Back to Journals » Journal of Pain Research » Volume 13
Depression and Anxiety as Moderators of the Pain-Social Functioning Relationship in Youth with Sickle Cell Disease
Authors Valrie C ![]() , Floyd A, Sisler I, Redding-Lallinger R
, Floyd A, Sisler I, Redding-Lallinger R ![]() , Fuh B
, Fuh B
Received 11 November 2019
Accepted for publication 19 March 2020
Published 8 April 2020 Volume 2020:13 Pages 729—736
DOI https://doi.org/10.2147/JPR.S238115
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor E Alfonso Romero-Sandoval
Cecelia Valrie,1,2 Alfonso Floyd,1 India Sisler,3 Rupa Redding-Lallinger,4 Beng Fuh5
1Department of Psychology, Virginia Commonwealth University, Richmond, VA, USA; 2Institute for Inclusion, Inquiry, and Innovation, Virginia Commonwealth University, Richmond, VA, USA; 3Department of Pediatrics, Virginia Commonwealth University, Richmond, VA, USA; 4Departments of Pediatrics and Internal Medicine, University of North Carolina at Chapel Hill, Chapel Hill, NC, USA; 5Department of Pediatrics, East Carolina University, Greenville, NC, USA
Correspondence: Cecelia Valrie
Department of Psychology, Virginia Commonwealth University, 806 W Franklin St, Richmond, VA 23284 Tel +1 804 827 1562
Fax +1 804 828 2237
Email [email protected]
Purpose: Youth with sickle cell disease (SCD), a genetic disorder of red blood cells, may experience acute pain episodes lasting 2 to 3 days on average. While existing research has demonstrated associations between SCD pain and poor social functioning in youth with SCD, there are no data on whether symptoms of depression and anxiety modify the relationship between pain and functional outcomes in pediatric pain populations. It was hypothesized that more symptoms of depression and anxiety would exacerbate the relationship between high pain and poor social functioning in youth with SCD.
Patients and Methods: We conducted a cross-sectional study of 114 youth with SCD and their guardians assessing the youth’s pain, social functioning, and symptoms of depression and anxiety.
Results: Analyses indicated that elevated levels of depressive symptoms were related to poorer self-reported interpersonal skills. More anxiety symptoms were related to better guardian-reported social skills and weakened the relationship between high pain frequency and poor self-reported interpersonal skills.
Conclusion: Findings build on previous work supporting the need for multidisciplinary approaches to care for youth with SCD who experience pain, and provide rationale for future studies to investigate the direct and possible moderating effects of depression and anxiety symptoms on other functional outcomes in youth with SCD and other pediatric pain populations.
Keywords: sickle cell, pain, children, adolescents, mental health, functional outcomes
Introduction
Sickle cell disease (SCD) is a genetic disorder of red blood cells that affects approximately 100,000 Americans and millions worldwide.1 Pain due primarily to vaso-occlusion is the hallmark complication of SCD. Youth with SCD may experience acute pain episodes lasting about 2 to 3 days on average that may transition to chronic pain in late adolescence. Youth with SCD are also at risk of poor social functioning, as evidenced by several studies that have indicated that having SCD is linked to feelings of social isolation,2 a lack of peer relationships,3,4 and poor social skills and social competence in youth.5–9 In addition, pain has been linked to poor social functioning in youth with SCD.3,10 A study of 327 children with the HBSS genotype of SCD linked high pain frequency to more reported problems in school, higher rates of shyness and loneliness, increased victimization by peers, and less friendships.11 This relationship may be due to SCD pain resulting in increased school absences and reduced participation in afterschool activities, which may limit opportunities for youth with SCD to develop their social skills.12,13
The biopsychosocial model of pediatric pain by Valrie and colleagues14 proposes that pain interacts with other factors, such as mood, to influence functional outcomes. A systematic review found strong evidence for a relationship between high pain frequency and more symptoms of depression and anxiety in youth with SCD, and findings also indicated that more symptoms of depression and anxiety were related to high pain-related impairment.15 In addition, a study of adolescents with SCD found that high levels of stress and negative mood were associated with increased school absences and decreased participation in everyday social and home activities (Gil et al 2003), When youth who experience more symptoms of depression and anxiety have a SCD pain episode, it could make it harder for them to cope effectively with the pain, leading to increased impairments in social functioning. This is consistent with findings from a study that indicated that youth with SCD who experienced vaso-occlusive pain were at a greater risk for medical complications during depressive periods, as they had lower pain thresholds and impaired pain-coping abilities.16
Adult pain studies have indicated that more depressive symptoms increase the relationship between high pain and poor functional outcomes.17,18 Findings from a study of 42 adolescents with SCD indicated that depression and anxiety symptoms do not mediate the association between pain frequency and functional outcomes (ie, physical functioning and self-esteem).19 However, there are no data on whether symptoms of depression and anxiety modify the relationship between pain and functional outcomes in pediatric pain populations. The current study aims to begin to address this gap by investigating whether symptoms of depression and anxiety moderate the relationship between pain and social functioning in youth with SCD. It was hypothesized that more symptoms of depression and anxiety would exacerbate the relationship between high pain and poor social functioning in youth with SCD.
Patients and Methods
We conducted a cross-sectional study assessing pain, social functioning, and symptoms of depression and anxiety. Youth with SCD and their guardians were recruited from three regional pediatric SCD clinics in the southeastern United States during the youth’s scheduled appointments. The dyads were recruited between 2011 and 2015. Of the 154 youth who were eligible for the study, 123 (80%) completed interviews, 12 (8%) declined to be interviewed, and 19 (12%) could not be reached to be scheduled for an interview. In addition, data from 9 dyads were not used: 2 dyads did not have complete social functioning data, 4 youth meet criteria for chronic SCD pain (eg, reporting pain episodes on at least 50% of days in the last year),20 and 3 did not have complete pain data. Youth with evidence of chronic SCD pain were deleted because the relationships between the variables being studied may be different if the pain is chronic.
The final sample size was 114 youth and their guardians. Participants were included in the study if they were between the ages of 8 to 17 years, diagnosed with SCD, experienced at least one vaso-occlusive pain episode within the past year, and were English speaking. Participants were excluded if they had a comorbid pain diagnosis, neurological impairment that could impede completion of the survey questionnaires, were receiving blood transfusion therapy, or were experiencing an acute medical event at the time of recruitment. The study procedure was approved and monitored by the institutional review boards at Virginia Commonwealth University, East Carolina University, and the University of North Carolina at Chapel Hill. Prior to the study, guardians provided consent, and youth provided assent for participation in the study. The guardian consent and youth assent forms were written and informed by the Declaration of Helsinki, and the study was conducted in accordance with the Declaration of Helsinki. Following consent and assent, youth and guardian participants completed the study measures, and each received a $20.00 gift card as compensation.
Measures
Demographic and Medical Information
Guardians reported on their youth’s age in years and sex. Information indicating whether youth participants were on currently prescribed hydroxyurea and their SCD genotypes were extracted from their electronic medical records. Genotypes were used as an indicator of SCD severity, with HbSS and HbS/β0 indicating more severe disease, while HbSC, HbS/β+, and other genotypes indicating moderate severity.
Pain
Guardians reported on the youth’s pain frequency, duration, and severity over the past year using the Structured Pain Interview (SPI).21 Pain frequency was defined as the number of SCD pain episodes (ie, pain due to SCD that lasted at least 20 min) the youth experienced in the past year. Pain duration was defined as the average duration of these pain episodes, and pain severity was the average rating of the pain episodes on a 11-point Likert scale from “no pain” (0) to “pain as bad as it can be” (10). The SPI has been validated for youth with SCD and has been found to have acceptable interrater and test–retest reliability over a 9- to 12-month period.21
Social Functioning
Social functioning was assessed using the parent-report social skills subscale and the self-report interpersonal relations subscale of the Behavior Assessment System for Children, Second Edition (BASC-2).22 The BASC-2 is widely used in mental health and educational settings, and has been normed on a large representative sample. The combined gender norms were used for the BASC-2 scoring. The social skills subscale measures the youth’s ability to socially engage with others in comparison to his/her peers. The interpersonal relations subscale measures the youth’s ability to develop and sustain relationships with peers, family members, and teachers. Higher scores indicate better social adjustment. Scores between 31 and 40 were considered “at risk”, and those at 30 or below were considered clinically significant for maladaptation.
Depression and Anxiety Symptoms
Internalizing symptoms were assessed using the youth self-reported depression and anxiety subscales of the BASC-2.22 A T score of less than 60 is considered not clinically concerning, while scores between 60 and 69 are considered “at risk” for emotional maladjustment, and scores of 70 and above are considered “clinically significant.”
Proposed Analysis
All data were analyzed using SAS 9.4 for Windows. Descriptive statistics for all of the variables of interest were calculated: means, SDs, and ranges for continuous variables and percentages for categorical variables. Correlations and t-tests were calculated to assess the relationships between possible covariates for the subsequent analyses (ie, age, sex, SCD genotype severity, and hydroxyurea use) and social functioning. Possible covariates that were moderately related to social functioning (p < 0.10) were retained for subsequent regression analyses. To examine whether depression and anxiety symptoms moderate the relationship between pain and social functioning, a series of regression models were calculated predicting the two social functioning variables using the pain variables, symptoms of depression and anxiety, and the interactions between the pain variables and symptoms of depression and anxiety. To decrease collinearity between the variables and interaction terms, the pain variables and symptoms of depression and anxiety were centered prior to calculating the interaction terms. We probed significant interactions (p < 0.05) using moderation models run using Hayes’ PROCESS macro in SAS.
For guardian-reported social skills, the skew of 0.08 and kurtosis of −0.63 were in the acceptable ranges (skew between −1 and +1 and kurtosis between −2 and +2). For self-reported interpersonal skills, the scores appeared skewed (skew = −1.86) and to have high kurtosis (kurtosis = 3.26), which may have impacted residuals associated with the regression model predicting self-reported interpersonal skills. As an assumption of linear regressions is that their residuals are normally distributed, we examined the skew and kurtosis for the residuals as well as the QQ plots for each of the regression models calculated. The skew and kurtosis of the residuals for the models were found to be in the acceptable range, and the QQ plots were found to be acceptable. Thus, the regression results were presented without transformations.
Results
Table 1 provides demographic, clinical, pain, psychological symptoms, and social functioning data. The average internalizing symptoms and social functioning scores were in the not clinically concerning range. However, approximately 11% of the sample scored in the at-risk or clinically significant range for depression symptoms, 22% for anxiety symptoms, 20% for guardian-reported social skills, and 9% for self-reported interpersonal relations. Notably, pain frequency, duration, and severity were not significantly correlated (p > 0.05), with correlation coefficients ranging from −0.09 to 0.02. Pain frequency (skew = 2.79) and pain duration (skew = 8.72) were highly skewed, while pain severity (skew = −0.41) was not. Notably, there are no assumptions in linear regression models about the distribution of independent variables, and without clear theoretical reasons, it is not recommended to remove observations as they may lead to important findings. Also, we decided to not transform the data as each of the pain variables has a clear meaning, which aids in interpreting the data.
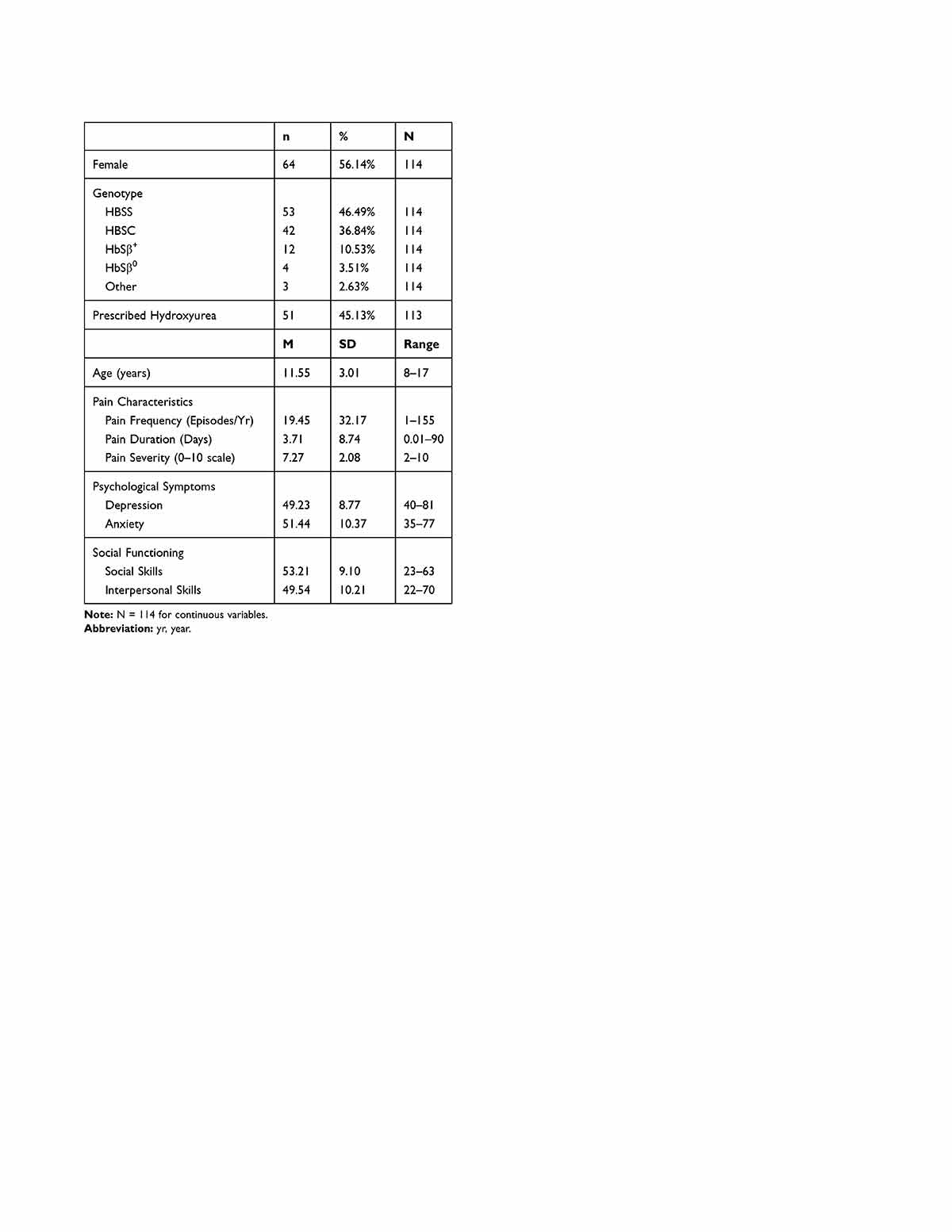 |
Table 1 Demographic, Clinical, Pain, Psychological, and Social Functioning Data |
Correlations and t-tests were calculated examining the relationships between possible covariates and social functioning. Age was not correlated with guardian or self-reported social functioning scores at the p < 0.10 level. Table 2 provides t-test results investigating for differences in social functioning based on sex, SCD genotype severity, and whether hydroxyurea is prescribed. Notably, guardians tended to rate females higher than males on social skills, while female youth self-rated themselves significantly lower than male youth on interpersonal skills. Based on these analyses, the subsequent regression models predicting guardian-reported social skills and self-reported interpersonal skills controlled for sex and SCD genotype.
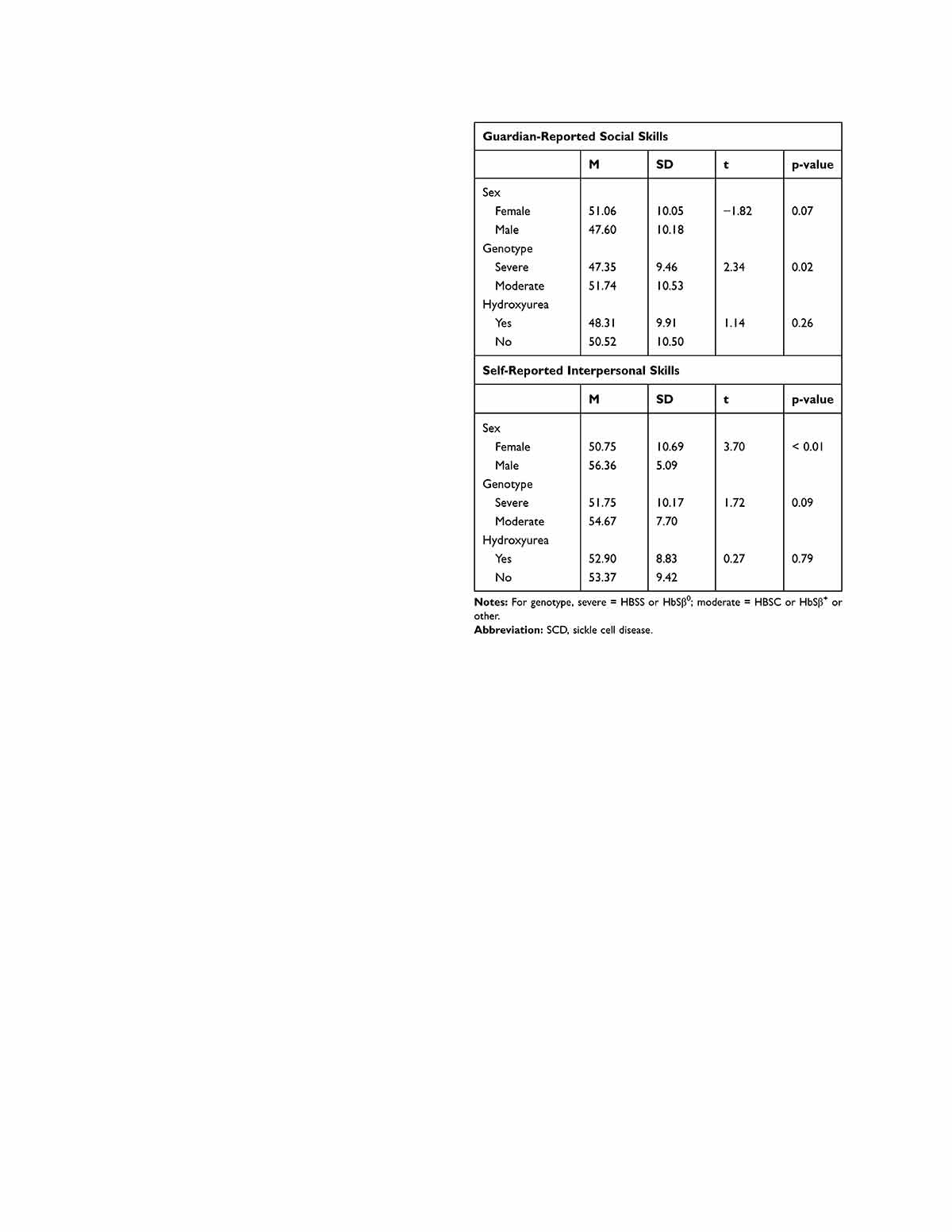 |
Table 2 Comparison of Social Functioning by Sex, SCD Genotype, and Hydroxyurea Use |
Multiple regression models were then run to predict guardian-reported social skills and self-reported interpersonal skills (See Table 3). The model predicting guardian-reported social skills was significant (F = 2.05, p = 0.02) and accounted for 11% of the variance. Being male, having a more severe SCD genotype, and reporting fewer anxiety symptoms were uniquely related to poorer guardian-reported social skills. The model predicting self-reported interpersonal skills was significant (F = 4.98, p <0.01) and accounted for 31% of the variance. Being female, high pain severity, and more symptoms of depression were uniquely related to poorer self-reported interpersonal skills. Also, the interaction between pain frequency and anxiety symptoms was a significant predictor. Simple slopes analyses to probe the interaction between pain frequency and anxiety symptoms revealed that high pain frequency was not significantly related to poorer self-reported interpersonal skills at low levels anxiety symptoms (p = 0.08), medium (p = 0.29), or high levels of anxiety symptoms (p = 0.24). However, the pattern of findings indicated that as anxiety symptoms increase, the relationship between high pain frequency and poor self-reported interpersonal skills weakens (see Figure 1).
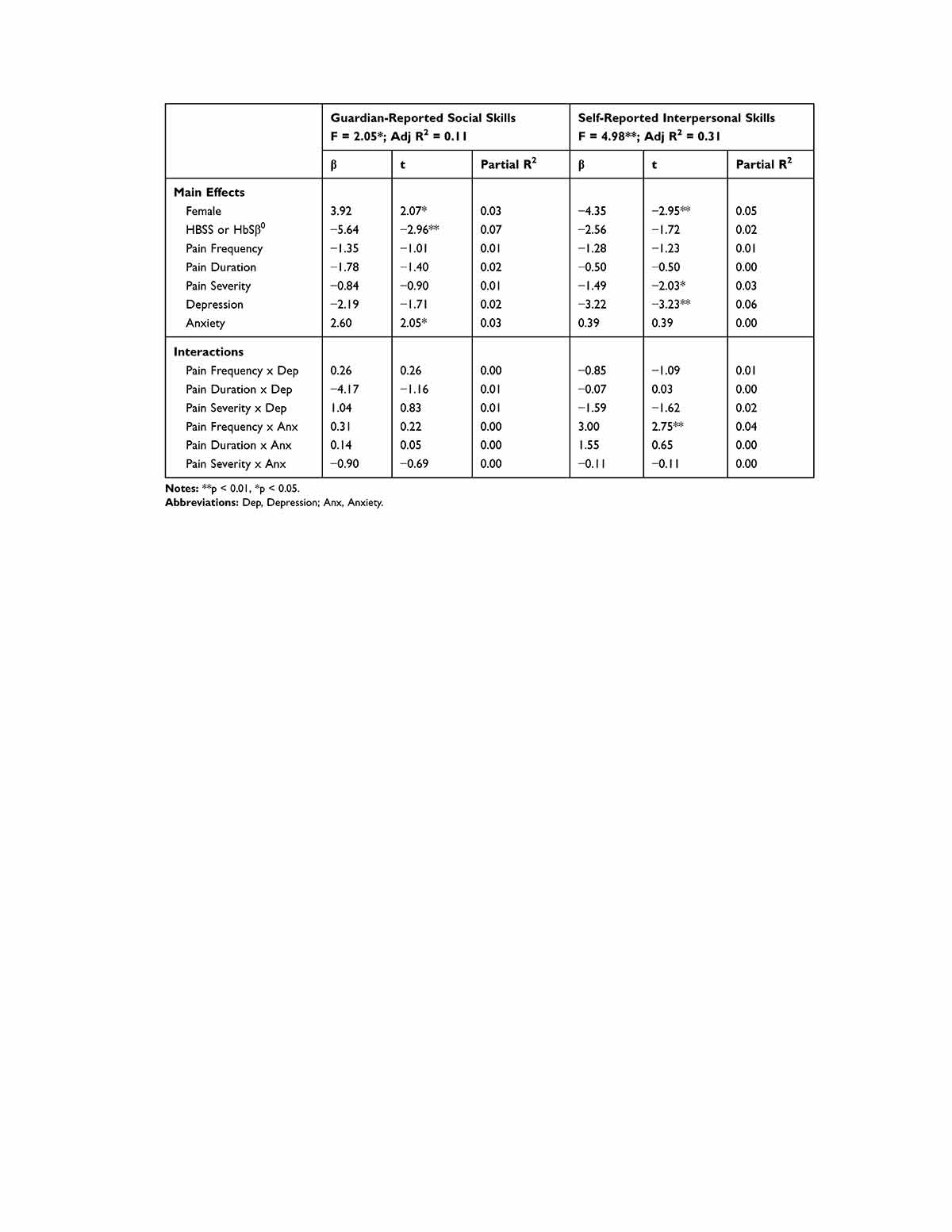 |
Table 3 Regression Models Predicting Social Functioning (N = 114) |
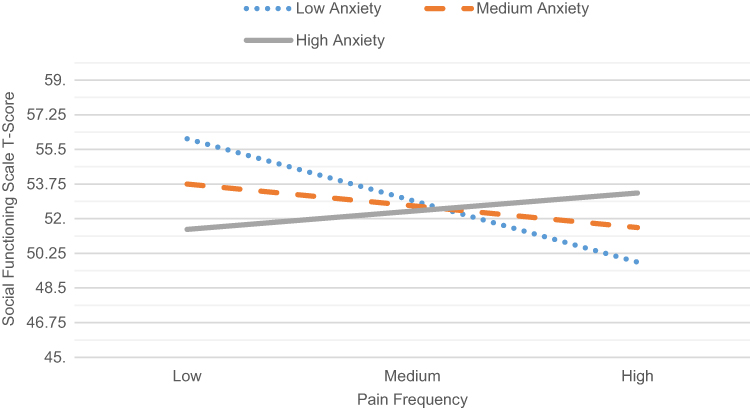 |
Figure 1 Interaction between pain frequency and self-reported interpersonal skills at varying levels of anxiety symptoms. |
Discussion
This is the first study to examine whether symptoms of depression and anxiety modify the relationship between pain and functional outcomes in youth with SCD. The average level of depressive and anxiety symptoms observed in the sample was in the non-clinical range, with about 11% to 22% of the youth scoring in the at-risk or clinically significant ranges. These data are consistent with previous studies that indicated depression rates in youth with SCD ranging from 4% to 75%, and anxiety ranging from 8% to 41%.15 However, despite the majority of our sample reporting subclinical levels of depression and anxiety symptoms, results still indicated that these symptoms influenced the relationship between pain and social functioning.
Inconsistent with our hypothesis, depressive symptoms did not modify the relationship between pain and social functioning. Notably, more depressive symptoms were related to poor self-reported interpersonal skills over and above the influence of pain. Depressed youth may be more likely to socially isolate themselves; thus, removing themselves from opportunities to develop their social skills and gain valuable social support. This explanation is supported by study findings that have associated high negative mood to increased school absences and decreased participation in social activities in adolescents with SCD.23 Research also indicates that symptoms of depression are associated with disruptions in social skill development in healthy children and adolescents, particularly in their ability to establish and maintain satisfying relationships with their peers.24 These findings are, however, inconsistent with study findings indicating that more symptoms of depression appear to bolster the association between high pain and poor functional outcomes, such as medical complications in youth with SCD,16 functional limitations in older adults,17 and non-medical use of opioids in adults.18 Overall, these findings support the need for systematic assessment and treatment of symptoms of depression as part of clinical care for youth with SCD.
Also, inconsistent with our hypothesis, more anxiety symptoms weakened the relationship between high pain frequency and poor self-reported interpersonal skills. This is the first study to examine whether anxiety symptoms moderate the relationships between pain and functional outcomes in pediatric pain patients. Findings also indicated that more symptoms of anxiety were related to better guardian-reported social skills. It may be that youth with more symptoms of anxiety are more attuned to others’ perceptions and responses to them, which impacts their social skill development. Youth with higher levels of anxiety may also be more likely to seek social support in response to their pain, and thus, seek out more social interactions and develop stronger social skills to better access support. It could also be that youth with less symptoms of anxiety may be less vigilant in attending to signs of impending pain episodes, and thus, react more strongly when pain episodes do occur. More research is needed to elucidate how symptoms of anxiety are associated with social functioning in youth with SCD. Notably, the measure used in the current study was focused on assessing general anxiety symptoms, but youth may have interpreted the questions as being focused on their SCD specific symptoms. Future research should focus on specific worries that youth with SCD may experience, and examine how different types of anxiety symptoms may be associated with functional outcomes in this population.
Sex was related to guardian-reported and self-reported social functioning; however, the findings conflicted based upon reporter. Specifically, guardians reported that males were at higher risk for poor social functioning than females; however, males were more likely to self-report better social functioning than females. The findings relating being female to poor social competence in youth with SCD are consistent with prior studies that indicated females are rated as less socially competent by their peers and teachers when compared to their healthy peers.7,8 However, there has been no prior research relating being male to poor social functioning in this population. Overall, our findings are contradictory and suggest a need for more research to explore the relationship between sex and social functioning for youth with SCD.
Limitations of our study include that pain patterns were assessed retrospectively and via guardian-report. Pain reports may have been influenced by recall bias due to deficits in memory or caregiver distress.25 Also, pain is a subjective experience; thus, guardian-report may have led to underestimates of youth pain as it would be reflective of guardian observed pain behaviors and pain as reported to the guardian by the youth. However, parent-proxy reports for pain experiences are commonly used and have been validated for pediatric pain populations,26,27 and the measure used in the current study has been validated for youth with SCD and used across multiple studies,28–31 allowing for comparison of findings. Still, future studies should incorporate youth reports of their pain. Lastly, the current study exclusively focused on negative emotions. This is in contrast to a growing body of research indicating positive affect is associated with reduced pain and better functional outcomes in pain patients (eg, reduced sleep disturbance and physical dysfunction).32 Positive affect has also been found to buffer the effects of pain on general functioning and well-being in patients with rheumatoid arthritis and other persistent pain conditions. Future research is needed to examine positive affect as a moderator of the relationships between pediatric SCD pain and functional outcomes.
Despite these limitations, the current study offers initial evidence for the influence of symptoms of depression and anxiety on the relationship between pediatric pain and functional outcomes. It builds on previous work supporting the need for multidisciplinary approaches to care for youth with SCD who experience pain.33,34 It also provides support for the applicability of Valrie’s biopsychosocial model of pediatric pain14 for understanding the experiences of youth with SCD, and rationale for future studies to investigate the possible moderating role of depression and anxiety symptoms on other functional outcomes in youth with SCD and other pediatric pain populations.
Conclusion
More depressive symptoms were related to poor self-reported interpersonal skills. In contrast, more anxiety symptoms were related to guardian-reported social skills and weakened the relationship between high pain frequency and poor self-reported interpersonal skills. Future studies are needed to fully elucidate the direct or moderating effects of depression and anxiety symptoms on social functioning and other functional outcomes in youth with SCD, and how negative and positive affect may influence associations between pain and functional outcomes in this population and other pediatric pain populations.
Acknowledgments
The authors thank the youth with SCD and their guardians for their participation in this research study. This work was supported by funding from the National Heart, Lung, and Blood Institute of the National Institutes of Health (Grant number NIHK01HL103155), and the American Society of Hematology.
Disclosure
Cecelia Valrie reports grants from the National Institute of Health and American Society of Hematology, during the conduct of the study. The authors report no other conflicts of interest in this work.
References
1. Hassell KL. Population estimates of sickle cell disease in the U.S. Am J Prev Med. 2010;38(4):S512–521. doi:10.1016/j.amepre.2009.12.022
2. PA F, King S, Stinson JN, McGrath PJ, MacDonald AJ, Chambers CT. Social functioning and peer relationships in children and adolescents with chronic pain: a systematic review. Pain Res Manag. 2010;15(1):27–41. doi:10.1155/2010/820407
3. Erskine R. Adolescent boys with sickle cell disease: a qualitative study. Clin Child Psychol Psychiatry. 2012;17(1):17–31. doi:10.1177/1359104511399843
4. Noll RB, Kiska R, Reiter-Purtill J, Gerhardt CA, Vannatta K. A controlled, longitudinal study of the social functioning of youth with sickle cell disease. Pediatrics. 2010;125(6):e1453–1459. doi:10.1542/peds.2009-2996
5. Hensler M, Wolfe K, Lebensburger J, et al. Social skills and executive function among youth with sickle cell disease: a preliminary investigation. J Pediatr Psychol. 2014;39(5):493–500. doi:10.1093/jpepsy/jst138
6. Noll RB, Reiter-Purtill J, Vannatta K, Gerhardt CA, Short A. Peer relationships and emotional well-being of children with sickle cell disease: a controlled replication. Child Neuropsychol. 2007;13(2):173–187. doi:10.1080/09297040500473706
7. Noll RB, Ris MD, Davies WH, Bukowski WM, Koontz K. Social interactions between children with cancer or sickle cell disease and their peers: teacher ratings. J Dev Behav Pediatr. 1992;13(3):187–193. doi:10.1097/00004703-199206000-00006
8. Noll RB, Vannatta K, Koontz K, Kalinyak K, Bukowski WM, Davies WH. Peer relationships and emotional well-being of youngsters with sickle cell disease. Child Dev. 1996;67(2):423–436. doi:10.1111/j.1467-8624.1996.tb01743.x
9. Rodrigue JR, Streisand R, Banko C, Kedar A, Pitel PA. Social functioning, peer relations, and internalizing and externalizing problems among youth with sickle cell disease. Children’s Health Care. 1996;25(1):37–52. doi:10.1207/s15326888chc2501_4
10. Wagner JL, Connelly M, Brown RT, Taylor LC, Rittle C, Wall-Cloues B. Predictors of social anxiety in children and adolescents with sickle cell disease. J Clin Psychol Med Settings. 2004;11(4):243–252. doi:10.1023/B:JOCS.0000045344.05747.d3
11. Barbarin OA, Whitten CF, Bonds SM. Estimating rates of psychosocial problems in urban and poor children with sickle cell anemia. Health Soc Work. 1994;19(2):112–119. doi:10.1093/hsw/19.2.112
12. Shapiro BS, Dinges DF, Orne EC, et al. Home management of sickle cell-related pain in children and adolescents: natural history and impact on school attendance. Pain. 1995;61(1):139–144. doi:10.1016/0304-3959(94)00164-A
13. Telfair J. Factors in the long term adjustment of children and adolescents with sickle cell disease: conceptualizations and review of the literature. J Health Soc Policy. 1994;5(3–4):69–96. doi:10.1300/J045v05n03_06
14. Valrie CR, Bromberg MH, Palermo T, Schanberg LE. A systematic review of sleep in pediatric pain populations. J Dev Behav Pediatr. 2013;34(2):120–128. doi:10.1097/DBP.0b013e31827d5848
15. Reader SK, Rockman LM, Okonak KM, Ruppe NM, Keeler CN, Kazak AE. Systematic review: pain and emotional functioning in pediatric sickle cell disease. J Clin Psychol Med Settings. 2019. doi:10.1007/s10880-019-09647-x
16. Unal S, Toros F, Kutuk MO, Uyaniker MG. Evaluation of the psychological problems in children with sickle cell anemia and their families. Pediatr Hematol Oncol. 2011;28(4):321–328. doi:10.3109/08880018.2010.540735
17. Ko KT, Yu SH, Lee CY, Tseng HY, Chiu YF, Hsiung CA. Moderating effect of depression on the association between pain and activities of daily living in older adults. Psychogeriatrics. 2018;18(5):379–387. doi:10.1111/psyg.12332
18. Mason MJ, Golladay G, Jiranek W, et al. Depression moderates the relationship between pain and the nonmedical use of opioid medication among adult outpatients. J Addict Med. 2016;10(6):408–413. doi:10.1097/ADM.0000000000000253
19. Barakat LP, Patterson CA, Daniel LC, Dampier C. Quality of life among adolescents with sickle cell disease: mediation of pain by internalizing symptoms and parenting stress. Health Qual Life Outcomes. 2008;6(1):60. doi:10.1186/1477-7525-6-60
20. Dampier C, Palermo TM, Darbari DS, Hassell K, Smith W, Zempsky W. AAPT diagnostic criteria for chronic sickle cell disease pain. J Pain. 2017;18(5):490–498. doi:10.1016/j.jpain.2016.12.016
21. Gil KM, Williams DA, Thompson RJ
22. Reynolds C, Kamphaus R. BASC-2 Behavior Assessment for Children Manual. Circle Pines, MN: American Guidance Service. 2004.
23. Gil KM, Carson JW, Porter LS, et al. Daily stress and mood and their association with pain, health-care use, and school activity in adolescents with sickle cell disease. J Pediatr Psychol. 2003;28(5):363–373. doi:10.1093/jpepsy/jsg026
24. Segrin C. Social skills deficits associated with depression. Clin Psychol Rev. 2000;20(3):379–403. doi:10.1016/S0272-7358(98)00104-4
25. Pannucci CJ, Wilkins EG. Identifying and avoiding bias in research. Plast Reconstr Surg. 2010;126(2):619–625. doi:10.1097/PRS.0b013e3181de24bc
26. Irwin DE, Gross HE, Stucky BD, et al. Development of six PROMIS pediatrics proxy-report item banks. Health Qual Life Outcomes. 2012;10(1):22. doi:10.1186/1477-7525-10-22
27. Singh A, DasGupta M, Simpson PM, Panepinto JA. Use of the new pediatric PROMIS measures of pain and physical experiences for children with sickle cell disease. Pediatr Blood Cancer. 2019;66(5):e27633. doi:10.1002/pbc.27633
28. Gil KM, Anthony KK, Carson JW, Redding-Lallinger R, Daeschner CW, Ware RE. Daily coping practice predicts treatment effects in children with sickle cell disease. J Pediatr Psychol. 2001;26(3):163–173. doi:10.1093/jpepsy/26.3.163
29. Schatz J, Schlenz AM, McClellan CB, et al. Changes in coping, pain, and activity after cognitive-behavioral training: a randomized clinical trial for pediatric sickle cell disease using smartphones. Clin J Pain. 2015;31(6):536–547. doi:10.1097/AJP.0000000000000183
30. Schlenz AM, Schatz J, Roberts CW. Examining biopsychosocial factors in relation to multiple pain features in pediatric sickle cell disease. J Pediatr Psychol. 2016;41(8):930–940. doi:10.1093/jpepsy/jsw003
31. Valrie CR, Gil KM, Redding-Lallinger R, Daeschner C. The influence of pain and stress on sleep in children with sickle cell disease. Children’s Health Care. 2007;36(4):335–353. doi:10.1080/02739610701601353
32. Hanssen MM, Peters ML, Boselie JJ, Meulders A. Can positive affect attenuate (persistent) pain? State of the art and clinical implications. Curr Rheumatol Rep. 2017;19(12):80. doi:10.1007/s11926-017-0703-3
33. Noronha SA, Sadreameli SC, Strouse JJ. Management of sickle cell disease in children. South Med J. 2016;109(9):495–502. doi:10.14423/SMJ.0000000000000523
34. Balsamo L, Shabanova V, Carbonella J, et al. Improving care for sickle cell pain crisis using a multidisciplinary approach. Pediatrics. 2019;143(5):e20182218. doi:10.1542/peds.2018-2218
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.