Back to Journals » Clinical, Cosmetic and Investigational Dentistry » Volume 8
Dental management in patients with hypertension: challenges and solutions
Authors Southerland JH, Gill DG, Gangula PR, Halpern LR, Cardona CY, Mouton CP
Received 29 October 2015
Accepted for publication 10 March 2016
Published 17 October 2016 Volume 2016:8 Pages 111—120
DOI https://doi.org/10.2147/CCIDE.S99446
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Christopher E. Okunseri
Janet H Southerland,1 Danielle G Gill,1 Pandu R Gangula,2–4 Leslie R Halpern,1 Cesar Y Cardona,5 Charles P Mouton6
1Department of Oral and Maxillofacial Surgery, 2Department of Oral Biology and Research, 3Department of Physiology, 4Center for Women's Health Research, 5Department of Internal Medicine, 6Department of Family and Community Medicine, Meharry Medical College, Nashville, TN, USA
Abstract: Hypertension is a chronic illness affecting more than a billion people worldwide. The high prevalence of the disease among the American population is concerning and must be considered when treating dental patients. Its lack of symptoms until more serious problems occur makes the disease deadly. Dental practitioners can often be on the frontlines of prevention of hypertension by evaluating preoperative blood pressure readings, performing risk assessments, and knowing when to consider medical consultation of a hypertensive patient in a dental setting. In addition, routine follow-up appointments and patients seen on an emergent basis, who may otherwise not be seen routinely, allow the oral health provider an opportunity to diagnose and refer for any unknown disease. It is imperative to understand the risk factors that may predispose patients to hypertension and to be able to educate them about their condition. Most importantly, the oral health care provider is in a pivotal position to play an active role in the management of patients presenting with a history of hypertension because many antihypertensive agents interact with pharmacologic agents used in the dental practice. The purpose of this review is to provide strategies for managing and preventing complications when treating the patient with hypertension who presents to the dental office.
Keywords: high blood pressure, dental, guidelines, inflammation, metabolic disease, blood pressure medicines
Introduction
Hypertension is known as the “silent killer” and affects 80 million adults older than 20 years in the US alone1 and just <1 billion people worldwide.1–3 By 2025, the number of patients diagnosed with hypertension is expected to be 1.56 billion.3 Hypertension is responsible for >7 million deaths annually4 and is one of the leading risk factors for cardiovascular disease mortality.5 The disease is defined as systolic blood pressure (SBP) of 140 mmHg or diastolic blood pressure (DBP) ≥90 mmHg, or any persons being currently prescribed antihypertensive medicine for the purpose of managing hypertension.1,2,6 In addition, hypertension is defined as blood pressure readings elevated on at least two occasions with or without provocation.1
Hypertension is divided into two main categories: essential/primary hypertension and secondary hypertension.7,8 Lack of identifiable causative factors for elevated blood pressure is known as essential or primary hypertension, making up ~90%–95% of all hypertensive cases. Secondary hypertension, for which there is an identifiable cause, affects 5%–10% of US adults who are diagnosed with hypertension.2,7,9 Disorders associated with secondary hypertension include vascular diseases such as coarctation of the aorta and systemic diseases such as Cushing’s syndrome; obstructive sleep apnea; adrenal medullary dysfunction; and hormonal dysfunction, ie, primary hyperaldosteronism, pheochromocytoma, hyperthyroidism, hyperparathyroidism, and hypothyroidism. Other factors contributing to hypertension include substance abuse, alcohol consumption, contraceptive use, and chronic kidney disease.2,7,10–12
It is estimated that 17.3% of the 80 million US adults with hypertension are undiagnosed.1 Undiagnosed hypertension has been proven to shorten a life span by 10–20 years.13 The number of people with hypertension in the US and worldwide, the number of people with undiagnosed hypertension, and the future growth of the disease make hypertension a public health concern. It is important that the oral health care practitioner is well versed on the challenges involved in prevention, management, and treatment options for this population of patients, as well as on the available opportunities that may improve overall patient care and treatment outcomes in the dental office. The role of the dental practitioner as a part of the overall health care team is often overlooked but should be considered important in screening for hypertension. An entry point for many individuals in the general population into the health care system may indeed be a dental visit, as dental disease represents a significant problem, specifically as it relates to pain and infection. Thus, dental practitioners can play a vital role in screening for undiagnosed hypertension, with subsequent referral to a medical practitioner, thereby having an impact on both morbidity and mortality.
The purpose of this review article is to provide an overview of concerns regarding treating patients with hypertension and provide recommendations that are helpful in managing a broad spectrum of these patients who present to the dental office.
Classification and guidelines
The American Heart Association recommends routine blood pressure screenings starting at the age of 20 years and then at least every 2 years with blood pressures <120/80 mmHg. The reports of the Seventh and Eighth Joint National Committee (JNC-7 and JNC-8) provide guidelines for blood pressure management and treatment.14,15 The JNC-8 panel stated that the >140/90 mmHg definition for hypertension from the JNC-7 report remains the standard for diagnosis of individuals who do not have additional comorbidities. The current references for evaluation of hypertension outline normal blood pressure as SBP <120 mmHg and DBP <80 mmHg, prehypertension as SBP 120–139 mmHg or DBP 80–89 mmHg, Stage I hypertension as SBP 140–159 mmHg or DBP 90–99 mmHg, and Stage II hypertension as SBP ≥160 mmHg or DBP ≥100 mmHg (Table 1).9,14 A blood pressure measuring >180/120 mmHg with or without end-organ damage is considered hypertensive crisis. Finally, persistently elevated blood pressure in an office setting in patients who have had no previous elevated readings within a 24-hour period is considered “white coat” hypertension.9,12 White coat hypertension is confirmed by home blood pressure readings of <135/85 mmHg or 24-hour ambulatory blood pressure monitoring with results showing readings of <130/80 mmHg.16 Hypertension in the setting of certain systemic illnesses such as diabetes and chronic kidney dysfunction requires judicious monitoring to achieve a target blood pressure of <130/80 mmHg.1,14,15
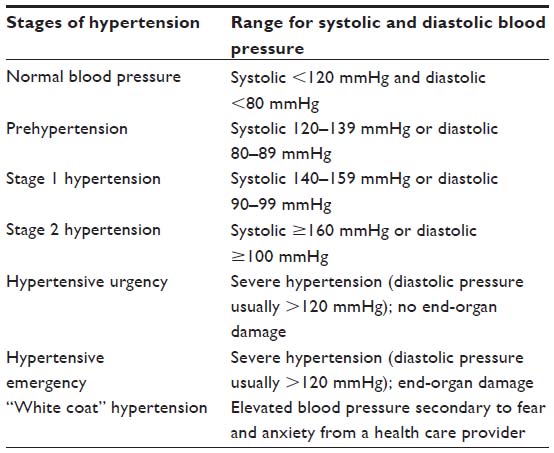 | Table 1 Classification of hypertension according to the JNC6 and JNC714,17 |
It is important to be comfortable with identifying disorders associated with hypertenison and making decisions about proper treatment planning which would include emergent evaluation as needed for treatment as well as outpatient referral and follow up. Obtaining blood pressure readings before the administration of local anesthesia provides a baseline status to identify those who may be medically unstable to undergo treatment. This practice should be invoked for both new and routine patients.11 This practice allows dental practitioners to treat patients in a safer environment as well as improving overall health outcomes for patients diagnosed with hypertension by referring patients early for hypertension management.
Blood pressure can be easily measured via the auscultatory method with a mercury, aneroid, or hybrid sphygmomanometer.11 The mercury sphygmomanometers are considered the most accurate devices to measure blood pressure, but the use of these devices has decreased.12 Aneroid devices are the type most commonly used in dental offices. They are easy to use; however, they require regular calibration at least every 6 months.12 Automatic digital devices for the arm, wrist, or finger are also widely used among practicing physicians and patients who monitor their pressures at home. It is recommended that they too be regularly calibrated to ensure they are accurate.11
Proper technique for obtaining accurate blood pressure measurements mandates that a patient be seated quietly for at least 5 minutes in a chair, feet on the floor and arms supported at heart level.2,9 An appropriate-sized cuff, a cuff bladder that encircles at least 80% of the arm, should be used to ensure accuracy and at least two measurements should be taken during the visit.2,12,11
For those patients who are normotensive or with prehypertension, providing thorough education is key to prevention. Explaining risk factors (Table 2) associated with the disease and providing advice on lifestyle modifications, such as weight loss, diet modifications (dietary approaches to stop hypertension or DASH), decreased sodium intake, increased physical activity, and restricted alcohol intake could prove to be life saving in this population.11,12,14
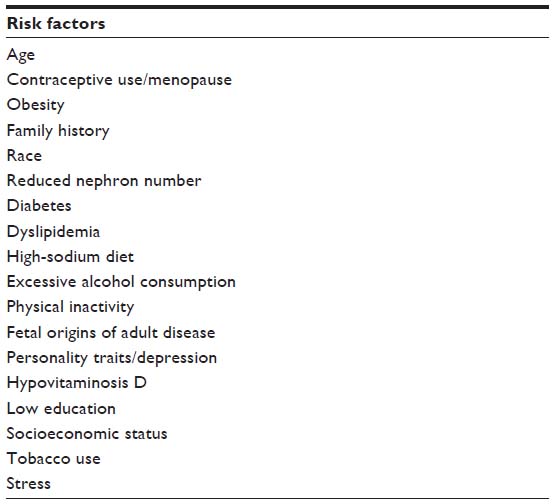 | Table 2 Risk factors for primary hypertension according to the JNC617 |
Pharmacology of antihypertensive medications
Medications used in the treatment of hypertension are substantial and cover a variety of categories in terms of their function and action. The physiologic/pharmacologic mechanism(s) of action of most antihypertensive medications is (are) via baroreceptors and the adrenergic pathway(s) centrally, as well as through peripheral pathways via the renin–angiotensin–aldosterone system.8 Antihypertensives can be administered as monotherapy or as a combination of two or more agents to reach a blood pressure target of <150/90 mmHg or 130–140/90 mmHg for individuals with moderate-to-severe renal/diabetic disease(s).1 The literature suggests almost equivalent blood pressure-lowering effects of the following six major classes of antihypertensive agents when used as monotherapy: thiazide diuretics, beta-blockers, angiotensin-converting enzyme inhibitors (ACEIs), angiotensin II receptor blockers, calcium channel blockers (CCBs), and alpha-2 blockers. Standard doses of most antihypertensive agents reduce blood pressure by 8–10/4–7 mmHg.21 The dental provider should be familiar with medications that could potentially adversely affect blood pressure control (Table 3), as well as commonly prescribed antihypertensive medications, their side effects, and drug–drug interactions (Table 4). The major antihypertensive groups are discussed in the following sections.
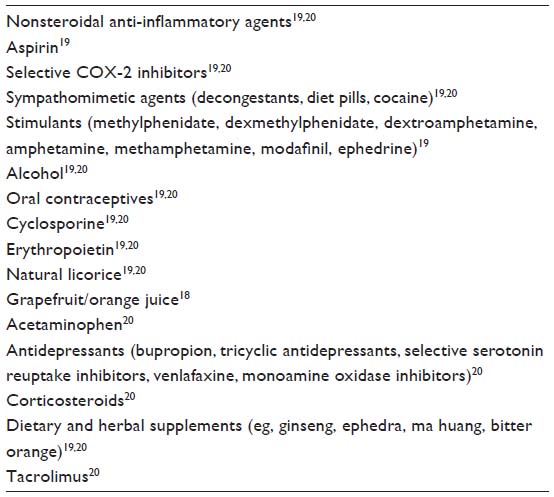 | Table 3 Factors that interfere with control of blood pressure |
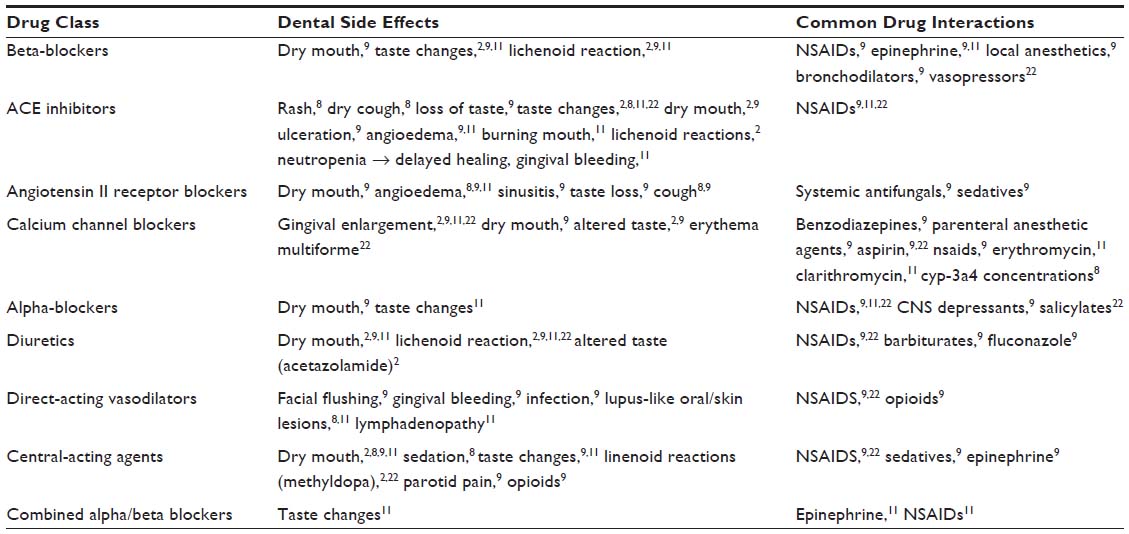 | Table 4 Common antihypertensive drug classes, dental side effects, and drug–drug interactions |
Diuretics
By altering the way the kidney controls sodium, diuretics promote the production of urine by increasing the excretion of sodium and water from the bodies, decreasing blood volume, and therefore, decreasing blood pressure.8 This regulation of sodium and water occurs at various segments of the renal tubular system.8 Diuretics used in the management of hypertension include loop, thiazides, and potassium-sparing diuretics. Examples of commonly used diuretics include thiazide-type diuretics such as chlorthalidone, hydrochlorothiazide, and indapamide. The other class of diuretics includes the loop diuretics (furosemide, torsemide, bumetanide, and ethacrynic acid) and potassium-sparing diuretics (spironolactone, amiloride, triamterene, and eplerenone).8 Side effects associated with this class of medications include hypokalemia, hyperlipidemia, constipation, hyperglycemia, muscle cramps, headache, increased perspiration, volume depletion that may lead to extreme thirst and dry mouth, and orthostatic hypotension.23 Ototoxicity, most likely associated with ethacrynic acid use, is also an associated adverse effect.8 Ototoxicity occurs most frequently in settings of rapid intravenous administration and is least likely to occur oral administration; it can manifest as a constellation of symptoms that include tinnitus, hearing impairment, deafness, vertigo, and a sense of fullness behind the ears. These are symptoms that patients may relay to their dental practitioner.24 Adverse drug–drug interactions with diuretics are commonly seen with nonsteroidal anti-inflammatory drugs (NSAIDs) (resulting in a decreased antihypertensive effect), concomitant barbiturate use (resulting in orthostatic hypertension), and elevated plasma levels of fluconazole and erythromycin when used simultaneously.23
Beta-blockers
Beta-blockers are drugs that bind to beta-adrenoceptors, reducing the rate and contractility of the heart9 and ultimately affecting cardiac output.8 Beta-blockers are further divided into two subgroups, cardioselective and nonselective beta-blockers. Cardioselective beta-blockers act on beta-1 receptors, avoiding the beta-2 receptors of the lungs and vascular smooth muscle cells. Examples include metoprolol, atenolol, nebivolol,8 and bisoprolol.23 Nonselective beta-blockers include carvedilol, propranolol, nadolol,8 and sotalol.23 Common side effects include bradycardia, hypotension, dizziness, shortness of breath, and fatigue.8,21 Adverse drug–drug interactions with NSAIDs can lead to decreased antihypertensive effects.23 Interactions with local anesthetics can lead to a decreased rate of amide metabolism when taken concomitantly with beta-blockers.25
ACE inhibitors
ACEIs function by decreasing the production of angiotensin II, increasing bradykinin levels, reducing sympathetic nervous system activity, and decreasing cardiac workload.8 The commonly prescribed drugs include captopril, enalapril, lisinopril, benazepril, and ramipril.23 Adverse effects from ACEIs may cause a dry and nonproductive cough, angioedema, hypotension, headache, weakness, and abnormal taste.23 ACEIs may also be implicated in acute kidney injury owing to their effect of decreasing angiotensin II production and, in essence, resulting in decreased ability to constrict the efferent arteriole and maintain glomerular filtration when renal perfusion is low. Susceptible patients include those with bilateral renal artery stenosis or unilateral stenosis in the setting of a single kidney. Patients with volume depletion due to decreased by-mouth intake in the setting of recent dental manipulation, diarrhea, or intake of diuretics can also potentially be at risk.24 Concomitant use of cyclosporines with ACEIs may contribute to an increased risk of acute renal failure, while concomitant use of NSAIDs may lead to antihypertensive effects similar to those seen with beta-blockers; but the latter may also lead to increased risk of acute kidney injury, especially in patients who are volume depleted.23,26
Angiotensin II receptor blockers
Angiotensin II receptor blockers are a group of antihypertensive agents that selectively inhibit angiotensin II via competitive inhibition of the angiotensin II receptor.21 This causes a vasodilatory response of the blood vessels in the glomerulus and a concomitant drop in blood pressure.27 Drugs prescribed in this category are irbesartan, candesartan, telmisartan, olmesartan, losartan, and valsartan.28 Adverse effects present similarly to ACEIs; however, cough and angioedema are significantly less.8 Losartan, due to its association with the cytochrome P450 system, is potentially likely to interfere with other drugs, such as cimetidine, fluconazole, indomethacin, phenobarbital, and rifampin.28
Calcium channel blockers
CCBs or calcium channel antagonists reduce vascular resistance through L-channel blockade, which reduces intracellular calcium, causing vasodilation. By blocking calcium entry into the cell, CCBs can stimulate vascular smooth muscle relaxation (vasodilation), in addition to provoking a negative ionotropic and chronotropic effect. This causes a decrease in conduction velocity within the heart, particularly at the atrioventricular node.29 There are three major classes of CCBs.8 The most commonly used are the smooth muscle selective class, dihydropyridines. Drugs of this category include amlodipine, felodipine, nifedipine, isradipine, nicardipine, and nisoldipine.8 The nondihydropyridines include benzothiazepines and phenylalkylamines. Verapamil, a diphenylalkylamine, and diltiazem, a benzothiazepine, are used to treat blood pressure, both affecting cardiac and vascular smooth muscle cells.8 Adverse reactions include flushing, headache, dizziness, excessive hypotension, reflex tachycardia, and peripheral edema.8 The incidence of gingival hyperplasia with the use of CCBs ranges from 1.7% to 38%.9 Nifedipine is most commonly associated with gingival hyperplasia.9 Surgery may reduce the painful bleeding gums, but drug cessation is usually necessary for complete resolution of symptoms. Drug–drug interactions can be seen when combining CCBs and benzodiazepines, usually resulting in increased sedation.23 Elevated levels of calcineurin inhibitors such as cyclosporine or tacrolimus may be apparent when taken concurrently with CCBs, especially diltiazem and verapamil.30 Drugs such as erythromycin, cimetidine, and rifampin have also been reported to increase and/or decrease plasma levels of CCBs.23
Alpha-blockers
Alpha-blockers or alpha-adrenergic antagonists act on the sympathetic autonomic nerves that innervate blood vessels by binding to alpha-adrenergic receptors located on the vascular smooth muscle cells, thereby decreasing peripheral vascular resistance.8 Alpha-blockers are categorized as noncompetitive and competitive alpha-adrenoceptor blockers.8 The nonselective antagonists are usually reserved for use in hypertensive emergencies caused by a pheochromocytoma. Most common drugs prescribed for a pheochromocytoma are phenoxybenzamine and phentolamine.23 Selective alpha-blockers include prazosin, terazosin, and doxazosin.8 These drugs are most often used in combination with other drugs due to weak therapeutic outcomes associated with monotherapy.8 These drugs often present with various side effects, including orthostatic hypotension, dizziness, nausea, vomiting, and reflex hypertension.8
Dental considerations
While there is no demonstrated direct connection between dental treatment and complications of hypertension,2 it is important for oral health care providers to understand the potential risks and complications that may occur while these individuals are receiving treatment in the dental practice setting. The following are examples.
Side effects of hypertensive drugs
High blood pressure medications, similar to other drugs, can cause side effects and adverse reactions. It is important that the oral health care provider has an understanding of the different types of reactions they can cause. While most people have mild or no side effects from taking hypertensive medications, it is still important to stay informed and work closely with the physician to manage any concerns associated with these medications. The patient’s physician is able to select from a number of medication options if side effects are experienced by the patient. Drug–drug interactions and oral side effects are common. Tables 4 and 5 outline antihypertensive drug classes associated with oral side effects and drug–drug interactions. Common drug interactions that may be encountered in the dental office involve medications often prescribed by the dental professional. Routine and surgical procedures in the dental office usually require administration of local anesthetics with or without epinephrine, which may react adversely with beta-blockers. In addition, conscious sedation has become a common practice in many dental offices in management of patients with fear and anxiety. Moreover, NSAIDs and antifungals are commonly prescribed for oral pain and fungal infections. Understanding how these drugs may interact is essential in the effective management of the hypertensive patient.
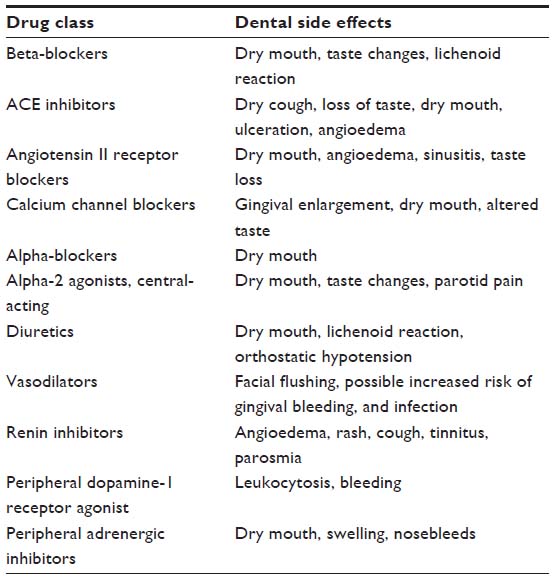 | Table 5 Common antihypertensive dental side effects8,9 |
Oral complications associated with taking antihypertensive medications can range from dry mouth, alterations in taste, gingival enlargement, and lichenoid reactions. When any of these signs or symptoms are observed, consultation with prescribing physician may be indicated if unable to be resolved using other modalities. Evaluation of the medications list and potential side effects may be indicated.
Hypertensive crisis
Among adults who have been diagnosed with hypertension, the incidence of hypertensive crisis is ~1%.4 Although rare, the US has ~500,000 cases each year.4 Hypertensive crisis or acute hypertension3 can be further subdivided into urgency and emergency. Significantly elevated blood pressure (systolic pressure ≥180 mmHg and/or diastolic pressure ≥120 mmHg) with no associated end-organ damage is categorized as hypertensive urgency.3,4,8 Hypertensive emergency is defined as elevated blood pressure associated with target organ damage.2–4,8 There are many risk factors that are associated with hypertensive crisis, but generally, medication noncompliance is one of the most significant factors.3,8
A thorough history should be taken while in the office. Issues to consider when patients present with elevated blood pressure >180/120 mmHg or an acute rise in blood pressure after a previously normal baseline are the following:31 neurologic deficits associated with ischemic or hemorrhagic stroke, nausea and vomiting associated with hypertensive encephalopathy and increased intracranial pressure, chest discomfort associated with myocardial ischemia or aortic dissection, back pain associated with aortic dissection, and dyspnea associated with pulmonary edema. Pregnancy can precipitate/exacerbate severe hypertension, with resulting preeclampsia and risk for eclampsia, which can be life-threatening. Pharmacologic agents that can produce a hyperadrenergic state, such as cocaine, amphetamine, phencyclidine, or monoamine oxidase inhibitors, must be documented and discontinued. Recent discontinuation of clonidine or other sympatholytic agents can also cause a significant rise in blood pressure8 (Table 6). Ensuring that the patient receives proper medical attention can prove to be life-saving in this population.
 | Table 6 Hypertensive emergency drugs8,10,14,31 |
Complications associated with use of vasoconstrictors
A number of vasoconstrictors are used in dentistry today, most commonly epinephrine.32,33 In dentistry, other than its use in the treatment of medical emergencies such as anaphylactic shock, epinephrine is used in conjunction with local anesthetics and as a hemostatic agent. Epinephrine acts to reduce the rate of absorption of anesthetic from the site of injection, preventing subsequent toxicity and allowing for profound anesthesia at the site of infiltration or nerve block.2,32,34 Local anesthesia with added vasoconstriction has proven beneficial as a hemostatic agent.2,32 Epinephrine is also used independently in retraction cord to improve overall vision and control hemorrhage prior to taking impressions for crown and bridge.
The advantages of using epinephrine in the dental setting are clear, but its use in patients who are hypertensive still remains a subject of debate. Risks associated with epinephrine in the hypertensive population include increased risk of acute hypertensive or hypotensive episodes, angina pectoris, arrhythmias, and myocardial infarction.35 Caution is required when administering local anesthetics or other applications, ie, gingival retraction cord, with epinephrine when performing in-depth restorative rehabilitation.35 Abu-Mostafa et al32 suggested that the amount of epinephrine associated with local anesthetics can influence hemodynamics in a patient. The above studies concluded that concentrations of 1:80,000 significantly affected SBP and DBP, as well as affecting the heart rate; 1:100,000 concentrations can exacerbate SBP and heart rate; and 1:200,000 is limited to exacerbation of heart rate, however, significantly less than that with previous concentrations. Their recommendation was to consider concentrations of 1:200,000 for local anesthesia before tooth extraction to prevent significant hemodynamic changes.32 However, the use of impregnated retraction cord has been discouraged in patients with uncontrolled hypertension.12,34,36 Maximum dosing for adults with questionable uncontrolled hypertension and/or cardiovascular disease is 0.04 mg, totaling two or four cartridges depending on the epinephrine concentration present in the cartridges.10,34,37
Within the literature, there are varying opinions on treating otherwise healthy patients who present with intense uncontrolled pain in the setting of hypertension. Pain and stress can significantly contribute to increased blood pressure and therefore, increase the risk for adverse cardiovascular events. Administration of local anesthesia with vasoconstrictor has been proven to aid in the reduction of pain and improvement of blood pressure measurements.12 Stress management, antianxiety techniques, and allowing the patient to ask questions and voice concerns about procedures may also aid in overall reduction of blood pressure.11
There are a number of drug interactions associated with the use of vasoconstrictors. Epinephrine has been shown to react with some antihypertensive agents as well as other drugs.34 The use of epinephrine and monoamine oxidase inhibitors may induce hypertensive crisis.34 Phenothiazine compounds are known to cause orthostatic hypotension. Providers who treat patients who are prescribed these drugs should be cautious when administering local anesthesia with added vasoconstrictor. Intravascular injection in patients prescribed phenothiazine could worsen the hypotensive effect.34 Hypertension and reflex bradycardia are potential consequences of a combination of beta-blocker and epinephrine.34 Epinephrine and tricyclic antidepressants may cause acute hypertensive changes.2,34 Diuretics often produce hypokalemia, which may be exacerbated by epinephrine and may possibly lead to development of arrhythmia. Epinephrine and cocaine often result in blood pressure spikes and fatal dysrhythmias.34 Although there is no absolute contraindication for using epinephrine in the range of 0.04–0.06 mg,10,37 dental care should be postponed for 24 hours following suspected cocaine use.34
Bleeding
Elevated blood pressure can lead to excessive intraoperative bleeding during surgical procedures.38 Again, knowing the history of the patient plays a role in deciding when to perform certain procedures, and precautions should be taken when performing surgeries. Due to a number of different comorbidities, people are prescribed various anticoagulant medications for treatment. It is generally recommended that for patients who have an international normalized ratio value of <4 anticoagulation is not terminated for a minor surgery.39 For aspirin and other antiplatelet drugs, such as rivaroxaban and clopidogrel, the recommendation again is to continue medication during minor surgery without interruption.40 Various hemostatic agents can be used to help control bleeding. Application of local anesthesia with vasoconstrictors, chitosan-based products, bone wax, fibrin sealants, epsilon-aminocaproic acid, tranexamic acid, oxidized cellulose, aluminum chloride, ferric sulfate, aluminum potassium sulfate, zinc chloride, trichloroacetic acid, and tannic acid, as well as utilizing cordless retraction techniques helps in controlling bleeding when performing surgical or restorative procedures.41,42
Blood pressure values and risk assessment
A blood pressure measurement of 180/110 mmHg as the absolute cutoff for any dental treatment has been well published throughout the literature.2,9,13,37 Studies43 have shown that there is no increased risk for adverse perioperative outcomes for patients undergoing treatment with a blood pressure <180/110 mmHg. For patients who have histories that include previous hypertensive-related organ damage, which include myocardial infarctions, strokes, or labile angina, the absolute cutoff that has been published may, in fact, be too high for this particular subset to undergo treatment, even on an emergent basis. Judgment should be used when treating these patients accordingly.
Completing a history and physical examination helps in making a thorough risk assessment.37 Bavitz9 recommends completing a patient’s risk assessment before undertaking dental procedures. This may be the key in assessing the likelihood of complications and risk of cardiac events. The classification by the American Society of Anesthesiologists (Table 7) and use of metabolic equivalents (METs) could be helpful when stratifying the risk associated with treating patients in a dental setting.37
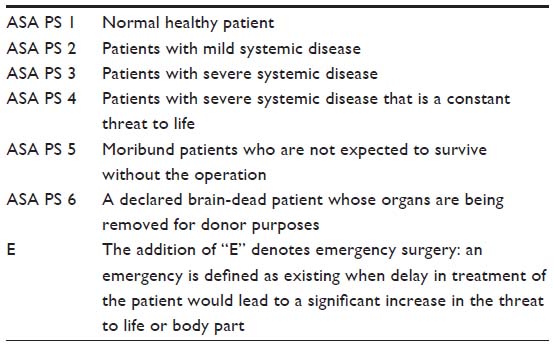 | Table 7 ASA PS classification system43–45 |
One MET is defined as 3.5 mL of oxygen consumed per kilogram body mass per minute.43 The use of METs is a quantifying value used as a test of one’s ability to perform physical work (Table 8). It has been estimated that patients who are able to perform tasks ≥10 METs are at a significantly less risk for experiencing an adverse cardiovascular event.43 For patients who are American Society of Anesthesiologists Class III–IV or have a MET capacity of ≤4, it has been encouraged to break procedures into multiple quadrants and retake blood pressures after one quadrant of dentistry. A slow technique with aspiration avoids intravascular injection by the operator and may reduce adverse reactions. The suggested rate for this procedure is 1 mL/min.34
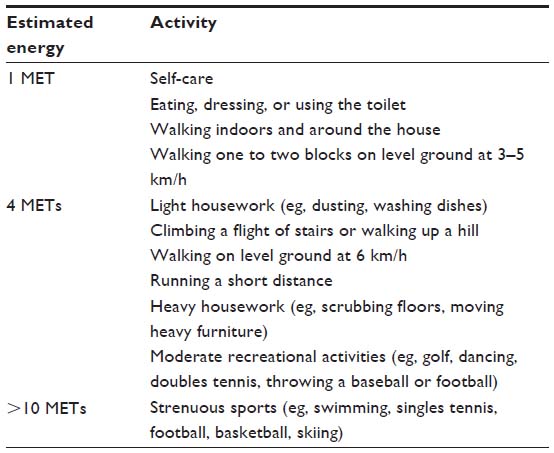 | Table 8 Estimated energy requirement for various activities37,44 |
Along with obtaining initial preoperative vital signs, knowing a patient’s physical and functional status could prove beneficial when making decisions about treatment. Stress management, short duration morning appointments, slow position changes, and establishing profound local anesthesia can prevent extreme changes in overall hemodynamics.11 Treatment and treatment setting also play a role with overall decision making. In the end, the benefits of proceeding with a procedure must outweigh any systemic risks that could potentially occur.11
Racial/ethnicity disparity-associated hypertension
Prevalence of hypertension among African Americans is ranked the highest in the world,9 representing 41.4% of hypertensive patients.1 This number is significantly higher than in the Caucasian or Mexican American adult populations.46 Compared with Caucasians, African Americans develop hypertension earlier in life and their average blood pressures are much higher.1 As a result, African Americans have a 1.3-times greater rate of nonfatal stroke, 1.8-times greater rate of fatal stroke, 1.5-times greater rate of death attributable to hemodialysis, and 4.2-times greater rate of end-stage kidney disease.1 African Americans are also less likely to be at goal blood pressure while being prescribed medication.46 Whether the differences lie in access to care, poor diagnoses, poor treatment/medication noncompliance, or socioeconomic status, it is the duty of the primary health care provider, including the dentist, to aid in the prevention and education of hypertension.
Conclusion
The management of the hypertensive patient, particularly within a dental setting, is a well-discussed topic in the literature. New information about hypertensive patients is published often, and the management is often changed. It is important to implement these new changes to maintain the best quality of care when treating patients. A dental provider must have knowledge of the disease, know current therapeutic options, and possess the ability to educate and provide access to care for patients. The recommendation for managing these patients is mainly based on one’s judgment as a practitioner. Before proving care to these patients, the practitioner should be able to assess patient health status and make proper decisions based on the following factors: baseline blood pressure, urgency of the procedure, functional and physical status, and time and invasiveness of the procedure. Most importantly, when in doubt, medical advice should be considered. The health of the patient must always come first.
Disclosure
The authors report no conflicts of interest in this work.
References
Mozaffarian D, Benjamin EJ, Go AS, et al. American Heart Association Statistics Committee and Stroke Statistics Subcommittee. Heart disease and stroke statistics – 2015 update: a report from the American Heart Association. Circulation. 2015;131(4):e29–e322. | |
Hogan J, Radhakrishnan J. The assessment and importance of hypertension in the dental setting. Dent Clin North Am. 2012;56(4):731–745. | |
Pak KJ, Hu T, Fee C, Wang R, Smith M, Bazzano LA. Acute hypertension: a systematic review and appraisal of guidelines. Ochsner J. 2014;14(4):655–663. | |
Salkic S, Batic-Mujanovic O, Ljuca F, Brkic S. Clinical presentation of hypertensive crises in emergency medical services. Mater Sociomed. 2014;26(1):12–16. | |
Danaei G, Finucane M, Lin JK, et al. Global Burden of Metabolic Risk Factors of Chronic Diseases Collaborating Group (Blood Pressure). National, regional, and global trends in systolic blood pressure since 1980: systematic analysis of health examination surveys and epidemiological studies with 786 country-years and 5.4 million participants. Lancet. 2011;377(9765):568–577. | |
Yoon SS, Burt V, Louis T, Carroll MD. Hypertension Among Adults in the United States, 2009–2010. Hyattsville: National Center for Health Statistics; 2012:1–8. | |
Akpunonu BE, Mulrow PJ, Hoffman EA. Secondary hypertension: evaluation and treatment. Dis Mon. 1996;42(10):609–722. | |
Whalen K, Finkle R, Panavelil TA. Lippincott Illustrated Reviews: Pharmacology. 6th ed. Philadelphia: Wolters Kluwer; 2015. | |
Bavitz JB. Dental management of patients with hypertension. Dent Clin North Am. 2006;50(4):547–562, vi. | |
Holm SW, Cunningham LL Jr, Bensadoun E, Madsen MJ. Hypertension: classification, pathophysiology, and management during outpatient sedation and local anesthesia. J Oral Maxillofac Surg. 2006;64(1):111–121. | |
Little J, Falace D, Miller C, Rhodus N. Dental Management of the Medically Compromised Patient. 6th ed. St. Louis: Mosby; 2002. | |
Popescu SM, Scrieciu M, Mercut V, Tuculina M, Dascalu I. Hypertensive patients and their management in dentistry. ISRN Hypertens. 2013;2013:1–8. | |
Becker DE. Preoperative medical evaluation: part 1: general principles and cardiovascular considerations. Anesth Prog. 2009;56(3):92–102. | |
National High Blood Pressure Education Program. The Seventh Report of the Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure. Bethesda: National High Blood Pressure Education Program; 2004. | |
James PA, Oparil S, Carter BL, et al. 2014 evidence-based guideline for the management of high blood pressure in adults: report from the panel members appointed to the Eighth Joint National Committee (JNC 8). JAMA. 2014;311(5):507–520. | |
Judd E, Calhoun DA. Management of hypertension in CKD: beyond the guidelines. Adv Chronic Kidney Dis. 2015;22(2):116–122. | |
Kaplan NM. The 6th joint national committee report (JNC-6): new guidelines for hypertension therapy from the USA. Keio J Med. June,1998;47(2):99–105. | |
Babaei H. Antihypertensive Drugs. Rijeka: InTech; 2012. | |
Calhoun DA, Jones D, Textor S, et al. Resistant hypertension: diagnosis, evaluation, and treatment: a scientific statement from the American Heart Association Professional Education Committee of the Council for High Blood Pressure Research. Hypertension. 2008;51(6):1403–1419. 20. | |
Viera, AJ. Resistant hypertension. The Journal of the American Board of Family Medicine 2012; 25(4):487–495. | |
Kasper DL, Harrison TR. Harrison’s Principles of Internal Medicine. New York: McGraw-Hill, Medical Pub. Division; 2005. | |
Muzyka BC, Glick M. The hypertensive dental patient. J Am Dent Assoc. 1997;128;1109–1120 | |
Li YR. Cardiovascular Diseases: From Molecular Pharmacology to Evidence-Based Therapeutics. Hoboken: John Wiley and Sons, Inc.; 2015. | |
Brunton LL, Parker K, Blumenthal D, Buston L. Goodman and Gilman’s Manual of Pharmacology and Therapeutics. 2nd ed. New York: McGraw-Hill; 2008. | |
Becker DE, Reed KL. Essentials of local anesthetic pharmacology. Anesth Prog. 2006;53(3):98–108. | |
Pazhayattil GS, Shirali AC. Drug-induced impairment of renal function. Int J Nephrol Renovasc Dis. 2014;7:457–468. | |
Arima S, Endo Y, Yaoita H, et al. Possible role of P-450 metabolite of arachidonic acid in vasodilator mechanism of angiotensin II type 2 receptor in the isolated microperfused rabbit afferent arteriole. J Clin Invest. 1997;100(11):2816–2823. | |
Barreras A, Gurk-Turner C. Angiotensin II receptor blockers. Proc (Bayl Univ Med Cent). 2003;16(1):123–126. | |
Kapoor AK, Raju SM. Illustrated Medical Pharmacology. 1st ed. New Delhi: Jaypee Brothers Medical Publishers; 2013. | |
Danovitch GM. Handbook of Kidney Transplantation. 5th ed. Philadelphia: Wolters Kluwer Health/Lippincott Williams and Wilkins; 2010. | |
Marik PE, Varon J. Hypertensive crises: challenges and management. Chest. 2007;131(6):1949–1962. | |
Abu-Mostafa N, Aldawssary A, Assari A, Alnujaidy S, Almutlaq A. A prospective randomized clinical trial compared the effect of various types of local anesthetics cartridges on hypertensive patients during dental extraction. J Clin Exp Dent. 2015;7(1):e84–e88. | |
Abu-Mostafa N, Al-Showaikhat F, Al-Shubbar F, Al-Zawad K, Al-Zawad F. Hemodynamic changes following injection of local anesthetics with different concentrations of epinephrine during simple tooth extraction: a prospective randomized clinical trial. J Clin Exp Dent. 2015;7(4):e471–e476. | |
Balakrishnan R, Ebenezer V. Contraindications of vasoconstrictors in dentistry. Biomed Pharmacol J. 2013;6(2):409–414. | |
Bader JD, Bonito AJ, Shugars DA. Cardiovascular Effects of Epinephrine on Hypertensive Dental Patients. Evidence Report/Technology Assessment Number 48. (Prepared by Research Triangle Institute under Contract No. 290-97-0011.) AHRQ Publication No. 02-E006 Rockville, MD: Agency for Healthcare Research and Quality. July 2002. | |
Tavares M, Lindefjeld Calabi KA, San Martin L. Systemic diseases and oral health. Dent Clin North Am. 2014;58(4):797–814. | |
Aubertin MA. The hypertensive patient in dental practice: updated recommendations for classification, prevention, monitoring, and dental management. Gen Dent. 2004;52(6):544–552. | |
Herman WW, Konzelman JL Jr, Prisant LM; Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure. New national guidelines on hypertension: a summary for dentistry. J Am Dent Assoc. 2004;135(5):576–584. quiz 653–654. | |
Perry DJ, Noakes TJ, Helliwell PS; British Dental Society. Guidelines for the management of patients on oral anticoagulants requiring dental surgery. Br Dent J. 2007;203(7):389–393. | |
Chassot PG, Marcucci C, Delabays A, Spahn DR. Perioperative anti- platelet therapy. Am Fam Physician. 2010;82(12):1484–1489. | |
Ogle OE, Swantek J, Kamoh A. Hemostatic agents. Dent Clin North Am. 2011;55(3):433–439. | |
Tarighi P, Khoroushi M. A review on common chemical hemostatic agents in restorative dentistry. Dent Res J (Isfahan). 2014;11(4):423–428. | |
Barnes JN, Joyner MJ. Physical activity and cardiovascular risk: 10 metabolic equivalents or bust. Mayo Clin Proc. 2013;88(12):1353–1355. | |
Graham L. ACC/AHA release guidelines on perioperative cardio- vascular evaluation for noncardiac surgery. Am Fam Physician. 2008;15(77):1748–1751. | |
Owens WD, Felt JA, and Spitznagel EL Jr. ASA physical status classifications: a study of consistency of ratings. Anesthesiology. October, 1978;49(4):239–243. | |
Mueller M, Purnell TS, Mensah GA, Cooper LA. Reducing racial and ethnic disparities in hypertension prevention and control: what will it take to translate research into practice and policy? Am J Hypertens. 2014;28(6):699–716. |
 © 2016 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2016 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.