")
Back to Journals » ClinicoEconomics and Outcomes Research » Volume 15
Descriptive Epidemiology and Outcomes of Patients with Short Stay Hospitalizations for the Treatment of Congestive Heart Failure in the US
Authors Zilberberg MD , Nathanson BH, Sulham K, Mohr JF, Goodwin MM, Shorr AF
Received 9 December 2022
Accepted for publication 2 February 2023
Published 24 February 2023 Volume 2023:15 Pages 139—149
DOI https://doi.org/10.2147/CEOR.S400882
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Samer Hamidi
Marya D Zilberberg,1 Brian H Nathanson,2 Katherine Sulham,3 John F Mohr,3 Matthew M Goodwin,3 Andrew F Shorr4
1EviMed Research Group, LLC, Goshen, MA, USA; 2Optistatim, LLC, Longmeadow, MA, USA; 3scPharmaceuticals, Burlington, MA, USA; 4Washington Hospital Center, Washington, DC, USA
Correspondence: Marya D Zilberberg, EviMed Research Group, LLC, PO Box 303, Goshen, MA, 01032, USA, Email [email protected]
Background: Congestive heart failure (CHF) hospitalizations cost the US $35 billion annually. Two-thirds of these admissions, generally requiring Methods: Among patients discharged with CHF as the principal diagnosis (PD), we compared characteristics and outcomes between those with hospital length of stay (LOS) 3 days (long, LLOS) in a cross-sectional multicenter analysis within the 2018 National Inpatient Sample. We applied complex survey methods to calculate nationally representative results.
Results: Among 4,979,350 discharges with any CHF code, 1,177,910 (23.7%) had CHF-PD, of whom 511,555 (43.4%) had SLOS. Patients with SLOS were younger (>/=65 years: 68.3% vs 71.9%), less likely covered by Medicare (71.9% vs 75.4%), and had a lower comorbidity burden (Charlson: 3.9 [2.1] vs 4.5 [2.2) than patients with LLOS; they less frequently developed acute kidney injury (0.4% vs 2.9%) or a need for mechanical ventilation (0.7% vs 2.8%). A higher proportion with SLOS than with LLOS underwent no procedures (70.4% vs 48.4%). Mean LOS (2.2 [0.8] vs 7.7 [6.5]), direct hospital costs ($6150 [$4413]) vs $17,127 [$26,936]), and aggregate annual hospital costs $3,131,560,372 vs $11,359,002,072) were all lower with SLOS than LLOS. All comparisons reached alpha = 0.001.
Conclusion: Among patients admitted for CHF, nearly ½ have LOS
Keywords: congestive heart failure, epidemiology, outcomes, hospital, costs
Introduction
Hospitalizations are a major driver of healthcare costs in the US, constituting nearly 1/3 of total US healthcare expenditures.1 In addition to the adverse economic consequences, hospitalization disrupts patients’ lives and exposes them to risks of contracting hospital-acquired complications (HAC). In 2016, for example, there were nearly 50,000 cases of HACs responsible for over 3000 deaths and $2 billion in excess costs in the US.2 For these reasons, many interventions focus on preventing hospitalization.
Congestive heart failure (CHF) represents a leading reason for hospitalization. Annually in the US there are over 4 million admissions that involve CHF, adding in aggregate $35 billion in direct costs, and accounting for 75–80% of the total annual direct costs associated with CHF care.3–5 Further raising these costs is the potential for HACs in this disproportionately elderly population. For example, recent analyses suggest that one out of every 13 patients admitted with CHF develops hospital-acquired pneumonia, leading to a substantially elevated subsequent risk of death.6
According to some calculations, as many as 2/3 of all admissions for the treatment of CHF are potentially avoidable.7 Some of the common features of such admissions include: 1) not requiring advanced care beyond intravenous (IV) diuresis, 2) lack of the need for an escalation of such therapy, and 3) short durations of hospital stay (LOS), generally under four days. Since worsening signs and symptoms of congestion due to fluid overload are the most common reasons for hospitalization among patients with CHF, one can postulate that at least some of these admissions could be avoided with optimizing diuresis strategies among persons likely not to require a prolonged hospital stay.8,9 While it is understood that patients admitted for CHF exacerbations on average spend 5.4 days in the hospital, this value, representing the mean of those with both short and long stays, does not shed light on the potential to reduce hospital days and the attendant cost savings.10 To understand the present-day volume and outcomes of such potentially avoidable hospitalizations in the US, we conducted an analysis in the National Inpatient Sample (NIS) comparing patients with shorter LOS (≤3 days) and longer LOS (>3 days) so as to describe similarities and differences between their characteristics and outcomes, as well as to quantify the annual aggregate hospital costs for those potentially avoidable hospitalizations.
Materials and Methods
Data Availability
The data that support the findings of this study are available from the corresponding author upon reasonable request.
Ethics Statement
Because this study used publicly available fully de-identified data, it was exempt from ethics review under US 45 CFR 46.101(b)4.11
Study Design and Patient Population
We conducted a multicenter cross-sectional study of adult patients (age >/= 18 years) admitted to all US acute care hospitals in the year 2018 for treatment of CHF. Our case identification approach relied on a previously published administrative algorithm, as recommended by the American College of Cardiology (ACC)/American Heart Association (AHA) guidelines and included the following ICD-10-CM codes: I11.0, I13.0, I13.2, I50.1, I50.20, I50.21, I50.22, I50.23, I50.30, I50.31, I50.32, I50.33, I50.40, I50.41, I50.42, I50.43, I50.9.12–14 To optimize the specificity of this algorithm we also included patients with DRG codes 291, 292, 293.
Because we sought to describe the population that could potentially avoid hospitalization due to worsening heart failure, we included only discharges with CHF as the principal diagnosis, indicating that it was the primary reason for admission. We excluded all transfers from another acute care institution, as data on their hospitalization at the referring hospital are not available in the NIS. We defined a hospital’s CHF caseload as a proportion of all admissions at that hospital that fit the CHF criteria.
Data Source
The NIS, a database publicly available from the Agency for Healthcare Research and Quality, approximates a 20-percent stratified sample of discharges from US community hospitals, excluding rehabilitation and long-term acute care hospitals.15 It is specifically designed to identify, track, and analyze national trends in health care utilization, access, direct hospital costs and charges, quality, and outcomes. NIS cost-to-charge ratios (CCRs) are calculated as the ratio of total costs to total charges based on the cost report for specific hospitals.16 The CCRs are in turn applied to total charges, as reported on inpatient encounter records, to produce an estimate of direct service delivery costs. Covering approximately 97% of the US population, complex survey methods estimate over 35 million annual hospitalizations, and aid in developing national estimates for specific conditions listed in the database.15
The unit of analysis in this database is a discharge and not a patient. Thus, it is not feasible to distinguish rehospitalizations from index hospitalizations for any single patient. In the current manuscript, we use the terms “hospitalization”, “admission”, and “discharge” interchangeably.
Statistical Analyses
We compared demographic, clinical, and hospital characteristics of the individual discharges, as well as their hospital outcomes between the groups requiring shorter LOS (SLOS, defined as </= 3 days) and longer LOS (LLOS, defined as > 3 days). Between these groups, we further stratified comparisons of hospital mortality by age (under 65 vs 65+ years), gender, race, and day of hospitalization to characterize further subgroups likely to be considered high- vs low-risk for outpatient therapy.
We report continuous variables as means with standard deviations (SD) and as medians with interquartile ranges (IQR), and categorical variables as percentages based on complex survey methods that weight strata provided by NIS. For the rare occasion where a stratum contained a single hospitalization, the stratum was centered at the grand mean rather than the stratum mean. Because the intent of the study was to provide descriptive epidemiology of potentially avoidable hospitalizations in the US, we did not attempt to model the outcomes to adjust for confounding.
Results
Among 4,979,350 discharges with any CHF code, 1,177,910 (23.7%) had CHF-PD, of whom 511,555 (43.4%) had SLOS, with the rest having LLOS. Compared to LLOS, a lower proportion of SLOS were hospitalized in urban teaching institutions (62.7% vs 69.9%) and in hospitals located in the Northeast (16.1% vs 20.8%), and a higher proportion in small hospitals (24.9% vs 20.9%) and in the West (19.6% vs 15.4%) (Table 1). The proportion of hospitalizations for CHF associated with shorter vs longer LOSs did not vary as a function of hospital mean CHF caseload volume. While there were minimal differences between the groups by race, patients with SLOS were younger (>/=65 years: 68.3% vs 71.9%), less likely to be covered by Medicare (71.9% vs 75.4%), and had a lower co-morbidity burden (mean Charlson: 3.9 [2.1] vs 4.5 [2.2]) than patients with LLOS (Table 1). As for individual comorbidities, nearly all patients suffered from hypertension, and nearly all enumerated conditions were more prevalent in LLOS than SLOS (Figure 1). Notably, discharges in the LLOS group were far more likely to have such disorders as cardiac arrhythmias, fluid and electrolyte imbalances, complicated diabetes, and renal failure, to name a few.
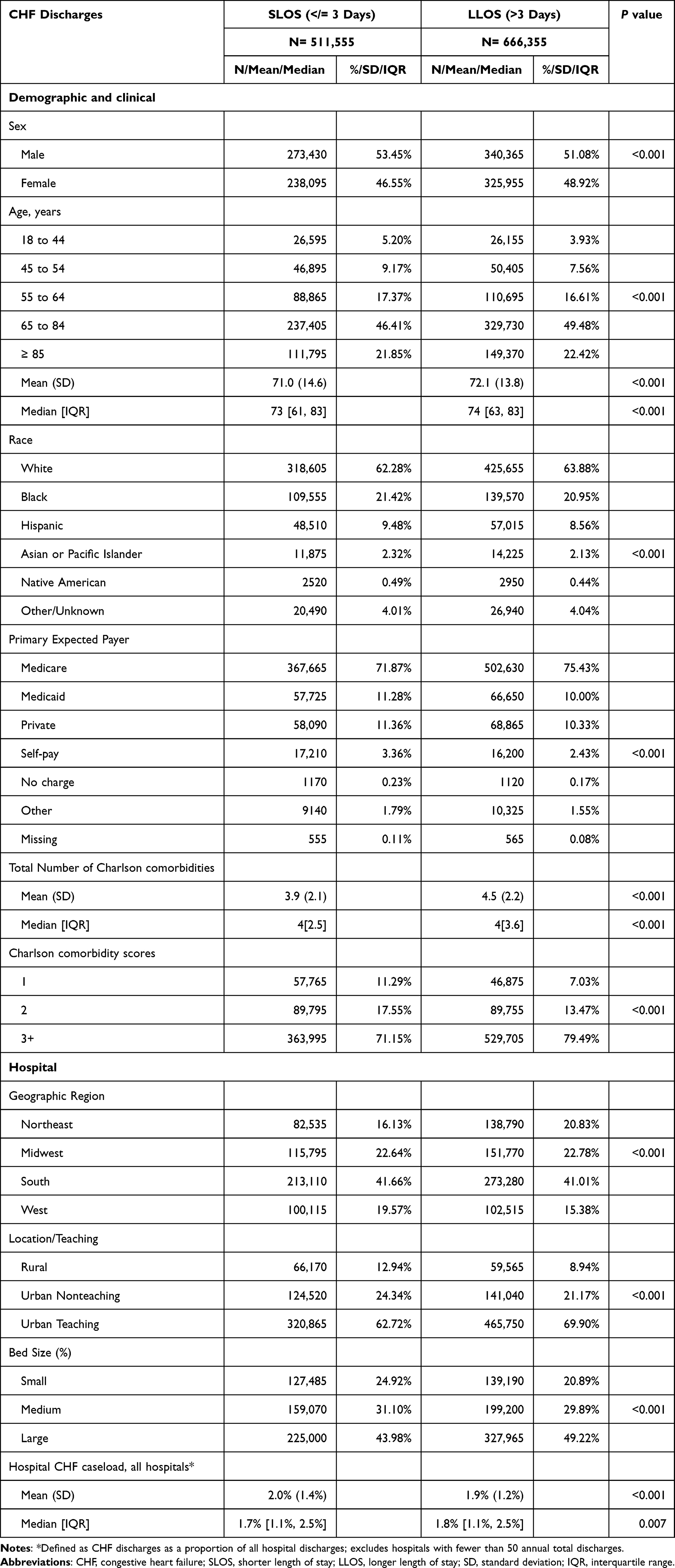 |
Table 1 Baseline Characteristics |
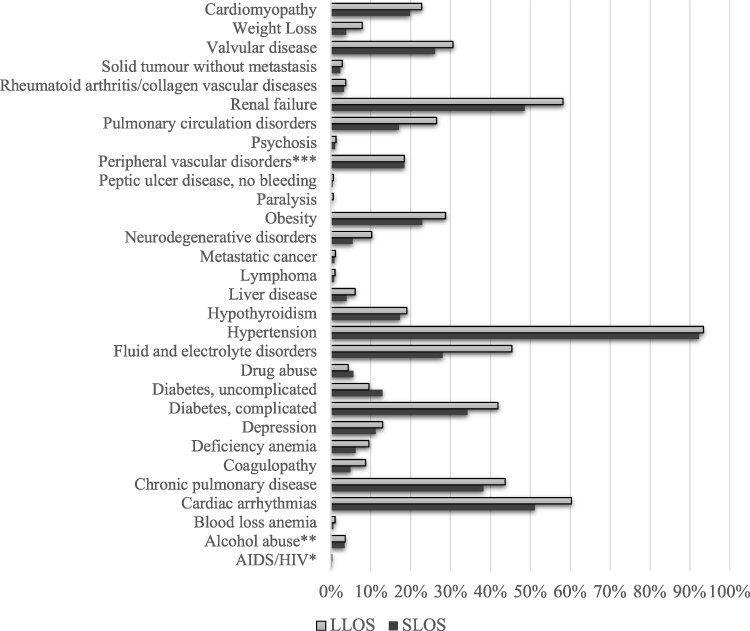 |
Figure 1 Individual comorbidities. P values for all comparisons are <0.001 with the exception of: *P=0.070, **P=0.063, ***P=0.714. Abbreviations: SLOS, shorter length of stay; LLOS, longer length of stay. |
The two groups were similar with regard to admission source (nearly 90% from the emergency department), and admission type (>95% non-elective; ie, urgent or emergent) (Table 2). Compared to those with LLOS, during hospitalization, patients with SLOS were less likely to develop acute kidney injury (20.3% vs 39.0%), need dialysis (0.4% vs 2.9%), or require mechanical ventilation (0.7% vs 2.8%). Patients with SLOS underwent fewer procedures overall (0.5 [1.1] vs 1.5 [2.6]), and a higher proportion had no procedures (70.4% vs 48.4%) than those with LLOS. Mean LOS was 2.2 (0.8) days in SLOS and 7.7 (6.5) in LLOS, and more in SLOS had a routine discharge home (61.8% vs 39.7%). Mean direct hospital costs in LLOS ($17,127 [$26,936]) were ~ 3-fold higher than those in SLOS ($6150 [$4413]). The aggregate annual costs mirrored individual costs, with $11,359,002,072 among discharges with LLOS and $3,131,560,372 with SLOS (Table 2).
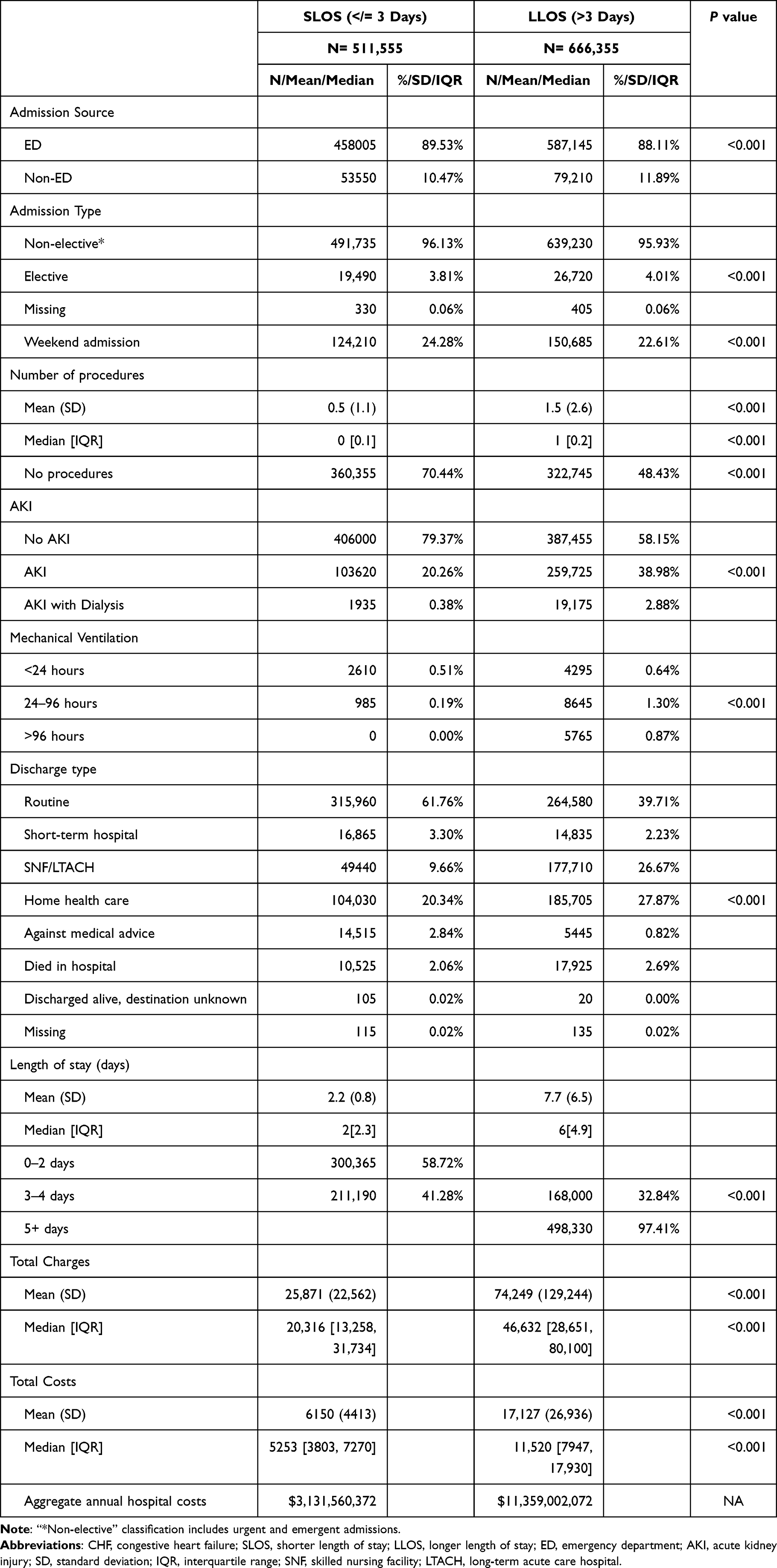 |
Table 2 Hospitalization Characteristics and Outcomes |
In the comparisons stratified by age, gender, and race, mortality was consistently lower in SLOS than LLOS group. These differences were larger among those under 65 years than 65 years or older (Figure 2). Similar distinctions persisted across gender and certain racial groups. The highest percent mortality occurred among those whose LOS was shortest (10.6% on admission day), followed by late in the hospitalization, on day 10 and beyond (5.7%) (Figure 2).
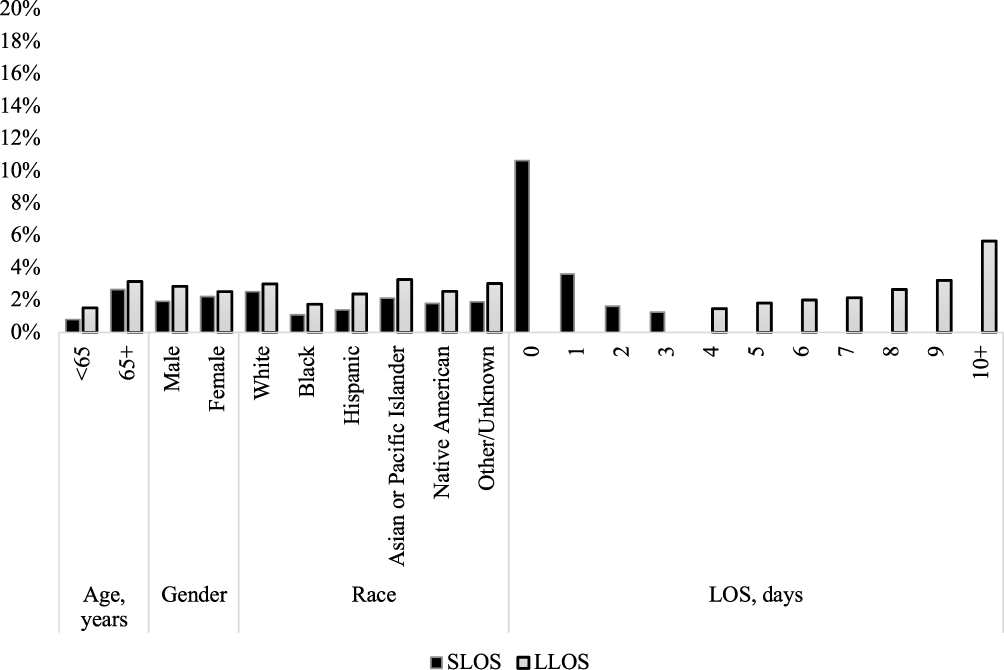 |
Figure 2 Stratified mortality*. *P values for all comparisons are <0.001. Abbreviations: SLOS, shorter length of stay; LLOS, longer length of stay. |
Discussion
We have demonstrated that among patients admitted specifically for the management of CHF exacerbation, 43% require 3 days or fewer in the hospital, with one-half of these discharged after only 2 days. Furthermore, nearly ¾ of the SLOS group did not require any procedures during their hospitalization. The mean direct hospital costs in the SLOS group were $6150, or about 1/3 of the costs in LLOS, or $17,127. Because all of the admissions were specifically for the treatment of CHF, it is fair to assume that the entirety of these costs can be attributed to CHF. To put this into context, reimbursements for DRGs 291, 292, and 293 are $7764, $5286, and $3611, respectively, with the weighted mean payment of $6944.17 While costs with SLOS were lower than those in the LLOS group, they were not inconsequential, adding up in aggregate to over $3 billion in 2018. The characteristics of those with short admissions for CHF raise the issue of whether the admission was avoidable altogether, potentially avoiding the inconvenience and risks associated with hospitalization while also saving the healthcare system substantial resources.
Our findings have several important implications. First, if even one-half of this population could be successfully treated as outpatients, over $1.5 billion could be saved annually in both CHF-related and general healthcare costs for these patients. A recent systematic review of literature dealing with costs of heart failure in the US noted that hospitalization costs vary based on the presence of comorbidities and age.18 It is, therefore, possible that at least some of the reduction in the cost of SLOS compared to LLOS is due to a somewhat younger and less chronically ill population comprising the former group. However, it is very likely that a much greater proportion of this difference is driven by the large gap in the hospital LOS between SLOS and LLOS groups. Regardless of the reasons, the fact remains that cost savings from avoiding these admissions could be significant. And given that over 2/3 of this population is on Medicare, these savings would be a substantial advance toward its solvency. Second, a hospitalization necessarily exposes a patient to the risk of contracting a HAC. For example, a recent analysis from Japan suggests that 8% of patients hospitalized for treatment of a CHF exacerbation develop HAP, one of the costliest and deadliest of HACs.6 In this study, incident HAC raised the risk of hospital death to staggering degree from 1% in its absence to 12% in the presence of HAP. In addition, the rate of CHF worsening rose 4-fold from the baseline of 7% to 28%, along with a consequent LOS prolongation. Although we were unable to explore incident HACs or their impacts in the current analysis, it is quite likely that at least some of the patients in the SLOS group developed HACs, which incurred costs that were potentially avoidable if the in hospitalization had not transpired. Third, and along the same lines, it is possible and even likely that some of the patients in the LLOS were subjects who might otherwise have been discharged earlier were it not for the development of some nosocomial complication. The precise impact of HACs on this population is a question that needs attention in future studies.
Our study builds on previous efforts to define groups of CHF patients who, despite being admitted for the management of their exacerbations, may, given minor treatment pathway alterations, be able to avoid hospitalization. Greene and coworkers analyzed a large and geographically diverse US multicenter electronic health record database between 2007 and 2018 with the view to further our understanding of inpatient CHF treatment intensity.7 They discovered that in a cohort of over 22,000 adult patients with a reduced ejection fraction hospitalized for CHF exacerbations and with no evidence of a concurrent acute coronary syndrome, approximately 2/3 did not require escalation of their treatment beyond IV diuretic started at admission. Despite having the shortest time on diuretics, this group was nevertheless least likely to die or to require a readmission within 30 days of discharge relative to other groups where treatment had been escalated. Although our population is slightly different from that examined by Greene et al we did focus on patients admitted specifically for the treatment of CHF, and by contrasting groups based on their hospital LOS, attempted to identify a group that, similar to that in the Greene analysis, might be considered less complex and resource intensive than others. Although our estimate of 43% of this population falling into this category is lower than the prior number, it is still quite substantial. We add to the literature on this population by quantifying explicitly not only its annual volume in the US, but also the potential opportunity for cost savings if inpatient treatment could be avoided.
Our study, although large and highly generalizable, has a number of limitations. Because our case definition relied on administrative coding, there may be misclassification. However, we did employ a previously published algorithm that has been used routinely by many other investigators and recommended in the ACA/AHA guidelines.12–14 Another important limitation is our inability to differentiate between initial and repeat hospitalizations. However, given the aim of the study, this did not preclude us from estimating the full burden of hospitalizations for the treatment of a CHF exacerbation. Because the study is purely descriptive, we did not attempt to draw any inferences or causalities, and thus confounding is not a concern. The structure of the current dataset did not allow us to explore drug treatments given to these patients, and this may have contributed to misclassifying other conditions that mimic CHF as actual CHF. However, since we focused specifically on patients with the principal diagnosis of CHF, it, and not another cause, is likely to have been the primary reason for admission.
Conclusions
In summary, we have quantified not only the current annual burden of inpatient admissions for CHF in the US, but also described in detail a group of patients whose hospitalizations may be averted by retooling some outpatient procedures and making them more conducive to effective outpatient diuresis. This group of patients is large and costly, and the savings from converting their treatment from inside the hospital to the outpatient setting would be substantial, even if even a fraction of this population could avoid admission. Future investigations need to provide more granular descriptions of this population to establish in detail how to identify these patients a priori. In addition, data on the incidence of various important HACs complicating these potentially avoidable admissions would contribute to a fuller picture of their healthcare resource utilization.
Abbreviations
CHF, congestive heart failure; PD, principal diagnosis; LOS, length of stay; SLOS, short LOS; HLOS, long LOS; HAC, hospital-acquired complications; IV, intravenous; NIS, National Inpatient Sample; ACC, American College of Cardiology; AHA, American Heart Association; CCR, cost-to-charge ratio; SD, standard deviation; IQR, interquartile range.
Data Sharing Statement
The data that support the findings of this study are available from the corresponding author upon reasonable request.
Ethics Statement
Because this study used publicly available fully de-identified data, it was exempt from ethics review under US 45 CFR 46.101(b)4.11
Acknowledgments
No person other than the listed authors participated in the study, its design, or its reporting.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study was supported by a grant from scPharmaceuticals, Burlington, MA, USA. Portions of these data have been presented as a poster at the HFSA 2022 annual conference.
Disclosure
- MDZ’s employer, EviMed Research Group, LLC, has received research grant support from scPharmaceuticals, Burlington, MA, USA. Also, reports grants as a consultant from Merck, Melinta, Pfizer, Spero, Astellas, Shionogi and Lungpacer; owns stocks from J&J, outside the submitted work.
- BHN’s employer, OptiStatim, LLC, has received support from EviMed Research Group, LLC, Goshen, MA, USA.
- KS has consulted for and reports personal fees from scPharmaceuticals, Burlington, MA, USA.
- JFM is an employee scPharmaceuticals, Burlington, MA, USA.
- MMG is an employee scPharmaceuticals, Burlington, MA, USA.
- AFS is a clinical consultant to EviMed Research Group, LLC, Goshen, MA, USA. He has been a clinical consultant to and has received research grant support from scPharmaceuticals. Also, he has received grant support and/or has served as a consultant to Spero, Melinta, Pfizer, Astellas, Shionogi, and Lungpacer.
References
1. Kurani N, Ortaliza J, Wager E, Fox L, Amin K. How has US spending on healthcare changed over time? Peterson-KFF health system tracker; 2022. Available from: https://www.healthsystemtracker.org/chart-collection/u-s-spending-healthcare-changed-time/#Contribution%20to%20change%20in%20total%20national%20health%20expenditures,%20from%202019-2020,%20by%20spending%20category.
2. IBM Watson Health Research Brief. Hospital-acquired conditions lead to avoidable cost and excess deaths; 2018. Available from: https://www.ibm.com/downloads/cas/X97QXLER.
3. Patel J. Heart failure population health considerations. Am J Manag Care. 2021;27(suppl 9):S191–S5.
4. Khan SU, Khan MZ, Alkhouli M. Trends of clinical outcomes and healthcare resource use in heart failure in the United States. J Am Heart Assoc. 2020;9:e016782. doi:10.1161/JAHA.120.016782
5. Heidenreich PA, Fonarow GC, Opsha Y, Sandhu AT, Sweitzer NK, Warraich HJ. Economic issues in heart failure in the United States. J Card Fail. 2022;28:453–466. doi:10.1016/j.cardfail.2021.12.017
6. Tada A, Omote K, Nagai T, et al. Prevalence, determinants, and prognostic significance of hospital acquired pneumonia in patients with acute heart failure. J Clin Med. 2020;9:2219. doi:10.3390/jcm9072219
7. Greene SJ, Triana TS, Ionescu-Ittu R, et al. In-Hospital therapy for heart failure with reduced ejection fraction in the United States. JACC Heart Fail. 2020;8:943–953. doi:10.1016/j.jchf.2020.05.013
8. Mullens W, Damman K, Harjola V-P, et al. The use of diuretics in heart failure with congestion – a position statement from the heart failure association of the European Society of Cardiology. Eur J Heart Fail. 2019;21:137–155. doi:10.1002/ejhf.1369
9. Greene SJ, Mentz RJ, Fleker M. Outpatient worsening heart failure as a target for therapy: a review. JAMA Cardiol. 2018;3:252–259. doi:10.1001/jamacardio.2017.5250
10. Agency for Healthcare Research and Quality HCUPNet Healthcare Cost and Utilization Project Hospital Inpatients National Statistics. National diagnoses – Clinical Classification Software Refined (CCSR), principal diagnosis: CIR019 heart failure; 2018. Available from: hcupnet.ahrq.gov.
11. US Department of Health and Human Services Office for Human Research Protections. Human subject regulations decision charts. Available from https://www.hhs.gov/ohrp/regulations-and-policy/decision-charts/index.html.
12. Akintoye E, Briasoulis A, Egbe A, et al. National trends in admission and in-hospital mortality of patients with heart failure in the United States (2001–2014). J Am Heart Assoc. 2017;6:e006955. doi:10.1161/JAHA.117.006955
13. American Heart Association. American Heart Association get with the guidelines – heart failure HF factsheet; 2016. Available from: https://www.heart.org/idc/groups/heart-public/@wcm/@hcm/@gwtg/documents/downloadable/ucm_467882.pdf.
14. Presley CS, Min JY, Chipman J, et al. Validation of an algorithm to identify heart failure hospitalisations in patients with diabetes within veterans health administration. BMJ Open. 2018;8:e020455. doi:10.1136/bmjopen-2017-020455
15. Overview of the National (Nationwide) Inpatient Sample (NIS). Available from: https://www.hcup-us.ahrq.gov/nisoverview.jsp.
16. Pickens GT, Liang L, Roemer M HCUP cost-to-charge ratio methodologies. 2021. HCUP methods series report # 2021-05 ONLINE; 2021. U.S. Agency for Healthcare Research and Quality. Available from: http://www.hcupus.ahrq.gov/reports/methods/methods.jsp.
17. Centers for Medicare and Medicaid Services. FY 2022 IPPS final rule home page. Available from: https://www.cms.gov/medicare/acute-inpatient-pps/fy-2022-ipps-final-rule-home-page#Tables.
18. Urbich M, Globe G, Pantiri K, Heisen M, Bennison C, Wirtz HS. A systematic review of medical costs associated with heart failure in the USA (2014–2020). Pharmacoeconomics. 2020;38:1219–1236. doi:10.1007/s40273-020-00952-0
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.