")
Back to Journals » Patient Preference and Adherence » Volume 16
Dental Patients’ Medical Information Disclosure and Sociodemographic Determinants: A Cross Sectional Study
Authors Bin Mubayrik A , Al Ali HH , Alomar SA, Alduweesh R, Alfurayh S, Alojaymi T, Tuwaym M
Received 10 October 2022
Accepted for publication 23 November 2022
Published 9 December 2022 Volume 2022:16 Pages 3195—3206
DOI https://doi.org/10.2147/PPA.S392837
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Johnny Chen
Azizah Bin Mubayrik,1 Hafsah Hassan Al Ali,2 Sadeem Ali Alomar,2 Reem Alduweesh,3 Shada Alfurayh,3 Tagreed Alojaymi,3 Malath Tuwaym3
1Oral Medicine and Diagnostic Science Department, College of Dentistry, King Saud University, Riyadh, Kingdom of Saudi Arabia; 2College of Dentistry, King Saud University, Riyadh, Kingdom of Saudi Arabia; 3General Practitioner, Riyadh, Kingdom of Saudi Arabia
Correspondence: Azizah Bin Mubayrik, Oral Medicine and Diagnostic Science Department, College of Dentistry, King Saud University, 3680 - King Saud University Unit No. 3ar, Riyadh, 12372-7453, Kingdom of Saudi Arabia, Email [email protected]
Objective: To evaluate the patient’s willingness to declare their medical history to their dentists against demographic and medical information.
Methods: A self-administered structured questionnaire regarding common chronic condition and pregnancy awareness and attitude toward medical information disclosure to their dentists was designed employing a five-point Likert-type scale. The questionnaire was distributed to among sample of adults. Data were collected and statistically analyzed using descriptive statistics, t-tests, ANOVA, and P values.
Results: A total of 573 questionnaires were completed. Only 61.3% were willing to share their medical history with the dentist and 76.1% will disclose previous complications of their condition in the dental office. Two third 71.9%of the sample will disclose about medications and 76.1% will disclose pregnancy month. There was lack of education regarding health conditions, 73.3% did not receive any information about their medications. While 72.8% did not receive any information regarding complications of their disease and 76.3% were not told what to do if complication arises.
Conclusion: The population’s willingness to reveal their medical information in the dental office is crucial. Though was within acceptable limit but still deficient. Age, education, occupation and marital status have a significant effect on disclosing and awareness. Educating patients and raising their awareness may aid in reducing emergencies, errors, and legal issues in the dental office.
Keywords: dental patients, medical conditions, disclosure, sociodemographic
Introduction
The importance of accurate dental records cannot be overlooked. It is essential for patient’s care, transfer, and quality control, thus improving care quality.1 An accurate and complete history requires effective communication with the patient.2 Active listening along with careful questioning are essential to obtain a thorough, accurate history.3 The greatest part of the medical history is obtained during the interview.3,4 A comprehensive and accurate medical history allows professionals to provide patients with the best of their abilities. Gathering a patient’s medical history gives the dentist an important direction and data that aid in diagnosing and treatment planning.3 AN inaccurate medical history can interfere with the correct diagnosis, safe management, and ultimately decision making.1–4 Hence, eliciting a comprehensive patient history is an essential tool to prevent undesired events during or after the treatment.1 It is worth mentioning that recording medical history usually relies on the information provided by the patient.2 It has been shown that in less than 13% of the visit time is given to talking to patients.5 A study was done by Beckman and Frankel reported that most patients struggle with expressing their concerns and only 23% of them were able to openly talk.6 In a narrative published in 2015 in respect with the medical history, the finding indicated that it assists in reaching an accurate diagnosis, a treatment plan modification, and a treatment prognosis because of the detailed information obtained.5 It has also a substantial effect on building patient rapport, providing information, education, and management.5
Increasing the awareness of health care providers and patients regarding the importance of accurate history taking is crucial for both sides. None of the reviewed English literature evaluated the patient’s willingness to disclose their medical conditions.5 The purpose of this study is to evaluate the patient’s willingness to declare their medical history to their dentists against demographic and medical information.
Materials and Methods
A cross-sectional survey was designed and distributed to explore the public’s attitudes and knowledge towards chairside dental screening and laboratory investigations. After reviewing the current literature on this topic, the researchers designed a structured, self-administered questionnaire to fulfill the study objectives. The questionnaire was developed in Arabic with different questioning types. The questionnaire was divided into the following three parts. Part 1 contained questions about demographic data; namely, age, sex, education level, occupation, marital status and last visit. Part 2 included questions related to information received by their treating dentists or physician on binary “yes or no” closed-ended questions. The third part contained a set of questions to gather information from research participants about awareness, willingness, and attitudes toward disclosing their medical histories to their attending dentists. It employed a five-point Likert-type scale with points on the scale indicating measures ranging from very important, important, neutral, unimportant, and totally unimportant, to indicate the extent to of agreement or disagreement or a neutral response. The participants were anonymous, and the questionnaire contained no identifiable information about the participants. Participation in this study was completely voluntary, and the questionnaire took approximately 5 minutes to complete. The questionnaire created using Google survey forms was distributed through social media outlets, such as Twitter and WhatsApp to convenient sample.
Statistical Analysis
Data was collected, analyzed, summarized, and presented in tables. All statistical analyses were performed using the Statistical Package for Social Sciences program (version 22). Descriptive statistics, such as frequency distributions, were performed. We used t-tests and one-way analysis of variance (ANOVA) to measure the relationship between variables. P values ≤.05 were considered statistically significant.
Ethics Approval and Informed Consent
The ethical approval was obtained from the Research Ethics Committee, Deanship of Scientific Research, King Saud University, Riyadh, Saudi Arabia (KSU-IRB 017E). Participation was voluntary, and consent was obtained prior to contribution. All participants were informed about the purpose of the study before contribution. This study was conducted in accordance with the Declaration of Helsinki.
Results
A total of 573 participants completed the survey. The majority of participants were females (73.9%). The sociodemographics and characteristics of the sample are summarized in Figures 1 and 2 and Table 1. Almost all participants (97%) had previously visited the dental office and (42.4%) received their dental therapy within the last 6 months (Figure 2).
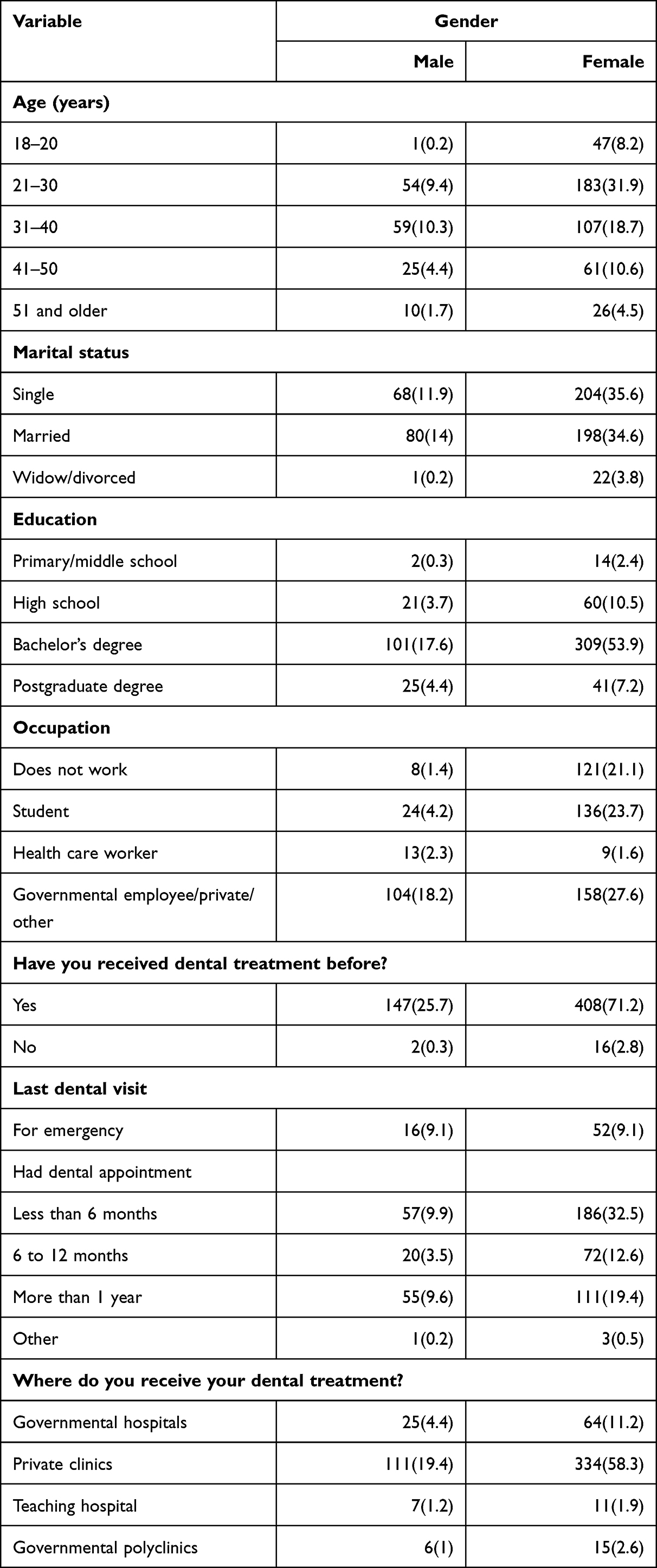 |
Table 1 Sociodemographic and Characteristics of the Sample |
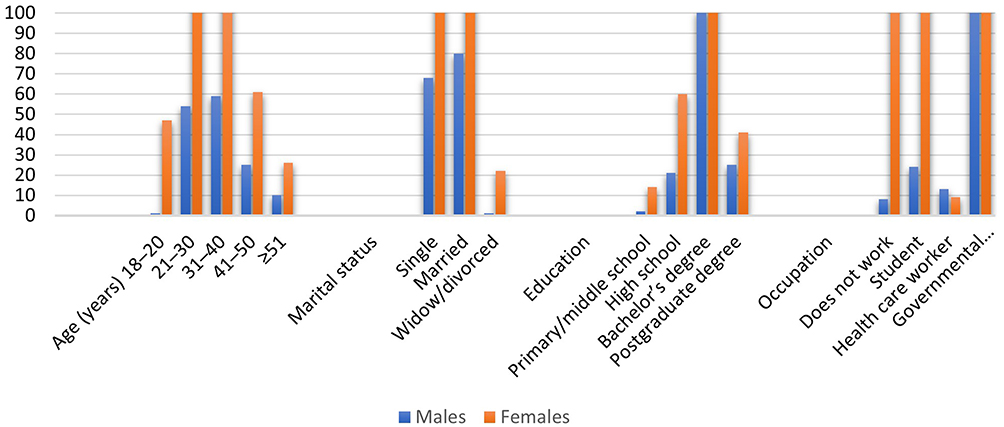 |
Figure 1 Sociodemographics and characteristics of the sample. |
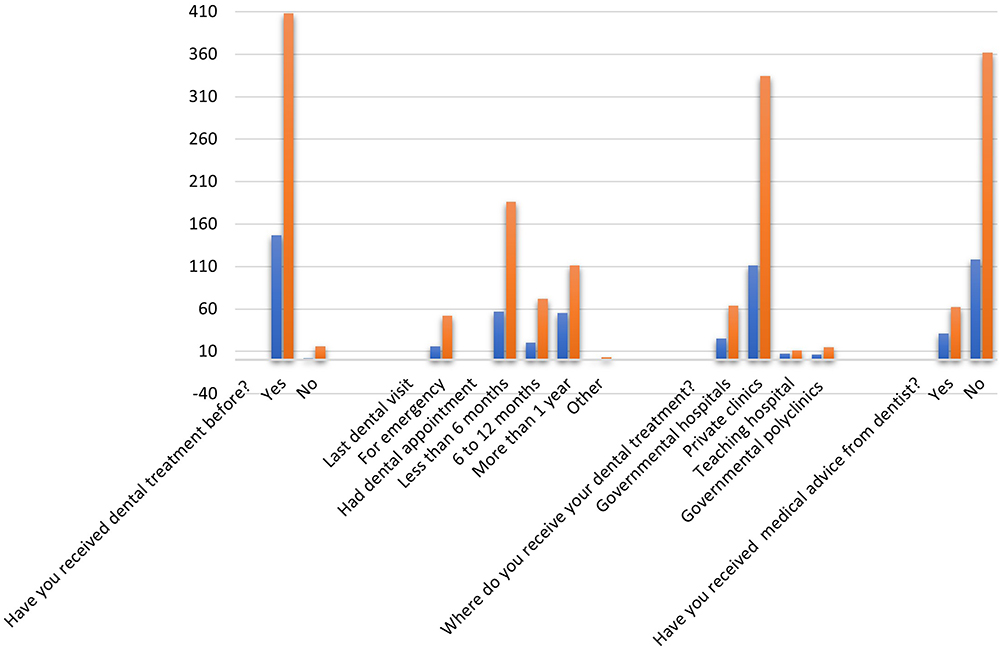 |
Figure 2 The sample of the characteristics regarding last visit, hospital and consultation from a dentist regarding medical condition. |
Figure 3 and Table 2 show the responses of the participants regarding information received by their treating dentists. Almost three-quarters of the sample’s participants (72.8%) revealed that they did not receive any information from their treating dentist regarding any possible complications from a disease or drugs. Similarly, 61.4% of participants have not been told about any possible mouth symptoms due to a disease or using medicines or interference with anesthesia (61.3%). Likewise, (75.7%) were not alerted about any medication complications with dental treatment. Four hundred thirty-seven participants (76.3%) were not told what to do if a complication arose and 80.6% of the participants have not alerted or heard the instructions about the appropriate vital signs to perform dental treatment.
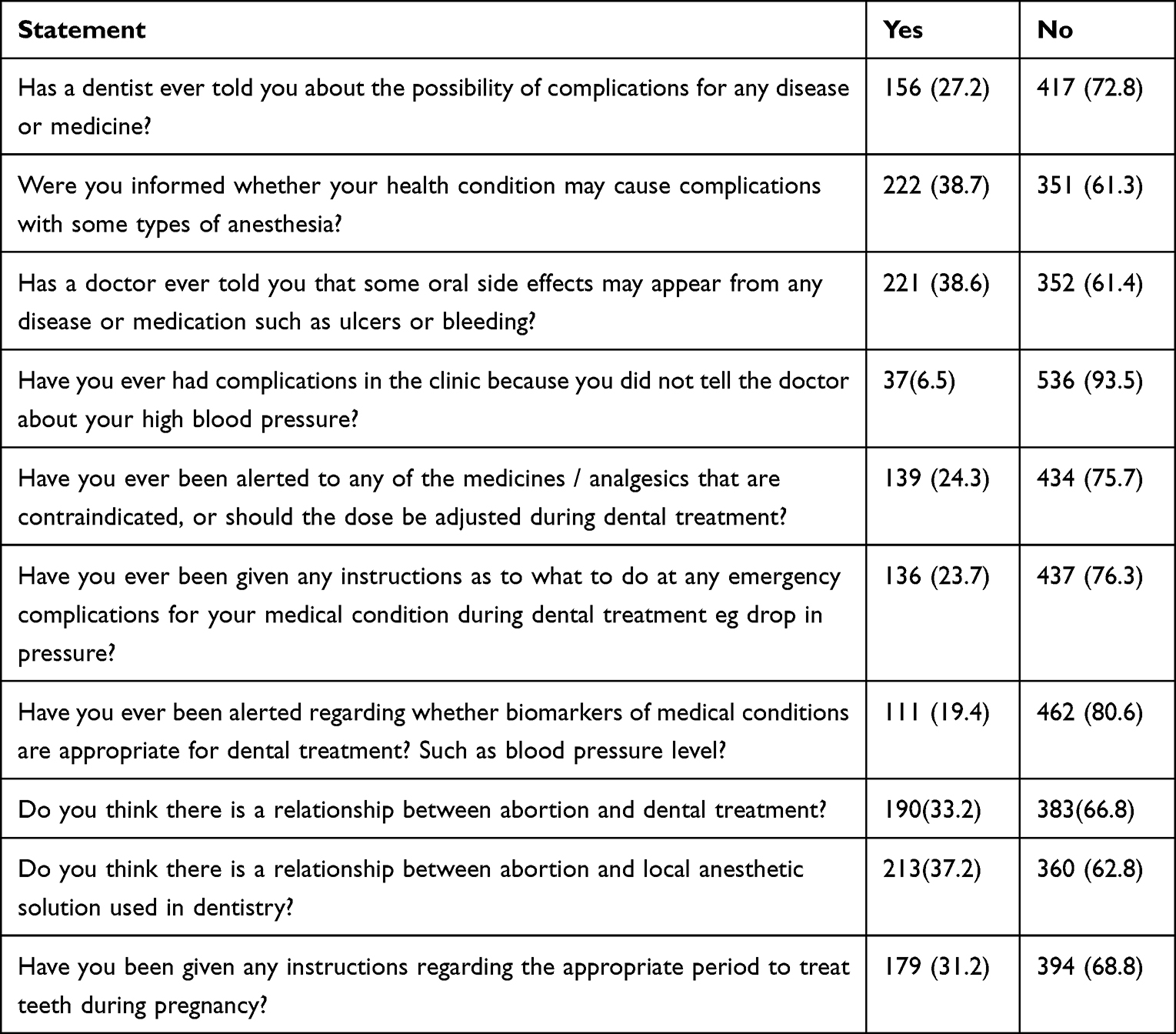 |
Table 2 Responses of Participants Regarding Information Received by Their Treating Dentists/Physician |
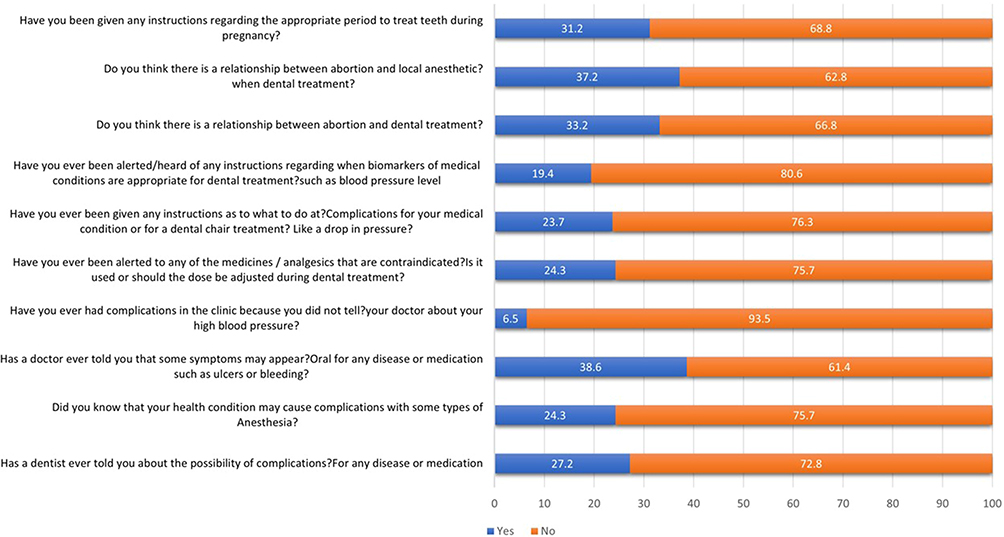 |
Figure 3 Graphical representations of the responses of the participant regarding information received by their treating dentist in percentage. |
Table 3 shows the willingness and attitudes of the study participants to declare their medical history to their treating dentist. More than half of the sample (61.3%, n=351) were willing to tell their dentist about any disease before performing a dental procedure. Forty-four (44.1%) of the participants also think that giving their treating dentist the name and the number of their supervising doctor is important. As regards to their knowledge and awareness of common oral diseases the results are summarized in Table 3.
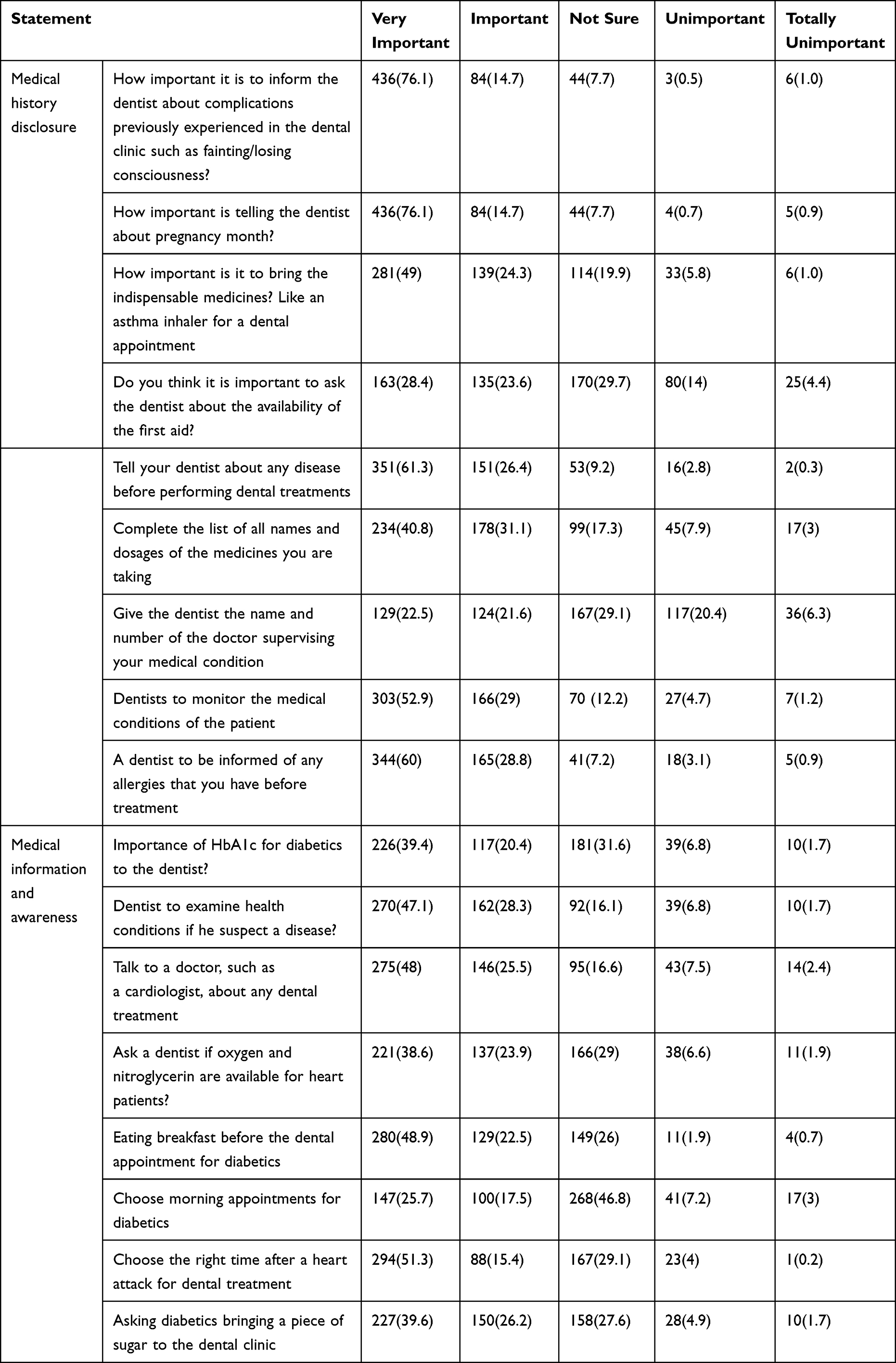 |
Table 3 Awareness, Willingness, and Attitudes of the Study Participants to Declare Their Medical Status to Their Treating Dentists |
The significance of association between disclosure and sociodemographic data is represented in Tables 4 and 5. There was no significant association between gender and disclosure.
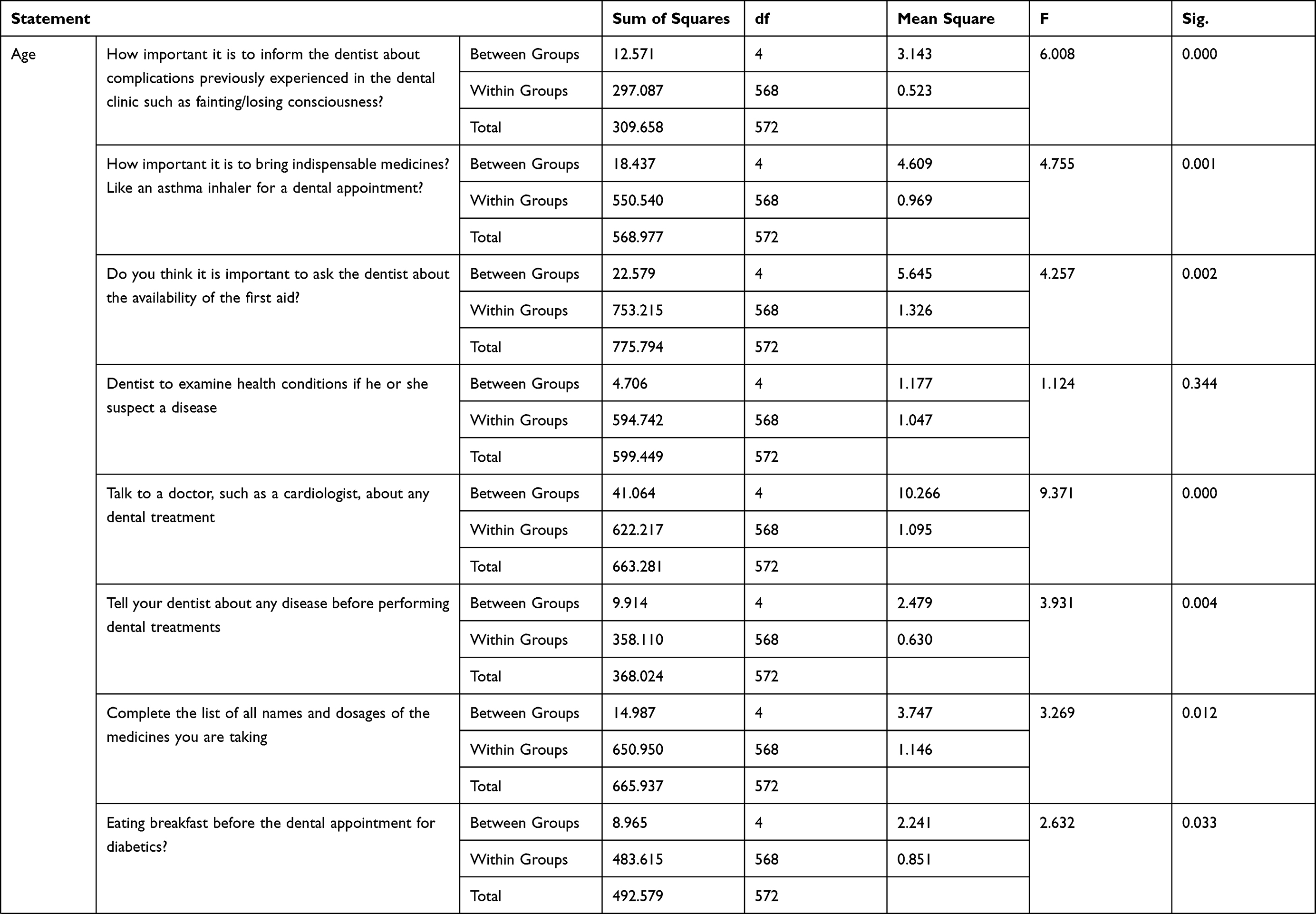 | 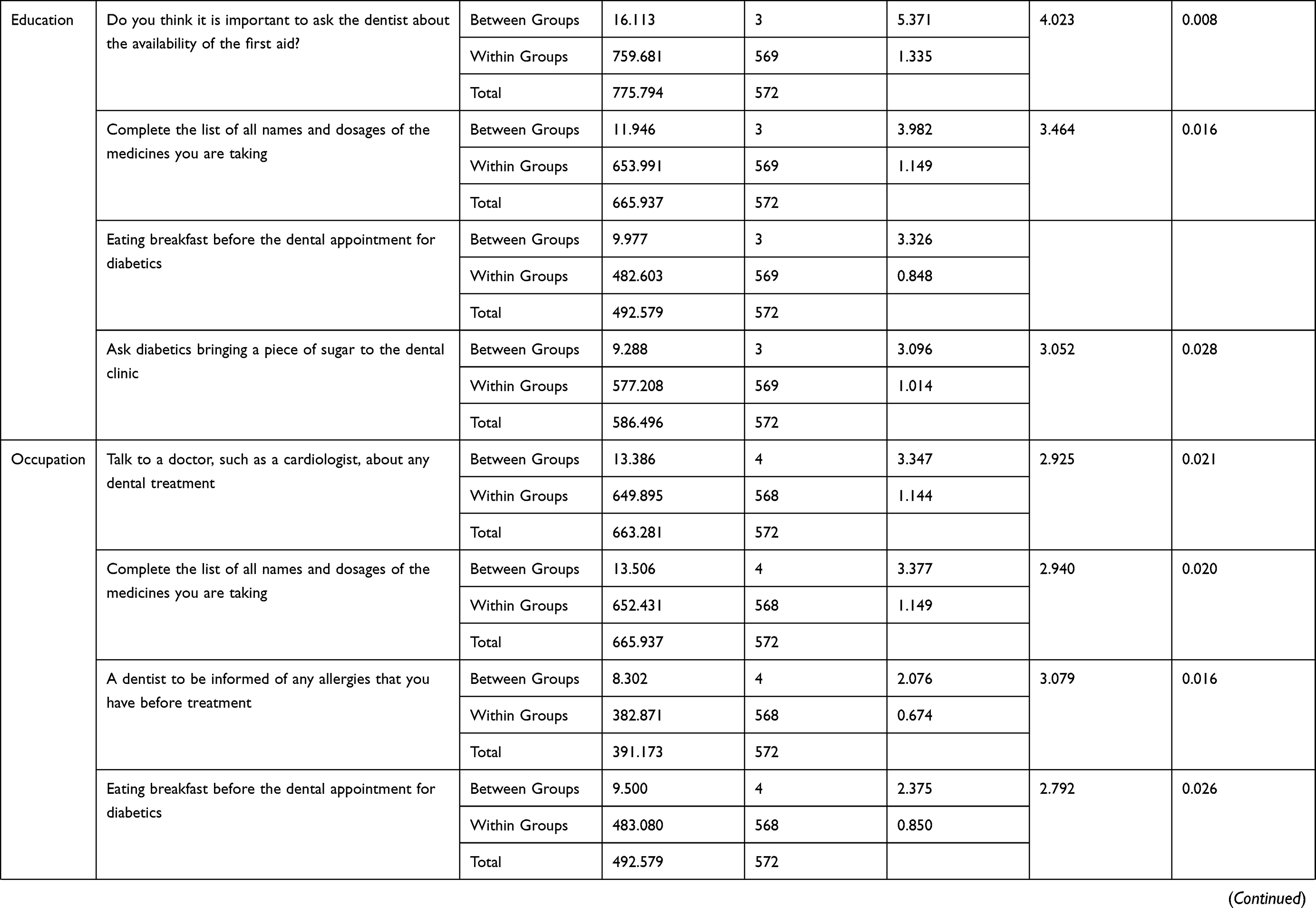 | 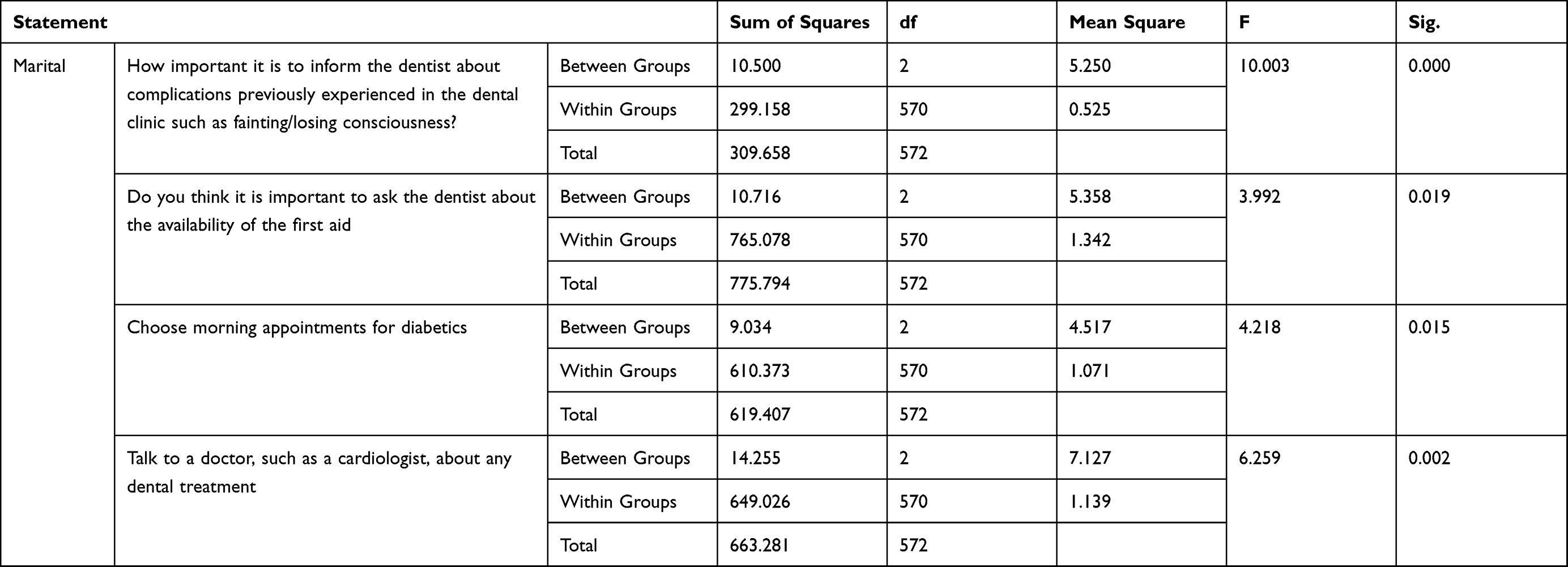 |
Table 4 Disclosure of Medical History versus Sociodemographic Data |
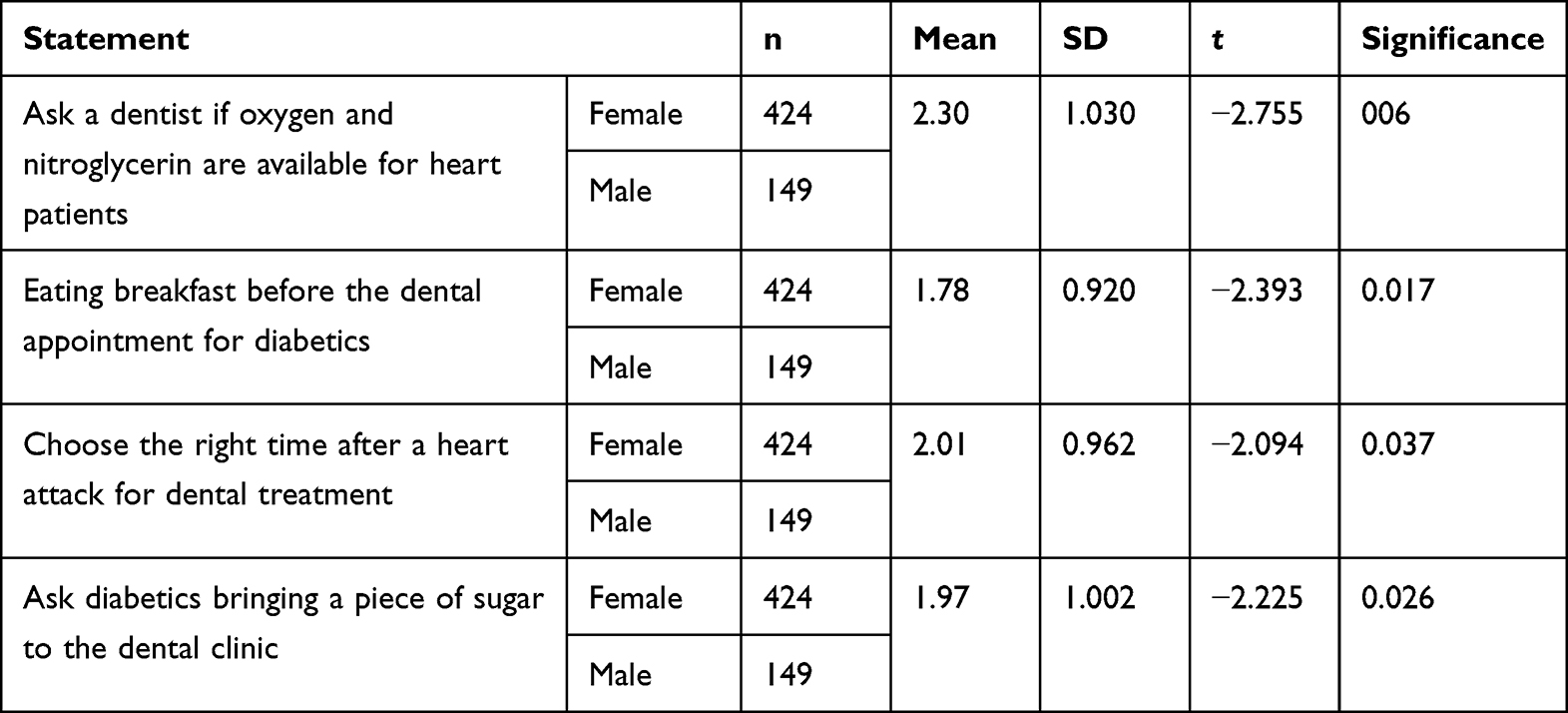 |
Table 5 t-test for the Analysis of Association Between Genders Regarding Medical Condition Information in the Dental Office |
Discussion
The medical history is an important foundation for the dentist’s diagnosis, treatment planning, and prevention of potential complications. It aids in identifying undiagnosed cases and high-risk individuals to preclude emergencies in dental clinics. In general, most of the sample thought that it is important to declare their medical history to their dentists. Updating and revising medical history are essential to anticipate possible medical emergencies and to minimize risk.7
Our investigation revealed that most of the participants agreed that informing the dentist about any disease before therapy is essential prior to dental treatment. Medical emergencies in the dental office even though rare can be life-threatening. It has been reported that an accurate medical history aids in emergency prevention,8 ensuring effective and safe dental management particularly for inevitable dental emergencies in the dental office. Acquiring a patient’s history depends mostly on the patient’s understanding and skillful communication. It is therefore essential to train the students to develop communication skills.9 Obtaining history through automated self-reporting touch screen tablets has been reported to be effective and satisfactory.10 Barriers to sufficient history taking such as lack of time should be addressed and tackled for both the practitioner and the patient.
Despite the participants’ agreement on the importance of disclosure, most of them did not receive health education from their dentists. It has been shown that a lack of professional communication reduces the trust and the compliance of the patients.9 Similarly, education increases compliance of patients. It also aids in patients’ self-care and monitoring of diseases so they can get prompt, appropriate medical care.11,12 An accurate history requires good communication with the patient and guardian along with collaborating with the physician.13
Even though most of the participants believed that it is crucial to inform a dentist about pregnancy, our study indicated the lack of knowledge in regard to pregnancy and dental care. Similar results were reported in the literature among females.14,15 This may demand the institution of patient education and updating by obstetricians and dentists.
Overall, our investigation revealed acceptable awareness concerning common chronic diseases. However, there was a deficiency in knowledge as regards to the importance of emergency equipment availability. It is crucial that the patients get professional health education on their diseases, including information on potential emergencies, preparation and response strategies/ procedures, Studies have shown that health education improves patients’ compliance and persistence.11,12,16
Our results indicated gender disparities in terms of information on common medical conditions. Males were more to know and ask about emergency equipment and management. This could be explained by the fact that males are more affected by chronic diseases such as cardiovascular diseases.
Our investigation indicated that age, education, occupation, and marital status are important predictors in the disclosure of medical history to their dentists. Al-Khashan et al reported there was a difference in the needs, barriers, and preferences of health education.17 Those differences could explain the disparities in disclosure. Health education should be carried out with an emphasis on transparency by the patient to ensure safety. These variations may account for the discrepancies in disclosure. To maintain a patient’s safety, health education should place a strong emphasis on transparency.
To the best of knowledge this is the first study investigating patient disclosure in the reviewed English literature. Further studies are required to ascertain the results including barriers to disclosure.
Conclusion
Our findings suggested that healthcare professionals are not adequately educating patients on their health. Collaboration among medical professionals to manage a patient may help with the patient’s education and understanding of the relationship between medical issues and dental management. This may also aid in reducing medical errors and legal issues in the field. Continuous health care training and education may improve professionals’ patient education quality. Additionally, our investigation demonstrated a decent readiness to reveal health issues for the treating dentist. However, disclosure was affected by sociodemographic characteristics.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Yarmohammadian MH, Raeisi AR, Tavakoli N, Nansa LG. Medical record information disclosure laws and policies among selected countries; a comparative study. J Res Med Sci. 2010;15(3):140–149.
2. Collier A. The importance of adequate history taking in dentistry. Dent Nurs. 2014;10(5):288–290. doi:10.12968/denn.2014.10.5.288
3. Muhrer JC. The importance of the history and physical in diagnosis. Nurse Pract. 2014;39(4):30–35. doi:10.1097/01.NPR.0000444648.20444.e6
4. Greenwood M. Essentials of medical history-taking in dental patients. Dent Update. 2015;42(4):308–315. doi:10.12968/denu.2015.42.4.308
5. Mortazavi H, Rahmani A, Rahmani S. Importance, advantages, and objectives of taking and recording patient’s medical history in dentistry. Int J Med Rev. 2015;2(3):287–290.
6. Beckman HB, Frankel RM. The effect of physician behavior on the collection of data. Ann Intern Med. 1984;101(5):692–696. doi:10.7326/0003-4819-101-5-692
7. Jevon P. Medical emergencies in the dental practice poster: revised and updated. BDJ Team. 2020;7(10):38–46. doi:10.1038/s41407-020-0474-y
8. Shampaine GS. Patient assessment and preventive measures for medical emergencies in the dental office. Dent Clin North Am. 1999;43(3):383–400. doi:10.1016/S0011-8532(22)00798-4
9. Polova EA, Antonova EA, Semeleva EI. The analysis of the medical information needs for patients in dentistry. Juvenis Scientia. 2021;7(2):27–33. doi:10.32415/jscientia_2021_7_2_27-33
10. Arora S, Goldberg AD, Menchine M. Patient impression and satisfaction of a self-administered, automated medical history taking device in the emergency department; 2014. Available from: https://search-ebscohost-com.sdl.idm.oclc.org/login.aspx?direct=true&db=edssch&AN=edssch.oai%3aescholarship.org%2fark%3a%2f13030%2fqt8px936m7&site=eds-live.
11. Gold DT, McClung B. Approaches to patient education: emphasizing the long-term value of compliance and persistence. Am J Med. 2006;119(4 Suppl 1):S32–7. doi:10.1016/j.amjmed.2005.12.021
12. Sharaf F. Impact of health education on compliance among patients of chronic diseases in Al Qassim, Saudi Arabia. Int J Health Sci. 2010;4(2):139–148.
13. Gusmini MA, De Sa AC, Feng C, Arany S. Predictors of dental complications post‐dental treatment in patients with sickle cell disease. Clin Exp Dent Res. 2021;7(1):11–19. doi:10.1002/cre2.335
14. Soegyanto AI, Larasati RN, Wimardhani YS, Özen B. Mother’s knowledge and behaviour towards oral health during pregnancy. Pesquisa Brasileira em Odontopediatria e Clínica Integrada. 2020;20. doi:10.1590/pboci.2020.113
15. Pattanshetti K, Kothari HP, Tiwari J, et al. Assessment of knowledge and attitude of expectant mothers regarding effect of their oral health and its influence on the infant oral health. Int J Clin Pediatr Dent. 2020;13(5):471–475. doi:10.5005/jp-journals-10005-1817
16. Shetty M, Alva H, Hegde C, Krishna DP. Medical and dental emergencies and complications in dental practice and its management. J Educ Ethics Dent. 2013;2:13. doi:10.4103/0974-7761.115144
17. Al-Khashan HI, Almulla NA, Galil SA, Rabbulnabi AA, Mishriky AM. Gender differences in health education needs and preferences of Saudis attending Riyadh Military Hospital in the Kingdom of Saudi Arabia. J Family Community Med. 2012;19(3):172–177. doi:10.4103/2230-8229.102317
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.