Back to Journals » Medical Devices: Evidence and Research » Volume 18
Design and Development of a Simple Screw Mechanism for a Low-Cost Neonatal Syringe Pump
Received 6 September 2024
Accepted for publication 31 March 2025
Published 16 September 2025 Volume 2025:18 Pages 447—459
DOI https://doi.org/10.2147/MDER.S489922
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Oliver Norton, Prashant Jha
Department of Biomedical and Imaging Sciences, King’s College London, London, UK
Correspondence: Prashant Jha, Email [email protected]
Background: Approximately 2.3 million neonates die annually. UNICEF proposes that the deployment of specialist, quality neonatal care could help reduce neonatal mortality rates by 28% by 2025. Syringe pumps are a key medical device for providing accurate and precise fluid and drug delivery to neonates. However, syringe pumps are expensive, complicated to use and not designed for the additional challenges of providing quality healthcare in low resource healthcare settings. Several open-source designs for low-cost syringe pumps already exist, however, they all have respective limitations.
Objective: To design and test a simple, open-source, screw mechanism, with the potential to be used in a future low-cost syringe pump.
Methods and Materials: A low-cost screw mechanism for a syringe pump, using a non-captive stepper motor, was developed. The prototype’s accuracy was tested using 5mL, 20mL, 30mL and 60mL syringes at different rates. The rate was measured by recording the changing mass of saline fluid dispensed onto a weighing scale. The mean flow rate error from each run was calculated as the time taken to infuse 75% of the nominal volume, as per the ISO 286020:2020 standard.
Results: The prototype produced a total mean flow rate error of 0.38%± 1.62%. All errors were within the 3% limit (Z-score: 0.125) stipulated by the UNICEF and NEST360 target product profile. Compared to the other open-source designs, the prototype has the fewest parts, can accommodate a range of syringe sizes and is more accurate than many of the other open-source designs. Future work should involve testing the device with more viscous fluids, a greater range of rates and microstep settings, and improving the accuracy with further software and hardware development.
Keywords: syringe pump, low-cost, neonatal, open-source
Introduction
Global Neonatal Mortality
In 2023, there was an estimated 2.3 million neonatal deaths.1 These were predominantly in low- and lower-middle-income countries (LLMICs).2 In Sub-Saharan Africa and South Asia, neonatal mortality rates (NMR) were 26 and 21 deaths per 1,000 live births1 respectively. This is significantly greater than the third Sustainability Development Goal (SDG), “to ensure healthy lives and promote wellbeing for all at all ages”,3,4 of 12 deaths per 1,000 live births. Global efforts to achieve this goal have resulted in a 43% reduction in the global NMR5 since 2000. However, this is not enough, with the average NMR only predicted to reduce to 18 deaths per 1,000 live births5 by the 2030 deadline. This has been called the “survival gap”3 by UNICEF. The UNICEF “Survive and thrive: transforming care for every small and sick newborn” campaign3 suggested that the gap could be reduced by implementing several strategies, including the deployment of higher quality, specialist neonatal care. The campaign suggested that, by 2025, deploying specialist neonatal care could lower the NMR by 28%.3 Maternal and stillbirth mortality rates could also be reduced by a further 19%.3
Syringe Pumps
One element of providing quality, specialist neonatal care is medical devices. According to The World Health Organization, syringe pumps are a “priority medical device”.6–8 They are frequently used to treat newborns as they can precisely deliver small volumes of fluids at a controlled rate. This precision can aid in infant hydration, nutrition and drug delivery.9,10
In LLMICs, healthcare facilities often have too few trained healthcare workers,11–13 leading to missed dosages of drugs and fluids. The automation of the infusion process, by syringe pumps, improves the quality and continuity of care,8,14 while also freeing up healthcare worker’s time to treat more patients.15
Appropriate Medical Devices
Previously, an estimated 38%16 of medical devices, donated to LLMICs, went unused. Although donated with good intentions, they can be inappropriate for these healthcare settings. Undertrained clinical staff and infrastructure limitations can lead to the disuse of complicated medical devices, causing hospital storage issues and incurring disposal costs.8,16–18
Many global bodies, including the United Nations and the World Health Organization, now promote the local production of medicines and medical devices in developing countries.19 However, complex medical devices may be harder to manufacture, requiring more intricate production techniques, financial investment and training. There are also other general challenges to deploying medical devices in LLMICs, such as unreliable utilities.20
In addition to these complications, syringe pumps face specific barriers to being successfully deployed in LLMICs. Syringe pumps require luer lok syringes and intravenous lines as consumables. These can be specific to the syringe pump’s brand. Therefore, any disruption to the supply of the specific infusion consumables can limit a pump’s use.
Many pumps have additional functionalities, such as drug libraries, complicating their use. Given that LLMICs have too few sufficiently trained staff,11,13 this can result in user errors,21 inflicting comorbidities on patients.21 This also increases the difficulty of servicing the pumps. Technicians require more maintenance training and equipment to ensure the device functions correctly and safely.
To help medical device innovators overcome these challenges, UNICEF and NEST360, an international alliance aimed at improving outcomes for sick and premature neonates in Africa, released a Target Product Profile (TPP) for syringe pumps.10 The TPP details requirements for syringe pumps specifically designed for low-resource neonatal healthcare settings.
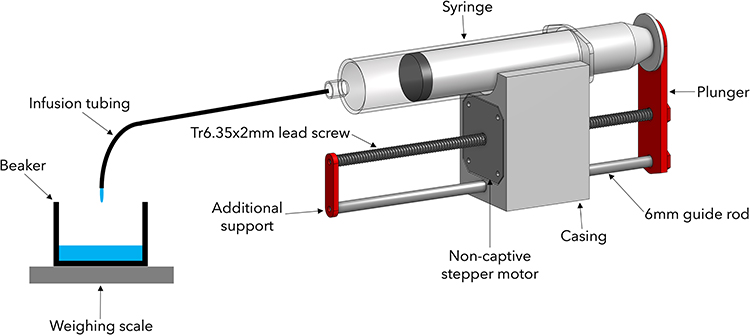 |
Figure 1 Experimental Setup Using Prototype. |
The syringe pump TPP advocates for a syringe pump to be able to accommodate luer lok syringes of various sizes and brands. This aims to help overcome the issue of the inconsistent supply of consumables. To ensure quality care, the TPP also recommends that a pump should be able to produce infusion rates between 0.1–60.0mL/hr, with an optimal accuracy of ±1% and a minimum of ±3%.
Current Syringe Pump Prototypes
Open-source designs allow for the local development and manufacturing of medical devices within the countries where they are needed.22–24 This reduces costs, accommodates local challenges and allows for more rapid deployment of the devices. It has been widely suggested that 3D printers could play a role in facilitating these goals, with projects already benefiting from their use.25–27
Several attempts have been made to develop an open-source, low-cost, syringe pump.28–35 A brief literary search was conducted to identify low-cost syringe pumps using the Scopus and IEEE Xplore databases. On 1/8/2024, limiting the results to peer-reviewed publications between 2014 and 2024, 8 different syringe pump prototypes, that also reported accuracy testing results, were identified (Table 1). Bolts and screws were not counted as parts as the number of required fixings was not presented in all of the papers.
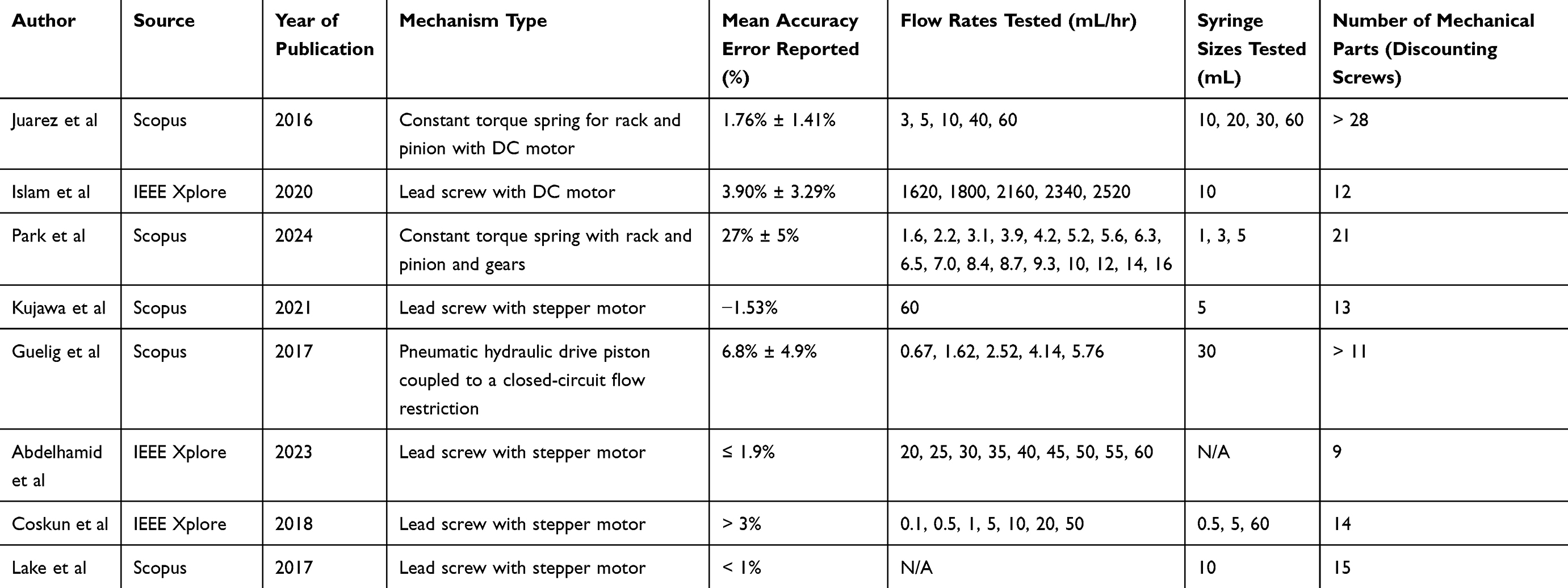 |
Table 1 Comparison of Open-Source Low-Cost Syringe Pumps |
Only 3 of the pumps met the minimal TPP accuracy requirement of 3% for all tests.10 However, it should be noted that the design by Coskun et al36 only produced 1 error greater than 3% during testing.
Lake et al produced the most accurate design,37 with an average error of less than 1%. Their design was based upon one by Wijnen et al35 which achieved an accuracy of less than 5% during testing. Lake et al achieved this improved accuracy by creating a closed-loop feedback system, using a pressure sensor, amplified with PID control. However, this increased the number of parts and complexity of the system. This design also required specific parts for each syringe size, which is not appropriate for a clinical setting where they may be misplaced.
Using the scale method to measure rate,38 the design by Kujawa et al39 was the next most accurate, producing an average error of −1.53% at 75% of the nominal volume, as per ISO 286020:2020 standards. However, this reported error was only based on 1 test at the maximum required flow rate of the TPP. Testing the device with a greater range of syringe sizes and at more rates would better evaluate the design. Though it did have fewer parts than the design by Lake et al, it was only able to accommodate syringes up to 20mL.
Of these 3 pumps, the design by Abdelhamid et al40 had the fewest parts but was also the least accurate, with the greatest error being 1.9%. This design was tested at 9 different rates, however, it was not declared what syringe size it was tested with. Further clarification or testing would allow for a better evaluation of the design.
Although these three prototypes are accurate enough for the TPP specification,10 none of the designs have presented results that test a range of rates and syringe sizes. Furthermore, there are design limitations, such as parts specific to syringe sizes and additional fixings. Therefore, an open-source, low-cost syringe pump mechanism, with sufficiently reported accuracy, that is simpler and more versatile, would be a beneficial alternative for medical device manufacturers in LLMICs.
Aim
The authors have designed and prototyped a mechanism for a low-cost syringe pump. This paper reports the results of testing the accuracy of the prototype.
Methods and Materials
Materials
This mechanism functions using a non-captive stepper motor with a Tr6.35x2mm lead screw, a guide rod, a plunger, an additional support piece, and a casing for the motor (Figures 1, 2 and Table 2). For this prototype, the infusion rate is controlled by an Arduino Mega 2560 microcontroller (Figure 3) since they are easy to use and widely available. However, a lower-cost microcontroller, which is still able to provide UART communication, would be equally acceptable with suitable alterations to the operating code (Listing 1).
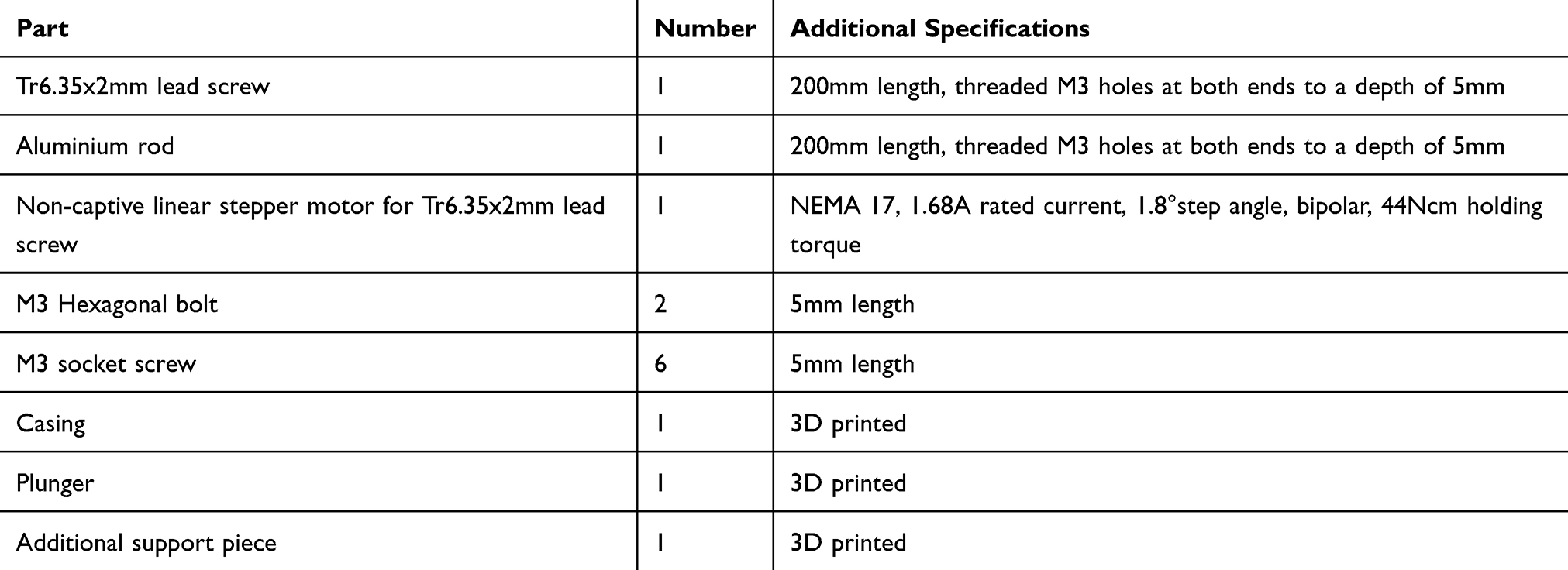 |
Table 2 Mechanism Parts List |
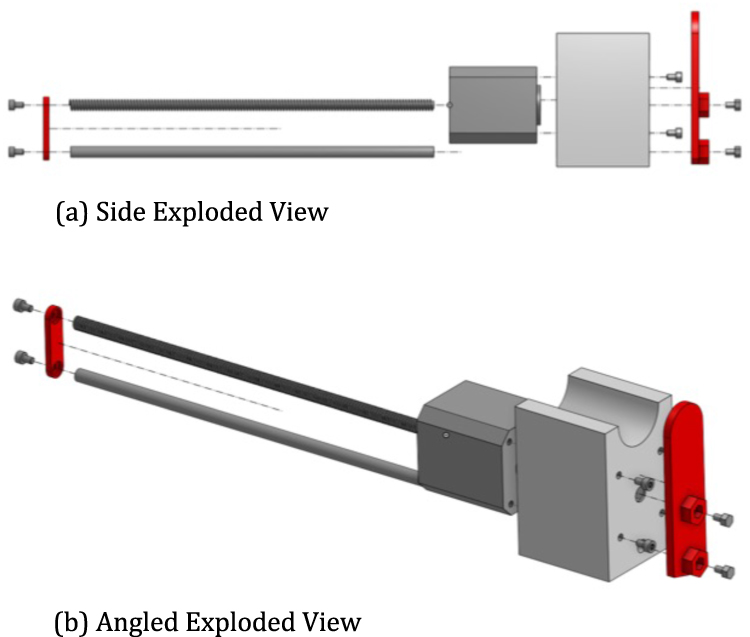 |
Figure 2 Exploded Views of Prototype Syringe Pump. (a) Side Exploded View. (b) Angled Exploded View. |
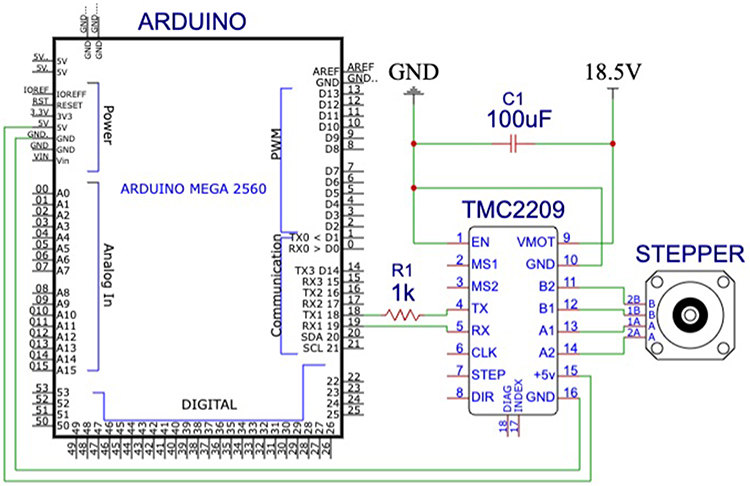 |
Figure 3 Prototype Syringe Pump Circuit Diagram. |
The lead screw is prevented from rotating by the guide rod, which moves through the casing (Figure 1). The screw and rod are attached to the plunger using the hexagonal M3 bolts. The guide rod restricts the plunger’s rotation thus causing the screw to move linearly rather than rotationally. The plunger then pushes against the syringe, displacing the fluid within it. An additional support piece joins the other ends of the screw and guide rod to ensure that they remain parallel.
The 3D printed parts were created using a fuse deposition modeling printer, with 1.75mm PLA filament and 0.4mm nozzle. A triangle pattern infill of 5%, with 4 vertical and 5 horizontal shells, was chosen for the casing and additional support piece. A 50% infill was used for the plunger piece to prevent deformation. These specifications were chosen to balance physical requirements, print time, material consumption, weight and strength.
The prototype is assembled by first attaching the stepper motor to the casing using 4 of the socket screws (Figure 2). The lead screw is then manually rotated through the stepper motor till it is halfway. Next, the hexagonal bolts are through the hexagonal holes in the plunger (Figure 2). The lead screw is then inserted into the plunger’s upper hole and screwed on till tight. The guide rod is then pushed through the casing and into the remaining hole in the plunger and screwed on tight too. Finally, the support piece is screwed to the lead screw and rod using the remaining 2 socket screws. The electronics can then be connected (Figure 3).
This prototype used a TMC2209 motor driver (Figure 3), produced by TRINAMIC Motion Control, which is commonly used on 3D printers making it widely available and low-cost.41 The TMC2209 also has a UART mode, requiring fewer wires and allowing for bidirectional communication which gives access to additional features of the driver. In this mode, the TMC2209 can control the stepper motor using an internal step pulse generator, allowing a range of microcontrollers to be used to control the mechanism. Its StallGuard4™ feature can be used for stall detection and sensorless homing.41 CoolStep™ current control prevents the motor and driver from overheating, thus reducing energy wastage by up to 75%.41 The StealthChop2™ feature aids in silent motor operation.41
Given the need for accurate infusions, rounding errors can make a significant impact. The TMC2209 has a clock speed of 12MHz for internal step pulse generation.41 This means that rounding errors can be already greater than the minimum requirement of 3%.10 To reduce the effect of this error, a simple algorithm was also included in the design (Listing 1). If the calculated microsteps per period (No) was.3,0.4,0.5,0.6, or.7, then the microcontroller would oscillate the number of microsteps between the rounded integer value (Ni) and plus or minus one after each full step, depending on the direction of rounding. This produced an average number of microsteps per cycle of Ni ± 0.5 which is closer to No. This was achieved using the TMC2209 clock speed and the TSTEP address of the TMC2209.

(2) Using the Arduino micros() function, which returns the number of microseconds since the start of the current program, a counter can be created. When the time between steps reaches T, 1 is added or subtracted from the number of steps per cycle.
(3) The counter is then zeroed and starts again.
Methods
The method used to evaluate the device’s benchtop accuracy was the same used by Juarez et al38 to evaluate another low-cost syringe pump prototype. The rate was calculated by continuously measuring the changing mass of saline solution dispensed into a beaker, from a syringe, using the prototype (Figure 1).
The method was repeated with different brands and sizes of luer lok syringes to thoroughly evaluate the prototype’s mechanism compared to the TPP. The syringes were filled with 0.9% saline solution to better emulate the clinical use of the device. For half of the experiments, a 100mmHg back pressure was applied to simulate infant blood pressure.42
The International Electrotechnical Commission (IEC 60601-2-24:2012)43 does not have standards for flow rates greater than 5mL/hr or infusions less than 2 hours. Therefore, the International Organization for Standardization (ISO 286020:2020)44 mean flow rate equation was used to calculate the mean flow rates of the infusions except for the 60mL infusions at 5mL/hr, where the IEC 60601-2-24:2012 could be used.
Microstep Calibration
Before the experiments were conducted on all the syringe sizes and rates, the optimum number of microsteps was established since more microsteps increase accuracy but affects incremental torque per microstep.45 This calibration was done with a 60mL syringe at 60mL/hr with 100mmHg back pressure using the method. These variables were chosen since this would cause the greatest demand on the prototype, being the largest syringe and fastest rate tested. Sixteen, thirty-two and sixty-four microsteps were tested. These values were chosen to balance torque per microstep and accuracy since they are central values in the potential microstep settings. The accuracy algorithm was then deployed to measure its success in reducing the effect of rounding errors.
Method
- A KERN CFS 300–3 weighing scale was used to measure the weight. The scale was connected to a PC using an RS232 cable at 9600 baud. An empty beaker was placed on the weighing scales.
- The syringe size was then selected and filled with 0.9% saline solution beyond the maximum volume printed on the syringe. Infusion tubing was then connected to the end of the syringe and the syringe plunger pushed until it reached the maximum measured volume of the syringe. This was done to ensure no air was in the syringe or line.
- The device was then primed for the infusion by reversing the motor direction. The syringe was fixed to the device and the plunger’s position was adjusted so that it pushed firmly against the syringe.
When simulating the 100mmHg back pressure (P), the pump was placed 1.36m (h) lower than the beaker as per the hydrostatic formula:

Where ρsaline is the density of the saline solution.
- The end of the intravenous line was then placed on the edge of the beaker so that drops of water would be collected in it (Figure 1). The taro function, on the weighing scales, was then used to set the measured weight to zero.
- KERN’s BalanceConnection software was run on the PC to periodically record the weight measured by the scale. The sample interval was set to 10 seconds for all the infusions, except for the 60mL at 5mL/hr which was set to 60 seconds, to ensure appropriate resolution.
- The desired rate of infusion was then entered, using the Arduino IDE. The rate was controlled by varying VELOCITY (Listing 1). The code was then uploaded to the microcontroller to begin the infusion.
- The recording was then started, with the readings exported into Microsoft Excel.
- Once the infusion was complete, the data logging was stopped. Any data that was recorded before or after the infusion was then removed.
- The mean flow rate (Qm) was calculated by measuring the time taken (T) for 75% of the nominal volume (Vn) to infuse, as per ISO 286020:2020 standards:

(10) The error was then calculated by subtracting the expected flow rate from the mean flow rate.
Data Presentation
The results of the device’s benchtop accuracy testing were presented in a table In accordance with IEC 60601-2-24 standards,38,43 trumpet curves46 were created for the 60mL saline at 5mL/hr, both with and without back pressure, to assess variations in accuracy during the infusion between the 2nd and 6th hours. This was done by grouping the 420 measurements, between hours 2 and 6, into 418 overlapping observation windows (Pn) which are the average flow rate of 3 successive flow rates. P1,
P60, P120, P180, P240, P300, P360 and P418 were then selected as points as these were every half an hour. The maximum positive and negative percentage errors, within the range of these P values, were then calculated. These were plotted, alongside the total mean flow rate (P418), to produce the trumpet curve.
Results
When calibrating the microsteps, using a 60mL syringe at 60mL/hr with 100mmHg back pressure, 16 microsteps produced the most accurate result (Table 3). Thus, 16 microsteps was chosen for testing the other rates and syringe sizes.
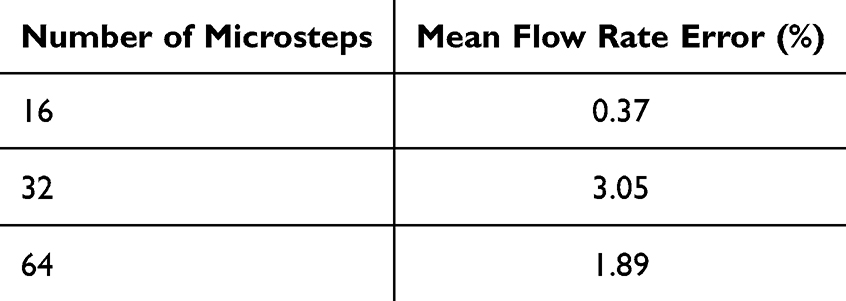 |
Table 3 Results of Microstep Calibration Using a 60mL at 60mL/hr with 100mmHg Back Pressure |
Implementing the accuracy algorithm improved the accuracy by an average of 0.51% (Table 4). However, it decreased the accuracy for the 60mL at 5mL/hr infusion. This may be due to the compounding of errors over time since the infusion was significantly longer than the others tested. Therefore, the algorithm was applied for the other tests but not on the 60mL infusions at 5mL/hr.
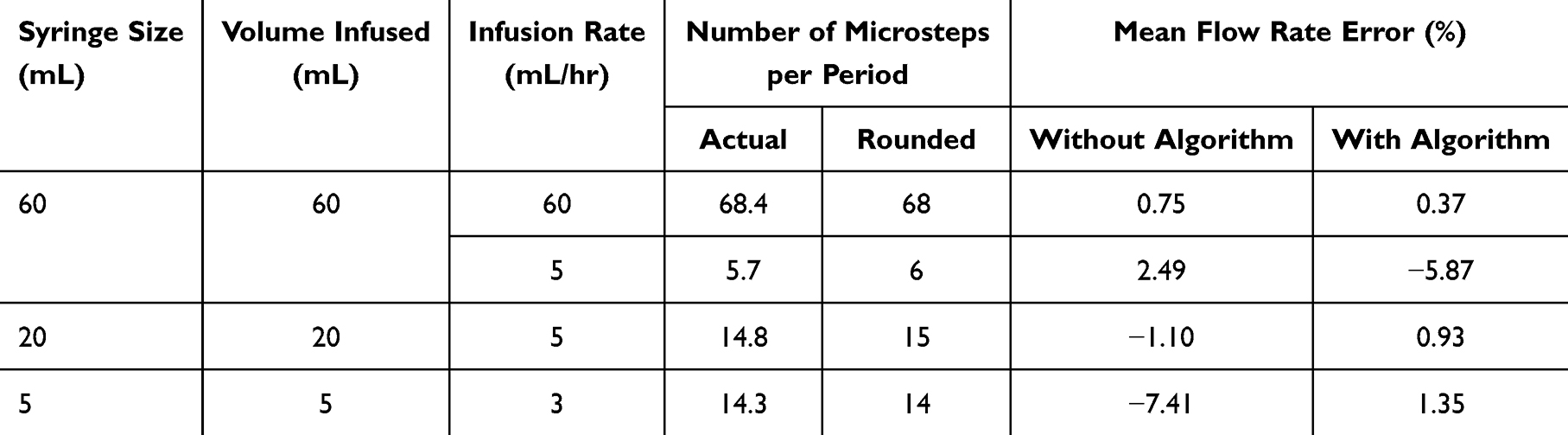 |
Table 4 Mean Flow Rate Errors Without and with Accuracy Algorithm |
From the mean flow rate testing, the error without back pressure was 0.73%±1.71%, while with back pressure it was 0.02%±1.44%. The mechanism performed more accurately and precisely, when under the additional force from the back pressure, in almost every test. Given this systematic difference, there may be an issue in the design. However, a comparison of the results, using a two-sample unequal variance t-test, produced a p-value of 0.49, showing a non-significant difference between them. Further testing would help clarify this. Overall, the total mean flow rate error was 0.38%±1.62%. This is within the 3% requirement (Z-score: 0.125).
The smallest absolute mean flow rate error was the 60mL syringe with 60mL at 60mL/hr with 100mmHg back pressure. The 30mL syringe with 30mL at 5mL/hr produced the largest absolute error (Table 5). Furthermore, both tests of the 30mL syringe had the largest negative accuracy errors. This was unexpected since it is less fluid than in a 60mL syringe so should require less force and produce a more accurate infusion. It may be explained, though, by additional friction between the syringe’s barrel and plunger due to the syringe’s design or manufacturing. This would require extra force to overcome and thus reduce accuracy. Despite this, the mechanism still produced absolute errors less than 3%, demonstrating its ability to overcome differences between syringe brands.
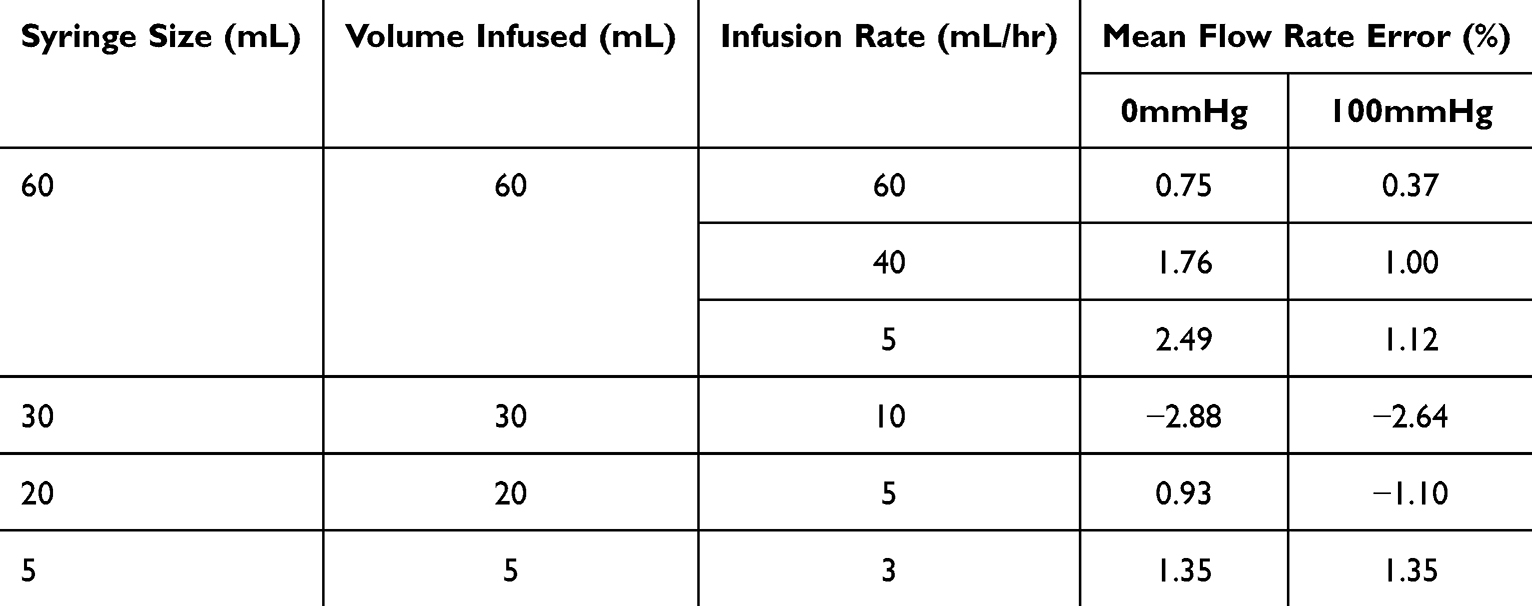 |
Table 5 Results of Mean Flow Rate Testing with Sixteen Microsteps |
The 60mL syringe with 60mL at 5mL/hr produced an error of 2.49% without back pressure (Table 5 and Figure 4) and 1.12% with back pressure (Table 5 and Figure 5). Considering Figure 4, the mean is close to the maximum positive flow rate throughout the infusion, compared to the maximum negative flow rate measurements. This shows that the flow rate is reasonably consistent throughout, with only a few larger random negative errors. However, Figure 5 shows a less stable infusion when back pressure was applied. The closeness of the maximum positive and negative flow rate errors, between the P120 and P360 observation windows, shows a stable infusion with few random errors. In the P418 window, however, the maximum positive error increases. Given the overall mean flow rate error was increased by this, it suggests that many of the errors were larger and positive in this window compared to the previous ones. Since this only occurred in the sixth window, it could have been caused by a disturbance in the experimental setup. Repeating the experiment would evaluate this.
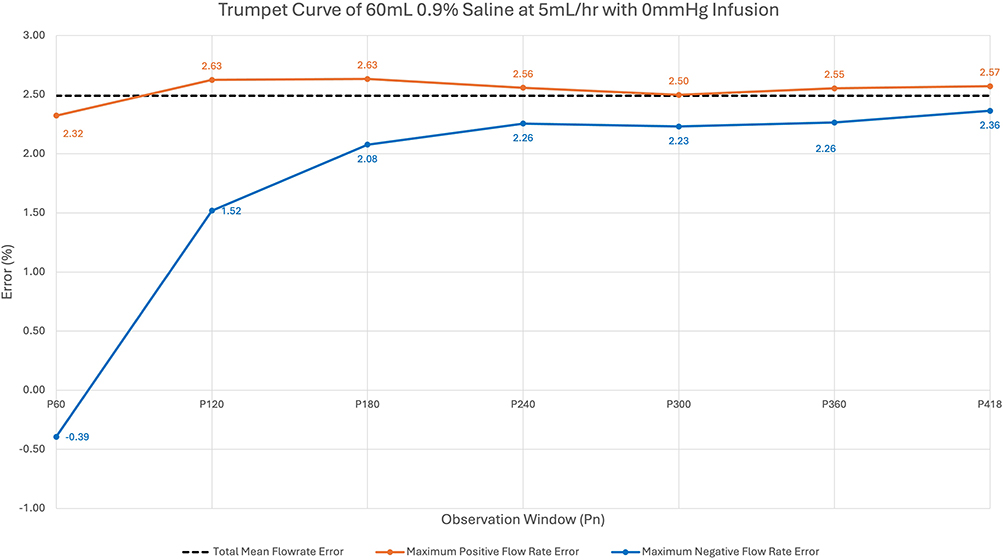 |
Figure 4 Trumpet Curve of 60mL Infusion of 0.9% Saline at 5mL/hr with 0mmHg Back pressure. |
 |
Figure 5 Trumpet Curve of 60mL Infusion of 0.9% Saline at 5mL/hr with 100mmHg Back pressure. |
Discussion
This open-source design is simple, low-cost and portable The design only requires 6 mechanical parts and 8 bolts (Figure 2 and Table 2) that are available online or can be fabricated using a 3D printer, a lathe, and a threading tap. Fewer parts decrease material costs, lower manufacturing complexity, and reduce size and weight for improved portability and storability. Spare parts can be easily procured online or 3D printed for rapid maintenance and repairs. This makes servicing simpler and faster for hospital technicians resulting in continuous pump usage.
Unlike the other screw-based syringe pump designs (Table 1), there is no need for additional screw and guide rod supports. This means the prototype weighs less than 500g and has a reduced footprint. Thus, a syringe pump medical device, designed around this mechanism, would likely be easier to store and transport between wards. Furthermore, this design can accommodate generic consumables and luer lok syringes of any size between 5mL and 60mL without modification, unlike other mechanisms (Table 1).
Limitations of Materials
The accuracy algorithm improved the accuracy of the infusions in 3 of the 4 tests (Table 4), suggesting that it may contribute to improving the accuracy of the device.
However, it reduced the accuracy of the 60mL at 5mL/hr infusion by 11.59%. This suggests that purely UART mode, even with a software solution applied, is not accurate enough for this application. In future prototypes, other protocols, such as STEP/DIR or SPI, should be investigated as they can operate faster and more efficiently than UART. This should reduce accuracy errors further and remove the need for a software solution, however, it may increase the code’s complexity. Furthermore, if bidirectional communication is no longer required, a simpler, lower-cost motor driver could also be used.
Another method of improving accuracy could be the inclusion of a closed feedback loop system; in the same way, Lake et al37 were able to increase the accuracy of Wijnen et al’s design.35 A slide potentiometer could provide low-cost absolute position tracking information. Alternatively, a rotary encoder could be used to provide relative positional information compared to an origin point. Either of these solutions would then allow the microcontroller to adjust the velocity during the infusion to ensure better accuracy. This may remove the need for a software solution, but the feedback loop may increase the complexity of the code. Furthermore, introducing more mechanical parts will increase both the cost and intricacy of the design, in turn reducing serviceability. A cost-benefit analysis will need to be conducted to evaluate any development against the improved accuracy and precision of infusions.
A further potential limitation of this mechanism is durability. The screw and guide rod extend beyond the mechanism’s casing so are not protected by it. Due to this, they are vulnerable to being damaged or bent if a prototype is dropped. Drop testing will need to be used to evaluate the effects of this.
Limitations of Method
A limitation of this method was only testing the design’s accuracy using 0.9% saline solution. Neonates who are unable to accept enteral feeding require parenteral nutrition to prevent malnutrition and nutritional deficits, which limits development and positive outcomes.47 Parenteral nutrition contains lipids, carbohydrates, and proteins, making it more viscous than 0.9% saline solution. A more viscous solution, in the syringe, will produce a greater back pressure on the mechanism, meaning that the motor will require greater torque per microstep to achieve the necessary infusion rates.
The lowest rate tested was 3mL/hr. However, the NEST360/UNICEF specification10 requires pumps to achieve rates as low as 0.1mL/hr. Furthermore, only three settings of microstepping were tested. Future testing should involve fluids of different viscosities, a greater range of infusion rates and more microstepping settings.
An additional limitation is that the literary search was only conducted on two databases. A wider search across more sources would have provided more devices against which the mechanism could be compared.
Future Work
Further work should include the development of a fully functional prototype syringe pump device. This involves following the guidance of the TPP10 to ensure that the device has all of the necessary features. Once a prototype has been developed, it should be presented to clinicians and other stakeholders for their feedback as part of the user-centric, iterative co-design process. Their responses will help to determine future design decisions. Additional technical testing, such as battery life and durability, should then be conducted. Eventually, clinical validation should go ahead to further validate the device. This will allow for accreditation from governing bodies.
Conclusion
This report presented an open-source prototype mechanism, designed to be simple and low-cost, for a neonatal syringe pump. The mechanism’s accuracy was tested by recording the time taken to infuse 75% of the nominal volume, as per ISO 286020:2020 standards.44 Rates between 3mL/hr and 60mL/hr were tested on 5mL, 20mL, 30mL and 60mL syringes. During testing, the mechanism achieved a mean accuracy of 0.38%±1.62%; within the 3% error requested by the UNICEF and NEST360 TPP.10 An accuracy algorithm was also tested, however, it was not shown to have a consistently beneficial effect on the prototype’s accuracy.
Future testing should involve a greater range of rates and more viscous fluids. Further advancements can be made to the mechanism, such as using the SPI protocol for velocity control and a closed-loop feedback system for positional accuracy. A complete syringe pump device, based upon this prototype, could now be developed, but concerns such as durability should be addressed.
Data Sharing Statement
The data that support the findings of this study are available from the corresponding Prashant Jha, P.J., upon reasonable request.
Acknowledgment
The authors have no acknowledgements.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was supported by the UK Engineering and Physical Sciences Research Council under Grant EP/R513064/1.
Disclosure
The authors have no competing interests for this work.
References
1. UNICEF. Neonatal mortality. 2025. Available from: https://data.unicef.org/topic/child-survival/neonatal-mortality/.
2. Lucia H, Sinae L, Yang L, et al. Levels and Trends in Child Mortality 2021. Technical report, UNICEF, World Health Organization, World Bank Group, United Nations, 2021.
3. UNICEF and World Health Organization. SURVIVE and THRIVE Transforming care for every small and sick newborn. Technical report, 2019.
4. United Nations. The Sustainable Development Goals Report. Technical report, 2021.
5. UNICEF. Data and Analytics Section. Progress on children’s well-being centring child rights in the 2030 Agenda for every child, a sustainable future. Technical report.
6. Organisation for Economic Co-operation and Development, World Health Organization, and World Bank Group. Delivering quality health services: a global imperative for universal health coverage. Technical report, 2018.
7. World Health Organization. WHO Guidelines for Safe Surgery 2009 Safe Surgery Saves Lives. Technical report, 2009.
8. World Health Organization. Medical devices: managing the Mismatch An outcome of the Priority Medical Devices project. Technical report, 2010.
9. Kirby R, Molyneux E, Langton J, Werdenberg J, Palamountain K. Newborn Technology Landscape: technologies for Newborn Care in Low-Resource Settings: 10th Edition Technical Report. Technical report, NEST360, 2023.
10. Kirby R, Palamountain K. Target Product Profiles for Newborn Care in Low-Resource Settings (v1.2). 2020.
11. Boniol M, Kunjumen T, Siyam A, Campbell J, Diallo K, Diallo K. The global health workforce stock and distribution in 2020 and 2030: a threat to equity and ‘universal’ health coverage? BMJ Global Health. 2023;7(6):e009316. doi:10.1136/bmjgh-2022-009316
12. World Health Organization. Health Workforce;2013.
13. World Health Organization. Nursing and Midwifery. 2024.
14. Oosting RM, Wauben LSGL, Groen RS, Dankelman J. Equipment for essential surgical care in 9 countries across Africa: availability, barriers and need for novel design. Health Technol. 2019;9(3):269–275. doi:10.1007/s12553-018-0275-x
15. John GM, Andrew JML, Lars H, et al. Global Surgery 2030: evidence and solutions for achieving health, welfare, and economic development. Lancet. 2015;386(9993):569–624.
16. Perry L, Malkin R. Effectiveness of medical equipment donations to improve health systems: how much medical equipment is broken in the developing world? Med Biol Eng Comput. 2011;49(7):719–722. doi:10.1007/s11517-011-0786-3
17. World Health Organization. Medical Device Donations: Considerations for Solicitation and Provision.
18. UNICEF and World Health Organization. Protect the promise: 2022 progress report on the Every Woman Every Child Global Strategy for Women’s, Children’s and Adolescents’ Health (2016–2030). Technical report, 2022.
19. United Nations, United Nations Industrial Development Organization. United Nation UNCTAD, UNAIDS, UNICEF, and The Global Fund. Interagency Statement on Promoting Local Production of Medicines and other Health Technologies. Technical report, 2019.
20. World Health Organization. The World Bank, International Renewable Energy Agency, and Sustainable Energy for All. Energizing Health: Accelerating Electricity Access in Health-Care Facilities. 2023.
21. U.S. Food and Drug Administration. Infusion Pumps —. FDA. 2018.
22. Aufieri R, Picone S, Paolillo P. Collaborative development of open source-appropriate technologies: a way to reduce the global access gap? BMJ Innovations. 2015;1(2):37–38. doi:10.1136/bmjinnov-2014-000034
23. De Maria C, Mazzei D, Ahluwalia A. Open source biomedical engineering for sustainability in African healthcare: combining academic excellence with innovation.
24. Niezen G, Eslambolchilar P, Thimbleby H. Parisa Eslambolchilar, and Harold Thimbleby. Open-source hardware for medical devices. BMJ Innovations. 2016;2(2):78–83. doi:10.1136/bmjinnov-2015-000080
25. Ibrahim AMS, Jose RR, Rabie AN, Gerstle TL, Lee BT, Lin SJ. Three-dimensional printing in developing countries. Plastic Reconst Surg Global Open. 2015;3(7):e443. doi:10.1097/GOX.0000000000000298
26. UNICEF Office of Innovation. Encouraging Student Humanitarian Work. 2015.
27. UNICEF Office of Innovation. Are You an Open Source Technology Start-Up? 2016.
28. Abu-Haydar E, Katuntu D, Bauer J, et al. User-Centered Design: developing the RELI Delivery System - a Low-Cost, Non-Electric, Pneumatic Infusion Pump. Med Dev. 2021;14:185–192. doi:10.2147/MDER.S295893
29. Islam MR, Rusho RZ, Islam SMR. Design and implementation of low cost smart syringe pump for telemedicine and healthcare.
30. Khan MA, Mazhar O, Tehami S.
31. Sadegh-Cheri M. Using the recycled parts of a computer dvd drive for fabrication of a low-cost arduino-based syringe pump. J Chem Educ. 2022;99(2):525. doi:10.1021/acs.jchemed.1c00260
32. Samokhin AS. Syringe pump created using 3d printing technology and arduino platform. J Anal Chem. 2020;75(3):416–421. doi:10.1134/S1061934820030156
33. Supriyanto A, Anggriani R, Suciyati SW, Surtono A, Hadi S, Hadi S. A control system on the syringe pump based on arduino for electrospinning application. J Phys Sci. 2021;32:1–12. doi:10.21315/jps2021.32.1.1
34. Vigneshwari N, Saranraj V, Ibrahim AM, Girivasan K.
35. Wijnen B, Hunt EJ, Anzalone GC, Pearce JM. Open-source syringe pump library. PLoS One. 2014;9:e107216. doi:10.1371/journal.pone.0107216
36. Coskun H, Gul O, Ferhanoglu O, Gokdel YD. Design and implementation of a low-cost high-performance syringe pump system.
37. Lake JR, Heyde KC, Ruder WC. Low-cost feedback-controlled syringe pressure pumps for microfluidics applications. PLoS One. 2017;12:e0175089. doi:10.1371/journal.pone.0175089
38. Juarez A, Maynard K, Skerrett E, et al. AutoSyP: a Low-Cost, Low-Power Syringe Pump for Use in Low-Resource Settings. American JTrop Med Hyg. 2016;95(4):964–969. doi:10.4269/ajtmh.16-0285
39. Kujawa M, a SM, Gonet M, Pietrzyk R, Czechowski T, Aj Baranowski M. Low-cost, programmable infusion pump with bolus mode for in-vivo imaging. HardwareX. 2021;9:e00194. doi:10.1016/j.ohx.2021.e00194
40. Abdelhamid T, Aboumeshrafa K, Rahma AG. Design and experiment of an open-source syringe pump for blood flow applications.
41. TRINAMIC Motion Control GmbH & Co. KG. TMC2209 Datasheet. Technical report.
42. Earley A, Fayers P, Ng S, Shinebourne EA, De Swiet M. Blood pressure in the first 6 weeks of life. Arch Dis Childhood. 1980;55(10):755. doi:10.1136/adc.55.10.755
43. International Electrotechnical Commission. IEC 60601-2-24:2012 — IEC Webstore. 2012.
44. ISO. ISO 28620:2020 - Medical Devices — Non-Electrically Driven Portable Infusion Devices. 2020.
45. GMBH DRFRITZFAULHABER, KG CO. Stepper motor technical note: microstepping myths and realities. Technical report, DR. FRITZ FAULHABER GMBH & CO. KG, 2020.
46. Pleus S, Kamecke U, Waldenmaier D, Freckmann G. Reporting Insulin Pump Accuracy: trumpet Curves According to IEC 60601-2-24 and Beyond. J Diabet Sci Technol. 2019;13(3):592–596. doi:10.1177/1932296818806509
47. Mustapha M, Wilson KA, Barr S. Optimising nutrition of preterm and term infants in the neonatal intensive care unit. Paediatrics Child Health. 2021;31:31–45.
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.