Back to Journals » Risk Management and Healthcare Policy » Volume 13
Dental Facilities During the New Corona Outbreak: A SWOT Analysis
Authors Gaffar B ![]() , Alhumaid J, Alhareky M, Alonaizan F
, Alhumaid J, Alhareky M, Alonaizan F ![]() , Almas K
, Almas K ![]()
Received 3 June 2020
Accepted for publication 8 August 2020
Published 25 August 2020 Volume 2020:13 Pages 1343—1352
DOI https://doi.org/10.2147/RMHP.S265998
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Marco Carotenuto
Balgis Gaffar,1 Jehan Alhumaid,1 Muhanad Alhareky,1 Faisal Alonaizan,2 Khalid Almas1
1Preventive Dental Sciences Department, College of Dentistry, Imam Abdulrahman Bin Faisal University, Dammam, Saudi Arabia; 2Restorative Dental Sciences Department, College of Dentistry, Imam Abdulrahman Bin Faisal University, Dammam,Saudi Arabia
Correspondence: Balgis Gaffar Tel +966 542269941
Email [email protected]
Abstract: Recently, there have been many global outbreaks of diseases. The latest is the coronavirus disease of 2019 (COVID-19) pandemic. The virus has spread worldwide and is transmitted mainly through droplets or by touching contaminated surfaces. Globally, healthcare systems are challenged due to a lack of workplace safety and professional obligations in addition to the rapid spread of the virus. Dental facilities are at greater risk due to the nature of dental care. The aim of this review study was to provide a situational analysis within dental facilities during the new COVID-19 outbreak. Published papers concerning dental facilities and COVID-19 were retrieved from PubMed, search engines, and organizational websites. All data were reviewed, arranged into themes, and then categorized either as strengths or weaknesses with respect to addressing the COVID-19 pandemic in dental facilities, and accordingly, threats and possible opportunities to the handling of the pandemic were identified. Preparedness of dental facilities during the current pandemic is a weakness that needs to be addressed promptly. Shortage of dental care providers, cyber security, economic losses, and ethical challenges are possible threats due to the current outbreak. Coordination and prompt communication among all healthcare providers during such outbreaks is a strength that needs to be supported. This strengths, weaknesses, opportunities, and threats (SWOT) analysis can be a useful tool for guiding decision-making as it is crucial during the current pandemic to work on weaknesses, avoid threats, and utilize all future opportunities.
Keywords: COVID-19, dental clinics, SWOT, preparedness, challenges
Introduction
Recently many global outbreaks have occurred, including the severe acute respiratory syndrome coronavirus (SARS-CoV-1) in 2003,1 the middle east respiratory syndrome coronavirus (MERS-CoV) in 2012,2 Ebola3 and Zika viruses in 2014,4 and last, the pandemic of severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2).2 The new coronavirus 2019, COVID-19, originated in late 2019 in Wuhan, China, rapidly spread, and has affected more than 200 countries worldwide.2 Within a short period of time, strict public health measures were applied worldwide ranging from social distancing to remote working to complete lockdown in some countries in an attempt to stop the virus spread.2 Viral transmission occurs mainly through inhalation, direct mucous contact with salivary droplets, and/or contact with contaminated objects and surfaces.5,6 Up to date, no treatment or vaccines exist; therefore, prevention via halting the transmission chain is crucial. Although the spread of the virus is slowing nowadays, the World Health Organization (WHO) is warning of another wave that will infect many more people worldwide.7 A lack of complete understanding of the behavior of the new coronavirus, its prevention, treatment, and resources to prepare in many developed countries exists. Similarly, a need to identify the gaps within dental facilities and to evaluate the challenges faced during the current outbreak also is present. This process is crucial in order to propose and investigate new recommendations and opportunities within dental practice areas.
During acceleration of the COVID-19 pandemic, global healthcare systems have become overwhelmed with the risk of infection and providing care.2 A strengths, weakness, opportunities, and threats (SWOT) analysis can offer policy makers a sound basis for strategy development and structured planning for handling the COVID-19 pandemic in dental facilities.8,9 Allocating resources and estimating risks would also be of great help to private practice owners. Strengths and weaknesses as determined by the analysis are the positive and negative characteristics within the dental facilities, while threats and opportunities are external factors that can be avoided or utilized.9 This review study is intended to provide a situational analysis within dental facilities during the new coronavirus outbreak.
Methodology
A SWOT analysis is a common systematic tool used by evaluation specialists in any field of study.8,9 SWOT refers to the strengths and weaknesses that are the internal characteristics of a system, which need to be emphasized or addressed, respectively, while opportunities and threats are external factors or elements that should be used or avoided.9 Strengths and weaknesses can be identified by internal appraisal (interviews with experts, records, published, and/or unpublished data), while opportunities and threats are identified by an external assessment or analysis.9
The following questions guided the search to use SWOT for assessing the impact of the current outbreak on dental facilities:
- What are the weaknesses that were reported during the current COVID-19 outbreak?
- What strengths exist within dental facilities that should be emphasized and sustained?
- What are the possible opportunities that dental facilities should utilize or consider?
- What are the threats that dental facilities may face in the future under similar conditions?
A literature review was conducted. Reviews, original studies, commentaries, letters to editors, and both governmental and international guidelines were searched. As most organizations and institutions had made their content opened access since the COVID outbreak, two electronic databases: (1) PubMed and (2) search engines (Google Scholar and Google) were searched. Key words used in the search were “dental facility AND COVID”, “dentists AND COVID”, “dental AND COVID”, and “COVID AND dental AND economic”. Information and guidelines posted on the Ministry of Health website and international dental associations were also used. Each author carried out the search at his/her own discretion. A shared folder was created to eliminate duplicates. Articles were included if they were in the English language, published during the period from December 2019 until April 2020, and were reporting or discussing the impact of COVID-19 on dentistry. Articles in languages other than English, with no full text, and/or not related to the COVID-19 pandemic were excluded. A total number of 117 articles were retrieved, 36 were with no full text or duplicates, five were in Chinese and so were excluded. We ended up with 76 published papers in addition to official documents and governmental websites (Figure 1). Each author was assigned a number of articles or documents and had to list the main points addressed in them (shown in Supplementary file). A virtual meeting was conducted to arrange all of the addressed issues and concerns that were classified as themes. All themes were classified into four categories based on the SWOT parameters: (1) strengths, (2) weakness, (3) threats, or (4) opportunities (Table 1).
 |
Table 1 Strengths, Weaknesses, Threats and Opportunities Within Dental Facilities |
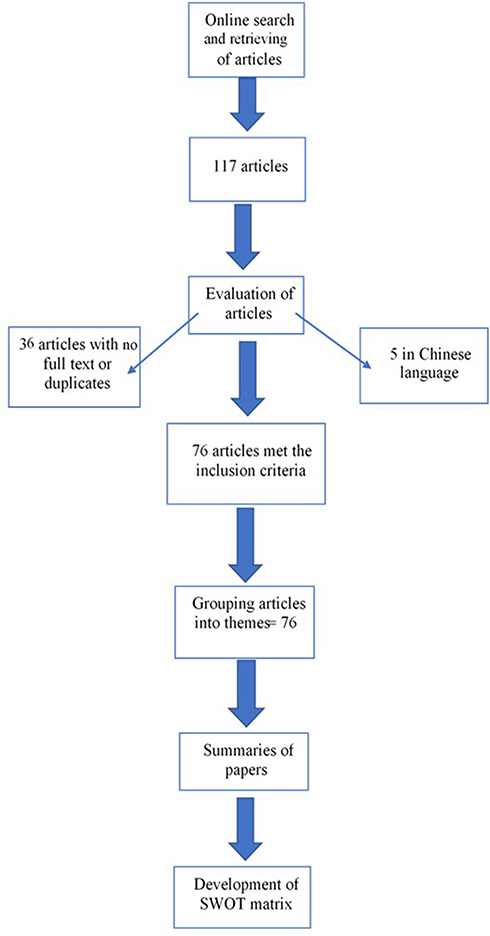 |
Figure 1 Flow chart of the review process. |
Discussion
Although the COVID-19 pandemic has affected almost the entire world, the severity, adopted measures, and consequences differ from one country to another. Similarly, the situational analysis presented in this paper is applicable to all countries, yet the prioritization of the concerns will vary. From the reviewed literature, several strengths, weaknesses, opportunities, and threats were identified.
Strengths
Four-Handed Dentistry
The role of a dental assistant (DA) varies across the different dental practices, ranging from chairside assistance, infection control, and sterilization, to the provision of preventive dental care.10 Four- or six-handed dentistry refers to the one or two trained, competent, chair side assistant/s who work regularly with the dentist to provide dental care.10 Although mainly introduced as an ergonomics concept, the role of dental assistants in infection control also cannot be overlooked.10 The latest recommendations by the Centers for Disease Control (CDC) in the United States emphasized the use of four-handed dentistry as part of engineering controls and work practices during emergency dental care.11
As the backbone of any dental facility, whether it is solo or a part of a hospital, dental care providers (DCPs) are responsible for their own safety and the safety of their patients and other staff members. The safety of the dental team and patients should be a priority. The American Dental Association (ADA) and Health Authorities have set guidelines for the provision of dental treatment.12,13 Similarly, different government bodies have provided detailed protocols for DCPs ranging from patient triage, dental care, infection control, and patients referral.14,15 Clear government guidelines and practice policies reduce the burden and stress on care providers, eventually reducing the chances of error and violations.
A conceptual model for factors influencing the decision to provide care is presented in Figure 2.
 |
Figure 2 Factors influencing the decision whether to provide care during an outbreak or not. |
Inter-Professional Care
Recently, inter-professional care (IPC) has been promoted to expand the scope of dental practices to provide primary healthcare.16 Dentists can help to improve the healthcare system by providing screening, diagnosis, and even treatment for certain medical conditions.17 During the current outbreak, many dental care providers have volunteered to provide care to COVID-19 patients, and dental facilities have been utilized in certain countries to accommodate the overwhelming number of patients.18 Dentists are assisting in hospitals by taking vital signs, performing COVID-19 testing, triaging, treating emergencies, administering injectables, and writing prescriptions. After additional training, oral surgeons can also intubate and provide general anesthesia.19,20 Dentists can also play a crucial role in the identification of patients attending dental clinics by proper triaging and assessment.12,13
Certain oral conditions have also been linked to COVID-19, and as such can be detected by DCP; these conditions include salivary gland infections (saliva test positive for COVID-19) and taste abnormalities.21
In the same context, the COVID-19 infection is thought to aggravate some oral conditions, especially in those with autoimmune diseases or those on prolonged medication use.22 DCPs are supposed to work side-by-side with medical healthcare providers in monitoring the oral health status of those staying in intensive care units or those who have been treated for COVID-19 for long periods.22
Proper investigation of patients’ medical and social wellbeing can also lead to identifying any psychological conditions as a result of the current situation.23 An increase in reported cases of domestic violence, and suicide because of the current lockdown has been noted.24 Dentists can also detect signs and symptoms of abuse;25 such cases should be reported immediately to specialized medical staff and related authorities.24
Weaknesses
Nature of Dental Care
Dental care providers and dental settings are exposed to more occupational hazards.26 Closeness to patients and the nature of dental practice put dental practitioners at greater risk than other healthcare providers.27 DCPs are frequently exposed to aerosols and splatter, blood, and body fluids in addition to suspended particulate matter.5,6,28,29 These challenges increase even more during times of outbreaks, and given the nature of dental facilities, this exposure affects not only DCPs but poses a public threat.30–32 Such outbreaks always require extra infection control measures, logistics, facility and staff preparedness, proper identification, and prompt management.33 However, dental facilities, DCPs, and supporting staff are not always well equipped to deal with these outbreaks.5,6,20,30,33
As part of the national and international recommendations, dentists should be gowned, shielded, and masked.11–15,33 Body language and eye contact are essential elements for maintaining rapport with patients, and patients have been shown to feel relaxed when they are able to see their doctor’s facial expression, which is why a change in the patient–dentist relationship is likely to occur.34
Preparedness of Dental Facilities
Figure 3 addresses the factors that can influence the preparedness and readiness of dental facilities during outbreaks.
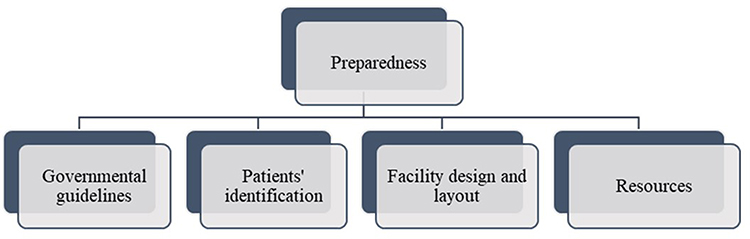 |
Figure 3 Factors influencing preparedness of dental facilities. |
Facility Design and Layout
A separate designated area is needed within the faculty as a triage area.30,33,34 Similarly, a negative pressure room with a minimum of 12 air changes per hour is needed for the emergency treatment of confirmed or suspected COVID-19 patients.30 It is also advised that mechanical ventilation be initiated between patients.30,34
Patients’ Identification
Receptionists and security personnel are the first to come into contact with patients. In cases such as the COVID-19 outbreak, the patients should be assessed ideally before coming to the clinic, but if that assessment is not possible, they should be assessed as soon as they arrive.5,32 Figure 4 shows the four levels at which all patients should be assessed. Due to the inconsistent global morbidity and mortality behavior of the contagion, compliance with preventive measures, such as social distancing, hand washing, and facemask usage, is becoming more difficult for the masses.35 These difficulties add to the perceived stress among the patient population. The lack of confidence of the public consumers of information is also prevalent and growing rapidly due to the advent and excessive use of social media and various inconsistent virtual platforms.35 The emergence of growing dissatisfaction and disbelief in scientific information resulting from rampant disinformation without any scientific evidence is also becoming prevalent.35
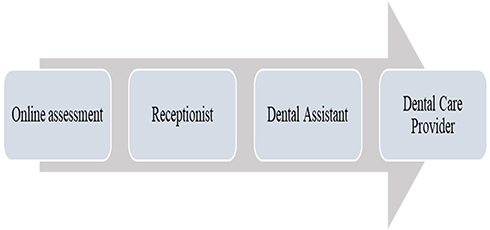 |
Figure 4 Patients’ assessment stages. |
Patients should be encouraged to disclose any medical conditions or illness as patients usually tend to hide such information in the fear that they will be deprived of treatment. Detailed medical history, including travel history, contact with animals, residence, and a checklist with COVID-19 signs and symptoms are crucial for patient identification.5,11–15
Clear information explaining the consequences of concealing medical information/condition should be visible to patients. Wall-mounted infographics and displays are an ideal choice for health education, and shared hard copies should be avoided.11–15
Governmental Policies and Guidelines
Ministries of Health (MoH) or Department of Health, licenses dental facilities based on certain criteria that include but are not limited to qualified personnel, facilities and equipment, quality of care, and infection control. However, these infection control measures are not always closely monitored unless a violation report is made, especially in the private sector.36,37 In some countries, dentistry is even practiced without any license.38 With the serious recent outbreaks and pandemics, MoH or competent healthcare authorities should have regular inspections to track any violations. During the COVID-19 outbreak, clear universal guidelines and restrictions were initiated within medical facilities; however, the responses have varied among dental facilities.18,26 Dental regulatory bodies do not have policies to support dental practices in times of crisis, especially in developing countries.39 Testing dental professionals should be given the same priority by authorities as that for other healthcare providers.40–42
Resources
The COVID-19 pandemic has led to a dramatic rise in the demand for surgical masks, goggles, gloves, and gowns. It has been estimated that a 40% increase in manufacturing is needed to meet these demands.43,44 The main suppliers of these materials are in Asia, mainly China and the Pacific, so in addition to the cost of personal protective equipment (PPE), the cost of transportation and shipping also exists.44,45 Additionally, there are the costs of hand hygiene materials and items needed for patients undergoing triage, such as no-touch thermometers and thermal imaging cameras.11–15
As part of respiratory precautions, it is recommended that healthcare providers use an N95 respirator or wear a surgical mask along with a face shield.12–15,28 Although no significant difference was found between them in regard to preventing influenza,46 however a comparison of the effectiveness of masks against the COVID-19 virus during dental procedures requires clinical trials to determine its filter performance and facial fit.47 Manpower is another point to consider, and although in dental settings enough number of care providers is not a problem but having trained DCPs and supporting staff is a serious issue.12
Threats
The current situation has significantly affected many industries in addition to dental services. Many countries worldwide are under lockdown and people have been instructed to work from home. This type of work situation has led to the closure of many dental practices and the suspension of elective dental treatment in the rest.11–15,20,48 On the other hand, these decisions have serious consequences that cannot be ignored both on the professional and financial levels in addition to presenting ethical challenges.18 The rising protest in industrialized democracies is also on the increase and has mainly imploded due to economic hardships and lack of social and financial sustainability.35
Economic Challenges
Healthcare facilities have been tremendously affected either directly by the overload of patients or indirectly by the constraints in response to the virus spread.43 Dental practices have been mostly affected by the later.32,44 The use of dental services and dental visits had significantly decreased during the COVID-19 outbreak.49,50 A reduction by three-tenths in non-urgent dental care and a 38% reduction in emergency dental care, especially in cities with higher cases of COVID-19, has been reported.49 These findings can be the result of the quarantine restrictions on transportation or the patients’ fears of acquiring the infection.44 In the same context, the use of dental services is closely linked to insurance coverage; therefore, with the increase in unemployment due to the COVID-19 outbreak, the demand for dental care has decreased.44
It is expected that the impact on private dental facilities would be even more noticeable. Some have estimated that financial loss may reach up to 70%.45 A recent study predicted that dental care spending in the United States could decline by up to 66% in 2020 and 32% in 2021.44
In the same context, preventing the spread of infection relies on the effective use of PPE, such as isolation suits and air-purifying respirators, which also add to the financial burden of a dental practice.32 Similarly, the cost of staff training, signages, and hygienic supplies is also increasing. Even dental equipment will undergo a different path to cope with future outbreaks; external mouth suctions, commercial air purifiers, and air exchange devices are some examples being under current investigations.34 Negative pressure operatories will no longer be optional but rather will be a requirement.43
The practice of dentistry itself is expected to change to eliminate aerosol generation and will include aerosol-free cavity prevention, sealants, atraumatic restorative treatment, and vital pulp therapy.50,51
The design of dental clinics and hospitals will need to be reoriented in order to reduce the infection transmission and achieve a level of social distancing. This design may include the premises and equipment costs in addition to changes in staffing structure, thus adding to the financial burdens of the COVID-19 outbreak.43,44
The impact of the corona outbreak on dental economics is expected to continue for years, and recovery will depend on many factors, such as removal of restrictions, availability of a COVID-19 vaccine, and the availability of workplace safety measures.44
Ethical Obligations
“To treat or not to treat” is the question dentists face nowadays. Apart from their fears of contracting the infection,52 dentists are challenged by their ethical obligations.18 The CDC in the United States and ADA recommend that only emergency and urgent dental treatment to be provided under-restricted infection control measures.11,12 Emergency dental care should be provided in cases of uncontrolled bleeding, cellulitis, or facial trauma that may lead to airway obstruction,11,12 while dental trauma, severe dental pain interfering with sleep, dental treatment required prior to critical medical surgeries, or biopsy of suspicious lesions come under urgent dental care.11,12
In the same context, certain protocols should be followed when managing an urgent or emergency case to prevent the spread and optimize the care starting with triaging, disinfection procedures, instrumentation, and the use of novel treatments approaches.28,29 Minimally invasive treatments for pediatric patients,53 single file mechanized nickel-titanium (NiTi) instrumentation for endodontic treatments,51 or an open approach for tracheostomy in case of oral surgeries are some of the recommended novel treatments.18,48
Dentists’ decision to provide care should be based primarily on patient safety and then on a dental hierarchy of needs in line with the Maslow hierarchy of needs, that is to fulfill wellbeing first.54 Dental facilities should adopt a referral and emergency system that allows patients with dental emergencies to be treated while protecting themselves and other patients.
In the same context, these restrictions can affect serious dental conditions, such as early detection and proper diagnosis of oral cancer.55 On the other hand, cancellation of patient appointments, and suspension of elective treatment present the dentists with dento-legal aspects. Another ethical dilemma that has been raised is referrals of suspected cases to a hospital that can result in wider population exposure.56
A major challenge would also be to restore the confidence of our patient population due to fear of contagion, lack of complete understanding of the COVID-19, unavailability of evidence-based therapeutic cure, and absence of clinically proven vaccine against COVID-19.57 Patient education, updates on infection control procedures, and consultations could be possible strategies to consider when dealing with reluctant patients.58
Dental Care Providers Shortage
Healthcare taskforce attrition is possible given the high death rate and infection among them.40 Large numbers of healthcare workers became infected while caring for COVID-19 patients, and death cases were also reported among ophthalmologists and ear, nose and throat specialists.59 Dentists are at a relatively high risk for contracting COVID-19; dental facilities should consider the consequences of losing their staff as a result of becoming infected or dying.60 Dental care providers who suffer from signs and symptoms of flu are not supposed to come to work or come into contact with patients. Those individuals who are at higher risk (elderly, medically compromised, pregnant) should avoid treating patients and can only work in screening and triaging. Stress levels are also high during this period either due to the psychological impact of the lockdown or the workload or both. Stress is one of the leading causes of burnout among dental care providers that can lead to prolonged sick leaves or even early retirement.61
Cyber Security
The COVID-19 outbreak had directed many people from different sectors to work from home in addition to undertaking online schooling and telemedicine. An increase in attempted cyber-attacks from 30 per 1000 endpoints in February to 145 threats in April 2020 was found.62 Apart from the financial fraud data loss resulting from cybercrimes, securing the confidentiality of patient information is serious issue that can threaten dental services.
Opportunities
The world has changed drastically in order to cope with the sudden COVID-19 outbreak. In a short period of time, people have managed to use available resources to adapt to the current situation starting with working from home to reusing and recycling existing resources to meet the demands of the healthcare sector. Many lessons can be learned from this outbreak, and many future opportunities should be considered in order to avoid such consequences in the future.
Information Technology (IT)
Telemedicine services, patient advice lines, and augmented telephone triage systems are some examples of IT uses in healthcare.63 Tele-dentistry is defined as “the practice of using videoconferencing technologies to diagnose and provide advice about treatment over a distance”.64 It combines technology and dental care, thus linking DCPs and patients. Patient consultations using teledentistry can either be real-time consultation, store-and-forward consultation, remote patient monitoring, or mobile health.64,65 Tele-dentistry can also be used for patient screening.65
With the evolution in IT and the success of teledentistry, all dental facilities should be encouraged to adopt an online booking system. This adoption has many benefits not only reduces risk during times of outbreaks but also allows patient to fill medical record or book a convenient appointment, therefore reducing the time spent at front desks and increasing patients’ satisfaction as well as treatment outcomes.65 As patients fill medical records at their convenience with no fear of patients becoming frustrated or overwhelmed by the request for too much data, a lot of information can be included in medical records, which can allow better diseases screening, prevention, and control.42 It would also be possible to link individuals’ dental records with their medical records allowing also for better evaluation of patients’ medical condition and treatment planning. This process will also facilitate the referral process between different departments and professions. During the COVID-19 outbreak, remote consultations and prescribing were found to be successful.31,42 Online consultations can be used to screen, filter symptomatic patients, relieve symptoms in addition to soothing dentally anxious patients.66,67
Mobile Dental Units
Due to the current restrictions on public transport and the weaknesses within dental facilities addressed earlier, it would be worthy to use mobile dental units and domiciliary visits. In addition to providing cost-efficient services, reaching remote and unserved populations, mobile dental units could also be used in a hospital environment for safer work practices.68
Economic Support
Dental services are not risk-free. Health insurance offers coverage for disability or medical, surgical, and/or hospital costs, including guaranteed treatment, long-term care, travel insurance, and personal injury coverage. Dental insurance offers high-cost dental insurance coverage. Private dental facility owners can consider insurance companies, and an arrangement may be negotiated to mitigate the financial difficulties that have been previously discussed.
Governments can also offer support through loans, mortgages, and rental payments.43,69 Federal Emergency Powers in the United States (US) have permitted the development of rules and guidelines that can help to relieve the financial impact of shutdowns due to the virus.70 Braiding and blending of public funds and consolidation between different hospitals and different healthcare providers are examples of solutions considered in the US to raise healthcare spending in the public sector.71,72
All healthcare providers should be granted health insurance and paid sick leaves, and in cases of such outbreaks, an increase in income should also be considered. Similarly, teledentistry should be covered by insurance to ensure its sustainability.
Research and Innovation
The world and the field of dentistry will never be the same after the COVID-19 outbreak. Studies are being carried worldwide to fully understand the nature of the new coronavirus. Clinical trials are being conducted to find a vaccine or treatment. Current studies are investigating modes of transmission, control of infection spread, and influence on dental facilities. Some researchers are investigating the effectiveness of different chemicals for disinfection or oral control of this virus.21,73 However, the impact of the current COVID-19 outbreak is expected to cause a huge shift in the direction of dental research.73 Virtual reality, artificial intelligence, and telehealthcare are some examples of expected research interests as a result of the digital transformation.73,74 It is also expected that the dental industry will witnesses a competitive trend with respect to redesigning dental units and equipment. The use of information technology to predict oral health behaviors or patterns of dental visits presents another unprecedented research area.
The SWOT analysis identifies issues but does not provide solutions or prioritization of the identified concerns. The literature review carried may have overlooked or oversimplified some data due to the limited space; thus, some bias is likely to have occurred. Additionally, this type of review analysis may have been influenced by the authors’ views on the subject.
Despite the limitations, the SWOT analysis is a useful tool to guide decision makers and practice owners.
Conclusion
Due to the sudden and spread of the current outbreak, most of the healthcare systems were not well prepared. Lack of resources, training of service providers, and difficulties with proper patient identification in addition to the nature of dental care (aerosol generation and closeness to the patients) are weaknesses that policy makers, hospital administrators, and practice owners need to prioritize in their preparedness plans. In the same context, healthcare institutions should consider the financial consequences and attrition of workforce as a result of the current outbreak in their strategic plans. Coordination and prompt communication among all healthcare providers during such outbreaks is crucial and is a strength that needs to be supported. Research and IT are great opportunities that can reimburse the losses due to the COVID-19 pandemic if they are well utilized. This paper paves the way for investigating the impact of the highlighted opportunities in controlling future outbreaks. We also expect that policy makers can use this preliminary analysis to address weaknesses and threats to satisfactory management of dental practices during this pandemic.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Disclosure
The authors declare no conflicts of interest for this work.
References
1. Ksiazek TG, Erdman D, Goldsmith CS, et al. A novel coronavirus associated with severe acute respiratory syndrome. New England j Med. 2003;348(20):1953–1966. doi:10.1056/NEJMoa030781
2. Fini MB. What dentists need to know about COVID-19. Oral Oncol. 2020;28:104741. doi:10.1016/j.oraloncology.2020.104741
3. Gomes MFC, Pastore y Piontti A, Rossi L, et al. Assessing the international spreading risk associated with the 2014 West African Ebola outbreak. Plos Currents Outbreaks. 2014 Available from: https://dx.doi.org/10.1371%2Fcurrents.outbreaks.cd818f63d40e24aef769dda7df9e0da5.
4. Heukelbach J, Alencar CH, Kelvin AA, de Oliveira WK. Pamplona de Góes Cavalcanti L. Zika Virus Outbreak in Brazil J Infect Dev Ctries. 2016;10:116–120. doi:10.3855/jidc.8217
5. Peng X, Xu X, Li Y, Cheng L, Zhou X, Ren B. Transmission routes of 2019-nCoV and controls in dental practice. Int J Oral Sci. 2020;12:9. doi:10.1038/s41368-020-0075-9
6. Izzetti R, Nisi M, Gabriele M, Graziani F. COVID-19 transmission in dental practice: brief review of preventive measures in Italy. J Dent Res. 2020:0022034520920580.
7. WHO Rolling updates on coronavirus disease (COVID-19): WHO characterizes COVID-19 as a pandemic. Available from: https://www.who.int/emergencies/diseases/novel-coronavirus-2019/events-as-they-happen.
8. Terzić Z, Vukašinović Z, Bjegović-Mikanović V, Jovanović V, Janičić R. SWOT analysis: the analytical method in the process of planning and its application in the development of orthopaedic hospital department. Srp Arh Celok Lek. 2010;138(78):473–479. doi:10.2298/SARH1008473T
9. Gürel E, Tat M. SWOT analysis: A theoretical review. J Int Social Res. 2017;10:994–1006. doi:10.17719/jisr.2017.1832
10. Finkbeiner BL. Four-Handed Dentistry: A Handbook of Clinical Application and Ergonomic Concepts. New Jersey: PrenticeHall; 2000.
11. Centers for Disease Control and Prevention. Interim infection prevention and control guidance for dental settings during the COVID-19 response; 2020. Available from: https://www.cdc.gov/coronavirus/2019-ncov/hcp/dental-settings.
12. American Dental Association. ADA interim guidance for minimizing risk of COVID-19 transmission. Available from: https://www.ada.org/~/media/CPS/Files/COVID/ADA_COVID_Int_Guidance_Treat_Pts.pdf?utm_source=cpsorg&utm_medium=covid-cps=virus-lp&utm_content=cv-pm-ebd-interim-response&utm_campaign=covid-19.
13. Dental emergency protocol during COVID-19 pandemic. Available from: https://www.moh.gov.sa/Ministry/MediaCenter/Publications/Documents/MOH-Dental-emergency-guidline.pdf.
14. Novel coronavirus english, ministry for health, malta. Available from: www.covid19health.gov.mt.
15. Coronavirus guidance not just for NHS practices, British Dental Association. Available from: https://bda.org/news-centre/blog/Pages/Coronavirus-guidance-not-just-for-NHSpractices.aspx.
16. Gambhir RS. Primary care in dentistry - an untapped potential. J Family Med Prim Care. 2015;4(1):13–18. doi:10.4103/2249-4863.152239
17. Pollack HA, Metsch LR, Abel S. Dental examinations as an untapped opportunity to provide HIV testing for high-risk individuals. Am J Public Health. 2010;100(1):88–89. doi:10.2105/AJPH.2008.157230
18. Coulthard P. Dentistry and coronavirus (Covid-19) moral decision-making. Br Dent J. 2020;228:503–505. doi:10.1038/s41415-020-1482-1
19. Dentists can register to help with state’s COVID-19 pandemic response. Available from: https://www.cda.org/Home/News-and-Events/Newsroom/Article-Details/dentists-can-register-to-help-with-states-covid-19-pandemic-response.
20. Odeh ND, Babkair H, Abu‐Hammad S, Borzangy S, Abu‐Hammad A, Abu‐Hammad O. COVID-19: present and future challenges for dental practice. Int J Environ Res Public Health. 2020;17(9):3151. doi:10.3390/ijerph17093151
21. Sabino-Silva R, Jardim ACG, Siqueira WL. Coronavirus COVID-19 impacts to dentistry and potential salivary diagnosis. Clin Oral Investig. 2020;1–3.
22. Dziedzic A, Wojtyczka R. The impact of coronavirus infectious disease 19 (COVID-19) on oral health. Oral Dis. 2020;1–4. doi:10.1111/odi.13359
23. Pereira LJ, Pereira CV, Murata RM, Pardi V, Pereira-Dourado SM. Biological and social aspects of coronavirus disease 2019 (COVID-19) related to oral health. Braz Oral Res. 2020;34:e041. doi:10.1590/1807-3107bor-2020.vol34.0041
24. COVID-19 and violence against women what the health sector/system can do. Available from: https://apps.who.int/iris/bitstream/handle/10665/331699/WHO-SRH-20.04-eng.pdf.
25. El Tantawi M, Gaffar B, Arheiam A, et al. Dentists’ intention to report suspected violence: a cross-sectional study in eight Arab countries. BMJ Open. 2018;8(3):e019786. doi:10.1136/bmjopen-2017-019786
26. Fallahi HR, Keyhan SO, Zandian D, Kim SG, Cheshmi B. Being a front-line dentist during the Covid-19 pandemic: a literature review. Maxillofac Plast Reconstr Surg. 2020;42:12. doi:10.1186/s40902-020-00256-5
27. Gamio L. The workers who face the greatest coronavirus risk. Available online: https://www.nytimes.com/interactive/2020/03/15/business/economy/coronavirus-worker-risk.html?action=click&module=Top+Stories&pgtype=Homepage.
28. Benzian H, Niederman R. A dental response to the COVID-19 pandemic Safe Aerosol-Free emergency(SAFER) dentistry. Front. Med.2020;7:520.
29. Ge ZY, Yang LM, Xia JJ, Fu XH, Zhang YZ. Possible aerosol transmission of COVID-19 and special precautions in dentistry. J Zhejiang Univ-SCI B. 2020;16:1–8.
30. Koutras S, Govender S, Wood NH, Motloba PD. COVID-19 pandemic and the dental practice. S Afr Dent j. 2020. 75. 3. 119–125. doi:10.17159/2519-0105/2020/v75no3a1
31. Briggs L. Dental practice during a pandemic. BDJ Team. 2020;7(4):20–21. doi:10.1038/s41407-020-0288-y
32. Ren YF, Rasubala L, Malmstrom H, Eliav E. Dental care and oral health under the clouds of COVID-19. JDR Clin Transl Res. 2020;5:202–210. doi:10.1177/2380084420924385
33. Ather A, Nikita B, Ruparel NB, Diogenes A, Hargreaves KM. Coronavirus disease 19 (COVID-19): implications for clinical dental care. J Endod. 2020;46:5. doi:10.1016/j.joen.2020.03.008
34. Halepas S, Ferneini EM. A pinch of prevention is worth a pound of cure: proactive dentistry in the wake of COVID-19. J Oral and Maxillofa Surg. 2020;78(6):860–861. doi:10.1016/j.joms.2020.03.036
35. Everett J, Colombatto C, Chituc V, Brady WJ, Crockett M. The effectiveness of moral messages on public health behavioral intentions during the COVID-19 pandemic. PsyArXiv 2020.
36. Fulford MR, Stankiewicz NR. The regulation of infection control. In: Infection Control in Primary Dental Care. Springer International Publishing; 2020:
37. Fulford MR, Stankiewicz NR. The concept of decontamination in dentistry. In: Infection Control in Primary Dental Care. Springer International Publishing; 2020:
38. Lok V, Kruger E, Tennant M. Patient complaints in dentistry: a western Australian retrospective analysis-19962004. Asia Pacific J Health Management. 2007;2(2):34.
39. Calisher C, Carroll D, Colwell R, et al. Statement in support of the scientists, public health professionals, and medical professionals of China combatting COVID-19. Lancet. 2020;395:e42–3. doi:10.1016/S0140-6736(20)30418-9
40. Adams JG, Walls RM. Supporting the health care workforce during the COVID-19 global epidemic. JAMA. 2020;323(15):1439–1440. doi:10.1001/jama.2020.3972
41. Dave M, Seoudi N, Coulthard P. Urgent dental care for patients during the COVID-19 pandemic. Lancet. 2020;395:1257. doi:10.1016/S0140-6736(20)30806-0
42. Saltaji H, Sharaf KA. COVID-19 and orthodontics: a call for action. Am J Orthod Dentofacial Orthop. 2020;158(1):12–13. doi:10.1016/j.ajodo.2020.04.006
43. Ferneini EM. The financial impact of COVID-19 on our practice. J Oral Maxillofac Surg off J Am Assoc Oral Maxillofac Surg. 2020;78:1047–1048. doi:10.1016/j.joms.2020.03.045
44. Nasseh K, Vujicic M. Modeling the impact of COVID-19 on U.S. dental spending. Health policy institute research brief. American dental association; April 2020. Available from: https://www.ada.org/~/media/ADA/Science%20and%20Research/HPI/Files/HPIBrief_0420_1.pdf?la=en.
45. IDA News. Scale of dental collapse highlighted in survey. Available from: http://irish dental association. newsweaver. com/newsletter/13ct csav 7cz1 cys2 2xtzj2? a= 1& p= 56657247& t= 22322575.
46. Radonovich LJ, Simberkoff MS, Bessesen MT, et al. N95 respirators vs medical masks for preventing influenza among health care personnel: a randomized clinical trial. JAMA. 2019;322(9):
47. Hafizi D, Walter M, MacDougall. Masks During Aerosol Generating Dental Procedures: Clinical Effectiveness and Guidelines. Ottawa: CADTH; 2020. Mar. CADTH rapid response report.
48. Meng L, Hua F, Bian Z. Coronavirus disease 2019 (COVID‐19): emerging and future challenges for dental and oral medicine. J Dent Res. 2020;22034520914246. doi:10.1177/0022034520914246
49. Guo H, Zhou Y, Liu X, Tan J. The impact of the COVID-19 epidemic on the utilization of emergency dental services. J Dent Sci. 2020;0–3. https://doi.org/10.1016/j.jds.2020.02.002.
50. Yang Y, Zhou Y, Liu X, et al. Health services provision of 48 public tertiary dental hospitals during the COVID-19 epidemic in China. Clin Oral Invest. 2020;24:1861–1864. doi:10.1007/s00784-020-03267-8
51. Yu J, Zhang T, Zhao D. Characteristics of endodontic emergencies during COVID-19 outbreak in Wuhan. J Endod. 2020;46:730–735. doi:10.1016/j.joen.2020.04.001
52. Ahmed MA, Jouhar R, Ahmed N, et al. Fear and practice modifications among dentists to combat novel coronavirus disease (COVID-19) outbreak. Int J Environ Res Public Health. 2020;17(8):2821. doi:10.3390/ijerph17082821
53. Cianetti S, Pagano S, Nardone M, Lombardo G. Model for taking care of patients with early childhood caries during the SARS-Cov-2 pandemic. Int J Environ Res Public Health. 2020;17:3751. doi:10.3390/ijerph17113751
54. Berlin-Broner Y, Levin L. Dental hierarchy of needs’ in the COVID-19 era-or why treat when it doesn’t hurt. Oral Health Prev Dent. 2020;18(2):95.
55. Casamassimo PS, Townsend JA, Litch CS. Pediatric dentistry during and after COVID-19. Pediatr Dent. 2020;42:87–90.
56. Arduino PG, Conrotto D, Broccoletti R. The outbreak of Novel Coronavirus disease (COVID-19) caused a worrying delay in the diagnosis of oral cancer in north-west Italy: the turin metropolitan area experience. Oral Dis. 2020. doi:10.1111/odi.13362
57. Goodman JL, Borio L. Finding effective treatments for COVID-19: scientific integrity and public confidence in a time of crisis. JAMA. 2020;323:1899–1900. doi:10.1001/jama.2020.6434
58. Tao ZY, Chu G, McGrath C, et al. Nature and diffusion of COVID-19–related oral health information on Chinese social media: analysis of tweets on weibo. J Med Internet Res. 2020;22(6):e19981. doi:10.2196/19981
59. Wu Z, McGoogan JM. Characteristics of and important lessons from the coronavirus disease 2019 (COVID-19) outbreak in China: summary of a report of 72 314 cases from the chinese center for disease control and prevention. JAMA. doi:10.1001/jama.2020. 2648
60. Jones DS. History in a crisis—lessons for Covid-19. N Engl J Med. 2020;382:1681–1683. doi:10.1056/NEJMp2004361
61. Plessas A, Delgado MB, Nasser M, Hanoch, David Y, Moles R. Impact of stress on dentists’ clinical performance. A systematic. Community Dent Health. 2018;35:9–15. doi:10.1922/CDH_4118Plessas07
62. Ahmad, Tabrez, Corona Virus (COVID-19) pandemic and work from home: challenges of cybercrimes and cybersecurity. Available from: http://dx.doi.10.2139/ssrn.3568830.
63. Maret D, Peters OA, Vaysse F, Vigarios E. Integration of telemedicine into the public health response to COVID-19 must include dentists. Int Endod J. 2020;53:880–881. doi:10.1111/iej.13312
64. Cook J, Austen G, Stephens C. Videoconferencing: what are the benefits for dental practice? Br Dent J. 2000;188:67–70. doi:10.1038/sj.bdj.4800391
65. Villa A, Sankar V, Shiboski C. Tele (oral) medicine: a new approach during the COVID-19 crisis. Oral Dis. 2020. doi:10.1111/odi.13364
66. Wu M, Chang YC. COVID-19 and its implications in the management of resource infrastructure [published online ahead of print, 2020 Apr 26]. J Dent Sci. 2020;15(2):225–226. doi:10.1016/j.jds.2020.04.008
67. Machado RA, De Souza NL, Oliveira RM, Júnior HM, Bonan PRF. Social media and telemedicine for oral diagnosis and counselling in the COVID-19 era. Oral Oncol. 2020;105:104685. doi:10.1016/j.oraloncology.2020.104685
68. Offner D, Fernandez De Grado G, Strub M, Belotti L, Deboscker S, Musset AM. Mobile dental delivery system: an effective protocol for hygiene and disinfection. Int J Environ Res Public Health. 2020;17:1603. doi:10.3390/ijerph17051603
69. Darwish S. COVID-19 Considerations in Dental Care. Dent Update. 2020;47:287–302. doi:10.12968/denu.2020.47.4.287
70. Gostin LO, Hodge JG, Wiley LF. Presidential powers and response to COVID-19. JAMA. 2020;323:1547. doi:10.1001/jama.2020.4335
71. Butler SM. After COVID-19—thinking differently about running the health care system. JAMA Health Forum. 2020;1:e200478. doi:10.1001/jamahealthforum.2020.0478
72. Cutler DM, Nikpay S, Huckman RS. The business of medicine in the era of COVID-19. JAMA. 2020;323:2003–2004. doi:10.1001/jama.2020.7242
73. Chan WCW. Nano research for COVID-19. ACS Nano. 2020;14(4):3719–3720. doi:10.1021/acsnano.0c02540
74. Joda T, Bornstein MM, Jung RE, Ferrari M, Waltimo T, Zitzmann NU. Recent trends and future direction of dental research in the digital era. Int J Environ Res Public Health. 2020;17:1987. doi:10.3390/ijerph17061987
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.