettes in his/her past history was defined as a smoker. Of the 198 patients, 183 had lung adenocarcinoma, eight had squamous cell carcinoma, four had adenosquamous carcinoma, and three had other types of carcinoma, including large cell carcinoma, sarcomatoid carcinoma, and bronchoalveolar carcinoma. Disease stages were classified according to the National Comprehensive Cancer Network guideline in 2014. The percentage of patients with stage IA to IIIA disease was 92.4%, including 62 stage IA, 38 stage IB, 18 stage IIA, five stage IIB, and 60 stage IIIA NSCLC. The remaining were three stage IIIB cases and 12 stage IV cases. Of the 198 patients, 45 were well differentiated, 108 were moderately differentiated, 38 were poorly differentiated, and seven were uncertain.
In total, 34 plasma samples were EGFR mutation positive. The result of analysis on the correlation between the patient characteristics and the sensitivity of plasma detection showed no significant difference between the ratio and age, sex, smoking history, and histological type. The overall sensitivity of the EGFR mutation status in our study was 17.2%. However, the sensitivity was enormously different in tumor, node, and metastasis (TNM) stages and differentiation subgroups. The sensitivity of IA and IB was 1.6% and 7.9%, respectively, which was significantly lower than 33.3% in IIIA. For patients with poor differentiation, the sensitivity was 36.8%, which was significantly higher than that in patients with high differentiation (0%, P=0.00) and moderate differentiation (15.7%, P=0.01). Table 1 shows patient characteristics and the results of subgroup sensitivity analysis. Figure 1 shows the tendency of sensitivity in subgroups of differentiation and TNM stage.
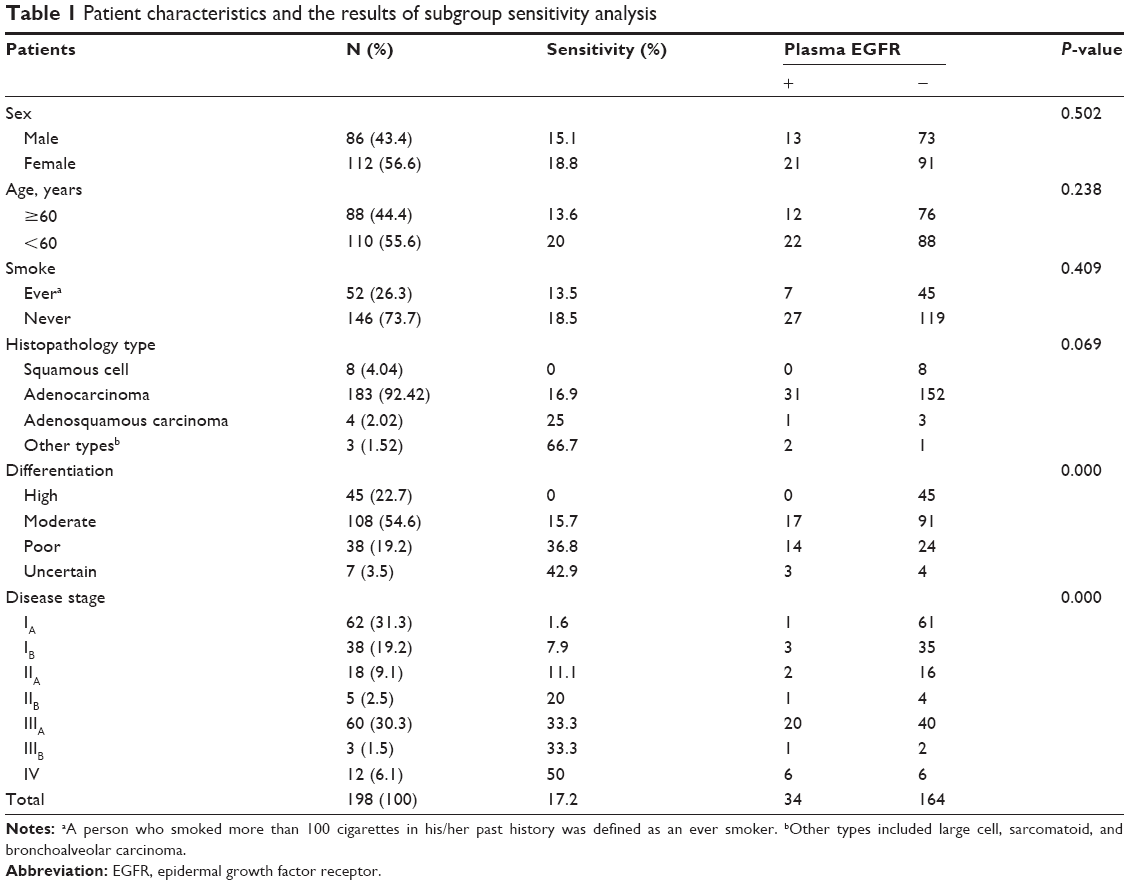 | Table 1 Patient characteristics and the results of subgroup sensitivity analysis |
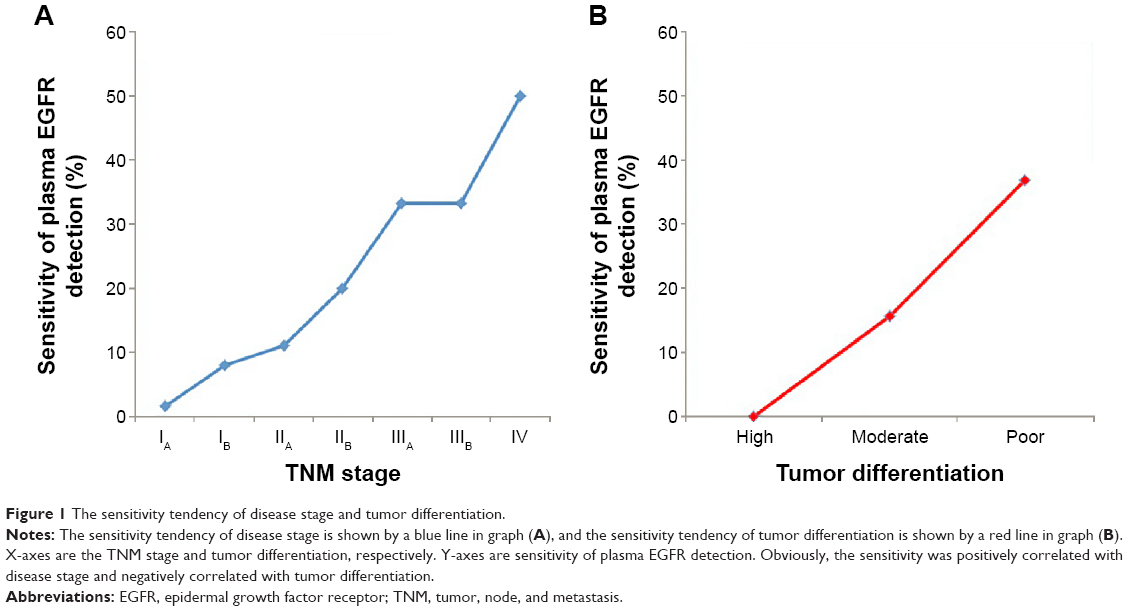 | Figure 1 The sensitivity tendency of disease stage and tumor differentiation. |
Plasma and tissue mutation types
Tissue and plasma mutations were detected using the Scorpion-ARMS method, showing that most mutations were single mutations and the others were double mutations.
The details of plasma and tissue single mutations and the positive ratio of different single mutation types are summarized in Table 2. There were 188 tissue single mutations and 32 plasmas single mutations. Exon 19 deletion mutation (19-del) and exon 21 L858R point mutation (L858R) were more frequently seen in the tissue samples, which is consistent with our previous study.26 In the plasma samples, 23 exon 19 deletion mutations, five exon 21 L858R mutations, three L861Q mutations, and one exon 20 insertion were detected, without seeing T790M, G719X, and S768I mutations. The positive mutation type in the plasma sample was identical to that in the paired tissue sample. The result indicated a high consistency between the positive mutation types detected in the plasma and corresponding tissue.
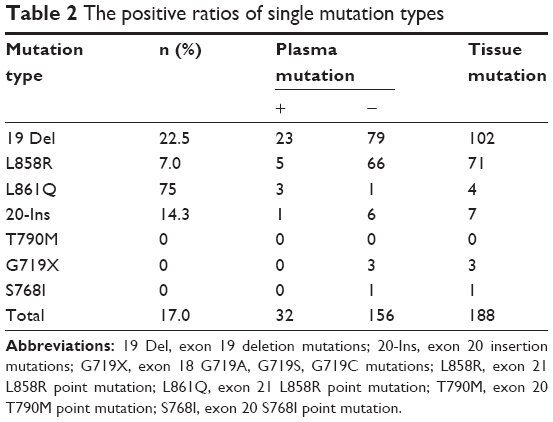 | Table 2 The positive ratios of single mutation types |
The positive ratio of exon 19 deletion mutations was 22.5%; the positive ratio of L858R, 20 insertions, and L861Q mutation was 7.0%, 14.3%, and 75%, respectively. However, T790M, G719X, and S768I were all zero. Our study showed that the positive ratio of mutation types in plasma was statistically different from each other (P=0.003). We further analyzed the correlation between the positive ratio of 19 deletions and L858R, and found that the positive ratio of 19 deletions was significantly better than that of L858R in plasma (P=0.011).
Double mutations are shown in Table 3. Among the ten tissue samples with double mutations, there were G719X and S768I mutations in four, 19 deletions and L858R mutations in two, and L858R mutations and T790M in two samples. The other two tissue samples were detected with 19 deletions, G719X and 19 deletions, T790M, respectively. However, both of their paired plasma samples were mutation negative. Noticeably, the mutation type of the two plasma samples was basically the same as their paired tissue samples, except additional exon 19 deletion mutation, which was not detected in the paired tissue samples.
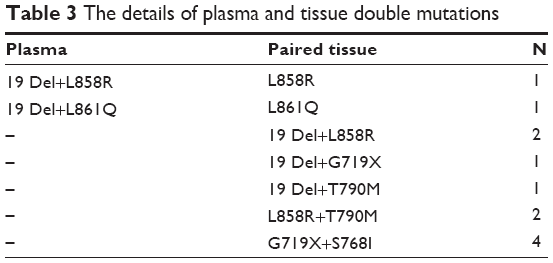 | Table 3 The details of plasma and tissue double mutations |
Correlation between the concentration of cfDNA and patient characteristics
Table 4 shows the concentration of extracted cfDNA in a 2 mL plasma sample. The median concentration was 17.34 μg/mL (range: 2.01–92.80 μg/mL). No significant correlation between the plasma concentration of cfDNA and patient characteristics of age, sex, smoking history, histologic type, or TNM staging system was found in our study.
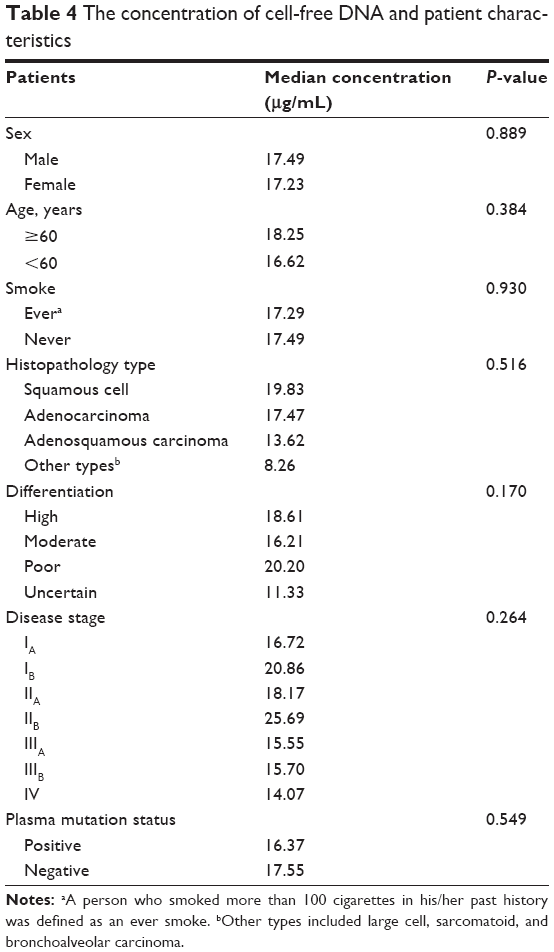 | Table 4 The concentration of cell-free DNA and patient characteristics |
Discussion
It is usually difficult to obtain a tissue sample for EGFR detection because of either loss of the surgical opportunity in some advanced/metastatic patients, potential surgical complications, or economic considerations. In addition, the procedure of obtaining a tumor sample may increase the risk of cancer “seeding” to other sites.27 So it is important to seek a surrogate sample for EGFR detection. It is relatively easy to obtain body fluid through minimally invasive means. In addition, it is realizable for clinical dynamic monitoring of cfDNA, which allows a potentially successful change in the treatment course, for example, acquired resistance to TKIs. Therefore, using blood for EGFR detection has been a hot spot in recent years and liquid biopsy may be megatrends of detections in the future. Most previous studies focused on advanced and metastatic patients,28–33 and there are few experimental data concerning EGFR mutations in the plasma of early-stage NSCLC patients.
The aim of our study was to assess EGFR mutation detection in the plasma of early-stage NSCLC patients, in an attempt to provide more convincing experimental data for clinical practice. In this study, we collected 198 plasma samples from paired patients whose tissue EGFR mutations were positive. A total of 183 (92.4%) patients were in the early stage (IA–IIIA), in whom the overall sensitivity was 17.2% versus 0%, and 36% in other two previous studies.19,20 We analyzed the correlation of sensitivity between the different subgroups and found that the sensitivity was positively correlated with the TNM stage, and negatively correlated with differentiation. The sensitivity of stage IA and IIIA was 1.6% and 33.3%, respectively, and that of stage IV was 50%, which is consistent with that reported in the published literature. The sensitivity of high differentiation was 0% versus 36.8% for poor differentiation, the difference being statistically different. It is therefore prudent to recommend using plasma to detect EGFR mutations in early-stage (IA, IB, and IIA) NSCLC patients, or those with high differentiation, because of the extremely low sensitivity. However, the sensitivity rate increased dramatically in stage IIIA patients and those with poor differentiation. Therefore, blood analysis for EGFR mutations could be effectively used as a biomarker in IIIA or poorly differentiated tumors for diagnosis, dynamic monitoring of cfDNA, and prediction of TKI resistance, especially in NSCLC patients whose tissue cannot be obtained readily by surgery. However, more studies with larger sample sizes are needed to verify the reliability of plasma EGFR detection of squamous, adenosquamous, and other types (large cell, sarcomatoid, and bronchoalveolar) of lung cancer. Our ongoing research plans to assess the correlation between the plasma detection results in early-stage NSCLC and patient PFS/overall survival, hoping that it could be used to estimate the prognosis of early-stage NSCLC patients.
Tissue-based EGFR detection is the standard for prediction of clinical TKI treatment responses and prognoses. Our study found that, although 94.1% (32/34) plasma samples had identical mutations with their paired tissue samples, there were still two plasma samples whose mutation types were not detected in the paired tissues. Kimura et al33,34 observed the same phenomenon in their studies. The possible reason may be due to tumor heterogeneity. Gerlinger et al35 demonstrated that a portion taken from different parts of a primary tumor and its metastases showed extensive inter- and intratumoral evolution. Tumor samples might not carry EGFR mutations detected in plasma. On the contrary, plasma contains comprehensive genotypic information that comes from different parts of the tumor. Traditional tissue-based EGFR detection generally ignored the complexity of the genomic mutation of the tumor. Tumoral heterogeneity highlights the difficulty of diagnosis and dictating a therapeutic course based on single tissue detection. Our study also found that 164 tissue samples tested were positive for EGFR mutations but were negative in the paired plasma samples, and most of them were from early-stage NSCLC patients. In a previous study, Ren et al20 showed a similar condition. Schwarzenbach et al13 demonstrated that apoptotic and necrotic cells released nuclear and mitochondrial DNA into the circulation in the process of cellular destruction. It is more difficult to detect tumor-derived cfDNA because of few apoptotic and necrotic tumor cells that release EGFR DNA into blood in the early stage. So, more sensitive detection methods are needed in the future.
Our study showed no significant difference between the concentration of cfDNA and age, sex, smoking history, histologic type, or TNM stage. The exact mechanism of cfDNA remains uncertain. The mechanism can be broadly categorized as passive and active. According to the passive hypothesis, cfDNA is mainly released from healthy, inflamed, or diseased (cancerous) tissue cells undergoing apoptosis or necrosis, and rarely from apoptotic and necrotic tumor cells. For this reason, the concentration of cfDNA could not change with patient characteristics. Simultaneously, highly sensitive measurement methods and equipment are required for detecting trace amounts of tumor-derived cfDNA and analyze the correlation between the cfDNA concentration and patient characteristics.
Plasma sample detection can provide a noninvasive way to gain genotypic information, and therefore has broad application prospects in the future. As the sample size in our study was not large enough, it was difficult to assess the plasma mutation data of adenosquamous carcinoma and large cell carcinoma in the present study. In our ongoing prospective study, we shall use larger amounts of plasma and modify the methods for cfDNA isolation and measurement, hoping to improve the sensitivity of plasma EGFR detection. Our ongoing research plans to estimate the prognosis of early-stage NSCLC patients using plasma EGFR detection.
Conclusion
Plasma cfDNA may be a surrogate and noninvasive strategy for EGFR mutation detection in early-stage NSCLC. We recommend using plasma cfDNA as a biomarker in stage IIIA or poorly differentiated tumors for gene diagnosis, especially in the patients whose tissue samples cannot be obtained by surgery. Plasma samples can really reflect the patients’ EGFR mutation types. In addition, they may contain more comprehensive genotypic information that comes from different parts of the tumor than tissue specimens. Our experimental data showed plasma cfDNA concentration does not vary with the patient characteristics.
Acknowledgments
The authors are grateful to Amoy Diagnostics Corporation (Xiamen, People’s Republic of China) for all help to conduct the study. This work was supported by the Institutional Review Board of the Fourth Military Medical University and grant support from this institute.
Disclosure
The authors report no conflicts of interest in this work.
References
Jemal A, Bray F, Center MM, Ferlay J, Ward E, Forman D. Global cancer statistics. CA Cancer J Clin. 2011;61(2):69–90. | ||
Jemal A, Siegel R, Ward E, Murray T, Xu J, Thun MJ. Cancer statistics. CA Cancer J Clin. 2007;57(1):43–66. | ||
Jemal A, Siegel R, Ward E, et al. Cancer statistics. CA Cancer J Clin. 2006;56(2):106–130. | ||
Lynch TJ, Bell DW, Sordella R, et al. Activating mutations in the epidermal growth factor receptor underlying responsiveness of non-small-cell lung cancer to gefitinib. N Engl J Med. 2004;350(21):2129–2139. | ||
Paez JG, Janne PA, Lee JC, et al. EGFR mutations in lung cancer: correlation with clinical response to gefitinib therapy. Science. 2004;304(5676):1497–1500. | ||
Han SW, Kim TY, Hwang PG, et al. Predictive and prognostic impact of epidermal growth factor receptor mutation in non-small-cell lung cancer patients treated with gefitinib. J Clin Oncol. 2005;23(11):2493–2501. | ||
Lee JS, Park K, Kim SW, et al. A randomized phase III study of gefitinib (IRESSA) versus standard chemotherapy (gemcitabine plus cisplatin) as a first-line treatment for never-smokers with advanced or metastatic adenocarcinoma of the lung. J Thorac Oncol. 2009;4(9 Suppl 1):S283. | ||
Mok TS, Wu YL, Thongprasert S, et al. Gefitinib or carboplatin-paclitaxel in pulmonary adenocarcinoma. N Engl J Med. 2009;361(10):947–957. | ||
Mitsudomi T, Morita S, Yatabe Y, et al. Gefitinib versus cisplatin plus docetaxel in patients with non-small-cell lung cancer harbouring mutations of the epidermal growth factor receptor (WJTOG3405): an open label, randomised phase 3 trial. Lancet Oncol. 2010;11(2):121–128. | ||
Maemondo M, Inoue A, Kobayashi K, et al. Gefitinib or chemotherapy for non-small-cell lung cancer with mutated EGFR. N Engl J Med. 2010;362(25):2380–2388. | ||
Costa DB, Kobayashi S, Tenen DG, Huberman MS. Pooled analysis of the prospective trials of gefitinib monotherapy for EGFR-mutant non-small cell lung cancers. Lung Cancer. 2007;58(1):95–103. | ||
Jung K, Fleischhacker M, Rabien A. Cell-free DNA in the blood as a solid tumor biomarker – a critical appraisal of the literature. Clin Chim Acta. 2010;411(21–22):1611–1624. | ||
Schwarzenbach H, Hoon DS, Pantel K. Cell-free nucleic acids as biomarkers in cancer patients. Nat Rev Cancer. 2011;11(6):426–437. | ||
Zhou J, Shi YH, Fan J. Circulating cell-free nucleic acids: promising biomarkers of hepatocellular carcinoma. Semin Oncol. 2012;39(4):440–448. | ||
Stroun M, Maurice P, Vasioukhin V, et al. The origin and mechanism of circulating DNA. Ann N Y Acad Sci. 2000;906:161–168. | ||
Mok T, Wu YL, Lee JS, Yu CJ. Detection and dynamic changes of EGFR mutations from circulating tumor DNA as a predictor of survival outcomes in NSCLC patients treated with first-line intercalated erlotinib and chemotherapy. Clin Cancer Res. 2015;21(14):3196–3203. | ||
Brevet M, Johnson ML, Azzoli CG, Ladanyi M. Detection of EGFR mutations in plasma DNA from lung cancer patients by mass spectrometry genotyping is predictive of tumor EGFR status and response to EGFR inhibitors. Lung Cancer. 2011;73(1):96–102. | ||
He C, Liu M, Zhou C, et al. Detection of epidermal growth factor receptor mutations in plasma by mutant-enriched PCR assay for prediction of the response to gefitinib in patients with non-small-cell lung cancer. Int J Cancer. 2009;125(10):2393–2399. | ||
Zhao X, Han RB, Zhao J, et al. Comparison of epidermal growth factor receptor mutation statuses in tissue and plasma in stage I-IV non-small cell lung cancer patients. Respiration. 2013;85(2):119–125. | ||
Ren J, Song GH, Zhang LJ, et al. Low correspondence of EGFR mutations in tumor tissue and paired serum of non-small-cell lung cancer patients. Chin J Cancer Res. 2010;22(1):27–31. | ||
Bates JA, Taylor EJ. Scorpion ARMS primers for SNP real-time PCR detection and quantification of Pyrenophora teres. Mol Plant Pathol. 2001;2(5):275–280. | ||
Goto K, Ichinose Y, Ohe Y, et al. Epidermal growth factor receptor mutation status in circulating free DNA in serum: from IPASS, a phase III study of gefitinib or carboplatin/paclitaxel in non-small cell lung cancer. J Thorac Oncol. 2012;7(1):115–121. | ||
Douillard JY, Ostoros G, Cobo M, et al. Gefitinib treatment in EGFR mutated Caucasian NSCLC: circulating-free tumor DNA as a surrogate for determination of EGFR status. J Thorac Oncol. 2014;9(9):1345–1353. | ||
Diehl F, Schmidt K, Choti MA, et al. Circulating mutant DNA to assess tumor dynamics. Nat Med. 2008;14(9):985–990. | ||
Pao W, Ladanyi M. Epidermal growth factor receptor mutation testing in lung cancer: searching for the ideal method. Clin Cancer Res. 2007;13(17):4954–4955. | ||
Lai Y, Zhang Z, Li J, et al. EGFR mutations in surgically resected fresh specimens from 697 consecutive Chinese patients with non-small cell lung cancer and their relationships with clinical features. Int J Mol Sci. 2013;14(12):24549–24559. | ||
Robertson EG, Baxter G. Tumour seeding following percutaneous needle biopsy: the real story! Clin Radiol. 2011;66(11):1007–1014. | ||
Kuang Y, Rogers A, Yeap BY, et al. Noninvasive detection of EGFR T790M in gefitinib or erlotinib resistant non-small cell lung cancer. Clin Cancer Res. 2009;15(8):2630–2636. | ||
Kimura H, Kasahara K, Kawaishi M, et al. Detection of epidermal growth factor receptor mutations in serum as a predictor of the response to gefitinib in patients with non-small-cell lung cancer. Clin Cancer Res. 2006;12(13):3915–3921. | ||
Kimura H, Kasahara K, Shibata K, et al. EGFR mutation of tumor and serum in gefitinib-treated patients with chemotherapy-naive non-small cell lung cancer. J Thorac Oncol. 2006;1(3):260–267. | ||
Bai H, Mao L, Wang HS, et al. Epidermal growth factor receptor mutations in plasma DNA samples predict tumor response in Chinese patients with stages IIIB to IV non-small-cell lung cancer. J Clin Oncol. 2009;27(16):2653–2659. | ||
Yung TK, Chan KC, Mok TS, Tong J, To KF, Lo YM. Single-molecule detection of epidermal growth factor receptor mutations in plasma by microfluidics digital PCR in non-small cell lung cancer patients. Clin Cancer Res. 2009;15(6):2076–2084. | ||
Kimura H, Suminoe M, Kasahara K, et al. Evaluation of epidermal growth factor receptor mutations in serum DNA as a predictor of response to gefitinib (IRESSA). Br J Cancer. 2007;97(6):778–784. | ||
Moran MT, Sanchez JM, Isla D, et al. High correspondence between EGFR mutations in tissue and in circulating DNA from non-small-cell lung cancer (NSCLC) patients (p) with poor performance status (PS). J Thorac Oncol. 2007;2(8):s444. | ||
Gerlinger M, Rowan AJ, Horswell S, et al. Intratumor heterogeneity and branched evolution revealed by multiregion sequencing. N Engl J Med. 2012;366(10):883–892. |
 © 2015 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2015 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.