")
Back to Journals » Clinical Interventions in Aging » Volume 10
Dental prophylaxis decreases the risk of acute myocardial infarction: a nationwide population-based study in Taiwan
Authors Lee Y, Hu H, Chou P, Chu D
Received 16 May 2014
Accepted for publication 27 June 2014
Published 6 January 2015 Volume 2015:10 Pages 175—182
DOI https://doi.org/10.2147/CIA.S67854
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Ya-Ling Lee,1,2 Hsiao-Yun Hu,2,3 Pesus Chou,2 Dachen Chu2,4,5
1Department of Dentistry, Taipei City Hospital, 2Institute of Public Health and Community Medicine Research Center, National Yang-Ming University, 3Department of Education and Research, Taipei City Hospital, 4Department of Health Care Management, National Taipei University of Nursing and Health Sciences, 5Department of Neurosurgery, Taipei City Hospital, Taipei, Taiwan
Purpose: To investigate the association between periodontal disease (PD) and acute myocardial infarction (AMI), and evaluate the effect of dental prophylaxis on the incidence rate (IR) of AMI.
Methods: The Longitudinal Health Insurance Database 2000 from the National Health Insurance program was used to identify 511,630 patients with PD and 208,713 without PD during 2000–2010. Subjects with PD were grouped according to treatment (dental prophylaxis, intensive treatment, and PD without treatment). The IRs of AMI during the 10-year follow-up period were compared among groups. Cox regression analysis adjusted for age, sex, socioeconomic status, residential urbanicity, and comorbidities was used to evaluate the effect of PD treatment on the incidence of AMI.
Results: The IR of AMI among subjects without PD was 0.19%/year. Among those with PD, the IR of AMI was lowest in the dental prophylaxis group (0.11%/year), followed by the intensive treatment (0.28%/year) and PD without treatment (0.31%/year; P<0.001) groups. Cox regression showed that the hazard ratio (HR) for AMI was significantly lower in the dental prophylaxis group (HR =0.90, 95% confidence interval =0.86–0.95) and higher in the intensive treatment (HR =1.09, 95% confidence interval =1.03–1.15) and PD without treatment (HR =1.23, 95% confidence interval =1.13–1.35) groups than in subjects without PD.
Conclusion: PD is associated with a higher risk of AMI, which can be reduced by dental prophylaxis to maintain periodontal health.
Keywords: periodontal disease, acute myocardial infarction, dental prophylaxis, dental scaling
Introduction
Coronary heart disease (CHD) is the leading cause of morbidity and mortality worldwide, with a prevalence ranging from 2%–20%.1,2 Acute myocardial infarction (AMI) is a CHD-related event that may result in sudden death. The risk factors for CHD include age, male sex, hypertension, diabetes mellitus, dyslipidemia, smoking, and inflammatory diseases, such as periodontal disease (PD).3–6
About 20%–50% of the population worldwide has PD.7–9 This disease is caused by the accumulation of a specific bacterial biofilm around teeth. The initial presentation is reversible gingivitis, which can be treated after biofilm removal.10–12 As PD progresses, destruction of the periodontal connective tissue and alveolar bone ultimately lead to tooth loss.13 Increased tooth brushing frequency has been found to reduce the serum concentrations of C-reactive protein and fibrinogen, suggesting that the improvement of periodontal conditions can reduce a patient’s systemic inflammatory status.14
Some previous researchers have concluded that poor periodontal status is associated with an increased risk of CHD.13,15–18 Deep periodontal pockets have been found in individuals who have experienced AMI and have been associated with an increased incidence of this event.19–21 A larger variation of subgingival anaerobic microflora has also been observed in those who have experienced AMI and is considered to be a potential risk indicator.22,23 However, other reports showed no significant relationship between PD and CHD.24,25 The relationships of PD and its treatment with the incidence of AMI remain unclear.
A retrospective cohort study was conducted using the Taiwanese National Health Insurance Research Database (NHIRD) to estimate the incidence rates (IRs) of AMI among subjects with PD and different PD treatment groups.
Methods
This study received full review by the local institutional review board (Taipei City Hospital Institutional Review Board number: TCHIRB-1020705-E). The institutional review board waived the need for written informed consent from study subjects because all potentially patient-identifying information was encrypted.
Data source
The compulsory, universal National Health Insurance (NHI) program in Taiwan covers up to 99% of the nation’s inhabitants. In conjunction with the NHI Bureau, the National Health Research Institute established the NHIRD to provide useful epidemiological information for basic and clinical research in Taiwan. The National Health Research Institute administers the NHIRD in a manner that ensures all beneficiaries’ privacy and confidentiality, and provides access to researchers only upon ethical approval.
For this study, the Longitudinal Health Insurance Database 2000 (LHID 2000) was used. The LHID 2000 is a standardized sample file for research use provided by the National Health Research Institute, and consists of comprehensive use and enrollment information for a randomly selected sample of 1 million NHI beneficiaries, representing approximately 5% of all enrollees in Taiwan in 2000. A multistage stratified systematic sampling design was used and it was found that there were no statistically significant differences in sex or age between the sample group and all enrollees. The identification of patients in the LHID 2000 is encrypted to protect their privacy, as this database includes information about medical orders, treatment procedures, and medical diagnoses (coded based on the International Classification of Diseases, 9th Revision, Clinical Modification [ICD-9-CM]).
Study cohort
The cohort for this retrospective study was drawn from 1 million beneficiaries sampled randomly from all beneficiaries listed in the NHIRD in the year 2000 (ie, the LHID 2000). Only subjects aged ≥20 years were included (723,024 beneficiaries; Figure 1). The subjects were included into the PD cohort if they visited an ambulatory care provider due to PD (ICD-9-CM codes 523.0–523.5) during the study period. Patients who developed AMI before PD diagnosis (n=2,066) and individuals of unknown sex (n=615) were excluded. Individuals with no diagnosis of PD from 2000–2010 served as the control group (n=208,713; followed for 2,248,618 person-years).
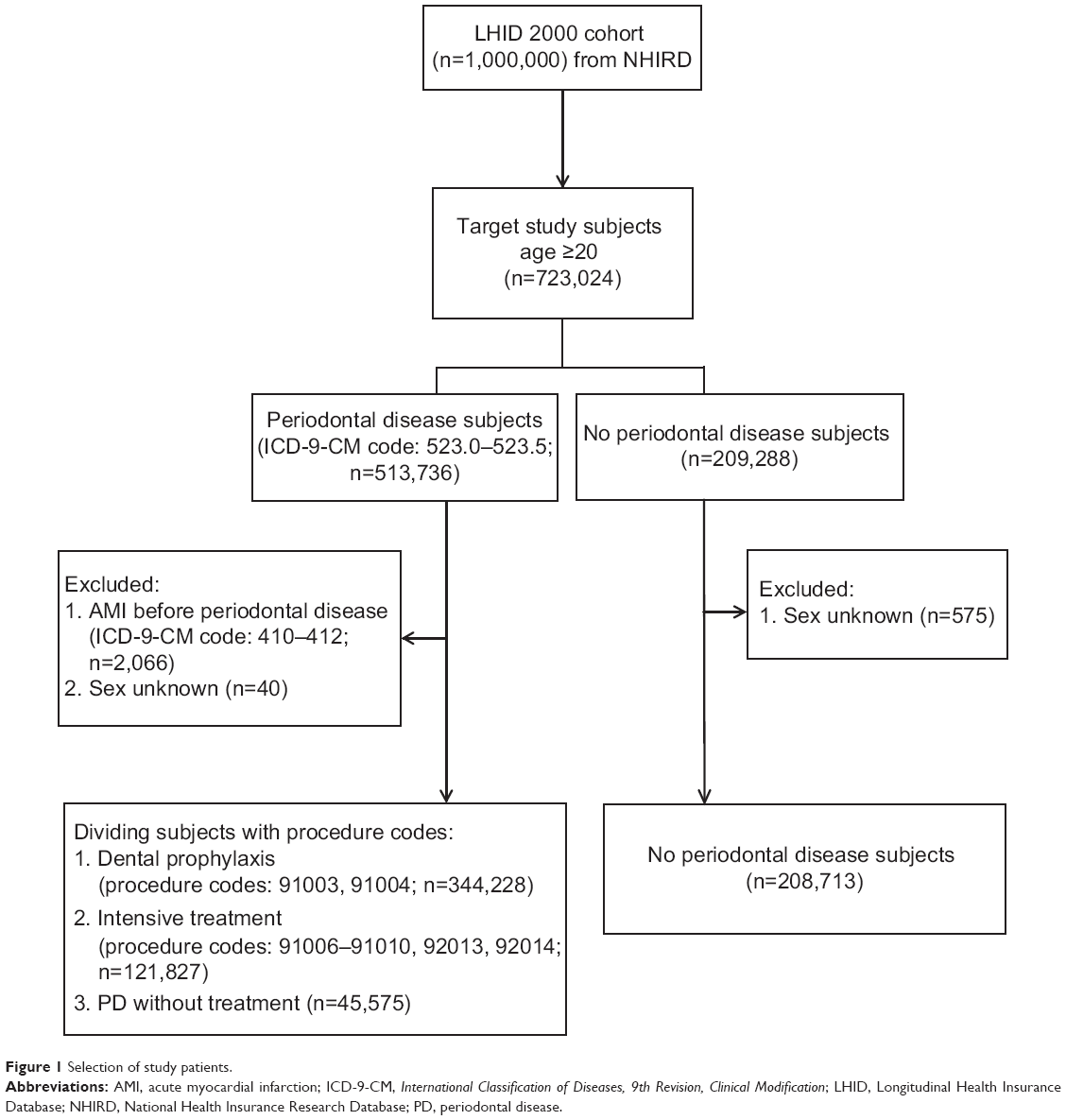 | Figure 1 Selection of study patients. |
The PD group (ICD-9-CM codes 523.0–523.5) was divided into three treatment groups:
- Dental prophylaxis (n=344,228; followed for 2,807,865 person-years): PD patients who only received dental prophylaxis (procedure codes: 91003, 91004) during the following period.
- Intensive treatment (n=121,827; followed for 789,518 person-years): PD patients who received treatments such as subgingival curettage and root planning (procedure codes: 91006–91008) and/or periodontal flap operation (procedure codes: 91009, 91010) and/or tooth extraction (procedure codes: 92013, 92014).
- PD without treatment (n=45,575; followed for 170,754 person-years): PD patients who received no treatments.
Thus, a total of 720,343 subjects followed for 6,016,755 person-years were included in this study. Participants were followed from the cohort entry date (the first date of an ambulatory care visit due to PD for the PD group and January 1, 2000 for the control group) until the date of hospitalization due to AMI (ICD-9-CM codes 410–412), death, or end of the study period (December 31, 2010).
The socioeconomic status variable had five categories. People with a well-defined monthly payroll were classified into three categories: =NT$40,000, NT$20,000–$39,999, and <NT$20,000 (NT$: New Taiwan dollars; US$1 is approximately worth NT$30). People without a well-defined monthly wage could either enroll through unions or associations, such as farmers’ associations, or through local government offices. Those who enrolled through local government offices included self-employed, retirees, corner store owners, or low-income people. People without a well-defined monthly payroll were categorized into two groups: union or association members and people enrolled in local government offices.
The residential urbanicity was classified into three categories: urban classification for metropolitan cities; suburban classification for all other cities and counties; and rural classification for all townships and rural areas.
In the analysis of AMI comorbidities, including atrial fibrillation (ICD-9-CM code 437.3), diabetes (ICD-9-CM code 250), hypertension (ICD-9-CM codes 401–405), dyslipidemia (ICD-9-CM code 272), chronic kidney disease (ICD-9-CM code 585), and peripheral vascular disease (ICD-9-CM codes 440.2, 440.3, 440.9, 443, 444.21, 444.22), only subjects with more than three outpatient visits during the study period were included to increase the validity of diagnoses in the administrative data set.
Statistical methods
Statistical analyses were performed using the SAS® statistical package (version 9.2; SAS Institute, Cary, NC, USA). The IRs of AMI among patients with PD and control subjects were compared. The χ
Results
A total of 10,046 patients developed AMI during the follow-up period (IR =0.17%/year; Table 1). The IR of AMI increased with age from 0.03%/year among subjects aged 20–44 years to 0.24% and 0. 61%/year among those aged 45–64 years and >65 years, respectively (P<0.001). The IR of AMI was higher among men than women (0.21% versus 0.13%/year) and was significantly higher among subjects with atrial fibrillation (0.88%/year), diabetes mellitus (0.55%/year), hypertension (0.49%/year), dyslipidemia (0.37%/year), chronic kidney disease (0.87%/year), and peripheral vascular disease (0.52%/year) than people without these comorbidities (all/P<0.001).
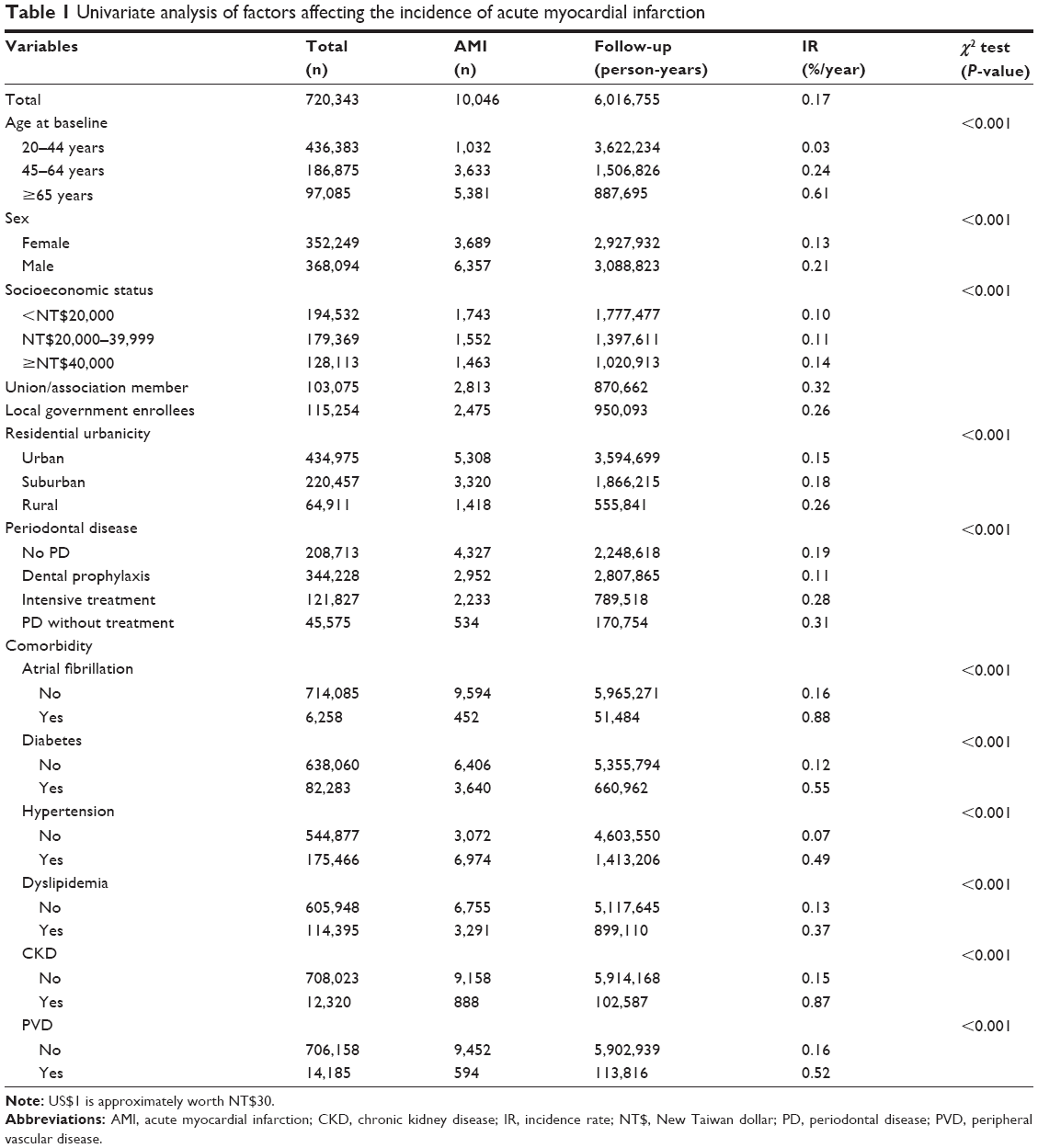 | Table 1 Univariate analysis of factors affecting the incidence of acute myocardial infarction |
A total of 4,327 people without PD developed AMI (IR =0.19%/year). Among those with PD, the IR of AMI was lowest in the dental prophylaxis group (0.11%/year) and highest in the PD without treatment group (0.31%/year;P<0.001).
When comparing IRs of AMI after being stratified by age, sex, socioeconomic status, residential urbanicity, and comorbidity variables (Table 2), the lowest IR of the PD population always appeared in the dental prophylaxis group, followed by the intensive treatment group and PD without treatment group (P<0.001 or/P=0.013 for the trend test).
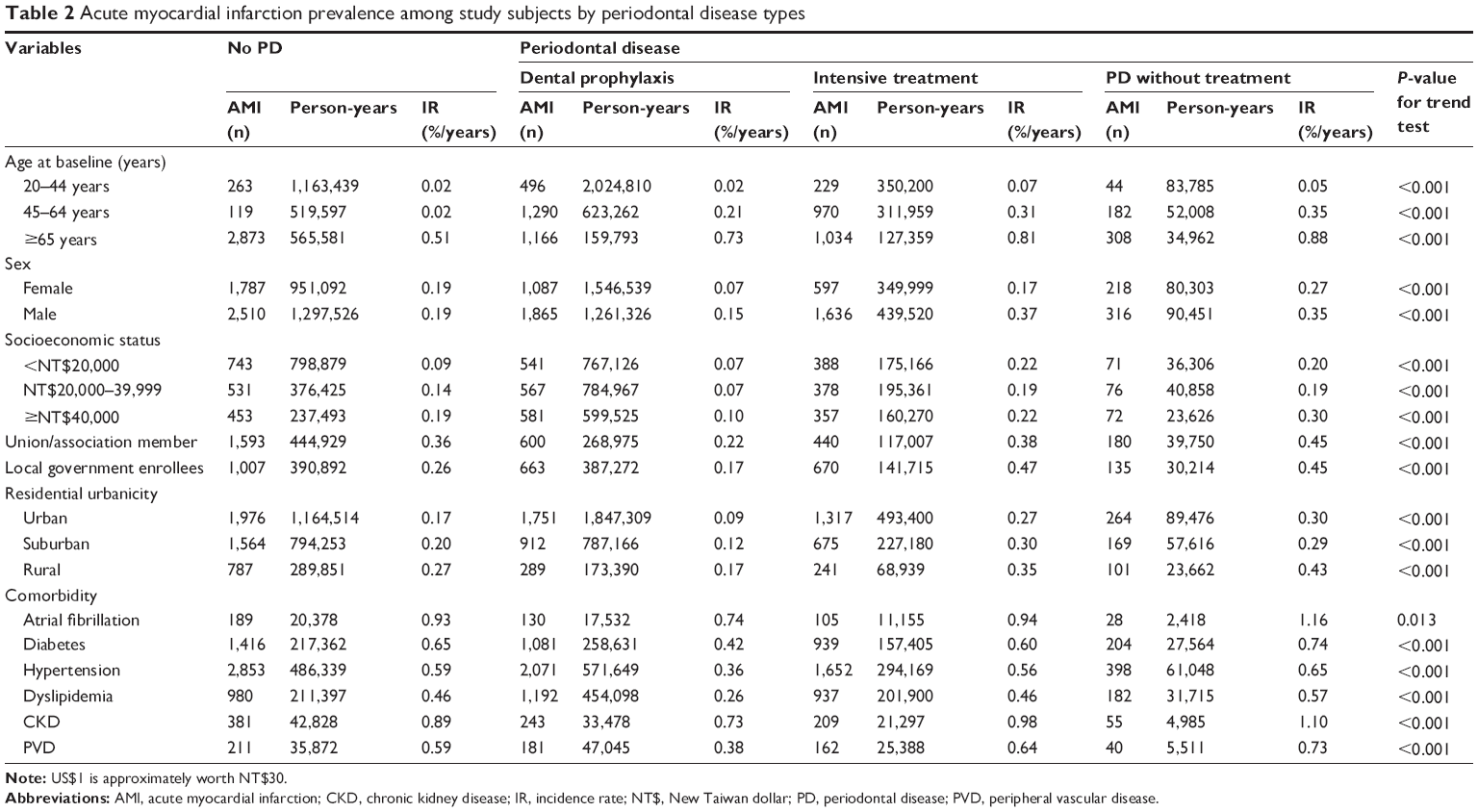 | Table 2 Acute myocardial infarction prevalence among study subjects by periodontal disease types |
Cox regression analysis adjusted for age, sex, socioeconomic status, residential urbanicity, and comorbidities showed that the HR of AMI was significantly lower in the dental prophylaxis group (HR =0.90, 95% CI =0.86–0.95) and higher in the intensive treatment (HR =1.09, 95% CI =1.03–1.15) and PD without treatment (HR =1.23, 95% CI =1.13–1.35) groups than among subjects with no PD (Table 3). The r2 correlate of the Cox regression model was 2.38%.
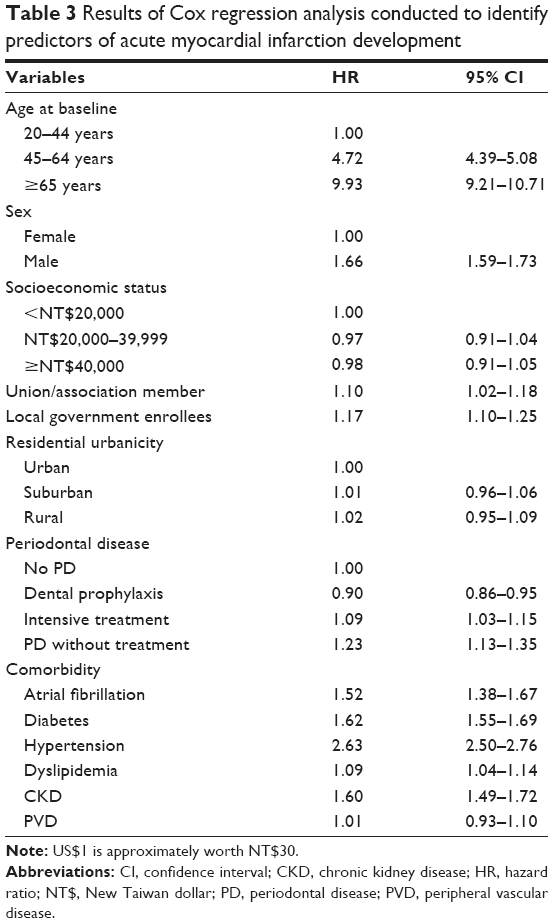 | Table 3 Results of Cox regression analysis conducted to identify predictors of acute myocardial infarction development |
Discussion
This is the first nationwide, population-based study to examine the strength of association between periodontal treatment and the incidence of AMI. The results of this study demonstrated that PD is a significant risk factor for AMI, and that dental prophylaxis protects against AMI development.
The findings support the concept that inflammatory diseases such as PD may play a role in the pathogenesis of AMI. The association of PD with the prevalence of CHD suggests that inflammation may be a potential mechanism involved in the regulation of the atherosclerotic process.26,27 PD may induce immune cells to secrete the inflammatory cytokines thromboxane A2, interleukin 1β, prostaglandin E2, and tumor necrosis factor α, which trigger and exacerbate atherogenetic and thromboembolic processes, resulting in CHD.26,28–30 Poor periodontal condition was also reported to be associated significantly with an increased concentration of C-reactive protein,31–34 a well-studied inflammatory marker and an independent predictor of CHD.35,36 In addition to circulating inflammatory factors, oral microbial organelles circulating in the blood have been proposed to lead to the increased incorporation of PD pathogens in atherosclerotic plaque.26,37 The attached PD pathogens can then adhere to vascular cells, inducing vascular infection and atherothrombosis and eventually causing AMI.38
The HRs among the different PD treatment groups were statistically significantly different. Sometimes this can be due to the very huge sample size used. However, the authors believe that the difference of HR among PD treatment groups had clinical significance. Other different approaches to PD-related conditions also showed a similar finding in the association with AMI. The National Health and Nutrition Examination Survey III cohort study found that patients with severe PD had a four-fold higher risk of myocardial infarction than those without PD.39 Infections of dental origin have also been documented in patients experiencing myocardial infarction.40 Periodontal pocket depth has been reported to be associated with the IR of AMI.19,20 Tooth loss, an indicator of PD history, was significantly related to carotid intima-media thickness, a strong predictor of myocardial infarction and stroke.37,41 Treatment of PD resulting in a beneficial effect on vascular diseases such as AMI and stroke was also reported.42–44 The results of a cross-sectional randomized clinical study suggested that nonintensive, Phase I periodontal therapy decreased serum immunoglobulin G and immunoglobulin M levels in patients who developed AMI.42 A 7-year cohort study by Chen et al showed that frequent tooth scaling reduced the IR and risk of AMI among subjects aged >50 years.43 In a previous study, it was found that dental prophylaxis reduced the risk of ischemic stroke in subjects with PD, especially those aged 20–44 years.44
Several limitations of this study must be considered. First, the use of administrative data and the retrospective design may have resulted in bias with respect to diagnoses. A further concern is the nonresponder bias/selection bias. Although the NHI program in Taiwan covered up to 99% of the nation’s inhabitants and provides free dental check-ups and prophylaxis twice a year to promote the prevention of PD, some PD patients may not be included in this NHI database because they did not have health insurance or did not seek treatment or check-up. However, the NHI Bureau routinely samples patient charts in different medical centers to validate database quality and minimize miscoding or misclassification. In addition, patients with PD were identified using both ICD-9-CM diagnostic codes and PD treatment codes in this study to minimize classification errors. Only patients with more than three outpatient visits were included in the analysis of AMI and comorbidities to reduce nondifferential misclassification bias. Second, the lack of information provided by the NHIRD on other risk factors for PD and AMI, such as education, family history, body mass index, and smoking status, could reduce the feasibility and accuracy of the interpretation of analytical outcomes. However, several recent studies have indicated that the significant associations of PD with AMI and recurrent cardiovascular events in patients developing myocardial infarction are independent of smoking status.34,45–47 PD has also been demonstrated to contribute to elevated C-reactive protein levels in nondiabetic, nonsmoking patients who have experienced AMI.48
Conclusion
The current study demonstrated that PD is correlated with the risk of AMI, and that dental prophylaxis can significantly reduce the IR of AMI. Patients who receive regular prophylactic dental treatment are more likely to have healthier periodontal conditions and less likely to have systemic chronic inflammatory reactions, resulting in a lower IR of AMI.
Disclosure
The authors report no conflicts of interest in this work. All authors take responsibility for all aspects of the reliability and freedom from bias of the data presented and their discussed interpretation.
References
Roger VL, Go AS, Lloyd-Jones DM, et al. Heart disease and stroke statistics – 2012 update: a report from the American Heart Association.Circulation. 2012;125(1):e2–e220. | ||
Management of stable angina pectoris. Recommendations of the Task Force of the European Society of Cardiology.Eur Heart J. 1997;18(3): 394–413. | ||
Greenland P, Knoll MD, Stamler J, et al. Major risk factors as antecedents of fatal and nonfatal coronary heart disease events.JAMA. 2003; 290(7):891–897. | ||
Kiechl S, Egger G, Mayr M, et al. Chronic infections and the risk of carotid atherosclerosis: prospective results from a large population study.Circulation. 2001;103(8):1064–1070. | ||
Dietrich T, Jimenez M, Krall Kaye EA, Vokonas PS, Garcia RI. Age-dependent associations between chronic periodontitis/edentulism and risk of coronary heart disease.Circulation. 2008;117(13):1668–1674. | ||
Sanz M, D’Aiuto F, Deanfield J, Fernandez-Aviles F. European workshop in periodontal health and cardiovascular disease – scientific evidence on the association between periodontal and cardiovascular diseases: a review of the literature.Eur Heart J Suppl. 2010;12(Suppl B):B3–B12. | ||
Albandar JM, Rams TE. Global epidemiology of periodontal diseases: an overview.periodontol 2000. 2002;29:7–10. | ||
Dye BA, Tan S, Smith V, et al. Trends in oral health status: United States, 1988–1994 and 1999–2004.Vital Health Stat 11. 2007;248:1–92. | ||
Albandar JM. Underestimation of periodontitis in NHANES surveys.J Periodontol. 2011;82(3):337–341. | ||
Petersen PE, Ogawa H. Strengthening the prevention of periodontal disease: the WHO approach.J Periodontol. 2005;76(12):2187–2193. | ||
Socransky S, Haffajee A. Microbiology of Periodontal Disease: introduction.Periodontology. 2005;38:9–12. | ||
Paster BJ, Boches SK, Galvin JL, et al. Bacterial diversity in human subgingival plaque.J Bacteriol. 2001;183(12):3770–3783. | ||
Pihlstrom BL, Michalowicz BS, Johnson NW. Periodontal diseases.Lancet. 2005;366(9499):1809–1820. | ||
de Oliveira C, Watt R, Hamer M. Toothbrushing, inflammation, and risk of cardiovascular disease: results from Scottish Health Survey.BMJ. 2010;340:c2451. | ||
Loesche WJ, Schork A, Terpenning MS, Chen YM, Kerr C, Dominguez BL. The relationship between dental disease and cerebral vascular accident in elderly United States veterans.Ann Periodontol. 1998;3(1):161–174. | ||
Wu T, Trevisan M, Genco RJ, Dorn JP, Falkner KL, Sempos CT. Periodontal disease and risk of cerebrovascular disease: the first National Health and Nutrition Examination Survey and its follow-up study.Arch Intern Med. 2000;160(18):2749–2755. | ||
Bahekar AA, Singh S, Saha S, Molnar J, Arora R. The prevalence and incidence of coronary heart disease is significantly increased in periodontitis: a meta-analysis.Am Heart J. 2007;154(5):830–837. | ||
Humphrey LL, Fu R, Buckley DI, Freeman M, Helfand M. Periodontal disease and coronary heart disease incidence: a systematic review and meta-analysis.J Gen Intern Med. 2008;23(12):2079–2086. | ||
Emingil G, Buduneli E, Aliyev A, Akilli A, Atilla G. Association between periodontal disease and acute myocardial infarction.J Periodontol. 2000;71(12):1882–1886. | ||
Geerts SO, Legrand V, Charpentier J, Albert A, Rompen EH. Further evidence of the association between periodontal conditions and coronary artery disease.J Periodontol. 2004;75(9):1274–1280. | ||
Andriankaja OM, Genco RJ, Dorn J, et al. The use of different measurements and definitions of periodontal disease in the study of the association between periodontal disease and risk of myocardial infarction.J Periodontol. 2006;77(6):1067–1073. | ||
Dogan B, Buduneli E, Emingil G, et al. Characteristics of periodontal microflora in acute myocardial infarction.J Periodontol. 2005; 76(5):740–748. | ||
Stein JM, Kuch B, Conrads G, et al. Clinical periodontal and microbiologic parameters in patients with acute myocardial infarction.J Periodontol. 2009;80(10):1581–1589. | ||
Hujoel PP, Drangsholt M, Spiekerman C, DeRouen TA. Periodontal disease and coronary heart disease risk.JAMA. 2000;284(11): 1406–1410. | ||
Howell TH, Ridker PM, Ajani UA, Hennekens CH, Christen WG. Periodontal disease and risk of subsequent cardiovascular disease in U.S. male physicians.J Am Coll Cardiol. 2001;37(2):445–450. | ||
Lockhart PB, Bolger AF, Papapanou PN, et al. Periodontal disease and atherosclerotic vascular disease: does the evidence support an independent association? A scientific statement from the American Heart Association.Circulation. 2012;125(20):2520–2544. | ||
Scannapieco FA, Bush RB, Paju S. Associations between periodontal disease and risk for atherosclerosis, cardiovascular disease, and stroke. A systematic review.Ann Periodontol. 2003;8(1):38–53. | ||
Stein JM, Smeets R, Reichert S, et al. The role of the composite interleukin-1 genotype in the association between periodontitis and acute myocardial infarction.J Periodontol. 2009;80(7):1095–1102. | ||
Lowe GD. The relationship between infection, inflammation, and cardiovascular disease: an overview.Ann Periodontol. 2001;6(1):1–8. | ||
Mustapha IZ, Debrey S, Oladubu M, Ugarte R. Markers of systemic bacterial exposure in periodontal disease and cardiovascular disease risk: a systematic review and meta-analysis.J Periodontol. 2007; 78(12):2289–2302. | ||
Wu T, Trevisan M, Genco RJ, Falkner KL, Dorn JP, Sempos CT. Examination of the relation between periodontal health status and cardiovascular risk factors: serum total and high density lipoprotein cholesterol, C-reactive protein, and plasma fibrinogen.Am J Epidemiol. 2000;151(3):273–282. | ||
Ridker PM, Silvertown JD. Inflammation, C-reactive protein, and atherothrombosis.J Periodontol. 2008;79(8 Suppl):1544–1551. | ||
Noack B, Genco RJ, Trevisan M, Grossi S, Zambon JJ, De Nardin E. Periodontal infections contribute to elevated systemic C-reactive protein level.J Periodontol. 2001;72(9):1221–1227. | ||
Deliargyris EN, Madianos PN, Kadoma W, et al. Periodontal disease in patients with acute myocardial infarction: prevalence and contribution to elevated C-reactive protein levels.Am Heart J. 2004;147(6): 1005–1009. | ||
Yeboah J, McClelland RL, Polonsky TS, et al. Comparison of novel risk markers for improvement in cardiovascular risk assessment in intermediate-risk individuals.JAMA. 2012;308(8):788–795. | ||
Di Napoli M, Schwaninger M, Cappelli R, et al. Evaluation of C-reactive protein measurement for assessing the risk and prognosis in ischemic stroke: a statement for health care professionals from the CRP Pooling Project members.Stroke. 2005;36(6):1316–1329. | ||
Desvarieux M, Demmer RT, Rundek T, et al. Periodontal microbiota and carotid intima-media thickness: the Oral Infections and Vascular Disease Epidemiology Study (INVEST).Circulation. 2005;111(5):576–582. | ||
Dorn BR, Dunn WA Jr, Progulske-Fox A. Invasion of human coronary artery cells by periodontal pathogens.Infect Immun. 1999;67(11): 5792–5798. | ||
Arbes SJ Jr, Slade GD, Beck JD. Association between extent of periodontal attachment loss and self-reported history of heart attack: an analysis of NHANES III data.J Dent Res. 1999;78(12):1777–1782. | ||
Willershausen B, Kasaj A, Willershausen I, et al. Association between chronic dental infection and acute myocardial infarction.J Endod. 2009; 35(5):626–630. | ||
Desvarieux M, Demmer RT, Rundek T, et al. Relationship between periodontal disease, tooth loss, and carotid artery plaque: the Oral Infections and Vascular Disease Epidemiology Study (INVEST).Stroke. 2003;34(9):2120–2125. | ||
Gunupati S, Chava VK, Krishna BP. Effect of Phase I periodontal therapy on anti-cardiolipin antibodies in patients with acute myocardial infarction associated with chronic periodontitis.J Periodontol. 2011; 82(12):1657–1664. | ||
Chen ZY, Chiang CH, Huang CC, et al. The association of tooth scaling and decreased cardiovascular disease: a nationwide population-based study.Am J Med. 2012;125(6):568–575. | ||
Lee YL, Hu HY, Huang N, Hwang DK, Chou P, Chu D. Dental prophylaxis and periodontal treatment are protective factors to ischemic stroke.Stroke. 2013;44(4):1026–1030. | ||
Andriankaja OM, Genco RJ, Dorn J, et al. Periodontal disease and risk of myocardial infarction: the role of gender and smoking.Eur J Epidemiol. 2007;22(10):699–705. | ||
Mattila KJ, Nieminen MS, Valtonen VV, et al. Association between dental health and acute myocardial infarction.BMJ. 1989; 298(6676): 779–781. | ||
Dorn JM, Genco RJ, Grossi SG, et al. Periodontal disease and recurrent cardiovascular events in survivors of myocardial infarction (MI): the Western New York Acute MI Study.J Periodontol. 2010;81(4): 502–511. | ||
Kodovazenitis G, Pitsavos C, Papadimitriou L, et al. Periodontal disease is associated with higher levels of C-reactive protein in non-diabetic, non-smoking acute myocardial infarction patients.J Dent. 2011;39(12): 849–854. |
 © 2015 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2015 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.