")
Back to Journals » Clinical, Cosmetic and Investigational Dermatology » Volume 13
Depression and Anxiety in Patients with Bullous Pemphigoid: Impact and Management Challenges
Authors Kluger N , Pankakoski A, Panelius J
Received 26 November 2019
Accepted for publication 3 January 2020
Published 21 January 2020 Volume 2020:13 Pages 73—76
DOI https://doi.org/10.2147/CCID.S212984
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Jeffrey Weinberg
Nicolas Kluger, Anna Pankakoski, Jaana Panelius
Department of Dermatology, Allergology and Venereology, Helsinki University Hospital, Helsinki, Finland
Correspondence: Nicolas Kluger
Department of Dermatology, Skin and Allergies Hospital, Meilahdentie 2, PO Box 160, Helsinki 00029 HUS, Finland
Email [email protected]
Abstract: Bullous pemphigoid is the most common autoimmune subepidermal blistering disease of the skin and mucous membranes. It is also associated with high mortality and poor prognosis due to advanced age of the patients and coexisting comorbidities. There is a dearth of data in the literature regarding depression and anxiety among those patients. The objective of this brief review is to discuss the intertwining relationship between depression and anxiety with bullous pemphigoid.
Keywords: anxiety, bullous pemphigoid, corticosteroids, depression, drug-induced bullous pemphigoid, quality of life
Introduction
Bullous pemphigoid (BP) is the most common autoimmune subepidermal blistering disease of the skin and mucous membranes.1 It affects mainly the elderly patients aged ≥65 years and displays its highest incidence after the age of 90.2,3 In Europe, its incidence ranges from 2.5 to 42.8 per 10,00,000 person-years.4 BP presents as tense blisters leaving erosions and crusts and erythema, associated with urticarial plaques and itch.1–3 BP is also associated with high mortality and poor prognosis due to advanced age of the patients and comorbidities.5–10 In this brief review, we discuss the relationships between depression and anxiety with BP (Figure 1).
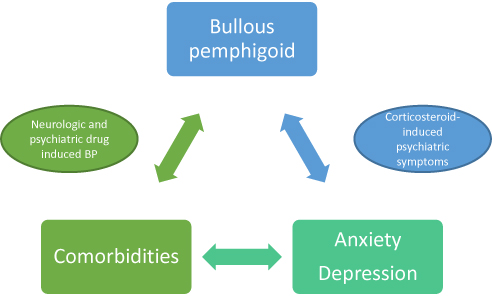 |
Figure 1 Intertwining between depression and anxiety with bullous pemphigoid and associated comorbidities. Pemphigoid and any associated comorbidities may be responsible for anxiety or depression. Drugs given to treat anxiety or depression might be a potential trigger of BP. Additionally, cross-reactive immune responses between neural and cutaneous antigens may also have an influence. On the other hand, systemic corticosteroids to treat bullous pemphigoid may induce psychiatric complications. |
Quality of Life in Patients with Bullous Pemphigoid
The morbidity of BP and its impact on the quality of life (QoL) are significant.1 BP causes significant physical discomfort (itchy patches, blisters, erosions) and physical limitations. Besides time spent on treatment, financial burden (high number of corticosteroid tubes, nurse at home) and social misconceptions should not be forgotten. For a patient treated with the recommended 30 g/day clobetasol propionate cream protocol,5 the costs for the treatment of one patient with potent topical corticosteroids during 4 months will be €174.80 ($224.57) in the Netherlands.11 However, this pharmaco-economic evaluation does not include body application by home care nurses that can substantially increase the total costs.11 Studies have shown the impact on the QoL of patients with autoimmune bullous diseases (AIBD).12,13 However, most of these studies have focused on pemphigus12,13 or BP patients are analyzed along with other AIBD.14 To the best of our knowledge, only Kouris et al have specifically reported on BP’s impact on QoL. In their series of 57 patients with BP, they found that patients had higher scores for depression compared to sex- and gender-matched healthy controls, but did not find any difference for anxiety. The patients had a higher perception of loneliness and social isolation compared to the controls. There was a positive correlation between depression and loneliness scores.15 BP may result in restrictions on work and daily activities, patients may be concerned about their appearance, the BP treatment and its probable recurrence.15 It is however important to stress that the series of patients in the report by Kouris et al was small and included quite young people. The mean age was 59 years, which is far from being representative of the typical population of BP patients (≥70 years-old). In another small comparative study, DeGrazia et al found that patients with atopic dermatitis and BP shared similar experience and QoL impact in relation to chronic itch.16
A questionnaire specific to AIBD was recently developed: the Autoimmune Bullous Disease Quality of Life (ABQOL). It was found to be more sensitive than the Dermatology Life Quality Index (DQLI). It explores 17 items including depression, anxiety, relationships, social life, etc.17 However, we did not find any publication about its use in “real life” with large cohort of BP patients.
Bullous Pemphigoid and Neurological and Psychiatric Disorders
BP is associated with various comorbidities including neurological and psychiatric disorders. In Finland, Försti et al found patients with various central nervous system disorders were at higher risk of developing BP. They included multiple sclerosis, various forms of dementia, cerebral strokes, and hemorrhages as well as epilepsy. They also found various psychiatric conditions, mostly schizophrenia, and personality disorders, but also bipolar disorders and major depression as risk factors.18 Association with neurological conditions and psychiatric disorders have been observed also in other epidemiological studies.19–21 Link with psychiatric conditions is not consistently found in every series.19,22 Bastuji-Garin et al observed that patients with BP were more likely to have bipolar disorder (4%) compared with controls.23 Conversely, a large US study showed that patients with BP that were hospitalized were more likely to have psychoses or depression (among others) but no bipolar disorder.24 One appealing hypothesis is that neurodegeneration or neuroinflammation could lead to a cross-reactive immune response between neural and cutaneous antigens and the failure of self-tolerance. Indeed, BP autoantigens BP180 and BP230 are expressed in the central nervous system.25 Circulating BP antibodies have been found in some patients with neurological diseases such as dementia and Parkinson’s disease but is not known for patients with psychiatric conditions.25
Drug-Induced Bullous Pemphigoid
Drug-induced BP is a well-known subset of BP.26 Medications to treat any associated comorbidities should be investigated. Until recently, the list of culprit drugs is rather small regarding psychiatric disorders. Neuroleptics have been reported to be associated,27 and anecdotal case reports have been published with risperidone28 or with fluoxetine.29 Varpuluoma et al published recently a study from the Finnish Care Register of Health.30 They found that a very large number of drugs intended from neurologic or psychiatric conditions were associated with an increased risk of BP.30 Drugs that particularly elevated the risk for BP included periciazine, melperone, haloperidol, biperiden, and risperidone. However, adjusted odd ratio for antidepressants such as escitalopram, venlafaxine or duloxetine were also significantly associated with BP.30
Corticosteroids-Induced Mood Changes
Superpotent topical corticosteroids are currently the gold standard treatment.1 However, they may be difficult to initiate because of the necessity of help at home (partner or other family members; home nurses). Different national health-care systems may not be always supportive enough in terms of costs. Oral corticosteroid can be the first choice of treatment in case of generalized disease.1 Nevertheless, psychiatric side effects from corticosteroids include mood disorders (mania, mixed states, depression), anxiety, panic disorders, delirium, agitation, insomnia or suicidal behaviour.31 Symptoms usually occur within the first 1 to 2 weeks after initiation and are dose related.31,32 The risk of depression may increase with prolonged or chronic exposure.31 The first step of treatment in case of psychiatric corticosteroid-induced symptoms is corticosteroid dose reduction or withdrawal.31 In a spirit of completeness, we wish to remind that both adrenal insufficiency33 and Cushing syndrome may present as depression.34
In conclusion, BP may impact the QoL of the patients with possible direct effect on anxiety or depression. However, the review of the literature shows a dearth in terms of publications on the topic. Depression and anxiety may be related to other comorbidities, such as dementia.35,36 BP induced by medications given to treat depression or anxiety should be kept in mind. Corticosteroids may be associated with acute psychiatric symptoms, including depression or anxiety.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Feliciani C, Joly P, Jonkman MF, et al. Management of bullous pemphigoid: the European Dermatology Forum consensus in collaboration with the European Academy of Dermatology and Venereology. Br J Dermatol. 2015;172(4):867–877. doi:10.1111/bjd.2015.172.issue-4
2. Schmidt E, Zillikens D. Pemphigoid diseases. Lancet. 2013;381(9863):320–332. doi:10.1016/S0140-6736(12)61140-4
3. Daniel BS, Murrell DF. Review of autoimmune blistering diseases: the Pemphigoid diseases. J Eur Acad Dermatol Venereol. 2019;33(9):1685–1694. doi:10.1111/jdv.v33.9
4. Försti AK, Jokelainen J, Timonen M, Tasanen K. Increasing incidence of bullous pemphigoid in Northern Finland: a retrospective database study in Oulu University Hospital. Br J Dermatol. 2014;171(5):1223–1226. doi:10.1111/bjd.13189
5. Joly P, Roujeau JC, Benichou J, et al.; Bullous Diseases French Study Group. A comparison of oral and topical corticosteroids in patients with bullous pemphigoid. N Engl J Med. 2002;346(5):321–327. doi:10.1056/NEJMoa011592
6. Parker SR, Dyson S, Brisman S, et al. Mortality of bullous pemphigoid: an evaluation of 223 patients and comparison with the mortality in the general population in the United States. J Am Acad Dermatol. 2008;59(4):582–588. doi:10.1016/j.jaad.2008.07.022
7. Joly P, Baricault S, Sparsa A, et al. Incidence and mortality of bullous pemphigoid in France. J Invest Dermatol. 2012;132(8):1998–2004. doi:10.1038/jid.2012.35
8. Gual A, Mascaró JM
9. Lee JH, Kim SC. Mortality of patients with bullous pemphigoid in Korea. J Am Acad Dermatol. 2014;71(4):676–683. doi:10.1016/j.jaad.2014.05.006
10. Kalinska-Bienias A, Lukowska-Smorawska K, Jagielski P, Kowalewski C, Wozniak K. Mortality in bullous pemphigoid and prognostic factors in 1st and 3rd year of follow-up in specialized centre in Poland. Arch Dermatol Res. 2017;309(9):709–719. doi:10.1007/s00403-017-1772-x
11. Terra JB, Potze WJ, Jonkman MF. Whole body application of a potent topical corticosteroid for bullous pemphigoid. J Eur Acad Dermatol Venereol. 2014;28(6):712–718. doi:10.1111/jdv.2014.28.issue-6
12. Sebaratnam DF, McMillan JR, Werth VP, Murrell DF. Quality of life in patients with bullous dermatoses. Clin Dermatol. 2012;30(1):103–107. doi:10.1016/j.clindermatol.2011.03.016
13. Zhao CY, Murrell DF. Outcome measures for autoimmune blistering diseases. J Dermatol. 2015;42(1):31–36. doi:10.1111/jde.2014.42.issue-1
14. Kalinska-Bienias A, Jakubowska B, Kowalewski C, Murrell DF, Wozniak K. Measuring of quality of life in autoimmune blistering disorders in Poland. Validation of disease - specific Autoimmune Bullous Disease Quality of Life (ABQOL) and the Treatment Autoimmune Bullous Disease Quality of Life (TABQOL) questionnaires. Adv Med Sci. 2017;62(1):92–96. doi:10.1016/j.advms.2016.07.002
15. Kouris A, Platsidaki E, Christodoulou C, et al. Quality of life, depression, anxiety and loneliness in patients with bullous pemphigoid. A case control study. An Bras Dermatol. 2016;91(5):601–603. doi:10.1590/abd1806-4841.20164935
16. DeGrazia TM, Liu Y, Bradley B, et al. LB1101 Itch and quality of life impact in atopic dermatitis vs bullous pemphigoid. J Invest Dermatol. 2019;139(9):b14. doi:10.1016/j.jid.2019.06.066
17. Sebaratnam DF, Hanna AM, Chee SN, et al. Development of a quality-of-life instrument for autoimmune bullous disease: the Autoimmune Bullous Disease Quality of Life questionnaire. JAMA Dermatol. 2013;149(10):1186–1191. doi:10.1001/jamadermatol.2013.4972
18. Försti AK, Jokelainen J, Ansakorpi H, et al. Psychiatric and neurological disorders are associated with bullous pemphigoid - a nationwide Finnish Care Register study. Sci Rep. 2016;6:37125. doi:10.1038/srep37125
19. Casas-de-la-Asunción E, Ruano-Ruiz J, Rodríguez-Martín AM, Vélez García-Nieto A, Moreno-Giménez JC. Association between bullous pemphigoid and neurologic diseases: a case-control study. Actas Dermosifiliogr. 2014;105(9):860–865. doi:10.1016/j.ad.2014.04.013
20. Tarazona MJ, Mota AN, Gripp AC, Unterstell N, Bressan AL. Bullous pemphigoid and neurological disease: statistics from a dermatology service. An Bras Dermatol. 2015;90(2):280–282. doi:10.1590/abd1806-4841.20153334
21. Kalińska-Bienias A, Kowalczyk E, Jagielski P, Bienias P, Kowalewski C, Woźniak K. The association between neurological diseases, malignancies and cardiovascular comorbidities among patients with bullous pemphigoid: case-control study in a specialized Polish center. Adv Clin Exp Med. 2019;28(5):637–642. doi:10.17219/acem/90922
22. Pankakoski A, Sintonen H, Ranki A, Kluger N. Comorbidities of bullous pemphigoid in a Finnish cohort. Eur J Dermatol. 2018;28(2):157–161. doi:10.1684/ejd.2018.3243
23. Bastuji-Garin S, Joly P, Lemordant P, et al., French Study Group for Bullous Diseases. Risk factors for bullous pemphigoid in the elderly: a prospective case-control study. J Invest Dermatol. 2011;131(3):637–643. doi:10.1038/jid.2010.301
24. Ren Z, Hsu DY, Brieva J, Silverberg NB, Langan SM, Silverberg JI. Hospitalization, inpatient burden and comorbidities associated with bullous pemphigoid in the U.S.A. Br J Dermatol. 2017;176(1):87–99. doi:10.1111/bjd.2017.176.issue-1
25. Försti AK, Huilaja L, Schmidt E, Tasanen K. Neurological and psychiatric associations in bullous pemphigoid-more than skin deep? Exp Dermatol. 2017;26(12):1228–1234. doi:10.1111/exd.13401
26. Stavropoulos PG, Soura E, Antoniou C. Drug-induced pemphigoid: a review of the literature. J Eur Acad Dermatol Venereol. 2014;28(9):1133–1140. doi:10.1111/jdv.2014.28.issue-9
27. Bastuji-Garin S, Joly P, Picard-Dahan C, et al. Drugs associated with bullous pemphigoid. A case-control study. Arch Dermatol. 1996;132(3):272–276. doi:10.1001/archderm.1996.03890270044006
28. Wijeratne C, Webster P. Risperidone and bullous pemphigoid. Am J Psychiatry. 1996;153(5):735.
29. Rault S, Grosieux-Dauger C, Verraes S, Bernardeau K, Durlach A, Bernard P. Bullous pemphigoid induced by fluoxetine. Br J Dermatol. 1999;141(4):755–756. doi:10.1046/j.1365-2133.1999.03130.x
30. Varpuluoma O, Jokelainen J, Försti AK, et al. Drugs used for neurologic and psychiatric conditions increase the risk for bullous pemphigoid: a case-control study. J Am Acad Dermatol. 2019;81(1):250–253. doi:10.1016/j.jaad.2019.02.017
31. Kenna HA, Poon AW, de Los Angeles CP, Koran LM. Psychiatric complications of treatment with corticosteroids: review with case report. Psychiatry Clin Neurosci. 2011;65(6):549–560. doi:10.1111/j.1440-1819.2011.02260.x
32. Brown ES, Khan DA, Nejtek VA. The psychiatric side effects of corticosteroids. Ann Allergy Asthma Immunol. 1999;83(6 Pt 1):
33. Virtanen R, Viikari J. Depression as a first symptom of Addison disease. Duodecim. 1998;114(14):1420–1421.
34. Young CA, Williams IR, MacFarlane IA. Unrecognised Cushing’s syndrome and adrenal suppression due to topical clobetasol propionate. Br J Clin Pract. 1991;45(1):61–62.
35. Enache D, Winblad B, Aarsland D. Depression in dementia: epidemiology, mechanisms, and treatment. Curr Opin Psychiatry. 2011;24(6):461–472. doi:10.1097/YCO.0b013e32834bb9d4
36. Ray S, Agarwal P. Depression and Anxiety in Parkinson Disease. Clin Geriatr Med. 2020;36(1):93–104. doi:10.1016/j.cger.2019.09.012
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.