Back to Journals » Journal of Pain Research » Volume 14
Denying the Truth Does Not Change the Facts: A Systematic Analysis of Pseudoscientific Denial of Complex Regional Pain Syndrome
Authors Bharwani KD ![]() , Kersten AB, Stone AL, Birklein F, Bruehl S, Dirckx M, Drummond PD
, Kersten AB, Stone AL, Birklein F, Bruehl S, Dirckx M, Drummond PD ![]() , Gierthmühlen J, Goebel A, Knudsen L, Huygen FJPM
, Gierthmühlen J, Goebel A, Knudsen L, Huygen FJPM
Received 26 June 2021
Accepted for publication 3 September 2021
Published 27 October 2021 Volume 2021:14 Pages 3359—3376
DOI https://doi.org/10.2147/JPR.S326638
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Robert Twillman
KD Bharwani,1,* AB Kersten,1,* AL Stone,2 F Birklein,3 S Bruehl,2 M Dirckx,1 PD Drummond,4 J Gierthmühlen,5 A Goebel,6 L Knudsen,7 FJPM Huygen1
1Center for Pain Medicine, Department of Anesthesiology, Erasmus MC University Medical Center, Rotterdam, the Netherlands; 2Department of Anesthesiology, Vanderbilt University Medical Center, Nashville, TN, USA; 3Department of Neurology, University Medical Center of the Johannes Gutenberg University Mainz, Mainz, Germany; 4Discipline of Psychology, College of Science, Health, Engineering and Education, Murdoch University, Perth, WA, Australia; 5Division of Neurological Pain Research and Therapy, Department Neurology, University Hospital of Schleswig-Holstein, Campus Kiel, Kiel, Germany; 6Director of the Pain Research Institute Reader in Pain Medicine, University of Liverpool Honorary Consultant in Pain Medicine, Walton Centre NHS Foundation Trust, Liverpool, UK; 7The National Rehabilitation Centre for Neuromuscular Diseases, Aarhus, Denmark
*These authors contributed equally to this work
Correspondence: KD Bharwani Tel +31107040704
Email [email protected]
Purpose: Several articles have claimed that complex regional pain syndrome (CRPS) does not exist. Although a minority view, it is important to understand the arguments presented in these articles. We conducted a systematic literature search to evaluate the methodological quality of articles that claim CRPS does not exist. We then examined and refuted the arguments supporting this claim using up-to-date scientific literature on CRPS.
Methods: A systematic search was conducted in MEDLINE, EMBASE and Cochrane CENTRAL databases. Inclusion criteria for articles were (a) a claim made that CRPS does not exist or that CRPS is not a distinct diagnostic entity and (b) support of these claims with subsequent argument(s). The methodological quality of articles was assessed if possible.
Results: Nine articles were included for analysis: 4 narrative reviews, 2 personal views, 1 letter, 1 editorial and 1 case report. Seven points of controversy were used in these articles to argue that CRPS does not exist: 1) disagreement with the label “CRPS”; 2) the “unclear” pathophysiology; 3) the validity of the diagnostic criteria; 4) CRPS as a normal consequence of immobilization; 5) the role of psychological factors; 6) other identifiable causes for CRPS symptoms; and 7) the methodological quality of CRPS research.
Conclusion: The level of evidence for the claim that CRPS does not exist is very weak. Published accounts concluding that CRPS does not exist, in the absence of primary evidence to underpin them, can harm patients by encouraging dismissal of patients’ signs and symptoms.
Keywords: complex regional pain syndrome, pathophysiology, treatment, chronic pain
Introduction
Complex regional pain syndrome (CRPS) is defined by the International Association for the Study of Pain as
a syndrome characterized by a continuing (spontaneous and/or evoked) regional pain that is seemingly disproportionate in time or degree to the usual course of pain after trauma or other lesion. The pain is regional (not in a specific nerve territory or dermatome) and usually has a distal predominance of abnormal sensory, motor, sudomotor, vasomotor, edema, and/or trophic findings.1
Reported incidence rates vary between 5.5 and 26.2 per 100.000 person-years and women are more often affected than men.2,3 A definitive pathophysiology of CRPS is still not completely clear, but knowledge regarding its pathophysiological mechanisms has progressed significantly in recent years. Despite these advances, there are still voices questioning the legitimacy of this condition.
In the past few years, several articles have been published that claim that CRPS does not exist as a distinct clinical and diagnostic entity. While the large majority of the scientific literature provides evidence supporting the existence of CRPS, it is nonetheless important to understand the arguments and concerns that are presented in these critical articles.
There is a risk that published accounts concluding that CRPS does not exist, despite the absence of primary evidence to underpin these claims, may harm patients by encouraging dismissal of patients’ CRPS signs and symptoms. Consequently, vulnerable patients might feel invalidated and misunderstood, appropriate treatment withheld and recovery jeopardized. Therefore, we propose that to the extent that these critical claims are inaccurate or misleading, such claims should be challenged to mitigate their potential adverse effects. In addition, understanding the basis of these critical arguments and concerns could potentially help guide future research and support improvements in diagnosis and therapy protocols.
To our knowledge, there has been no prior integration of the critical literature that denies CRPS as a diagnostic entity. Therefore, we conducted a systematic search of the literature to evaluate the methodological quality of articles that claim CRPS is not a legitimate condition. Based on the results of this literature search, we then employed an empirical approach to analyze and refute the arguments used to support the claim that CRPS does not exist.
Methods
With the help of an experienced biomedical information specialist, we searched the MEDLINE, EMBASE and Cochrane CENTRAL databases from inception until the 4th of July 2019 for English-language articles debating the existence of CRPS. The search strategies can be found in Appendix 1. All article types were included in this review.
Two investigators (AK, KB) independently selected articles based on title and abstract. The full-text of the identified articles was then screened, and articles were selected for inclusion in this review if a) a claim was being made that CRPS does not exist or that CRPS is not a distinct diagnostic entity, and if b) the claim was subsequently supported by arguments or if controversies were described. When there was disagreement between the two investigators regarding the inclusion of an article, a third investigator was consulted (FH). The reference lists of included articles were also screened for relevant studies.
The two investigators further assessed the quality of the included articles by examining the study designs. The methodological strength of included narrative reviews was scored using the Scale for the Assessment of Narrative Review Articles (SANRA). The following elements are included in the SANRA scale: the importance of the article, the aim, the literature search, referencing, scientific reasoning and the presentation of data. Scores were compared and consensus was reached on the final scores.
Finally, the two investigators summarized the arguments used to support the claim that CRPS does not exist and identified seven main points of controversy raised across the identified articles.
Results
Search Results
Our search yielded 1048 articles, which were screened on title and abstract. This resulted in 13 articles that were eligible for full-text screening. The reference lists of the 13 articles were screened, and 3 additional articles were found which were also screened on full-text. Of the 16 articles assessed on full-text, 9 articles were included in this review and seven articles were excluded: one article because it was written in Dutch,4 one because it was an abstract for a conference5 and five articles because they did not primarily focus on the claim that CRPS does not exist6–10 (see Figure 1). The 9 included articles consisted of 4 narrative reviews, 2 personal views, 1 letter, 1 editorial and 1 case report (see Table 1).
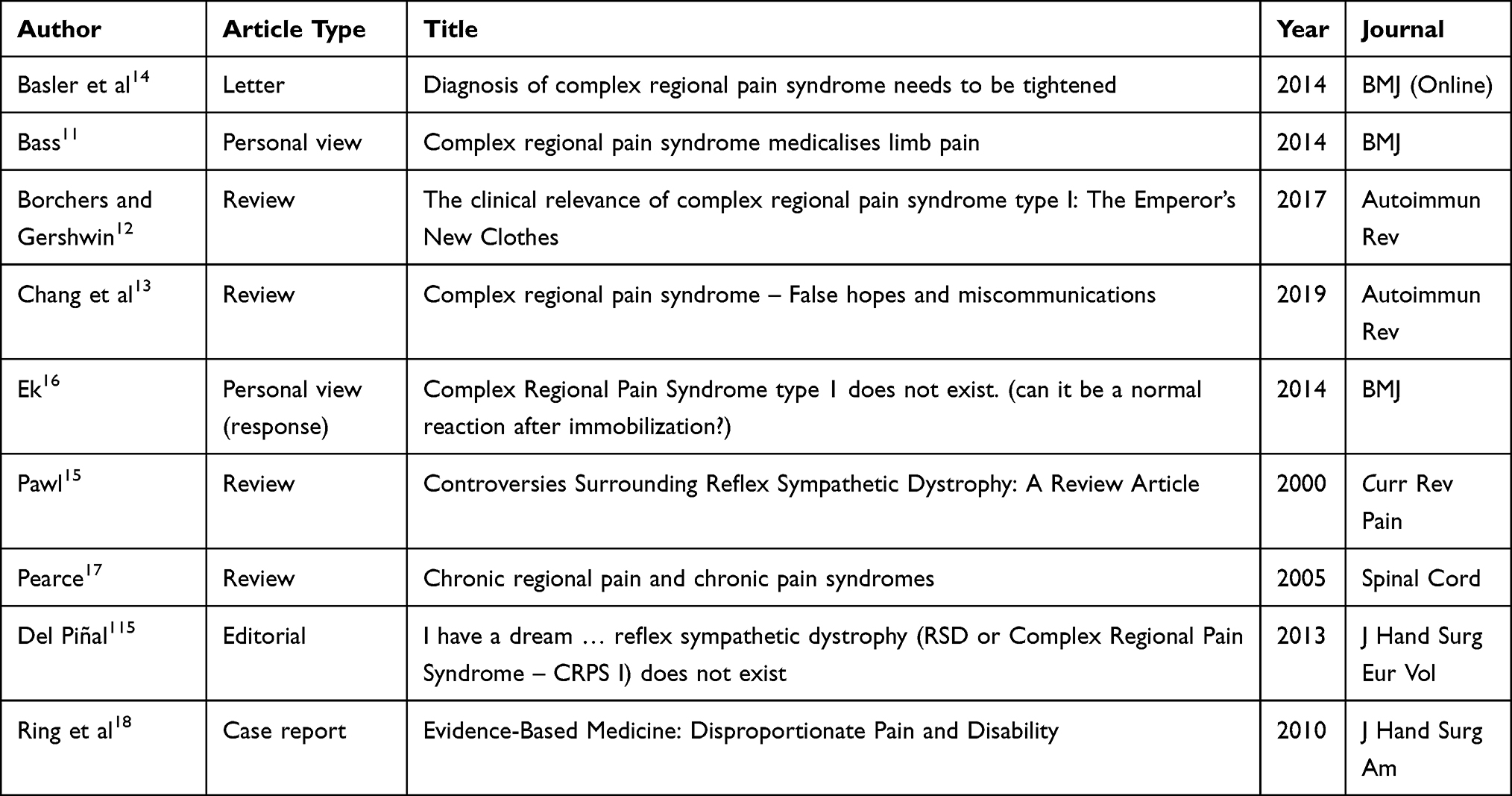 |
Table 1 Articles Included in This Review After Full-Text Screening |
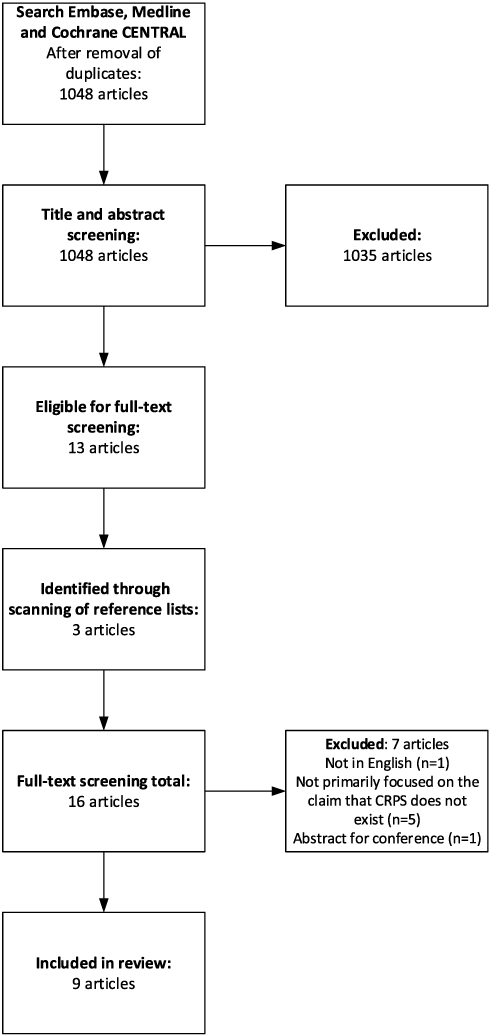 |
Figure 1 Flow diagram of article selection. |
Quality Assessment of Narrative Reviews
The outcome of the quality assessment of the four identified narrative reviews using the SANRA scale is provided in Table 2. It is notable that in only one review did the authors express their aim, albeit vague, for writing the article. Also, in all four reviews, it is not clear whether a literature search was conducted. Referencing was inconsistent or minimal in three of the four articles. Overall, the review of Chang et al scored the highest, with eight out of twelve points. The second highest scoring article was the review by Borchers and Gershwin, with six out of twelve points. After that, Pawl et al and Pearce et al followed with four out of twelve points.
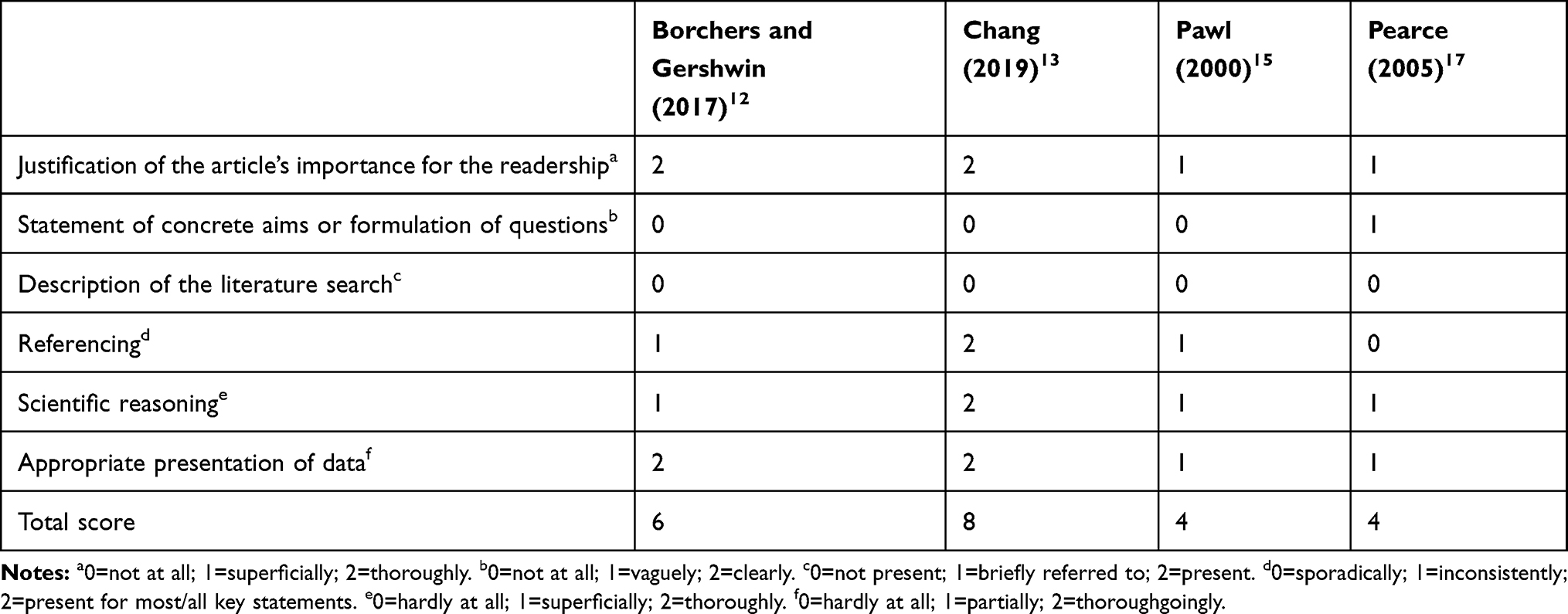 |
Table 2 Methodological Strength of the Published Narrative Reviews as Assessed by the SANRA |
Points of Controversy
Analysis of the nine included articles led to identification of seven different points of controversy that were used by the various authors to argue that CRPS is not a diagnostic entity (see Table 3). The arguments regarding the definition of CRPS and the diagnostic criteria were mentioned most often (by eight different authors). The argument that CRPS represents symptoms normally seen after immobilization was mentioned in five articles. Arguments that other causes explain the signs and symptoms of CRPS, that psychological factors cause CRPS, or that the pathophysiology is unclear are mentioned in four articles. One author mentioned weaknesses in the methodology of CRPS research.
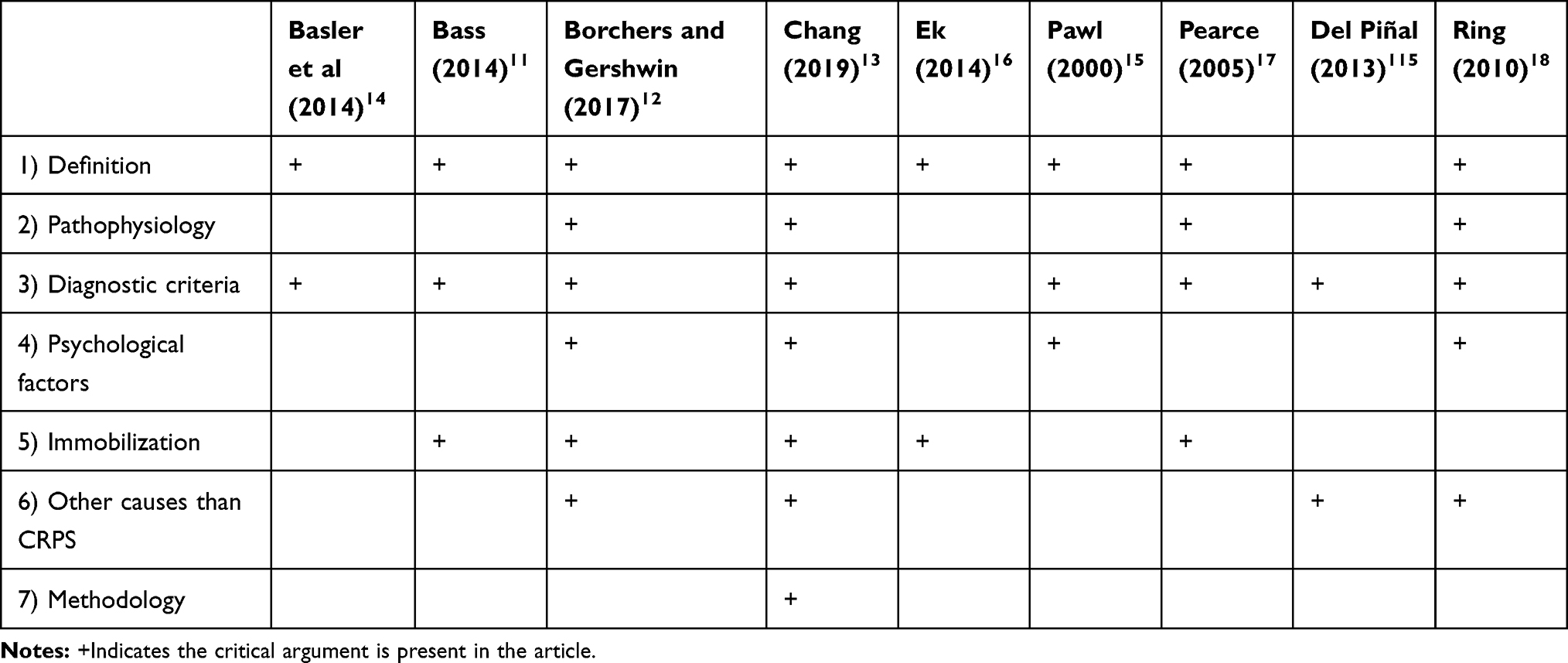 |
Table 3 Critical Arguments Mentioned in Each Article |
Discussion
Concerning the methodological quality of the articles summarized above, it is remarkable that the identified articles consisted exclusively of narrative reviews, personal views, a letter, an editorial and a case report. The level of evidence presented by these articles against the existence of CRPS as a diagnostic entity is therefore weak. When assessing the quality of the narrative reviews more in depth, only two out of the four narrative reviews scored more than half of the possible points on the SANRA. This illustrates that the methodological quality of the narrative reviews was low.
The arguments used to support the claim that “CRPS does not exist” are summarized below, followed by counterarguments based on available scientific literature on CRPS that refute each argument.
CRPS Should Not Be Called CRPS
Seven articles criticize the label “CRPS” for various reasons.11–18 It is stated that the “label” does not say anything about the underlying pathophysiology and that it medicalizes non-specific symptoms.11,13,17,18 In the view of Borchers and Gershwin, CRPS is merely a description of signs and symptoms that can be observed in many other diseases,12 implying that CRPS is not a distinct diagnostic entity. From this critical perspective, once such a diagnosis that medicalizes non-specific symptoms is communicated to the patient, the physician’s diagnosis causes a nocebo effect within the patient, in which hearing about potential symptoms or negative treatment outcomes can induce or increase symptoms. Thus, it is argued that patients develop symptoms consistent with CRPS simply by learning about the diagnosis and the expected pattern of symptoms. This argument implies that patients who believe that they are ill with “CRPS” then adopt the sick-role assigned to them.11 Subsequently, this nocebo effect can also encourage immobilization and pain avoidance behavior.16 Concerns are also raised that other psychosocial conditions which may be primary drivers of dysfunction are masked by applying the diagnostic label “CRPS” to patients.17 It is also argued that the CRPS diagnostic label legitimizes the overuse of pain medication13 and may contribute to secondary gain (eg sickness benefits) that then maintains the symptoms.15 Finally, these critics note that beliefs about CRPS-recovery influence the chronicity of the condition more than the severity of the injury itself,11 again implying that the condition is maintained by patients adopting the “role” of the CRPS patient.
Refutation
The term CRPS was indeed coined specifically as a means to describe clinical signs and symptoms without implying any specific pathophysiology.19 CRPS is explicitly described as a syndrome, which is “a group of signs and symptoms that occur together and characterize a particular abnormality or condition” (Merriam-Webster Dictionary).20 Although the criticism that CRPS is a descriptive label is true, this has no bearing on the existence of CRPS as a syndrome. In 1993, at the Orlando conference at which diagnostic terminology issues regarding the condition were first addressed in an international consensus format, the term CRPS was proposed because prior diagnostic labels, such as reflex sympathetic dystrophy (RSD), implied a specific pathophysiology that had been proven incorrect or incomplete.19 Therefore, there was a need for a new name independent of the presumed pathophysiology. The task force that created the diagnostic label CRPS was concerned that new scientific discoveries regarding the pathophysiology of this condition would constantly require a new classification or name. Thus, the acronym CRPS was introduced as an umbrella term which accounted for the prior diagnostic labels such as RSD (now CRPS type I) and causalgia (now CRPS type II), while forming a new diagnostic category that 1) allowed a differential diagnosis of CRPS from other conditions, 2) helped improve clinical uniformity when diagnosing patients, 3) allowed better identification of subgroups of CRPS type I and II, and 4) allowed identification of other CRPS subtypes in the future.19 The task force consistently refers to CRPS as an umbrella term for the group of disorders which were previously labelled RSD and causalgia.19 Pain was considered to be the cardinal symptom for the grouping of these disorders: patients fulfilling all or many of the criteria for the previous disorders but without pain would not be considered to have CRPS.19 The term complex was chosen to reflect the variable clinical phenomena displayed in each group. The term regional was chosen because the regional distribution of the pain and the accompanying symptoms and signs (edema, skin blood flow abnormality, abnormal sudomotor activity) was considered to be a hallmark of these disorders: the pain and accompanying symptoms and signs usually affect the distal part of a limb, beyond the territory of an injured nerve, and show progressive changes in intensity which can spread proximally and can vary with time. The accompanying clinical symptoms and signs are found in the region of the pain following the inciting event.19 To prevent patients with symptoms and signs that were anatomically, physiologically or temporally related to direct effects of an injury or trauma (eg, inflammation as part of normal healing), known disease with related presentation (eg, Raynaud's, deep vein thrombosis), or patients with a myofascial syndrome from being labeled with CRPS, an exclusion criterion was defined making it clear that CRPS is a diagnosis by exclusion: if the pain and accompanying symptoms and signs could be explained by another condition, CRPS would be excluded.19 Thus, patients who are suspected of having CRPS should be carefully examined for differential diagnostic purposes.
Other objections concerning the label CRPS, such as the nocebo effect accounting for patients’ CRPS signs and symptoms, are based on the a priori assumption that CRPS does not, in fact, exist. Nocebo effects, in which the patient’s knowledge of expected symptoms may induce or increase symptoms, are not unique to CRPS. The same criticism could potentially apply to any medical diagnosis, particularly to pain disorders due to the inherently subjective nature of pain. The extent of these nocebo effects depends on how physicians communicate with patients about symptoms, diagnoses and treatment expectations.21–24 There is no research to support the argument that providing CRPS as a diagnostic label for patients who meet Budapest criteria induces the nocebo effect any more than providing, for example, a migraine headache label for patients who meet criteria for that diagnosis.
Of course, secondary gain factors can contribute to chronic disease and influence symptoms in most chronic pain conditions (eg, chronic back pain25). It is a logical fallacy to argue that documented individual cases, in which secondary gain appears to account for self-induced CRPS-like features,26 necessarily mean that CRPS features in all patients are accounted for by secondary gain.
There is No Clear Pathophysiology
In four papers, critical remarks are made regarding the lack of a definitive pathophysiology of CRPS.12,13,17,18 Some of these arguments focus on the heterogeneity in signs and symptoms of CRPS. For example, patients may display either a cold or a warm extremity, with skin that may appear either blue or red. These very different signs and symptoms are interpreted as pointing towards very different pathophysiological mechanisms, which in turn lead the critics to believe that there can be no common underlying pathophysiological mechanism of CRPS.12,15 Likewise, the variable clinical course of the disease leads to uncertainty about a common underlying pathophysiology.17 Even though different possible pathophysiological mechanisms are hypothesized in the literature, Chang et al assert that a direct relationship between trauma and prolonged chronic CRPS has not been proven and that there is no biological explanation for the development of CRPS following minor traumas, such as cuts, bumps, contusions and bruises that occur in everyday life.13 Chang et al further write that studies on CRPS often do not elaborate on details such as the inciting event or the duration of immobility, so the association between these factors and the development of CRPS is unknown.13 Interestingly, the second author in the manuscript by Chang et al is a corporate defense attorney routinely defending large corporations against claims of injury-related CRPS. Thus, the arguments presented by Chang et al must be considered in light of the potentially biased opinions of this author.13 Nevertheless, the confusion surrounding the causes and pathophysiology of CRPS must be addressed.
Refutation
Historically, the medical field has assumed psychological or psychosomatic origins of symptoms when there is a lack of knowledge or understanding of pathophysiological mechanisms. A typical example is dystonia-like spasmodic torticollis. This movement disorder was long considered to be a psychogenic disorder (turning the head away) due to a lack of structural changes. However, as research progressed, findings from electrophysiological and imaging studies revealed torticollis as a disorder of sensory-motor integration circuits in the brain, which can be successfully treated with botulinum toxin injections instead of ineffective psychotherapy, which had been used for decades. Further, neurogenetic studies showed genetic involvement in certain subtypes of dystonia and at present, the classification of dystonia is even informed by neurogenetics.27
Similar pathophysiology-focused arguments also apply to widely accepted pain syndromes, such as fibromyalgia and chronic nonspecific low back pain, which have a pathophysiology that is multifactorial and not entirely clear.28–36 No credible sources argue that these conditions are not legitimate and/or are not distinct chronic pain conditions simply because their pathophysiology is not completely understood. While the pathophysiology of CRPS is also not completely understood, several mechanisms have been uncovered in recent studies, which may have been overlooked by the authors of these reviews.37,38 It has become clear that patients meeting CRPS diagnostic criteria regularly display a pattern of findings indicating several likely pathophysiologic mechanisms.
Although Chang et al argument that there is no conclusive biological explanation yet for the development of CRPS following minor trauma, may in a strict sense be correct, there is evidence from both human and animal studies consistent with the idea that minimal distal nerve injury (such as might occur after minor trauma) may be involved in CRPS,39–42 even in the absence of obvious nerve dysfunction on clinical examination or electromyography (EMG)/nerve conduction velocity (NCV) testing. Work in a post-fracture CRPS-Type I animal model further suggests that biochemical changes in the local milieu after injury, such as B-cell activation, increased interleukin(IL)-1β and enhanced substance P (SP) signaling, contribute to the development of CRPS after injury.43–45 Findings such as these certainly weaken arguments raised by critics that the occurrence of CRPS after minor injury is unexplainable and therefore existence of the condition itself is implausible. To further address claims that CRPS pathophysiology is unknown, we now briefly review the extensive research literature on CRPS mechanisms.
Autonomic Nervous System Mechanisms
A variety of studies indicate that autonomic nervous system alterations contribute to CRPS. CRPS is associated with both regional disturbances in sympathetic nervous system (SNS) activity in the affected limb46 and a range of systemic autonomic disturbances and central changes in autonomic drive.47–49 Consistent with the latter, early bilateral reductions in SNS-mediated vasoconstrictor responses post-fracture prospectively identify patients who subsequently go on to develop CRPS, suggesting a potential contributory role.50,51 Regarding specific autonomic changes, early studies suggested a regional reduction in turnover of the SNS neurotransmitter norepinephrine,52,53 which together with upregulated adrenoceptor responses,54 might contribute to altered vasoregulation in the CRPS affected limb. Evidence from more recent experimental studies evaluating the effects of the α1-adrenoceptor agonist phenylephrine46 and the α1-adrenoceptor antagonist prazosin55 in CRPS-affected limbs specifically support activation of α1-adrenoceptors on primary afferent fibers by norepinephrine as a contributor to the dynamic mechanical allodynia and punctate hyperalgesia associated with CRPS.46,55
Central Nervous System Mechanisms
Evidence for central nervous system involvement in CRPS predominantly emerges from neuroimaging studies. Cortical reorganization, as evidenced by a reduction in size of the representation of the CRPS-affected limb in the somatosensory cortex compared with the contralateral limb, has been observed in CRPS and is thought to explain some sensory features of CRPS such as its glove- or stocking-like distribution (ie not conforming to a specific dermatome or to a specific peripheral nerve distribution).56–61 Furthermore, the degree of cortical reorganization has been shown to positively correlate with the pain intensity and the amount of hyperalgesia, as well as tactile acuity, in CRPS patients.56,57,59 However, it must be stated that these very consistent findings were recently challenged.62
Patients with CRPS also exhibit impairments in endogenous pain inhibitory pathways in the brain,63,64 increased glucose metabolism in pain-related brain regions,65 and alterations within the default mode network during resting-state fMRI.66,67 Longitudinal studies suggest that successful treatment of CRPS may normalize changes in brain structure and function, such as a reversal of primary somatosensory cortex reorganization;58 an increase in gray matter in the dorsolateral prefrontal cortex, thalamus, basal ganglia, amygdala, and hippocampus; and enhanced functional connectivity between the dorsolateral prefrontal cortex and the periaqueductal gray, a primary source of endogenous pain inhibition.68
Inflammatory Mechanisms
Growing evidence indicates a role for inflammatory changes, including autoimmunity, neurogenic inflammation and neuroinflammation as a contributor to certain subgroups of CRPS. For example, recent brain imaging studies suggest increased microglial activation in CRPS patients, and thus a potential role for neuroinflammation in CRPS.69,70 In the periphery, multiple studies indicate that patients with CRPS exhibit a pro-inflammatory cytokine pattern.71–81 These pro-inflammatory changes have been observed at multiple biological levels, ranging from mRNA76 to suction blister fluid and skin biopsies obtained from the CRPS-affected extremity.71,81–83
Neurogenic inflammation occurs when peptidergic primary afferents are activated and release SP or calcitonin gene-related peptide (CGRP). These substances mainly bind to the neurokinin-1 (NK-1) receptor and the calcitonin receptor-like receptor (CRLR), respectively, and they induce protein extravasation, vasodilatation and warming of the skin, all of which are characteristic features of CRPS. In early posttraumatic CRPS, patients exhibit enhanced electrically evoked plasma extravasation and vasodilatation responses.84 In chronic CRPS, the total number of epidermal nerve fibers including the peptidergic nerve fibers is reduced in most cases39 or unchanged in some.85 Furthermore, the anti-inflammatory protease network in patients with CRPS may be less effective than in both healthy controls and other chronic pain conditions. Evidence for this comes from CRPS-linked differences in degradation pathways for the inflammatory mediator bradykinin86 and increased sensitivity of SP receptors87 in CRPS patients’ affected limbs compared to their contralateral limbs.
Immune Mechanisms
Autoimmune processes appear to represent another mechanism that may contribute to CRPS, based on the presence of antinuclear antibodies and surface-binding immunoglobulin G (IgG) serum-autoantibodies in a substantial subset of patients with CRPS88–90 and abnormalities in both circulating and tissue-resident T-cell sub-populations.91,92 Autoimmune mechanisms are further supported by studies using a passive transfer model demonstrating that administration of IgG from CRPS patients can induce CRPS-like features (eg, prolonged swelling, hyperalgesia) in animals following injury,93 a finding that depends on spinal IL-1ß mediated mechanisms.37 Nociceptors (A-delta and C fibers), but not touch-related fibers, are abnormally activated in mice following transfer of IgG from donor CRPS patients, with IgG from CRPS patients with severe pain eliciting the strongest mechanical hyperalgesia in mice.94 Passive transfer of serum immunoglobulin M from patients in the early stages of CRPS also consistently elicits hyperalgesia in a passive-transfer tibia fracture-casting model.95 Importantly, the changes induced in these passive transfer models are strictly unilateral – affecting only the injured rodent limb— and are “invisible” to normal assessment methods: there is no systemic inflammatory response and no regional tissue destruction; the main antibody effect is limb-confined pain-sensitization.93–95
Genetic Factors and Epigenetic Changes
Familial aggregation of CRPS cases suggests a potentially heritable component of CRPS risk.96–98 The most consistent genetic findings regarding CRPS suggest genetic differences in the human leukocyte antigen (HLA) system, the system underlying the adaptive immune response.99–105 Epigenetic modifications provide an additional path for transmitting CRPS risk, and the most widely studied of these is DNA methylation.106,107 A recent study revealed 48 differentially methylated cytosine-phosphate-guanine dinucleotide (CpG) sites between CRPS and non-CRPS neuropathic pain patients, despite comparable pain intensity, with the top two sites being in the COL11A1 and HLA-DRB6 genes.108 The latter finding mirrors the genetic evidence for HLA system involvement in CRPS, as well as results of a small study suggesting differential gene expression in the HLA-DRB6 gene between CRPS patients and healthy controls.109 This work also revealed significantly enriched methylation in immune-related genetic pathways, consistent with a role for immune mechanisms in CRPS.108
Putting the Pieces Together
In summary, extensive literature using a variety of research methods indicates that a set of mechanisms reflecting autonomic, brain plasticity, inflammatory, immune, and genetic/epigenetic factors, is consistently associated with a diagnosis of CRPS.110,111 If CRPS pain and symptoms were purely the result of being given a label, or represented broad nonspecific complaints or underlying psychosocial issues, there would be no reason for the studies summarized above to show consistent patterns of association with a CRPS diagnosis compared to a non-CRPS pain diagnosis, to show unilateral clinical and biochemical changes, or for these changes to reverse in some cases with CRPS-focused treatment. Critics argue that seemingly very divergent clinical presentations, such as a warm/red limb versus a cold/blue limb, imply opposite mechanisms and therefore different pain conditions. However, as substantiated above, enhanced inflammation and altered autonomic function provide mechanisms that could explain both abnormally warm and cold skin. Results of a large prospective clinical study of CRPS, including both acute CRPS and chronic CRPS patients, demonstrated that the characteristic warm CRPS presentation evident in acute CRPS often changes over time within individuals to the cold CRPS presentation more common in chronic CRPS.112 Furthermore, it has been shown that signs and symptoms of CRPS are dynamic, ie, can change at different time points dependent, for example, on surrounding temperature,113 and that different clinical phenotypes of CRPS exist.114
Other prospective work suggests that elevations in inflammatory mediators (cytokines and peptides), which can contribute to edema as well as skin redness, are present in acute CRPS patients but generally normalize within the first 18 months post-onset.81 Evidence that the presentation and mechanisms of CRPS can change over time within individuals argues for a single syndrome that evolves in character over time rather than these differing CRPS presentations reflecting two different, unrelated syndromes. Findings such as these are more consistent with clinical patient subtypes within the CRPS diagnostic label rather than distinct conditions.
The Diagnostic Criteria Lack Validity
A criticism often mentioned is the lack of validity of the diagnostic criteria for CRPS11–15,17,18,115 (See Table 4). Several problems are noted, including the specificity, validity, interobserver reliability, and objectivity of the criteria; the presence of different sets of criteria; and lastly the existence of a condition named CRPS-Not Otherwise Specified (NOS). The individual criteria are considered non-specific and subjective, and the symptoms described in the criteria (at least when considered individually) are very common in other diseases.11–13,115 These critics argue that CRPS is often overdiagnosed, implying that this overdiagnosis relates to poor diagnostic criteria. These critics support this claim with a study in which CRPS was found to be diagnosed incorrectly in 72% of the cases by family physicians or community specialists,116 and another study with a similar design, which found that CRPS was diagnosed incorrectly in 77% of the cases.117 These critical authors argue that CRPS symptoms are grouped under the assumption that they share the same pathophysiology, but that this has not been objectified,13 and furthermore, that the symptoms can often be either decreased or increased, which indicates opposite activity of the underlying mechanism.15 Related to this is the argument that the somewhat heterogeneous clinical presentations and multiple mechanisms associated with CRPS imply that CRPS is a “garbage basket” diagnosis, and that its diagnostic criteria inappropriately group together multiple unrelated conditions.12 It is claimed that CRPS is a diagnosis of exclusion, but in scientific research it is unclear in what way and how thoroughly other diagnoses have been ruled out.12 One author even claims that only hand surgeons should be allowed to diagnose CRPS of the hand, because they are the only ones who are able to properly rule out other causes for the pain in the hand.115 While the point regarding overdiagnosis of CRPS has some merit, particularly with use of the older 1994 IASP criteria, the 2012 Budapest criteria have shown evidence of validity when properly applied.118
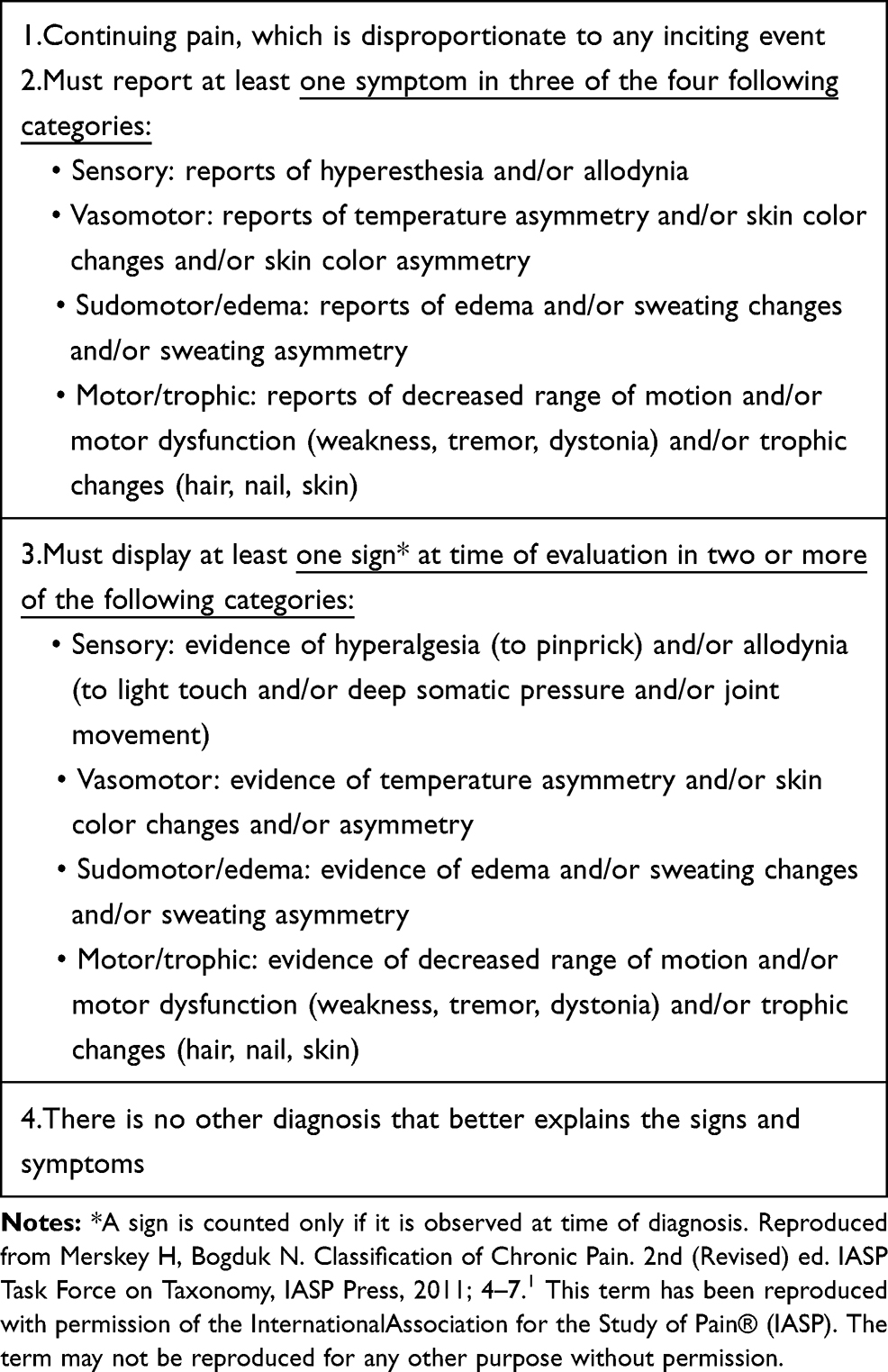 |
Table 4 Budapest Clinical Diagnostic Criteria for CRPS |
However, there are also some points of criticism regarding the methods used to validate the Budapest criteria.118 The criteria were validated in a group of 113 CRPS-I patients and 47 non-CRPS neuropathic pain patients, and the relative ability to distinguish between CRPS patients and non-CRPS patients using the former IASP versus the new Budapest diagnostic criteria was tested.118 The first objection is that there is no gold standard against which the criteria can be validated.12 The second point of criticism is about the control group in this validation study, of which it is said that 85% had easily recognizable neuropathic conditions in specific dermatomes or peripheral nerve distribution zones without autonomic symptoms, making it uncomplicated to distinguish these conditions from CRPS.13 The third point is about the specificity, on which Chang et al conclude that in 30% of cases, a physician would incorrectly identify a patient with an uncomplicated neuropathy as having CRPS and confirm a diagnosis of CRPS in 99% of the cases with criteria that only have a specificity of 40%.13 Lastly, it is noted that the existence of the CRPS-NOS category enables everyone with chronic pain to be diagnosed with CRPS.12,15
Refutation
The studies cited above regarding dramatic rates of CRPS misdiagnosis do not indicate problems with the criteria themselves. Borchers and Gershwin12 use the results of Mailis-Gagnon et al116 to argue broadly against CRPS as a diagnosis. In fact, results of both this study and the study by Frölke et al117 highlight problems in application of the diagnostic criteria rather than the criteria themselves, with misdiagnosis in both studies due in most cases to failure to properly rule out other conditions that might account for the signs and symptoms (criterion 4 of the Budapest criteria). It needs to be pointed out that a diagnosis of CRPS can only be made when all four criteria are fulfilled (see Table 4). Improper application of the CRPS criteria, particularly by non-specialist clinicians, does not invalidate the condition as a diagnosis.
Other criticisms of the CRPS diagnostic criteria are in part justified, because there are indeed limitations to the criteria. Regarding comments that the criteria are too subjective, this is accurate with regard to the self-reported symptoms, and to some degree, certain signs that require patient input for evaluation (allodynia, hyperalgesia, weakness, limited active range of motion). However, by their nature, existence of pain and descriptions of pain characteristics are always subjective. There is no objective tool yet that can be used to validate the presence of specific pain characteristics. Other diagnostic signs including changes in skin color, temperature, sweating and edema are truly objective (observable by clinicians without patient input). Partial reliance on self-report of subjective symptoms for diagnosis is, however, common in all psychiatric conditions and many medical conditions, particularly those involving an inherently subjective phenomenon such as pain.119–121 In contrast to the previous (1994) IASP criteria in which the diagnosis could be made based on self-reported symptoms only, the 2012 IASP (Budapest) criteria explicitly require that clinical signs be present, with this change implemented specifically to address this subjectivity issue.
Regarding methodology, validation of the Budapest criteria as done by Harden et al,118 in which the new criteria are compared to old criteria in order to validate the new criteria, can indeed be considered limited because these older criteria cannot truly serve as a gold standard. These efforts to validate the CRPS criteria therefore addressed incremental validity rather than absolute validity. Research is being carried out into a possible role for biomarkers in CRPS,122–124 but because no definitive biomarker has yet been found, a clear gold standard for diagnosis remains elusive. At present, CRPS is a clinical diagnosis that can in some cases be supported by objective tests, such as triple-phase-bone scintigraphy.125 Arguments highlighted above would imply that there should be no diagnostic criteria for CRPS until a definitive biomarker has been identified, or further, that the condition should not be considered valid until a gold standard biomarker is identified. This argument runs contrary to accepted practice in other medical (eg, primary headache disorders, seronegative rheumatic arthritis) and psychiatric diagnostic systems, in which similar methods to those used to validate the CRPS criteria are considered standard and acceptable even in the absence of a clear gold standard.126
We do not view the criticism of the control groups used in validation of the CRPS criteria as justified, because it is inevitable that control groups in scientific research do not consist of the “borderline” cases, as such cases minimize the ability to identify real group differences. The results of the Harden et al validation study showed a sensitivity of 0.99 and a specificity of 0.68 for the Budapest criteria, which is a substantial improvement compared to the 1994 IASP criteria.118 From one perspective, this means that in 32% of the cases, the diagnosis of CRPS is still made in patients that do not actually have CRPS, a situation that is less than ideal. Nonetheless, the Harden et al validation work indicated that patients meeting the Budapest criteria for CRPS can be distinguished from other neuropathic pain conditions that are confined to a (single) dermatome or peripheral nerve distribution zone with a reasonable degree of specificity (0.68).118 This highlights that despite the absence of a clear gold standard, the signs and symptoms in the criteria, taken as a set, are reasonably distinct from non-CRPS neuropathic pain conditions (ie, CRPS looks different than non-CRPS pain). This issue of treating criteria as a set of features is crucial – while individual criteria may be common to other disorders, a point highlighted by critics, their occurrence in combination with each other in a single patient is what distinguishes CRPS from other pain conditions. The current diagnostic criteria (ie the Budapest criteria), despite the flaws mentioned above, remain the only validated tool to diagnose CRPS.
From a broad perspective, criticism of the methods used to validate CRPS as a means of dismissing the condition are unwarranted. Until recently, efforts to create validated criteria for diagnosing chronic pain disorders in a systematic way were limited to very few specific conditions (eg, headache disorders, fibromyalgia). In this sense, the validated criteria for CRPS, even if limited, are a step beyond criteria available for diagnosing most other chronic pain conditions, yet no one seems to be arguing that those other pain conditions do not exist simply because they do not have validated criteria. Validation of the CRPS criteria has in fact been used as an exemplar in ongoing efforts to create a comprehensive, validated chronic pain taxonomy.126,127
Criticisms that focus on the existence of multiple competing diagnostic criteria are easily dismissed. The international standard for CRPS diagnosis is the criteria contained in the official updated (2012) IASP taxonomy, which are currently being integrated into the upcoming 11th version of the International Classification of Diseases (ICD-11). These are the only criteria that have been subjected to systematic validation research, even if such research has limitations. All other CRPS diagnostic criteria were published by individual authors and are not endorsed by any large organization of pain professionals. Clinicians and researchers who rely on these other diagnostic criteria are not using state-of-the-art diagnostic criteria, and CRPS diagnoses using these other criteria are questionable.
Criticisms of CRPS-NOS as a “diagnosis” are valid, and this term is subject to potential misinterpretation. CRPS-NOS was added to the taxonomy to parallel standard practice in the much more well-developed psychiatric diagnostic taxonomy at the time (ie, DSM-IV). As with psychiatric diagnosis, it was intended to be a descriptive label for patients who have never fully met the CRPS criteria, but who appear to show features of CRPS and in whom no other condition could be identified to explain the symptoms. It is not a formal diagnosis and does not have any diagnostic criteria, so it cannot be validated. Valid criticisms of the descriptive term CRPS-NOS, however, imply nothing about the validity of the actual CRPS criteria.
Finally, we would like to discuss the adaptations made to the diagnostic criteria and CRPS subtypes by the IASP CRPS Special Interest Group during a workshop in Valencia, Spain in September 2019.128 This workshop was convened to review perceived ambiguities in the diagnostic criteria and to review issues faced in the application of these criteria both in the research and clinical setting. During this workshop, a third CRPS subtype was introduced. This third subtype, “CRPS with Remission of Some Features” was introduced to describe patients who in the past were diagnosed with CRPS according to the new IASP clinical diagnostic criteria but who currently (ie at this moment in time) display insufficient symptoms and signs to meet the diagnostic criteria. With the introduction of this third subtype, it is made clear that a reduction in symptoms and signs does not automatically mean an improvement in patient quality of life, pain symptoms or lived experiences. The term CRPS NOS was also revisited during this workshop and it was made clear that this term was reserved for patients who display some but not all symptoms and signs of CRPS required for diagnosis, and no other diagnosis better explains these symptoms and signs.128
Psychological Factors Play a Role in the Development of CRPS
Categorizing CRPS as primarily a psychological disorder is done in two different ways, namely by stating that CRPS is caused by psychological factors or stating that CRPS is a psychiatric disease. Pawl15 considers psychosocial factors to play a significant role in the generation of CRPS, because psychiatric comorbidity and personality abnormalities are claimed to be more often seen in CRPS patients than in healthy people.129 Borchers and Gershwin suggest that CRPS is a psychiatric disorder that requires psychological therapy as the primary form of treatment.12 The authors point out that many of the signs and symptoms of CRPS can be easily artificially induced, that it is impossible to distinguish CRPS from somatoform disorders or malingering, and that there is a great deal of secondary gain for patients.12 The secondary gain specifically reveals itself in the medico-legal setting.13
Refutation
The conclusion drawn by Pawl et al in the year 2000, namely that psychosocial factors play a role in the generation of CRPS, can be refuted by more recent studies. A systematic review from 2009 shows that there is no association between a variety of psychological factors and the development of CRPS and that only the occurrence of stressful life events is associated (not necessarily causally) with CRPS.130 Additionally, a prospective study was carried out in 596 patients presenting with a single fracture in the emergency room, which found no relation between standard psychological factors and subsequent development of CRPS.131 Moreover, in a prospective study of patients following knee arthroplasty surgery, there was no association between preoperative psychosocial status and CRPS status at 6 month follow-up.132 Furthermore, a retrospective case-control study assessing the medical history of CRPS patients prior to the onset of disease found that psychological factors were not associated with CRPS.133 Finally, we note that there is no doubt that the intensity of pain symptoms in CRPS may be associated (bidirectionally) with psychosocial factors (eg, enhancing or enhanced by negative affect). However, links between psychosocial factors and chronic pain status are well known to occur across chronic pain syndromes as a class.134–137
We disagree with the idea that CRPS cannot be distinguished from somatoform disorders for two reasons. The first reason is the difference in clinical presentation, as somatoform disorders are characterized by excessive thoughts, feelings or behaviors related to the somatic symptoms in the absence of significant physical findings, whereas in CRPS this is not the case. That is, a somatoform disorder would not be preferentially diagnosed rather than CRPS for a patient showing sufficient objective signs of CRPS (eg edema, warm and red skin), even if they showed a high level of distress and intense focus on those symptoms. Second, in CRPS, objective biochemical changes are found (detailed above). These point to an underlying pathophysiology that would not be seen in psychiatric (somatoform) disorders. Furthermore, the fact that there may be malingerers does not undermine the existence of CRPS, because malingerers can be seen in any field of medicine.
Symptoms of CRPS are a Normal Reaction to Immobilization
In five different articles,11–13,16,17 the authors draw the conclusion that CRPS is just a normal reaction to immobilization based on studies that find temperature and color differences after short-term immobilization. Borchers and Gershwin also point out that normal healing is associated with pain and inflammation and that recovery can take a long time for some patients.12
Refutation
The three articles cited by critics to prove that CRPS symptoms are a normal reaction to immobilization, when examined in detail, were not intended to refute the existence of CRPS,45,138,139 but to explain underlying pathophysiology. All immobilization models used for the investigation of CRPS pathophysiology evoke some but not all symptoms of CRPS. In the study by Terkelsen et al, the authors draw the conclusion that forearm immobilization (via casting) does not represent a complete human model of acute CRPS138 and in the study by Guo et al, the authors draw the conclusion that in their animal model, immobilization via casting only causes a CRPS-like syndrome of brief duration.45 Singh et al found that immobility and dependency cause temperature and color differences, but they did not try to model CRPS.139 The only conclusion that can possibly be drawn from these studies is that immobilization may play a contributory role in generating or exacerbating signs and symptoms of CRPS. However, this is no controversy as activation and mobilization to counteract immobilization is a generally accepted treatment for CRPS.140,141 Furthermore, in the study by Terkelsen et al, forearm immobilization in humans induced cold and mechanical hyperalgesia, but spontaneous pain, a defining diagnostic criterion for CRPS, was absent on cast removal and during the follow-up period of 28 days.138 The other two studies did not study the effect of immobilization on pain.45,139 In the absence of studies demonstrating that immobilization alone can induce not only skin color and temperature changes, but also intense chronic pain for months or years, arguments attributing CRPS solely to immobilization are pure speculation. In conclusion, these articles cannot be used as an argument to support claims that CRPS does not exist.
There are Always Other Causes That Explain the CRPS Symptoms
In order to diagnose someone with CRPS, other causes for the signs and symptoms should be excluded. However, two authors firmly state that there is always another cause for the signs and symptoms of patients, leading to the conclusion that the diagnosis of CRPS can almost never be made.12,115 The list of causes they consider for CRPS-like symptoms consists of unstable fractures; subclinical nerve entrapments; dysvascular states; pain-triggering pathology such as glomus tumors, varicella zoster reactivation, Lyme disease, and mononeuropathies; and psychiatric conditions. Further, one author states that complications of surgery are masked when diagnosing the pain with CRPS, because the doctors can easily blame CRPS as the cause of the symptoms, while the actual cause lies in mistakes or complications created by the doctors themselves.13
Refutation
Critics’ statements that there is always another cause other than CRPS for signs and symptoms that look like CRPS are made entirely as a matter of belief, with no evidence to support this, and make the unwarranted a priori assumption that CRPS does not exist. The list of differential diagnoses for CRPS is long and consists of the following categories of disease: neuropathic pain-like syndromes, myofascial pain syndromes, inflammation, vascular diseases and psychological disorders.141 These other causes for the signs and symptoms must be considered thoroughly and diagnostic tests can be used to exclude other disorders.142 However, after doing so, there still remain patients who meet the criteria for CRPS and who do not have any of the other disorders as mentioned by Borchers and Gershwin12 and Del Piñal.115 These are the patients that fulfil the 2012 IASP (Budapest) criteria for CRPS. Eventually, even Del Piñal admitted that there may be a number of patients with CRPS115 and we share this view.
Methodology in CRPS Studies is Flawed
Although only one article pays attention to the methodology used in CRPS studies,13 we still chose to include this argument in this review because we consider this an important point. Chang et al claim that good quality scientific studies on CRPS with a proper sample size do not exist, because CRPS is so rare that it is impossible to include sufficient participants in a study.13 He supports this argument by calculations that researchers would need to follow 400,000 participants for 5 years to see 100 cases of CRPS develop of which only 26 patients would develop chronic CRPS.
Refutation
We agree that the rarity of this disease often makes it difficult to achieve optimal sample sizes in CRPS research studies. However, this problem is not new and is shared by many other rare diseases. In addition, Chang et al base their claim on the argument that it is impossible to include sufficient participants (and thus reach sufficient statistical power) with a disease incidence of 5.5 per 100,000 person years as found by Sandroni et al.3 Although this calculation by Chang et al is not incorrect, it is important to consider that incidence rates in person years are most applicable in the same (or similar) setting that they were measured in and cannot easily be generalized to other populations. This is illustrated by the higher CRPS incidence rate that was found in a study by de Mos et al in a Dutch population: 26.2 per 100,000 person years.2 In addition, a Dutch prospective cohort study in 596 patients with a single fracture of a limb (rather than in the general population) showed a CRPS incidence rate of 7% using the Budapest criteria.143 If this incidence rate was to be used in the calculation by Chang et al, it would return a more positive outcome. Additionally, Chang et al's comments are applicable only to prospective studies seeking to study factors influencing the onset of CRPS. Other study designs, such as prospective studies of patients with recent onset CRPS can be used instead of prospective studies enrolling individuals before they develop CRPS, and these can achieve the required sample sizes much more easily (although these designs also have limitations). We agree that in common with other rare disorders, it can be challenging to reach the “generally accepted” power of 80% and level of significance of 0.05 when comparing with controls, but increased focus on registries,144,145 long duration studies and multisite studies to expand the pool of CRPS patients are ways around these issues and have been and are currently ongoing.
Conclusion
Articles have appeared repeatedly in the peer-reviewed literature that argue against the existence of CRPS as a distinct chronic pain syndrome. When such articles are read by clinicians not intimately familiar with the CRPS literature, the critical arguments raised may appear compelling on the surface, and lead to potential harm to patients in terms of both hindering a positive provider–patient relationship and delaying appropriate treatment. This review indicates that the criticisms raised by these authors, on the whole, are not supported by the CRPS evidence base. Critical arguments presented either ignore (intentionally or otherwise) or selectively interpret the CRPS research literature, which provides ample evidence to refute the criticisms raised. In the highest quality critiques, many of the criticisms raised seek to apply higher standards of validation to CRPS than are applied to most other chronic pain conditions, many of which are also incompletely understood, yet no one disputes that they are real conditions. Contrary to what many authors suggest, research into CRPS is not led by blind-faith in the condition. Rather, we believe research into CRPS represents the core of science: trying to uncover the unknown. There is a grain of truth in some of the criticisms raised, and there are indeed limitations to the CRPS diagnostic criteria due to limitations of the scientific literature. It is hoped that this review, by presenting both criticisms and relevant literature to refute each, may help guide future research and enhance scientific understanding and the clinical care of CRPS patients.
Highlights
- Many clinicians are skeptical about the existence of CRPS, leading to dismissal of signs and symptoms of patients.
- The level of evidence for the claim that CRPS does not exist is very weak.
- Published accounts claiming CRPS does not exist are harmful to patients.
Author Contributions
All authors made substantial contributions to conception and design, acquisition of data, or analysis and interpretation of data; took part in drafting the article or revising it critically for important intellectual content; agreed to submit to the current journal; gave final approval of the version to be published; and agreed to be accountable for all aspects of the work.
Funding
There is no funding to report.
Disclosure
Dr Amanda Stone reports grants from IASP, grants from NIH, outside the submitted work. Dr S Bruehl reports personal fees from NeuroBo, outside the submitted work. Prof. Dr. Janne Gierthmühlen report Travel support from Novartis, Pfizer, Grünenthal, personal fees from Lilly GmbH, TAD Pharma, personal fees from Certkom, outside the submitted work. Dr A Goebel report production of medico-legal reports for the Court. Prof. Dr. FJPM Huygen report personal fees from ABBOTT, grants, personal fees from Saluda, personal fees from Boston Scientific, personal fees from Grunenthal, personal fees from Pfizer, outside the submitted work. The authors report no other conflicts of interest in this work.
References
1. Merskey H, Bogduk N. Classification of Chronic Pain. 2nd (Revised) ed. IASP Task Force on Taxonomy, IASP Press, 2011; 4–7
2. de Mos M, de Bruijn AG, Huygen FJ, Dieleman JP, Stricker BH, Sturkenboom MC. The incidence of complex regional pain syndrome: a population-based study. Pain. 2007;129(1–2):12–20.
3. Sandroni P, Benrud-Larson LM, McClelland RL, Low PA. Complex regional pain syndrome type I: incidence and prevalence in Olmsted county, a population-based study. Pain. 2003;103(1–2):199–207.
4. Frölke JPM, Van Dongen RT, Van De Meent H. Complex regional pain syndrome type 1: negating the myth. Ned Tijdschr Geneeskd. 2015;159(4):2138–2141.
5. Iolascon G. Definition of the complex regional pain syndrome. Osteoporosis Int. 2018;29(1):S114–S115.
6. Bass C, Yates G. Complex regional pain syndrome type 1 in the medico-legal setting: high rates of somatoform disorders, opiate use and diagnostic uncertainty. Med Sci Law. 2018;58(3):147–155.
7. Borchers AT, Gershwin ME. Complex regional pain syndrome: a comprehensive and critical review. Autoimmun Rev. 2014;13(3):242–265.
8. Hawley JS, Weiner WJ. Psychogenic dystonia and peripheral trauma. Neurology. 2011;77(5):496–502.
9. Ochoa JL. Reflex? Sympathetic? Dystrophy? Triple questioned again. Mayo Clin Proc. 1995;70(11):1124–1126.
10. Taskaynatan MA, Balaban B, Karlidere T, Ozgul A, Tan AK, Kalyon TA. Factitious disorders encountered in patients with the diagnosis of reflex sympathetic dystrophy. Clin Rheumatol. 2005;24(5):521–526. doi:10.1007/s10067-005-1082-0
11. Bass C. Complex regional pain syndrome medicalises limb pain. BMJ. 2014;348:g2631.
12. Borchers AT, Gershwin ME. The clinical relevance of complex regional pain syndrome type I: the Emperor’s new clothes. Autoimmun Rev. 2017;16(1):22–33.
13. Chang C, McDonnell P, Gershwin ME. Complex regional pain syndrome – false hopes and miscommunications. Autoimmun Rev. 2019;18(3):270–278.
14. Basler MH, Rae CP, Stewart G. Diagnosis of complex regional pain syndrome needs to be tightened. BMJ (Online). 2014;348. doi:10.1136/bmj.g4029
15. Pawl RP. Controversies surrounding reflex sympathetic dystrophy: a review article. Curr Rev Pain. 2000;4(4):259–267.
16. Ek J. Complex Regional Pain Syndrome type 1 does not exist. (can it be a normal reaction after immobilization?). BMJ. 2014;348. doi:10.1136/bmj.g2631
17. Pearce JMS. Chronic regional pain and chronic pain syndromes. Spinal Cord. 2005;43(5):263–268.
18. Ring D, Barth R, Barsky A. Evidence-based medicine: disproportionate pain and disability. J Hand Surg (USA). 2010;35(8):1345–1347.
19. Stanton-Hicks M, Janig W, Hassenbusch S, Haddox JD, Boas R, Wilson P. Reflex sympathetic dystrophy: changing concepts and taxonomy. Pain. 1995;63(1):127–133.
20. Syndrome. Merriam-Webster.com Dictionary, Merriam-Webster. Merriam-Webster.
21. Aslaksen PM, Lyby PS. Fear of pain potentiates nocebo hyperalgesia. J Pain Res. 2015;8:703–710.
22. Colloca L, Benedetti F. Nocebo hyperalgesia: how anxiety is turned into pain. Curr Opin Anaesthesiol. 2007;20(5):435–439.
23. Reicherts P, Gerdes AB, Pauli P, Wieser MJ. Psychological placebo and nocebo effects on pain rely on expectation and previous experience. J Pain. 2016;17(2):203–214.
24. Colloca L, Finniss D. Nocebo effects, patient-clinician communication, and therapeutic outcomes. JAMA. 2012;307(6):567–568.
25. Romano JM, Turner JA, Jensen MP, et al. Chronic pain patient-spouse behavioral interactions predict patient disability. Pain. 1995;63(3):353–360.
26. Mailis-Gagnon A, Nicholson K, Blumberger D, Zurowski M. Characteristics and period prevalence of self-induced disorder in patients referred to a pain clinic with the diagnosis of complex regional pain syndrome. Clin J Pain. 2008;24(2):176–185.
27. Newby RE, Thorpe DE, Kempster PA, Alty JE. A history of dystonia: ancient to modern. Mov Disord Clin Pract. 2017;4(4):478–485.
28. Deyo RA, Rainville J, Kent DL. What can the history and physical examination tell us about low back pain? JAMA. 1992;268(6):760–765.
29. Staud R. Is it all central sensitization? Role of peripheral tissue nociception in chronic musculoskeletal pain. Curr Rheumatol Rep. 2010;12(6):448–454.
30. Goubert D, Oosterwijck JV, Meeus M, Danneels L. Structural changes of lumbar muscles in non-specific low back pain: a systematic review. Pain Physician. 2016;19(7):E985–E1000.
31. Chou D, Samartzis D, Bellabarba C, et al. Degenerative magnetic resonance imaging changes in patients with chronic low back pain: a systematic review. Spine (Phila Pa 1976). 2011;36(21 Suppl):S43–53.
32. Aoyagi K, He J, Nicol AL, et al. A subgroup of chronic low back pain patients with central sensitization. Clin J Pain. 2019;35(11):869–879.
33. Polli A, Godderis L, Ghosh M, Ickmans K, Nijs J. Epigenetic and miRNA expression changes in people with pain: a systematic review. J Pain. 2019;21(7–8):763–780.
34. Banfi G, Diani M, Pigatto PD, Reali E, Cell T. Subpopulations in the physiopathology of fibromyalgia: evidence and perspectives. Int J Mol Sci. 2020;21:4.
35. Hauser W, Henningsen P. Fibromyalgia syndrome: a somatoform disorder? Eur J Pain. 2014;18(8):1052–1059.
36. Deyo RA. Diagnostic evaluation of LBP: reaching a specific diagnosis is often impossible. Arch Intern Med. 2002;162(13):
37. Helyes Z, Tekus V, Szentes N, et al. Transfer of complex regional pain syndrome to mice via human autoantibodies is mediated by interleukin-1-induced mechanisms. Proc Natl Acad Sci USA. 2019;116(26):13067–13076.
38. Guo TZ, Wei T, Tajerian M, et al. Complex regional pain syndrome patient immunoglobulin M has pronociceptive effects in the skin and spinal cord of tibia fracture mice. Pain. 2020;161(4):797–809.
39. Oaklander AL, Rissmiller JG, Gelman LB, Zheng L, Chang Y, Gott R. Evidence of focal small-fiber axonal degeneration in complex regional pain syndrome-I (reflex sympathetic dystrophy). Pain. 2006;120(3):235–243.
40. Albrecht PJ, Hines S, Eisenberg E, et al. Pathologic alterations of cutaneous innervation and vasculature in affected limbs from patients with complex regional pain syndrome. Pain. 2006;120(3):244–266.
41. Siegel SM, Lee JW, Oaklander AL. Needlestick distal nerve injury in rats models symptoms of complex regional pain syndrome. Anesth Analg. 2007;105(6):1820–1829, table of contents.
42. Rasmussen VF, Karlsson P, Drummond PD, et al. Bilaterally reduced intraepidermal nerve fiber density in unilateral CRPS-I. Pain Med. 2018;19(10):2021–2030.
43. Li WW, Sabsovich I, Guo TZ, Zhao R, Kingery WS, Clark JD. The role of enhanced cutaneous IL-1beta signaling in a rat tibia fracture model of complex regional pain syndrome. Pain. 2009;144(3):303–313.
44. Li WW, Guo TZ, Shi X, et al. Autoimmunity contributes to nociceptive sensitization in a mouse model of complex regional pain syndrome. Pain. 2014;155(11):2377–2389.
45. Guo TZ, Offley SC, Boyd EA, Jacobs CR, Kingery WS. Substance P signaling contributes to the vascular and nociceptive abnormalities observed in a tibial fracture rat model of complex regional pain syndrome type I. Pain. 2004;108(1–2):95–107.
46. Drummond PD, Morellini N, Finch PM, Birklein F, Knudsen LF. Complex regional pain syndrome: intradermal injection of phenylephrine evokes pain and hyperalgesia in a subgroup of patients with upregulated alpha1-adrenoceptors on dermal nerves. Pain. 2018;159(11):2296–2305.
47. Wasner G, Heckmann K, Maier C, Baron R. Vascular abnormalities in acute reflex sympathetic dystrophy (CRPS I): complete inhibition of sympathetic nerve activity with recovery. Arch Neurol. 1999;56(5):613–620.
48. Wasner G, Schattschneider J, Heckmann K, Maier C, Baron R. Vascular abnormalities in reflex sympathetic dystrophy (CRPS I): mechanisms and diagnostic value. Brain. 2001;124(Pt 3):587–599.
49. Knudsen LF, Terkelsen AJ, Drummond PD, Birklein F. Complex regional pain syndrome: a focus on the autonomic nervous system. Clin Auton Res. 2019;29(4):457–467.
50. Schurmann M, Gradl G, Andress HJ, Furst H, Schildberg FW. Assessment of peripheral sympathetic nervous function for diagnosing early post-traumatic complex regional pain syndrome type I. Pain. 1999;80(1–2):149–159.
51. Vogel T, Gradl G, Ockert B, Pellengahr CS, Schurmann M. Sympathetic dysfunction in long-term complex regional pain syndrome. Clin J Pain. 2010;26(2):128–131.
52. Drummond PD, Finch PM, Smythe GA. Reflex sympathetic dystrophy: the significance of differing plasma catecholamine concentrations in affected and unaffected limbs. BRAIN. 1991;114(5):2025–2036.
53. Harden RN, Duc TA, Williams TR, Coley D, Cate JC, Gracely RH. Norepinephrine and epinephrine levels in affected versus unaffected limbs in sympathetically maintained pain. Clin J Pain. 1994;10(4):324–330.
54. Arnold JM, Teasell RW, MacLeod AP, Brown JE, Carruthers SG. Increased venous alpha-adrenoceptor responsiveness in patients with reflex sympathetic dystrophy. Ann Intern Med. 1993;118(8):619–621.
55. Drummond ES, Maker G, Birklein F, Finch PM, Drummond PD. Topical prazosin attenuates sensitivity to tactile stimuli in patients with complex regional pain syndrome. Eur J Pain. 2016;20(6):926–935.
56. Juottonen K, Gockel M, Silén T, Hurri H, Hari R, Forss N. Altered central sensorimotor processing in patients with complex regional pain syndrome. Pain. 2002;98(3):315–323.
57. Maihofner C, Handwerker HO, Neundorfer B, Birklein F. Patterns of cortical reorganization in complex regional pain syndrome. Neurology. 2003;61(12):1707–1715.
58. Maihöfner C, Handwerker HO, Neundörfer B, Birklein F. Cortical reorganization during recovery from complex regional pain syndrome. Neurology. 2004;63(4):693–701.
59. Pleger B, Ragert P, Schwenkreis P, et al. Patterns of cortical reorganization parallel impaired tactile discrimination and pain intensity in complex regional pain syndrome. Neuroimage. 2006;32(2):503–510.
60. Pleger B, Tegenthoff M, Ragert P, et al. Sensorimotor retuning [corrected] in complex regional pain syndrome parallels pain reduction. Ann Neurol. 2005;57(3):425–429.
61. Veldman PH, Reynen HM, Arntz IE, Goris RJ. Signs and symptoms of reflex sympathetic dystrophy: prospective study of 829 patients. Lancet. 1993;342(8878):1012–1016.
62. Mancini F, Wang AP, Schira MM, et al. Fine-grained mapping of cortical somatotopies in chronic complex regional pain syndrome. J Neurosci. 2019;39(46):9185–9196.
63. Freund W, Wunderlich AP, Stuber G, et al. The role of periaqueductal gray and cingulate cortex during suppression of pain in complex regional pain syndrome. Clin J Pain. 2011;27(9):796–804.
64. Klega A, Eberle T, Buchholz HG, et al. Central opioidergic neurotransmission in complex regional pain syndrome. Neurology. 2010;75(2):129–136.
65. Shiraishi S, Kobayashi H, Nihashi T, et al. Cerebral glucose metabolism change in patients with complex regional pain syndrome: a PET study. Radiat Med. 2006;24(5):335–344.
66. Baliki MN, Mansour AR, Baria AT, Apkarian AV. Functional reorganization of the default mode network across chronic pain conditions. PLoS One. 2014;9(9):e106133.
67. Bolwerk A, Seifert F, Maihofner C. Altered resting-state functional connectivity in complex regional pain syndrome. J Pain. 2013;14(10):1107–1115e1108.
68. Erpelding N, Simons L, Lebel A, et al. Rapid treatment-induced brain changes in pediatric CRPS. Brain Struct Funct. 2016;221(2):1095–1111.
69. Jeon SY, Seo S, Lee JS, et al. [11C]-(R)-PK11195 positron emission tomography in patients with complex regional pain syndrome: a pilot study. Medicine (Baltimore). 2017;96(1):e5735.
70. Jung YH, Kim H, Jeon SY, et al. Brain metabolites and peripheral biomarkers associated with neuroinflammation in complex regional pain syndrome using [11C]-(R)-PK11195 positron emission tomography and magnetic resonance spectroscopy: a pilot study. Pain Med. 2019;20(3):504–514.
71. Huygen FJPM, De Bruijn AGJ, De Bruin MT, George Groeneweg J, Klein J, Zijlstra FJ. Evidence for local inflammation in complex regional pain syndrome type 1. Mediators Inflamm. 2002;11(1):47–51.
72. Schinkel C, Gaertner A, Zaspel J, Zedler S, Faist E, Schuermann M. Inflammatory mediators are altered in the acute phase of posttraumatic complex regional pain syndrome. Clin J Pain. 2006;22(3):235–239.
73. Schinkel C, Scherens A, Köller M, Roellecke G, Muhr G, Maier C. Systemic inflammatory mediators in post-traumatic Complex Regional Pain Syndrome (CRPS I) - Longitudinal investigations and differences to control groups. Eur J Med Res. 2009;14(3):130–135.
74. Alexander GM, van Rijn MA, van Hilten JJ, Perreault MJ, Schwartzman RJ. Changes in cerebrospinal fluid levels of pro-inflammatory cytokines in CRPS. Pain. 2005;116(3):213–219.
75. Maihofner C, Handwerker HO, Neundorfer B, Birklein F. Mechanical hyperalgesia in complex regional pain syndrome: a role for TNF-alpha? Neurology. 2005;65(2):311–313.
76. Uceyler N, Eberle T, Rolke R, Birklein F, Sommer C. Differential expression patterns of cytokines in complex regional pain syndrome. Pain. 2007;132(1–2):195–205.
77. Wesseldijk F, Huygen FJ, Heijmans-Antonissen C, Niehof SP, Zijlstra FJ. Tumor necrosis factor-alpha and interleukin-6 are not correlated with the characteristics of Complex Regional Pain Syndrome type 1 in 66 patients. Eur J Pain. 2008;12(6):716–721.
78. Wesseldijk F, Huygen FJ, Heijmans-Antonissen C, Niehof SP, Zijlstra FJ. Six years follow-up of the levels of TNF-alpha and IL-6 in patients with complex regional pain syndrome type 1. Mediators Inflamm. 2008;2008:469439.
79. Birklein F, Schmelz M, Schifter S, Weber M. The important role of neuropeptides in complex regional pain syndrome. Neurology. 2001;57(12):2179–2184.
80. Blair SJ, Chinthagada M, Hoppenstehdt D, Kijowski R, Fareed J. Role of neuropeptides in pathogenesis of reflex sympathetic dystrophy. Acta Orthop Belg. 1998;64(4):448–451.
81. Lenz M, Uceyler N, Frettloh J, et al. Local cytokine changes in complex regional pain syndrome type I (CRPS I) resolve after 6 months. Pain. 2013;154(10):2142–2149.
82. Birklein F, Drummond PD, Li W, et al. Activation of cutaneous immune responses in complex regional pain syndrome. J Pain. 2014;15(5):485–495.
83. Heijmans-Antonissen C, Wesseldijk F, Munnikes RJ, et al. Multiplex bead array assay for detection of 25 soluble cytokines in blister fluid of patients with complex regional pain syndrome type 1. Mediators Inflamm. 2006;2006(1):28398.
84. Weber M, Birklein F, Neundorfer B, Schmelz M. Facilitated neurogenic inflammation in complex regional pain syndrome. Pain. 2001;91(3):251–257.
85. Drummond PD, Finch PM, Gibbins I. Innervation of hyperalgesic skin in patients with complex regional pain syndrome. CLIN J PAIN. 1996;12(3):222–231.
86. Konig S, Bayer M, Dimova V, et al. The serum protease network-one key to understand complex regional pain syndrome pathophysiology. Pain. 2019;160(6):1402–1409.
87. Leis S, Weber M, Isselmann A, Schmelz M, Birklein F. Substance-P-induced protein extravasation is bilaterally increased in complex regional pain syndrome. Exp Neurol. 2003;183(1):197–204.
88. Kohr D, Singh P, Tschernatsch M, et al. Autoimmunity against the beta2 adrenergic receptor and muscarinic 2 receptor in complex regional pain syndrome. Eur J Pain Suppl. 2011;5(1):48.
89. Dubuis E, Thompson V, Leite MI, et al. Longstanding complex regional pain syndrome is associated with activating autoantibodies against alpha-1a adrenoceptors. Pain. 2014;155(11):2408–2417.
90. Dirckx M, Schreurs MW, de Mos M, Stronks DL, Huygen FJ. The prevalence of autoantibodies in complex regional pain syndrome type I. Mediators Inflamm. 2015;2015:718201.
91. Russo MA, Fiore NT, van Vreden C, et al. Expansion and activation of distinct central memory T lymphocyte subsets in complex regional pain syndrome. J Neuroinflammation. 2019;16(1):63.
92. Heyn J, Azad SC, Luchting B. Altered regulation of the T-cell system in patients with CRPS. Inflamm Res. 2019;68(1):1–6.
93. Tekus V, Hajna Z, Borbely E, et al. A CRPS-IgG-transfer-trauma model reproducing inflammatory and positive sensory signs associated with complex regional pain syndrome. Pain. 2014;155(2):299–308.
94. Cuhadar U, Gentry C, Vastani N, et al. Autoantibodies produce pain in complex regional pain syndrome by sensitizing nociceptors. Pain. 2019;160(12):2855–2865.
95. Guo TZ, Shi X, Li WW, Wei T, Clark JD, Kingery WS. Passive transfer autoimmunity in a mouse model of complex regional pain syndrome. Pain. 2017;158(12):2410–2421.
96. de Rooij AM, de Mos M, Sturkenboom MC, Marinus J, van den Maagdenberg AM, van Hilten JJ. Familial occurrence of complex regional pain syndrome. Eur J Pain. 2009;13(2):171–177.
97. de Rooij AM, de Mos M, van Hilten JJ, et al. Increased risk of complex regional pain syndrome in siblings of patients? J Pain. 2009;10(12):1250–1255.
98. Higashimoto T, Baldwin EE, Gold JI, Boles RG. Reflex sympathetic dystrophy: complex regional pain syndrome type I in children with mitochondrial disease and maternal inheritance. Arch Dis Child. 2008;93(5):390–397.
99. Klein J, The SA. HLA system. First of two parts. N Engl J Med. 2000;343(10):702–709.
100. Klein J, Sato SA, Mackay IR, Rosen FS. The HLA System. N Engl J Med. 2000;343(11):782–786. doi:10.1056/NEJM200009143431106
101. Kemler MA, van de Vusse AC, van den Berg-Loonen EM, Barendse GA, van Kleef M, Weber WE. HLA-DQ1 associated with reflex sympathetic dystrophy. Neurology. 1999;53(6):1350–1351. doi:10.1212/WNL.53.6.1350
102. van de Beek WJ, Roep BO, van der Slik AR, Giphart MJ, van Hilten BJ. Susceptibility loci for complex regional pain syndrome. Pain. 2003;103(1–2):93–97.
103. Vaneker M, Van Der Laan L, Allebes W, Goris RJ. Genetic factors associated with complex regional pain syndrome 1: HLA DRB and TNF alpha promotor gene polymorphism. Disabil Med. 2002;2:69–74.
104. van Hilten JJ, van de Beek WJ, Roep BO. Multifocal or generalized tonic dystonia of complex regional pain syndrome: a distinct clinical entity associated with HLA-DR13. Ann Neurol. 2000;48(1):113–116.
105. Van Rooijen DE, Roelen DL, Verduijn W, et al. Genetic HLA associations in complex regional pain syndrome with and without dystonia. J Pain. 2012;13(8):784–789.
106. Epigenetics: DU. The origins and evolution of a fashionable topic. Dev Biol. 2016;416(1):249–254.
107. Tost J. DNA methylation: an introduction to the biology and the disease-associated changes of a promising biomarker. Methods Mol Biol. 2009;507:3–20.
108. Bruehl S, Gamazon ER, Van de Ven T, et al. DNA methylation profiles are associated with complex regional pain syndrome after traumatic injury. Pain. 2019;160(10):2328–2337.
109. Jin EH, Zhang E, Ko Y, et al. Genome-wide expression profiling of complex regional pain syndrome. PLoS One. 2013;8(11):e79435.
110. Bruehl S. An update on the pathophysiology of complex regional pain syndrome. Anesthesiology. 2010;113(3):713–725.
111. Gierthmuhlen J, Binder A, Baron R. Mechanism-based treatment in complex regional pain syndromes. Nat Rev Neurol. 2014;10(9):518–528.
112. Bruehl S, Maihofner C, Stanton-Hicks M, et al. Complex regional pain syndrome: evidence for warm and cold subtypes in a large prospective clinical sample. Pain. 2016;157(8):1674–1681.
113. Krumova EK, Frettlöh J, Klauenberg S, Richter H, Wasner G, Maier C. Long-term skin temperature measurements - A practical diagnostic tool in complex regional pain syndrome. Pain. 2008;140(1):8–22.
114. Dimova V, Herrnberger MS, Escolano-Lozano F, et al. Clinical phenotypes and classification algorithm for complex regional pain syndrome. Neurology. 2020;94(4):e357–e367.
115. Del Piñal F. Editorial. I have a dream … reflex sympathetic dystrophy (RSD or Complex Regional Pain Syndrome - CRPS I) does not exist. J Hand Surg Eur Vol. 2013;38(6):595–597.
116. Mailis-Gagnon A, Lakha SF, Allen MD, Deshpande A, Harden RN. Characteristics of complex regional pain syndrome in patients referred to a tertiary pain clinic by community physicians, assessed by the Budapest clinical diagnostic criteria. Pain Med. 2014;15(11):1965–1974.
117. Frölke JP, vRA, deWaardt D, et al. Complex regionaal pijnsyndroom type 1? Bij 77% van de patienten een andere diagnose gesteld. [Complex regional pain syndrome type 1? In 77% of people had a different diagnosis]. Ned Tijdschr Geneeskd. 2009;153(12):550–553.
118. Harden RN, Bruehl S, Perez RSGM, et al. Validation of proposed diagnostic criteria (the “Budapest Criteria”) for complex regional pain syndrome. Pain. 2010;150(2):268–274.
119. Ohrbach R, Dworkin SF. AAPT diagnostic criteria for chronic painful temporomandibular disorders. J Pain. 2019;20(11):1276–1292.
120. Arnold LM, Bennett RM, Crofford LJ, et al. AAPT diagnostic criteria for fibromyalgia. J Pain. 2019;20(6):611–628.
121. Paice JA, Mulvey M, Bennett M, et al. AAPT diagnostic criteria for chronic cancer pain conditions. J Pain. 2017;18(3):233–246.
122. Birklein F, Ajit SK, Goebel A, Perez R, Sommer C. Complex regional pain syndrome - phenotypic characteristics and potential biomarkers. Nat Rev Neurol. 2018;14(5):272–284.
123. Bharwani KD, Dik WA, Dirckx M, Huygen F. Highlighting the role of biomarkers of inflammation in the diagnosis and management of complex regional pain syndrome. Mol Diagn Ther. 2019;23(5):615–626.
124. Konig S, Schlereth T, Birklein F. Molecular signature of complex regional pain syndrome (CRPS) and its analysis. Expert Rev Proteomics. 2017;14(10):857–867.
125. Wüppenhorst N, Maier C, Frettlöh J, Pennekamp W, Nicolas V. Sensitivity and specificity of 3-phase bone scintigraphy in the diagnosis of complex regional pain syndrome of the upper extremity. Clin J Pain. 2010;26(3):182–189.
126. Bruehl S, Ohrbach R, Sharma S, et al. Approaches to demonstrating the reliability and validity of core diagnostic criteria for chronic pain. J Pain. 2016;17(9 Suppl):T118–131.
127. Dworkin RH, Bruehl S, Fillingim RB, Loeser JD, Terman GW, Turk DC. Multidimensional Diagnostic Criteria for Chronic Pain: introduction to the ACTTION-American Pain Society Pain Taxonomy (AAPT). J Pain. 2016;17(9 Suppl):T1–9.
128. Goebel A, Birklein F, Brunner F, et al. The Valencia consensus-based adaptation of the IASP complex regional pain syndrome diagnostic criteria. Pain. 2021;162(9):2346.
129. Monti DA, Herring CL, Schwartzman RJ, Marchese M. Personality assessment of patients with Complex Regional Pain Syndrome type I. Clin J Pain. 1998;14(4):295–302.
130. Beerthuizen A, van ‘t Spijker A, Huygen FJPM, Klein J, de Wit R. Is there an association between psychological factors and the Complex Regional Pain Syndrome type 1 (CRPS1) in adults? A systematic review. Pain. 2009;145(1–2):52–59.
131. Beerthuizen A, Stronks DL, Huygen FJ, Passchier J, Klein J, Spijker AV. The association between psychological factors and the development of complex regional pain syndrome type 1 (CRPS1)–a prospective multicenter study. Eur J Pain. 2011;15(9):971–975.
132. Harden RN, Bruehl S, Stanos S, et al. Prospective examination of pain-related and psychological predictors of CRPS-like phenomena following total knee arthroplasty: a preliminary study. Pain. 2003;106(3):393–400.
133. de Mos M, Huygen FJ, Dieleman JP, Koopman JS, Stricker BH, Sturkenboom MC. Medical history and the onset of complex regional pain syndrome (CRPS). Pain. 2008;139(2):458–466.
134. Bruehl S, Husfeldt B, Lubenow TR, Nath H, Ivankovich AD. Psychological differences between reflex sympathetic dystrophy and non-RSD chronic pain patients. Pain. 1996;67(1):107–114.
135. Bruehl S, Chung OY, Burns JW. Differential effects of expressive anger regulation on chronic pain intensity in CRPS and non-CRPS limb pain patients. Pain. 2003;104(3):647–654.
136. Bean DJ, Johnson MH, Kydd RR. Relationships between psychological factors, pain, and disability in complex regional pain syndrome and low back pain. Clin J Pain. 2014;30(8):647–653.
137. Edwards RR, Dworkin RH, Sullivan MD, Turk DC, Wasan AD. The role of psychosocial processes in the development and maintenance of chronic pain. J Pain. 2016;17(9 Suppl):T70–92.
138. Terkelsen AJ, Bach FW, Jensen TS. Experimental forearm immobilization in humans induces cold and mechanical hyperalgesia. Anesthesiology. 2008;109(2):297–307.
139. Singh HP, Davis TR. The effect of short-term dependency and immobility on skin temperature and colour in the hand. J Hand Surg Br. 2006;31(6):611–615.
140. Perez RS, Zollinger PE, Dijkstra PU, et al. Evidence based guidelines for complex regional pain syndrome type 1. BMC Neurol. 2010;10:20.
141. van Eijs F, Stanton-Hicks M, Van Zundert J, et al. Evidence-based interventional pain medicine according to clinical diagnoses. 16. Complex regional pain syndrome. Pain Pract. 2011;11(1):70–87.
142. Bharwani KD, Dirckx M, Huygen FJPM. Complex regional pain syndrome: diagnosis and treatment. BJA Education. 2017;17(8):262–268.
143. Beerthuizen A, Stronks DL, Van’t Spijker A, et al. Demographic and medical parameters in the development of complex regional pain syndrome type 1 (CRPS1): prospective study on 596 patients with a fracture. Pain. 2012;153(6):1187–1192.
144. Shenker N, Goebel A, Rockett M, et al. Establishing the characteristics for patients with chronic Complex Regional Pain Syndrome: the value of the CRPS-UK registry. Br J Pain. 2015;9(2):122–128.
145. Bisla J, Ambler G, Frank B, et al. Successful and unsuccessful recruitment and retainment strategies in a UK multicentre drug trial for a rare chronic pain condition which performed above target. Br J Pain. 2019;14(3):171–179.
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.