Back to Journals » Clinical, Cosmetic and Investigational Dentistry » Volume 16
Dental Clinicians’ and Technologists’ Experiences and Perspectives on Removable Complete Denture Fabrication Services in Makerere University Dental Hospital, Uganda
Authors Nono D ![]() , Akugizibwe M, Bagenda G, Okullo I, Rwenyonyi CM
, Akugizibwe M, Bagenda G, Okullo I, Rwenyonyi CM
Received 9 September 2024
Accepted for publication 3 December 2024
Published 6 December 2024 Volume 2024:16 Pages 499—511
DOI https://doi.org/10.2147/CCIDE.S495315
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Christopher E. Okunseri
David Nono,1– 4 Mathias Akugizibwe,5 Godfrey Bagenda,6 Isaac Okullo,3 Charles Mugisha Rwenyonyi3
1Department of Clinical Research, Central University of Nicaragua, Managua, Nicaragua; 2Department of Clinical Research, Texila American University, Georgetown, Guyana; 3Department of Dental Technology, Makerere University, Kampala, Uganda; 4Department of Research, Uganda Institute of Allied Health and Management Sciences-Mulago, Kampala, Uganda; 5Department of Research, Medical Research Council/Uganda Virus Research Institute & London School of Hygiene and Tropical Medicine, Kampala, Uganda; 6Department of Anatomy, Makerere University, Kampala, Uganda
Correspondence: David Nono, Department of Dental Technology, Makerere University, Kampala, Uganda, Tel +256773502059; +256701909347, Email [email protected]
Background: Globally, there is growing concern regarding mouth sores, occlusion, cost, ridge resorption, and retention, in the delivery of removable complete dentures fabrication services brought about by the aging of the population and poor oral healthcare. The therapy for edentulous patients can be realized through the use of conventional removable complete dentures, implant-supported prostheses, and computer-aided design/computer-aided manufacturing (CAD/CAM). In Uganda, the therapy for edentulous patients has predominantly been realized through the use of conventional removable complete dentures. There has been a discernible difference in the number of visits and remake rate between removable complete dentures that were made conventionally and digitally. This present study, therefore, aimed to explore dental clinicians’ and technologists’ experiences and perspectives on removable complete denture fabrication services.
Methods: The study employed a qualitative design, 25 in-depth interviews were conducted with dental clinicians and technologists at Makerere University Dental Hospital. Both practicing dental technologists and clinicians were purposively selected after providing written informed consent. Interviews’ audios were transcribed verbatim, coded in NVivo 14 and data were analyzed thematically.
Results: Clinical and socio-demographic assessments like age, oral hygiene, ridge level, underlying health conditions, and mental stability of the patient were done by dental clinicians before removable complete denture fabrication. Dental technologists and clinicians mentioned patients having a lot of expectations relating to being able to eat whatever they like and improving physical appearance. However, the patients also had fears and concerns about discomfort, and some worried that they would swallow the dentures.
Conclusion: Prior assessments were the basis for planning for complete denture therapy. Patients’ fears and expectations can effectively be addressed in the consent process since adequate information can be shared and the patients can be psychologically prepared to receive the denture treatment.
Keywords: complete denture therapy, computer-aided design, computer-aided manufacturing, dental technologists, dental clinicians
Introduction
Removable Complete Denture (RCD) fabrication services are becoming increasingly important on a global scale as a result of the improved lifespan of the population and inadequate preventive services.1 The therapy for edentulous patients can be realized through the use of conventional removable complete dentures (RCDs), implant-supported prostheses, and computer-aided design/computer-aided manufacturing (CAD/CAM).2,3 According to Clark et al,1 there has been a discernible difference in the number of visits and remake rate between RCDs that were made conventionally and digitally.
The usage of CAD/CAM technology has significantly increased as a result of quick delivery services of various dental restorations.4 Additionally, advancements in partially or fully digital workflows have made it possible to fabricate RCD in fewer, shorter sessions and with the use of materials that have better qualities.5 Moreover, it has been demonstrated that CAD/CAM-based RCDs release less monomer than traditional RCDs, which has several benefits with regard to practical applicability.6 Studies showed that the use of CAD/CAM technology has demonstrated promise for streamlining the fabrication procedure and enhancing RCD fitness and retention,7 which have a major impact on patients’ speech and masticatory abilities, and eventually improve their quality of life.8
In Uganda, the therapy for edentulous patients has predominantly been realized through the use of conventional complete dentures. The fabrication of a complete denture entails several steps, which include diagnosis, treatment planning, impression taking and border molding, dental model casts and occlusal rim blocks, bite registration, selection and set-up of artificial teeth, wax denture try-in, and denture processing and insertion.9
Despite the Uganda National Oral Health Policy,10 which recommends the fabrication of RCDs for the treatment of edentulous patients using internationally accepted guidelines,10 there are no published data on the experiences of technologists or clinicians in the fabrication of RCD. The aim of the present study was to explore the experiences and perspectives of dental clinicians and technologists in RCD fabrication services at Makerere University Dental Hospital, Uganda.
Materials and Methods
Study Design
The study employed a qualitative design to explore the experiences of RCD fabrication services among dental clinicians and technologists. It was conducted using in-depth interviews of dental clinicians and technologists guided by data saturation.
Study Site
The study was conducted in Makerere University Dental Hospital in Kampala. Kampala is the capital city of Uganda. The hospital is a teaching and health service delivery facility of Makerere University. It is the largest and adequately equipped dental facility employing the highest number of dental specialists in Uganda. It has a well-established prosthetic dental laboratory and offers specialized dental services including rehabilitation of edentulous patients with RCD mostly staff and students of the University and other communities outside the University at a minimal fee. The hospital attends to approximately 660 outpatients per month, of which about 20 are rehabilitated using RCD (Registry of Dental Records, 2022). The selected participants were actively practicing dentistry, particularly in the area of RCD fabrication.
Selection of Study Participants
Purposive sampling was used to select key informants in consideration of areas of their clinical services. The selection also included variation in duration of practice, level of training, roles in denture fabrication procedures, and fitting to ensure a fair representation of the study population. The last key informants (13th dental clinician and 12th technologist) were determined based on data saturation, where continuing to collect more data would not yield any new insights or codes.
Inclusion Criteria
Dental clinicians and technologists participating in the provision of RCDs in Makerere University Hospital.
Exclusion Criteria
Dental clinicians and technologists who were sick and unable to participate in the study.
Data Collection
Before participating in the study, written informed consent was provided by the participants. They were assured of confidentiality such that no identifiers like names were used in data collection and preparation of reports. The research assistants personally approached dental practitioners to invite them to participate in the study. The interviews were conducted in a conducive environment preferred by the participants, ensuring confidentiality and privacy in the comfort of the participants to share their insights. The interview comprised open-ended questions with probes to prompt dialogue and unmediated opinions on aspects of experiences and perspectives toward RCD fabrication. Data collection and the subsequent analysis were conducted as an interactive process. The last participant for IDI was established by informational redundancy, ie when the discussion or interview generated no new information.11,12 The interview for each respondent took 30 to 45 minutes and was audio-recorded. This was done with the help of a trained research assistant with a background in social sciences and experience in qualitative research.
Quality Control
The data collection tools were pretested by the principal investigator, and amendments were made to improve their validity and reliability. The research assistant was trained in data collection. The key informant interviews were audio-recorded to capture any discussion that may have been missed in taking notes. Additional notes capturing body language and gestures during the interviews were also recorded. To guarantee reliability, four standards were applied: credibility, confirmability, dependability, and transferability. Peer debriefing and enlisting the assistance of more seasoned qualitative researchers who evaluated and provided feedback on the study technique and findings to guarantee that the data were correct and pertinent helped to establish credibility. The research background, including the features of the chosen individuals and environment, is thoroughly explained in the methods section. The detailed description of the techniques and analysis employed allowed for the replication of the study. In order to ensure that the research study’s conclusions were unbiased and founded on the testimonies and statements of the participants, a clearly defined coding scheme was used to generate codes and identify trends in the analysis.
Data Management and Analysis
Data management involved the transcription of interview verbatim recordings. Data were analyzed thematically.13 This happened in the context that, after transcription, the 25 transcripts: 12 for the dental technologists and 13 for the dental clinicians were read and re-read by a social scientist with a qualification of a Bachelor’s degree in Sociology for purposes of familiarizing with the data and to identify the emerging sub-themes and themes. The social scientist presented the sub-themes to the rest of the research team where these were discussed and adopted as guiding codes for data coding in NVivo.14. The coded data was used to generate the coding summary reports, which were read by the social scientist to identify the emerging themes. At this level, some of the sub-themes that compared similar in data content were merged into one theme, while those that contained identical data were adopted. The agreed upon themes were revised and named to ensure that they are accommodative and representative of our data. The final themes were adopted and used to present and interpret our findings, while evidenced by personal experiences of the participants that were captured as individual quotes.
Ethical Considerations
Ethical approval of the protocol was obtained from the Makerere University School of Health Sciences Research and Ethics Committee (Reference Number: MAKSHSREC-2023-486) as well as the Uganda National Council for Science and Technology (Reference Number: HS3092ES). Permission to carry out the study was obtained from the administration of Makerere University Dental Hospital. Written informed consent, which included publication of anonymized responses/direct quotes, was obtained from all the participants who took part in the study in accordance with the Helsinki Declaration.14 All the data collected were kept securely in a cabinet under lock and key and only accessible to the investigator.
Results
The study involved 25 respondents with varying demographic characteristics. Eighteen were male while 7 were female. All the respondents had either a Bachelor in Dental Surgery or a Bachelor of Dental Technology: Thirteen were registered dental clinicians (surgeons) and 12 dental technologists. Most of the participants were in the age range of 26–35 years (Table 1).
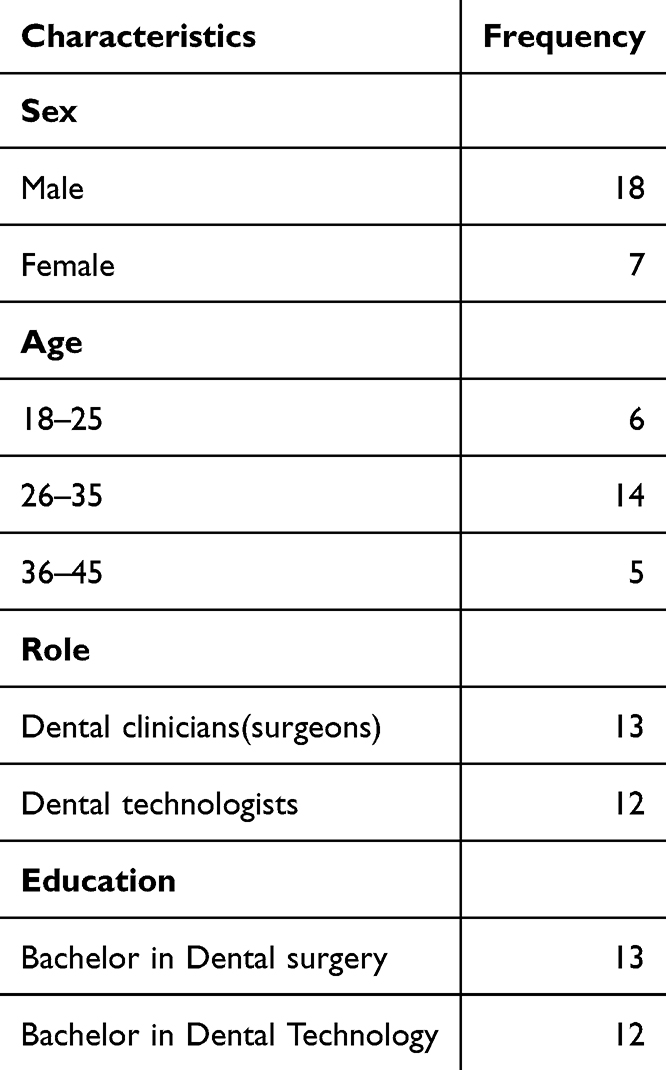 |
Table 1 Participant Socio-Demographics (N = 25) |
Three themes emerged from the data (Table 2).
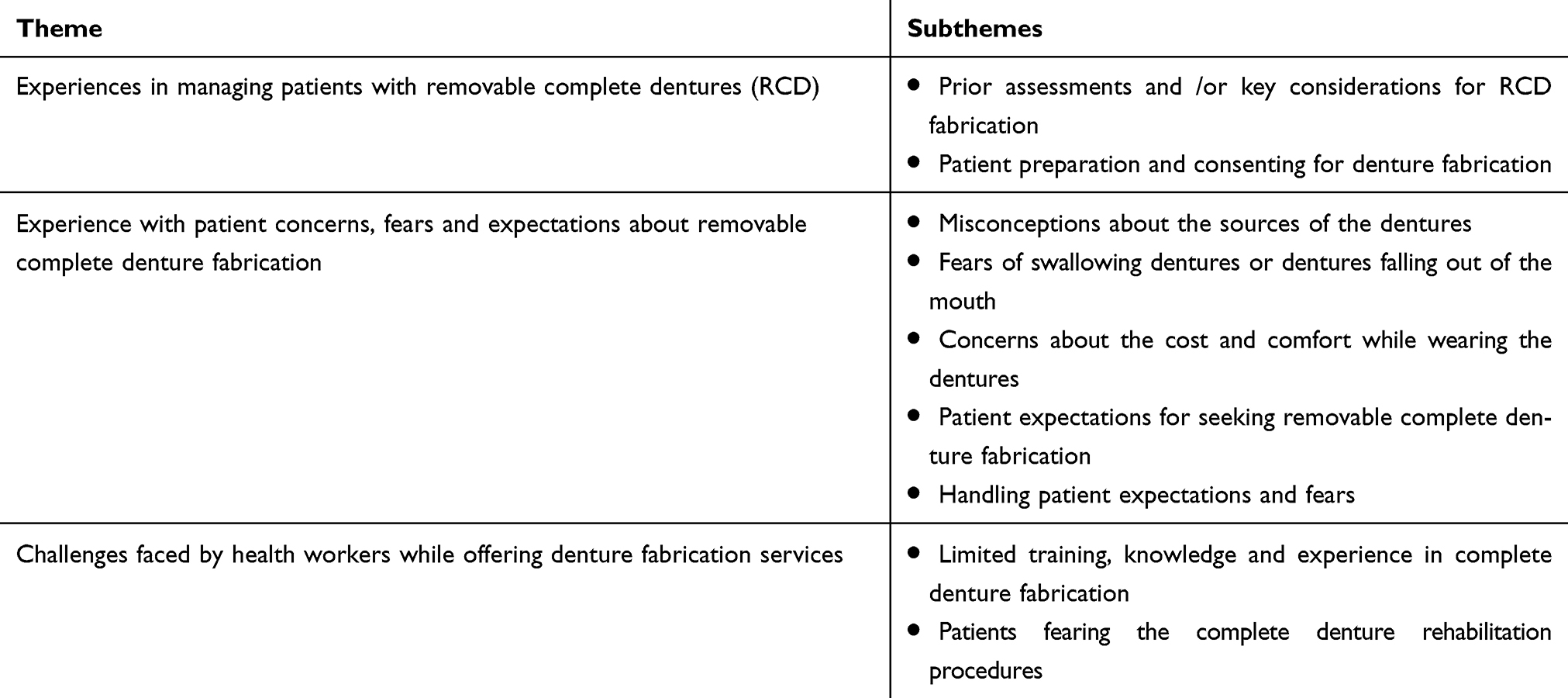 |
Table 2 Themes and Subthemes |
Experiences in Managing Patients with Removable Complete Dentures (RCD)
Prior Assessments and /or Key Considerations for RCD Fabrication
When asked to describe how they determine whether a patient is fit to receive RCD, participants mentioned two key categories of considerations, namely, clinical and socio-demographic assessments or considerations. In terms of clinical assessments or considerations, dental practitioners reported that they consider the underlying conditions that could be associated with loss of teeth or how to manage post-insertion activities. Conditions like the morphology of the ridges, oral hygiene, and if the patient is living with diseases, for example, diabetes, hypertension, and ulceration might propel the dental practitioners to make very critical considerations before recommending RCD fabrication. Sometimes they recommended not to fabricate RCD at all if the patient’s conditions were not good, but also, if they discovered that RCD may lead to severe management outcomes, they did not advise the patient to opt for RCD. The details are given below:
For some patients with a condition which is not well managed like Diabetes Mellitus, it affects the soft tissues of the periodontium and such conditions must be put into consideration. (P001_40-year-old_ Male _dental surgeon)
The oral hygiene of the patient was also a key factor to consider:
The key factor that must be observed whenever we provide removable complete denture is the oral hygiene because if your oral hygiene is not ideal you will misuse or will not take care of the complete denture. (P001_40-year-old_ Male _dental surgeon)
Equally, assessing whether the mouth has been prepared to receive the RCD or not was a key consideration. It was revealed that in cases of loss of teeth due to accidents, one would require the wounds to first heal and also to ensure that all the retained roots have been extracted:
You examine the patient’s mouth to determine whether he or she qualifies for a complete denture, and then you do mouth preparation. You remove any retained roots and give the patient 3 months for the wounds to adequately heal before starting complete denture fabrication processes. (P001_40-year-old_ Male _dental surgeon)
Relatedly, the morphology of the patient’s ridge also determines whether to have RCD fabrication or not or whether to use denture adhesives or implant support:
First of all, I look at the ridge and decide if it favors a complete denture in terms of height and width for support, retention, and stability. (P023_26 year-old_Male_dental surgeon)
The mental stability of the patient was also a key clinical consideration before recommending a complete denture fabrication.
For any patient getting a complete denture, they should be mentally ready to have it [denture]. (P002_42 year-old_Female_dental surgeon)
The other key demographic consideration is the age of the patient. Participants revealed that because some patients who needed complete dentures were the elderly, there were concerns regarding their ability to adjust to living with and maintaining the appliances, which may not be possible.
I had a patient whose relatives wanted to offer her an RCD and they did all that it took; they paid the money and the appliance was delivered, but the old woman threw the appliance away because she said that at her age she does not need it. (P001_40-year-old_ Male _dental surgeon)
Similarly, another participant narrated:
Most of them are elderly patients, some having other conditions like high blood pressure and diabetes mellitus, and even some of them having psychotic problems, which may be a challenge for them to follow the instructions of using complete dentures. (P003_43 year-old_Male_dental surgeon)
Other considerations included patients with periodontitis or sometimes the grade of the teeth mobility (grade two or three) was reported to influence the decision to either make a complete denture or not.
Patients who have teeth that are periodontally compromised to grade three mobility, but not for removal because the patient is not mentally ready… those are hopeless. But if the teeth have grade-two mobility, one can leave them and make for them transitional dentures. (P013_25_year-old_Female_ dental intern)
Patient Preparation and Consenting for Denture Fabrication
To broaden our understanding of the knowledge and experiences of dental practitioners who offer denture fabrication services, we took an interest in exploring whether and how the patients are prepared and consented before the procedures are done. Our study revealed that before the decision to have the patient undergo denture fabrication, dental practitioners indicated many key steps that are taken into account. Among many, the willingness of the patient and consenting to the procedures was key. Also, patients are given enough information, especially for them to know that the appliance is removable and will need to be cleaned. For some categories of patients like the old and those with mental health problems, the dental practitioners ensure that the caretakers are involved in all the procedures. Given that the complete dentures are foreign to the human body, dental practitioners ensure that patients are also told about the likely inconvenience that involves the dentures in order to get prepared to adjust and live with them.
We always tell them about the discomfort of the denture during chewing, the possibility of roughness that could injure the gum, the bulkiness that may restrict tongue movement, and keeping it clean. However, with time they get used to the dentures. (P003_43 year_Male dental surgeon)
Some dental practitioners talked about the duration and the fees it will take for the patient to have their dentures fixed as another factor to consider, thus the participant elaborated:
You make patients aware [that,] for example, this is going to take a long time to accomplish. Then for the payment of money, you can tell, them, to keep saving, to pay for the costs involved. (P014_23 year-old_Female_dental surgeon)
While consenting patients, the focus is largely on giving the patients as much information as possible to ensure that they clearly understand all it takes. The common information provided relates to the benefits, side effects, and the cost of treatment.
We explain every procedure to the patients. The other issue is monetary expenses because you explain to them how much it costs, and so on. (P001_40 year-old_Male dental surgeon)
We do this for all patients who need dentures because we have to explain to them the benefits, but also the side effects of complete dentures. (P002_42 year-old_Female dental surgeon)
However, as opposed to other forms of consent that are normally sought, some dental practitioners revealed that they do not give written informed consent, but rather, implied consent.
Not entirely written informed consent, but most times when they come, that is implied consent. They tell you what they want for, example, tooth replacement and so you let them know what you’re going to do for them and your expectations, and if they’re ready for that treatment, you go on and provide it. (P013_25_year-old_Female dental surgeon)
As part of the consenting process, dental practitioners’ focus is always on providing details like the advantages, disadvantages, risks, and visual demonstrations of how the denture looks and how to care for the denture. The implication of this is that the patients make informed decisions.
I first tell them about the treatment for example, I bring an actual denture so they can see how it looks like or show them photographs or videos. Then, I educate them about the advantages, disadvantages, risks, and complications of dentures. I also educate them on denture care. (P014_23 year-old_Female_dental surgeon)
Another participant also revealed that the consent they obtained was not comprehensive enough to qualify as informed consent. The participants were given little information and not in detail. As it is supposed to be.
I try, but from the informed consent I know, it is not complete. We just tell the patient what a complete denture is, the advantages and disadvantages, and not so much information. That is why I’m saying it’s not complete. (P015_31_year-old_Male dental surgeon)
In some cases, dental practitioners conceal some information so that the patient is only given the information that will propel them to accept the denture procedures if the dental practitioner thinks that it will help the patient.
There are some instances where I tend to withhold some information from the patient because I want them to benefit or to get at least the best option. Let me say, I drive them to something that will benefit them. (P018_30 year-old_Male dental surgeon)
Some participants admitted that although written consent would be the best, they do not document the processes, but rather they mostly do verbal consenting.
Truth be told, we don’t usually document informed consent. We usually tell patients what procedure we are going to do. (P023_26 year-old_Male_dental surgeon)
Experience with Patient Concerns, Fears and Expectations About Removable Complete Denture Fabrication
Misconceptions About the Sources of the Dentures
Participants revealed several perceptions that patients have about the RCD. Some fears were linked to misconceptions and rumors. One of the participants indicated that some patients came thinking they would be given teeth that are plucked out of the corpses of white people as stated:
Yes, there are many concerns, some patients said they think we go and pick these teeth from dead bodies. (P001_40 -year-old_Male dental surgeon)
Fears of Swallowing Dentures or Dentures Falling Out of the Mouth
Dental practitioners mentioned that patients feared that maybe at some point, while asleep or eating, they could easily swallow the dentures and end up suffocating. Also, some patients were worried that there could be an incident where the dentures could fall out in public, especially when the person is speaking.
Some patients actually think they will swallow the dentures and suffocate. Then the other fear could be when they are speaking in public, these dentures could fall out of their mouths. (P002_42-year-old_Female_dental surgeon)
Concerns About the Cost and Comfort While Wearing the Dentures
Participants further revealed that patients also worried about how comfortable they would be after getting the complete denture. Some patients fear that wearing complete dentures could have health implications, fearing that it may cause cancer on top of fearing that they could easily swallow the dentures by accident.
We have had cases where clients have said that they fear complete dentures can cause certain illnesses like cancer. We have had cases where patients who think they can swallow the dentures. (P004_33-year-old_Male_dental surgeon)
Regarding the discomfort, some complained that the complete dentures were sometimes too much extended especially the upper side, which caused the mouth to start feeling heavy.
Some patients were complaining that they feel the mouth is heavy while others also felt the dentures especially, the upper one was overly extended. (P001_40-year-old_Male_dental surgeon)
Equally, technologists expressed that most patients feared the associated costs of having a complete denture but also feared that the material from which the dentures are made could cause cancer.
There are a lot of fears that these complete dentures are way too expensive. Then sometimes they think that the material from which the complete dentures are made are not bio-compatible and can cause cancers. (P020_34-year-old_Male_dental surgeon)
Some patients feared the size of the dentures, especially when the dental practitioners were demonstrating to them, they worried about how the dental practitioners would manage to fix it in their mouth. They feared that they may not eat well seeing that the size of the denture was big.
Sometimes when you’re explaining to them you have to have also a kind of sample to show them how it looks like. So, a person will see and say; doctor this thing looks big, will I be able to use it? (P002_42 year-old_Female_dental surgeon)
Patient Expectations for Seeking Removable Complete Denture Fabrication
We also aimed to understand from the dental practitioners what the patients’ expectations are when they come for removable complete denture services. Our findings revealed several expectations that patients had. Largely, patients were expectant that they would be able to have their beauty, especially when they smile, restored so that they were able to speak freely in public, and since most of them had stopped eating certain foods, they expected to start eating foods like meat after having their dentures.
I want my smile again, eat meat, and speak freely in public. These are some of the things that lower someone’s self-esteem. (P001_40 year_old_Male- dental surgeon)
Some dental practitioners revealed to have encountered female patients who wanted to have dentures so that they could restore their physical appearances to attract men and give birth to children and also get job opportunities, which they thought to have missed because of having no teeth. In this case, self-esteem was always key for the patients.
Many of the patients are looking out to restore cosmetic appearance. A thirty-year-old woman with no teeth blamed her entire life on the fact that she didn’t have a husband and children because she didn’t have teeth a child. This psychologically affected her. (P002_42 year-old-Female-dental surgeon)
Another patient also revealed similar insights indicating:
They said it has been a while without having teeth and they just want to look younger and more beautiful in order to prepare a date. (P007_27 year-old_Male-dental surgeon)
A few participants narrated that some patients have the desire to look even better than they used to look before they lost their teeth. They have a belief that dental practitioners can fabricate the dentures and make them look much better than they used to look. Other patients seek services to restore their teeth that look exactly like their lost ones.
They come with a lot of expectations in that someone would want you to place teeth that exactly look like what they had lost. They will expect to function normally like the way they used to speak. (P003_43 year-old_Male_dental surgeon)
In preference, some of the patients do not expect to receive removable dentures, but rather, they expect to receive fixed dentures that are permanent. Besides, some patients expect to spend very little time at the clinic. Some health workers attributed the patients’ high expectations to limited knowledge about the denture fabrication procedures.
Handling Patient Expectations and Fears
Given the dental practitioners’ observation that most patients come with high expectations due to the limited knowledge about RCD fabrication. Comprehensive counseling is very key in handling patients’ high expectations.
When the patients come, I will have to counsel them that what they are going to get is not going to be like their natural teeth. (P003_43-year_Male_dental surgeon)
Also, while explaining to the patients, the focus is put on detailed information that eliminates fears, for example, information about the dentures falling out, and eating limitations.
If somebody came fearing the adverse effect of cancer, you counsel him/her with assurance that dentures do not cause the same. (P004_33 year-old_Male_dental surgeon)
We explain and assure them that they can’t swallow the dentures and as long as the denture has been well made, it should not even fall out in public when they are speaking. We explain to them there are things that they cannot eat like meat unless it is well cooked. (P002_42 year-old_Female_dental surgeon)
Dental practitioners do explain to the patients in simple language for easy and quick comprehension.
In most cases, we give them adequate information in simple language to alleviate the fears and also assure them that in the long run, they will get used to the denture. (P001_40 year-old_Male dental surgeon)
Challenges Faced by Health Workers While Offering Denture Fabrication Services
Limited Training, Knowledge and Experience in Complete Denture Fabrication
Participants revealed that they experienced a lot of practical and knowledge-related challenges. These included limited knowledge about denture fabrication among practitioners. Equally, some dental practitioners reported working with inexperienced staff who are not well trained in complete denture fabrication. To them, this hinders the delivery of quality services in the process of denture fabrication. One of the health workers noted this to be a very big gap in the professional service:
There is a big gap in the lower cadres who are not formally taught about complete dentures, but yet, they are treating patients with complete dentures, which has messed up the quality, the professionalism of the whole process. (P001_40 year-old_Male_dental surgeon)
Patients Fearing the Complete Denture Rehabilitation Procedures
Some dental practitioners reported to have experienced challenges related to patients who fear the procedures and are tense, which sometimes leads to poor positioning and eventually poor impressions. One of the participants revealed that when the patient is not relaxed, it becomes hard to make a proper impression.
You want to take the impression, but the patient is not relaxed. If you tell them to bite in centric occlusion on occlusal bite block, they can give you different bites to the extent that you always fail in getting accurate measurements. (P003_43 year-old_Male_dental surgeon)
Discussion
The present study established the baseline data of the experiences and perspectives of RCD fabrication services among dental clinicians and technologists that could be used for related future studies. Several themes relating to experiences in managing patients with removable complete dentures; experience with patient concerns, fears and expectations about removable complete denture fabrication; and challenges faced by health workers while offering denture fabrication services were explored.
While demonstrating that knowing the patient’s unique demands like occlusal rim block (ORB) height, denture retention, esthetics and state of oral health is essential before beginning the complete denture construction process, our findings are consistent with those of other studies.15 It is worth noting that since good treatment planning has an impact on the process outcomes, dental clinicians and technologists must perform comprehensive assessments of patient’s oral hygiene, dental impressions, and radiographic evaluations.
In support of previous studies,16 the present study discovered that effective communication and patient education are essential for preparing individual patients for the denture fabrication process. Therefore, beyond verbal and implied consent, which were sometimes accepted by patients, clinicians and technologists need to engage patients in a thorough consenting process to aid informed decision-making.17 This can be through explaining the steps involved, potential benefits and risks, and expected outcomes of denture treatment.18 After all, obtaining informed consent ensures that patients understand the nature of the procedure, their role in the treatment process, and the expected outcomes, thus promoting patient satisfaction and adherence to treatment and denture management plans.15
In the present study, dental professionals stated that RCD provides several advantages to edentulous patients, including enhanced masticatory function, self-esteem, and general quality of life. This finding was in line with other authors19,20 who have found comparable results like complete dentures being able to improve speech, making chewing and digestion easier, increasing self-confidence, and improving social relations by restoring oral function and beauty. Acknowledging these advantages is essential to encouraging patients to seek denture care and follow maintenance and post-treatment guidelines.21 For complete dentures to be fabricated and fitted successfully, ideal vertical and occlusal dimensions must be achieved. Evaluating aspects including patient comfort, phonetics, occlusal stability, and face aesthetics are necessary for accurate height measurement.21
In the present study, dental professionals indicated that patients were sometimes afraid of the RCD fabrication process for a variety of reasons, such as pain, discomfort, expense, and perceived functional or cosmetic constraints. Therefore, effective communication, empathy, and patient-centered treatment are necessary to address these issues. In a similar vein, other studies17 ascertained that to allay concerns and improve patient satisfaction and compliance, clinicians and technologists must pay attention to patients’ fears and anxieties and offer comfort, knowledge, and support throughout treatment. Additionally, providing individualized and patient-centered treatment requires an awareness of patients’ expectations and reasons for seeking denture fabrication.22 Dentures may be desired by patients to improve their quality of life, relieve discomfort, improve appearance, or restore oral function.23
The present study revealed mutual understanding and satisfaction of dental clinicians and technologists connected to treatment goals of patients’ expectations, preferences and values in support of previous findings. Health professionals need to foster a collaborative and multidisciplinary approach that involves clear communication, shared decision-making, ongoing feedback and evaluation because patients come to them with a variety of expectations. Furthermore, Sudheer and Vivekananda24 reported that to achieve the best results, dental technicians and clinicians must therefore customize treatment plans to each patient’s needs and preferences, answering any concerns and changing the course of action as needed. It is important to manage patient expectations by informing patients about the benefits and limitations of denture therapy, encouraging reasonable expectations and offering continuing support and direction to improve patient outcomes. However, when offering denture fabrication services, dental professionals may run into several obstacles, such as a lack of resources, technological difficulties, scheduling conflicts and patient-related issues including non-compliance or irrational expectations.25 To overcome these obstacles, creative service delivery methods, professional development, and organizational support are needed.24 Patel et al26 advised that partnerships with pertinent stakeholders and community resources together with cooperative efforts by dental practitioners, technicians, and support personnel can assist in removing obstacles and improving the caliber and accessibility of denture fabrication services.
Conclusion
The findings of the present study provided valuable insights into the experiences and perspectives of dental clinicians and technologists in managing patients with complete dentures.
Prior assessments were key in helping the dentists to ascertain the patients’ oral condition to support the complete denture treatment, and how to best plan for this treatment given the oral condition for each individual patient. It is on this basis that the dentists could best explain to the patients the state of their mouth and what will be required to make for them teeth replacements and also clearly guide them on what kind of denture they will receive, the limitations they could find while using the dentures so that they do not have unrealistic expectations so that they are prepared psychologically, implying that the consenting process is key in addressing patients fears and expectations about denture usage through providing adequate information about complete denture treatment.
Recommendations
Patient education programs should be introduced to inform the general public about removable complete denture fabrication to solve fears and anxiety. Dental professionals should offer detailed explanations to patients without reservation for them to get detailed information that would enable them to decide about having a complete denture. Regular reviews and assessments of dental practitioners’ practices should be conducted to ensure adherence to evolving best practices. These reviews can inform ongoing education initiatives and contribute to the continuous improvement of dental care quality.
Implications for Clinical Practice
While obtaining patient consent is a standard practice, the revelation that some practitioners may conceal information for motivational purposes raises ethical concerns. Dental practitioners should uphold transparent and comprehensive informed consent practices, providing patients with all necessary information to make informed decisions about their dental care. Given the impact of patient expectations and fears on the denture fabrication process, dental practitioners should prioritize effective communication and also addressing concerns and fears through detailed and understandable explanations, particularly in layman’s language.
Limitations of the Study
This was a qualitative study with a small sample size and from one health facility. In addition, all the respondents had either a Bachelor in Dental Surgery or a Bachelor of Dental Technology. It was not possible to get perspectives and experiences from dental health professionals with higher qualifications or related dental qualifications. Generalizing the results to a broader population may require caution, and future research should aim for more diverse participant representation and use mixed-method studies.
Abbreviations
ORB, Occlusal rim block; RCD, Removable complete denture.
Data Sharing Statement
Data sources are available on request. The request can be sent to the corresponding author at [email protected].
Ethics Approval and Consent to Participate
Ethical approval of the protocol was obtained from the Makerere University School of Health Sciences Research Ethics Committee (Reference Number: MAKSHSREC-2023-486) as well as the Uganda National Council for Science and Technology (Reference Number: HS3092ES). Permission to carry out the study was obtained from the administration of Makerere University Dental Hospital. Written informed consent, which included publication of anonymized responses/direct quotes, was obtained from all the participants who took part in the study. The purpose of the study was explained to the participants, and their participation was voluntary. Their agreement to participate in the study did not waive their rights in any way, and this was in accordance with the Helsinki Declaration.14 All the data collected were kept securely in a cabinet under lock and key and only accessible to the investigator.
Acknowledgments
The authors are grateful to the Government of Uganda through the Makerere University Research and Innovations Fund, the MAK-RIF secretariat for supporting this study, and participants for their willingness to participate in the study. This paper has been uploaded to Research Square as a reprint: https://www.researchsquare.com/article/rs-4362028/v1.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This research was supported by the Government of Uganda through the Makerere University Research and Innovations Fund (grant number MAK-RIF ROUND 5, 2023–2024). The views expressed herein are those of the authors and do not necessarily represent the views of the Government of Uganda, Makerere University, or the MAK-RIF secretariat.
Disclosure
The authors declare that there are no conflicts of interest.
References
1. Clark WA, Brazile B, Matthews D, Solares J, De Kok IJ. A comparison of conventionally versus digitally fabricated denture outcomes in a university dental clinic. J Prosthodontics. 2021;30(1):47–50. doi:10.1111/jopr.13273
2. Miranda BB, Dos Santos MB, Marchini L. Patients’ perceptions of benefits and risks of complete denture therapy. J Prosthodontics. 2014;23(7):515–520. doi:10.1111/jopr.12164
3. Xie Q, Ding T, Yang G. Rehabilitation of oral function with removable dentures–still an option? J Oral Rehabil. 2015;42(3):234–242. doi:10.1111/joor.12246
4. Soltanzadeh P, Suprono MS, Kattadiyil MT, Goodacre C, Gregorius W. An in vitro investigation of accuracy and fit of conventional and CAD/CAM removable partial denture frameworks. J Prosthodontics. 2019;28(5):547–555. doi:10.1111/jopr.12997
5. Maragliano‐Muniz P, Kukucka ED. Incorporating digital dentures into clinical practice: flexible workflows and improved clinical outcomes. J Prosthodontics. 2021;30(S2):125–132. doi:10.1111/jopr.13277
6. Steinmassl PA, Wiedemair V, Huck C, et al. Do CAD/CAM dentures really release less monomer than conventional dentures? Clin Oral Investig. 2017;21:1697–1705. doi:10.1007/s00784-016-1961-6
7. Baba NZ, AlRumaih HS, Goodacre BJ, Goodacre CJ. Current techniques in CAD/CAM denture fabrication. Gen Dent. 2016;64(6):23–28.
8. Steinmassl O, Dumfahrt H, Grunert I, Steinmassl PA. CAD/CAM produces dentures with improved fit. Clin Oral Investig. 2018;22:2829–2835. doi:10.1007/s00784-018-2369-2
9. Prakash P, Singh K, Bahri R, Bhandari SK. Utility versus futility of facebow in the fabrication of complete dentures: a systematic review. J Indian Prosthodont Soc. 2020;20(3):237–243. doi:10.4103/jips.jips_402_19
10. Ministry of Health. Patient’s Rights and Responsibilities Charter. 2019. Available from: http://library.health.go.ug/sites/default/files/resources/Final%20copy%20of%20the%20PATIENT%20RIGHTS%20%26%20RESPONSIBILITY%20CHARTER.pdf.
11. Guest G, Namey E, Chen M. A simple method to assess and report thematic saturation in qualitative research. PLoS One. 2020;15(5):e0232076. doi:10.1371/journal.pone.0232076
12. Hennink M, Kaiser BN. Sample sizes for saturation in qualitative research: a systematic review of empirical tests. Soc sci med. 2022;292:114523. doi:10.1016/j.socscimed.2021.114523
13. Braun V, Clarke V. Toward good practice in thematic analysis: avoiding common problems and be (com) ing a knowing researcher. Int J Transgend Health. 2023;24(1):1–6. doi:10.1080/26895269.2022.2129597
14. World Medical Association. Declaration of Helsinki: ethical principles for medical research involving human subjects. J Am Med Assoc. 2013;310(20):2191–2194. doi:10.1001/jama.2013.281053
15. Mubaraki MQ, Moaleem MM, Alzahrani AH, et al. Assessment of conventionally and digitally fabricated complete dentures: a comprehensive review. Materials. 2022;15(11):3868. doi:10.3390/ma15113868
16. Chiramana S, Ashok K. Examination, diagnosis and treatment planning for complete denture therapy–a review. J Orofacial Sci. 2010;2(3):29–35. doi:10.4103/0975-8844.103500
17. Campbell SD, Cooper L, Craddock H, et al. Removable partial dentures: the clinical need for innovation. J Prosthetic Dent. 2017;118(3):273–280. doi:10.1016/j.prosdent.2017.01.008
18. Mersel A, Carles S. Oral Health: Ethical and Clinical Concerns. In: Treatment Dilemmas for Vulnerable Patients in Oral Health: Clinical and Ethical Issues. Springer International Publishing; 2022:1–44.
19. Jain R, Pamecha S, Jain GC. Realeff-relevance in complete dentures. Int J Innov Eng Tech. 2012;1(4):44–47.
20. Cunha TR, Della Vecchia MP, Regis RR, et al. A randomised trial on simplified and conventional methods for complete denture fabrication: masticatory performance and ability. J Dent. 2013;41(2):133–142. doi:10.1016/j.jdent.2012.09.008
21. Janeva NM, Kovacevska G, Elencevski S, Panchevska S, Mijoska A, Lazarevska B. Advantages of CAD/CAM versus conventional complete dentures-a review. Open Access Maced J Med Sci. 2018;6(8):1498. doi:10.3889/oamjms.2018.308
22. Forbes-Haley C. An Investigation into Aspects of Resin Retained Bridge Design on Aesthetics and Oral Health Related Outcomes. United Kingdom: University of Bristol; 2022.
23. Lone MA, Kumar B, Musharraf H, et al. Current trends in complete denture education in undergraduate dental colleges of Pakistan. J Pak Med Assoc. 2023;73(10):2029–2035. doi:10.47391/JPMA.9710
24. Sudheer A, Reddy GV, Reddy G. Behavior shaping of complete denture patient: a theoretical approach. J Contemp Dent Pract. 2012;13(2):246–250. doi:10.5005/jp-journals-10024-1131
25. Anadioti E, Musharbash L, Blatz MB, Papavasiliou G, Kamposiora P. 3D printed complete removable dental prostheses: a narrative review. BMC Oral Health. 2020;20:1–9. doi:10.1186/s12903-020-01328-8
26. Patel J, Jablonski RY, Morrow LA. Complete dentures: an update on clinical assessment and management: part 1. Br. Dent. J. 2018;225(8):707–714. doi:10.1038/sj.bdj.2018.866
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.