Back to Journals » Clinical, Cosmetic and Investigational Dermatology » Volume 16
Dermatologists Should Encourage and Resume Photoprotection in Patients with Photodermatoses and Melasma Following the COVID-19 Pandemic
Authors Chaisuwannarak K, Rujitharanawong C, Chaiyabutr C, Wongpraprarut C ![]() , Silpa-archa N
, Silpa-archa N
Received 18 August 2023
Accepted for publication 7 October 2023
Published 18 October 2023 Volume 2023:16 Pages 2937—2946
DOI https://doi.org/10.2147/CCID.S432108
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Jeffrey Weinberg
Kornkanok Chaisuwannarak, Chuda Rujitharanawong, Chayada Chaiyabutr, Chanisada Wongpraprarut, Narumol Silpa-archa
Department of Dermatology, Faculty of Medicine Siriraj Hospital, Mahidol University, Bangkok, Thailand
Correspondence: Narumol Silpa-archa, Department of Dermatology, Faculty of Medicine Siriraj Hospital, Mahidol University, Bangkok, Thailand, Email [email protected]
Background: The COVID-19 pandemic may alter individuals’ perspectives and behaviors regarding sun exposure and photoprotection. Presently, there is a paucity of information about how the pandemic influences photoprotection in photodermatoses and melasma.
Objective: To compare the photoprotection attitudes and behaviors of individuals with photodermatoses and melasma with those of a control group (other dermatologic patients) before and during the COVID-19 pandemic.
Methods: A questionnaire-based, cross-sectional study was conducted among Thai patients with photodermatoses, melasma, and other dermatological conditions between August 2021 and November 2022. Each of the three groups consisted of 35 patients.
Results: Among the 105 patients, 81.9% were female, and the mean age was 45.83 years. Over 80% of individuals who used surgical masks daily for 4 to 8 hours believed that these masks provided skin protection from the sun. The duration of sun exposure and the frequency of photoprotection practices decreased significantly in all groups during the COVID-19 pandemic compared to the pre-pandemic period. Sunscreen was the most prevalent form of photoprotection, but its usage declined considerably during the pandemic. Upon physical examination, the photodermatoses and control groups exhibited unchanged skin conditions, while the patients with melasma demonstrated improved skin conditions during the pandemic.
Conclusion: Owing to increased indoor activities and the perception that face masks could block sunlight, the COVID-19 pandemic led to notable reductions in sun exposure and photoprotective practices. Despite the absence of photodermatoses exacerbation and the observed improvements in patients with melasma, consistent and effective photoprotection must continue to be promoted.
Keywords: COVID-19 pandemic, melasma, photodermatoses, photoprotection
Introduction
The coronavirus disease 2019 (COVID-19) outbreak has resulted in a global crisis. Severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) is primarily transmitted through respiratory droplets and close contact. Airborne transmission may occur through the formation of aerosols.1 To prevent transmission, it is crucial to practice good hygiene, such as handwashing, avoiding crowded places, and utilizing protective equipment such as face masks and face shields.2,3
Photodermatoses are abnormal skin conditions to ultraviolet (UV) radiation, visible light, or artificial light sources. These can be classified into four categories: immunology-mediated photodermatoses, chemical and drug-induced photosensitivity, photo-aggravated dermatoses, and genetic disorders. Melasma is an acquired pigmentary disorder which is photoexacerbated.4,5 Sun protection measures are essential to protect the skin from these conditions. They include wearing sunglasses, protective clothing, and wide-brimmed hats; seeking shade during the sun’s peak hours (10 AM to 2 PM); and applying appropriate sunscreen. The American Academy of Dermatology recommends using broad-spectrum sunscreen with a sun protection factor of 30 or higher and water resistance. An application amount of 2 mg/cm2 is suggested for the skin surface, or as per the revised “teaspoon rule”, 1 teaspoon (5 mL) should be used for the face, head, and neck. Furthermore, the “two-finger rule” proposes utilizing 1 gram, corresponding to the amount on two fingertips for cream-based sunscreens. In outdoor situations, sunscreen should be reapplied every 2 hours to ensure continued protection.6,7
There is a need for more research on the impact of the COVID-19 pandemic on photoprotection attitudes and behaviors. Our study aimed to compare the attitudes and behaviors of photoprotection of individuals with photodermatoses and melasma with those with other dermatologic conditions before and during the COVID-19 pandemic. By understanding the changes in photoprotection behaviors and attitudes during the pandemic, we hope to provide guidance and recommendations to individuals with skin conditions to ensure that they are adequately protected from harmful UV radiation.
Material and Methods
This questionnaire-based cross-sectional study was conducted from August 3, 2021, to November 1, 2022. The Siriraj Institutional Review Board Ethics Committee approved the study protocol, at Mahidol University, Bangkok, Thailand (SI-593/2021). This study complies with the declaration of Helsinki. The authors obtained informed consent from patients for the use of their questionnaire data in the study.
Participants
We recruited Thai patients at least 18 years and older who were diagnosed with photodermatoses, melasma on the face, and other dermatologic conditions unrelated to sunlight, as examined at the outpatient Dermatology Department of Siriraj Hospital. The recruited patients attended the general dermatology, phototherapy, melasma, and autoimmune clinics. However, patients who did not use face masks and face shields during the COVID-19 pandemic were excluded from this study.
The present investigation aimed to compare the photoprotection attitudes and behaviors of individuals with photodermatoses and melasma with those of a control group: other dermatologic patients. The calculation of the representative sample size for this study was drawn from research by Chanprapaph et al,8 Maymone et al,9 and Gavelan et al.10 They found that sunscreen use among photodermatoses, melasma, and non-photosensitive skin diseases was 94%, 88%, and 52.3%, respectively. Based on this, the behavior of sunscreen use among sun-related and non-sun-related skin diseases would be approximately 90% and 55%, respectively. Using a two-sided type I error of 0.05, a power of 90%, and a ratio of n1:n2 of 2:1, the calculated sample size was 82 from two independent proportions.11 To account for potential incompleteness in questionnaires, 105 representative samples were sent to potential participants.
Questionnaire
A self-administered questionnaire was utilized in this study to gather information from participants. The questionnaire was divided into four parts. The first part included demographic data such as gender, age, education level, income, type of work, disease diagnosis, and disease duration for patients with photodermatoses, melasma, and other dermatologic conditions. The second part focused on photoprotection attitudes and behaviors before the COVID-19 pandemic. The aspects examined were sun exposure, frequency of sun protection, and protective methods used: wearing sunscreens, sunglasses, wide-brimmed hats, caps, umbrellas, or long-sleeved shirts, and seeking shade. This part also explored details of sunscreen application, such as the sunscreen type, amount used per facial area, and sunscreen characteristics. The third part focused on photoprotection attitudes and behaviors during the COVID-19 pandemic and compared them with those before the pandemic. This part included questions about the duration of sun exposure, frequency of sun protection, sunscreen characteristics, use of face masks and face shields (including types and duration of use), and the participants’ attitudes toward their ability to protect themselves from sunlight. The fourth part of the questionnaire was physician evaluations. It focused on disease diagnosis and clinical changes before and during the COVID-19 pandemic.
Statistical Analysis
The statistical analysis was conducted using IBM SPSS Statistics for Windows, version 27 (IBM Corp, Armonk, NY, USA). Descriptive statistics were used for categorical variables such as frequencies and percentages. Continuous variables are presented as means and standard deviations. Comparisons between two groups of quantitative data were performed using the independent t-test or the Mann–Whitney U-test. Associations between categorical variables and the study groups were analyzed using the chi-squared test. For comparisons between more than two groups of quantitative data, one-way ANOVA was used for variables with a normal distribution, while the Kruskal–Wallis H-test was used for non-normally distributed variables. McNemar test was used to compare changes in qualitative data within the same group before and during the COVID-19 pandemic. Probability (P) values < 0.05 were considered statistically significant.
Results
Table 1 details the demographic data of the 105 patients in the study. Thirty-five patients were diagnosed with photodermatoses (chronic actinic dermatitis, polymorphous light eruptions, actinic prurigo, and lupus erythematosus), and 35 had melasma. The remaining 35 patients served as the control group; they had conditions such as androgenetic alopecia and vitiligo (non-facial). The average baseline melasma area and severity index score for melasma patients was 13.05 (normal range = 0–48). Most patients in each of the three groups engaged in indoor activities (82.9%, 94.3%, and 85.7%, respectively). The mean disease durations of the photodermatoses, melasma, and control patients were 71.53 ± 43.68 months, 55.67 ± 42.89 months, and 33.29 ± 48.36 months, respectively (P = 0.001).
 |
Table 1 Baseline Characteristics of Photodermatoses, Melasma and Control Patients |
Table 2 presents the sun exposure and sun-protection behavior of photodermatoses, melasma, and control patients before and during the COVID-19 pandemic. Before the pandemic, photodermatoses patients mainly experienced 1 to 2 hours of daily sunlight exposure (37.1%), while melasma patients typically had 0.5 to 1 hour per day (34.3%). In contrast, most control patients were exposed for less than 0.5 hours daily (40.0%; P = 0.008). In terms of sun protection frequency before the pandemic, most photodermatoses and melasma patients used protection more than 50% of the time (45.7% and 88.6%, respectively), whereas the majority of control patients used protection less than 50% of the time (51.4%; P < 0.001). The most commonly used photoprotection method in the photodermatoses group was sunscreen (80.0%), followed by the use of umbrellas (71.4%) and seeking shade or using a sun visor (28.6%). In the melasma group, the primary method was sunscreen (97.1%), followed by umbrellas (65.7%) and wide-brimmed hats or caps (22.9%). For the control group, the most frequently used protective measure was sunscreen (74.3%), followed by umbrellas (42.9%) and seeking shade (31.4%).
 |
Table 2 Sun Exposed and Sun-Protection Behavior of the Photodermatoses, Melasma, and Control Patients Before and During the COVID-19 Pandemic |
During the COVID-19 pandemic, photodermatoses patients were typically exposed to sunlight for 1 to 2 hours per day (48.6%), while most melasma patients were exposed for 0.5 to 1 hour per day (42.9%). However, the majority of control patients were exposed for less than 0.5 hours per day (54.3%; P < 0.001). In terms of sun-protection frequency during the pandemic, most photodermatoses and control patients used protection less than 50% of the time (62.9% and 48.6%, respectively), whereas the majority of melasma patients used protection more than 50% of the time (71.4%; P = 0.001). The most commonly used photoprotection method in all three groups was sunscreen. Data analysis revealed significant differences in sun exposure (P = 0.025) and the frequency of sun protection (P = 0.001) before and during the COVID-19 pandemic.
Table 3 demonstrates the characteristics of sunscreen use among photodermatoses, melasma, and control patients before and during the COVID-19 pandemic. Before the pandemic, most patients used sunscreen daily (54.3% of photodermatoses patients, 82.9% of melasma patients, and 34.3% of control patients). Interestingly, all patients in the melasma group reported consistently using sunscreen (P = 0.001). The most common sunscreen formulation used by photodermatoses, melasma, and control patients was cream (74.3%, 68.6%, and 42.9%, respectively). Regarding the amount of sunscreen used per application, most photodermatoses and control patients used 1 fingertip unit or a single 10-Baht-coin-sized (FTU/10-Baht-coin) portion (40.0% and 40.0%, respectively), while the majority of melasma patients used a 2 FTU/10-Baht-coin portion size (57.1%; P = 0.073).
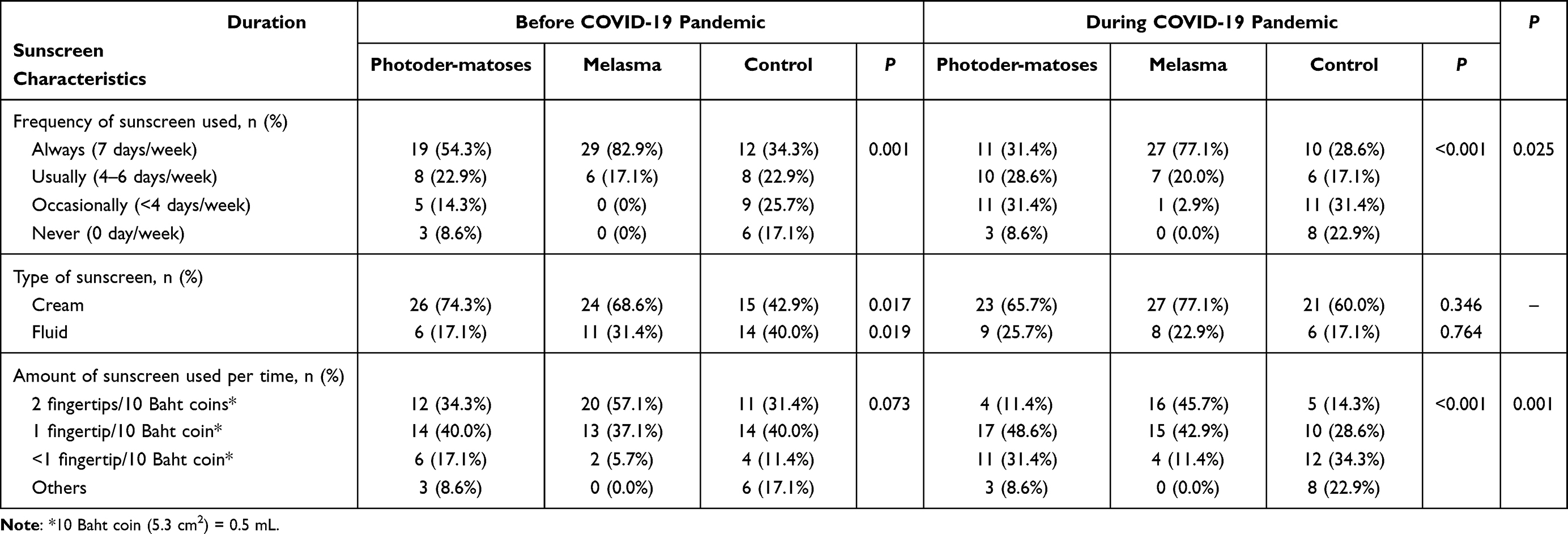 |
Table 3 Comparison of the Sunscreen Characteristics of the Photodermatoses and Melasma Patients with Those of the Controls Before and During the COVID-19 Pandemic |
During the pandemic, 31.4% of photodermatoses patients used sunscreen daily or occasionally, and 77.1% of melasma patients used it daily. However, most control patients used it only occasionally (31.4%; P < 0.001). The three groups’ most common type of sunscreen was cream (65.7%, 77.1%, and 60.0%, respectively). Regarding the amount of sunscreen used per application, most photodermatoses patients maintained a 1 FTU/10-Baht-coin portion size per application (48.6%), whereas most control patients used less than a 1 FTU/10-Baht-coin portion size per application (34.3%). On the other hand, the majority of melasma patients continued to use a 2 FTU/10-Baht-coin portion size (P < 0.001). There were significant differences in the frequency and amount of sunscreen used before and during the COVID-19 pandemic (P = 0.025 and 0.001, respectively). Compared with the control group, the photodermatoses and melasma patients tended to use sunscreen with higher sun protection factors (≥ 30), broader spectrum protection, higher UVA protection, and water resistance.
Regarding why some patients did not use sunscreen, most patients in the photodermatoses and control groups cited spending more time indoors (28.6% and 45.7%, respectively) as their primary reason. Other reasons were feeling uncomfortable when using sunscreen (17.1% in both groups) and believing that using sunscreen was a waste of time (2.9% in the photodermatoses group; 11.4% in the control group). In contrast, patients in the melasma group were more likely to cite spending more time indoors (14.3%) as well as feeling uncomfortable (8.6%) and preferring to use other forms of photoprotection (2.0%) as their reasons for not using sunscreen.
Table 4 summarizes the photodermatoses, melasma, and control patients’ attitudes toward and characteristics of using face masks and face shields during the COVID-19 pandemic. A higher proportion of photodermatoses and melasma patients considered that face masks protected their skin from sun rays (51.4% and 60.0%, respectively) than control patients (37.1%; P = 0.013). After wearing face masks, a higher proportion of photodermatoses and melasma patients reported improvement in their skin conditions (25.7% and 54.3%, respectively) compared with control patients (5.7%; P < 0.001). Most patients in all three groups believed that face shields did not protect their skin from the sun’s rays (88.9%, 85.7%, and 66.7%, respectively).
 |
Table 4 Comparison of the Face Mask and Face Shield Characteristics of the Photodermatoses and Melasma Patients with Those of the Controls During the COVID-19 Pandemic |
The majority of patients used surgical masks (77.1% of photodermatoses patients, 85.7% of melasma patients, and 82.9% of control patients). Fabric masks were the second most common type of mask used followed by N95 masks. Most patients in all three groups wore masks between 4 and 8 hours daily (51.4% of photodermatoses patients, 42.9% of melasma patients, and 45.7% of control patients). However, most patients did not use face shields during the COVID-19 pandemic. Among those who did use face shields, the majority wore them for less than 4 hours per day.
Table 5 shows the physician evaluations before and during the COVID-19 pandemic. Most photodermatoses and control patients had unchanged skin conditions (P = 0.070 and 0.003, respectively). Specifically, unchanged skin conditions were found in 100% of photodermatoses patients with chronic actinic dermatitis, 80% with polymorphous light eruptions, 100% with actinic prurigo, and 81.8% with lupus erythematosus. Similarly, 89.5% of control patients with hair disorders and 81.3% with vitiligo had no change in their skin conditions. In contrast, the majority of melasma patients experienced an improvement in their skin condition (57.1%; P < 0.001), as reflected by a decrease in the mean melasma area and severity index score from 13.05 to 11.13.
 |
Table 5 Physician Evaluations of the Photodermatoses, Melasma and Control Patients Before and During the COVID-19 Pandemic |
Discussion
Photodermatoses and melasma are skin conditions that are exacerbated by excessive sun exposure. The pandemic may change people’s views and practices toward sun exposure and photoprotection due to spending more time indoors and using face masks and face shields.
During the COVID-19 pandemic, more photodermatoses and melasma patients believed that face masks could protect their skin from sunlight than the control group (P = 0.013). A French study evaluated the sun protection levels of different types of face masks during the pandemic. It was found that all types of surgical masks blocked some UVA and UVB rays with similar ultraviolet protection factor values (6–11). Furthermore, French research showed that fabric masks made from dark-colored fabrics blocked more UV light than lighter-colored fabrics, indicating that there is no need to apply sunscreen on the parts of the face covered by the mask.12 Another study conducted in South Korea found that black-colored, multilayered respirator masks provided complete protection against UVA, infrared A (IR-A), and visible light.13 Moreover, previous research revealed that visible light exposure was a possible cause for melasma, and tinted sunscreen provided visible light protection in melasma patients.5 All patients (100%) in our study followed the Thai government’s rules and recommendations on wearing face masks during the pandemic and knew how COVID-19 was transmitted. Specifically, we found that most patients (81.9%) used surgical masks, and 46.7% wore them between 4 and 8 hours daily. A previous study in Thailand revealed that 97.6% wore a face mask outside the home.14 In Italy, a study found that most individuals (72.5%) wore face masks, 56.5% used surgical masks, and 53.0% used disposable masks.15 Based on the photoprotection impact of masks and our patients’ behavior while wearing masks during the pandemic, this could be one of the explanations for melasma improvement.
Regarding photoprotective behaviors before the COVID-19 pandemic, patients in the photodermatoses group had a longer duration of sun exposure than the melasma and control groups, particularly those exposed for more than 2 hours per day. However, most patients in all groups used sun protection more than 50% of the time, with sunscreen being the most commonly used UV protective measure. Most melasma patients used sunscreen daily, while some patients in the other groups used it occasionally or never. The main reasons for not using sunscreen were spending more time indoors and experiencing discomfort. Further analysis showed that many patients in the photodermatoses and control groups used insufficient sunscreen, whereas the melasma group tended to use adequate amounts. However, most photodermatoses and melasma patients used broad-spectrum sunscreen with sun protection factors ≥ 30, higher UVA protection, and water resistance than the control group.
Lowered photoprotection compliance in photodermatoses than in melasma patients in our study could be due to the chronicity of photodermatoses and may not be cosmetically related. As a consequence, the need for sun protection is neglected. Other studies in the United States found that 88% of melasma patients reported using sunscreen,9 while in Malaysia, only 50% of systemic lupus erythematosus patients reported using sunscreen.16 Research in the United States and Sweden also found lower rates of sunscreen use among systemic lupus erythematosus patients (29.8% and 38.8%, respectively).17,18 In our study, the skin conditions of the photodermatoses patients did not worsen but remained unchanged, despite a significant decrease in sunscreen usage. This finding may be because these individuals increased their time indoors during the pandemic, reducing their overall exposure to sunlight.
This study was limited by the sample being restricted to patients from the outpatient Dermatology Department at Siriraj Hospital, meaning its findings may not be generalizable to other locations. Another limitation is the use of self-administered questionnaires, which may have resulted in incomplete understanding and inaccurate answers from some patients. Additionally, recall bias may have occurred when asking about sunscreen usage and other behaviors before the COVID-19 pandemic.
Conclusions
The COVID-19 pandemic led to significant decreases in sun exposure and sunscreen usage across all groups due to increased indoor activities and the understanding that face masks could block sunlight. However, melasma patients were more aware of photoprotection and used more adequate amounts of sunscreen, improving their skin conditions. Although there was an improvement in the melasma patients and no worsening in the photodermatoses patients, it is still vital for dermatologists to encourage the use of sun protection measures. Doing so is critical now that the pandemic is under control and most patients have resumed their usual lifestyles.
Acknowledgments
We thank Mrs. Nerisa Thornsri for her assistance with the statistical analyses. The authors are also indebted to Mr. David Park for the English-language editing of this paper.
Disclosure
The authors report no relevant financial or nonfinancial conflicts of interest.
References
1. Guo YR, Cao QD, Hong ZS, et al. The origin, transmission and clinical therapies on coronavirus disease 2019 (COVID-19) outbreak – an update on the status. Mil Med Res. 2020;7(1):11. doi:10.1186/s40779-020-00240-0
2. Park SH. Personal protective equipment for healthcare workers during the COVID-19 pandemic. Infect Chemother. 2020;52(2):165–182. doi:10.3947/ic.2020.52.2.165
3. Goh Y, Tan BYQ, Bhartendu C, Ong JJY, Sharma VK. The face mask: how a real protection becomes a psychological symbol during Covid-19. Brain Behaves Immun. 2020;88:1–5. doi:10.1016/j.bbi.2020.05.060
4. Lehmann P, Schwarz T. Photodermatoses: diagnosis and treatment. Dtsch Arztebl Int. 2011;108(9):135–141. doi:10.3238/arztebl.2011.0135
5. Morgado-Carrasco D, Piquero-Casals J, Granger C, Trullàs C, Passeron T. Melasma: the need for tailored photoprotection to improve clinical outcome. Photodermatol Photoimmunol Photomed. 2022;38(6):515–521. doi:10.1111/phpp.12783
6. Mancuso JB, Maruthi R, Wang SQ, Lim HW. Sunscreens: an update. Am J Clin Dermatol. 2017;18(5):643–650. doi:10.1007/s40257-017-0290-0
7. Passeron T, Lim HW, Goh CL, et al. Photoprotection according to skin phototype and dermatoses: practical recommendations from an expert panel. Eur Acad Dermatol Venereol. 2021;35(7):1460–1469. doi:10.1111/jdv.17242
8. Chanprapaph K, Ploydaeng M, Pakornphadungsit K, Mekwilaiphan T, Vachiramon V, Kanokrungsee S. The behavior, attitude, and knowledge towards photoprotection in patients with cutaneous/systemic lupus erythematosus: a comparative study with 526 patients and healthy controls. Photochem Photobiol Sci. 2020;19(9):1201–1210. doi:10.1039/d0pp00073f
9. Maymone MBC, Neamah HH, Wirya SA, Patzelt NM, Zancanaro PQ, Vashi NA. Sun-protective behaviors in patients with cutaneous hyperpigmentation: a cross-sectional study. J Am Acad Dermatol. 2017;76(5):841–846.e2. doi:10.1016/j.jaad.2016.12.018
10. Gavelan ET, Anduaga ES, Ramos W, Saldaña LS, Sialer MDC. Knowledge, attitudes and practices about sun exposure and photoprotection in outpatients attending dermatology clinics at four hospitals in Lima, Peru*. An Bras Dermatol. 2011;86(6):1122–1128. doi:10.1590/S0365-05962011000600009
11. Rosner B. Thomson learning. In: Fundamentals of Biostatistics.
12. Couteau C, Paparis E, Coiffard L. What level of photoprotection can be obtained using facial mask? Determining effectiveness using an in vitro method. Dermatol Ther. 2021;34(3):e14837. doi:10.1111/dth.14837
13. Park SJ, Cho JH, Ham MS, Seo SH, Ahn HH, Kim DH. What type of face mask should we choose in coronavirus disease 2019 pandemic considering photoprotective effectiveness? Photodermatol Photoimmunol Photomed. 2022;38(6):548–554. doi:10.1111/phpp.12788
14. Kaewpan W, Rojpaisarnkit K, Pengpid S, Peltzer K. Factors affecting face mask-wearing behaviors to prevent COVID-19 among Thai people: a binary logistic regression model. Front Psychol. 2022;13:996189. doi:10.3389/fpsyg.2022.996189
15. Cazzaniga S, Pezzolo E, Colombo P, Naldi L. Face mask use in the community and cutaneous reactions to them during the COVID-19 pandemic: results of a national survey in Italy. Dermatol Rep. 2022;14(3):9394. doi:10.4081/dr.2022.9394
16. Abdul Kadir WD, Jamil A, Shaharir SS, Md Nor N, Abdul Gafor AH. Photoprotection awareness and practices among patients with systemic lupus erythematosus and its association with disease activity and severity. Lupus. 2018;27(8):1287–1295. doi:10.1177/0961203318770016
17. Gutmark EL, Lin DQ, Bernstein I, Wang SQ, Chong BF. Sun use in patients with cutaneous lupus erythematosus. Br J Dermatol. 2015;173(3):831–834. doi:10.1111/bjd.13736
18. Nived O, Andersson M, Lindgren M, et al. Adherence with advice and prescriptions in SLE is mostly good, but better follow up is needed: a study with a questionnaire. Lupus. 2007;16(9):701–706. doi:10.1177/0961203307080635
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Prevention of Melasma During Pregnancy: Risk Factors and Photoprotection-Focused Strategies
Zhao L, Fu X, Cheng H
Clinical, Cosmetic and Investigational Dermatology 2024, 17:2301-2310
Published Date: 15 October 2024