Back to Journals » Advances in Medical Education and Practice » Volume 13
Dentists’ Attitude Towards Dental Treatment of Disabled Patients
Authors Salah A ![]() , Hashim R
, Hashim R ![]() , Salah S, Majeed AS, Abdulkareem Al-Hamdan S, Mohamed M
, Salah S, Majeed AS, Abdulkareem Al-Hamdan S, Mohamed M
Received 8 August 2022
Accepted for publication 30 November 2022
Published 14 December 2022 Volume 2022:13 Pages 1489—1496
DOI https://doi.org/10.2147/AMEP.S384112
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Md Anwarul Azim Majumder
Afraa Salah,1 Raghad Hashim,2 Shaymaa Salah,3 Athmar Shakir Majeed,3 Sarah Abdulkareem Al-Hamdan,1 Malaz Mohamed1
1Clinical Sciences, Ajman University, Ajman, United Arab Emirates; 2Basic Sciences, Ajman University, Ajman, United Arab Emirates; 3Psychology Department, Baghdad University, Baghdad, Iraq
Correspondence: Afraa Salah, Ajman University, Tel +971507271158, Email [email protected]
Background: Dental care is widely acknowledged as one of the most significant challenges facing individuals with disabilities. These patients cannot care for themselves and more attention should be paid to these individuals, particularly in oral health care.
Aim of the Study: This research investigates the knowledge and expertise of the dentists at Ajman University regarding the treatment of individuals with disabilities and the factors influencing their ability to treat these patients in private practice.
Materials and Methods: Methods included a descriptive cross-sectional survey employing 18 fixed-choice questions administered to a representative sample of 150 dentists working in the Ajman University area (Both Ajman and Fujairah campuses).
Results: Most participants admitted to a lack of ideal expertise in working with individuals with disability. However, being in the minority, such individuals have acceptable experience to provide the first line treatment.
Conclusion: The vast majority of participants expressed limitations with their training and limitations with an advanced level of care for this popular one. Other factors influencing the treatment of individuals with disabilities included the time it takes to treat the patients, inability to communicate with such patients, lack of patient collaboration, fear of causing harm to the patient and auxiliary staff and diminished patient compliance.
Keywords: dentist, attitudes, individuals with disabilities
Introduction
Patients are considered disabled if they suffer from any condition, whether physical or mental, that inhibits their capacity to operate normally, restricts their range of motion, or prevents them from carrying out an activity as intended. There are various impairments, including the following: a visual impairment, sometimes known as a visual handicap, is an impairment of visual function caused by either farsightedness or near-sightedness.1 Deafness is a hearing impairment caused by faults affecting one or both. These flaws can cause temporary or permanent damage, resulting in either partial or complete hearing loss in those who are deaf. A condition that affects one’s intelligence and may lead to difficulties in comprehending, communicating, or carrying out tasks correctly. The term “physical disability” refers to a lack of partial or complete mobility that prevents an individual from performing typical responsibilities.2
Every day, there are more and more people in the world who are living with a disability. The impacted population is around one billion people throughout the globe. Dental and medical practitioners have significant difficulties providing adequate treatment for impaired individuals. It is well acknowledged that people with impairments face substantial challenges in obtaining dental treatment. Establishing communication and understanding with the patient is essential to the successful delivery of dental treatment and is the primary focus of the dental treatment process. Several problems make it difficult for impaired people to get dental care. Some of the challenges that dental clinics face include communication issues with patients, difficulties with patients’ mobility, and inadequate patient preparation for dental treatment.
The participants’ caregivers are also an essential part of this process. They are accountable for ensuring that disabled persons continue practising healthy eating habits and oral hygiene appropriate for their particular impairment. Dentists are an essential part of the system that drives this loop. Clinical training, previous dental experience, abilities, and the right attitude are all crucial components in providing dental care to impaired patients efficiently and effectively. The level of comprehension and educational preparation a dentist possesses correlates with the dentist’s attitudes and desire to provide dental care to patients with disabilities.3,4 The dental curriculum, dental courses, and clinical practices have a significant role in determining how dentists feel about the care of impaired patients.
A graduating dentist who had participated in training programs focused on providing care to impaired patients had good attitudes and high levels of confidence when providing treatment. Dentists with less worry because they have successfully managed to treat many dental diseases, emergency cases, and psychological problems among patients have confidence in handling future obstacles. According to the findings of clinical investigations, the two primary obstacles to dental treatment for disabled patients are their condition and the level of preparation their dentist provides.1,4 It is believed to be vital for dentists to have completed educational practice and participated in various seminars and practical training to provide dental care to individuals with disabilities.3
Individuals with disabilities are considered a significant group when they suffer from many dental disorders and illnesses. Due to the substantial risk of dental caries and periodontal disorders among the afflicted population, they must get dental treatment for the whole of their lives.4,5 The quality of the education being provided will affect the treatment offered to these patients. It will also increase the dentist’s confidence, attitude, professional behavior, and practice, reducing the differences between patients with special needs care and patients who do not have special needs care. There will be a 65% rise in the number of disabled people living in the USA by 2030.5 This rise is expected to take place.
The American Academy of Pediatric Dentistry (AAPD) surveyed around 5000 general dentistry practitioners over the summer of 2001 to learn more about how children are treated in their offices. According to the findings of this research, dentists who have experience working with patients with special needs care are more likely to care for patients with special needs and treat them.4,6
In 2003, the methods to provide students with the required knowledge about patients with special needs care and procedures shifted from formal lectures and tests to case-based, multidisciplinary teaching and learning. Before 2003, legal lectures and tests were used to teach students. All of these alterations have been made to increase the number of dental practitioners competent to handle patients with specific requirements while also making those patients feel more at ease and giving them greater self-assurance.7,8
The Commission approved new guidelines for dental and dental hygiene education programs on Dental Accreditation on July 30, 2004, to ensure both didactic and clinical learning opportunities for students to prepare better dentists to provide care for patients with special needs.3 In 2004, 295 dental students from five schools surveyed their attitudes toward treating patients with intellectual disabilities. More than 60% of respondents said they lack the necessary expertise and clinical connection to work with impaired individuals.7,8
In 2010, research was conducted on graduating dentists from the Pacific region to investigate their perceptions of the dental care of impaired patients. The findings of the study showed that graduates have a high level of appreciation for training courses for the dental management of disabled patients; however, they still require experience that is more clinical with a variety of different types of disabled patients suffering from a variety of other disabilities.4,8 Many researchers in Canada, the Netherlands, Malaysia, Australia, and England have studied the primary challenges impaired individuals face while seeking dental c re. According to the findings, dentists’ perspectives on the dental care of disabled patients are influenced by several factors, including a deficiency in clinical experience, inadequate dental education training gained from their dental schools, a lack of self-assurance, and the nature of the disability.8
Materials and Methods
This study was a descriptive cross-sectional and involved using a validated questionnaire9 (Appendix 1). Informed consent were signed by the participants involved in the study in the first page of the study questionnaire as they aware that their consent to participate is part of the study.The questionnaire initially modified through multiple phases, including reviewing the questions by subject matter experts in which 150 participants from Ajman University responded to the questionnaire. The responses were moderated to allow consistency in the answered questions. In the end, an examination using main components was carried out to eliminate questions that measured the same variable—the updated questionnaire comprised 17 chosen items. The research ethics committee at Ajman University reviewed the revised study proposal and gave their clearance to go forward with it (Ref. GD-2017/18-03S). Afterwards, an email version of the questionnaire was sent to a random sample of 150 dentists.
The questionnaire comprised demographic analysis, such as the participant’s gender, age, and level of education; the number of years of experience; and degree of expertise working with patients with special needs care. The data were analyzed using the Statistical Package for the Social Sciences, version 21.0 (developed and distributed by SPSS Inc.) to estimate descriptive features and frequencies. The following section demonstrates circumstances relating to the interactions with individuals with disabilities. Topics covered include better facilities for treatment; the best specialists who did the therapy; oral health issues faced by this community category; and what kind of treatment was provided. The last section addresses dentists’ worries about these patients and discusses the informational prerequisites that dentists must meet to treat these patients.(Appendix 1)
Results
Participants and Demographics
Table 1 indicates that 150 people participated in the study, including 88 females (59%) and 62 males (41%). Most of them were between 20 and 29 (70. %). The most participants, 79 in total, were from the medical practitioner (general practitioner) category (52. %). The majority of the participants, 113 (75.3%), had experience ranging from one to five years. The many dental treatment environments available to impaired people are shown in Table 2. Most dentists would instead do dental work in a hospital environment, which is 100 (66. %). However, the speciality of pediatric dentistry is the one most equipped to offer oral care for kids with disabilities. Oral care for people with disabilities is shown in Table 3. More than half of the participants agree that it is vital for impaired individuals to have good oral health throughout their lives (54%). Moreover, close to 97 participants (64.7%) think that deficient patient are at a significantly increased risk of contracting oral illnesses.
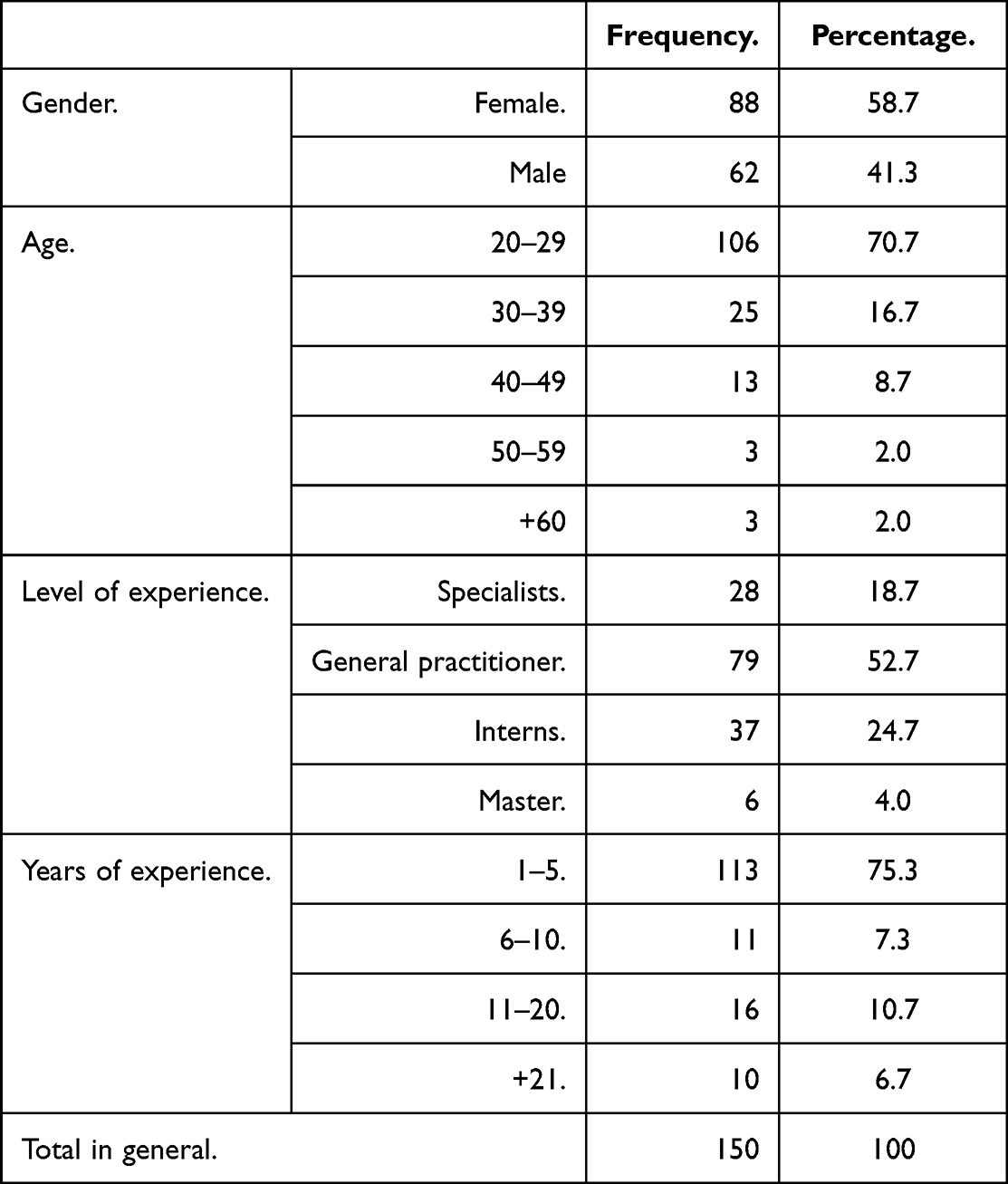 |
Table 1 Demographic Characteristics of Participants |
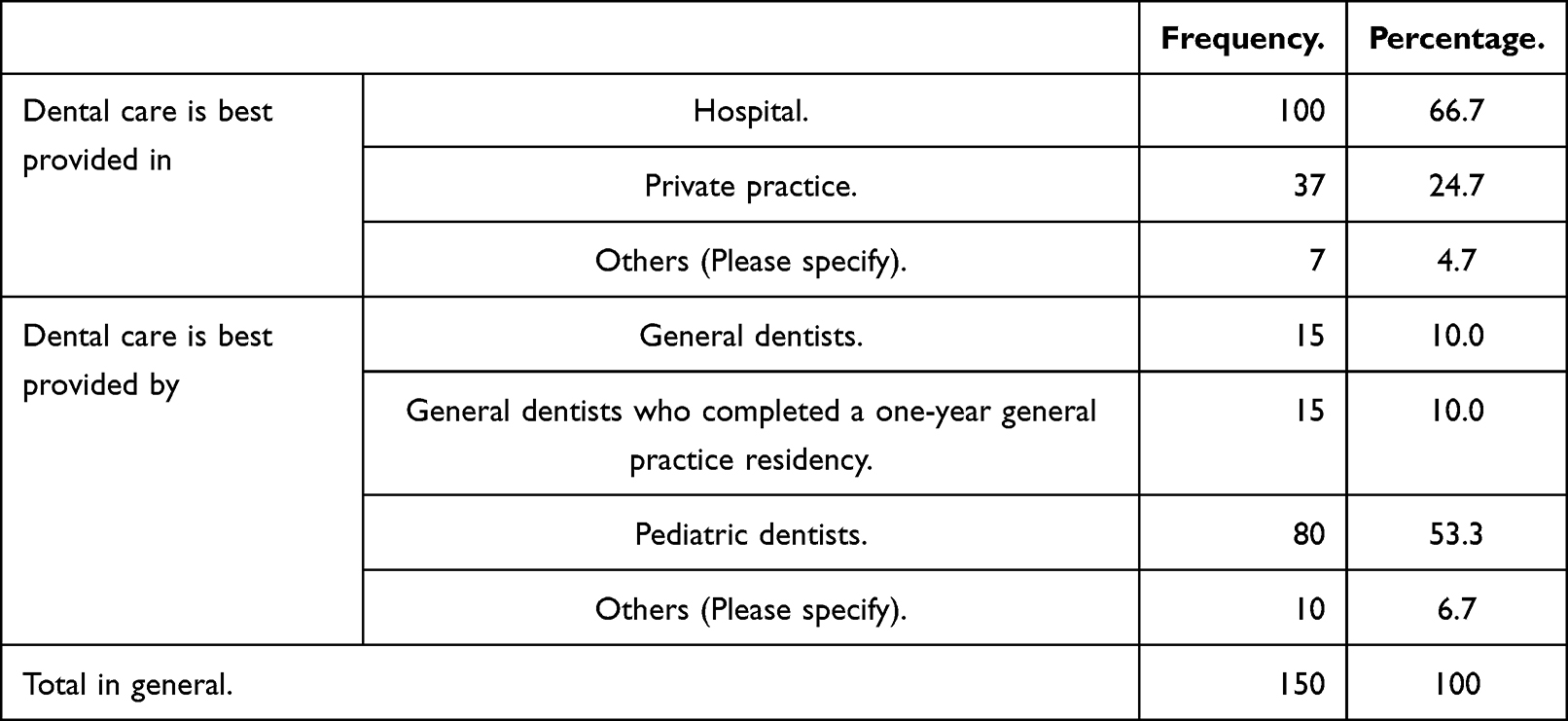 |
Table 2 Dentists’ Perspectives on the Treatment Environment for Impaired Patients |
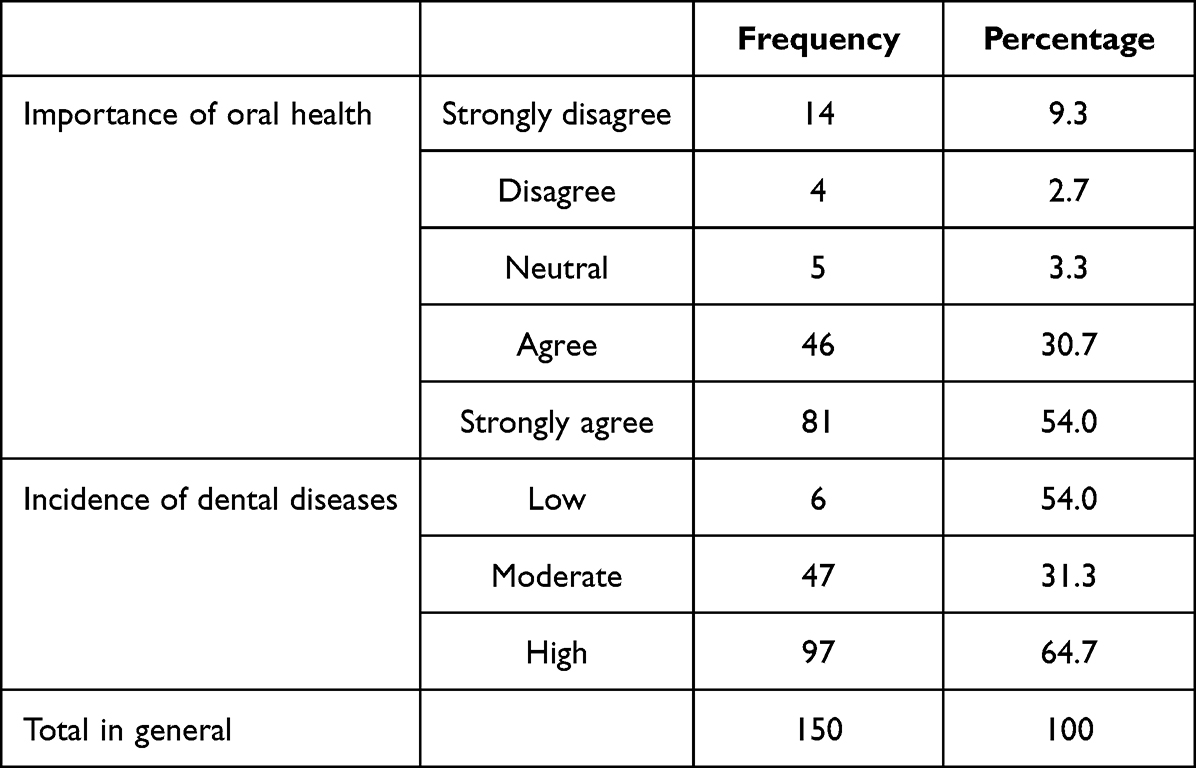 |
Table 3 Dentists’ Perspectives on the Oral Health of Disabled Patients |
Expertise
The participants’ level of training ranged from specialists (18.7%) and general practitioners (52.7%) to interns (24.7%) and masters (4%). About 46.7% of the participants said they had minimal experience dealing with special needs. In comparison, just 2% have a significant amount of expertise working with patients with special needs. The number of dentists willing to treat these patients was 73.3%, and they were prepared to refer them if the therapy became too difficult. It depends on the kind of impairment, whether physical or developmental delay and the kind of treatment the patient requires. Regarding the context of interactions with patients with special needs, those with no prior experience showed the highest percentage, which was 23 3%. This was followed by work-related interactions, which led to 22%, followed by friend-related interactions, which showed 13.3%, followed by family member-related interactions, which showed 11.3%, and then school-related interactions, which showed 6.7%.
Level of Comfort with Treatment
Participants reported learning about patients during geriatric rounds, direct patient care delivery, volunteering at the Latifa hospital, and consulting with the counsellors. When asked how comfortable they felt while administering the therapy, the majority of individuals gave neutral responses (45.3%), followed by positive responses (32.7%), negative responses (14.7%), strongly positive responses (4.7%), and strongly negative responses (2%). The concerns of the dentists when it comes to the delivery of treatment to individuals with disabilities were categorized as follows: 1- (44%) of dentists assign somewhat option regarding their ability to provide ideal treatment.2- (35.5%) of dentists assign somewhat option regarding the required time for treating these patient.
3- (38%) of the respondents said they were concerned about the inability to interact with the patients. 4- (36.7%) respondents chose somewhat option regarding patients ability to cooperate with them. 5-The majority of respondents ranked their concern about the patient being injured as much, (34.7%).Similarly, (30.7%) of dentists ranked their fear of harm themselves during dental treatment. Table 4. When it comes to the kinds of patients with special needs that dentists are willing to treat patients with developmental delay or physical disability.
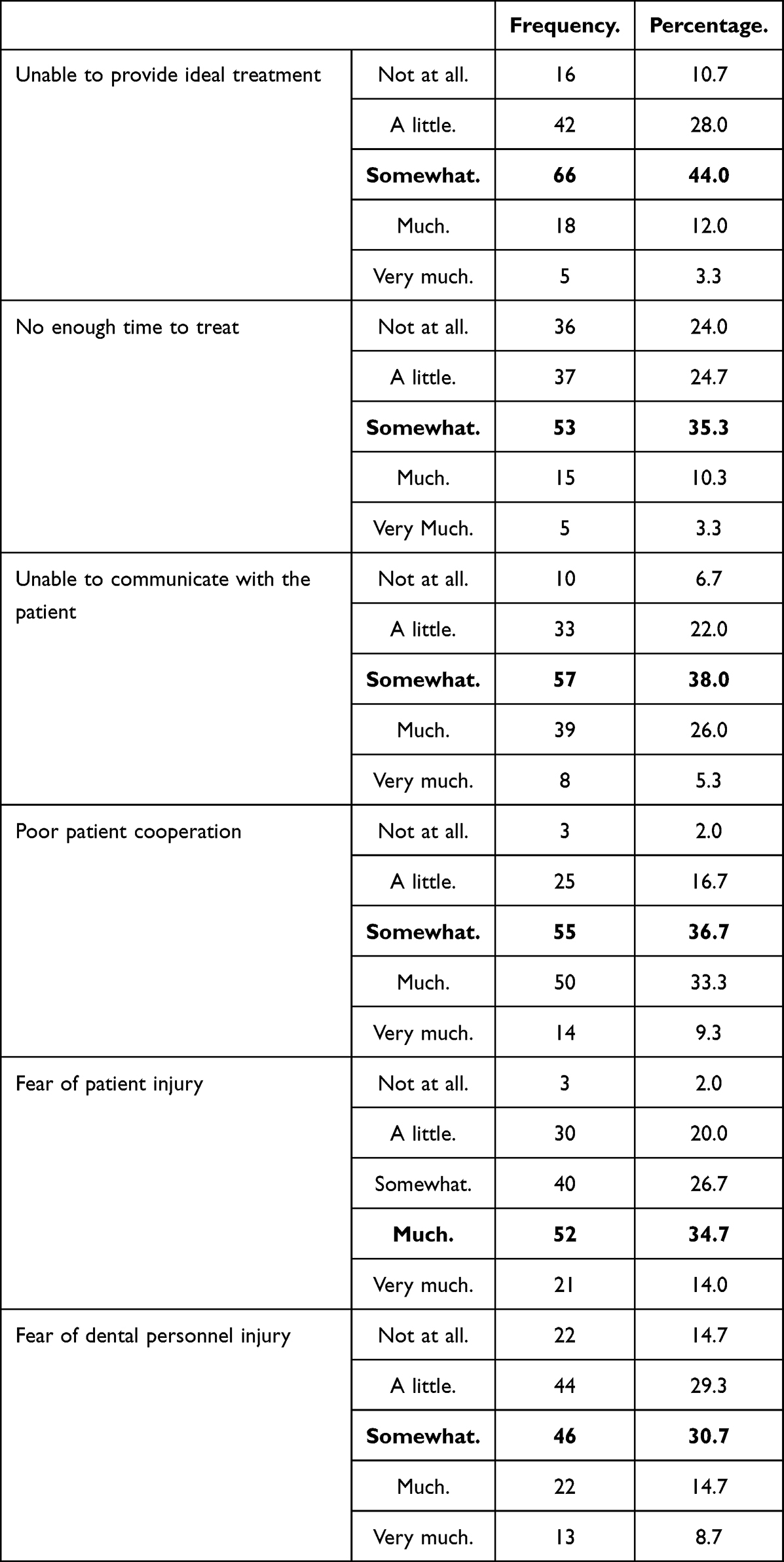 |
Table 4 Dentists’ Perspectives on the Level of Comfort of Treatment of Disabled Patients |
Reasons for Treating Patients with Special Needs Care
According to the chance that the dentist will try the treatment, 73.3% of the dentists chose that they would attempt to treat and refer if the treatment becomes too complex. While 20% of doctors will never treat a patient and refer them to a specialist, only 4.7% of doctors will treat every patient. Additionally, some specialists have stated that they may perform surgeries or that they can help patients in the best way possible, depending on how cooperative the patient is with the treatment type.
Treatment Facility
The dentists will give appropriate preventative care, examination, and ultimately simple restorations, simple extractions, endodontic therapy, and dentures, all of which have the same proportion. In addition, the dentists will supply dentures. While the lowest proportion of respondents disagreed with the statement that treatment facilities should be evaluated, the most significant percentage agreed. Regarding the necessary amount of clinical experience for a dentist to feel at ease, 34.7% of respondents said they agreed, 30.7% said they were indifferent, 24.7% said they were neutral, 6.7% said they strongly, and 2.7% said they disagreed. When discussing the level of experience, a dentist needs to have to perform the treatment; the requirements were listed in the following order: take continuing education courses, finish one year of general practice, specializing in dentistry by observing clinical demonstrations, perform simple restorations and extractions, and finally, I do not need any more experience.
Discussion
This research presents a variety of perspectives held by dentists studying at Ajman University about patients with special needs care and the best approach to taking care of them. Eighty- eight female and 62 male participants participated in the research. Female participants differed considerably from their male counterparts, and the choice of participants was random. It implies the facility seems to employ more female dentists than male dentists. The bulk of the participants were in the age range of 20 to 29 years old. The present study has the drawback of being based on a questionnaire, which means that the results may not accurately reflect the actual practices of the participants. When participants try to give the idea that they know how to work with patients with special needs, there is a chance that their responses will be distorted.
We consider this possibility. Most participants were general practitioners with an average of one to five years of experience, yet, they had minimal practice interacting with patients like these.2,10 Because the majority of the participants engage with one another in the context of their employment and because so few of them interact in the setting of their families, these individuals do not have much experience working with patients with special needs. Because of this, most of them experience fear and discomfort while delivering therapy; hence, they decide that the hospital is the ideal location to administer treatment to prevent any emergency. This conclusion was consistent with prior research on this subject.11,12 From this perspective, the vast majority of respondents felt that paediatric dentists should be the ones to provide the treatment because they have a higher level of education and expertise and more experience treating patients throughout their practice and speciality.3,14 Eighty-one of the dentists who participated in the study expressed their complete agreement with the statement that dental health is critical to overall health. In addition, there was a consensus among the participants (97 in total) that dental illnesses have a significant prevalence. When it came to providing dental treatment for people with special needs, the majority of the participants’ worries were somewhat related to the following issues: inability to provide ideal treatment, insufficient time to treat, failure to communicate with the patient, poor patient cooperation, and fear of injury to dental personnel.
When there is a significant worry over the potential for the patient to sustain an injury, participants would be willing to treat both types of special needs, including developmental delay and physical disabilities; however, they will attempt to treat by providing the following treatment: examination, preventive care, simple restorations, simple extractions, endodontic therapy, dentures, and refer if complicated. This is in addition to the concerns that were previously mentioned.
Some dentists have different viewpoints regarding behavior management and patient control, and others would like it if there was a workshop or a learning center where they could learn how to work with patients who have special needs, particularly patients who are unable to visit the dental clinic because of physical disabilities.8,13,14 On the other hand, when asked about how comfortable they were with the dentist while they were doing the treatment, 68% of subjects gave a neutral response. In addition, they concur with the notion that they require additional clinical experience to feel confident while providing dental treatment. Some examples of this other clinical experience include the following: observing clinical demonstrators performing restorations or extractions on patients with special needs; taking continuing education courses that are mainly geared toward providing dental treatment; completing a one-year residency in general practice; or specializing in pediatric dentistry. Despite this, 61 participants agree that having the facilities necessary to serve impaired patients will be essential to their dental training.15,17
Conclusion
Participant dentists raised significant concerns about their inability to provide ideal treatment for patients with special needs care. We conclude that the participant dentists’ limited treatment options for this population depend on their lack of adequate time and training, limited capacity to communicate with patients, patient adherence and the constant situational awareness of how to avoid unintentional injuries to patients that can lead to possible injuries to their clinical staff. Based on our research findings, we have some suggestions for you. Future training at Ajman University should focus on developing education and training for undergraduates and graduate dentists to improve their skills and confidence in the subject of special needs patients. This will help alleviate dentists’ concerns when treating patients with special needs, which should help reduce the anxiety that dentists feel when treating patients with special needs care. We need to establish specialized dentistry clinics for patients with particular requirements so that they may get a more comfortable and better-quality treatment.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Holzinger A, Lettner S, Franz A. Attitudes of dental students towards patients with special healthcare needs: can they be improved? Eur J Dent Educ. 2020;24(2):243–251. doi:10.1111/eje.12490
2. Loan P, Dao BS, Samuel Zwetchkenbaum DDS, Inglehart MR. General dentists and special needs patients: does dental education matter? J Dent Educ. 2005;69(10):1107–1115. doi:10.1002/j.0022-0337.2005.69.10.tb04011
3. da Rosa SV, Moys´es SJ, Theis LC, et al. Barriers in access to dental services hindering the treatment of people with disabilities: a systematic review. Int J Dent. 2020;2020(1):1–17. doi:10.1155/2020/9074618
4. Akiskal HS. Developmental pathways to bipolarity: are juvenile-onset depressions pre-bipolar. J Am Acad Child Adolesc Psychiatry. 1995;34:754–763. doi:10.1097/00004583-199506000-00016
5. Carlson GA, Loney J, Salisbury H, Kramer JR, Arthur C. Stimulant treatment in young boys with symptoms suggesting childhood mania: a report from a longitudinal study. J Child Adolesc Psychopharmacol. 2000;10(3):175–184. doi:10.1089/10445460050167287
6. Chávez EM, Subar, PE, Jeffrey M, Allen Wong EE, Glassman P. Perceptions of predoctoral dental education and practice patterns in special care dentistry. J Dent Educ. 2011;75(6):726–732. doi:10.1002/j.0022-0337.2011.75.6.tb05099.x
7. Barry Waldman H, Fenton SJ, Perlman SP, Cinotti DA. Preparing dental graduates to provide care to individuals with special needs. J Dent Educ. 2005;69(2):249–254. doi:10.1002/j.0022-0337.2005.69.2.tb03910.x
8. Khalifeh S, Yassin W, Kourtian S, Boustany RM. Autism in review. Liban Med J. 2016;64(2):110–115. doi:10.12816/0027470
9. Perusini D. Undergraduate dental students’ experiences and perceptions in the provision of dental treatment to persons with disabilities; 2013.
10. Patel KR, Cherian J, Gohil K, Atkinson D. Schizophrenia: overview and treatment options. P T. 2014;39(9):638–645. PMID: 25210417; PMCID: PMC4159061.
11. Krause M, Vainio L, Samuel Zwetchkenbaum MR, Inglehart MR. Dental education about patients with special needs: a survey of U.S. and Canadian dental schools. J Dent Educ. 2012;74(11):1179–1189. doi:10.1002/j.0022-0337.2010.74.11.tb04991.x
12. Schruers K, Koning K, Luermans J, Haack MJ, Griez E. Obsessive-compulsive disorder: a critical review of therapeutic perspectives. Acta Psychiatr Scand. 2005;111(4):261–271. doi:10.1111/j.1600-0447.2004.00502.x
13. Strober M, Carlson G. Bipolar illness in adolescents with major depression: clinical, genetic and psychopharmacologic predictors in a three-to- four year prospective follow-up investigation. Arch Gen Psychiatry. 1982;39:549–555. doi:10.1001/archpsyc.1982.04290050029007
14. World Health Organization. Mental health: strengthening mental health promotion. open society. Mental disability advocacy program. social care institute for excellence, electronic library for social care. Based on a summary of a report by the European Commission by Social Development Canada; 2004:1–2.
15. Weller EB, Weller RA, Fristad MA. Bipolar disorder in children: misdiagnosis, underdiagnoses and future directions. J Am Acad Child Adolesc Psychiatry. 1995;34:709–714. doi:10.1097/00004583-199506000-00010
16. Weil TN, Inglehart MR. Dental education and dentists’ attitudes and behavior concerning patients with autism. J Dent Educ. 2010;74(12):1294–1307. doi:10.1002/j.0022-0337.2010.74.12.tb05005.x
17. Weller EB, Weller RA, Danielyan AK. Mood disorders in prepubertal children. In: Wiener JM, Dulcan MD, editors. Textbook of Child and Adolescent Psychiatry. Washington, D C: American Psychiatric Publishing; 2004:418.
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.