Back to Journals » Clinical Ophthalmology » Volume 17
Descemet’s Membrane Endothelial Keratoplasty for Corneal Endothelial Failure Secondary to Three Types of Phakic Intraocular Lens – Retrospective Study
Authors Moura-Coelho N ![]() , Cunha JP, Dias-Santos A
, Cunha JP, Dias-Santos A ![]() , Dutra-Medeiros M, Papa-Vettorazzi R
, Dutra-Medeiros M, Papa-Vettorazzi R ![]() , Manero F, Güell J
, Manero F, Güell J
Received 30 December 2022
Accepted for publication 23 February 2023
Published 19 March 2023 Volume 2023:17 Pages 931—940
DOI https://doi.org/10.2147/OPTH.S401387
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Nuno Moura-Coelho,1– 4 João Paulo Cunha,4,5 Arnaldo Dias-Santos,2,6 Marco Dutra-Medeiros,2,6 Renato Papa-Vettorazzi,1 Felicidad Manero,1 José Güell1,3,7
1Cornea and Refractive Surgery Unit, Instituto Microcirugía Ocular (IMO) Barcelona, Barcelona, Spain; 2Ophthalmology, Faculdade de Ciências Médicas – Universidade Nova de Lisboa (NMS|FCM-UNL), Lisbon, Portugal; 3Anterior Segment, European School for Advanced Studies in Ophthalmology (ESASO), Lugano, Switzerland; 4Ophthalmology, Escola Superior de Tecnologias da Saúde de Lisboa (ESTeSL) – Instituto Politécnico de Lisboa, Lisbon, Portugal; 5Ophthalmology, Hospital CUF Cascais, Cascais, Portugal; 6Ophthalmology, Centro Hospitalar Universitário Lisboa Central (CHULC), Lisbon, Portugal; 7Ophthalmology, Universidad Autónoma de Barcelona (UAB), Barcelona, Spain
Correspondence: Nuno Moura-Coelho, Email [email protected]
Purpose: To analyze the outcomes of Descemet’s membrane endothelial keratoplasty (DMEK) for corneal endothelial failure secondary to phakic intraocular lens implantation (PIOL) at a reference center for corneal transplantation in Spain.
Design: Retrospective, single-surgeon case series.
Methods: Single-center analysis of patients who underwent DMEK for PIOL-related corneal decompensation between July 2011 and July 2020 with at least 6 months of follow-up postoperatively. Primary outcome was final best-corrected visual acuity (BCVA, logMAR) compared to pre-DMEK BCVA. Secondary outcomes analyzed included post-DMEK refractive spherical equivalent, endothelial cell loss (%ECL), and graft failure.
Results: Sixteen eyes (14 patients) underwent DMEK for PIOL-related corneal decompensation. Mean (SD) time to PIOL explantation was 9.3 (5.0) years, and median (P25-P75) time between PIOL explantation and DMEK surgery was 3 (2– 4) months. Median pre-DMEK BCVA was 0.80 (1.08– 0.60) logMAR. A statistically significant improvement in BCVA was observed 1 month after DMEK (p = 0.001), and median final BCVA was 0.15 (0.0– 0.35) logMAR (p = 0.002). Mean %ECL was 55.6 (18.7) % at 2-year follow-up and 61.7 (11.7) % in eyes with over 4 years of follow-up. Two eyes required re-bubbling (12.5%), one of which ended in primary graft failure (6.2%) and one eye had late endothelial graft failure (LEGF) at 4-year follow-up (1/15 grafts, 6.7%).
Conclusion: In patients with PIOL-related corneal decompensation, DMEK leads to good and clinically significant refractive and visual outcomes in the medium-long term, with a good safety profile. Prospective studies are encouraged to ascertain whether these cases are at increased risk of accelerated endothelial cell loss and LEGF.
Keywords: descemet membrane endothelial keratoplasty, endothelial keratoplasty, phakic intraocular lens, corneal endothelial failure
Plain Language Summary
- DMEK is safe and effective for corneal decompensation due to phakic IOLs.
- A two-staged approach (phakic IOL explantation, then DMEK) may be preferable.
- DMEK yields good refractive outcomes, relevant in previous refractive surgery cases.
- DMEK in this setting may have an increased endothelial cell loss rate.
Introduction
Despite the excellent long-term efficacy and safety profiles of phakic intraocular lenses (PIOLs) for the correction of moderate-to-high ametropia,1–4 accelerated endothelial cell loss is still the main concern after PIOL implantation,4,5 being the second most frequent indication for PIOL explantation (after cataract development).6–10 Up to 3–4% of patients with PIOL-related corneal decompensation may require corneal allograft transplantation. Although endothelial keratoplasty (EK) techniques have demonstrated to be effective for Fuchs’ endothelial corneal dystrophy (FECD) and pseudophakic bullous keratopathy (PPBK), there is a paucity of data on the outcomes of Descemet’s membrane endothelial keratoplasty (DMEK) and Descemet’s stripping endothelial keratoplasty (DSEK) for novel indications, including PIOL-related corneal decompensation.11–13 Since patients who underwent refractive surgery have higher visual and refractive expectations, endothelial keratoplasty (EK) techniques (particularly DMEK) may offer them better postoperative outcomes compared with penetrating keratoplasty (PKP).
The aim of this study was to analyze the anatomical and functional outcomes of DMEK surgery for PIOL-related corneal decompensation.
Materials and Methods
Study Design and Approval
We conducted a single-center, retrospective, interventional, noncomparative study of all cases of primary DMEK for PIOL-related corneal decompensation. All patients gave informed consent to review their medical records, and patient data confidentiality was guaranteed under the national laws for personal data protection and digital rights guarantee, as well as under the Regulation (EU) 2016/179 of the European Parliament for personal data protection. This study complied with the Declaration of Helsinki and was performed according to ethics committee approval (Comité Ético de Investigación- Instituto de Microcirugía Ocular – CEIm IMO, Spain).
Patients
Between July 2011 and July 2020, sixteen eyes of fourteen patients with PIOL-related corneal decompensation underwent primary DMEK by a single experienced DMEK surgeon (J.L.G.) and had ≥6 months of postoperative follow-up (F-U). All the DMEK cases were performed in our center, but the PIOL patients were from a broad source of referral.
Donor Tissue Protocol
Pre-cut corneal donor tissues for primary DMEK grafts were obtained from the Barcelona Tissue Eye Bank. Corneal tissue donation followed the national regulations for cadaver donors (BOE-A-2012-15715), and this was conducted in accordance with the Declaration of Istanbul. The mean age of the DMEK graft donors was 67.5 (10.7) years, and the mean ECD was 2520.6 (296.1) cells/mm2.
Surgical Technique
The incisions for DMEK, crystalline lens surgery and “foldable” PIOL explantation were the same, standardly located at 120°. In those cases of PMMA PIOL explantation, an independent incision was created at the surgical limbus and centered at 60°; once it was closed, both crystalline lens surgery and DMEK were performed through a standard 120°-centered 2.4-mm main incision.
All DMEK surgeries were performed under local anesthesia. The surgical technique for primary DMEK surgery was as previously described by our group.14,15 Briefly, after central descemetorhexis was performed under air and a surgical inferior peripheral iridectomy was made. The donor graft with a diameter 0.5–1.0 mm smaller than the descemetorhexis diameter was gently injected (using the Güell DMEK 2.2 injector, DK220; Medical, Thal, Switzerland), unfolded using indirect corneal manipulation, and 20% sulphur hexafluoride (SF6) was used as ocular endotamponade to ensure graft apposition onto the recipient’s posterior stroma. Subconjunctival methylprednisolone was administered at the end of the procedure.
Postoperative Protocol
The postoperative protocol was as our standard, including postoperative positioning regimens to ensure graft attachment,14 and immune rejection prophylaxis protocol, consisting of a) topical dexamethasone 0.1% every 2 hours for one day, 6 times daily for one week, then 4 times daily for 4 weeks and then tapered over 3 months and then maintained once daily (with careful monitoring of the intraocular pressure (IOP)); b) dexamethasone 0.05% ointment at night-time for 6 months and then stopped in the absence of inflammatory signs or symptoms; c) oral methylprednisolone slowly tapered off for the first 3 weeks (40 mg/day for 3 days; 20 mg/day for 3 more days; 10 mg/day for 1 week; and 10 mg every 48h for 1 week); and d) topical timolol 0.5% every 12 hours for twelve weeks, with additional IOP-lowering drugs if needed.
Data Collection
We analyzed demographic data (age, gender), time between PIOL implantation and explantation, the BCVA and refractive error (refractive spherical equivalent (RSE), in diopters) before PIOL explantation (± RLE) and before DMEK surgery, and the patients’ ECC and corneal pachymetry prior to DMEK. In cases where history was available, we also collected the data regarding the patient’s status prior to PIOL implantation surgery, including history of amblyopia or pathologic myopia, pre-PIOL BCVA, pre-PIOL RSE, PIOL type and spherical power.
We analyzed the post-DMEK BCVA at months 1 (M1), 3 (M3), 6 (M6), and at the last F-U observation; in cases with ≥1 or ≥2 years of F-U, these time-points were also analyzed.
Main Outcome Measures
The main outcome was improvement in BCVA at the last F-U observation compared with BCVA before DMEK (baseline).
Secondary Outcomes
Other outcomes analyzed were a) the proportion (%) of eyes reaching final BCVA ≤ 0.30 logMAR (≥20/40 Snellen), BCVA ≤ 0.10 logMAR (≥20/25 Snellen) and BCVA ≤ 0.00 logMAR (≥20/20 Snellen); b) change in RSE at final observation compared with pre-DMEK RSE; c) endothelial cell loss (%ECL); d) re-bubbling rate; e) immune rejection rate; f) primary and secondary graft failure rates; g) change in corneal pachymetry at last F-U compared with pre-DMEK; and h) postoperative complications after DMEK, including IOP spikes, ocular hypertension (OHT) or glaucoma, IOL opacification or cataractogenesis, and cystoid macular oedema (CMO).
Statistical Analysis
SPSS software (v 23.0; IBM Corp, Chicago, Illinois, USA) was used for the statistical analysis. Quantitative variables were described as mean (standard deviation) if they had a normal distribution, and parametric tests were applied in such case; quantitative variables without a normal distribution were described as median (P25-P75), and nonparametric tests were applied. Categorical variables were described in absolute and relative frequencies, and chi-square or Fisher exact tests were applied for comparison between categorical variables. The significance level α was 0.05.
Results
Baseline Data
Table 1 depicts the demographic and baseline data. Mean patient age was 49.2 (14.3) years. Four eyes (25%) had amblyopia, and three eyes (18.8%) had pathological myopia at the time of PIOL implantation. Five eyes (31.3%) had angle-supported PIOLs (AS-PIOL) implanted (Figure 1), two eyes (12.5%) had posterior-chamber collamer PIOLs (PC-PIOL), and the remaining nine eyes (56.2%) had anterior chamber (AC), iris-claw PIOLs (IC-PIOL); mean PIOL spherical power was- 10.20 ± 12.28 D. Two eyes (one patient) had an AC IC-PIOL implanted elsewhere (Worst phakic IOL) and was referred to us for corneal decompensation fourteen years after phakic IOL implantation. Visual acuity data prior to PIOL implantation were only available in four eyes, with a mean BCVA of 0.41 ± 0.28 logMAR. Mean time to PIOL explantation was 9.3 ± 5.0 years, with a mean BCVA prior to PIOL explantation of 0.45 ± 0.35 logMAR. The median time between PIOL (± RLE) and primary DMEK was 3 (2–4) months (range 1–28 months); staged DMEK (DMEK performed within 4 months of the PIOL explantation) was performed in twelve eyes (75%). Median BCVA prior to DMEK surgery (baseline BCVA) was 0.80 (1.08–0.60) logMAR, with a median RSE of −0.88 (−2.56 – +0.06) D.
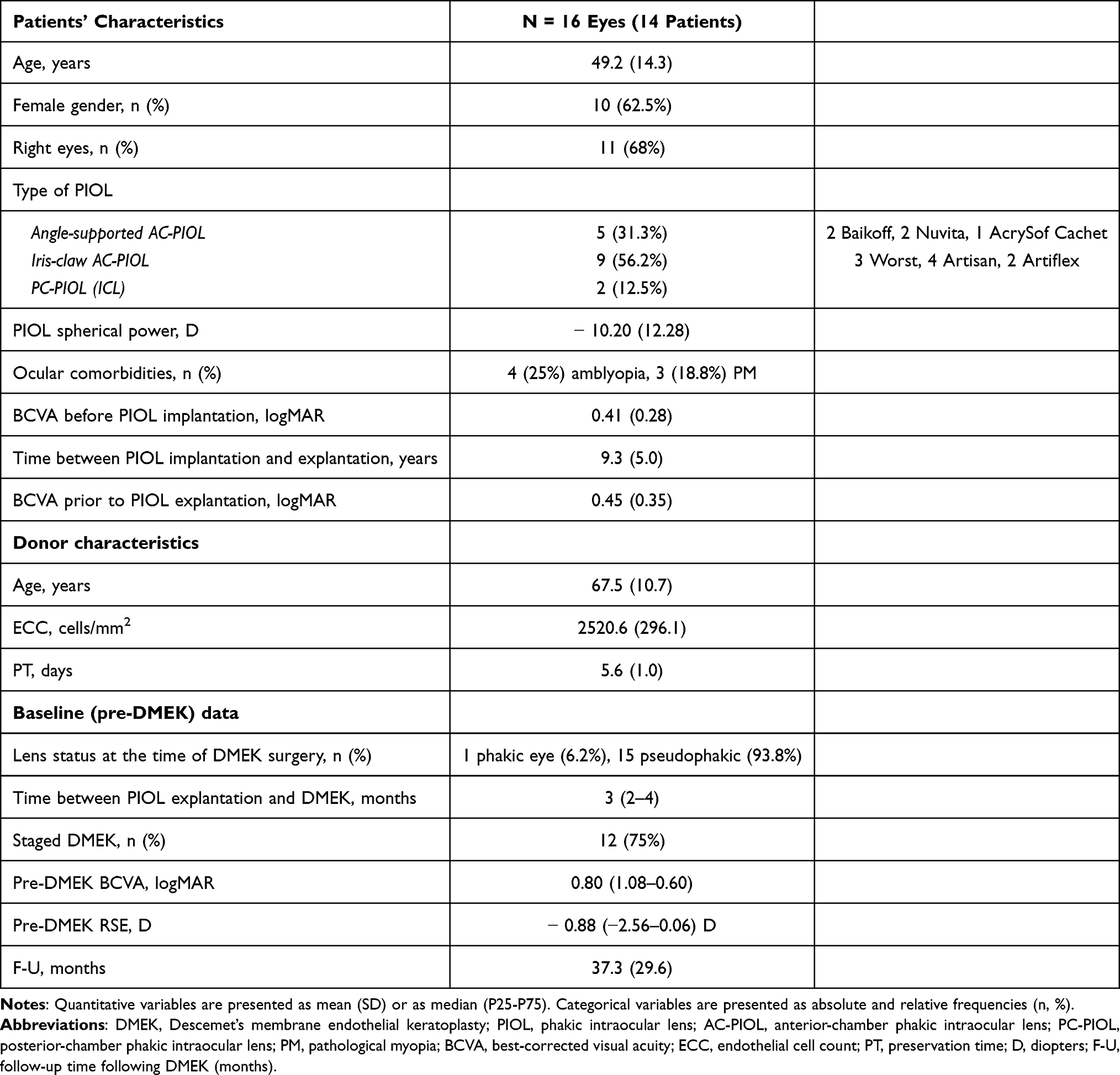 |
Table 1 Patients’ Demographics, Preoperative Characteristics, and Cornea Donor Data |
 |
Figure 1 Anterior segment photograph of a patient who underwent DMEK for PIOL-related corneal decompensation. (A) Corneal decompensation in an eye with an angle-support, phakic intraocular lens (BCVA = 20/40 Snellen). (B) 8 years after staged surgery (PIOL explantation plus RLE, followed by DMEK), showing a clear cornea (BCVA = 20/20 Snellen). |
Twelve eyes (75%) underwent staged DMEK (DMEK performed within ≤4 months of the PIOL explantation ± refractive lens exchange (RLE), and the median time between PIOL (± RLE) and primary DMEK was 3 (2–4) months (range 1–28 months). Fifteen eyes (93.8%) underwent RLE at the time of PIOL explantation. In all cases where RLE was performed, presence of posterior vitreous detachment and absence of peripheral retinal lesions that required prophylactic treatment was confirmed before the RLE surgery; one eye (6.2%) remained phakic at the time of the DMEK surgery because PVD was not present. When RLE was performed, IOL determination was based on optical biometry using the IOL Master 500 (until 2016) or the IOL Master 700 (since 2016), and the Haigis formula was adopted in most cases, targeting a residual spherical error between −0.75 and −1.25D.16
Primary Outcome - Visual Acuity
One eye (6.2%) had primary graft failure following DMEK (PGF) and was excluded from the BCVA analysis. In eyes without PGF (n = 15), mean F-U time was 37.3 ± 29.6 months (range 6–96 months); three eyes (20%) had <12-month postoperative F-U. As a group, median BCVA at last F-U observation was 0.15 (0.00–0.35) logMAR (20/23 Snellen equivalent), which was statistically significantly better compared with baseline BCVA (p-value = 0.002), as well as compared with BCVA before PIOL explantation (p = 0.004). In eyes without ocular comorbidities limiting visual potential, median final BCVA was 0.10 (0.00–0.23) logMAR (p = 0.017).
A statistically significant improvement in BCVA from baseline was observed as early as in the first postoperative month (median BCVA at M1 = 0.42 (0.50–0.20) logMAR; p = 0.001) and again at M3 post-DMEK (median BCVA at M3 = 0.25 (0.30–0.10 logMAR); p = 0.039) and remained stable for the two first postoperative years (Figure 2). Nine eyes (n = 9) had >2-year follow-up after DMEK, the final median BCVA was 0.10 (0.15–0.00) logMAR at 52.9 (28.3) months (not displayed in Figure 2). Three eyes (n = 3) had more than 5 years of F-U, with a final BCVA of 0.25 logMAR (20/25 Snellen) in one eye and 0 logMAR (20/20 Snellen) in the other two eyes.
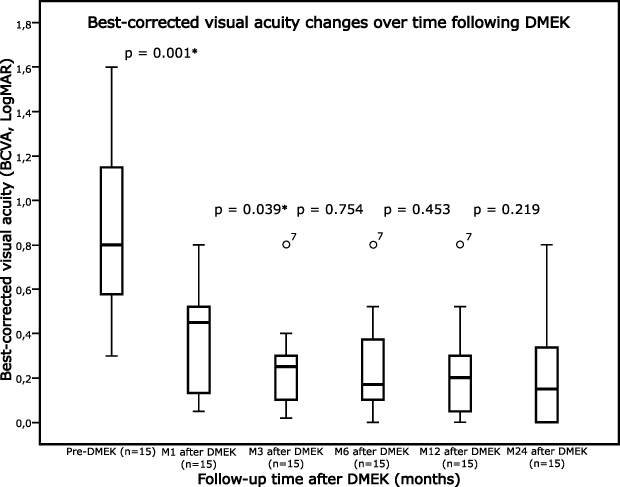 |
Figure 2 Box-plot charts showing the evolution in BCVA following Descemet’s membrane endothelial keratoplasty over a 24-month follow-up period. Statistically significant improvements in mean/median BCVA were observed at postoperative M1 (p = 0.001) compared with baseline pre-DMEK, and again at M3 compared with M1 (p = 0.039). Median BCVA remained stable thereafter during the 2-year follow-up. *P-value < 0.05. |
The proportion of eyes reaching final BCVA ≤ 0.30 logMAR (≥20/40 Snellen), BCVA ≤ 0.10 logMAR (≥20/25 Snellen) and ≤0.00 logMAR (≥20/20 Snellen) were 73.3%, 40%, and 26.7%, respectively; after excluding eyes with ocular comorbidities limiting visual potential, these proportions increased to 87.5%, 62.5%, and 37.5%, respectively.
The median final RSE after DMEK was −0.50 (−1.25–0.00) D. One eye remained phakic after DMEK and had a final refraction of −14.25 DS −1.50 DC (160°), and one eye underwent photorefractive keratectomy (PRK) 2 years after DMEK and reached plano refraction.17 Excluding these two cases, 8 eyes (62%) had a final RSE within ± 0.50 D of emmetropia, and 10 eyes (77%) had a final RSE within ± 1.00 D of emmetropia.
Endothelial Cell Count and Corneal Thickness
Corneal thickness after DMEK decreased from 651.1 ± 66.0 µm to 492.1 ± 37.0 µm. Mean ECC at 2-year F-U was 1042.6 ± 418.0 cells/mm2), with a mean %ECL of 55.6 ± 18.7%. In eyes with >2 years of follow-up (n = 9), after excluding one eye which had late endothelial graft failure (LEGF) at 4-year follow-up, mean total %ECL was 61.7 ± 11.7% (range = 47–77%). Two eyes (n = 2) had 8 years of follow-up, with a mean %ECL of 69.8 ± 1.2% (Table 2).
 |
Table 2 Efficacy and Safety of Descemet Membrane Endothelial Keratoplasty for Phakic Intraocular Lens-Related Corneal Decompensation |
Postoperative Complications
Two eyes (12.5%) developed graft detachment requiring re-bubbling, one of which ended in PGF. We observed no cases of immune rejection episodes.
One eye (6.2%) developed CMO 3 months after DMEK, with a BCVA of 0.40 logMAR (20/50 Snellen equivalent), which was resolved at 6-month F-U with intravitreal sustained-released dexamethasone implant injection, maintaining a BCVA of 0.00 logMAR (20/20 Snellen) at 4-year follow-up. Seven pseudophakic patients developed posterior capsular opacification (PCO) during the follow-up. In three eyes, visual acuity at M6 follow-up was hindered by PCO, and these cases had significant improvement in vision following Nd:YAG laser posterior capsulotomy.
DMEK Survival and Graft Failure
In one eye, the cornea (1/16 eyes, 6.2%) failed to clear following DMEK (PGF). This eye had a graft detachment for which rebubbling was performed, although anatomical reattachment was successful, the graft failed and a repeat DMEK was performed.
Of the functioning grafts (n = 15), one eye (1/15 eyes, 6.7%) evolved to LEGF (final ECC = 551 cells/mm2, representing a 73.8% endothelial cell loss), diagnosed at 4-year F-U. This eye also developed OHT following DMEK, which may have been an important contributing factor to increased %ECL and to graft failure. Graft survival rates at 1-year and at 2-year follow-up after DMEK were 93.8%. Five eyes had F-U ≥4 years, with 4 out of those 5 eyes (80%) having clear corneas at 4-year follow-up. Survival rates throughout the follow-up are shown in Figure 3.
 |
Figure 3 Survival rates after Descemet’s membrane endothelial keratoplasty (DMEK) performed for phakic intraocular lens-related corneal decompensation. Abbreviations: PGF, primary graft failure; LEGF, late endothelial graft failure. |
Discussion
Although there is an increase in the endothelial cell (EC) loss rate after PIOL implantation,3,5 the published rates of PIOL explantation due to accelerated EC loss and corneal decompensation are highly variable, ranging from 0% to 32%.6–9 Phakic IOL explantation for this indication usually occurs over the long term, with reported average times to explantation ranging between 7 and 13.8 years after implantation.6–9 Although we did not observe cases of intraoperative complications during phakic IOL explantation, this surgery is not without risks and may be technically challenging, and especially in the case of angle supported PIOLs (but also in the cases of iris claw-PIOLs and, to a lesser degree, with PC-PIOLs), the risk of intraoperative hemorrhage and iris damage is not negligible and may even adversely affect the outcomes of subsequent DMEK surgery.
In our study, DMEK proved feasible in the setting of PIOL-related corneal decompensation, in line with previous reports.11,12 Although some authors have advocated simultaneous PIOL explantation and EK,13 we consider that a staged approach is preferable in this setting for two main reasons: 1) the risk of intraoperative bleeding during explantation which would complicate DMEK surgery; and 2) in less severe cases we believe that if the PIOL explantation (± RLE) procedure is uneventful, some patients may retain sufficiently acceptable BCVA to delay or prevent DMEK surgery. In the study of López et al,12 only one case underwent quadruple procedure (simultaneous PIOL explantation + cataract surgery + DMEK), and it ended in PGF, which supports our notion that a two-staged approach may be preferable. Highly myopic eyes with very deep AC may pose surgical challenges for DMEK surgery. However, collapsing the AC in these myopic eyes can be relatively simple (unlike the challenges with deep AC of aphakic eyes or vitrectomized eyes) by carefully removing small volumes of aqueous humor from the AC via the main incision, and thus unscrolling the DMEK graft in these eyes is feasible by DMEK surgeons who have completed the learning curve of DMEK surgery.
In our study, clinical and statistically significant changes in BCVA occurred as early as 1 month following DMEK, and stability was observed in the medium term. Our findings are similar to those of Fernandez López et al and Liarakos et al.11,12 Importantly, we also found that BCVA did not significantly deteriorate after multiple surgeries, which is a possible risk owing to factors such as limbal stem cell deficiency, low-grade chronic inflammation, and postoperative complications such as OHT, glaucoma or posterior segment complications. Of note, if eyes with ocular comorbidities limiting visual potential were excluded, we found a high proportion of eyes reaching higher levels of BCVA (≥20/25 and ≥20/20 Snellen), comparable with previous reports of DMEK for other indications.18–22 Although eyes with PIOL-related corneal decompensation are often considered complicated eyes for DMEK grafting, we have found that DMEK is feasible and resulted in superior visual outcomes compared with DSEK for this indication.11,23,24
We have achieved a high proportion of eyes with good refractive outcomes (RSE within 0.50 and within 1.00 D of target refraction). In the setting of PIOL-related corneal decompensation requiring DMEK, the decision to perform RLE is not always straightforward: 1) these patients are usually relatively younger than those undergoing DMEK for other indications, 2) the risk of long-term complications following crystalline lens surgery may be increased, as these eyes are usually highly myopic, 3) corneal transparency may pose a surgical challenge for crystalline lens removal, and 4) IOL power determination may be challenging due the corneal decompensation. However, myopic patients tend to have cataract onset at an earlier age. Besides, cataractogenesis or cataract progression is to be expected following DMEK, and later cataract surgery may put DMEK grafts at risk of EC loss and graft failure. In addition, if RLE is not performed, these patients may be at risk of significant anisometropia and aniseikonia if the fellow eye is left with a PIOL. Finally, these are patients who underwent refractive surgery and who have a higher expectation of spectacle independence. Importantly, in patients in which RLE is considered, the refractive target should be shifted by −0.75 to −1.25 D to compensate the expected hyperopic shift induced by corneal deturgescence.16,25,26
We observed a mean %ECL of 55% at 2 years, and of 61% in eyes with medium-long term follow-up times (range 2.5–8 years). Our EC loss rates were considerably lower than those of a previous study.12 However, our 2-year EC loss was somewhat higher than the reported average of 48%±16% (although within this range) of a recently published model of EC loss following DMEK.27 Besides, these rates appear to be higher compared with our own results for DMEK for other indications,15,19 as well as with medium-term DMEK studies, where reported %ECL 4 to 5 years after DMEK ranged between 48% and 59%.20–22,28 Finally, in the two eyes with 8-year follow-up, we observed an average EC loss rate comparable to that reported 10 years after DMEK.22 Taken altogether, these findings suggest that these eyes may be at risk of accelerated EC loss following DMEK. This has also been reported in one study which reported a 42–47% EC loss rate at 6-month follow-up,11 and in another study where the authors observed an average of 77% EC loss one year after DMEK.12 Potential factors contributing to increased EC loss in this setting may include iris changes and chronic low-grade subclinical AC inflammation. We additionally postulate that the presence of PIOL induces a significant EC loss also at the periphery of the corneal endothelial layer, which probably relates with the observation of higher EC loss; this may be the case especially in angle-supported PIOLs, or possibly with PC-PIOL with a narrow angle or a large vault. Increased EC loss may pose these eyes at increased risk of LEGF over the medium-to-long term. We have found an 80% graft survival rate in eyes with ≥4-year follow-up (4 out of 5 eyes with 48-month follow-up), which is lower in comparison with reported 83–96% graft survival rates at 5–7 years for other indications.20–22,28
Although this study has a relatively small cohort size, this is the largest study reporting outcomes of DMEK for PIOL-related corneal decompensation to date, with a mean 3-year follow-up period which allows us to draw important conclusions regarding visual outcomes and complications after DMEK. In addition, it provides relevant insight into the refractive aspects of DMEK surgery, reinforcing the notion that DMEK may be ideal in managing corneal decompensation in refractive patients.29 Although in our study one eye underwent PRK after DMEK with excellent outcomes, keratorefractive surgery in DMEK eyes must be decided with great caution, since corneal deturgence after DMEK may be associated with a thinner-than-normal central cornea, steeper pachymetric progression from the thinnest point to the periphery, and higher posterior elevation values.17
In conclusion, DMEK is surgically feasible in eyes with PIOL-associated corneal decompensation, resulting in early, clinically significant visual improvement, and with a high proportion of eyes reaching high levels of BCVA and very good refractive outcomes. However, these eyes may have an increased rate of EC loss following DMEK and thus a higher risk of LEGF. We consider that larger, prospective studies are needed to ascertain two main aspects: 1) whether PIOL-related corneal decompensation is associated with inferior outcomes compared with DMEK performed for other indications such as Fuchs’ dystrophy and 2) to determine whether a two-staged approach has a superior efficacy and safety profile compared with simultaneous PIOL-explantation and crystalline lens surgery.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
No funding was received for this study.
Disclosure
Dr. Güell has been a consultant for Alcon, Ophtec, Meditec Zeiss, Kowa Co Ltd, Théa Laboratories, RxSight, and Calhoun Vision. Dr. Moura-Coelho, Dr. Cunha, Dr. Dias-Santos, Dr. Dutra-Medeiros, Dr. Papa-Vettorazzi, and Dr. Manero have no conflicts of interest in this work.
References
1. Papa-Vettorazzi MR, Moura-Coelho N, Manero F, Cruz-Rodriguez JB, Elies D, Güell JL. Long-term efficacy and safety profiles of iris-fixated foldable anterior chamber phakic intraocular lens implantation in eyes with more than 10 years of follow-up. J Cataract Refract Surg. 2022;48(9):987–992. doi:10.1097/j.jcrs.0000000000000937
2. Papa-Vettorazzi MR, Güell JL, Cruz-Rodriguez JB, Moura-Coelho N, Elies D. Long-term efficacy and safety profiles after posterior chamber phakic intraocular lens implantation in eyes with more than 10 years of follow-up. J Cataract Refract Surg. 2022;48(7):813–818. doi:10.1097/j.jcrs.0000000000000848
3. Monteiro T, Correia FF, Franqueira N, Mendes JC, Pinto C, Vaz F. Long-term efficacy and safety results after iris-fixated foldable phakic intraocular lens for myopia and astigmatism: 6-year follow-up. J Cataract Refract Surg. 2021;47(2):211–220. doi:10.1097/j.jcrs.0000000000000419
4. Kohnen T, Kook D, Morral M, Güell JL. Phakic intraocular lenses: part 2: results and complications. J Cataract Refract Surg. 2010;36:2168–2194. doi:10.1016/j.jcrs.2010.10.007
5. Packer KT, Vlasov A, Greenburg DL, et al. U.S. military implantable collamer lens surgical outcomes: 11-year retrospective review. J Cataract Refract Surg. 2022;48(6):649–656. doi:10.1097/j.jcrs.0000000000000818
6. Alió JL, Toffaha BT, Peña-Garcia P, Sádaba LM, Barraquer RI. Phakic intraocular lens explantation: causes in 240 cases. J Refract Surg. 2015;31(1):30–35. doi:10.3928/1081597X-20141202-01
7. Jonker SMR, van Averbeke AAC, Berendschot TTJM, Saelens IEY, Nuijts RMMA. Risk factors for explantation of iris-fixated phakic intraocular lenses. J Cataract Refract Surg. 2019;45(8):1092–1098. doi:10.1016/j.jcrs.2019.03.009
8. Duignan ES, Quigley C, Treacy MP, Aldouri A, O’Keefe M. Iris-fixated phakic intraocular lens explantation. Eur J Ophthalmol. 2021;31(3):988–993. doi:10.1177/1120672120934985
9. Yildirim TM, Khoramnia R, Son HS, et al. Reasons for explantation of phakic intraocular lenses and associated perioperative complications: cross-sectional explant registry analysis. BMC Ophthalmol. 2021;21(1). doi:10.1186/s12886-021-01847-0
10. Moshirfar M, Imbornoni LM, Ostler EM, Muthappan V. Incidence rate and occurrence of visually significant cataract formation and corneal decompensation after implantation of verisyse/artisan phakic intraocular lens. Clin Ophthalmol. 2014;8:711–716. doi:10.2147/OPTH.S59878
11. Liarakos VS, Ham L, Dapena I, et al. Endothelial keratoplasty for bullous keratopathy in eyes with an anterior chamber intraocular lens. J Cataract Refract Surg. 2013;39(12):1835–1845. doi:10.1016/j.jcrs.2013.05.045
12. López EF, Martínez CP. Descemet membrane endothelial keratoplasty for corneal decompensation secondary to phakic intraocular lenses. J Ophthalmol. 2019;2019. doi:10.1155/2019/2038232
13. Nahum Y, Busin M. Quadruple procedure for visual rehabilitation of endothelial decompensation following phakic intraocular lens implantation. Am J Ophthalmol. 2014;158(6):1330–1334.e1. doi:10.1016/j.ajo.2014.09.002
14. Güell JL, Morral M, Gris O, Elies D, Manero F. Bimanual technique for insertion and positioning of endothelium-descemet membrane graft in descemet membrane endothelial keratoplasty. Cornea. 2013;32(12):1521–1526. doi:10.1097/ICO.0b013e3182933aee
15. Güell JL, Morral M, Gris O, Elies D, Manero F. Comparison of sulfur hexafluoride 20% versus air tamponade in descemet membrane endothelial keratoplasty. Ophthalmology. 2015;122(9):1757–1764. doi:10.1016/j.ophtha.2015.05.013
16. Moura-Coelho N, Güell JL. Refractive accuracy after cataract surgery and descemet membrane endothelial keratoplasty. Cataract Refract Surg Today Europe. 2022;17(8):12–14.
17. Moura-Coelho N, Manero F, Papa-Vettorazzi M, Amich N, Cunha J, Güell J. Photorefractive keratectomy after DMEK for corneal decompensation by phakic IOL. Eur J Ophthalmol. 2022;112067212110734. doi:10.1177/11206721211073429
18. Deng SX, Lee WB, Hammersmith KM, et al. Descemet membrane endothelial keratoplasty: safety and outcomes: a report by the American Academy of Ophthalmology. Ophthalmology. 2018;125(2):295–310. doi:10.1016/j.ophtha.2017.08.015
19. Moura-Coelho N, Manero F, Elies D, et al. Repeat descemet membrane endothelial keratoplasty for failed primary descemet membrane endothelial keratoplasty at a referral center for keratoplasty in Spain: DIMOEK study. Am J Ophthalmol. 2020;215:49–55. doi:10.1016/j.ajo.2020.03.015
20. Ham L, Dapena I, Liarakos VS, et al. Midterm results of descemet membrane endothelial keratoplasty: 4 to 7 years clinical outcome. Am J Ophthalmol. 2016;171:113–121. doi:10.1016/j.ajo.2016.08.038
21. Birbal RS, Dhubhghaill SN, Bourgonje VJ, et al. Five-year graft survival and clinical outcomes of 500 consecutive cases after descemet membrane endothelial keratoplasty. Cornea. 2020;39(3):290–297. doi:10.1097/ICO.0000000000002120
22. Vasiliauskaitė I, Oellerich S, Ham L, et al. Descemet membrane endothelial keratoplasty: ten-year graft survival and clinical outcomes. Am J Ophthalmol. 2020;217:114–120. doi:10.1016/j.ajo.2020.04.005
23. Hipólito-Fernandes D, Elisa-Luís M, Vieira M, et al. Long-term results of descemet-stripping automated endothelial keratoplasty for endothelial failure caused by phakic intraocular lenses. Eur J Ophthalmol. 2021;31(4):1688–1694. doi:10.1177/1120672120950936
24. Sikder S, Patel V, Holz HA, Mifflin MD, Davis S, Moshirfar M. Management of corneal endothelial decompensation caused by iris-fixated phakic intraocular lenses with descemet stripping automated endothelial keratoplasty. Cornea. 2011;30(9):1045–1047. doi:10.1097/ICO.0b013e3182035dd0
25. Ham L, Dapena I, Moutsouris K, et al. Refractive change and stability after descemet membrane endothelial keratoplasty: effect of corneal dehydration-induced hyperopic shift on intraocular lens power calculation. J Cataract Refract Surg. 2011;37(8):1455–1464. doi:10.1016/j.jcrs.2011.02.033
26. Schoenberg ED, Price FW, Miller J, McKee Y, Price MO. Refractive outcomes of descemet membrane endothelial keratoplasty triple procedures (combined with cataract surgery). J Cataract Refract Surg. 2015;41(6):1182–1189. doi:10.1016/j.jcrs.2014.09.042
27. Fajgenbaum MAP, Kopsachilis N, Hollick EJ. Descemet’s membrane endothelial keratoplasty: surgical outcomes and endothelial cell count modelling from a UK center. Eye. 2018;32(10):1629–1635.
28. Price DA, Kelley M, Price FW, Price MO. Five-year graft survival of descemet membrane Endothelial Keratoplasty (EK) versus descemet stripping EK and the effect of donor sex matching. Ophthalmology. 2018;125(10):1508–1514. doi:10.1016/j.ophtha.2018.03.050
29. Tong CM, Baydoun L, Melles GRJ. Descemet membrane endothelial keratoplasty and refractive surgery. Curr Opin Ophthalmol. 2017;28:316–325. doi:10.1097/ICU.0000000000000380
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.