Back to Journals » Neuropsychiatric Disease and Treatment » Volume 16
Depression, Anxiety and Primiparity are Negatively Associated with Mother–Infant Bonding in Japanese Mothers
Authors Motegi T, Watanabe Y ![]() , Fukui N
, Fukui N ![]() , Ogawa M, Hashijiri K, Tsuboya R, Sugai T, Egawa J, Araki R, Haino K, Yamaguchi M, Nishijima K, Enomoto T
, Ogawa M, Hashijiri K, Tsuboya R, Sugai T, Egawa J, Araki R, Haino K, Yamaguchi M, Nishijima K, Enomoto T ![]() , Someya T
, Someya T
Received 15 October 2020
Accepted for publication 27 November 2020
Published 14 December 2020 Volume 2020:16 Pages 3117—3122
DOI https://doi.org/10.2147/NDT.S287036
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Taro Kishi
Takaharu Motegi,1 Yuichiro Watanabe,1 Naoki Fukui,1 Maki Ogawa,1 Koyo Hashijiri,1 Ryusuke Tsuboya,1 Takuro Sugai,1 Jun Egawa,1 Rie Araki,2 Kazufumi Haino,3 Masayuki Yamaguchi,3 Koji Nishijima,4 Takayuki Enomoto,3 Toshiyuki Someya1
1Department of Psychiatry, Niigata University Graduate School of Medical and Dental Sciences, Niigata, Japan; 2Nursing, Niigata University Medical and Dental Hospital, Niigata, Japan; 3Department of Obstetrics and Gynecology, Niigata University Graduate School of Medical and Dental Sciences, Niigata, Japan; 4General Center for Perinatal, Maternal and Neonatal Medicine, Niigata University Medical and Dental Hospital, Niigata, Japan
Correspondence: Yuichiro Watanabe
Department of Psychiatry, Niigata University Graduate School of Medical and Dental Sciences, 757 Asahimachidori-Ichibancho, Chuo-Ku, Niigata 951-8510, Japan
Tel +81-25-227-2213
Fax +81-25-227-0777
Email [email protected]
Purpose: Postpartum depression is a well-known risk factor, and postpartum anxiety and parity are potential risk factors, for mother–infant bonding disorder. However, few studies have focused on the relationships among these factors and mother–infant bonding. This cross-sectional study explored the associations between depression, anxiety and parity, and mother–infant bonding.
Materials and Methods: Japanese mothers, both primiparas and multiparas, completed the Mother-to-Infant Bonding Scale (MIBS) and the Hospital Anxiety and Depression Scale (HADS) one month after childbirth. We performed a stepwise multiple regression analysis with the forward selection method to assess the effects of HADS anxiety and depression scores and parity as independent variables on mother–infant bonding as the dependent variable.
Results: A total of 2379 Japanese mothers (1116 primiparas and 1263 multiparas) took part in the study. MIBS score (2.89 ± 2.68 vs 1.60 ± 2.11; p < 0.0001) was significantly higher in primiparas than in multiparas. HADS anxiety (6.55 ± 4.06 vs 4.63 ± 3.41; p < 0.0001) and depression (6.56 ± 3.43 vs 5.98 ± 3.20; p < 0.0001) scores were also significantly higher in primiparas than in multiparas. A stepwise multiple regression analysis with the forward selection method revealed that HADS depression and anxiety scores and parity were significantly associated with MIBS score (p = 0.003, 0.015 and 0.023).
Conclusion: Depression, anxiety and primiparity were negatively associated with mother–infant bonding one month after childbirth.
Keywords: HADS, Japanese, MIBS, parity, postpartum
Introduction
Bonding disorder is a psychological state that leads to lack of affection and emotional bond with children. Parents with bonding disorder may have feelings of rejection or even hatred towards their children.1 Early detection and prevention of signs of bonding failure are very important in preventing child abuse, improving relationships with children, and supporting childcare.2
Systematic reviews have demonstrated that peripartum depression is negatively associated with mother–infant bonding3,4 and that peripartum anxiety may also have negative effects on mother–infant bonding.3 These findings remain controversial,4,5 but identifying and intervening in both depression and anxiety during the peripartum period are considered critical to prevent bonding disorder. However, few studies have investigated the effects of peripartum anxiety and depression simultaneously on mother–infant bonding with small sample sizes.6–11
One study found that 5.0% of 280 Japanese primiparas who were interviewed by trained midwives had experienced a major depressive episode within 3 months of childbirth.12 A meta-analysis of self-report questionnaire surveys found that the prevalence of depression at one month after childbirth was 14.3% in 108,431 Japanese mothers.13 By contrast, the prevalence of postpartum anxiety has been poorly studied. A self-report questionnaire survey reported that 26.2% of 1348 Japanese mothers had experienced anxiety at 3–4 months after childbirth.14 In Japan, many studies have shown that postpartum depression is negatively associated with mother–infant bonding,6–8,15–19 but few studies have evaluated the effects of postpartum anxiety on mother–infant bonding.7,8 Recent large-scale Japanese studies have provided evidence for associations of primiparity with poor mother–infant bonding18 and postpartum depression.13,18 However, there is little research, with inconsistent findings, on the influence of parity in postpartum anxiety in either Japan8 or elsewhere.4,9,10,20 It is still unclear how depression, anxiety, parity and mother–infant bonding are related in Japanese mothers.
This study aimed to assess whether primiparas showed poorer mother–infant bonding and worse symptoms of anxiety and depression than multiparas, and whether depression, anxiety and primiparity were negatively associated with mother–infant bonding.
Materials and Methods
Ethics Statement
This study followed the principles of the Declaration of Helsinki and was approved by the Ethics Committee of Niigata University and the ethics committees of the participating obstetric institutions. Written informed consent was obtained from all participants.
All relevant data are within the paper. We are not able to make the underlying data available to readers, because we do not have the permission of the committees to do so.
Participants
This study is part of the Perinatal Mental Health Research Project, which has been in progress since March 2017.21 We recruited participants from 34 obstetric institutions in Niigata Prefecture, Japan, and included pregnant Japanese women aged 18 years or older. We excluded pregnant women with serious physical complications, serious pregnancy complications, or severe psychiatric disorders (eg, severe schizophrenia or severe depression).
Measurements
The instruments were administered consecutively and self-completed at three time points: early pregnancy (approximately 12–15 weeks), late pregnancy (approximately 30–34 weeks) and postpartum (4 weeks after childbirth). This study is a sub-analysis of postpartum data up to December 2019.
The Mother-to-Infant Bonding Scale (MIBS) is a self-report questionnaire that evaluates the feelings of mothers towards their babies.22 This scale was originally developed as an eight-item questionnaire22 and was later modified to add two additional items.15 The MIBS contains 10 items that assess mother–infant bonding.15 Each item is graded on a four-point Likert-type scale (0–3). Higher MIBS scores indicate worse mother–infant bonding. The Japanese version of MIBS has been previously validated15 and is commonly used to assess mother–infant bonding in Japan.7,8,15,16,18,21
The Edinburgh Postnatal Depression Scale (EPDS) is the most widely used self-report questionnaire for screening for peripartum depression.6,9–11,13,15–19,23–25 However, this scale is not suitable for detecting peripartum anxiety.23 We therefore used the Hospital Anxiety and Depression Scale (HADS), which is a self-report questionnaire designed to identify anxiety and depression in non-psychiatric hospital outpatients.26 It has also been used in pregnant women.6–8,14,27–37 The HADS includes 14 questions, of which seven assess anxiety (items 1, 3, 5, 7, 9, 11, and 13) and seven depression (items 2, 4, 6, 8, 10, 12, and 14).26 Each item is graded on a four-point Likert-type scale (0–3). Higher HADS scores indicate more severe symptoms of anxiety and depression. The Japanese version of HADS38 has been validated in a previous study.39
Statistical Analysis
We compared the mean age, MIBS score, and HADS anxiety and depression scores for primiparas and multiparas using a t-test. To identify potential predictors of mother–infant bonding, we used simple regression analyses with HADS anxiety and depression scores, parity and age as independent variables and MIBS score as the dependent variable. We regarded variables with p values less than 0.1 as potential predictors. We then performed a stepwise multiple regression analysis with the forward selection method to assess the effects of potential predictors on mother–infant bonding. We used the Statistical Package for the Social Sciences (SPSS) version 25 (IBM Japan, Tokyo, Japan) for the statistical analyses.
Results
The study participants were 2379 mothers (1116 primiparas and 1263 multiparas). These individuals included 1755 mothers (853 primiparas and 902 multiparas) from a previous study reporting the factor structure of MIBS.21 The age of participants ranged from 18−50 years. Primiparas were significantly younger than multiparas (mean age ± SD: 31.0 ± 4.96 vs 33.0 ± 4.34 years; Table 1).
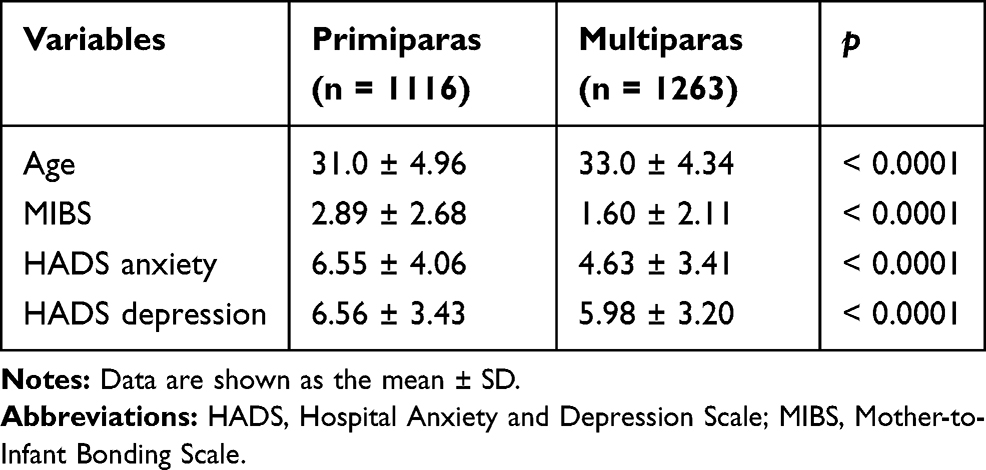 |
Table 1 MIBS and HADS Scores in Primiparas and Multiparas |
We assessed mother–infant bonding and symptoms of anxiety and depression using MIBS and HADS in 1116 primiparas and 1263 multiparas (Table 1). MIBS score (2.89 ± 2.68 vs 1.60 ± 2.11) was significantly higher in primiparas than in multiparas. HADS anxiety (6.55 ± 4.06 vs 4.63 ± 3.41) and depression (6.56 ± 3.43 vs 5.98 ± 3.20) scores were also significantly higher in primiparas than in multiparas. Cronbach’s α values for overall MIBS and HADS, anxiety and depression were 0.885, 0.751, 0.778 and 0.806, respectively.
Using simple regression analysis, we identified HADS anxiety score (r = 0.500 and p < 0.001), HADS depression score (r = 0.476 and p < 0.001) and parity (r = −0.264 and p < 0.001), but not age (r = 0.012 and p = 0.595), as potential predictors of mother–infant bonding. A stepwise multiple regression analysis with the forward selection method found that HADS depression score (standardized regression coefficient [SRC] = 0.454), HADS anxiety score (SRC = 0.359) and parity (SRC = −0.252) were significantly associated with MIBS score (Table 2).
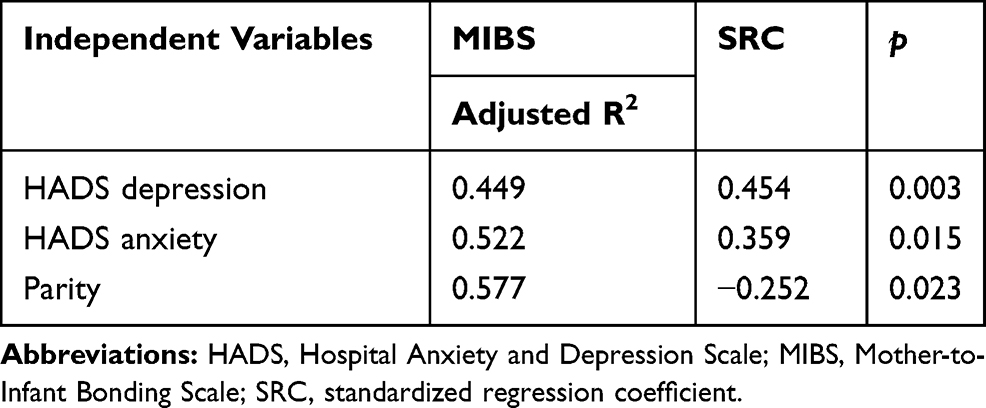 |
Table 2 Multiple Regression Analysis for the Effects of HADS Depression and Anxiety Scores and Parity on MIBS Score |
Discussion
In this study, 1116 primiparas had significantly higher MIBS and HADS scores than 1263 multiparas one month after childbirth. The Japan Environment and Children’s Study indicated that EPDS and MIBS scores one month after childbirth were significantly higher in 32,342 primiparas than in 44,031 multiparas.18 A meta-analysis showed that 35,023 Japanese primiparas had a significantly higher prevalence of postpartum depression measured using EPDS than 66,983 multiparas, with a relative risk of 1.76.13 Kita et al reported that primiparity was significantly correlated with HADS score one month after childbirth in 562 Japanese mothers.8 Taken together, these findings suggest that Japanese primiparas show poorer mother–infant bonding and worse symptoms of anxiety and depression than multiparas in the postpartum period. There may be some explanations for these differences. First, multiparas are likely to draw confidence from their previous experience, whereas childbirth and childcare are unknown events for primiparas.13,18,25 Second, women who suffered bonding failure, depression or anxiety during the peripartum period of their first birth may not want to give birth to a second child.13
Postpartum depression is a well-known risk factor for mother–infant bonding disorder.3,18 In our multiple regression analysis, depression had the most significant negative association with mother–infant bonding. At the second step of the multiple regression analysis, we observed a significant association between HADS anxiety score and MIBS score. Kita et al8 also reported that HADS anxiety score was significantly correlated with the scores of two MIBS subscales (lack of affection, and anger and rejection) one month after childbirth in 562 Japanese mothers. However, they used simple regression analysis. Using multiple regression analysis, Edhborg et al9 found that the score for the State-Trait Anxiety Inventory was inversely correlated with the score for the Postpartum Bonding Questionnaire (PBQ) at 2–3 months after childbirth in 674 Bangladeshi mothers. This suggests that there was a positive association between anxiety and mother–infant bonding. Tietz et al10 assessed depressive symptoms using EPDS, anxiety symptoms using the Anxiety Cognitions Questionnaire and the Body Sensations Questionnaire, and mother–infant bonding using PBQ in 78 German mothers at 2–8 months after childbirth. In simple regression analyses, symptoms of both depression and anxiety were significantly correlated with mother–infant bonding. In a multiple regression analysis, however, the association between symptoms of anxiety and mother–infant bonding was not significant after controlling for the effect of depressive symptoms. Lutkiewicz et al11 also reported similar results in 150 Polish mothers at 1–3 days after childbirth. These inconsistencies among studies may stem from differences in ethnicity, postpartum period, rating scale and statistical analysis. However, it is important to assess the impact of both postpartum depression and anxiety on mother–infant bonding. In our multiple regression analysis, we found the negative effect of primiparity on mother–infant bonding remained after controlling for depression and anxiety. This suggests that we should pay attention to symptoms of both depression and anxiety especially in primiparas, who are at higher risk of bonding disorders.
This study had some limitations. First, it was cross-sectional, and therefore able to show associations between HADS depression and anxiety scores and parity, and MIBS score. However, we could not determine causal relationships. Prospective studies will be needed to provide evidence for causation. Second, our 2379 participants may not be representative of the general population of postpartum Japanese women. However, they were recruited from 34 obstetric institutions in Niigata Prefecture. Our findings that primiparas show poorer mother–infant bonding and worse depressive symptoms than multiparas are consistent with those from earlier large-scale Japanese studies.13,18 We therefore speculate that our results are unlikely to be affected by sampling bias. Third, we did not adjust for potential confounders, such as employment, education, social support, partner relationship, attachment to own mother, and history of mental disorders,3,4,18,40–43 because these sociodemographic data were not available.
Conclusion
Depression, anxiety and primiparity were negatively associated with mother–infant bonding one month after childbirth.
Abbreviations
EPDS, Edinburgh Postnatal Depression Scale; HADS, Hospital Anxiety and Depression Scale; MIBS, Mother-to-Infant Bonding Scale; PBQ, Postpartum Bonding Questionnaire; SRC, standardized regression coefficient.
Acknowledgments
The authors greatly appreciate the support of all participants and staff of the participating obstetric institutions: Kameda Daiichi Hospital, Niitsu Obstetrics and Gynecology Clinic, Tomita Obstetrics and Gynecology Clinic, Honda Ladies Clinic, Agano City Hospital, Chihara Clinic, Sekizuka Clinic, Hirohashi Obstetrics and Gynecology Clinic, Niigata Saiseikai Sanjo Hospital, Saiseikai Niigata Hospital, Itoigawa Sogo Hospital, Niigata Prefectural Tokamachi Hospital, Takeyama Hospital, Watanabe Kinen Clinic, Kashiwazaki General Hospital and Medical Center, Kido Hospital, Tachikawa Medical Center, Saintpaulia Women’s Clinic, Nagaoka Chuo General Hospital, Arakawa Ladies Clinic, Ueda Ladies Clinic, Uonuma Kikan Hospital, Murakami General Hospital, Sado General Hospital, Tokunaga Ladies Clinic, Nagaoka Red Cross Hospital, Niigata Prefectural Shibata Hospital, Ladies Clinic Ishiguro, Angel Mother Clinic, Joetsu General Hospital, Niigata City General Hospital, Ojiya General Hospital, Watanabe Clinic, and Niigata University Medical and Dental Hospital. We thank Jennifer Barrett, PhD, and Melissa Leffler, MBA, from Edanz Group (https://en-author-services.edanzgroup.com/ac) for editing a draft of this manuscript.
This work was supported by Grants-in-Aid for Scientific Research (19K08040 to NF) from the Japan Society for the Promotion of Science, by a grant from the Niigata Medical Association (to TM), and by a grant from the Medical Association of Niigata City (to MO).
Disclosure
Toshiyuki Someya reports grants and personal fees from Astellas Pharma Inc., Eli Lilly Japan K.K., Mitsubishi Tanabe Pharma Co., Mochida Pharmaceutical Co., Ltd.,MSD K.K., Novartis Pharma K.K., Otsuka Pharmaceutical Co., Ltd., Shionogi Co., Ltd., and Sumitomo Dainippon Pharma Co., Ltd., during the conduct of the study. The authors report no other potential conflicts of interest in this work.
References
1. Kumar RC. “Anybody’s child”: severe disorders of mother-to-infant bonding. Br J Psychiatry. 1997;171(2):175–181. doi:10.1192/bjp.171.2.175
2. Kinsey CB, Hupcey JE. State of the science of maternal–infant bonding: A principle-based concept analysis. Midwifery. 2013;29(12):1314–1320. doi:10.1016/j.midw.2012.12.019
3. Tichelman E, Westerneng M, Witteveen AB, et al. Correlates of prenatal and postnatal mother-to-infant bonding quality: A systematic review. PLoS One. 2019;14(9):e0222998. doi:10.1371/journal.pone.0222998
4. McNamara J, Townsend ML, Herbert JS. A systemic review of maternal wellbeing and its relationship with maternal fetal attachment and early postpartum bonding. PLoS One. 2019;14(7):e0220032. doi:10.1371/journal.pone.0220032
5. Śliwerski A, Kossakowska K, Jarecka K, et al. The effect of maternal depression on infant attachment: A systematic review. Int J Environ Res Public Health. 2020;17(8):2675. doi:10.3390/ijerph17082675
6. Kokubu M, Okano T, Sugiyama T. Postnatal depression, maternal bonding failure, and negative attitudes towards pregnancy: a longitudinal study of pregnant women in Japan. Arch Womens Ment Health. 2012;15(3):211–216. doi:10.1007/s00737-012-0279-x
7. Kitamura T, Takegata M, Haruna M, et al. The Mother-Infant Bonding Scale: factor structure and psychosocial correlates of parental bonding disorders in Japan. J Child Fam Stud. 2015;24:393–401. doi:10.1007/s10826-013-9849-4
8. Kita S, Haruna M, Matsuzaki M, Kamibeppu K. Associations between intimate partner violence (IPV) during pregnancy, mother-to-infant bonding failure, and postnatal depressive symptoms. Arch Womens Ment Health. 2016;19(4):623–634. doi:10.1007/s00737-016-0603-y
9. Edhborg M, Nasreen HE, Kabir ZN. Impact of postpartum depressive and anxiety symptoms on mothers’ emotional tie to their infants 2-3 months postpartum: a population-based study from rural Bangladesh. Arch Womens Ment Health. 2011;14(4):307–316. doi:10.1007/s00737-011-0221-7
10. Tietz A, Zietlow A-L, Reck C. Maternal bonding in mothers with postpartum anxiety disorder: the crucial role of subclinical depressive symptoms and maternal avoidance behaviour. Arch Womens Ment Health. 2014;17(5):433–442. doi:10.1007/s00737-014-0423-x
11. Lutkiewicz K, Bieleninik Ł, Cieślak M, et al. Maternal–Infant Bonding and Its Relationships with Maternal Depressive Symptoms, Stress and Anxiety in the Early Postpartum Period in a Polish Sample. Int J Environ Res Public Health. 2020;17(15):5427. doi:10.3390/ijerph17155427
12. Kitamura T, Yoshida K, Okano T, et al. Multicentre prospective study of perinatal depression in Japan: incidence and correlates of antenatal and postnatal depression. Arch Womens Ment Health. 2006;9(3):121–130. doi:10.1007/s00737-006-0122-3
13. Tokumitsu K, Sugawara N, Maruo K, et al. Prevalence of perinatal depression among Japanese women: a meta-analysis. Ann Gen Psychiatry. 2020;19(1):41. doi:10.1186/s12991-020-00290-7
14. Sato Y, Kato T, Kakee N. A six-month follow-up study of maternal anxiety and depressive symptoms among Japanese. J Epidemiol. 2008;18(2):84–87. doi:10.2188/jea.18.84
15. Yoshida K, Yamashita H, Conroy S, et al. A Japanese version of Mother-to-Infant Bonding Scale: factor structure, longitudinal changes and links with maternal mood during the early postnatal period in Japanese mothers. Arch Womens Ment Health. 2012;15(5):343–352. doi:10.1007/s00737-012-0291-1
16. Matsunaga A, Takauma F, Tada K, Kitamura T. Discrete category of mother-to-infant bonding disorder and its identification by the Mother-to-Infant Bonding Scale: A study in Japanese mothers of a 1-month-old. Early Hum Dev. 2017;111:1–5. doi:10.1016/j.earlhumdev.2017.04.008
17. Ohara M, Nakatochi M, Okada T, et al. Impact of perceived rearing and social support on bonding failure and depression among mothers: A longitudinal study of pregnant women. J Psychiatr Res. 2018;105:71–77. doi:10.1016/j.jpsychires.2018.09.001
18. Tsuchida A, Hamazaki K, Matsumura K, et al. Changes in the association between postpartum depression and mother-infant bonding by parity: longitudinal results from the Japan Environment and Children’s Study. J Psychiatr Res. 2019;110:110–116. doi:10.1016/j.jpsychires.2018.11.022
19. Nakano M, Upadhyaya S, Chudal R, et al. Risk factors for impaired maternal bonding when infants are 3 months old: a longitudinal population based study from Japan. BMC Psychiatry. 2019;19(1):87. doi:10.1186/s12888-019-2068-9
20. Martínez-Galiano JM, Hernández-Martínez A, Rodríguez-Almagro J, et al. Relationship between parity and the problems that appear in the postpartum period. Sci Rep. 2019;9(1):11763. doi:10.1038/s41598-019-47881-3
21. Motegi T, Fukui N, Hashijiri K, et al. Identifying the factor structure of the Mother-to-Infant Bonding Scale for post-partum women and examining its consistency during pregnancy. Psychiatry Clin Neurosci. 2019;73(10):661–662. doi:10.1111/pcn.12920
22. Taylor A, Atkins R, Kumar R, Adams D, Glover V. A new Mother-to-Infant Bonding Scale: links with early maternal mood. Arch Womens Ment Health. 2005;8(1):45–51. doi:10.1007/s00737-005-0074-z
23. Cox JL, Holden JM, Sagovsky R. Detection of postnatal depression. Development of the 10-item Edinburgh Postnatal Depression Scale. Br J Psychiatry. 1987;150(6):782–786. doi:10.1192/bjp.150.6.782
24. Kubota C, Inada T, Nakamura Y, et al. Stable factor structure of the Edinburgh Postnatal Depression Scale during the whole peripartum period: results from a Japanese prospective cohort study. Sci Rep. 2020;17(15):17659. doi:10.3390/ijerph17155427
25. Takehara K, Tachibana Y, Yoshida K, et al. Prevalence trends of pre- and postnatal depression in Japanese women: A population-based longitudinal study. J Affect Disord. 2018;225:389–394. doi:10.1016/j.jad.2017.08.008
26. Zigmond AS, Snaith RP. The hospital anxiety and depression scale. Acta Psychiatr Scand. 1983;67(6):361–370. doi:10.1111/j.1600-0447.1983.tb09716.x
27. Abiodun OA. A validity study of the Hospital Anxiety and Depression Scale in general hospital units and a community sample in Nigeria. Br J Psychiatry. 1994;165(5):669–672. doi:10.1192/bjp.165.5.669
28. Condon JT, Corkindale C. The correlates of antenatal attachment in pregnant women. Br J Med Psychol. 1997;70(4):359–372. doi:10.1111/j.2044-8341.1997.tb01912.x
29. Herrmann C. International experiences with the Hospital Anxiety and Depression Scale–a review of validation data and clinical results. J Psychosom Res. 1997;42(1):17–41. doi:10.1016/s0022-3999(96)00216-4
30. Karimova G, Martin C. A psychometric evaluation of the Hospital Anxiety and Depression Scale during pregnancy. Psychol Health Med. 2003;8(1):89–103. doi:10.1080/1354850021000059296
31. JØ B, Mykletun A, Daltveit AK, et al. Neonatal outcomes in offspring of women with anxiety and depression during pregnancy. A linkage study from The Nord-Trøndelag Health Study (HUNT) and Medical Birth Registry of Norway. Arch Womens Ment Health. 2005;8(3):181–189. doi:10.1007/s00737-005-0090-z
32. Lee AM, Lam SK, Sze Mun Lau SM, et al. Prevalence, course, and risk factors for antenatal anxiety and depression. Obstet Gynecol. 2007;110(5):1102–1112. doi:10.1097/01.AOG.0000287065.59491.70
33. Qiao YX, Wang J, Li J, Ablat A. The prevalence and related risk factors of anxiety and depression symptoms among Chinese pregnant women in Shanghai. Aust N Z J Obstet Gynaecol. 2009;49(2):185–190. doi:10.1111/j.1479-828X.2009.00966.x
34. Ali NS, Azam IS, Ali BS, et al. Frequency and associated factors for anxiety and depression in pregnant women: a hospital-based cross-sectional study. ScientificWorldJournal. 2012;2012:653098. doi:10.1100/2012/653098
35. Waqas A, Raza N, Lodhi HW, et al. Psychosocial factors of antenatal anxiety and depression in Pakistan: is social support a mediator? PLoS One. 2015;10(1):e0116510. doi:10.1371/journal.pone.0116510
36. van de Loo KFE, Vlenterie R, Nikkels SJ, et al. Depression and anxiety during pregnancy: the influence of maternal characteristics. Birth. 2018;45(4):478–489. doi:10.1111/birt.12343
37. Çankaya S. The effect of psychosocial risk factors on postpartum depression in antenatal period: A prospective study. Arch Psychiatr Nurs. 2020;34(3):176–183. doi:10.1016/j.apnu.2020.04.007
38. Kitamura T. Hospital anxiety and depression scale. Arch Psychiatric Diagnostics Clin Evaluation. 1993;4:371–372.
39. Kugaya A, Akechi T, Okuyama T, et al. Screening for psychological distress in Japanese cancer patients. Jpn J Clin Oncol. 1998;28(5):333–338. doi:10.1093/jjco/28.5.333
40. Zdolska-Wawrzkiewicz A, Chrzan-Dętkoś M, Bidzan M. Maternal attachment style during pregnancy and becoming a mother in Poland. J Reprod Infant Psychol. 2018;36(1):4–14. doi:10.1080/02646838.2017.1395400
41. Zdolska-Wawrzkiewicz A, Bidzan M, Chrzan-Dętkoś M, et al. The dynamics of becoming a mother during pregnancy and after childbirth. Int J Environ Res Public Health. 2019;17(1):57. doi:10.3390/ijerph17010057
42. Zdolska-Wawrzkiewicz A, Chrzan-Dętkoś M, Pizuńska D, et al. Attachment styles, various maternal representations and a bond to a baby. Int J Environ Res Public Health. 2020;17(10):3363. doi:10.3390/ijerph17103363
43. Kucharska M. Selected predictors of maternal-fetal attachment in pregnancies with congenital disorders, other complications, and in healthy pregnancies. Health Psychology Rep. 2020. doi:10.5114/hpr.2020.97295
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.