Back to Journals » Clinical, Cosmetic and Investigational Dermatology » Volume 15
Dermatology Patients’ Knowledge of Sunscreen Guidelines at a University Hospital in Saudi Arabia
Authors Al-Balbeesi A ![]() , AlMukhadeb E
, AlMukhadeb E ![]() , BinMayouf M
, BinMayouf M ![]() , AlNasser S
, AlNasser S ![]() , Aldossari A
, Aldossari A ![]() , Alfaiz F
, Alfaiz F ![]() , Alyamani A
, Alyamani A ![]() , Alammari A, Almuhaideb Q
, Alammari A, Almuhaideb Q ![]()
Received 20 October 2022
Accepted for publication 14 December 2022
Published 29 December 2022 Volume 2022:15 Pages 2915—2923
DOI https://doi.org/10.2147/CCID.S393455
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Jeffrey Weinberg
Amal Al-Balbeesi,1,2 Eman AlMukhadeb,1,2 Mohammed BinMayouf,2 Sultan AlNasser,2 Abdulelah Aldossari,2 Fahad Alfaiz,2 Abduljabbar Alyamani,2 Ali Alammari,2 Qais Almuhaideb2
1Dermatology Department, King Khalid University Hospital, Riyadh, Kingdom of Saudi Arabia; 2College of Medicine, King Saud University, Riyadh, Kingdom of Saudi Arabia
Correspondence: Mohammed BinMayouf, Email [email protected]
Objective: The goal of this study is to assess the knowledge and attitude of dermatology patients regarding sunscreen use as recommended by the American Academy of Dermatology.
Methods: This was an observational cross-sectional study at a university hospital in Riyadh. Participants were asked to complete a questionnaire to measure their knowledge and attitude regarding sunscreen use. Results were analyzed using a chi-square test.
Results: Most participants heard about sunscreen (93.4%) and had indicated previous sunscreen use (72%). Sunscreen use was higher among women and participants with a postgraduate education. Sunscreen knowledge was higher among women, participants with non-photosensitive disorders, and participants with Fitzpatrick I, II, and III skin types. A total of 80% knew the worst time for sun exposure, but only 20.5% of the participants knew that sunscreen should be applied daily throughout the year, and 13.5% knew the correct minimum recommended SPF. A total of 34% were aware of the minimum time allowed for sunscreen application before sun exposure, and 20% were aware of the longest period allowed between reapplications. Only 4.5% knew the proper amount of sunscreen to cover the entire body.
Conclusion: Our study revealed that most participants had heard of sunscreen, however their knowledge of the guidelines for sunscreen use was poor. Only 33% of the participants had received a recommendation for using sunscreen from their general practitioner or dermatologist. More comprehensive and directed efforts need to be made in counselling and educating these patients on proper sunscreen practice.
Keywords: patient knowledge, dermatology, sunscreen, guidelines
Introduction
Approximately 50% of the Saudi population spends 10 hours or more in the sun per week.1 High amounts of ultraviolet (UV) radiation from excessive sun exposure cause many acute and chronic harmful effects on the skin.2 UV exposure is a recognized modifiable risk factor for squamous cell carcinoma, basal cell carcinoma, melanoma, and other skin malignancies.2–5 The incidence of skin cancer has increased so significantly in the past four decades that it has become one of the most common cancers globally, accounting for 33% of cancer cases worldwide.6 It is believed that 90% of SCCs and BCCs and 67% of melanomas are due to excessive sun exposure.4 The consequences of UVR exposure can be reduced through avoidance. Avoidance can be achieved by practicing sun-protective behaviors, including avoiding sun exposure between 10:00 a.m. and 2:00 p.m., staying in the shade, applying sunscreen agents, avoiding tanning beds, and using sun-protective clothing and garments.7–10
The American Academy of Dermatology (AAD) recommends, at minimum, using SPF-30 sunscreen daily 15 minutes prior to sun exposure. It also recommends covering the entire body with 30 mL of this sunscreen and reapplying it every two hours.11 An SPF of 30 is proposed as individuals tend to under apply sunscreen, reducing the actual SPF obtained from the intended product. A higher suggested SPF helps to compensate for sub-optimal application.
Adequate sunscreen application protects against sunburn, photoaging11 and has been shown to minimize incidences of cutaneous malignancies.12–15 Despite the importance of this practice, improper knowledge and use of sunscreen is common, a finding found in a variety of studies conducted around the world.16–19 Additionally, previous studies have found that the rates of sunscreen use in the Saudi population are much lower than those in Western communities.1 At present, there is a dearth of studies available that assess sunscreen use among dermatology patients. This study’s goal is to assess the knowledge and attitude of dermatology patients regarding sunscreen use, as recommended by the AAD.
Materials and Methods
This observational cross-sectional study included patients from the dermatology clinic at a university hospital in Riyadh, Saudi Arabia. Surveys were distributed from November 15, 2021, to December 6, 2021, to patients in the dermatology clinics’ waiting area. Participants were informed about the purpose of the study and after obtaining consent, all patients were eligible to be included, except for those with a documented sunscreen allergy. The questionnaire was adapted from “Patient Knowledge of Sunscreen Guidelines and Frequency of Physician Counseling: A Cross-Sectional Study” by Vasicek et al.20 The survey’s knowledge questions were based on AAD recommendations.11 The survey included four demographic questions concerning gender, age, education level, and the Fitzpatrick scale (determined by asking the participants about their tendencies to tan or become sunburned). Following these questions were those about the reason for visiting a dermatology clinic, a prior personal or family history of skin cancer, and sunscreen allergies. After these questions, the survey included six questions on knowledge, three questions on attitudes, and one question on the source that recommended sunscreen use. The Institutional Review Board of King Saud University approved and has given permission to conduct this study (Approval No. E-21-6244). This study complies with the Declaration of Helsinki.
Sample Size Calculation
In a nationwide survey of 2900 respondents conducted in Saudi Arabia, where there was a diverse age range (15–70 year old), with a mean age of 27.8 years, equal gender distribution between respondents and the majority having achieved a higher education, sunscreen use was concluded to reach 23.7%.21
Taken into consideration, with a confidence level of 95%, and accepting a difference of up to 5%, we required 277 subjects. The sample size was calculated using the following equation:  .
.
Participants Demographics
Of the 288 participants, 67% were female. Approximately 75.3% of the sample were less than 40 years old, and more than 50% had an undergraduate education. The most prevalent skin types were Fitzpatrick type III (21.9%) and IV (21.4%). A total of 72% of the participants had previously used sunscreen.
Statistical Analysis
Data was analyzed using the statistical package for the social sciences (SPSS), version 25. Categorical variables were presented as numbers and percentages and were compared using a chi-square test. All tests were 2-tailed, and a p-value of <0.05 was considered statistically significant.
Results
The relationship between demographic data and sunscreen use is shown in Table 1. Gender and educational levels were statistically significant, while age and skin type were statistically insignificant. Sunscreen use was higher among women than men (84.5% vs 47.4%, p < 0.001). It was also higher among the participants with a postgraduate education than among those with undergraduate and high school education (91.3% vs 76.4% vs 62%, p = 0.004). Dermatologists advised a total of 26% of participants to use sunscreen, while 22% of participants had not been previously advised by doctors to use sunscreen (Figure 1).
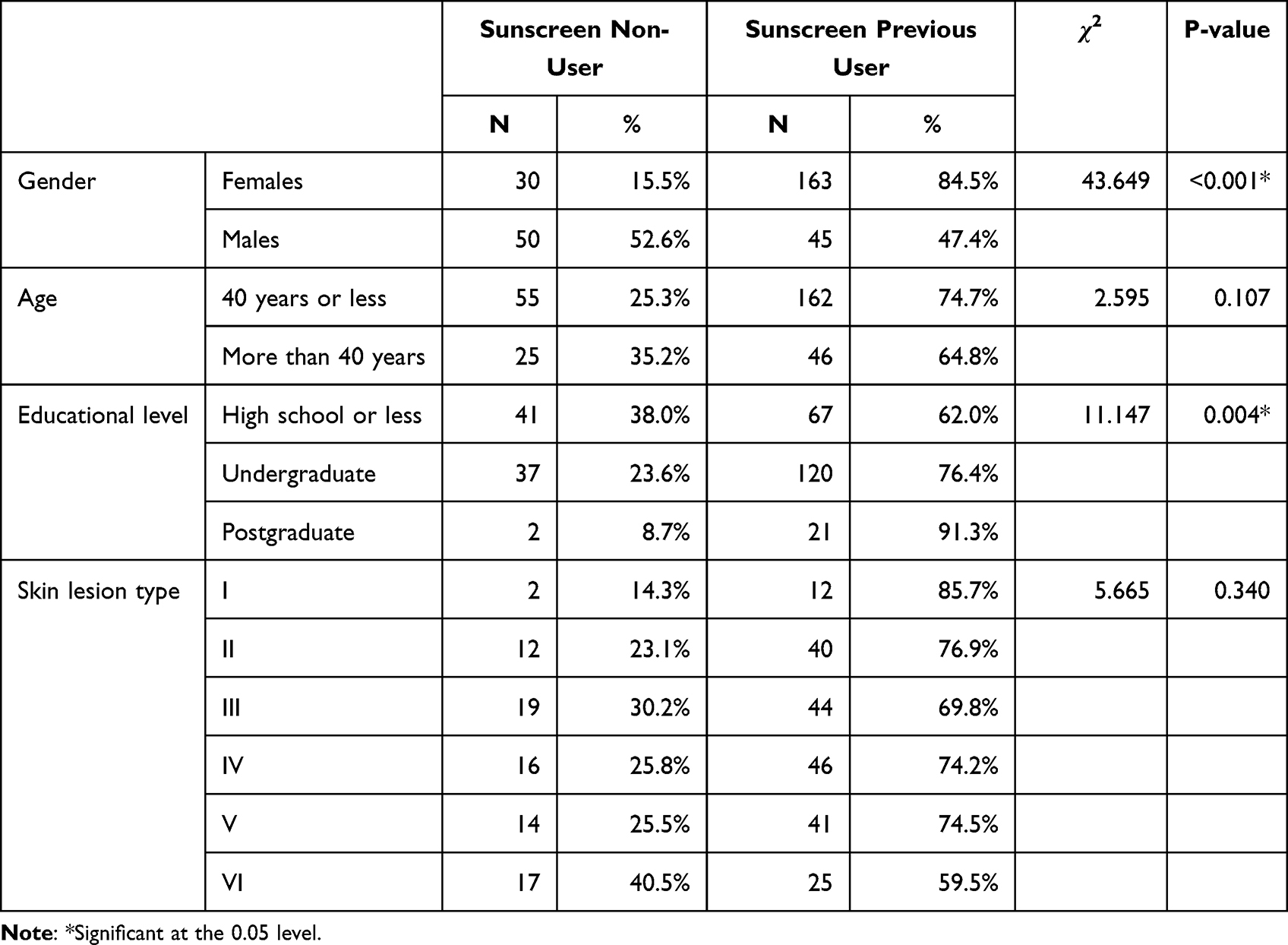 |
Table 1 Demographic Data of Studied Patients with Dermatological Diseases and Their Relation to Sunscreen Use (n = 288) |
 |
Figure 1 Percentage of participants advised by different sources to use sunscreen (n = 288). |
Relationship Between the History of Dermatological Problems and Sunscreen Use
Among the 72% of participants who reported previous use of sunscreen, sunscreen use was higher among those with photosensitive inflammatory disease, with no significant difference between that and other reasons for visiting the hospital, such as pigmentary disorders, non-photosensitive diseases, and photosensitive medications (79% vs 76% vs 72% vs 60%, respectively, p = 0.888). A history of skin cancer and sunscreen allergies was also insignificant. None of the participants had a family history of skin cancer (Table 2).
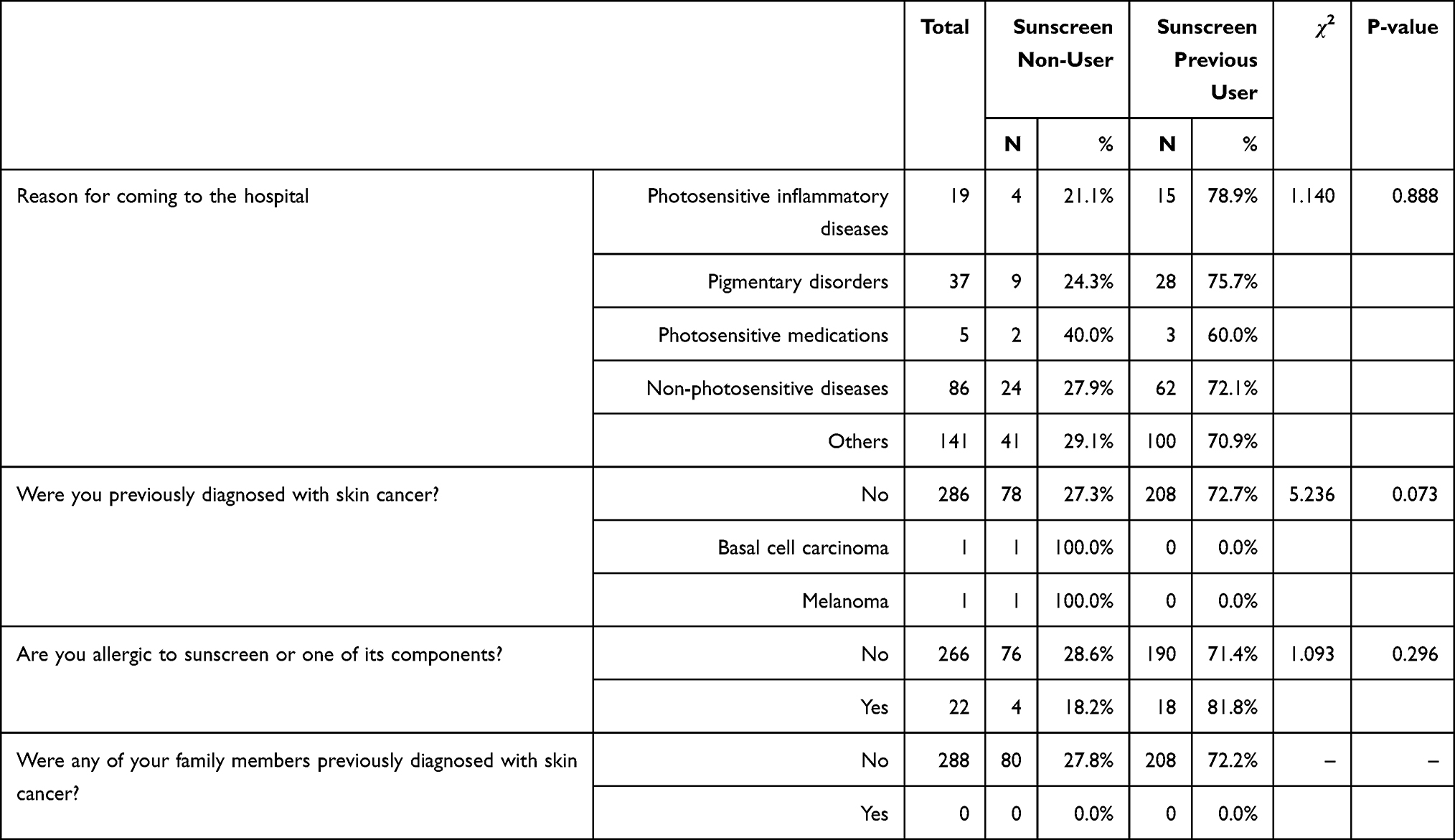 |
Table 2 Relationship Between History of Dermatological Problems and Sunscreen Use Among Study Participants (n = 288) |
Knowledge of Sunscreen
A total of 93.4% of the participants reported a previous knowledge of sunscreen. The participants’ responses to questions assessing their knowledge of proper sunscreen use are shown in Table 3. A total of 20.5% of the participants knew that sunscreen should be applied daily throughout the year, with approximately half (45.5%) choosing “when exposed to sun rays for a long period”. Only 13.5% of the participants knew the minimum recommended SPF (SPF 30), with the majority (58.3%) stating that they did not know. Only 4.5% knew the proper amount of sunscreen needed to cover the whole body (30 mL), with the most (53.8%) stating that they do not know. A total of 34% of the participants knew the minimum time for sunscreen application before sun exposure (15 minutes), while 20% knew the longest recommended period between reapplications (two hours). A total of 80% of the participants knew the worst time to be exposed to the sun (10 a.m.–4 p.m.) (Table 3).
 |
Table 3 Patients’ Knowledge of AAD’s Sunscreen Recommendations |
Relationship Between Knowledge of Proper Sunscreen Use and Other Variables
Women knew more about the optimum frequency of use and time before sun exposure than males, with a significant difference between them (84.7% vs 15.3%, p = 0.001 and 83.7% vs 16.3%, p < 0.001, respectively). The participants with non-photosensitive disorders knew more about the correct time to reapply sunscreen than those with photosensitive inflammatory and pigmentary diseases (34.8% vs 21.7% vs 8.7%, p = 0.030). Knowledge of the correct time to apply sunscreen before sun exposure was higher among those with Fitzpatrick skin types I, II, and III than those with skin types IV, V, and VI (55.1% VS 44.9%, respectively, p = 0.012) (Table 4).
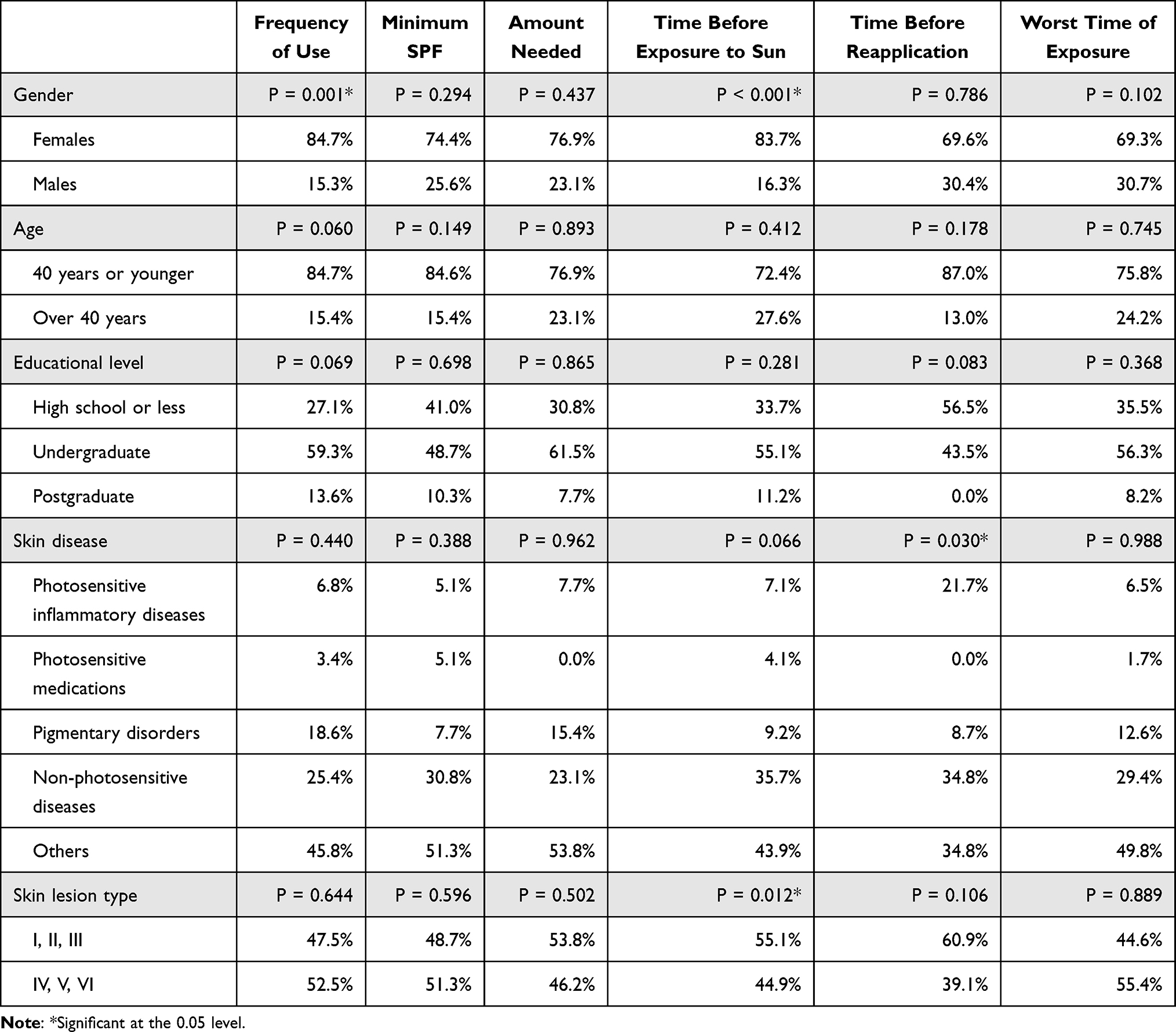 |
Table 4 Relationship Between Knowledge of Proper Sunscreen Use and Other Variables Among Study Participants (n = 288) |
Relationship Between Attitude Toward Sunscreen Use and Skin Type According to Fitzpatrick Classification
There was no significant relationship between the attitude toward sunscreen use and Fitzpatrick skin type, except that the sunscreen’s price impacted the participants’ choice of sunscreen (p = 0.026). Burns were higher among those who noted that the price had impacted their choice (51% vs 48.7%) (Table 5).
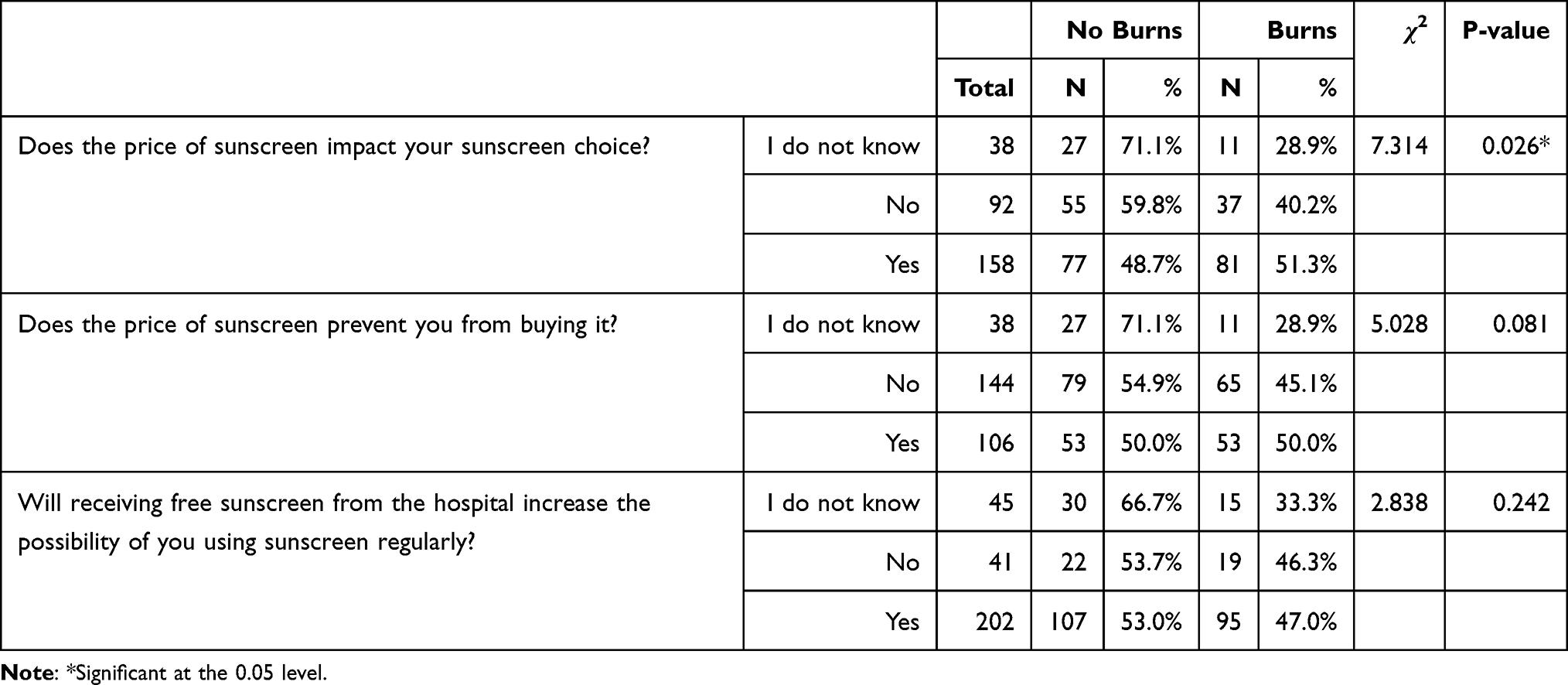 |
Table 5 Relationship Between Attitude Toward Sunscreen Use and Skin According to the Fitzpatrick Classification (n = 288) |
Discussion
Most participants had heard about sunscreen (93.4%) and had noted previous sunscreen use (72%). Previous studies conducted among the general Saudi Arabian population have presented lower results. A national study surveying multiple regions within the Kingdom found that 79% of the population have heard about sunscreen, with 58% reporting previous use and only 23.7%21 using it regularly. However, a study limited to one province in Saudi Arabia (Qassim) reported sunscreen use rates as low as 8.3%.1 An online questionnaire collected from residents of the Kingdom of Saudi Arabia and the Kingdom of Bahrain published similarly low results.22
The participants with skin disorders were expected to take more sun-protective measures, including sunscreen because of their diseases’ nature. They were also expected to have increased opportunities for sun protection counseling, because they visited the dermatology clinic more frequently than the general population. Recommendations from a dermatologist and personal diligence were our sample’s most widely cited reasons for sunscreen use. A study conducted in Lima, Peru, also found high rates of knowledge and use of photo-protectors among dermatology patients, with “78.9% of patients reporting that they knew about photo-protectors (sunscreens) and 52.3% reported that they used photo-protectors regularly”.23
Gender distinction was noted, with more women reporting sunscreen use, a finding that other studies have confirmed1,16,21–24 Traditional gender roles and societal norms greatly influence beliefs that impact sunscreen use. Women are typically the target audience of the skincare industry and are regular consumers of cosmeceutical products. They also place a much higher value on appearance and beauty, resulting in a more positive perception of sunscreen, which leads to higher use rates. Conversely, men regard sunscreen as a feminine concern and thus at odds with their gender role. A study that aimed to identify gender differences in sunscreen usage among young adults further elucidated that, despite similar beliefs about sunscreen use (in preventing sunburns and other health-related adverse effects related to sun exposure), men were found to use sunscreen less and believe it to be inconvenient. Notably, men were only likelier to use sunscreen after suffering from sunburns and when they would be spending many hours in the sun.25
Sunscreen use varied significantly according to educational level. The participants with higher education levels were likelier to have used sunscreen. This finding is supported by several studies in the literature,1,23,26,27 where higher education recipients were found to be more well versed on the detrimental effects of sun exposure and its link to skin cancer. They were also likelier to adopt measures to protect against sun exposure, such as wearing protective clothing and sunglasses and applying sunscreen.
Our study did not find any significant differences in sunscreen use among the participants based on their diagnoses. Equal utilization was seen among the participants, with the highest use rates among those suffering from photosensitive diseases, such as rosacea and cutaneous lupus (79%), and the lowest in those receiving photosensitive medications (60%). Surprisingly, the participants with non-photosensitive disorders were more aware of the correct time to reapply sunscreen than those with photosensitive and pigmentary diseases. Perhaps, regardless of diagnosis, the participants received a basic level of counseling from physicians. However, the counseling was incomplete, as the participants suffering from photosensitive disorders failed to show that they were more knowledgeable about sunscreen guidelines than other participants. Sunscreen use was also insignificantly related to a personal history of skin cancer. Previous studies, though, have shown that melanoma survivors28 and patients with nonmelanoma skin cancers29 were likelier to adopt sun-protective practices, such as sunscreen use, than the general population.
Our findings should be cautiously interpreted, as only two of the 288 participants noted a previous history of skin cancer because skin cancers are not frequently seen among the Saudi population. A systematic review evaluating the epidemiological patterns of skin disease in Saudi Arabia determined that the prevalence of malignant skin neoplasms was 5%.30 It is also noteworthy that most of our sample was relatively young. More than 75% were aged 40 or less. Skin cancer is a disease that is typically found among the elderly, with a mean age of 60 at diagnosis.
Although awareness of and the use of sunscreen were high, most participants displayed a lack of knowledge of the AAD’s guidelines for proper sunscreen use. Less than half of the participants correctly identified when to wear sunscreen, the frequency of application, the minimum recommended SPF level, the required amount to cover one’s body, and how long before sun exposure to apply sunscreen. In contrast, most of the sample correctly identified the worst time for sun exposure, a finding which can be explained by the fact that we live in a hot and sunny climate and our people are quite familiar when the sun’s rays are strongest, and the heat is at its height.
Overall, this lack of knowledge has been found in dermatology patients and the general population in many similar studies,16,17,20 further highlighting this issue.
Although several studies on the general population have established that Fitzpatrick types I, II, and III were associated with increased sunscreen use and more frequent application,24,27 our sample did not display any significant difference among the Fitzpatrick types. Only minor differences in knowledge of correct sunscreen use were noted among the different skin types. A similar study by Vasicek20 had similar results and determined that types I–III were only more knowledgeable about the correct minimum SPF. In our study, Fitzpatrick types I–III were likelier to select 15 minutes as the minimum time allowed for sunscreen to be applied before anticipated sun exposure. Aside from that awareness, the knowledge rates of the guidelines were equal.
Most participants agreed that the pricing of sunscreen impacted their choice of product but did not prevent them from buying products. Interestingly, most patients who agreed that price played a role in their choice had a history of sunburns. Considering this finding and our sample’s high rates of sunscreen usage, it can be concluded that those who sustained sunburns choose more expensive options in the hope that they will receive better protection. Another explanation is that most of our samples found sunscreen prices fair and affordable overall. Even though the price may have influenced their product choices, it did not prevent them from purchasing sunscreen.
Proper instruction on sunscreen use and sun protection is still necessary. The counseling of patients on sun protection and sunscreen use did not appear as comprehensive as it should be. One of the main issues identified in this study was that patients were poorly informed of proper sun protection based on the AAD guidelines. Increased counseling efforts with an emphasis on addressing this issue are critical. While one cannot force patients to adhere strictly to these guidelines, providing them with knowledge is imperative.
Knowledge, though, does not necessarily result in behavioral change, and the responsibility for sunscreen awareness should, therefore, not solely rest on the physician. The adoption of positive behaviors should begin at home at an early age. Significant sun exposure often starts in childhood during the formative years when significant opportunities exist for learning preventative habits and behaviors. Parents should encourage their children to adopt such measures. Schools in which health education is already part of the curriculum can play an integral role in cultivating positive attitudes toward sun protection. Educational campaigns organized by the public sector and involving local media outlets could also help encourage the adoption of sun protective practices.
Limitations
Data was collected from one location only: a university hospital in a metropolitan area. Our study was also conducted on a relatively small sample size. Moreover, most of our sample were female and less than 40 years of age. As a result, the patient sample might not represent all Saudi dermatology patients across the Kingdom. Another limitation is that a dermatologist reported, but did not confirm, skin types, different dermatological conditions, and previous skin cancer diagnoses. Moreover, our sample consisted of self-selected volunteers. Due to the study’s voluntary nature, not all participants agreed to participate in our survey; consequently, our results could be biased. A telephone-based survey was not conducted due the relatively complex structure of the questionnaire as many of the questions include multiple choices. Due to the intrusive nature of telephone-based surveys, fear of mishearing responses and concerns of interviewer and non-response bias, a self-administered survey was deemed most appropriate. Aside from one question assessing whether the participants used sunscreen, the survey did not determine their practices regarding established sunscreen guidelines. Instead, it ascertained their knowledge of sunscreen use. As previously noted, more knowledge does not always lead to better practices.
Conclusion
Our study revealed that most participants had heard of sunscreen, and the majority indicated previous sunscreen use. However, their knowledge of official recommendations for sunscreen use was poor. Every question concerning proper sunscreen use had a correct response rate of less than 50%. Only about 33% of the participants had been recommended to use sunscreen by their general practitioner or dermatologist. Patient’s dermatological condition had little effect on sunscreen use. Further studies comparing sunscreen use among patients with different dermatological conditions must be conducted on a wider scale to further explore this issue. General physicians and dermatologists must provide more comprehensive counseling and education on sunscreen, especially for people with photosensitive skin diseases with due diligence.
Acknowledgments
The authors would like to acknowledge Scribbr.com for their English editing services.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Al Robaee AA. Awareness to sun exposure and use of sunscreen by the general population. Bosn J Basic Med Sci. 2010;10(314–8). doi:10.17305/bjbms.2010.2678
2. Jansen R, Wang SQ, Burnett M, Osterwalder U, Lim HW. Photoprotection: part I. Photoprotection by naturally occurring, physical, and systemic agents. J Am Acad Dermatol. 2013;69:853.e1–12; quiz 865–6. doi:10.1016/j.jaad.2013.08.021
3. NTP. National Toxicology Program (NTP): 15th report on carcinogens.
4. Koh HK, Geller AC, Miller DR, Grossbart TA, Lew RA. Prevention and early detection strategies for melanoma and skin cancer: current status. Arch Dermatol. 1996;132:436–443. doi:10.1001/archderm.1996.03890280098014
5. Coups EJ, Manne SL, Heckman CJ. Multiple skin cancer risk behaviors in the U.S. Population. Am J Prev Med. 2008;34:87–93. doi:10.1016/j.amepre.2007.09.032
6. Rigel DS, editor. Cancer of the Skin. Philadelphia: Elsevier, Saunders; 2005.
7. Berret J, Liardet S, Scaletta C, Panizzon R, Hohlfeld P, Applegate LA. Use of sunscreens in families living in Switzerland. Dermatology. 2002;204:202–208. doi:10.1159/000057882
8. Emmons KM, Colditz GA. Preventing excess sun exposure: it is time for a national policy. J Natl Cancer Inst. 1999;91:1269–1270. doi:10.1093/jnci/91.15.1269
9. Jorgensen CM, Wayman J, Green C, Gelb CA. Using health communications for primary prevention of skin cancer: CDC’s choose your cover campaign. J Womens Health Gend Based Med. 2000;9:471–475. doi:10.1089/15246090050073530
10. Lim HW, Cooper K. The health impact of solar radiation and prevention strategies: report of the environment council, American academy of dermatology. J Am Acad Dermatol. 1999;41:81–99. doi:10.1016/s0190-9622(99)70412-3
11. Sunscreen FAQs. Available from: https://www.aad.org/public/everyday-care/sun-protection/sunscreen-patients/sunscreen-faqs.
12. Ghiasvand R, Weiderpass E, Green AC, Lund E, Veierød MB. Sunscreen use and subsequent melanoma risk: a population-based cohort study. J Clin Oncol. 2016;34:3976–3983. doi:10.1200/JCO.2016.67.5934
13. Olsen CM, Wilson LF, Green AC, et al. Cancers in Australia attributable to exposure to solar ultraviolet radiation and prevented by regular sunscreen use. Aust N Z J Public Health. 2015;39:471–476. doi:10.1111/1753-6405.12470
14. Green A, Williams G, Neale R, et al. Daily sunscreen application and betacarotene supplementation in prevention of basal-cell and squamous-cell carcinomas of the skin: a randomised controlled trial. Lancet. 1999;354(9180):723–729. doi:10.1016/S0140-6736(98)12168-2
15. Green AC, Williams GM, Logan V, Strutton GM. Reduced melanoma after regular sunscreen use: randomized trial follow-up. J Clin Oncol. 2011;29:257–263. doi:10.1200/JCO.2010.28.7078
16. Al-Qarqaz F, Marji M, Bodoor K. Awareness about proper use of sunscreen in people of color: a Jordanian-based survey. J Cosmet Dermatol. 2020;19:1131–1136. doi:10.1111/jocd.13120
17. Görig T, Schneider S, Seuffert S, Greinert R, Diehl K. Does sunscreen use comply with official recommendations? Results of a nationwide survey in Germany. J Eur Acad Dermatol Venereol. 2020;34:1112–1117. doi:10.1111/jdv.16100
18. Petersen B, Datta P, Philipsen PA, Wulf HC. Sunscreen use and failures--on site observations on a sun-holiday. Photochem Photobiol Sci. 2013;12:190–196. doi:10.1039/c2pp25127b
19. Geller AC, Colditz G, Oliveria S, et al. Use of sunscreen, sunburning rates, and tanning bed use among more than 10 000 US children and adolescents. Pediatrics. 2002;109:1009–1014. doi:10.1542/peds.109.6.1009
20. Vasicek BE, Szpunar SM, Manz-Dulac LA. Patient knowledge of sunscreen guidelines and frequency of physician counseling: a cross-sectional study. J Clin Aesthetic Dermatol. 2018;11:35–40.
21. AlGhamdi KM, AlAklabi AS, AlQahtani AZ. Knowledge, attitudes and practices of the general public toward sun exposure and protection: a national survey in Saudi Arabia. Saudi Pharm J. 2016;24:652–657. doi:10.1016/j.jsps.2015.04.002
22. Sultana N. Sun awareness and sun protection practices. Clin Cosmet Investig Dermatol. 2020;13:717–730. doi:10.2147/CCID.S265477
23. Thomas-Gavelan E, Sáenz-Anduaga E, Ramos W, Sánchez-Saldaña L. Knowledge, attitudes and practices about sun exposure and photoprotection in outpatients attending dermatology clinics at four hospitals in Lima, Peru. An Bras Dermatol. 2011;86:1122–1128. doi:10.1590/s0365-05962011000600009
24. Yan S, Xu F, Yang C, et al. Demographic differences in sun protection beliefs and behavior: a community-based study in Shanghai, China. Int J Environ Res Public Health. 2015;12:3232–3245. doi:10.3390/ijerph120303232
25. Abroms L, Jorgensen CM, Southwell BG, Geller AC, Emmons KM. Gender differences in young adults’ beliefs about sunscreen use. Health Educ Behav. 2003;30:29–43. doi:10.1177/1090198102239257
26. Falk M, Anderson CD. Influence of age, gender, educational level and self-estimation of skin type on sun exposure habits and readiness to increase sun protection. Cancer Epidemiol. 2013;37:127–132. doi:10.1016/j.canep.2012.12.006
27. Ermertcan AT, Oztürkcan S, Dinç G, Yurtman D, Pala T, Sahin MT. Sunscreen use and sun protection practices in students and personnel of Celal Bayar University. Photodermatol Photoimmunol Photomed. 2005;21:191–197. doi:10.1111/j.1600-0781.2005.00158.x
28. Mujumdar UJ, Hay JL, Monroe-Hinds YC, et al. Sun protection and skin self-examination in melanoma survivors. Psychooncology. 2009;18:1106–1115. doi:10.1002/pon.1510
29. Fischer AH, Wang TS, Yenokyan G, Kang S, Chien AL. Sunburn and sun-protective behaviors among adults with and without previous nonmelanoma skin cancer (NMSC): a population-based study. J Am Acad Dermatol. 2016;75:371–379.e5. doi:10.1016/j.jaad.2016.02.1236
30. Almohideb M. Epidemiological patterns of skin disease in Saudi Arabia: a systematic review and meta-analysis. Dermatol Res Pract. 2020;2020:5281957. doi:10.1155/2020/5281957
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.